


Highlights
-
• Six randomized controlled trials of cerebral aneurysms were analyzed, and hydrogel-based coiling (HBC) outcomes were compared to bare platinum coiling (BPC) outcomes.
-
• HBC cohorts had significantly lower aneurysm recurrence rates and higher follow-up occlusion rates.
-
• Our study may augment the current literature view on HBC utilization.
Introduction
Coiling has long been established as a safe and effective treatment option for cerebral aneurysms.Reference Brisman, Song and Newell1,Reference Lindgren, Vergouwen and Van Der Schaaf2 Bare platinum coiling (BPC) has been established as the standard of care in both ruptured and unruptured intracranial aneurysm coiling. However, it remains controversial whether there may be better options for treatment. Retreatment rates over time and the higher risk of incomplete initial occlusion compared to other coiling methods have prompted clinicians to explore other options of treatment.Reference Abi-Aad, Rahme and Patra3,Reference Cortese, Ghozy and Zarrintan4 One option that has shown potential to become the new standard of care is the hydrogel-based coiling (HBC). HBCs are a form of bioactive coiling that expand when in contact with blood. While investigation into the effectiveness and outcomes of the HBC in the treatment of intracranial aneurysms remains limited, few studies have highlighted its promising capabilities.
A recent systematic literature review analyzed recurrence at final follow-up, residual neck and dome rates and complications.Reference Abi-Aad, Rahme and Patra3 The study compared first- and second-generation HBC to BPC controls. While initial occlusion rates did not differ, it was revealed that first- and second-generation HBC had lower recurrence rate and higher packing density when compared to BPC. Another more recent meta-analysis compared five randomized controlled trials (RCTs) with patients receiving HBC and BPC for the treatment of ruptured and unruptured aneurysms.Reference Cortese, Ghozy and Zarrintan4 Both HBC and BPC had comparable initial occlusion rates and packing attenuation. However, it was found that HBC cohorts had lower recurrence rates at 18 months post-operation. The study concluded that HBC has similar safety profiles with lower rates of recurrence at follow-up.
Despite this, data on long-term outcomes are lacking from RCTs and remain scarce in alternative study designs. It remains challenging to form a complete picture of the safety profile and both the short- and long-term outcomes of HBC. This limitation makes it so that clinicians lack robust data that may help them take critical decisions, balance potential risks against benefits for each patient and avoid negative outcomes. Thus, in this study, our objective was to systematically analyze previous and novel RCTs to add onto our knowledge of HBC and its efficacy in treating intracranial aneurysms.
Methods
Study selection
A thorough review of different electronic databases was conducted, following the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA).Reference Page, McKenzie and Bossuyt5 These databases include PubMed, Google Scholar, EMBASE and Cochrane Library. Inclusion Criteria included 1) RCT post-2010, 2) directly compared patients who underwent HBC versus patients who underwent BPC and 3) studies only including intracranial aneurysms. Exclusion criteria included 1) any case reports, case series, case control studies and 2) any RCTs that compared other forms of bioactive coiling to BPC (Figure 1). MeSH terms included “Bare platinum coiling,” “hydrogel-based coiling,” “intracranial aneurysms,” “ruptured OR unruptured aneurysms,” “BPC and HBC” and “aneurysm coiling treatment.”
PRISMA flowchart.

Data extraction
Data extracted from the comprised studies included i) patients’ demographic data (age and gender), ii) mean sizes of presenting aneurysms and aneurysm necks and iii) ruptured/unruptured aneurysms. Clinical data extracted included i) aneurysm recurrence, ii) occlusion rate (immediate and at follow-up), iii) retreatment, iv) morbidity, v) mortality, vi) mRS scores post-treatment and vii) rates of complications.
The primary endpoints of this study were determined to be immediate occlusion, retreatment and aneurysm recurrence rates. Secondary endpoints comprised of occlusion rate at follow-up, morbidity, mortality and mRS scores (0–2) post-treatment.
Statistical analysis
R Studio Version 2025.09.0 + 387 was used for statistical analysis and plot generation. Dichotomous data were analyzed using the odds ratio (OR), while pooled weighted mean difference was implemented to analyze dichotomous data. For the majority of the reported results, an OR value was provided with 95% confidence intervals (CIs) using the Mantel–Haenszel method under a random-effects model with Hartung–Knapp adjustment to account for between-study variability. A continuity correction (0.5) was applied when zero events were present. For pooled weighted mean difference results, a t-test was conducted to detect if any statistically significant difference exists between both cohorts. All tests were two-tailed, and a p-value< 0.05 was determined significant.
Heterogeneity was assessed through the use of I 2 statistics. An I2 value ≥ 50% was considered highly heterogenous, and a random-effect model was employed. Forest plots were generated using the meta package in R Studio to visually summarize findings.
Risk of bias
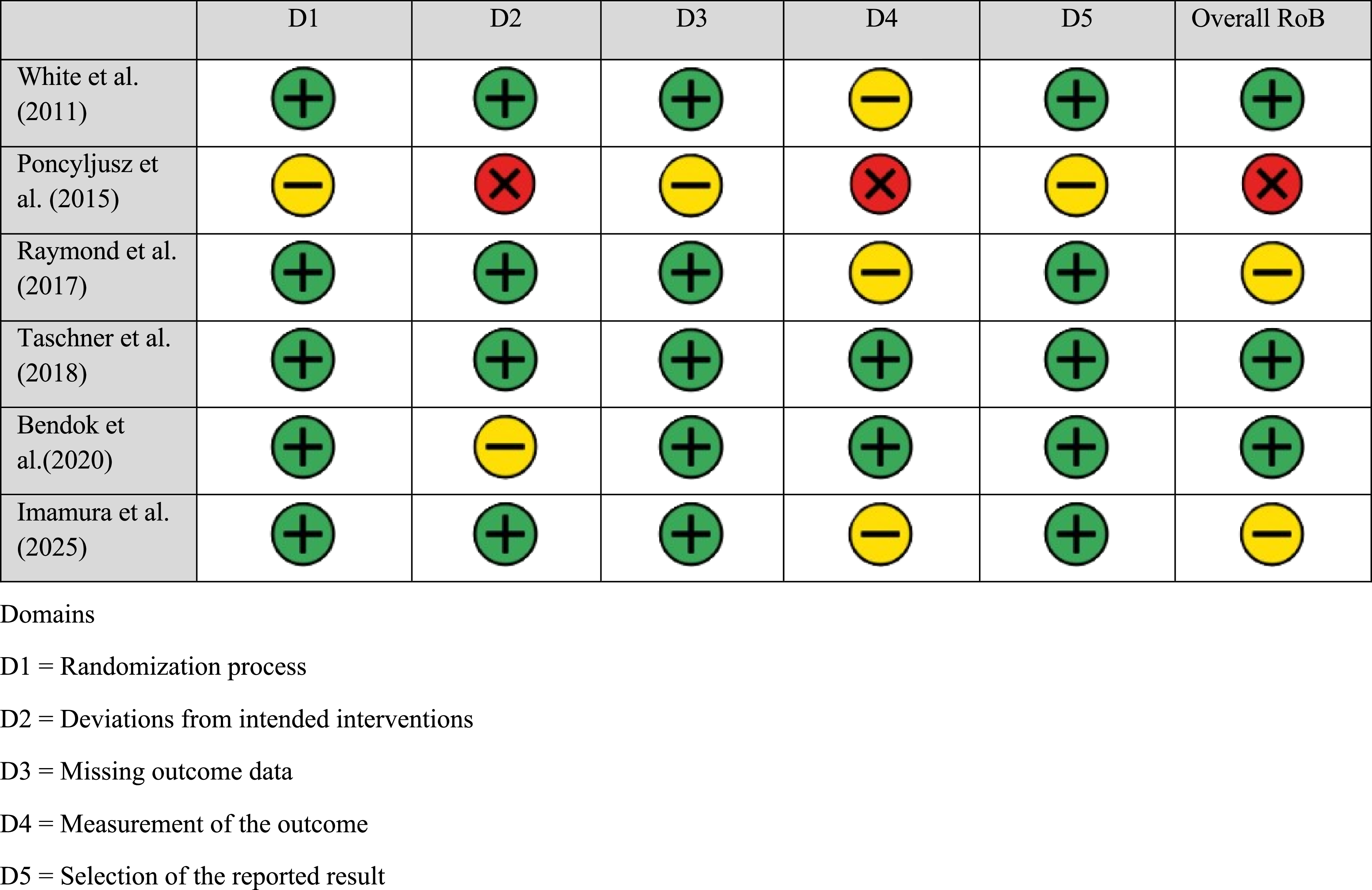
Risks were compared across all studies by two authors. Following the Cochrane risk of bias (Cochrane RoB 2) framework for RCTs,Reference Sterne, Savović and Page6 the biases compared included randomization, performance, attrition, detection and reporting/selection bias (Figure 2). The risk of bias for each domain was classified as low risk, some concerns or high risk, visually represented by green, yellow and red circles, respectively.
Summary table of the risk of bias of each study based on Cochrane RoB 2.

Results
Study inclusion and characteristics
A total of 153 studies were identified across all electronic databases (Figure 1). Out of these studies, 94 were not included as the methods of analysis did not align with our purpose of our systematic review. Furthermore, the application of the inclusion and exclusion criteria on the remaining 59 articles allowed us to exclude 53 studies, leaving us with a total of 6 RCTs.Reference Bendok, Abi-Aad and Ward7–Reference Poncyljusz, Zarzycki, Zwarzany and Burke12 A total of 2,551 patients were included in our study with 1278 in the HBC group and 1273 in the BPC group. Patient demographics were reported in Table 1. Out of all the studies included, five reported the gender split between patients. Out of all HBC patients, a reported 59.0% (n = 754) were females. A similar 59.1% (n = 752) female patients were reported in the BPC group. Excluding one study which only reported on unruptured aneurysms, 299 ruptured aneurysms were reported in HBC patients (23.4%) and 317 in BPC patients (24.9%). Mean ages were 55.84 and 56.89 in the HBC and BPC cohorts, respectively. Aneurysm dome sizes were similar between cohorts (8.51 mm in HBC vs. 8.71 mm in BPC), as were neck sizes (4.14 mm vs. 4.18 mm, respectively).
Demographics of patient population

HBC = hydrogel-based coiling; BPC = bare platinum coiling.
Primary and secondary outcomes
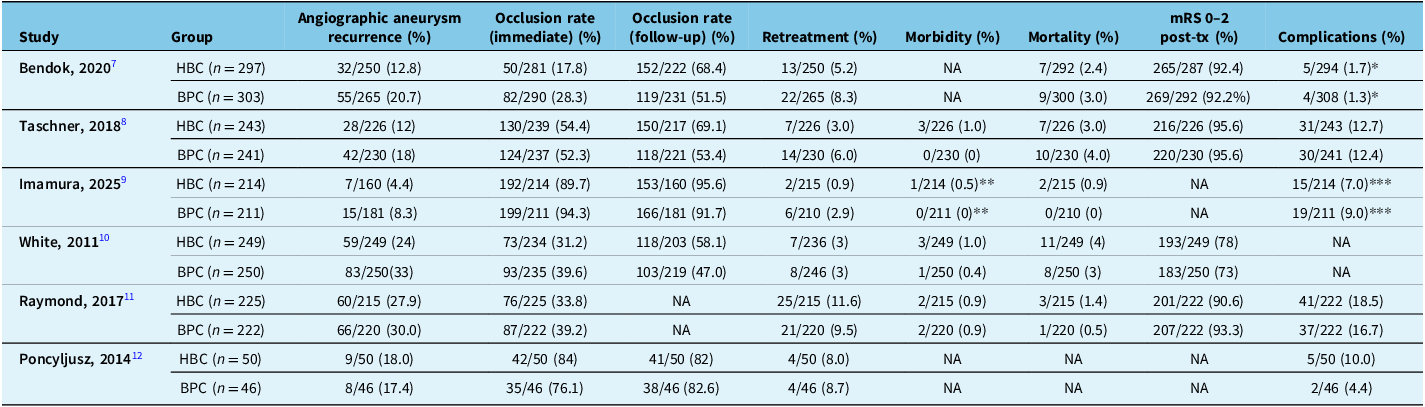
All results are reported in Table 2 and Figure 3. Primary endpoint analysis showed comparable results between both groups. While a trend was observed in favor of HBC patients when evaluating immediate occlusion rates, no significance was detected (OR 0.7682; 95% CI 0.5351; 1.1029; p = 0.1197). Retreatment rates indicated no significant differences between both cohorts (OR 0.7674; 95% CI 0.4759; 1.2373; p = 0.2135). Aneurysm recurrence rates were significantly reduced in the HBC cohort compared to BPC (OR 0.6807, 95% CI 0.5364; 0.8638, p = 0.0089).
Primary and secondary endpoints

* Only Includes Hemorrhage related to device and/or procedure.
** Any complication within 1 year of operation.
*** Any event or death within 30 days of operation.
HBC = hydrogel-based coiling; BPC = bare platinum coiling.
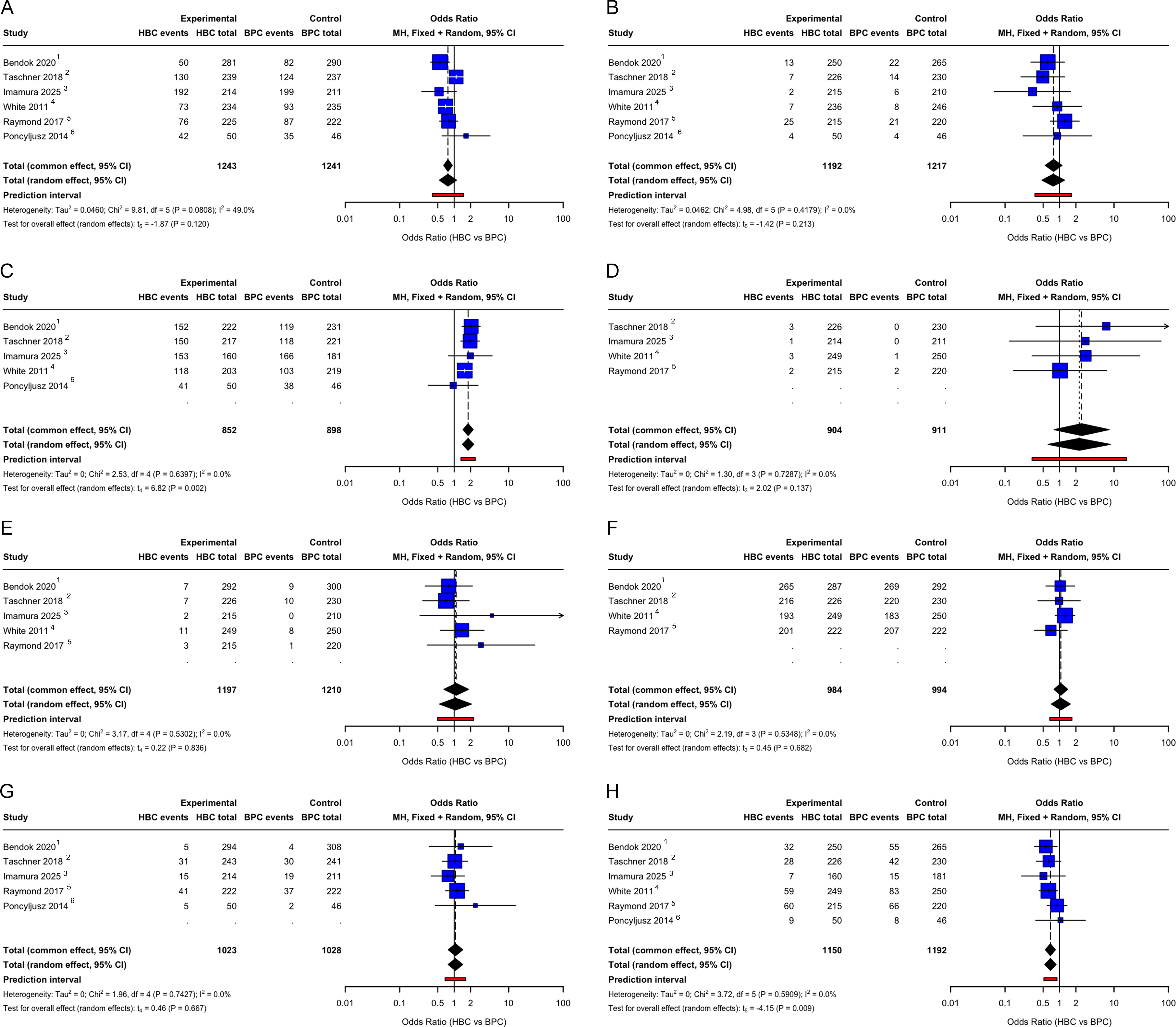
Forest plots of primary and secondary outcomes: (A) occlusion rates, (B) retreatement rates, (C) occlusion rates at follow-up, (D) morbidity, (E) mortality, (F) mRS scores, (G) complications and (H) recurrence.

Secondary endpoint analysis also showed variable results between both HBC and BPC cohorts. At follow-up, the HBC cohort had a 1.79-fold increase in successful occlusion compared to the BPC cohort (OR 1.7992, 95% CI 1.4167; 2.285, p = 0.0024). Morbidity and mortality rates did not show any changes between HBC and BPC (p = 0.1371 and p = 0.8364, respectively). In addition, there were no statistically significant differences when evaluating positive mRS scores (0–2) (p = 0.6819) and rate of complications (p = 0.6671) between both methods of coiling.
Discussion
HBC is the use of core platinum coils coated with hydrogel material containing several characteristics that are not available with standard BPC. HBC allows for the absorption of fluid and its subsequent expansion, resulting in higher packing densities.Reference Ferral13 While many intracranial aneurysms were occluded with the use of BPC, HBCs are gaining popularity as a potential alternative treatment. However, very limited research has been done to analyze the efficiency and safety profile of HBC. Xue et al.Reference Xue, Chen, Lin, Xu, Shen and Wang14 was one of the first groups to systematically evaluate RCTs that aimed to analyze the differences between HBC and BPC.Reference Xue, Chen, Lin, Xu, Shen and Wang14 The final version of the manuscript included 4 RCTs, which included 1,526 patients in total (HBC = 767; BPC = 759). Xue et al.Reference Xue, Chen, Lin, Xu, Shen and Wang14 also focused on periprocedural events including but not limited to failed procedure, coiled migration and perforation. It was found that HBC had no difference in terms of reducing these events. While it may be argued that this may be subject to physician expertise acting as a confounding variable, similar results to our paper in the post-procedural outcomes were reported. For example, no significant differences were seen in mid-term efficacy outcomes, which included intracranial aneurysm recurrences, complete occlusion and excellent functional outcomes (mRS = 0). Interestingly, HBC patients actually reported significantly better good functional outcomes (mRS = 0–2) post-procedure when compared with their BPC counterparts. Finally, while BPC patients revealed lower rates of recurrence (p = 0.008) and residual aneurysm (p = 0.002), both cohorts showed comparable results in stroke, morbidity and mortality rates. Xue et al.Reference Xue, Chen, Lin, Xu, Shen and Wang14 had shown that even though HBC may offer better results in some outcomes, its safety profile and overall efficacy were no different than BPC. A similar systematic review and meta-analysis was conducted 7 years later by Cortese et al.Reference Cortese, Ghozy and Zarrintan4 This time, 5 RCTs were included in the final version of the analysis with 2,126 patients (HBC = 1064 and BPC = 1062). In line with our findings, significant differences emerged only when assessing major recurrences (p = 0.03) and residual aneurysms (p = 0.01), both of which favored the HBC cohort. In addition, HBC trended toward better complete occlusion at follow-up, yet the results were still not significant (OR 1.21; 95% CI 0.99–1.48; p = 0.06). That said, after discovering substantial heterogeneity between the included studies (I 2 = 54%, p = 0.09), an outlier study was removed. Once the outlier was removed, a significantly higher rate of complete occlusion at the last follow-up was revealed in favor of the HBC group (OR 1.29; 95% CI 1.18–1.42; p = 0.001).
Results from Cortese et al.Reference Cortese, Ghozy and Zarrintan4 and Xue et al.Reference Xue, Chen, Lin, Xu, Shen and Wang14 helped shape our understanding of HBC’s safety profile and efficacy in treating patients.Reference Cortese, Ghozy and Zarrintan4,Reference Xue, Chen, Lin, Xu, Shen and Wang14 However, a key consideration is that these studies analyzed a total of nine RCTS, with four overlapping studies. In other words, only five RCTs comparing HBC to BPC in intracranial aneurysms were conducted and analyzed to this day. Therefore, the generalizability of both of these results remains limited, and further research would help strengthen these findings. Our study helps add to these findings by evaluating a sixth RCT conducted in 2024, adding 432 patients to be analyzed.Reference Imamura, Sakai and Sakai9
Previous non-RCT studies have also evaluated the differences between HBC and BPC in the past. As early as 2006, Gaba et al. compared 50 HBC aneurysms (17 small, 26 medium and 5 large) to 57 BPC aneurysms (29 small, 24 medium and 4 large) and looked to analyze many metrics including volume percentage occlusion (VPO) and length of hospital stay.Reference Gaba, Ansari, Roy, Marden, Viana and Malisch15 It was found that HBC yielded higher VPO compared to BPC (p = 0.016). On the other hand, no differences in length of hospital stay were detected. This study also found that although HBC incurred higher initial costs, these were balanced by reduced recurrence rates, something that clinicians may want to consider. This is especially relevant when discussing centers with limited resources. Therefore, it requires careful evaluation from the clinicians on site to judge whether the implementation of HBC for reducing recurrence rates is feasible. In 2014, Lee et al. tested both coiling methods in a single-center experience.Reference Lee, Seo and Lee16 This time, 430 and 253 intracranial aneurysms were compared in the HBC and BPC cohorts, respectively. Similar to our findings, the HBC cohort had lower recurrence rate (p < 0.001). The HBC cohort also had lower retreatment rate (p = 0.004) and higher packing density (p < 0.001) compared to the BPC group. Comparable results were observed when MacDonell et al. (2022) contrasted both coiling methods in treating the anterior communicating artery.Reference MacDonell, Field and Entezami17 Moreover, when conducting a subanalysis of only ruptured aneurysms, MacDonell et al. (2022) showed significantly lower recurrence rates in the BPC cohorts, suggesting a potential advantage of HBC in the treatment of ruptured aneurysms.
Other studies focused on comparing different generations of HBC. The first-generation hydrogen-based coil included a platinum core with an outer hydrogel coating. Second generations were then developed. These included three main parts: framing, filling and finishing coil. In addition, these coils had an inner hydrogel core with an outer platinum core, allowing it for similar usage and deployment compared to BPC.Reference Abi-Aad, Rahme and Patra3,Reference Ferral13 When Abi-Aad et al. (2022) compared both generations to BPC, it was revealed that first-generation HBC offered significantly lower recurrence rates (p = 0.02) (length of follow-up 7.5–18 months).Reference Abi-Aad, Rahme and Patra3 Moreover, first-generation HBC offered a packing density of 58.5%, while BPC only offered 24.1% (p < 0.001). Initial occlusion rates trended toward first-generation HBC but were not significant (48.4% HBC vs. 42.9% BPC, p = 0.08). When evaluating second-generation HBC, the authors also revealed significantly lower recurrence rates with HBC (p = 0.007). Additionally, patients treated with second-generation HBC were 28% less likely to experience residual aneurysm neck (p = 0.02) and 58% less likely to obtain retreatment therapy (p = 0.01)
It is essential to acknowledge the rapid progress being made in the development of HBC technologies. Specifically, the ability of hydrogel-based coils to undergo phase transitions in response to physical or chemical stimuli is an area of interest. One of the most recent inventions is a photo-modifiable, shear-thinning liquid embolic that can span multiple embolic categories. This system is mainly composed of HBC material and laser. Once coiling takes place, a microcatheter-like laser probe is shined at the liquid (inside of the aneurysm), rendering it semi-solid. This phase change ensures immediate complete occlusion of the area covered by liquid. It also enables reduction in the liquid escaping the aneurysm before occlusion.
While our study offers deeper understanding of HBC compared to BPC, it is important to recognize some of its limitations. Our study included approximately 2500 patients in total with an almost even split between HBC and BPC cohorts. Although this represents the largest patient cohort among systematic reviews to date, the sample size still limits the generalizability of the findings. Another limitation of this study is the possibility of the presence of confounding variables that may have affected statistical results. For example, the size of aneurysms as well as the neck sizes are variables that differ from one study to the other. These variations may act as confounding variables on the outcomes of HBC and BPC patients in the studies. Previous literature has shown that larger aneurysms and neck have been associated with worse outcomes.Reference Fukuda, Hyohdoh and Kawada18–Reference Futami, Misaki, Uno, Kamide and Nakada20 Additionally, while HBC is considered to be revolutionary in the field of interventional treatment, first-generation hydrogen-based coils were considered stiff, had limited versatility and were difficult to deploy and reposition. Therefore, centers with limited resources and without access to second-generation HBC should interpret our findings, as well as those from previous studies, with diligence. Challenges encountered by clinicians using first-generation HBC may lead to poorer outcomes, including higher complication, recurrence and retreatment rates compared with standard BPC. A subgroup analysis comparing first-generation to second-generation hydrogel coils was to be included in this study due to its value in helping us understand our results. It may assist in understanding more clearly whether the observed advantages differ between hydrogel coil generations. However, due to the unavailability of data in the included studies comparing hydrogel coil generations to BPC, this objective was aborted.
Conclusion
Our study showed comparable results between HBC and BPC cohorts. Comparative analysis of primary and secondary outcomes revealed a significant difference in aneurysm recurrence rates and follow-up occlusion rates, both favoring HBC. Collectively, these findings indicate that current evidence may still remain insufficient to establish a clear superiority or inferiority of either coiling technique. Further research and RCTs will be useful to increasingly understand the efficacy and safety profile of HBC. Analysis of other variables, such as aneurysm size, ruptured versus unruptured aneurysms, generations of HBC and financial resources available at each site, may assist clinicians in making critical decisions that will help minimize negative outcomes in patients with intracerebral hemorrhages.
Author contributions
AM and MM – manuscript creation and data analysis.
RK, MB, AM, SKP, VY, MM, MS and GPM – manuscript revision and review.
Funding statement
The authors have received no funding for this project.
Competing interests
The authors declare no conflict of interest.
Ethical standards
N/A.
Consent to participate
N/A.
Consent for publication
N/A.



 Open access
Open access