


Introduction
A central task in the study of developmental psychopathology is identifying factors that determine whether functioning will or will not be disrupted by a stressor. Resilience in the face of stress has been defined by Luthar (Reference Luthar2015) as “…positive adaptation despite experiences of significant adversity or trauma.” Resilience can be seen as a form of “reserve,” available under stress but not necessarily active under normal circumstances – akin to a monetary “rainy day fund” that normally sits dormant, but plays a critical buffering role under conditions of financial distress (Bergeman & Nelson, Reference Bergeman and Nelson2024). Importantly, Luthar (Reference Luthar2015) has argued that resilience is not simply an intra-individual trait: Factors such as the quality of close dyadic relationships, social support, and a positive view of one’s family are considered essential components of human resilience.
The COVID pandemic as an opportunity to study resilience
This study used the unique opportunity for research created by the multiple stressors accompanying the COVID pandemic to examine adolescent–family relationship factors as potential long-term sources of resilience with regard to both mental and physical health. Although the COVID pandemic clearly did not affect all individuals equally, a number of its effects (e.g., loss of normal routines, masking requirements, restricted movement and autonomy, disruption of normal services, etc.) were nearly universally experienced (Andrade et al., Reference Andrade, Hoyle and Burnell2023; Lakhan et al., Reference Lakhan, Agrawal and Sharma2020). Research since has found that the onset of the pandemic was followed by clear upticks in depression, anxiety and with some evidence of declines in self-reported health quality (Nochaiwong et al., Reference Nochaiwong, Ruengorn, Thavorn, Hutton, Awiphan, Phosuya, Ruanta, Wongpakaran and Wongpakaran2021; Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022; van de Weijer et al., Reference van de Weijer, de Vries, Pelt, Ligthart, Willemsen, Boomsma, de Geus and Bartels2022; Zhu et al., Reference Zhu, Jiang, Yang, Dzierzewski, Spruyt, Zhang, Huang, Ge, Rong and Ola2023). Hence this study examined relative changes in levels of depressive symptoms and reported health quality pre- and post-COVID to identify factors that would predict which individuals would or would not respond well to the stressors created by the pandemic.
Efforts to identify factors potentially offsetting the impact of the pandemic on mental and physical health outcomes have thus far identified exercise, self-reported levels of concurrent social support, and extraversion as leading to relative resilience (Hou et al., Reference Hou, Zhang, Cai, Song, Chen, Deng and Ni2020; Lancaster & Callaghan, Reference Lancaster and Callaghan2022; Wang et al., Reference Wang, Havewala and Zhu2024; Zhou & Yao, Reference Zhou and Yao2020). However, investigations to date have been largely limited to study of concurrent factors associated with resilience and have primarily relied upon self-report data. Relationship qualities prior to the onset of the pandemic that might predict resilience have gone largely unexamined.
The potential role of parental relationship quality
Although parental relationships gradually diminish in intensity over the course of adolescence (Rosenthal & Kobak, Reference Rosenthal and Kobak2010), they frequently offer continuing substantial support well into adulthood with the potential to affect well-being (Allen et al., Reference Allen, Costello, Kansky and Loeb2022; Allen et al., Reference Allen, Danoff, Costello, Loeb, Davis, Hunt, Gregory, Giamberardino and Connelly2023; Bouchard & Doucet, Reference Bouchard and Doucet2011; Zarit et al., Reference Zarit, Eggebeen and Bornstein2005). Life course studies suggest that, during periods of crisis, individuals, even as adults, are especially likely to draw support from their parents (Eggebeen & Davey, Reference Eggebeen and Davey1998). Developmental systems theory further supports this idea that family support may become particularly important under stress (Engert et al., Reference Engert, Blasberg, Kohne, Strauss and Rosendahl2021; Luthar et al., Reference Luthar, Cicchetti and Becker2000; Masten et al., Reference Masten, Lucke, Nelson and Stallworthy2021). To the extent adolescents establish parental relationships that can weather stress without devolving into hostile interaction patterns, these relationships appear likely to have stress buffering properties well into adulthood. This premise has, however, received scant empirical examination to date.
One well-established marker of the quality of parent–adolescent relationships is the dyadic process by which parents and adolescents jointly handle the adolesent’s developmental task of seeking autonomy in interactions with parents while trying to maintain a solid relationship and avoiding hostile interaction patterns. Mastery of such core developmental tasks is considered a key to longer-term resilience (Masten & Coatsworth, Reference Masten and Coatsworth1998). The overarching hypothesis this study examined was that family relationship qualities that facilitated progress in this task in adolescence would provide a source of resilience extending into adulthood.
Progress in establishing autonomy while maintaining strong relationships and avoiding hostile interactions with parents appears as a likely marker of future resilience in that it establishes a capacity to maintain key social relationships under stress. Success establishing autonomy and relatedness with parents in adolescence has been tied to progress in development across the life span, with links to prior attachment security assessed in infancy, to concurrent markers of functioning with peers in adolescence, to future functioning in social relationships beyond adolescence, and to avoidance of premature aging (Allen et al., Reference Allen, Chango and Szwedo2014; Allen et al., Reference Allen, Danoff, Costello, Loeb, Davis, Hunt, Gregory, Giamberardino and Connelly2023; Becker-Stoll et al., Reference Becker-Stoll, Fremmer-Bombik, Wartner, Zimmermann and Grossmann2008; Loeb et al., Reference Loeb, Davis, Costello and Allen2020). Conversely, hostility in such interactions has been linked to future peer struggles and markers of adult health risk (Allen et al., Reference Allen, Hauser, O’Connor and Bell2002; Allen et al., Reference Allen, Loeb, Tan, Narr and Uchino2017). The process of managing challenges to autonomy and relatedness has been described as a multi-party dance to which both parent and adolescent behavior contribute and it is the quality of this overall dance that marks the level of adaptation achieved (Allen et al., Reference Allen, McElhaney, Land, Kuperminc, Moore, OBeirne-Kelley and Liebman2003; Allen et al., Reference Allen, Porter, McFarland, Marsh and McElhaney2005). This perspective is in keeping with Masten’s (Reference Masten2007) definition of resilience in terms of “the capacity of dynamic systems to withstand or recover from significant disturbances.”
The role of family relationships as potential stress buffers beyond childhood has been supported in multiple studies (Luthar, Reference Luthar2015). For example, family warmth in childhood has been found to buffer the effects of bullying experienced in adolescence (Bowes et al., Reference Bowes, Maughan, Caspi, Moffitt and Arseneault2010). Similarly, parenting interventions have previously been found to improve adolescents’ adaptations to stress (Sandler et al., Reference Sandler, Schoenfelder, Wolchik and MacKinnon2011). Finally, and most germane to the current study, family cohesion has been found to predict resilience among teens at risk for depression, even when these teens were followed into early adulthood (Carbonell et al., Reference Carbonell, Reinherz, Giaconia, Stashwick, Paradis and Beardslee2002).
Potential mediators
Beyond adolescence, developmental cascade theory (Masten & Cicchetti, Reference Masten and Cicchetti2009) suggests that family relationship qualities in adolescence are likely to have their future effects mediated via future relationship qualities. Fully understanding the longer-term role of adolescent–family relationship qualities as potential sources of resilience requires identifying processes by which such qualities may operate to lead to resilience (Luthar & Cicchetti, Reference Luthar and Cicchetti2000). Most obviously, these adolescent interactions set the stage for establishing both the quality and quantity of future family relationships (e.g., how positively future family relationships are viewed and how much actual interaction takes place within them). Adult–parent relationships in turn have been linked to multiple markers of mental health (Steele & McKinney, Reference Steele and McKinney2020). In addition, the quality of family interactions in adolescence is likely to influence qualities of broader future social functioning (e.g., loneliness vs. social integration) (Masten et al., Reference Masten, Lucke, Nelson and Stallworthy2021; Masten & Cicchetti, Reference Masten and Cicchetti2010; Oudekerk et al., Reference Oudekerk, Allen, Hessel and Molloy2015). One of the longest standing findings in resilience research is the recognition that broad social integration and support plays a crucial role in adaptation to stress across the life span (Hauser & Allen, Reference Hauser, Allen, Kerig, Schulz and Hauser2012; Werner, Reference Werner1982). In contrast, poor social relationship quality has long been linked not only to poor mental health but also to risk of early mortality (Holt-Lunstad et al., Reference Holt-Lunstad, Smith and Layton2010).
The current study
This study examined functioning before and after the onset of the COVID pandemic to identify long-term predictors of resilience. Examining the COVID pandemic as a stressor offers important advantages in the study of risk and resilience. First, this approach at least partially addresses the problem that stressors and protective factors often covary (inversely), thus creating a built in research confound (Luthar et al., Reference Luthar, Cicchetti and Becker2000). The population-wide exposure to a significant number of COVID-related stressors, with subsequently observed population-wide declines in functioning, provides a unique opportunity to examine resilience in the face of a set of stressors that was not a result of behaviors by the individuals experiencing them. Being able to examine changes from before and after COVID onset using prospective data also makes it possible to begin to separate effects of exposure to stress from the potential effects of prior levels of functioning. For example, it has been documented that those reporting lower levels of social support were more likely to have reported poorer mental health in response to COVID (Zhou & Yao, Reference Zhou and Yao2020). Prospective research makes it possible to address the question: Did those with poor social support prior to COVID experience actual relative declines in mental health in response to the pandemic vs. simple continuation of pre-existing poor mental health? The occurrence of the pandemic thus creates a somewhat rare opportunity to explore resilience factors in relation to a series of stressors that were not self-generated to any significant degree. Of course, pre-existing factors (e.g., lack of financial resources, poor physical and mental health) were also influential in determining the degree of stress experienced (Nemani et al., Reference Nemani, Li, Olfson, Blessing, Razavian, Chen, Petkova and Goff2021; Whitehead et al., Reference Whitehead, Taylor-Robinson and Barr2021). A prospective design also allows at least some of these factors to be directly assessed and taken into account.
Finally, in addition to familial and social protective factors, broader demographic factors (e.g., gender and family income) were also considered, as these have been repeatedly identified as risk or protective factors, both more generally and with respect to COVID specifically (He et al., Reference He, Cabrera, Renteria, Chen, Alonso, McDorman, Kerlow and Reich2021; Luthar, Reference Luthar1999). Although not a primary focus of this study, simultaneous consideration of multiple risk and resilience factors makes it possible to reduce the likelihood that effects will be misattributed to a single factor, such as family relationship quality, that might just as readily be attributed to factors such as experience of poverty.
This multi-method study used a demographically heterogeneous community sample of adults, followed from adolescence into the mid-thirties, to identify pre-existing factors that would predict response to the pandemic in terms of two primary outcomes: depressive symptoms and physical health quality. The study first assessed the initial hypothesis that levels of functioning on both indices would display deterioration from pre- to post-COVID onset. It then examined the primary hypothesis that resilience in response to COVID would be predicted by mastery of adolescent efforts to establish a means of handling conflict with parents characterized by autonomy and relatedness and avoidance of hostility. Finally, the study went on to examine several potential mediators of predictions from early family experiences to outcomes via quality of adult–parental relationships and levels of broader social integration.
Method
Participants
This report is drawn from a larger longitudinal investigation of adolescent social development in familial and peer contexts. Original participants included 184 seventh and eighth graders (86 identified as male and 98 as female) followed over a 20-year period from ages 18 to 38, along with collateral data collected from observations of interactions with parents in late adolescence. The sample was racially/ethnically and socioeconomically diverse: 107 adolescents (58%) identified as White, 53 (29%) as African American, 15 (8%) as of mixed race/ethnicity, and 9 (5%) as being from other minority groups. Adolescents’ parents reported a median family income in the $40,000 – $59,999 range at the initial assessment. This compares to a median family income in the United States at the time (1998) of $48,000/year. These racial/ethnic and income distributions closely matched that of the city from which participants were drawn, reflecting that they all came from a public middle school serving city residents.
Participants were initially recruited from the 7th and 8th grades of a public middle school (Mean age = 13.3 years, SD = 0.64) drawing from suburban and urban populations in the Southeastern United States. Students and their peers were recruited via an initial mailing to all parents of students in the school along with follow-up contact efforts at school lunches. Families of adolescents who indicated they were interested in the study were contacted by telephone. If a student was identified as a close peer of a participant and agreed to participate in that capacity, they were no longer eligible to participate as primary participants, to reduce potential dependencies in the data. Of all students eligible for participation, 63% agreed to participate as either target participants or as peers providing extensive collateral information in a 3-hour session. All participants provided informed assent/consent (depending upon whether they were an adolescent or an adult) before each interview session, and parents provided informed consent for adolescents. Initial interviews took place in private offices within a university academic building. Follow-up assessments were conducted in the same setting, or for participants’ living at a distance, were conducted either in local settings (e.g., hotel conference rooms), or via mail or online survey.
Assessment ages
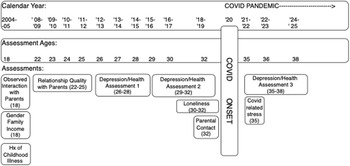
Figure 1 presents a graphic depiction of the timing of data collection relative to participant age and to calendar year of collection.
Study timeline and measurement occasions.
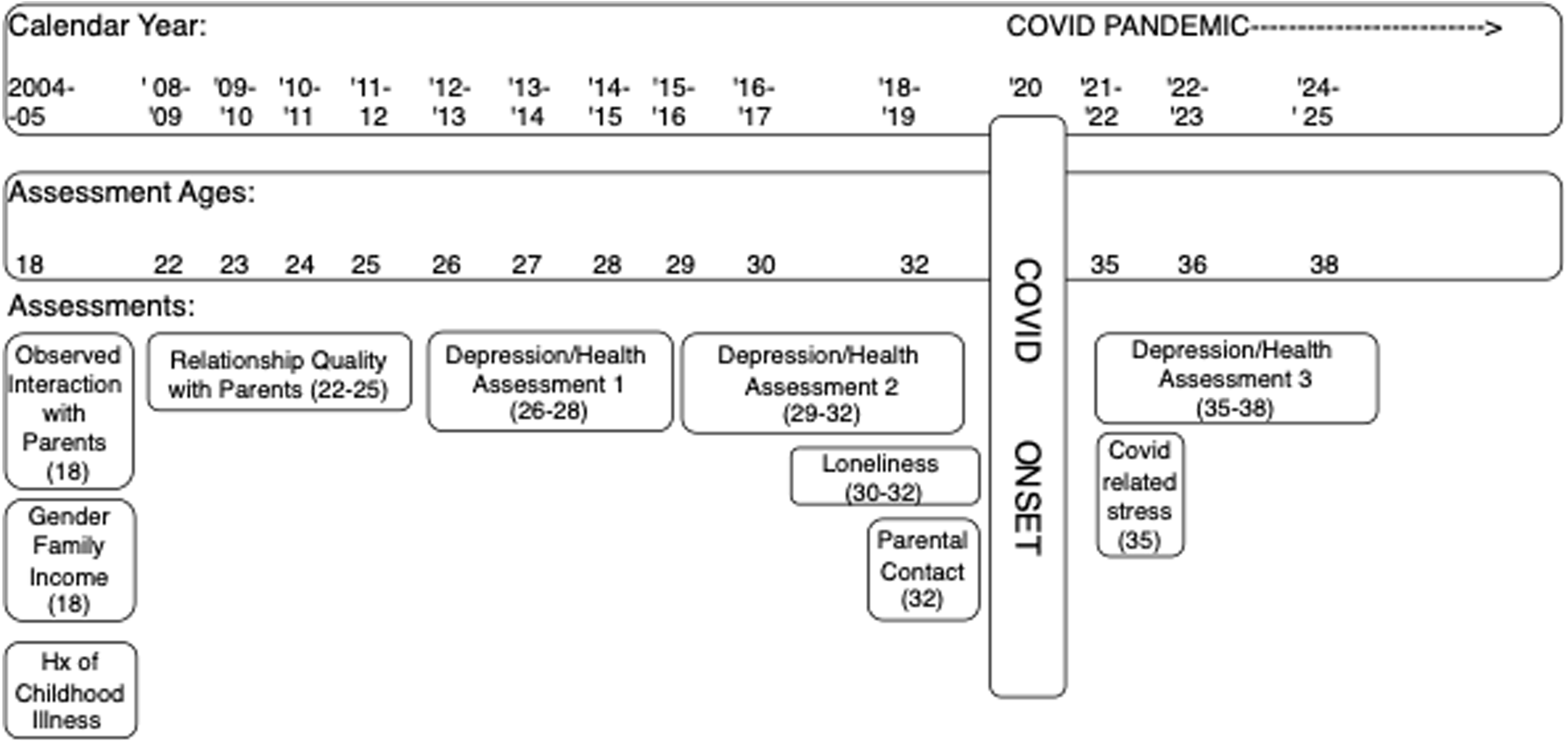
Participants were assessed repeatedly as follows: At age 18.3 (SD = 1.27) they were observed in video-recorded interaction tasks conducted separately with each parent. Mothers were age 47.4 (SD = 6.18) and fathers were age 50.4 (SD = 5.3) at this assessment point. All adolescents were still residing in their family of origin at this assessment. Participant reports of parental relationship quality were obtained at ages 21.7 (SD = 0.95), 22.8 (SD = 0.95), 23.8 (SD = 0.97) and 24.7 (SD = 0.96).
Pre-COVID assessments of depressive symptoms and health status were obtained at ages 28.6 (SD = 1.02), 30.2 (SD = 0.96), and 31.7 (SD = 0.99). Loneliness was assessed at the last two of these assessment waves and contact with parents was assessed at the final pre-COVID assessment wave. The last of these pre-COVID assessments was completed in August of 2019. Post-COVID onset assessments of depression and health were obtained at ages 34.7 (SD = 0.89), 36.3 (SD = 0.96), and 38.0 (SD = 0.95). These took place from July 2020 thru February 2024. Widespread COVID onset in the U.S. occurred in March 2020. For simplicity, measures obtained after July 2020 are referred to as post-COVID onset, or just post-COVID, though of course the pandemic has remained a substantial ongoing potential stressor into the present.
For post-hoc analyses examining patterns of change entirely within the pre-COVID era, assessments of depression and health were also obtained at ages 25.7 (SD = 0.99), 26.6 (SD = 1.00), and 27.7 (SD = 0.99). All ages are rounded in measures descriptions below.
Attrition analyses
Attrition analyses compared those participants with vs. without data at various points in the study. At the pre-COVID assessment, 97% of the original participants provided data; all six missing participants were male (p = .007). For the post-COVID assessment, 78% of the original sample had outcome data. Those missing outcome data were more likely to be male (33% missing males; 12% missing females, p < .001) but did not differ on any other measures. For observed adolescent–parent interactions, data were obtained from 60% of the original sample for mother–adolescent interactions and 36% for father-adolescent interactions. Those with missing interaction data had lower family income in adolescence, (p = .006), slightly worse pre-COVID health status (p = .04), and slightly poorer reported relationships to mothers in adulthood (p=.05).
To best address any potential biases due to attrition, full information maximum likelihood (FIML) methods were used with analyses including all variables that were linked to future missing data (i.e., where data were not missing completely at random). Because these procedures have been found to yield the least biased estimates when all available data are used for longitudinal analyses (relative to listwise deletion of missing data), even when data are not described as missing at random or missing completely at random (Arbuckle, Reference Arbuckle and Schumaker1996; Newman, Reference Newman2014), the entire original sample of 184 was utilized for these analyses. This full sample thus provides the best possible estimates of variances and covariances among all measures of interest and was least likely to be biased by missing data.
Procedure
In the initial introduction and throughout all sessions, confidentiality was assured to all study participants and adolescents were told that their parents and friends would not be informed of any of the answers they provided. Participants’ data were protected by a Confidentiality Certificate issued by the U.S. Department of Health and Human Services, which protected information from subpoena by federal, state, and local courts. Transportation and childcare were provided if necessary. Adolescent/adult participants and their parents were all paid for participation.
Measures
Depressive Symptoms (Ages 26–28, 29–32, 35–38) were assessed annually across the age ranges listed via the 21-item Beck Depression Inventory (Beck & Steer, Reference Beck and Steer1987). This instrument is a well-validated and widely accepted self-report measure of depressive symptomatology (Kazdin, Reference Kazdin1990). Items were rated on a Likert scale, summed for each year, and then aggregated across years to yield separate depressive symptom scores for the 26–28 (early adulthood) phase, the 29–32 (pre-COVID assessment), and the 35–38 (post-COVID assessment). Internal consistency was good as Cronbach α’s ranged from 0.88 to 0.92.
Adult Health Quality (Ages 26–28, 29–32, 35–38) was assessed annually across the age ranges listed via the 5-item Likert-style, self-report general health scale from the Medical Outcomes Study Short-form Health Survey (Ware et al., Reference Ware, Kosinski, Dewey and Gandek2000), in which participants first answered one question describing the overall state of their health: “In general, would you say your health is poor, fair, good, very good, or excellent.” This was followed by four additional statements for which participants were asked to rate how true or false each statement was for them, on a 5-point scale (i.e., Definitely True, Mostly True, Don’t Know, Mostly False, Definitely False). These included items such as “I tend to get sick a little easier than other people” (reverse-scored), “I am as healthy as anybody I know,” and “My health is excellent.” Resulting scores were multiplied by four to yield a 0- to 100-point scale. This approach has been used extensively and found to be not only strongly related to concurrent biological markers of health, but also to consistently yield strong predictions to future health, including mortality, even after adjustment for key covariates such as functional status, depression, and comorbidity (DeSalvo et al., Reference DeSalvo, Bloser, Reynolds, He and Muntner2006; McHorney et al., Reference McHorney, Ware and Raczek1993; Stewart et al., Reference Stewart, Hays and Ware1988). Internal consistency for the composite score was good as Cronbach α’s ranged from 0.73 to 0.85. Scores for health quality were averaged across the same age ranges as described above for depressive symptoms.
Observed autonomy and relatedness behaviors during a disagreements (Age 18)
Adolescents participated separately with each parent in a revealed differences task in which they discussed a significant issue about which they disagreed. Typical topics of discussion included money (19%), grades (19%), household rules (17%), friends (14%), and brothers and sisters (10%); other possible areas included communication, plans for the future, alcohol and drugs, religion, and dating. Video-recordings of these interactions were utilized to code the adolescent-parent interactions using the Autonomy and Relatedness Coding System (Allen et al., Reference Allen, Hauser, Bell and O’Connor1994). Concrete behavioral guidelines were utilized to code parents’ and adolescents’ speech in terms of four primary scales. The Displaying Relatedness scale captures validating statements and displays of engagement and empathy with the other party and their statements. The Displaying Autonomy scale captures behaviors in which the adolescent or mother present their reasoning underlying their disagreement in a confident, not shrill, manner. The Undermining Autonomy scale captures behaviors such as overly personalizing a disagreement, pressuring the adolescent to agree. The Relatedness-undermining Hostility scale captures behaviors expressing hostility toward another member either directly or implicitly by rudely interrupting/ignoring a family member. Two trained coders coded each interaction and their codes were then summed and averaged. Codes for both parties in the interaction were summed to yield scores for the dyad, in keeping with established work using this coding approach to capture systems level relationship processes (Allen et al., Reference Allen, McElhaney, Land, Kuperminc, Moore, OBeirne-Kelley and Liebman2003; Allen et al., Reference Allen, Porter, McFarland, Marsh and McElhaney2005). Inter-rater reliability, calculated using intraclass correlation coefficients, was 0.78, 0.70, 0.42 and 0.67 for mother-adolescent displaying relatedness, relatedness-undermining hostility, displaying autonomy, and undermining autonomy respectively and 0.76, 0.57, 0.61, and 0.70 for the same scales for father-adolescent interactions. These are considered in the good to excellent range for this statistic for all but the mother-adolescent displaying autonomy scale and the father-adolescent relatedness-undermining hostility scales, which were considered in the fair range (Cicchetti & Sparrow, Reference Cicchetti and Sparrow1981).
Paternal and maternal relationship quality with participant (Ages 22-25)
The Inventory of Parent and Peer Attachment (Armsden & Greenberg, Reference Armsden and Greenberg1987) was used annually during each age range listed to assess participants’ perceptions of the quality of their overall relationship with each parent. Relationship quality was calculated as the sum of 14 5-point Likert items capturing communication and trust and seven 5-point items capturing alienation in the relationship (reverse-scored). Scores were obtained separately from mothers and fathers and were averaged across ages to yield the final score for the quality of the participant’s relationship with each parent. Internal consistency was good throughout (Cronbach α ranged from 0.94 to 0.95).
Maternal and Paternal contact (Age 32). Participants were asked how often they had spoken with each parent (in person or via phone) in the past six months. Options ranged from 1 – “Not at all,” to 7 – “Every day or almost every day.”
Loneliness (Ages 30, 32) was assessed via the UCLA Loneliness Scale (Russell et al., Reference Russell, Peplau and Cutrona1980). This 20-item measure assesses loneliness using responses on a 4-point Likert-scale. Scores have been related to outcomes ranging from lower life satisfaction to attachment insecurity (Bowlby, Reference Bowlby1969/Reference Bowlby1982; Goswick & Jones, Reference Goswick and Jones1982; Kobak & Sceery, Reference Kobak and Sceery1988; Moore & Schultz, Reference Moore and Schultz1983). Scores were summed and then averaged across the two assessments to produce a score for early adulthood. Internal consistency for this scale was good (Cronbach α = 0.97).
COVID-related stress (Age 35)
This measure was developed for this study and captured levels of stress due to infection with the COVID virus for oneself, one’s family members and close friends (Cronbach’s α = 0.84), as well as levels of stress due to adverse changes in financial, employment, family life, and social life experiences due to COVID (Cronbach’s α = 0.79). All items were assessed on a scale ranging from 1 “not at all stressful” to 7 “extremely stressful.” Scores for the two different types of stress were standardized then summed to yield a total score for COVID-related stress.
History of serious childhood illness (Adult retrospective report)
Participants retrospectively reported the total number of a series of 43 distinct significant possible health problems first experienced prior to age 18 that led at some point to a hospitalization. Reported serious childhood illness has been found to be a significant predictor of self-reported adult health quality at age 25 (r = .24 p = .006) (Allen et al., Reference Allen, Uchino and Hafen2015). This measure was thus considered as a potential covariate in analyses.
Family income (Age 13)
Family income was measured as a percentage of the federal poverty line (which takes into account both total household income and the number of people supported by that income).
Results
Preliminary analyses
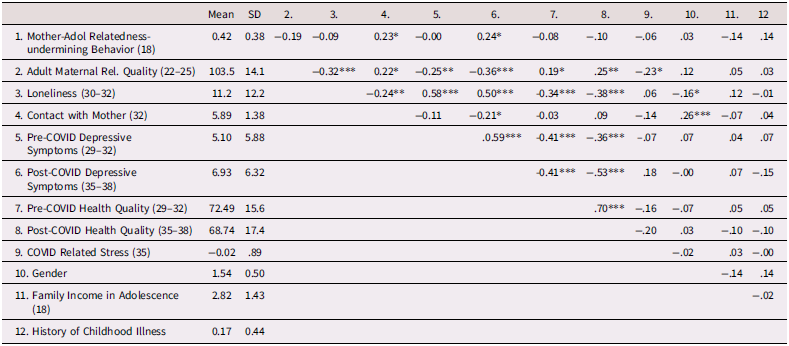
Table 1 presents means, standard deviations, and intercorrelations among the measures used in the primary analyses presented below. Bivariate relations for all other variables in the study are presented in Supplemental Tables A and B. Participant gender and baseline family income were included as covariates in all analyses. We also examined possible moderating effects of gender and family income on each of the relationships described in the primary analyses below. Moderating effects were assessed by creating interaction terms based on the product of the centered main effect variables. No moderating effects were detected with regard to any of the outcome or mediating variables assessed in the study. History of serious childhood illness was also examined as a potential predictor of reported health quality at multiple points in the study. No predictions were observed; hence this variable was not considered further.
Means, standard deviations, and intercorrelations among primary constructs
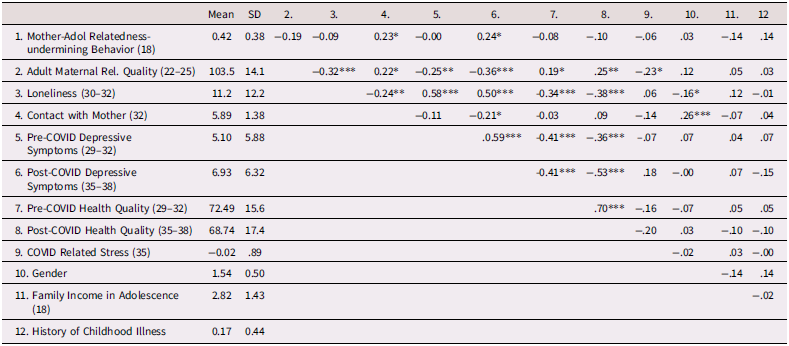
Note: Participant age(s) at time of assessment are in parentheses along with reporter source if other than self-report.
***p < .001. **p < .01. *p < .05.
Primary analyses
Analytic plan
T-tests were used to examine pre- post- changes in depressive symptoms and health status in relation to the COVID pandemic. For all other analyses, SAS PROC CALIS (version 9.4, SAS Institute, Cary, NC) was employed using full information maximum likelihood handling of missing data. Hierarchical linear regression analyses were first used to separately predict either depressive symptoms or health outcomes. Analyses first entered gender, adolescent-era family income and COVID-related stress as covariates, followed by pre-COVID measures of the outcome of interest and relevant predictors. Regressions were followed by path analyses in which all potential predictors for each path were entered into an initial model, with non-significant paths then deleted and fit indices used to assure that no significant, temporally feasible paths were omitted.
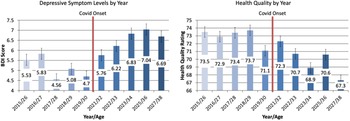
Change in depressive symptoms and health quality from pre- to post-COVID onset
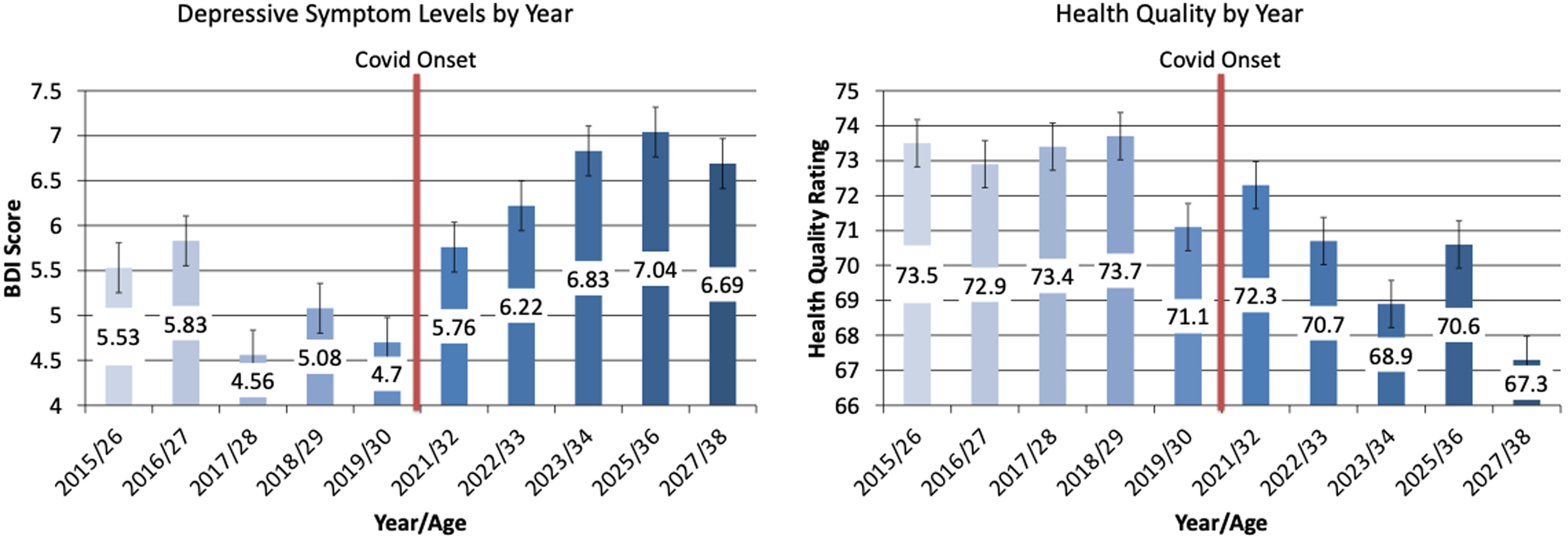
Analyses first examined whether there was actually an increase in depressive symptoms and a decrease in physical health quality from pre- to post-COVID onset assessments. Within subject T-tests examined absolute change in both depressive symptoms and health quality and indicated significant expected changes in both indicators (T depr. sx = 3.61, p < .001; T Phys Hlth. = −3.76 p < .001). To further assess whether these changes might potentially just be a continuation of longer-term trends (e.g., effects of aging vs. effects related to COVID), we similarly examined levels of change in the period from 4 to 6 years prior to COVID onset to the period 1 to 3 years prior to COVID onset. Results indicated no significant changes in depressive symptoms (p = .97) or reported health quality (p = .53) in the period leading up to the pandemic. We then further examined specific year-by-year levels of depressive symptoms and health quality over the period of the study extending up to six years pre-COVID. Results are presented in Figure 2 and show a clear uptick in symptoms and decline in health quality immediately following the onset of the pandemic.
Changes in depressive symptoms and health quality over time.
Predicting pre- to post-COVID relative change in depressive symptoms and physical health quality
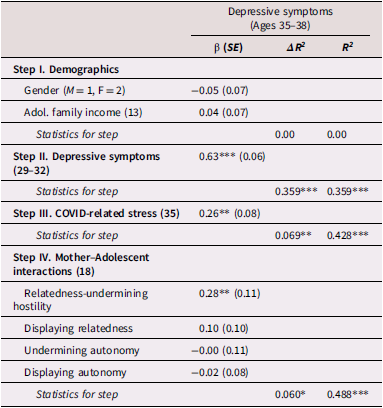
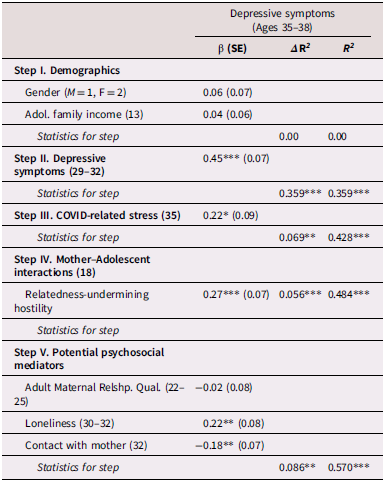
Results presented in Table 2 show, first, the expected significant degree of continuity in depressive symptoms across the age span examined. After accounting for that continuity, the level of reported COVID-related stress at age 35 predicted higher levels of depressive symptoms post-COVID. Next, parent–adolescent dyadic behavior was entered as a predictor. Mother–adolescent relatedness-undermining hostile behavior in late adolescence further predicted an increase in depressive symptoms from pre- to post-COVID as shown in Table 2. Analyses of father-adolescent interactions were not found to be a significant predictor (p = .79, Supplemental Table C). Hence father-adolescent interactions were not considered further in primary analyses regarding depressive symptoms.
Predictions to post-COVID depressive symptoms (Ages 35–38)
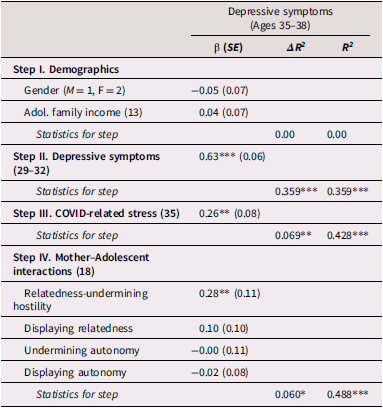
Note: Participant age(s) at time of assessment are in parentheses. β weights are from final model.
***p < .001. **p < .01. *p < .05.
Using the same approach as shown in Table 2, analyses examined parent–adolescent dyadic behavior as a predictor of relative change in physical health quality. The block of maternal-adolescent behaviors was not predictive of post-COVID health quality (Supplemental Table D). Father adolescent dyadic behavior was also not predictive of relative change in depressive symptoms or physical health quality (Supplemental Tables E, F & G).
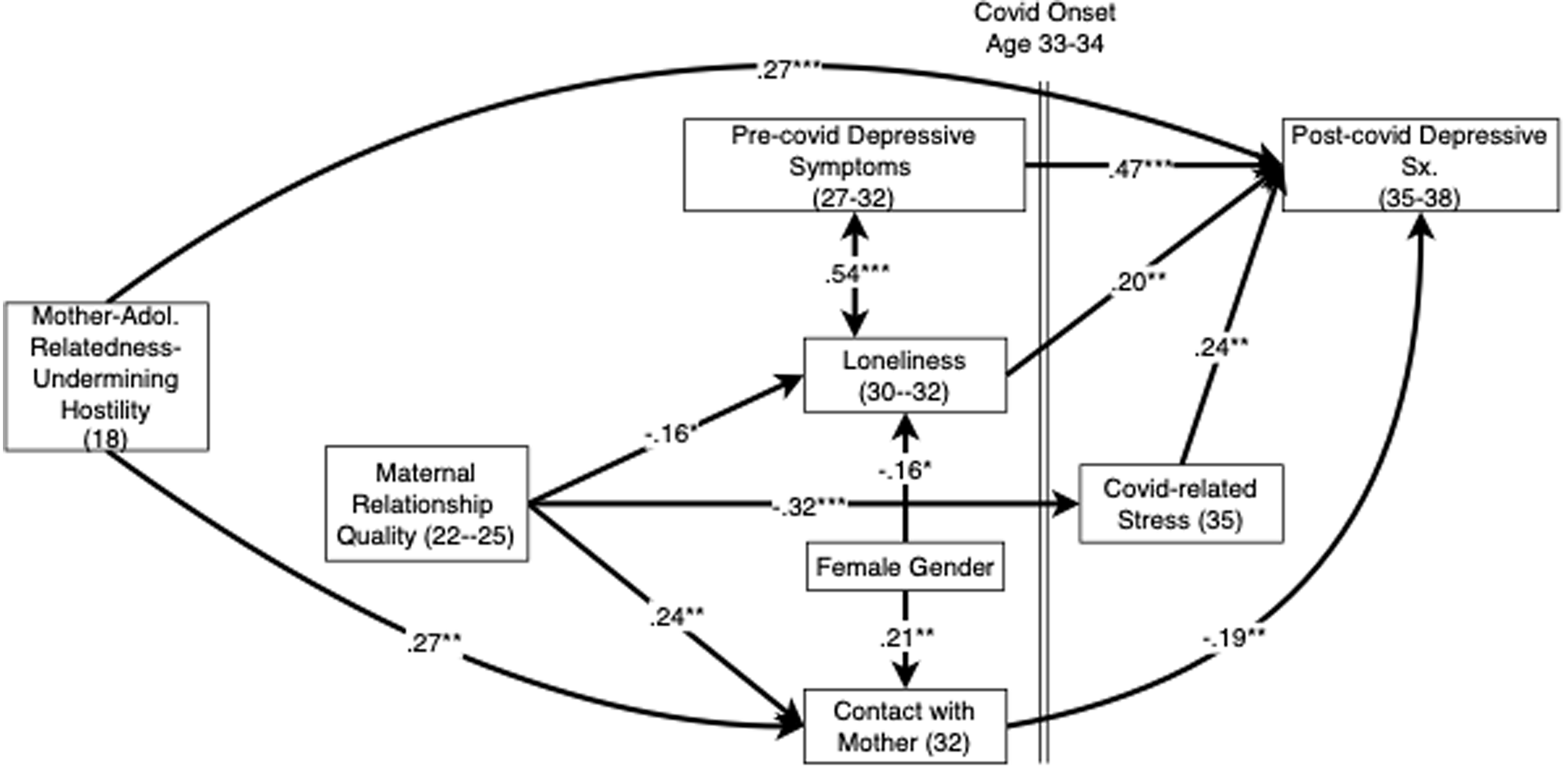
Potential mediators of change in depressive symptoms and physical health quality
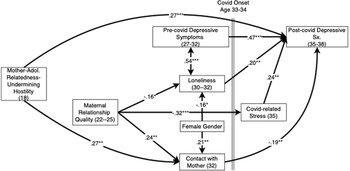
Table 3 presents analyses examining relational factors that potentially mediate the link between relatedness-undermining hostile mother–adolescent interactions and relative increases in depressive symptoms post-COVID. Both higher levels of loneliness at ages 30–32 and lower levels of contact with mothers at age 32 predicted relative increases in depressive symptoms from pre- to post-COVID assessments. Path analysis was then used to further explore this relationship. The final model, shown in Figure 3, fit the data well (χ2 (10) = 8.26, p = .60, GFI = 0.98, AGFI = 0.92, RMSEA = 0.00). (Statistics for fully saturated initial models are included in Supplemental Table H for all path models.) Mother–adolescent relatedness-undermining hostile behavior was found to directly predict post-COVID depressive symptoms (and was unrelated to symptom levels pre-COVID) and was also inversely predictive of future contact with mother at age 32. In addition, maternal relationship quality in early adulthood predicted future levels of contact with mothers at age 32, reduced loneliness at age 30 to 32, and lower COVID-related stress, each of which in turn predicted lower levels of depressive symptoms post-COVID.
Predictors of changing depressive symptom levels pre- and post-COVID.
Note: Pathways examined but found non-significant and dropped from the final model include all pathways from a given variable to all other variables to its right other than those paths already depicted. The one exception was female gender, which was examined as a potential predictor of all variables.
Predictions including mediators to post-COVID depressive symptoms (Ages 35–38)
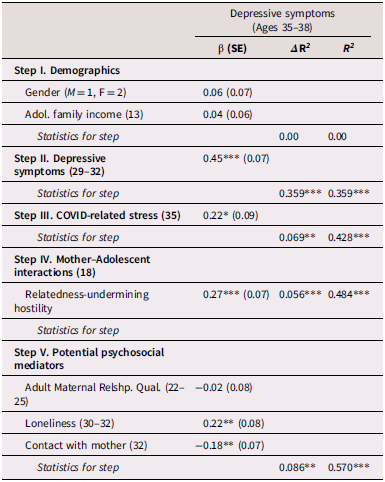
Note: Participant age(s) at time of assessment are in parentheses. β weights are from final model.
***p < .001. **p < .01. *p < .05.
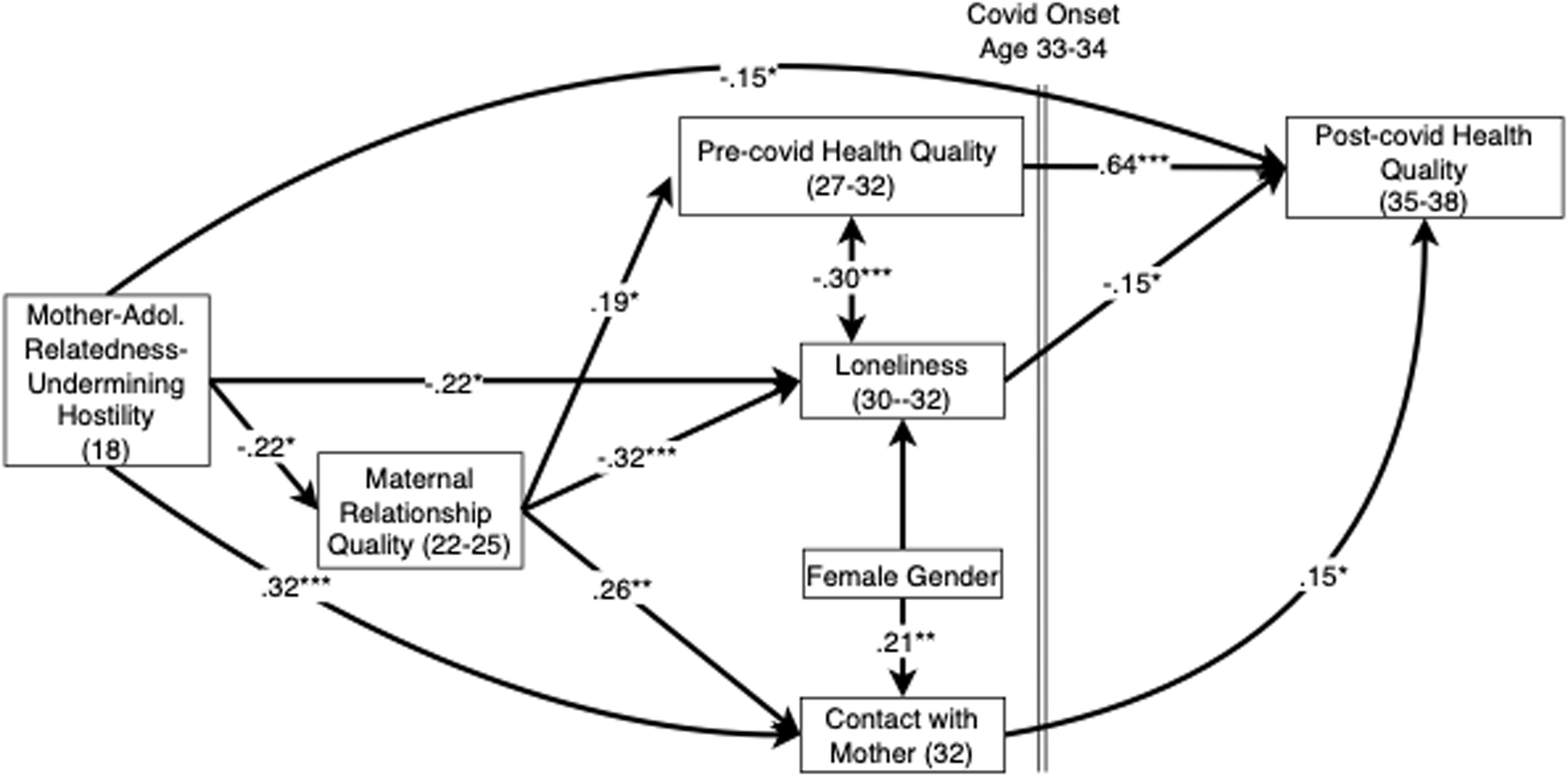
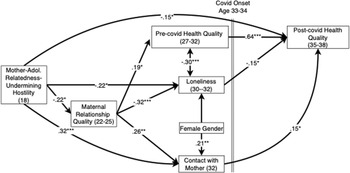
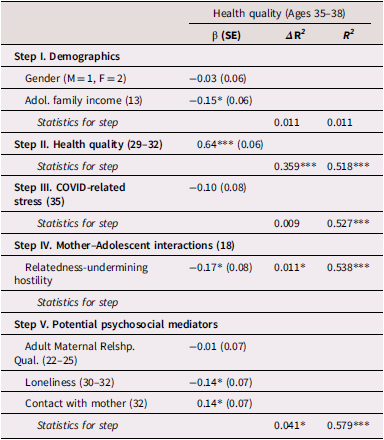
Analyses next examined predictors and potential mediators of relative changes in physical health quality. Maternal-adolescent relatedness-undermining hostile behavior was included in these analyses given that it was shown above to predict several relationship qualities later in development. Results shown in Table 4 support largely parallel those seen in predictions of depressive symptoms, with relative decreases in health quality predicted by relatedness-undermining hostile mother–adolescent interactions, greater adult loneliness, and less adult contact with mother. Figure 4 presents follow-up path analyses examining interrelations among these factors. The final model fit the data well (χ2 (8) = 10.1, p = .26, GFI = 0.98, AGFI = 0.93, RMSEA = 0.04). Observed maternal-adolescent relatedness-undermining hostile behavior was predictive of each of the three potential mediators. As with analyses of prediction of depressive symptoms, early adult maternal relationship quality appeared to mainly have its relation to future health quality mediated via loneliness, contact with mother and pre-COVID health quality. Prediction from mother–adolescent relatedness-undermining hostile behavior to future contact with mother was unexpectedly positive, though examination of zero-order correlations in Table 1 suggests this was likely a suppressor effect given the range of other significant predictions.
Predictors of changing health quality pre- and post-COVID.
Note: pathways examined but found non-significant and dropped from the final model include all pathways from a given variable to all other variables to its right other than those paths already depicted. The one exception was female gender, which was examined as a potential predictor of all variables.
Predictions including mediators to post-COVID health quality (Ages 35–38)
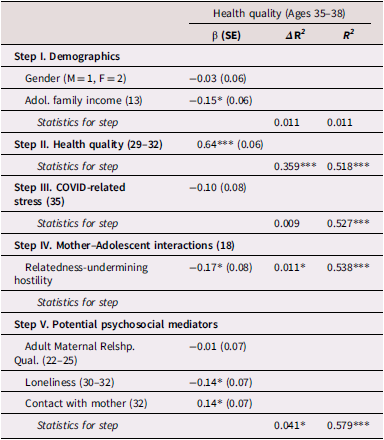
Note: Participant age(s) at time of assessment are in parentheses. β weights are from final model.
***p < .001. *p ≤ .05.
Post-hoc analyses
Effects as a possible result of aging/developmental change
Analyses next considered the possibility that the familial and social integration constructs examined were simply predictors of ongoing developmental change (i.e., irrespective of the presence of a major stressor). To test this possibility, we examined whether these constructs were predictive of changes taking place in the six years completely prior to COVID (i.e., predicting depressive symptoms and health quality changes from ages 26–28 to ages 29–32). Loneliness was not included in these models since it was assessed contemporaneously with the age 29–32 outcome assessments. Results, using the same regression approach in Tables 3 and 4, indicated no significant relation of the predictor variables to relative change in either outcome over the six years pre-COVID (p’s = .17 and .95 for depression and health models respectively). This indicates that the predictors examined were not simply predicting broad developmental change over time and were only predictive of change during the period immediately preceding and following the onset of the COVID pandemic.
Exploratory paternal relationship analyses beyond adolescence
Although no paternal relationship qualities in adolescence were found to be predictive of response to COVID stress, for exploratory purposes, post-hoc analyses considered whether paternal relationship qualities beyond adolescence might predict response to COVID stress. No effects were found for predictions of post-COVID depressive symptoms. However, in one analysis (paralleling Table 4 for mothers), greater contact with fathers at age 32 predicted relatively greater post-COVID health quality (Supplemental Table G).
COVID stress as a potential moderating variable
Although self-reported stress due to COVID was included as a covariate in all models, this post-hoc analysis considered whether it also might serve to moderate the effects of the predictors examined. Moderation was assessed as the product of the standardized form of the relevant variables. No significant moderation was observed.
Discussion
The results of this study provide evidence that maternal relationship qualities from late adolescence onward are linked to multi-decade resilience in the face of stress. The study utilized the widespread stress created by the COVID pandemic to examine which individuals would navigate this period without experiencing relative increases in depressive symptoms or decreases in physical health. We found that when mother-adolescent dyads were able to handle the stress of discussing a significant disagreement without devolving into hostility, those adolescents as adults were less likely to experience relative increases in depressive symptoms or decreases in physical health from the years prior to the onset of COVID to the years following its onset. These outcomes are significant given that depression has been identified as the single greatest source of disability worldwide (World Health Organization, Reference Organization2017) and reported health status has been found to consistently yield strong predictions to future health and mortality risk (DeSalvo et al., Reference DeSalvo, Bloser, Reynolds, He and Muntner2006; McHorney et al., Reference McHorney, Ware and Raczek1993; Stewart et al., Reference Stewart, Hays and Ware1988).
Effects of this early protective factor appear to have been potentially mediated both by future indicators of the adult child’s maternal relationship quality and by evidence of general social integration (i.e., the relative absence of loneliness) prior to the pandemic. To a large extent what this study found was evidence of downstream predictions from a resilient relationship, one that could maintain equilibrium even under stress. In adolescence the stress was observed in a discussion of a significant area of disagreement while being videorecorded. Success in managing this sort of stressful interaction without devolving into hostility may well have marked a relationship that was also going to be able to withstand the stress of the COVID pandemic. Establishing such a relationship was predictive of a better relationship with mothers and to lower loneliness in the years leading up to the pandemic – each of which was in turn predictive of better response in the years that followed. These results are in line with recent work suggesting the value in adopting a systems perspective on resilience (Masten, Reference Masten2024). This is also in keeping with the notion that progress in key developmental tasks – in this case, the adolescent’s need to establish autonomy without undermining relationships with parents – will be a likely source of future resilience.
Although there are several limits to the study as noted below, the findings establish the basic logic of identifying mother-adolescent relationship quality as a long-term source of resilience. First, that the pandemic did indeed appear to serve as a stressor in this sample as indicated by clear increases in depressive symptoms and decreases in health quality following its onset. Second, that relationship quality predicted better adjustment, even accounting for adjustment prior to the pandemic. And finally, relationship quality did not predict similar changes in the years leading up to the pandemic. Rather, it was only in the presence of a significant stressor that the effect of mother-adolescent relationship quality became apparent. Taken together, these findings suggest that what was being observed were true protective factors, in that they allowed the individual to continue to maintain their level of functioning even in the face of a significant stressor (Rutter, Reference Rutter2023).
These findings also extend our understanding of the role of mothers beyond late adolescence. As an individual’s focus shifts from parents to peers and romantic partners in the transition from adolescence to adulthood, the parent’s role, including their levels of contact with the adult offspring, recedes (Rosenthal & Kobak, Reference Rosenthal and Kobak2010). However, the present findings are consistent with the view that the supportive functions of parents, though largely dormant given the increased competence and independence that come with adulthood, nonetheless remain present to be called on when needed. This finding can be best interpreted in the context of attachment theory, which suggests that the parent-child attachment system appears designed to “turn on” under conditions of stress and leads the individual – whether an infant in pain, or an adult in challenging circumstances – to reach out to attachment figures for support (Bowlby, Reference Bowlby1973, Reference Bowlby1980). The present findings suggest that the time span over which this relationship remains active as a potential source of support can be quite extensive – up to 20 years in this case.
This study also found evidence that early adult maternal relationship quality predicted lower levels of COVID-related stress in some models. One explanation is that a positive ongoing maternal relationship might have operated as a source of emotional support. Alternatively, a positive relationship also could have reflected availability of financial backup in case of illness, job loss and related stressors. Relatedly, a history of low family income in adolescence predicted poorer health outcomes in some regression models. It may be that growing up in a family with fewer financial resources led to less capacity to weather the pandemic (i.e., via inability to work remotely, lack of financial buffers, etc. (Whitehead et al., Reference Whitehead, Taylor-Robinson and Barr2021)).
Notably, the clearest findings were obtained only with respect to the maternal-adolescent relationship, and only relative to the presence/absence of hostility in that relationship (as opposed to positive markers of progress in autonomy processes). These findings are consistent with an extensive literature suggesting that in spite of evolving family structures and gender roles, in most families, mothers still serve as primary caregivers (Allport et al., Reference Allport, Johnson, Aqil, Labrique, Nelson, Kc, Carabas and Marcell2018). Although gendered distinctions in parenting roles have tended to become less prominent over time, these data were first collected around 2003. Hence distinctions between maternal and paternal roles may have been stronger than than they are currently.
A contrasting perspective is suggested by findings in post-hoc analyses that levels of contact with fathers at age 32 were in fact linked to post-COVID health quality, controlling for prior health quality. This suggests the possibility that the much smaller number of father-adolescent interactions available in adolescence for this sample and lower reliability in coding father-adolescent interactions limited power in a way as to preclude detection of significant effects. Notably, the variable assessing age 32 levels of contact did not require fathers to be physically present; hence sample sizes were much larger. This issue of lack of father findings due to smaller numbers of fathers in most samples is one that inevitably pervades much developmental research and may well have been at play here.
It should also be noted that this paper has framed findings in terms of resilience, yet Luthar has suggested that resilience factors can and should be viewed as lying on a bipolar continuum (Luthar & Zelazo, Reference Luthar and Zelazo2003). This perspective is particularly relevant to this study, where findings could have just as easily been framed from a diathesis/stress/vulnerability perspective. Although we framed results as showing that establishing a parent-teen relationship able to avoid hostility when disagreeing was a source of potential resilience, the alternative perspective warrants consideration: A history of difficulties establishing autonomy without hostility by late adolescence could be seen as creating an underlying diathesis, such that when a potent new stressor emerges in adulthood the individual is particularly vulnerable to depressive symptoms and deterioration in health status. In this view, lack of progress in a key developmental task may create an enduring fragility vis a vis future stressors.
Several limitations in this study warrant note. Most importantly, although the COVID pandemic provided a unique opportunity to study a nearly universally experienced set of stressors, the pandemic did not affect all individuals equally; while all individuals experienced certain stressors, other stressors (e.g., severe illness, loss of job, etc.) were experienced unevenly. In particular, the study was not able to conduct in depth medical assessments to determine the precise physical impact of COVID exposure on participants. Relatedly, this study was not able to assess all relevant factors pre-COVID that might have influenced, not simply resilience, but also just how much stress a given individual actually experienced from pandemic-related stressors. It is possible that the factors identified as sources of resilience might also have been predictors of a lower frequency of stressors experienced and lower levels of stress as a result of COVID. As with most resilience research, it remains difficult to draw the line between factors that predict that a given experience will be less stressful to the individual vs. predicting that the actual stress of the experience will be less impactful (Luthar et al., Reference Luthar, Cicchetti and Becker2000). Although we sought to measure COVID-related stress and found this to be at least somewhat predictive of outcomes, our capacity as a field to capture the multi-faceted elements of such stress remains limited. It also seems likely that by accounting for COVID-related stress in analyses, we also removed some of the effects of that stress on individuals, given the difficulty of disentangling the two phenomena. This may have led to an underestimate of the protective effects of the relationship qualities assessed.
A second limitation of the study is that the years characterized by COVID were also characterized by innumerable other stressors, both on a population level, but also in developmental terms, as individuals progressed through their thirties. Although numerous studies have now suggested population wide negative effects from the pandemic (Nochaiwong et al., Reference Nochaiwong, Ruengorn, Thavorn, Hutton, Awiphan, Phosuya, Ruanta, Wongpakaran and Wongpakaran2021; Penninx et al., Reference Penninx, Benros, Klein and Vinkers2022; van de Weijer et al., Reference van de Weijer, de Vries, Pelt, Ligthart, Willemsen, Boomsma, de Geus and Bartels2022; Zhu et al., Reference Zhu, Jiang, Yang, Dzierzewski, Spruyt, Zhang, Huang, Ge, Rong and Ola2023), other factors, including the effects of physical aging could well have altered patterns of adaptation in ways this study was not able to capture. Thus, it was not possible to determine to what extent sample-wide adverse changes following the pandemic were in fact due to the effects of the pandemic vs. other factors. Also, although post-hoc analyses suggested that factors predicting resilience were not simply predicting changing levels of functioning across the years prior to COVID, this is not sufficient to establish that the observed changes in functioning post-pandemic were causally linked to the predictors examined. Finally, given the lack of a full cross-lagged design, the role of intervening factors as mediators of earlier family relationship qualities should only be considered suggestive at this point.
A third type of limitation regards predictions from adolescent-parent interactions: Caution must be used in interpreting predictions from both mother-adolescent and father-adolescent relatedness-undermining hostility to health outcomes as in both cases these predictions only appeared in some of the analyses examined. This limitation is particularly salient given the number of variables examined relative to the fairly modest sample size. Finally, several of the parent-adolescent interaction scales had relatively low reliabilities, which could account for the lack of findings with these scales.
Even given these limitations, this study demonstrates that in the context of a widespread, significant stressor, individuals who enjoyed positive maternal relationships and better social integration prior to the onset of the stressor fared significantly better than individuals lacking these advantages. Although these results obviously await further replication and generalization, they suggest a potential very long-term role for family relationship qualities as protective factors increasing the likelihood of resilience in the face of stress.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579426101448.
Data availability statement
Consent procedures originally used in this study did not allow for dissemination of the data to others, and critical data (observations) is not confidential). Hence data are not generally available to others, although inspection of data and results can be made via request to the first author.
Acknowledgments
This study was supported by grants from the National Institute of Child Health and Human Development and the National Institute of Mental Health (5R37HD058305-23, R01HD058305-16A1, R01-MH58066). Correspondence can be addressed to the first author at Department of Psychology, University of Virginia, PO Box 400400, Charlottesville, VA 22904-4400. Email: allen@virginia.edu. Phone: 434 982-4727.
Funding statement
This study was supported by grants from the National Institute of Child Health and Human Development and the National Institute of Mental Health (5R37HD058305-23, R01HD058305-16A1, R01-MH58066).
Competing interests
The authors declare no conflicts of interest.
Pre-registration statement
The study was not pre-registered as it was exploratory in nature.



 Open access
Open access