


The USA has doubled its maternal morbidity and mortality rate in the past 15 years(Reference Fleszar, Bryant and Johnson1), sustaining its place as the highest amongst developed countries(Reference Taylor2). Alarmingly, people of colour experience disproportionately higher rates of maternal mortality(Reference Fleszar, Bryant and Johnson1,Reference Pawar, Sarker and Caughey3) and worsened maternal(Reference Njoku, Evans and Nimo-Sefah4,Reference Venkatesh, Lynch and Powe5) and infant outcomes compared to White individuals(Reference Anderson, Rogers and Baer6). These higher rates are exemplified by Black individuals in Louisiana (Southern US state), who in 2020 were 2·5 times more likely to die from pregnancy-associated deaths compared to White individuals(Reference DeGruy, Teixeira and Evans7). Structural and institutional racism, along with economic and social factors, contribute to these health disparities(Reference Taylor2,Reference Anderson, Rogers and Baer6) . Health disparities are compounded when considering both an individual’s race and income(Reference Thomson, Moffat and Arisa8), each independent risk factors for adverse perinatal outcomes themselves(Reference Pawar, Sarker and Caughey3,Reference Maher, Ward and Hernandez9) .
An emerging mediator between race, income and maternal and infant health outcomes is food insecurity (FI), defined as a lack of consistent access to safe and nutritious foods(Reference Dolin, Compher and Oh10). The connection between FI and chronic health conditions is well established, but there is a paucity of pregnancy-specific literature(Reference Dolin, Compher and Oh10). Pregnant individuals may be particularly susceptible to FI due to increased nutritional requirements and the need to support adequate gestational weight gain (GWG) for fetal growth(Reference McKay, Spiteri and Zinga11). The limited research in pregnancy links FI and increased risk of pregnancy-induced hypertension(Reference Morales, Epstein and Marable12), gestational diabetes mellitus (GDM)(Reference Cooper, Graham and Kuo13) and inadequate or excessive GWG(Reference Leone, Fleischhacker and Anderson-Steeves14). Understanding the intricate relationship between maternal race, household income, FI and birth outcomes is vital to improve perinatal outcomes within vulnerable populations.
Periods of widespread social disruption such as natural disasters, economic downturns and public health emergencies can intensify existing racial and income-related disparities in access to healthy foods, leading to increased FI within vulnerable populations(Reference Leone, Fleischhacker and Anderson-Steeves14,Reference Azevedo, de Morais and Silva15) . These events often result in disrupted food production and availability, which disproportionately impacts consumers already vulnerable to or experiencing FI(Reference Leone, Fleischhacker and Anderson-Steeves14). Low-income individuals are less likely to have access to alternative options such as food delivery or bulk ordering to overcome these shortages, limiting their ability to adapt during crises(Reference McKay, Spiteri and Zinga11,Reference Leone, Fleischhacker and Anderson-Steeves14) . Moreover, FI is multifaceted and can be a result of many interconnected, non-food factors like changes in employment and income and limited access to food purchasing establishments (e.g. restricted supermarket availability)(Reference Dolin, Compher and Oh10,Reference Pryor and Dietz16) . These compounding burdens may contribute to disproportionately high rates of FI among people of colour, who frequently face structural barriers that heighten vulnerability, particularly during periods of crisis(Reference Coleman-Jensen, Rabbitt and Gregory17). These food and non-food disruptions may have contributed to people of colour experiencing double the FI compared to White counterparts(Reference Coleman-Jensen, Rabbitt and Gregory17). It may be hypothesised that pregnant individuals of colour and lower income also experienced increased FI during the COVID-19 pandemic(Reference Allen, Onsando and Patel18), given racial and income-related disparities in maternal and infant health outcomes persisted and possibly worsened during this time(Reference Njoku, Evans and Nimo-Sefah4,Reference Simpson19) .
To address this research question, our study had two aims: (1) examine differences in FI by race and income in individuals pregnant during the peak of a large-scale public health emergency; and (2) examine whether FI explained the relationship between race and income with maternal and infant health outcomes. Our three main hypotheses were (1) Black individuals and low-income individuals would have an increased risk of experiencing FI, (2) Black individuals and low-income individuals would have worse maternal and infant health outcomes and (3) race, income and FI, together, would negatively impact maternal and infant outcomes.
Methods
Overall study
This cross-sectional explanatory mixed-methods (QUAN → QUAL) study included an online survey followed by semi-structured interviews and follows mixed-methods reporting standards(Reference Hong, Gonzalez-Reyes and Pluye20). This postpartum cohort includes two populations: (1) recipients of Louisiana Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and (2) patients of a dedicated women’s specialty hospital in Baton Rouge, Louisiana. To be eligible for WIC, applicants must have a total household income at or below a level set by the US Department of Agriculture, which was 185 % of the Federal Poverty Guidelines in 2020–2021. For a family of four, the 2020 poverty guideline was set at $26 200; thus, the WIC eligibility limit was $48 470/year(21). The current manuscript focuses on White and Black individuals as Black individuals represent the largest racial minority group in Louisiana(22) and have notable disparities in maternal health outcomes relative to White individuals; nonetheless, all races were recruited for the survey portion to allow for broader representation. Individuals were between 6 and 18 months postpartum when the survey was available (December 2021–December 2022) and 1·5–3 years postpartum for semi-structured interviews (March–June 2023). Data from this cohort have been previously published, demonstrating the role of macrosystem factors – such as government assistance, employment and housing – in influencing postpartum mental health outcomes(Reference Kracht, Goynes and Dickey23). The current study examines a unique research question and utilises electronic health records not previously published. The Pennington Biomedical Research Center Institutional Review Board approved this study (#2021-042).
Quantitative: online survey
Inclusion criteria were individuals who were ≥ 18 years of age, delivered in Louisiana between 10 June 2020 and 10 June 2021, spoke English, and were willing to link their survey responses to their medical record and infant’s birth certificate information. The June 2020–July 2021 period represented the peak of the COVID-19 pandemic for the USA, including lockdowns and no vaccine available. A state-provided list of pregnant individuals enrolled in WIC and the selected hospital’s delivery records were used for recruitment. Recruitment methods included text messaging, phone calls and in-person contacts at postpartum appointments (hospital only).
Potential participants received a link to a secure website containing information on the study’s purpose. Once completing informed consent online, participants were asked to complete questionnaires (six domains: demographics, pregnancy and delivery experience, mental health, food access, pandemic-related life and hardship experiences) and indicate interest in the optional interview.
Demographics
Individuals reported age, race, ethnicity, education, household income, employment status and hospital of delivery. Household income was assessed at time of survey with the question ‘about how much is your combined annual income, meaning the total pre-tax income from all sources earned in the past year?’ Income status was defined as low-income (household income < $50K USD), middle-income ($50–99 999K USD) and high-income ($> 100K USD), with middle-and high-income groups combined for quantitative analysis. Employment was assessed in the context of the pandemic using the question ‘which of the following changes in employment occurred to you/your partner due to the COVID-19 outbreak?’ with answers regarding loss of job, hours, pay and job security, move to remote work, childcare challenges, increased hours and ‘other’. Participants who identified as ‘Black’ or ‘White’ were included in this analysis, and other races (e.g. Hispanic, Asian) were excluded due to sample size. We acknowledge race is not a biological variable but serves as an imperfect proxy for lived experiences due to systemic discrimination and structural racism(Reference Taylor2). However, considering race as a variable is essential to understand and address health inequities and structural racism driving observed disparities(Reference Fasanya, Hsiao and Armstrong-Sylvester24). Language referencing racial and ethnic groups within this study is derived from participant self-identification and current literature.
Food insecurity
FI was measured through the Six-Item Short Form of the Food Security Survey(25). This six-item questionnaire asked individuals about their experiences over the past 12 months regarding food availability, affordability of balanced meals, whether coping strategies were needed to stretch meals, and if financial constraints led to hunger. Response options varied by question: ‘often true, sometimes true, never true’, ‘yes, no’ and one requesting frequency monthly. Individuals who indicated ‘yes’ to financial or other constraints (i.e. score ≥ 2) were classified as having FI.
Maternal and infant outcomes and gestational weight gain
Maternal and infant outcomes were abstracted from individuals’ linked medical records, verified using birth certificate data and represented through binary metrics (‘yes’ or ‘no’). Pre-pregnancy BMI (pre-pregnancy weight (kg)/height [m2]) determined weight categories: underweight (< 18·5), normal weight (18·5–24·9), overweight (25–29·9) and obesity (≥ 30). Total GWG (delivery weight minus pre-pregnancy weight) was calculated, compared to the Institute of Medicine Guidelines for GWG (see online supplementary material, Supplemental Table 1), and categorised as inadequate, adequate or excessive(Reference Harville, Kracht and Cohen26). Maternal outcomes examined were GDM, hypertensive disorder of pregnancy (including preeclampsia), preterm birth (gestational age < 37 weeks) and caesarean section. Infant outcomes examined were low birthweight (LBW; birthweight < 2500 g), macrosomia (birthweight
 $ \ge $
4000 g), Apgar score at 5 min (≤ 6) and neonatal intensive care unit admission. Composite outcomes were calculated for birthing individuals and infants who developed any of those outcomes(Reference Venkatesh, Lynch and Powe5,Reference Zheng, Shen and Jiang27) .
$ \ge $
4000 g), Apgar score at 5 min (≤ 6) and neonatal intensive care unit admission. Composite outcomes were calculated for birthing individuals and infants who developed any of those outcomes(Reference Venkatesh, Lynch and Powe5,Reference Zheng, Shen and Jiang27) .
Qualitative: semi-structured interviews
Inclusion criteria for the interviews were: (1) completed the entire survey, (2) indicated interest, (3) identified as only ‘Black’ or ‘White’ and were recruited from the WIC sample or reported a household income > 100K. Since WIC enrolment is contingent on low household income, individuals identified through WIC were considered the low-income sample. The high-income sample was recruited amongst hospital participants who reported an annual household income of > $100K USD. We sought ten participants per income and race group (forty total), based on best practices for qualitative investigations(Reference Hennink and Kaiser28). Potential participants were invited in random order until group amounts were achieved.
Semi-structured interviews were conducted virtually by researchers trained in qualitative interviews using a secure online platform. After obtaining informed consent, interviewers followed a pre-piloted interview script discussing each individual’s pandemic experiences (see online supplementary material, Supplemental Table 2). All interviews were recorded and transcribed verbatim.
Data analysis
QUANT: Statistical analysis
The analytic plan was designed to assess whether FI was an intermediary variable between race, income, and maternal and infant health outcomes. Therefore, we first explored whether race and income were related to maternal and infant health outcomes, via ANOVA or chi-square tests. Second, we compared FI status by race and income using chi-square tests. Third, we performed logistic regression, stratified by race and income independently, to test whether race or income in individuals with FI was related to maternal and infant outcomes with a trend analysis. Regression models were adjusted for maternal age, education, unemployment and GWG category (inadequate, adequate or excessive) based on past literature(Reference Harville, Kracht and Cohen26). All analyses were conducted in R (version 4.3.2).
QUAL: Thematic analysis
After forty interviews, the transcripts were reviewed, and it was determined saturation was reached. Transcribed interviews were coded by three authors trained in qualitative analysis using inductive thematic analysis (i.e. iterative coding and coding tree development (topic, root codes and code names))(Reference Braun and Clarke29). An initial codebook was developed based on a review of the transcripts and refined to the final codebook after a second review. Each transcript was independently coded with any discrepancies resolved through discussion. Based on past literature, an emergent theme was identified if present within ≥ 20 % of the sample (n 8 of either race or income)(Reference Patton30). Finalised themes were informed by study aims. Data management was done through Atlas TI software.
Integration
Quantitative and qualitative results were mixed to compare inferences. Integrated results pertaining to the same concepts were illustrated in a joint display to provide a visual representation of the combined outcomes from both research methods(Reference Guetterman, Fetters and Creswell31).
Results
QUANT: Survey and birth certificate
Of the 2340 survey participants, only those with complete data on race, income, demographics and birth certificate information were included in the analysis (n 1691, Figure 1). Participants who indicated another race (e.g. Hispanic and Asian) or were mixed race were not explored due to insufficient power for these analyses (n 48). As shown in Table 1, 1158 White and 533 Black individuals were included, nearly half (44·7 %) were classified as low-income and a quarter reported FI (24·7 %). Significant differences across race and income were observed in maternal age, education, employment, pre-pregnancy BMI and FI (P’s < 0·05). Low-income White individuals were youngest at delivery (27·4 years), and high-income Black individuals were oldest (31·7 years). As expected, education was lower in low-income White (45·9 % < 13 years) and Black (41·4 % < 13 years) individuals compared to their high-income counterparts (White 9·8 % < 13 years; Black 11·3 % < 13 years; P < 0·001), and low-income White (45·9 %) and Black (35·2 %) individuals reported significantly higher amounts of FI compared to their high-income racial counterparts (White: 10·5 %; Black: 24·3 %; P < 0·001). Differences were also observed in GWG, preterm birth, caesarean section, LBW and macrosomia (P’s < 0·05); high-income Black individuals had the highest rates of caesarean delivery (40·9 %) relative to counterparts (range: 29·9–35·9 %), while low-income Black individuals had the highest rates of preterm birth (13·6 %) and LBW infants (13·2 %) relative to counterparts (preterm birth range: 7·8–9·5 %; LBW infant range: 5·5–7·8 %). These findings are mirrored in race-and income-stratified results (see online supplementary material, Supplemental Table 3). Differences in GDM, gestational hypertension and preeclampsia were noted when considering GWG category and race, or GWG category and income (see online supplementary material, Supplemental Tables 4, 5).
Flow diagram of participants. GWG, gestational weight gain.

Differences in demographic, maternal and infant health outcomes by race and income level (n 1691)

GWG, gestational weight gain; NICU, neonatal intensive care unit.
*P < 0·05.
^Assessed using a two-way ANOVA.
There were no differences in maternal and infant outcomes by FI status alone (see online supplementary material, Supplemental Table 6). On average, individuals with FI were younger, had lower education, were more likely to be unemployed and had a higher pre-pregnancy BMI compared to individuals without FI (see online supplementary material, Supplemental Table 6). In further exploration of this lack of association, increasing age was related to having GDM (P’s < 0·05), whereas being unemployed was related to lower risk of macrosomia but higher risk of LBW and neonatal intensive care unit admission (P’s < 0·05).
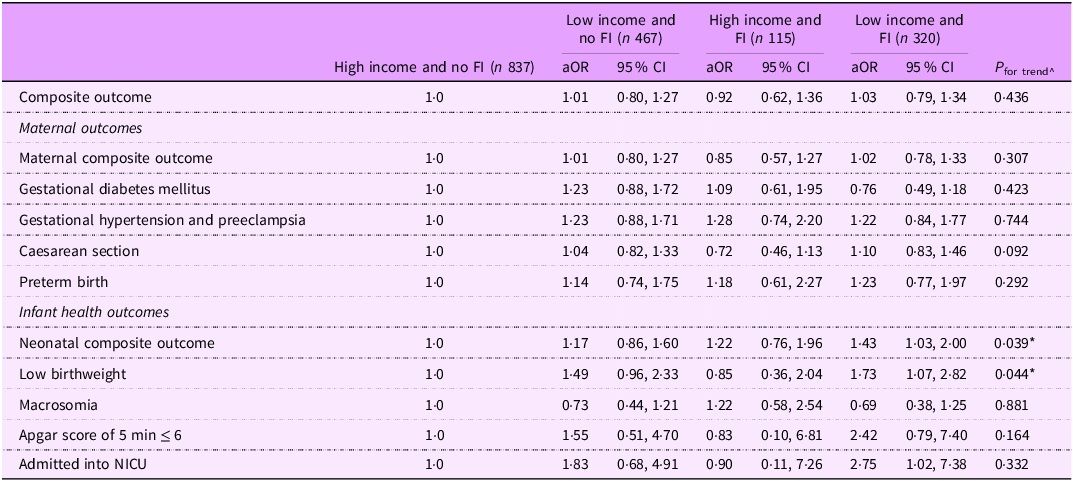
In models stratified by income and FI, trends for neonatal composite outcome and LBW infants emerged (Table 2). Low-income individuals with FI were 73 % (aOR 95 % CI: 1·07, 2·82) more likely to have LBW infants and 43 % (aOR 95 % CI: 1·03, 2·00) more likely to have infants with adverse outcomes compared to high-income individuals without FI. A similar trend was found by race and FI, where Black individuals with FI were 2·49 times (aOR: 95 % CI: 1·45, 4·29) as likely to have an LBW infant compared to White individuals without FI (see online supplementary material, Supplemental Table 7).
Associations between income level and food insecurity status with adverse pregnancy outcomes

FI, food insecurity; NICU, neonatal intensive care unit.
*P < 0·05.
^Assessed using a logistic regression with adjustment for age at delivery, education, unemployment and GWG groups; we treated the groups as an ordinal variable based on a logical sequence from high income and no FI to low income and having FI. This progression includes low income to be at higher risk regardless of FI. Therefore, this P-value is a P for trend.
QUAL: Semi-structured Interviews
Of the 111 individuals contacted, forty individuals – evenly distributed across race and income – completed interviews. Exclusion resulted from declined participation, disconnected numbers or inability to contact (initially or interview no-show/no response). Based on these interviews, three themes were identified regarding barriers and facilitators to food access and subsequent FI. Themes are described below, with representative quotes shown in Table 3.
Thematic findings related to food acquisition during the COVID-19 pandemic amongst race and income

Pandemic-related food access disparities
Most low-income individuals reported significant barriers to acquiring food during their pregnancy and in the pandemic, with experiences shaped by store closures, shortened hours and widespread shortages that severely limited their food supply. As participant #1 (White, low-income) noted, ‘the stores were wiped clean’. With little ability to shop at different stores, substitute missing items or pay for delivery services, these shortages substantially impacted low-income individuals’ eating habits during pregnancy. Reduced store hours further compounded challenges for low-income individuals, preventing them from shopping at times that fit their schedule, a barrier several noted as persisting 1·5 years later. In contrast, high-income individuals reported mild disruptions to food acquisition, such as reduced hours or missing a few food items in their grocery orders, but easily overcame barriers by substituting items or having them delivered.
Family support as a resource for low-income participants
Many low-income individuals reported relying more on partners or family members to access food during pregnancy due to concerns about virus transmission and other access barriers such as store hours. Low-income individuals often reported that family members assumed grocery shopping responsibilities, with some individuals also relying on their family for food when they did not have enough. These dependencies sometimes constrained food choices during pregnancy, as participants described having to eat whatever their family purchased, even if it was not what they preferred or considered healthy. One high-income individual described family assuming shopping responsibilities, but most used grocery delivery options to overcome food procurement barriers.
Pregnancy health conditions facilitating dietary changes
Many individuals reported feeling that they ate better during their pregnancy due to their diagnosis of GDM or other conditions, but these conditions varied by race and income. Low-income Black individuals and White individuals of both income levels said they became more conscious of their diets following a GDM diagnosis, often resulting in healthier eating habits, particularly regarding carbohydrate intake. Black individuals of both incomes also reported that they were diagnosed with other conditions or at high risk (e.g. preeclampsia, closely spaced pregnancies), which made them more conscious of their diet and physical activity.
Integration
As shown in Table 4, quantitative results revealed individuals with lower income and increased FI were more likely to experience adverse infant outcomes, as were Black individuals with FI, compared to their counterparts. Qualitative results complemented these findings, revealing nuances between racial and income groups regarding FI (e.g. store closures, food shortages and family support) and health perspectives (e.g. prenatal health conditions) that may have influenced individuals’ diets, GWG, and maternal and infant health outcomes.
Joint display of quantitative and qualitative findings, and meta-inference

GWG, gestational weight gain; LBW, low birthweight; NICU, neonatal intensive care unit; GDM, gestational diabetes mellitus; FI , food insecurity.
Discussion
This mixed-methods study aimed to understand the connections between maternal race, income and FI experiences with maternal and infant health outcomes among a diverse perinatal population during a large-scale public health emergency. Findings from this study can better inform multi-level approaches to support vulnerable individuals in other times of public health emergencies to improve maternal and infant health outcomes and subsequent long-term health. In this sample, Black individuals and low-income individuals were more likely to experience FI, but FI alone was not directly related to maternal and infant health outcomes. Rather, Black individuals and low-income individuals experienced more negative impacts on infant health when they also endured FI. Qualitative results revealed contextual considerations for food acquisition by income level and descriptions of beneficial health behaviour changes in response to pregnancy-related diagnoses. This study highlights an increased risk of adverse infant outcomes by race and income with concurrent FI, but a sparing of deleterious impacts on maternal outcomes, which may be attributed to differing family and individual changes or altered physician support due to the emergence of obstetrical complications such as GDM.
We found support for our hypothesis that Black individuals and low-income individuals would have an increased risk of experiencing FI. Our findings align with prior research demonstrating low-income and minority households have elevated risk of FI during the pandemic(Reference Leone, Fleischhacker and Anderson-Steeves14,Reference Morales, Morales and Beltran32) but contribute new evidence that pregnant individuals were also impacted. To cope with FI, some low-income individuals described using family support and social capital to buffer the impacts of FI, though most expressed the support was insufficient to fully overcome FI. Other studies have linked social support(Reference Leddy, Whittle and Shieh33) and social capital(Reference Lambert, Lutz and Orr34) with reduced FI; however, family support may not be a long-term solution, as these individuals’ families may be experiencing FI themselves as they likely share similar socio-economic characteristics outside of pandemic or emergency settings(Reference Odoms-Young and Bruce35), with probable magnification during crises as demonstrated during the COVID-19 pandemic(Reference Leone, Fleischhacker and Anderson-Steeves14). Rather, these findings may propose a double burden of FI during pregnancy, which calls for innovative solutions to help both pregnant individuals and the extended family.
We did not find support that FI itself is related to worsened maternal or infant health outcomes, which may be attributed to several factors. First, FI likely results from many interconnected elements (e.g. employment, transportation, etc.) which persist in non-pandemic contexts but were exacerbated during the pandemic(Reference Dolin, Compher and Oh10,Reference Pryor and Dietz16) . Upon further exploration, these factors were represented in the current study as individuals who experienced FI tended to be younger, less educated, unemployed and have a higher pre-pregnancy BMI; some of these factors were related to maternal and infant outcomes; thus, they may diminish or remove the direct effect of FI. Second, although social support and social capital were not assessed in the survey, prior research suggests that these factors may buffer the adverse effects of FI by providing emotional, material or community-level resources that mitigate its impact on health(Reference Leddy, Whittle and Shieh33,Reference Lambert, Lutz and Orr34) . Third, we only used two groups (FI and no FI) from the Six-item Short Form FI module(25). Utilising more nuanced categories (i.e. very low, marginal, etc.) obtained via longer or different instruments could increase the sensitivity of FI assessment and may provide further detail and differing results(Reference Crandall, Temple and Kong36). Lastly, we were not able to characterise the time frame, frequency or duration of FI. Others have demonstrated that having acute and chronic FI during pregnancy is associated with LBW through the mediator of depressive symptoms, indicating any FI experienced may be impactful(Reference Grilo, Earnshaw and Lewis37) but was not explored in this study. Still, one systematic review found that having FI, relative to no FI, was related to minimal change in GWG(Reference Nguyen, Bell and Andreae38), which may explain overall null associations with maternal outcomes tied to GWG.
We found full support for our hypothesis that race, income and FI would impact infant health outcomes, especially Black individuals were at much higher risk of having a LBW compared to counterparts. We examined the incidence of LBW rather than actual birthweight; however, our results echo prior research showing FI can negatively influence birthweight(Reference de Freitas Rocha, de Souza de Morais and Azevedo39,Reference Chowdhury, Dibley and Alam40) and add to the literature by demonstrating that race and income in combination with FI compound the risk of having an LBW infant. These findings have significant implications for short-term and long-term health. LBW individuals have increased risk of mortality and morbidities such as infection, breathing trouble, nervous and digestive system issues as infants(Reference Sangamam41,Reference Cortese, Moster and Wilcox42) , and higher risk of neurological disorders, impaired language development and academic performance, and chronic diseases such as obesity, metabolic disorders and CVD from childhood through adulthood(Reference Huang, Zhang and Sun43,Reference Stinson, Kromann Reim and Lund44) . Overall, existing risk factors, combined with perinatal FI, may increase the rate of LBW infants and subsequently a lifetime of obesity and associated health conditions. Beyond nutritional pathways, psychosocial mechanisms must also be considered, as recent research has demonstrated that FI is strongly linked to maternal mental health challenges that can reduce caregiving capacity, feeding quality and bonding, thus increasing the risk of adverse infant outcomes(Reference Rahi, Al Mashharawi and Harb45). Together, these findings highlight that the consequences of FI extend beyond nutrition to psychosocial domains, with maternal distress serving as a critical pathway that can amplify biological risks and perpetuate disparities in infant health outcomes.
There are four clear future directions for research and practice from this study. First, further mechanistic research is needed to understand the interconnected pathway between FI, GWG and subsequent maternal and infant outcomes. Longitudinal tracking of maternal outcomes and FI beginning in early pregnancy and followed post-birth may improve upon the current literature which presents discordant findings(Reference Dolin, Compher and Oh10–Reference Cooper, Graham and Kuo13,Reference Azevedo, de Morais and Silva15) , and incorporating assessments of coping mechanisms and social support could support a more robust evaluation of effects. Second, our findings emphasise the need to further explore how crises and natural disasters (e.g. hurricanes) impact FI, to inform emergency preparedness and intervention strategies. Third, future studies should broaden their scope to include a wider array of racial/ethnic and income backgrounds; culturally competent interventions that cater to the unique needs and priorities of different groups and communities are critical in effectively addressing GWG and perinatal health(Reference Getha-Taylor, Holmes and Moen46). Finally, our results demonstrate disparities in food accessibility that could be reduced by policy interventions that increase access to affordable and nutritious foods, such as promoting urban agriculture programmes(Reference Lofton, Martin and Kersten47), and community-supported agriculture programmes(Reference Martinez, Rosero and Thomas48), to improve food security.
Limitations and strengths
Strengths of this study include an evaluation of income alongside race, birth certificate and medical record assessed outcomes to overcome self-report bias for weight gain and other delivery outcomes, investigating various perinatal outcomes, and utilisation of a rigorous mixed-methods approach. Limitations of the study are primarily related to generalisability and study design. First, our analyses focused on Black and White participants given the study aims and sample size constraints, and findings amongst Black and White individuals of high and low income may not apply to other racial/ethnic populations, across other US states, or during non-pandemic times, though they parallel patterns of FI from prior research(Reference Dennard, Kristjansson and Tchangalova49,Reference Coleman-Jensen, Rabbitt and Gregory50) . Second, household size was not collected, which can limit the interpretation of income as a sole indicator of FI risk, though WIC eligibility is based on household size and income. Additionally, income and employment were assessed at survey completion (6–18 months postpartum) based on the past year or pandemic-related changes, which may not fully reflect participants’ circumstances during pregnancy. Third, the study did not assess the degree of participation in WIC services and thus cannot determine whether WIC enrolment may have mitigated or contributed to changes in FI. Lastly, individuals participated in the study during their later phase postpartum and of the pandemic which may not as accurately reflect their food acquisition experiences during the height of the pandemic and while pregnant. Therefore, timing of FI assessments and recall period are a critical consideration for future studies in pregnant individuals.
Conclusions
This study documented interactions between race, income, FI and infant health outcomes. Our findings demonstrate that addressing FI, particularly among low-income pregnant individuals and pregnant individuals of colour, is paramount to optimise infant outcomes for all. These results are especially relevant to periods of social or economic disruption, such as public health emergencies or natural disasters, where existing inequalities in access to nutritious foods are amplified and exacerbate the challenges faced by vulnerable populations.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980026101955
Acknowledgements
The authors would like to thank the participants in this study for their contribution and willingness to share their stories.
Authorship
M.S.D.: data curation, formal analysis, investigation, project administration, writing – original draft and writing – review and editing. K.O.G.: formal analysis, project administration and writing – original draft. C.L.K.: data curation, formal analysis, investigation, project administration, supervision, writing – original draft and writing – review and editing. B.J.: data curation and writing – review and editing. E.S.: data curation and writing – review and editing. J.B.: data curation and writing – review and editing. M.K.: conceptualisation, data curation, funding acquisition and writing – review and editing; Y.S.: formal analysis, writing – review and editing, validation and visualisation. G.H.: formal analysis, writing – review and editing, validation and visualisation. E.W.H.: conceptualisation, funding acquisition, supervision and writing – review and editing. E.F.S.: conceptualisation, funding acquisition, supervision and writing – review and editing. L.M.R.: conceptualisation, funding acquisition, supervision and writing – review and editing.
Financial support
This work was supported by the National Institutes of Health (C.L.K., grant numbers K99HD107158, P20GM144269; L.M.R., grant numbers R01NR017644, R01DK124806, U54GM104940; and G.H., grant number R01DK132011). The NIH had no role in the design, analysis or writing of this article. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests
The authors declare there are no competing or conflicts of interest associated with the present manuscript.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Pennington Biomedical Research Committee IRB. Written informed consent was obtained from all survey subjects; written and verbal informed consent was obtained from all interview subjects. Verbal consent was witnessed and formally recorded.







 Open access
Open access