Globally, psoriasis is a common, chronic papulosquamous skin disease and occurs at any age(Reference Griffiths, Armstrong and Gudjonsson1). More than 3 % of US adults are affected by psoriasis, and the prevalence has been increasing continuously(Reference Ruan, Lu and Chen2). Psoriasis exhibits typical skin lesions with epidermal hyperplasia and parakeratosis, along with mixed inflammatory infiltrates (lymphocytes and neutrophils), demonstrating that its clinical presentation reflects underlying inflammatory processes(Reference Knabel and Mudaliar3). Recently, psoriasis has been considered a systemic disease involving multiple organ systems and has been demonstrated to be causally related to CVD by previous Mendelian randomisation analysis(Reference Gao, Kong and Li4). Risk factors and pathogenic mechanisms such as smoking, obesity, dyslipidaemia and elevated levels of pro-inflammatory cytokines may occur simultaneously in psoriasis and CVD(Reference Hu and Lan5).
Fatty acids, fundamental nutrients for human health with specific metabolic and signalling functions, are typically composed of various long-chain fatty acids, which include SFA and unsaturated fatty acids(Reference Honda and Kabashima6). Unsaturated fatty acids are classified into several groups, such as n-3 PUFA and n-6 PUFA, depending on their chemical structure. Epidemiological studies suggested that PUFA may show potential as a safe, adjunctive treatment for a variety of skin diseases including psoriasis(Reference Guida, Napoleone and Trio7–Reference Qin, Wen and Bai10). Among PUFA, n-3 fatty acids (i.e. EPA and DHA supplementation, in a dose-dependent manner, result in inhibition of various pro-inflammatory mediators, and metabolisation of EPA a DHA leads to dampening of inflammation and finally inhibits the abnormal scaling of the skin(Reference Clark, Taghizadeh and Nahavandi11). Moreover, in psoriasis patients with obese, n-3 intake is beneficial to improve blood lipid levels and body weight loss(Reference Guida, Napoleone and Trio7). Diets are vital modifiable targets for atherosclerotic CVD (ASCVD) prevention and management, and the mechanism has been related to potential pro- or anti-inflammatory properties of the dietary pattern or dietary components(Reference Phillips, Chen and Heude12). Previous studies reported the beneficial relationship between dietary PUFA intake and cardiovascular health(Reference Elagizi, Lavie and O’Keefe13–Reference Jiang, Wang and Wang15). Less is known, however, about the effect of dietary PUFA intake on the association between ASCVD risk related to psoriasis.
Herein, we explored the effect of PUFA and its subtypes on the association between ASCVD risk and psoriasis by analysing the National Health and Nutrition Examination Survey (NHANES) database 2003–2006 and 2009–2014. Focusing on dietary modification, this study sought to develop health management approaches to support cardiovascular health in psoriatic patients
Methods
Study design and study subjects
Data for this cross-sectional study were screened from the NHANES database 2003–2006 and 2009–2014. The NHANES database is a representative cross-sectional survey of the all-institutionalised civilian population in the USA. It is a major project of the National Center for Health Statistics, a part of the Centers for Disease Control and Prevention, and is responsible for compiling life and health statistics. Subjects completed surveys about demographics, health history and diet, and they submitted blood and urine samples during physical examinations. The requirement of ethical approval for this was waived by the Institutional Review Board of the Yancheng Clinical College of Xuzhou Medical University and the First People’s Hospital of Yancheng, because the data were accessed from NHANES (a publicly available database). The need for written informed consent was waived by the Institutional Review Board of the Yancheng Clinical College of Xuzhou Medical University and the First People’s Hospital of Yancheng due to the retrospective nature of the study. This study was conducted according to the guidelines laid down in the Declaration of Helsinki.
The inclusion criteria were (1) subjects aged ≥ 40 years, (2) subjects with psoriasis history, (3) subjects with fatty acid intakes and (4) subjects with complete information for calculating 10-year ASCVD risk. The exclusion criteria were (1) subjects with CVD history and (2) subjects missing BMI calculating information.
Calculation of 10-year atherosclerotic CVD risk
The American College of Cardiology/American Heart Association pooled cohort 10-year risk of ASCVD score (%) was calculated based on age, gender, race, systolic blood pressure, diastolic blood pressure, total cholesterol, HDL-cholesterol, hypertension treatment, diabetes and smoking status(Reference Grundy, Stone and Bailey16). In the present study, subjects who scored ≥ 7·5 % were classified as having an elevated 10-year ASCVD risk, whereas those who scored < 7·5 % were identified as low-risk individuals.
Assessment of psoriasis
Psoriasis was defined by the question ‘Have you ever been told by a healthcare provider that you had psoriasis?’ or ‘Have you ever been told by a doctor or other healthcare professional that you had psoriasis?’ Subjects who answered ‘yes’ to any of the above questions were defined as having psoriasis.
Assessment of dietary PUFA and its subtypes intake
Dietary information was obtained from a 1-d 24-h dietary recall interview in NHANES(Reference Jiang, Yang and Li17). The 24-h dietary recall interview was conducted in person in the mobile exam centres by experienced interviewers. There were seven specific fatty acids in PUFA including n-3 EPA, DHA, DPA, α-linolenic acid (ALA) and stearidonic acid (SDA) and n-6 (linoleic acid and arachidonic acid). The daily dietary PUFA intake was calculated using the Dietary Research Food and Nutrition Database for Dietary Studies from the US Department of Agriculture(Reference Ahluwalia, Dwyer and Terry18). The PUFA intake and its subtypes were categorised into two levels based on the median level of intake. Since a large number of subjects had 0 intake of SDA, the SDA intake was divided into two groups of 0 g and > 0 g.
Potential covariates
This study included potential covariates to elucidate their possible effects on PUFA intake and the risk of psoriasis and 10-year ASCVD. The selected covariates were based on known risk factors for 10-year ASCVD identified in prior research(Reference Grundy, Stone and Bailey16). These covariates included age (< 60 and ≥ 60 years old), gender (female and male), race (non-Hispanic White, non-Hispanic Black, other race), education level (below high school, high school, college and above), marital status (married, never married, others), poverty-to-income ratio (PIR) (low income (≤ 1·3), middle income (1·3–3·5) and high income (> 3·5)), drinking status (yes/no), physical activity (< 750 met × min/week, ≥ 750 met × min/week, unknown), chronic kidney disease (CKD) (yes/no), autoimmune disease (yes/no), family history of myocardial infraction (yes/no), BMI (< 25 kg/m2/ ≥ 25 kg/m2), drug for dyslipidaemia (yes/no) and drug for psoriasis (yes/no), alanine transaminase (ALT) (U/L), aspartate aminotransferase (AST) (U/L), Hb (g/dl) and uric acid (mg/dl), total energy intake (kcal), SFA (g) and MUFA (g).
Physical activity was expressed as the metabolic equivalent task (MET) and calculated as follows: physical activity (met·min/week) = recommended MET × exercise time for corresponding activities (min/day) × the number of exercise days per week (day)(Reference Mendes, da Silva and Ramires19). CKD was defined as urine albumin-to-creatinine ratio > 30 mg/g or estimated glomerular filtration rate < 60 ml/min 1·73 m2(Reference Zhang, Chen and Zou20). The estimated glomerular filtration rate was calculated by the Chronic Kidney Disease-Epidemiology Collaboration equation (CKD-EPI), combined with parameters of serum creatinine, gender, age and race. The CKD-EPI equation is expressed by the following equation: 141 × min (Scr/κ, 1) α × max (Scr/κ, 1)−1·029 × 0·993 age × 1·108 (if female) × 1·159 (if black), κ is 0·7 for females and 0·9 for males, α is −0·329 for females and −0·411 for males, min indicates the minimum of Scr/κ or 1 and max indicates the maximum of Scr/κ or 1(Reference Inker and Titan21).
Statistics analysis
All statistical analyses were performed by SAS software (version 9·4, SAS Institute). Using the proc surveyfreq in SAS software, the final sample size was weighted with SDMVPSU, SDMVSTRA and WTDRD1. SDMVPSU means the masked variance unit pseudo-substrate is sdmvstra, and the masked variance unit pseudo-primary sampling unit is sdmvpsu. SDMVSTRA was the CI applied for evaluating the reliability of an estimate. WTDRD1 refers to the dietary day one 2-year sample weight.
Quantitative data were expressed as mean and se, and the weighted t test was used for comparison between the two groups. Categorical variables were described as the number and percentage (n (%)), and a weighted χ 2 test was used to analyse the differences of the categorical variables. Sensitivity analyses were performed to compare whether the results were different before and after imputation (online Supplementary Table S1). The baseline demographic information, disease history, laboratory parameters, physical examination and dietary intake information were included in a weighted univariate logistic regression model to screen for covariates associated with 10-year ASCVD risk (P < 0·05) (online Supplementary Table S2). Then, we controlled for these covariates in weighted multivariate logistic regression models to further explore the association between dietary PUFA intake, psoriasis and 10-year ASCVD risk with OR and 95 % CI. Model 1 was a crude model without adjusting covariates; model 2 adjusted common demographic information including age, gender, race, education level, marital status and PIR; in addition to these above covariates, model 3 further adjusted physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy intake, SFA, MUFA, ALT, AST, Hb and uric acid. We also conducted the multicollinearity test between independent variables based on each regulating factor with the evaluation index of the variance inflation factor (online Supplementary Table S3). The variance inflation factor is a common measure used to detect multicollinearity in regression analysis. It measures the degree to which the correlation between independent variables affects the variance of the regression coefficient estimate. Two-sided P < 0·05 was considered statistically significant.
Results
Characteristics of study population
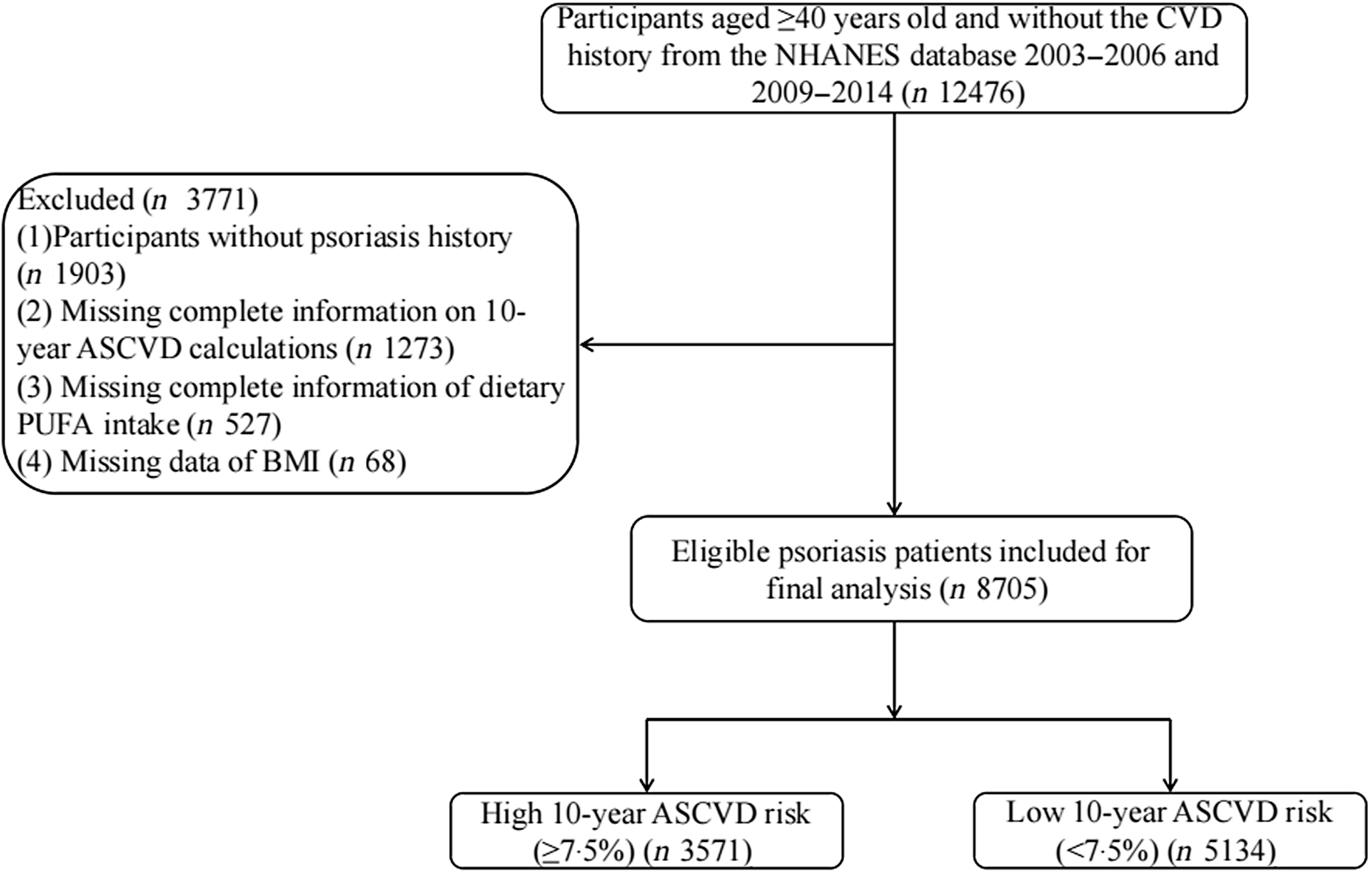
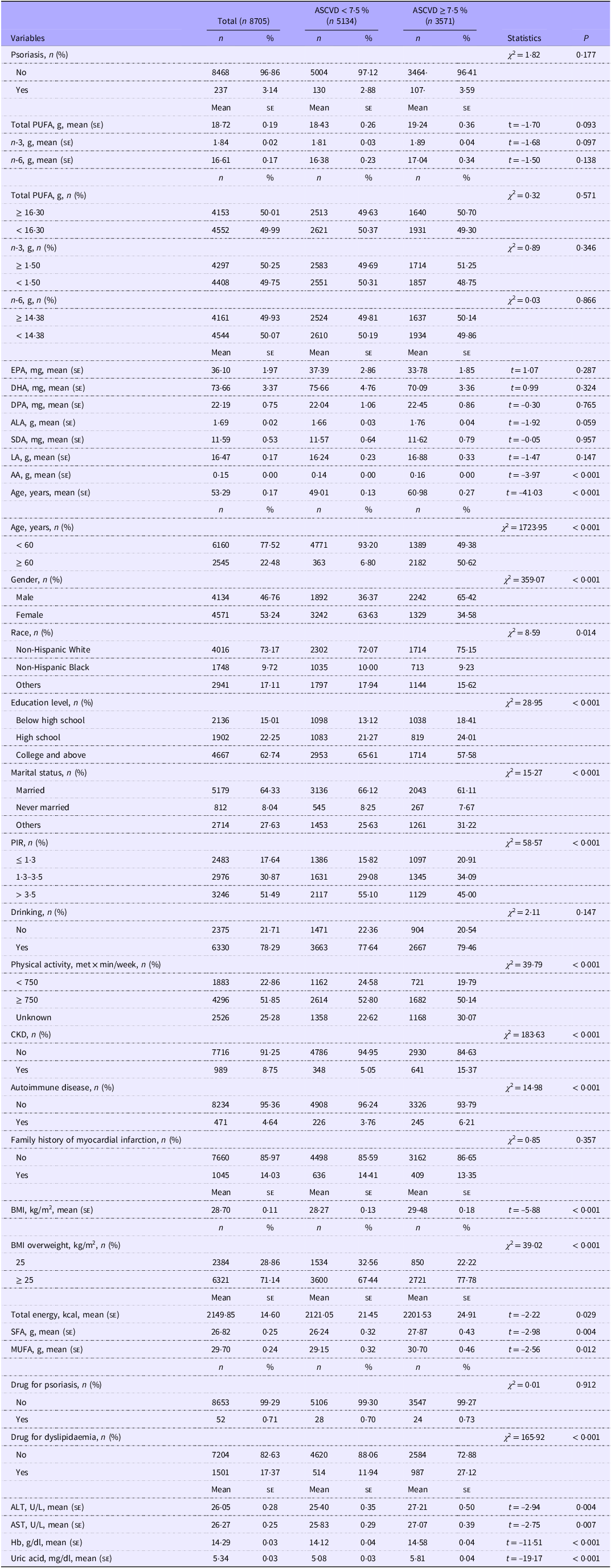
The flow chart of population screening is shown in Figure 1. Totally, 12 476 subjects aged ≥ 40 years old and without a CVD history were screened from the NHANES database. Among them, 1903 subjects without the psoriasis diagnosis assessment, 1273 subjects without the complete information on calculating of 10-year ASCVD risk, 527 subjects missing the complete fatty acids intake information and 68 subjects missing the BMI data were excluded. Finally, 8705 subjects were included, with a mean age of 53·29 (0·17) years old. Of whom, 3·571 (41·02 %) had high 10-year ASCVD risk (≥ 7·5 %). Characteristics of included participants are shown in Table 1. Differences were found in age, gender, race, level of education, PIR, physical activity and BMI, marital status, history of CKD and autoimmune disease, intake of total energy, SFA and PUFA between the two groups (all P < 0·05).
The flow chart of population screening. NHANES, National Health and Nutrition Examination Survey; ASCVD, atherosclerotic CVD.

Characteristics of subjects (Numbers and percentages; mean values and standard deviations)

ASCVD, atherosclerotic CVD; DPA, docosapentaenoic; ALA. octadecatrienoic; SDA, stearidonic acid; LA, linoleic acid; AA, arachidonic acid; PIR, poverty-to-income ratio; met, metabolic equivalent; CKD, chronic kidney disease; ALT, alanine transaminase; AST, aspartate aminotransferase.
t, t test.
Association of psoriasis, PUFA and 10-year atherosclerotic CVD risk
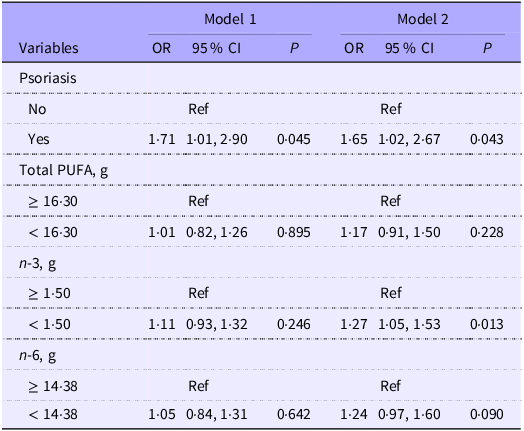
We employed two weighted logistic regression models to evaluate the association between psoriasis, total PUFA intake, n-3 intake, n-6 intake and 10-year ASCVD risk, as presented in Table 2. In fully adjusted model 2, we observed the risk of 10-year ASCVD in subjects with psoriasis increased by 65 % compared with subjects without psoriasis (OR 1·65; 95 % CI 1·02, 2·67). Compared with higher n-3 intake (≥ 16·30 g), lower n-3 intake (< 1·50 g) was associated with higher 10-year ASCVD risk (OR 1·27; 95 % CI 1·05, 1·53). No significant associations were found between intake of total PUFA intake and n-6 intake and 10-year ASCVD risk (all P > 0·05).
Association between PUFA, psoriasis and 10-year ASCVD risk (Odds ratios and 95 % confidence intervals)

Ref, reference; ASCVD, atherosclerotic CVD.
Model 1, adjusted age, gender, race, education level, marital status and PIR.
Model 2, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
Moderating effect of PUFA on the association between psoriasis and 10-year atherosclerotic CVD risk
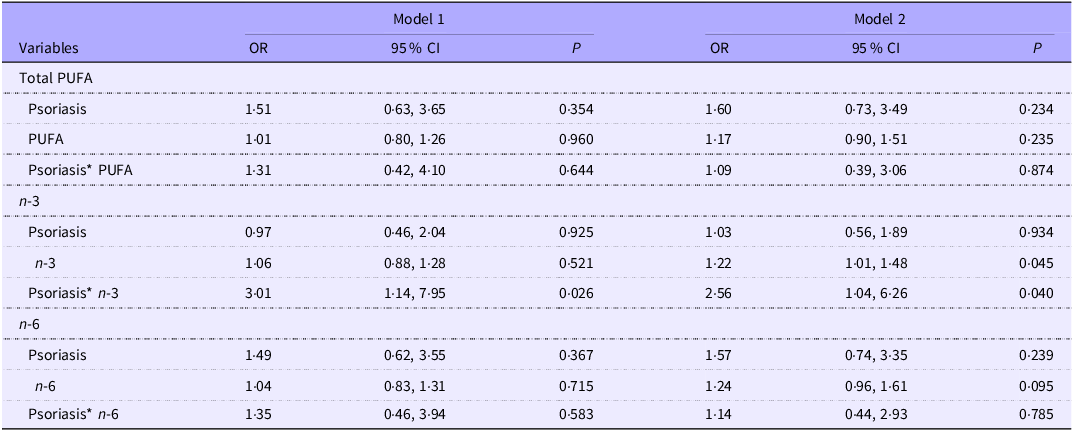
Two logistic regression models were conducted to explore whether PUFA have a moderating effect on the association between psoriasis and 10-year ASCVD risk, as shown in Table 3. After adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid, we observed subjects with psoriasis and n-3 intake were related to higher 10-year ASCVD risk (OR 2·56; 95 % CI 1·04, 6·26). No significant associations were found between total PUFA, n-6 and 10-year ASCVD risk among psoriasis patients (all P > 0·05).
Moderating effect of PUFA and its subgroup on the association between psoriasis and 10-year ASCVD risk (Odds ratios and 95 % confidence intervals)

Ref, reference; ASCVD, atherosclerotic CVD; *: moderating term.
Model 1, adjusted age, gender, race, education level, marital status and PIR.
Model 2, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
Association between psoriasis and 10-year atherosclerotic CVD risk in different n-3 intake levels
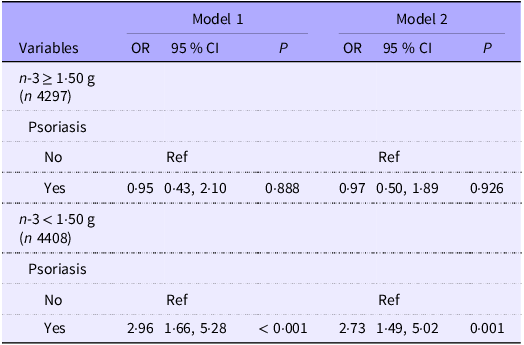
By validating the moderating effect of PUFA on psoriasis and 10-year ASCVD risk, we observed that n-3, the PUFA subtype, had a more significant moderating effect on psoriasis and 10-year ASCVD risk. The association between different levels of n-3 intake, psoriasis and 10-year ASCVD risk was further explored, as presented in Table 4. In fully adjusted model 2, we observed that subjects with lower n-3 intake (< 1·50 g) and psoriasis were related to higher 10-year ASCVD risk (OR 2·73; 95 % CI 1·49, 5·02).
Association between different levels of n-3 intake, psoriasis and 10-year ASCVD risk (Odds ratios and 95 % confidence intervals)

Ref, reference; ASCVD, atherosclerotic CVD.
Model 1, adjusted age, gender, race, education level, marital status and PIR.
Model 2, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
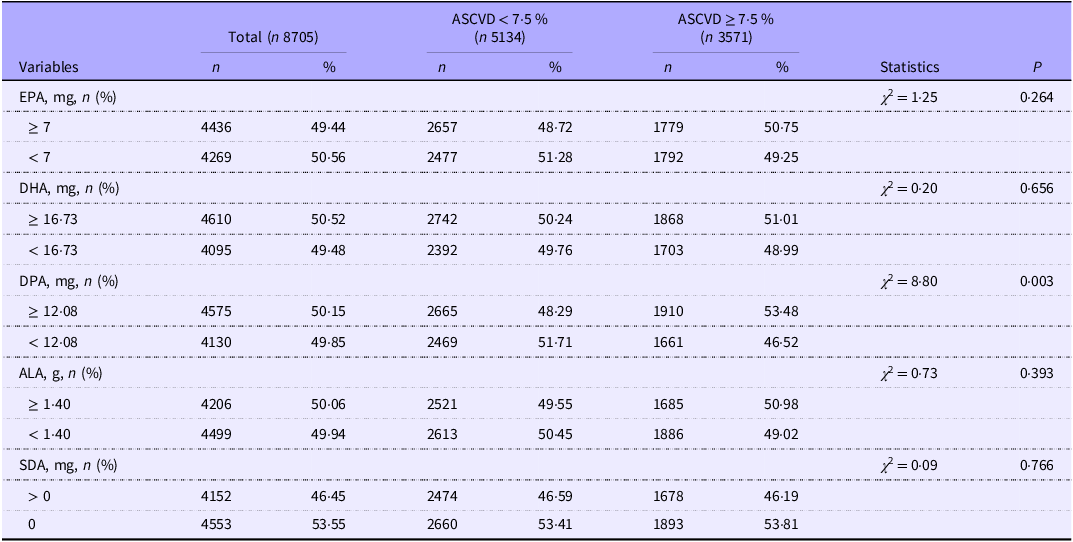
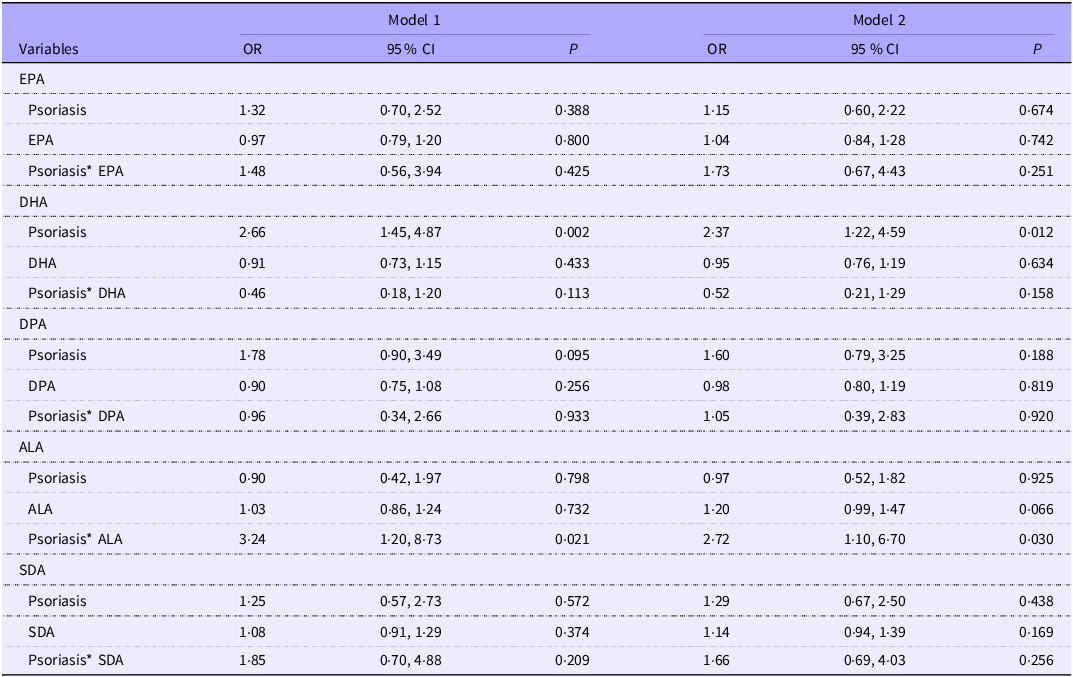
In addition, to explore the moderating effects of single n-3 components on the association of psoriasis and 10-year ASCVD risk, we performed two logistic regression analyses for each n-3 component. Table 5 represents each n-3 component intake in subjects with higher (≥ 7·5 %) and lower (< 7·5 %) 10-year ASCVD risk. Then, we explored the moderating effect of each single component of n-3 on the association between psoriasis and 10-year ASCVD risk, as shown in Table 6. After adjusting all covariates, we observed a significant moderating effect of ALA intake between psoriasis and 10-year ASCVD risk (OR 2·72; 95 % CI 1·10, 6·70).
Each n-3 intake in subjects with high or low 10-year ASCVD risk (Numbers and percentages)

ASCVD, atherosclerotic CVD; EPA, eicosapentaenoic; DPA, docosapentaenoic; ALA, octadecatrienoic; SDA, octadecatetraenoic.
The moderating effect of each single component of n-3 on the association between psoriasis and 10-year ASCVD risk (Odds ratios and 95 % confidence intervals)

Ref, reference; *: moderating term; ASCVD, atherosclerotic CVD; DPA, docosapentaenoic; ALA, octadecatrienoic; SDA, octadecatetraenoic.
Model 1, adjusted age, gender, race, education level, marital status and PIR.
Model 2, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
Association between α-linolenic acid intake, psoriasis and 10-year atherosclerotic CVD risk
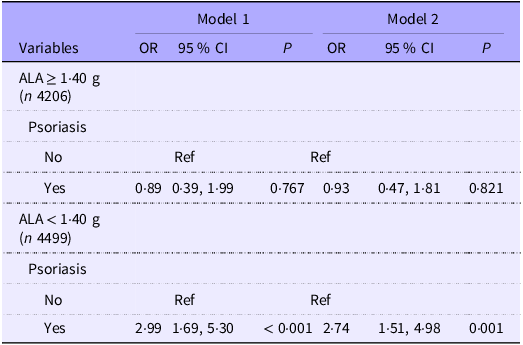
The association between different ALA intake levels of psoriasis and 10-year ASCVD risk is shown in Table 7. In the fully adjusted model, we observed that the risk of 10-year ASCVD was increased in subjects with psoriasis and lower ALA intake (< 1·40 g) (OR 2·74; 95 % CI 1·51, 4·98).
Association between ALA intake, psoriasis and 10-year ASCVD risk (Odds ratios and 95 % confidence intervals)

Ref, reference; ALA, octadecatrienoic; ASCVD, atherosclerotic CVD.
Model 1, adjusted age, gender, race, education level, marital status and PIR.
Model 2, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
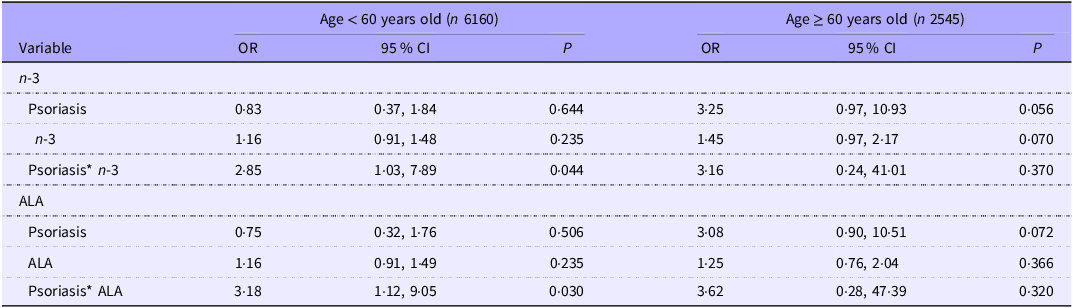
Subgroup analyses of the association between n-3, α-linolenic acid intake, psoriasis and 10-year atherosclerotic CVD risk based on age
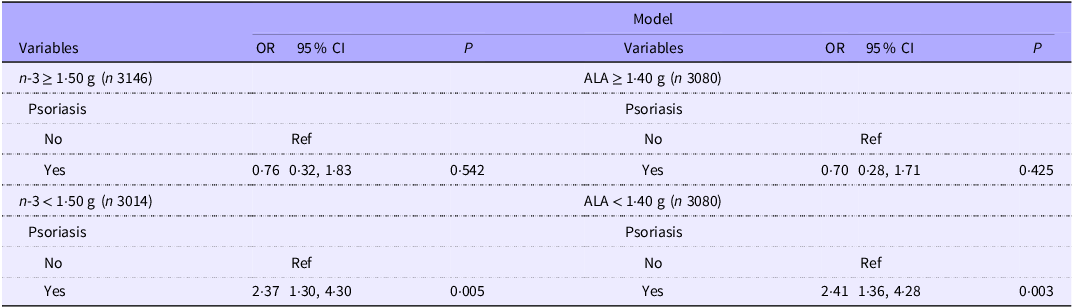
The total study population was divided into < 60 (n 6160) and ≥ 60 years (n 2545), and age-based subgroup analyses were performed to explore the stability of the moderating effect of n-3 and ALA intake on the association between psoriasis and 10-year ASCVD risk. The results suggested a moderating effect of n-3 and ALA intake on the association between psoriasis and 10-year ASCVD risk in the age group, as presented in Table 8. The effect of intake of n-3 and ALA on the association of psoriasis and 10-year ASCVD risk was more significant in those aged < 60 years than those aged ≥ 60 years (n-3: OR 2·85, 95 % CI 1·03, 7·89; ALA: OR 3·18, 95 % CI 1·12, 9·05). Moreover, compared with higher intake of n-3 and ALA, lower intake of n-3 and ALA were associated with higher psoriasis-related 10-year ASCVD risk in subjects aged < 60 years old (n-3: OR 2·37, 95 % CI 1·30, 4·30; ALA: OR 2·41, 95 % CI 1·36, 4·28) (Table 9).
The moderating effect of n-3 and ALA intake on the association between psoriasis and 10-year ASCVD risk based on age (Odds ratios and 95 % confidence intervals)

Ref, reference; *: moderating effect; ALA, octadecatrienoic; ASCVD, atherosclerotic CVD.
Model 1, adjusted age, gender, race, education level, marital status and PIR.
Model 2, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
The association between different levels of n-3 and ALA intake and psoriasis and 10-year ASCVD risk (Odds ratios and 95 % confidence intervals)

Ref reference; ALA, octadecatrienoic; ASCVD, atherosclerotic CVD.
Adjusted Model, adjusted age, gender, race, education level, marital status, PIR, physical activity, drug for dyslipidaemia, CKD, autoimmune disease, BMI overweight, total energy, SFA, MUFA, ALT, AST, Hb and uric acid.
This study conducted a multicollinearity analysis based on each regulating factor to validate the stability of the results. The findings indicated that there was no significant multicollinearity among the regulating factors and the confounding factors (online Supplementary Table S3).
Discussion
In this nationally representative cross-sectional study, n-3 intake was found to have a moderating effect on the psoriasis-related 10-year ASCVD risk. Maintaining high n-3 intake, especially ALA, may be an effective measure to improve and maintain the cardiovascular health of psoriasis patients.
There is increasing evidence to suggest that psoriasis, a systemic, autoimmune inflammatory disease, is related to increased CVD risk, and CVD is the leading cause of mortality and morbidity in psoriasis patients(Reference Gelfand, Troxel and Lewis22). As early as more than 50 years ago, researchers found in autopsies that psoriasis patients had higher levels of myocardial fibrosis and coronary atherosclerosis and that the vascular endothelium of both diseased and non-diseased skin became thinner and damaged(Reference Reed and Becker23). Subsequently, several epidemiological studies also demonstrated the association of psoriasis and poor cardiovascular events. In the 1970s, McDonald et al.(Reference McDonald and Calabresi24) suggested that the risk of occlusive dermatological vascular disease is significantly greater in psoriasis patients compared with non-psoriasis patients. A consensus drawn from AJC editors also reported that psoriasis was found to be related to coronary artery disease(Reference Friedewald, Cather and Gelfand25). However, these studies were small-scale and in primarily hospitalised cohorts. A prospective population-based study by Gelfand et al.(Reference Gelfand, Neimann and Shin26) in 2006 found that psoriasis may confer an independent risk of myocardial infarction (MI) and the relative risk was greater in young patients with severe psoriasis. A study from NHANES by Lai et al.(Reference Lai and Yew27) and Kan et al.(Reference Kan, Chen and Tao28) also yielded consistent conclusions. In the present study, we observed in the fully adjusted model, the 10-year ASCVD risk increased 65 % in psoriasis patients compared with non-psoriasis patients.
Several pathological mechanisms support the relationship between psoriasis and adverse cardiovascular events. The onset and progression of atherosclerosis involve a complex interaction among the endothelium, circulating lipids, platelets and the immune system, each of which is dysregulated in psoriasis(Reference Libby29). In psoriasis, the endothelium exhibits a pro-inflammatory phenotype, and several chemotactic and vascular adhesion molecules including VCAM1, CXCL10 and 1L-1β were observed to be upregulated(Reference Garshick, Barrett and Wechter30). Moreover, immune-mediated mechanisms including an abnormal myeloid cell response and direct cytokine-induced vascular injury may explain the potential link between psoriasis and atherosclerosis. In an atherosclerosis-prone mouse model of psoriasis, macrophages exhibit increased lipid uptake and foam cell formation(Reference Greb, Goldminz and Elder31). Several immune cells, including the neutrophil subtype known as low-density granulocytes, are related to non-calcified coronary plaque and induce endothelial damage in human beings(Reference Teague, Aksentijevich and Stansky32). The consequences of activation of the immune system include vascular arterial inflammation, with a relationship of psoriasis and vascular inflammation(Reference Teague, Aksentijevich and Stansky32).
A healthy dietary pattern can benefit multiple CVD risk factors. Recently, most of the international dietary guidelines now recommend replacing saturated fat with PUFA and MUFA. Three large trials assessing n-3 and cardiovascular health were conducted in 2018. Bowman et al.(Reference Bowman, Mafham and Wallendszus33) found no reduction in CVD risk when 1 g/d EPA and DHA intake was used for primary prevention in diabetic patients. However, not to be overlooked, there was a statistically significant 18 % relative risk reduction in vascular death, defined as death from CHD, stroke or other vascular causes. In a randomised, placebo-controlled trail, Manson et al.(Reference Manson, Cook and Lee34) drawn consistent conclusion with Bowman’s study that there was a significant reduction in total MI, which carried a hazard ratio of 0·71; 95 % CI 0·59, 0·9. Subjects consuming fewer than 1·5 fish meals per week and receiving n-3 supplementation had a significant reduction in major adverse cardiovascular events by 19 % and risk of MI by 40 %. Another Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Train (REDUCE-IT) in the USA reported that the outcomes including composite of CVD death, non-fatal MI, non-fatal stroke or CV revascularisation were reduced by 25 % in the treatment group(Reference Bhatt, Miller and Brinton35). A meta-analysis by Bernasconi et al.(Reference Bernasconi, Wiest and Lavie36) reported that EPA + DHA was related to statistically significantly lowered risk of CHD events and MI with equivalent risk reductions of 9 % and 13 %, respectively. Notably, this risk reduction was dose dependent for MI, as each additional 1 g/d was related to a significant risk reduction of 9 %. Li et al.(Reference Li, Shen and Guo37) conducted Mendelian randomisation analysis to explore the causal relationship between PUFA intake and the risk of psoriasis and found that circulating n-6 increased the risk of psoriasis, while n-3 reduced the risk of psoriasis. This study suggested that after a better understanding of PUFA intake and circulation, the public can be advised to modify their diet to reduce the risk of developing psoriasis.
We attempted to explain the modulating role of n-3 in the risk of psoriasis and 10-year ASCVD risk from a biomechanistic perspective. First, psoriasis is considered to be an autoimmune skin disease that secretes a large number of inflammatory cytokines, which in turn induce excessive proliferation of epidermal keratinocytes, and eventually, the interaction of the two cells produces a series of chronic inflammatory responses. An in vitro study tried to investigate the effects of ALA in the proliferation and differentiation of psoriasis keratinocytes in a skin model and found that ALA could reduce the activation of T-cell signalling pathways, thereby significantly reducing the secretion of inflammatory cytokines(Reference Morin, Simard and Rioux38). In addition, the benefits of n-3 intake for the maintenance of cardiovascular health have been widely discussed clinically. The role of n-3 in reducing the risk of ASCVD events comes in part from the reduction in TAG levels. n-3 reduces serum TAG levels by decreasing TAG synthesis and secretion and enhancing clearance from VLDL-cholesterol particles(Reference Backes, Anzalone and Hilleman39). In addition to regulating blood lipids, n-3 can also exert anti-atherosclerotic effects by regulating endothelial function, biofilm stability, inflammation and adhesion molecules, lipid peroxidation, etc., reducing plaque formation and stabilising plaques, reducing platelet activation and aggregation and regulating blood pressure and heart rate(Reference Sheikh, Vande Hei and Battisha40). It is worth mentioning that we did not observe moderating effects of EPA and DHA intake in the association between psoriasis and 10-year ASCVD risk, and we speculated that DHA and EPA intake may be generally lower in the USA population; second, the regulatory variable in this study was fatty acid intake rather than fatty acid levels in the body, so although EPA and DHA were not observed to have a significant regulatory role in the association of psoriasis and 10-year ASCVD risk, it does not mean that they do not play a role, and ALA is the basic substance that constitutes the cell membrane and biofilm of human tissues, which can be converted into EPA and DHA in the human body and absorbed by the body(Reference Plissonneau, Capel and Chassaing41).
Our study has several notable advantages. First, the large-scale sample and appropriate adjustment of covariates support the reliability and representativeness of our study. Second, to the best of our knowledge, this was the first study focused on the effect of dietary PUFA intake on the relationship between psoriasis and 10-year ASCVD risk. Our study provides some insight for clinicians and public health strategists on the potential benefits of increasing PUFA intake in the daily diet to maintain cardiovascular health in patients with psoriasis, with a better understanding of its optimal components and dosage. However, there were a few limitations worth noting. First, the cross-sectional study is a method for studying characteristics, phenomena or associations of human or social groups at different time points or in different regions. The design of a cross-sectional study has some inherent limitations. Data from cross-sectional studies are collected at a single point in time, and it is difficult to determine the temporal order of events or to determine whether a particular variable directly affects another variable. Therefore, our study cannot establish a cause association between the moderating effect of PUFA intake on psoriasis and 10-year ASCVD risk; additionally, cross-sectional studies are only based on known variables. However, residual confounding factors may have led to over- or -under-estimation of the association between exposure and outcomes; in observational studies, residual confounding may also interfere with the inference of the causality to some extent. Second, the diagnosis of psoriasis was based on self-reported questionnaires, introducing the possibility of recall bias. Third, the intake of PUFA in this study was obtained using a 24-h dietary recall interview. The 24-h dietary recall interview is a commonly used and flexible method to assess dietary intake, but objectively, it also has certain limitations. Respondents may not be able to accurately recall all foods and beverages ingested in the past 24 h; trace nutrient intake may fluctuate with seasons, dietary habits and individual differences, so a single 24-h dietary recall interview may not reflect long-term dietary intake; cooking method and food processing may affect the bioavailability and content of meals, but this information may have been overlooked in 24-h dietary recall interview. More large, multicentre prospective studies need to be designed in the future to further validate the modulating role of n-3, especially ALA, in psoriasis and 10-year ASCVD risk.
Conclusion
Our study provides evidence that dietary PUFA, especially ALA, may have a potential moderating effect on the relationship of psoriasis and 10-year ASCVD risk. Maintaining an adequate intake of PUFA may be a beneficial move to improve cardiovascular health in psoriasis patients. However, given the limitations of our study, further researches with well-designed prospective designs are needed to confirm the beneficial relationship between PUFA intake and 10-year ASCVD risk related to psoriasis.
Acknowledgements
None.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
X. L. designed the study, Y. L. wrote the manuscript, X. L. and Y. L. collected, analysed and interpreted the data, X. L. critically reviewed the manuscript and all authors read and approved the manuscript.
There are no conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525103437.