


Breast cancer (BC) is globally the most common cancer diagnosed among women and a leading cause of mortality(Reference Wilkinson and Gathani1). BC represents 23·8 % of total female cancer cases worldwide, accounting for more than 2 million new cases and over 666 thousand deaths according to the latest figures published in the Global Cancer Observatory (2022)(2). In recent decades, a concerning and rapid rise of BC incidence and mortality has been observed, especially in low-and middle-income countries (LMIC), where lifestyle transitions driven by globalisation and urbanisation substantially contributed to this rise(Reference Xu, Gong and Wang3,Reference Porter4) . Morocco, one of these LMIC that face challenges in managing the burden of BC, which, according to the recent statistics from the Cancer Registry of Casablanca, BC is the first cancer site diagnosed among women, accounting for 38·1 % of all cancer cases with an age-standardised rate of 45,5 /100·000 women(5).
Over the years, growing evidence has highlighted the role of modifiable lifestyle factors, such as obesity, physical activity, alcohol consumption, smoking and diet in cancer prevention including BC(Reference Kelsey and Berkowitz6–Reference Lamchabbek, Elattabi and Bour9). These lifestyle factors often interact with each other, making it challenging to estimate the separate associations between individual lifestyle factors and cancer outcomes(Reference Emmons10). Subsequently, researchers shifted their focus to lifestyle indexes that incorporate those modifiable risk factors, primarily developed based on established recommendations aimed at preventing chronic diseases such as cancer(Reference Thomson, McCullough and Wertheim11,Reference McCullough, Patel and Kushi12) .
Based on the World Cancer Research Fund and the American Institute for Cancer Research (WCRF/AICR) continuous update project, the WCRF/AICR have published in 2007 eight evidence-based recommendation related to body fat, physical activity and diet to promote cancer prevention(Reference Wiseman13). In 2018, WCRF/AICR have published ten updated guidelines for cancer prevention based on the latest scientific evidence(Reference Clinton, Giovannucci and Hursting14). Since the publication of the 2007 WCRF/AICR guidelines, numerous studies have assessed the relationship between adherence to these guidelines and cancer risk, including BC, most of these studies reported an inverse association with BC risk(Reference Solans, Chan and Mitrou15). These studies have often used various scoring algorithms to assess adherence to the recommendations, what complicates the comparability of findings across different studies. To address this issue, just after the publication of the updated WCRF/AICR guidelines in 2018, a standardised scoring algorithm was developed to assess adherence to the updated recommendations and enhance comparability between studies, through a collaborative effort involving international experts including researchers from USA National Cancer Institute (NCI) and WCRF/AICR Continuous Update Project Expert Panel(Reference Shams-White, Brockton and Mitrou16).
Studies examining adherence to the updated recommendations have consistently reported an inverse association with BC risk(Reference Clinton, Giovannucci and Hursting14). However, only eleven primary studies were published so far and most were conducted in high-income countries (n 10), which differ from LMIC in terms of dietary patterns and overall lifestyle habits(Reference Korn, Reedy and Brockton17–Reference Peng, Bassett and Hodge27). These differences highlight the need to assess the adherence to these recommendations and its association with BC risk in non-Western countries to ensure their global applicability.
Morocco, as an LMIC with distinct environmental, cultural and lifestyle characteristics, is also facing a concerning increase in BC cases(5). Subsequently, Morocco provides a relevant sitting for investigating the role of modifiable lifestyle factors on BC risk. Examining these factors within this context may provide valuable insights and address critical knowledge gaps regarding adherence to these recommendations among populations with similar socioeconomic and cultural profiles.
To the best of the authors’ knowledge, no studies have so far examined the association between WCRF/AICR score and BC risk among Moroccan women. The present study is the first large case–control investigation to assess whether higher adherence to these cancer prevention guidelines is associated with a reduced risk of BC in Morocco. Additionally, the study examines which specific recommendations are driving the association with a BC risk.
Materials and methods
Study design and setting
The database was derived from the BREAST Morocco study, a multicentre case–control study conducted across various hospital centres in multiple cities in Morocco (Ibn Rochd University Hospital in Casablanca, Hassan II University Hospital in Fez, Al Hoceima Oncology Centre, Sheikh Zayed Al Nahyan Oncology Hospital in Tangier and Al Hassani Provincial Hospital in Nador) between December 2019 and August 2023. The study involves a large sample size of 2800 participants, including 1400 cases and 1400 controls, matched by age (±5 years) and place of residence (urban or rural). The sample size for this case–control study had sufficient power to detect an OR of 1·5 or greater, of 80 % and a two-sided significance level of 5 % (α = 0·05).
Study population
All included BC cases were histologically confirmed as primary in situ or invasive diagnoses before undergoing any surgical intervention or cancer treatment, such as chemotherapy or radiotherapy. These cases were recruited from the oncology centre at the study sites.
Control participants were recruited within a maximum of 2 months of their matched case. They were randomly selected from the same hospital as the cases, specifically among healthy women attending with patients at the outpatient consultation centres for conditions unrelated to cancer, and with no current or prior history of cancer.
Eligibility criteria for both cases and controls included not being pregnant or lactating at the time of the study and having the ability to provide informed consent.
Data collections and assessment
During enrolment in this multicentre case–control study, six trained interviewers filled out face-to-face questionnaires and carried out all measurements with participants. The general questionnaire included socio-demographic data, such as age, education level, marital status and employment history. Also, it collected information about family cancer history and detailed reproductive health factors, such as age at menarche, parity, age at first full-term pregnancy, breast-feeding practices and menopausal status. Additionally, this questionnaire recorded participants’ hormone use, exposure to smoking, alcohol consumption and physical activity. More information about this study and the questionnaires was detailed previously(Reference Mane, Lamchabbek and Mrah28).
Socio-economic status, anthropometric and physical activity assessment
The participants’ socio-economic position was evaluated using a validated wealth score constructed based on various household assets. Morocco was one of the nations included in the development and validation of this socio-economic assessment approach, making it particularly well-suited for studies conducted in this context(Reference Townend, Minelli and Harrabi29).
To assess various aspects of body composition and fat distribution, a set of anthropometric measurements was collected such as weight, height, seated height, hip circumference and waist circumference, each measured using standardised and validated protocols to ensure reliability and consistency(Reference Lohman, Roache and Martorell30). Height was measured using a stadiometer, with participants standing on a flat, uncarpeted surface. Weight was recorded using a calibrated digital scale placed on a flat, stable surface. Participants were weighed in light clothing and without shoes to obtain accurate body mass measurements. The BMI was calculated by dividing the weight (in kilograms) by the square of the height (in metres) (BMI = weight (kg)/height2 (m)).
Physical activity (PA) was assessed using a structured questionnaire, previously employed in a published study conducted in Morocco(Reference Khalis, Chajès and Moskal31), with detailed information that capture physical activity level over the past 12 months and during life stages. The questionnaire captured self-reported PA across different domains, including occupational, recreational and household activities. Participants were asked to estimate the average number of hours spent per week in low, moderate and vigorous-intensity activities from Monday to Sunday, based on a typical week that reflects their usual lifestyle last year. The interviewers provided examples of PA types to help participants distinguish between intensity levels. In addition, participants were asked to describe their PA level during earlier life stages of life (childhood, adolescence and early adulthood) and the types and frequency of habitual activities including walking, stairs clamping and occupational tasks.
This approach allowed for the categorisation of individuals into different physical activity levels for subsequent analysis.
Dietary intake assessment
The dietary intake of participants was assessed using a validated Food Frequency Questionnaire (FFQ). The cases groups were asked to report their dietary habits during the last year preceding their diagnosis and for the control group to report dietary habits during the year prior to the interview. This FFQ was developed based on the European Global Asthma and Allergy Network’s (GA2LEN) FFQ, which was validated and adapted to reflect Moroccan context ensuring cultural relevance and applicability(Reference El Kinany, Garcia-Larsen and Khalis32).
The FFQ used in this study comprises a comprehensive list of 255 food items, grouped into thirty-two primary food categories specific of Moroccan cuisine. These food groups capture traditional Moroccan foods accounting for the rich diversity of Moroccan culinary traditions. Participants were asked to provide detailed responses for each food item listed. Nine frequency options were available, ranging from ‘never’ to ‘six or more times per day’. Additionally, portion size for each food item consumed was specified, using traditional local household measurements such as spoons, cups, bowls and plates. To calculate daily food intake, the frequency of consumption for each food item was multiplied by the portion size. Nutrient intake data were derived using food composition tables specific to the Moroccan population(Reference Khalis, Garcia-Larsen and Charaka33).
Structure and operationalisation World Cancer Research Fund and the American Institute for Cancer Research recommendations score
To enhance the comparability of the present study results with other studies used the 2018 WCRF/AICR guidelines to assess BC risk factors, we structured our score in accordance with the standardised scoring methodology recently proposed by the NCI collaborative group, whenever possible(Reference Shams-White, Brockton and Mitrou16). Our adherence score incorporated one specialised (breast-feeding if you can) and seven general WCRF/AICR recommendations (maintaining a healthy weight, engaging in regular physical activity, consuming a diet rich in wholegrains, vegetables, fruits and legumes, limiting the intake of energy-dense processed foods, red and processed meat consumption and sugar-sweetened beverages). The recommendation ‘limit alcohol consumption’ was not operationalised in this study, as 98·4 % of the study population reported no alcohol consumption. Consequently, this component was excluded from the score calculation. Each of the included components of the WCRF/AICR recommendations was calculated based on the predefined criteria from the NCI standardised score, using data collected through lifestyle and dietary questionnaires as follows:
-
1. Maintain a healthy weight: This recommendation was operationalised using two subcomponents measured waist circumference (cm) and BMI (kg/m2), calculated from measured height and weight, scored in accordance with National Cancer Institute guidelines.
-
2. Be physically active: To reflect relative levels of physical activity within the study population and due to data limitations in precisely assessing the NCI recommended cut-offs, we used control-based tertiles to categorise participants’ levels of moderate PA (0 points for the lowest tertile, 0·5 points for the middle tertile and 1 point for the highest tertile).
-
3. Eat a diet rich in wholegrains, vegetables, fruits and legumes: this recommendation was measured by two subcomponents, the daily intake of fruits and vegetables and dietary fibre (g/d), and compliance was assigned in accordance with the NCI’s scoring algorithm.
-
4. Limit consumption of ‘fast foods’ and processed foods high in fat, refined starches or sugars: in accordance with NCI scoring algorithm, this component was assessed using the NOVA classification system(34), which classifies foods items based on their degree of processing. To ensure specificity, food items already included in other components of the score (sugar-sweetened drinks, red meats and processed meats classified as ultra-processed foods) were excluded from the original NOVA UPF variable. An adapted variable, termed adapted ultra-processed food, was created. The percentage of total daily energy intake from aUPF was calculated and categorised into tertiles based on the control group (0 point for the lowest tertile, 0·5 points for the middle tertile and 1 point for the highest tertile).
-
5. Limit consumption of red and processed meat: Compliance was evaluated by assessing the daily intake of red and processed meat using FFQ data, and scoring was conducted in accordance with NCI scoring algorithm.
-
6. Sugar-sweetened beverages: this component was assessed using a the culturally adapted FFQ. In which, participants reported their usual intake of commonly consumed sweetened drinks, and compliance was assigned in accordance with the NCI’s scoring algorithm.
-
7. For mothers: breastfeed your baby, if you can: Breast-feeding information was collected through a detailed reproductive history questionnaire. The average duration was calculated by dividing the reported total duration by the number of children breastfed. The NCI scoring algorithm was applied only to parous women.
Each participant received a score based on their adherence to these recommendations. Specifically, one point was assigned for full adherence, half a point for partial adherence and zero points for non-adherence. For the two recommendations (eat a diet rich in wholegrains, vegetables, fruits and legumes and maintaining healthy weight) composed of two subcomponents, each subcomponent was scored separately, and the points were averaged to reflect balanced weighting (0 for non adherence, 0·25 for partial adherence and 0·5 and for full adherence).
The operationalisation of these components following the NCI standardised scoring algorithm and detailed criteria for assessing compliance are described in Table 1.
Operationalisation and distribution of the 2018 WCRF/AICR cancer prevention score components among cases and controls using the NCI standardised algorithm *

WCRF, World Cancer Research Fund; AICR, American Institute for Cancer Research; PA, physical activity; MET, metabolic equivalents; aUPF: adapted ultra-processed food.
P value; χ 2 test for qualitative variables.
* The score is based on NCI Standardised Algorithm.
† Adherence to the recommendation ‘Be a healthy weight’ is measured by two subgroups, BMI and waist circumference; adherence to the recommendation ‘Eat a diet rich in wholegrains, vegetables, fruit and beans’ is measured by two subgroups, fruit and vegetable intake and daily fibre intake.
‡ Recommendation only applied to parous women.
Statistical analysis
Data handling and cleaning
To address missing data, single imputation was performed using the median for continuous variables and the mode for categorical variables, as all variables had less than 5 % missing values, ensuring consistency in the data analysis. To address bias in self-reported dietary data, we compared participants’ energy intake to their estimated energy requirements, calculated using Schofield equation that accounts for age, gender, weight, height and activity level. Participants in bottom 1 % energy intake/estimated energy requirement ratio were identified as under-reporters and excluded from the study. As a result, fifty-four participants were removed, and the final sample includes 2746 participants(Reference Banna, McCrory and Fialkowski35–Reference Goldberg, Black and Jebb37).
The general characteristics of the population are presented using mean values for continuous variables and percentages for categorical variables. Logistic regression models were used to estimate OR of BC and the 95 % CI for each individual recommendation and for the overall WCRF/AICR score. Stratification by menopausal status (premenopausal v. postmenopausal) was used for both overall and for each individual recommendation. In the multivariate analyses, we adjusted for age at menarche (years), average daily caloric intake (kcal/day), physical activity (MET min/week), wealth score, educational level (illiterate, elementary /Koranic school, secondary school and high school/technical or professional school), occupation (housewife, employed and previous employed), history of oral contraceptive use (Yes, No), age at first full-term pregnancy (nulliparous, < 22 years and > 22 years), breast-feeding (never breastfeed, > 0–< 24 months, ≥ 24 month and nulliparous), age at menopause (premenopausal, < 50 years, > 50 years), family history of BC (Yes, No) and BMI (< 25 kg/m2, 25–29 kg/m2 and ≥ 30 kg/m2) (unless the variable was part of the recommendation evaluated). Additionally, in the stratified analysis by menopausal status, additional adjustments for the original matching variables, age and region were included, while no adjustment was made for age at menopause.
Tertiles of adapted ultra-processed food, physical activity and WCRF/AICR score were derived from the distribution among controls. All statistical analyses were performed with SPSS version 21.0 and were conducted separately for premenopausal and postmenopausal women.
Results
The general characteristics of the cases and controls in the study population are presented in Table 2. Compared to controls, women with BC were more likely to report a younger age at menarche, an older age at first full-term pregnancy and an older age at menopause. Use of oral contraceptives was also more frequent among cases. Furthermore, among parous women, breast-feeding practices differed markedly, with a significantly higher proportion of controls reporting breast-feeding for 24 months or more. A family history of cancer and BC was also more prevalent among cases.
General characteristics of the study population by case and control groups (n 2746)

Continuous variables are presented as means (sd) and categorical variables are presented as frequencies (%).
WC, waist circumference, WC, waist circumference, HC, hip circumference.
* P value; χ 2 test for categorical variables ant student t test for continuous variables.
† Among parous women.
‡ Among postmenopausal women.
Furthermore, cases had a lower wealth score, were less likely to have attained a higher educational level or be physically active and exhibited significantly higher mean values for all anthropometric indicators, including BMI, WC and HC.
Regarding dietary intake, total energy intake was slightly lower in cases than in controls. Compared with controls, cases consumed significantly fewer vegetables, fruits, unsaturated oils, nuts and seeds, whole grains and dietary fibre. Socio-demographic characteristics were broadly comparable between groups concerning education level differed, with a higher proportion of illiterate women among cases compared with controls. Likewise, occupational status differed.
Table 3 shows the OR (CI) for BC in relation to the WCRF/AICR score, both overall and stratified by menopausal status. Compared with the lowest adherence category, a significant trend of decreasing BC risk with increasing adherence was observed in the crude model, overall (OR = 0·20 (0·14, 0·26), P < 0·001) in premenopausal women (OR = 0·20 (0·14, 0·26), P < 0·001) and in postmenopausal women (OR = 0·11 (0·10, 0·16), P < 0·001). After adjusting for confounding factors, this inverse trend remained significant, overall (OR = 0·14 (0·11, 0·18), P < 0·001) as well as in premenopausal women (OR = 0·13 (0·09, 0·19), P < 0·001) and in postmenopausal women (OR = 0·12 (0·08, 0·17), P < 0·001). Furthermore, each one-point increase in adherence to the WCRF/AICR score was inversely associated with BC risk overall (OR = 0·33; 95 % CI: 0·29, 0·37, P < 0·001), as well as among both premenopausal women (OR = 0·29; 95 % CI: 0·24, 0·35, P < 0·001) and postmenopausal women (OR = 0·35; 95 % CI: 0·30, 0·41, P < 0·001).
Associations between the adherence to the overall 2018 WCRF/AICR cancer prevention recommendations using the NCI standardised scoring algorithm and breast cancer risk

Unadjusted model: Crude OR.
* Adjusted model: OR adjusted for age at menarche (years), average daily caloric intake (kcal/day), wealth score (continuous), educational level (illiterate, elementary /Koranic school, secondary school, high school /technical or professional school), occupation (housewife, employed, previous employed), history of oral contraceptive use (Yes, No), age at first full-term pregnancy (nulliparous, < 22 years,> 22 years), age at menopause (premenopausal, < 50 years, > 50 years), family history of breast cancer (Yes, No).
† Additional adjustments were made for the original matching variables (age and region), with no adjustment for age at menopause in analyses stratified by menopausal status.
‡ Tertile cut-off points were defined according to the distribution of the WCRF score among controls.
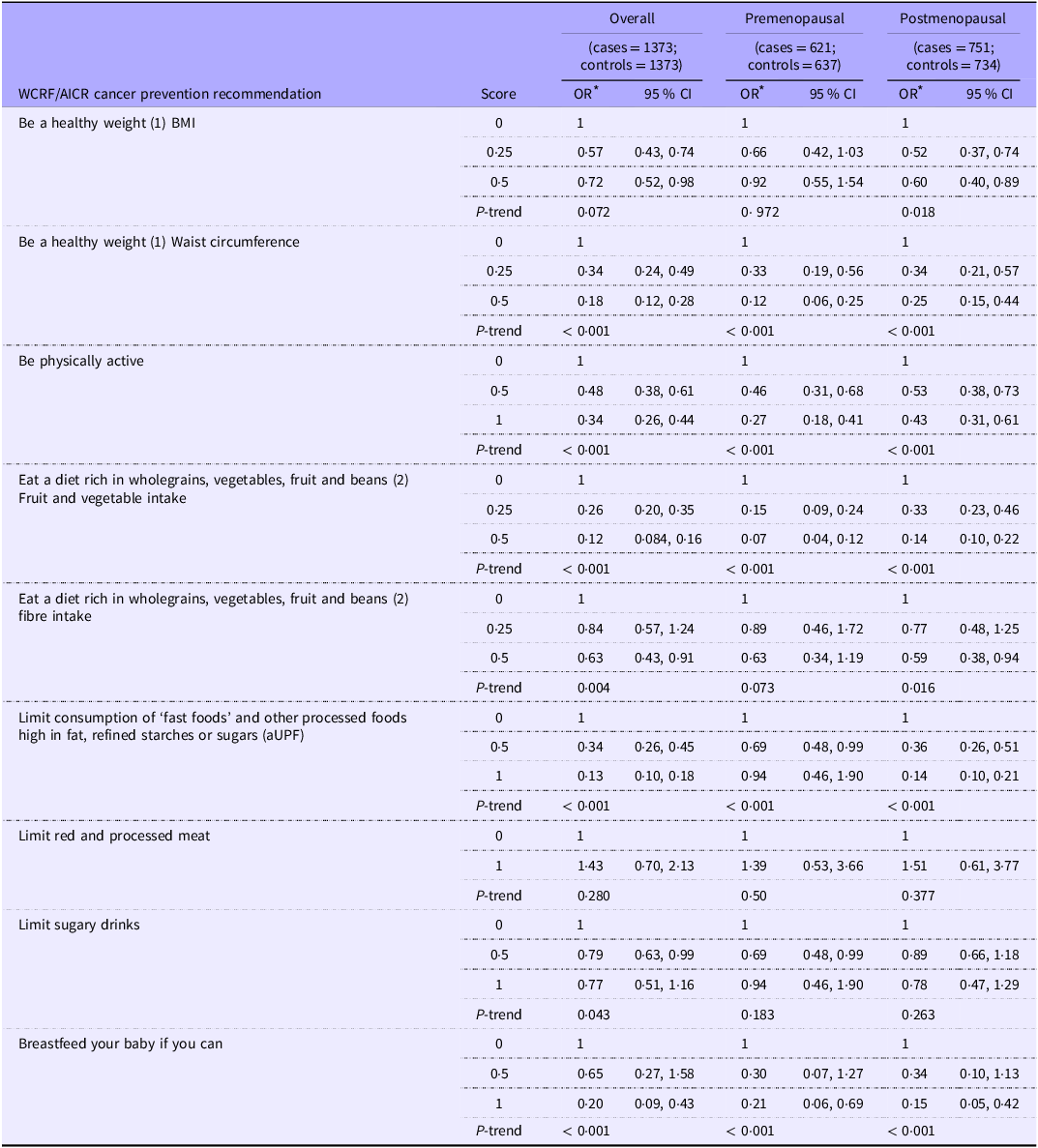
Table 4 presents the results of the association between BC risk and adherence to specific recommendations from the 2018 WCRF/AICR cancer prevention guidelines, adjusted for potential confounders. Adherence to the WCRF/AICR recommendation on maintaining a healthy weight, assessed by BMI and waist circumference, was associated with a significantly reduced BC risk. Specifically, waist circumference showed a strong inverse relationship with overall (OR = 0·18 (0·12, 0·28), P < 0·001) and both premenopausal (OR = 0·12 (0·06, 0·25), P < 0·001) and postmenopausal women (OR = 0·25 (0·15, 0·44), P < 0·001). For BMI, a significant inverse trend was observed only among postmenopausal women (OR = 0·60 (0·40, 0·89), P = 0·018), whereas no significant association was observed in both overall and premenopausal women.
Associations between the adherence to individual recommendations of the 2018 WCRF/AICR cancer prevention recommendation, using the NCI standardised score and breast cancer risk

WCRF/AICR, World Cancer Research Fund and the American Institute for Cancer Research; aUPF, adapted ultra-processed food according to NOVA classification.
All values are OR (95 % CI), and 0 indicates the lowest adherence to the specific recommendation.
* Adjusted for age at menarche (years), average daily caloric intake (kcal/day), physical activity (MET min/week), wealth score, educational level (illiterate, elementary /Koranic school, secondary school, high school /Technical or professional school),occupation(housewife, employed and previous Employed), history of oral contraceptive use (Yes, No), age at first full-term pregnancy (nulliparous, < 22 years,> 22 years), breastfeed infants (never breastfeed, > 0–< 24 months, ≥ 24 month, missing), age at menopause (Premenopausal, < 50 years, > 50 years), family history of breast cancer (yes, no) and BMI (< 25 kg/m2, 25–29 kg/m2, ≥ 30 kg/m2). Unless the variable was part of the recommendation evaluated, additional adjustments were made for the original matching variables (age and region), with no adjustment for age at menopause in stratified analyses by menopausal status.
(1) Adherence to the recommendation ‘Be a healthy weight’ is measured by two subgroups, BMI and waist circumference.
(2) Adherence to the recommendation ‘Eat a diet rich in wholegrains, vegetables, fruit and beans’ is measured by two subgroups, fruit and vegetable intake and daily fibre intake.
For dietary habit-related recommendations, significant trends of reduced BC risk were observed with increased fruit and vegetable intake, both in the overall group (OR = 0·12 (0·084, 0·16), P < 0·001), as well as in premenopausal women (OR = 0·07 (0·04, 0·12), P < 0·001) and postmenopausal women (OR = 0·14 (0·10, 0·22), P < 0·001). Similarly, increased fibre intake was associated with reduced risk overall (OR = 0·63 (0·43, 0·91), P < 0·001) and in postmenopausal women (OR = 0·60 (0·38, 0·96), P = 0·016). Limiting adapted ultra-processed food also showed significant trends of reduced risk both overall (OR = 0·13 (0·10, 0·18), P < 0·001) in postmenopausal women (OR = 0·14 (0·10, 0·21), P < 0·001). However, no significant trend in risk emerged for adherence to recommendations on meat and processed meat consumption or sugary drinks.
Adherence to physical activity recommendations was also associated with reduced BC risk, with significant trends, overall (OR = 0·34 (0·26, 0·44), P < 0·001), in premenopausal women (OR = 0·27 (0·18, 0·41), P < 0·001) and postmenopausal women (OR = 0·43 (0·31, 0·61), P < 0·001). Similarly, adherence to breast-feeding recommendation was associated with a significant reduction in BC risk overall (OR = 0·20 (0·09, 0·43), P < 0·001), as well as in premenopausal women (OR = 0·21 (0·06 0·69), P < 0·001) and postmenopausal women (OR = 0·15 (0·05, 0·42), < 0·001).
Discussion
This large-scale case–control study, the first in Morocco and among the pioneering investigations in LMIC to examine the relationship between adherence to the 2018 WCRF/AICR Guidelines and BC risk, suggests a strong inverse association between higher adherence to these guidelines and BC risk, both in the overall population and among premenopausal and postmenopausal women.
A particularly noteworthy aspect of our findings is the strength of the association between adherence to the WCRF/AICR recommendations and BC risk. The 67 % risk reduction observed for each one-point increment in our study is substantially greater than the more modest 10–11 % risk reduction reported in meta-analyses of studies from predominantly HIC(Reference Solans, Chan and Mitrou15,Reference Malcomson, Wiggins and Parra-Soto38) . This discrepancy needs careful consideration and highlights the importance of interpreting our results within the distinct context of our study population.
The existing body of evidence on the 2018 recommendations is still developing, with only a limited studies available. To date, only eleven primary studies have examined adherence to the updated 2018 recommendations in relation to BC risk, and the vast majority of these were cohort studies conducted in HIC(Reference Korn, Reedy and Brockton17–Reference Peng, Bassett and Hodge27). These populations differ markedly from LMIC like Morocco in their dietary patterns, lifestyle behaviours, socio-economic contexts and stages of nutritional transition(Reference Kang, Kang and Lim39,Reference Popkin and Ng40) . Therefore, direct comparisons should be interpreted with caution, as baseline risk profiles and environmental exposures may vary substantially between settings.
Additionally, several factors may help contextualise the strong association observed in our study. As a first consideration, we must acknowledge the potential for selection bias, a common limitation of case–control studies(41). The selection of controls in our study was hospital based, which may have resulted in a comparison group that is more health conscious than the general population, which may have potentially led to an overestimation of the true magnitude of the association and partly explaining the stronger association observed. Indeed, previous meta-analytic evidence has suggested that case–control designs tend to report stronger associations than prospective cohort studies in this area of research(Reference Clinton, Giovannucci and Hursting14).
Beyond selection bias, the distinct epidemiological and nutritional context of Morocco, a nation undergoing a rapid nutrition transition, likely plays a significant role. Unlike in many HIC where dietary patterns have become more homogeneous(42). Morocco is characterised by the coexistence of traditional plant-based dietary patterns and modern, Westernised eating habits(Reference Allali43,Reference Lamchabbek, Mane and Mrah44) . This variability may contribute to a more marked contrast across exposure groups, potentially allowing for a stronger detection of the benefits of a healthy lifestyle.
Our analysis of the individual components of the 2018 WCRF/AICR score revealed that the reduced risk of BC associated with high overall adherence was primarily driven by strong adherence to several key guidelines. Specifically, maintaining a healthy weight, being physically active, breast-feeding, consuming a diet rich in whole grains, vegetables and fruits and limiting the intake of processed foods high in fat, starches or sugars. Each of these recommendations was independently associated with a lower risk of BC in our study, a finding that was evident in both pre- and postmenopausal women. This aligns with the body of evidence demonstrating that healthy dietary and lifestyle patterns are protective against BC(Reference Xiao, Xia and Li45).
The biological plausibility for this is well-established; diets abundant in plant-derived nutrients are rich sources of antioxidants, bioactive anti-inflammatory compounds and phytochemicals, which may mitigate cellular damage and inhibit disease progression(Reference Turati, Rossi and Pelucchi46–Reference Steinmetz and Potter48). Conversely, unhealthy dietary patterns, often energy-dense and nutrient-poor, are known to promote chronic inflammation, oxidative stress and hormonal imbalances, all of which are established risk factors for carcinogenesis(Reference Xiao, Xia and Li45). Alongside diet, other lifestyle factors integral to the WCRF/AICR recommendations also play a crucial role. The global shift towards sedentary behaviours, a consequence of urbanisation and changing occupational patterns, has contributed to rising obesity rates and low physical activity levels in Morocco(Reference Najdi, El Achhab and Nejjari49). These lifestyle changes have significantly contributed to the emergence of NCD, including BC(Reference Chadli, Taqarort and El Houate50). Regular physical activity is associated with cancer prevention through multiple biological mechanisms, including reducing insulin resistance, modulating inflammation and regulating hormone metabolism, all of which play a key role in carcinogenesis(Reference Rogers, Colbert and Greiner51). Likewise, maintaining a healthy weight is a well-established protective factor against BC, as excess body fat contributes to chronic inflammation and increased estrogen production(Reference Khanna, Khanna and Khanna52,Reference Ellulu, Patimah and Khaza’ai53) . Our findings also confirmed the protective role of breast-feeding, which likely reduces BC risk by limiting a woman’s cumulative lifetime exposure to sex hormones, such as oestrogen, through the induction of amenorrhoea and the differentiation of breast tissue(54,Reference Obeagu and Obeagu55) .
This study has several notable strengths. It is the first of its kind in Morocco and one of the few in an LMIC setting to investigate the association between adherence to the updated WCRF/AICR guidelines and BC risk. Furthermore, the large sample size and the use of a validated FFQ, which was adapted for the local context, allowed for a robust assessment of dietary intake. However, the findings should be interpreted in consideration of some limitations. Due to its observational nature, this case–control study may be susceptible to recall bias. To minimise this limitation, trained interviewers assisted participants during the interviews to ensure accurate and reliable responses to the questionnaire. Additionally, cases were recruited at the time of diagnosis and before the initiation of treatment to minimise potential recall bias and ensure that data on pre-diagnostic exposures were collected before any treatment-related stress or lifestyle changes could influence participants’ responses.
Furthermore, the choice of hospital-based controls, as previously discussed, may have introduced selection bias. While we attempted to minimise this by matching for age and place of residence, and by recruiting controls from among visitors of patients with non-related cancer disease, the potential for bias cannot be fully excluded. Also, it should be noted that the FFQ was not originally designed to assess the level of food processing of the different food groups, requiring assumptions to be made when classifying the food groups according to the Nova classification. Although residual confounding cannot be entirely ruled out, as risk factors are often interrelated, efforts were made to minimise this limitation by applying a comprehensive statistical adjustment to account for potential confounders that could influence both exposure and outcomes.
Conclusion
In summary, the findings of this large-scale case–control study suggest that adherence to the 2018 WCRF/AICR guidelines is associated with a reduced risk of BC in Morocco, reinforcing the importance of comprehensive lifestyle modifications in BC prevention. Specifically, maintaining a healthy weight, engaging in regular physical activity, adopting a diet rich in plant-based foods while limiting processed foods and encouraging breast-feeding appear to be the key drivers of the observed inverse associations with BC. Future research should further explore the interaction between lifestyle factors and genetic predispositions to refine tailored prevention strategies for the Moroccan population.
Acknowledgements
We express our sincere gratitude to the leadership and staff of the participating hospital centers: the Ibn Rochd University Hospital in Casablanca, the Hassan II University Hospital in Fez, the Al Hoceima Oncology Centre, the Sheikh Zayed Al Nahyan Oncology Hospital in Tangier and the Al Hassani Provincial Hospital in Nador. Specifically, we extend our appreciation to the hospital directors, the heads of the medical departments and their dedicated personnel, whose support was instrumental in the data collection process. Most profoundly, the authors acknowledge the contribution of the women who volunteered their time and participation; this study would not have been feasible without their engagement.
This work was conducted under the auspices of the PHC Toubkal project (Reference No. 47363VA), which provided financial support for the mobility and collaborative activities between research teams in Morocco and France.
We used Open AI tools to assist with English language editing, in accordance with journal guidelines
IARC disclaimer: Where authors are identified as personnel of the International Agency for Research on Cancer/WHO, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/WHO.
This research received no external funding.
N. L., M. K. and I. H. conceived the study, designed the research and contributed to data interpretation. N. L., N. M., S. M. and C. E. were involved in data acquisition. N. L. led the statistical analyses and drafted the initial manuscript. All authors contributed to the critical review and revision of successive versions of the manuscript, and all have read and approved the final version.
The authors declare no conflicts of interest.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Ethics Committee at the Faculty of Medicine and Pharmacy of Casablanca (No. 09/16). Written informed consent was obtained from all subjects/patients.




 Open access
Open access