


An estimated 1.5 million youth under the age of 18 are arrested each year in the United States (Sickmund & Puzzanchera, Reference Sickmund and Puzzanchera2014), marking the beginning of their involvement with the juvenile legal system. System-involved youth experience higher rates of difficulties in the domain of behavioral health (Beaudry et al., Reference Beaudry, Yu, Långström and Fazel2021), which encompasses the full spectrum of externalizing (e.g., antisocial behavior, substance use, callous-unemotional [CU] traits) and internalizing (e.g., anxiety, depression) problems that individuals may face. While externalizing and internalizing problems are often treated as distinct constructs and studied separately, these behavioral health problems frequently co-occur and follow different developmental trajectories. Understanding how these patterns evolve together over time is essential for identifying system-involved youth at greatest risk for persistent difficulties.
Behavioral health problems among system-involved youth
Externalizing problems, characterized by outwardly directed behaviors such as aggression, antisociality, impulsivity, and substance use, are not only highly prevalent among system-involved youth but also strongly linked to their long-term legal and psychological outcomes. Research consistently shows that these behaviors are overrepresented in this population, with rates significantly higher than in community samples (Beaudry et al., Reference Beaudry, Yu, Långström and Fazel2021; Teplin et al., Reference Teplin, Abram, McClelland, Dulcan and Mericle2002). Moffitt’s (Reference Moffitt1993) dual taxonomy highlights heterogeneity in antisocial behavior trajectories, distinguishing youth whose antisocial behavior is limited to adolescence (i.e., adolescent-limited) from those whose problems persist across the life course (life-course persistent). More recent analytic approaches have extended this work by identifying two or three additional developmental trajectories, revealing patterns that range from consistently low involvement in antisocial behavior to steeply declining, persistently high, and in some cases gradually increasing involvement across adolescence (Kjellstrand et al., Reference Kjellstrand, Yu and Eddy2019; Mulvey et al., Reference Mulvey, Steinberg, Piquero, Besana, Fagan, Schubert and Cauffman2010; Nivard et al., Reference Nivard, Lubke, Dolan, Evans, Pourcain, Munafò and Middeldorp2017). However, most prior research models a single indicator at a time (e.g., antisocial behavior) and often draws from general population samples. As a result, these studies provide limited insight into how multiple domains of behavioral health co-develop and intersect, particularly among system-involved youth who frequently present with complex patterns of comorbidity.
While externalizing problems have been widely studied in system-involved youth, internalizing problems, such as anxiety and depression, are prevalent but less frequently examined. System-involved youth experience higher rates of internalizing problems compared to their nonsystem-involved peers (Beaudry et al., Reference Beaudry, Yu, Långström and Fazel2021; Kemp et al., Reference Kemp, Yurasek, Poindexter, Webb and Tolou-Shams2020; Krupa, Reference Krupa2024; Teplin et al., Reference Teplin, Abram, McClelland, Dulcan and Mericle2002). Although internalizing problems are prevalent in this population, their predictive role in adult legal outcomes is less clear. Prior research offers mixed findings, with some studies identifying internalizing symptoms as protective (e.g., Hirschfield et al., Reference Hirschfield, Maschi, White, Traub and Loeber2006), and others as risk-enhancing (e.g., Kjellstrand et al., Reference Kjellstrand, Yu and Eddy2019). These mixed findings suggest heterogeneity in how internalizing problems function across youth and underscore the need for models that account for interactions between internalizing symptoms and externalizing behaviors.
The Hierarchical Taxonomy of Psychopathology (HiTOP) offers one such model, providing a dimensional and empirically derived structure for understanding behavioral health. HiTOP explains comorbidity through shared etiological mechanisms and the organization of symptoms into related spectra and subfactors (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017; Krueger et al., Reference Krueger, Hobbs, Conway, Dick, Dretsch and Eaton2021). In this framework, externalizing and internalizing problems are not treated as discrete categories but interconnected dimensions of psychopathology, which may help explain why youth with persistent externalizing problems so often experience co-occurring internalizing difficulties. The dimensional perspective aligns with developmental cascades theory, which posits that difficulties or successes in one domain can “spill over” into other domains through reciprocal transactions and feedback loops, amplifying risk or protection across the life course (Masten & Cicchetti, Reference Masten and Cicchetti2010). Persistent externalizing problems may heighten exposure to stressful contexts (e.g., legal system involvement, strained family relationships) that, in turn, exacerbate internalizing symptoms. Internalizing difficulties may further impair coping strategies and emotional regulation, reinforcing externalizing behaviors. Together, these frameworks highlight the importance of examining the co-development of externalizing and internalizing problems to capture the mutually reinforcing processes that shape long-term behavioral health trajectories.
Longitudinal research provides growing support for this integrative perspective. Studies that have examined how internalizing problems co-develop longitudinally with externalizing problems in system-involved youth converge on a few key findings. First, youth with co-occurring internalizing and externalizing problems are at greater risk for negative outcomes, including legal system involvement, than youth with problems in just one domain (Achenbach et al., Reference Achenbach, Ivanova, Rescorla, Turner and Althoff2016; Estrada et al., Reference Estrada, Simmons and Baskin-Sommers2023). Second, increases in internalizing problems often predict subsequent increases in externalizing problems (Hussong et al., Reference Hussong, Jones, Stein, Baucom and Boeding2011) and vice versa (Moilanen et al., Reference Moilanen, Shaw and Maxwell2010; Van der Ende et al., Reference Van der Ende, Verhulst and Tiemeier2016), consistent with the cascade model. Critically, these patterns extend to long-term system involvement: youth with comorbid externalizing and internalizing problems face substantially elevated risks of adult criminal justice contact, with a significantly higher risk when compared to children with externalizing or internalizing problems only (Commisso et al., Reference Commisso, Geoffroy, Temcheff, Scardera, Vergunst, Côté, Vitaro, Tremblay and Orri2024; Copeland et al., Reference Copeland, Miller-Johnson, Keeler, Angold and Costello2007). Together, this evidence positions co-occurring internalizing and externalizing problems as a robust marker of elevated risk for persistent system involvement and underscores the value of modeling their co-development over time.
Multi-contextual influences on behavioral health
Understanding behavioral health development requires moving from describing patterns and change to examining how dynamic contextual risk and protective factors influence behavioral health in ways that could inform prevention or intervention efforts. Environmental contexts – such as family, peers, school, and neighborhoods – play a crucial role in shaping both externalizing and internalizing outcomes (Aldridge et al., Reference Aldridge, McChesney and Afari2018; Aldridge & McChesney, Reference Aldridge and McChesney2018; Brosschot et al., Reference Brosschot, Verkuil and Thayer2017; Conley et al., Reference Conley, Hernandez, Salvati, Gee and Baskin-Sommers2023; Estrada & Baskin-Sommers, Reference Estrada and Baskin-Sommers2024; Fay-Stammbach et al., Reference Fay-Stammbach, Hawes and Meredith2014). Foundational developmental theories (e.g., Bronfenbrenner’s social ecological model, Reference Bronfenbrenner1977) establish that understanding how these contexts operate together is critical for understanding youths’ developmental trajectories. Families and peers, conceptualized as microsystems that are more proximal to the youth, are theorized to have the strongest influence on youth outcomes. Neighborhoods, schools, and communities are conceptualized as distal exosystems that may contribute either directly to development or indirectly by influencing the conditions within the microsystems.
Externalizing and internalizing problems share many of the same contextual risk and protective factors, underscoring the importance of examining multiple contexts simultaneously. For example, parents play a central role in shaping behavioral health, with parental warmth and supervision serving as protective factors, while harsh discipline and neglect increase the risk for both anxiety and antisocial behavior (Hoeve et al., Reference Hoeve, Dubas, Eichelsheim, Van der Laan, Smeenk and Gerris2009; McLeod et al., Reference McLeod, Wood and Weisz2007). Similarly, peer relationships can buffer when supportive but exacerbate externalizing behaviors when characterized by delinquent peer influence (McGloin & Thomas, Reference McGloin and Thomas2019; Roach, Reference Roach2018). School environments also significantly contribute to behavioral health – positive teacher – student relationships and school engagement are linked to lower rates of depression and delinquency, whereas school disengagement and punitive disciplinary practices heighten risk (Skiba et al., Reference Skiba, Arredondo and Williams2014; Wang & Fredricks, Reference Wang and Fredricks2014). Lastly, neighborhood conditions, such as exposure to violence and socioeconomic disadvantage, have been linked to both internalizing and externalizing outcomes (Dierkhising et al., Reference Dierkhising, Ko, Woods-Jaeger, Briggs, Lee and Pynoos2013; McLaughlin et al., Reference McLaughlin, Green, Gruber, Sampson, Zaslavsky and Kessler2012). These factors operate dynamically, shaping youth development in ways that cannot be fully understood when examined in isolation.
Youth develop within these multiple contexts simultaneously, and their experiences within each influence development uniquely or synergistically (Mrug & Windle, Reference Mrug and Windle2010; Youngblade et al., Reference Youngblade, Theokas, Schulenberg, Curry, Huang and Novak2007). Studies examining the etiology and development of behavioral health problems have benefited from examining the relative risk and protection conferred by these intersecting contexts. For example, Simmons et al. (Reference Simmons, Mitchell-Adams and Baskin-Sommers2022) examined how environmental factors, including parental hostility, antisocial peers, community violence, and neighborhood disorder, influenced within-person changes in CU traits among system-involved youth. Their findings indicated that more proximal environmental conditions – such as negative parenting and affiliation with antisocial peers – had stronger and more consistent associations with CU traits than distal conditions like neighborhood disorder and community violence. At the same time, their study demonstrated that distal contexts, such as community violence, were also significantly associated with CU traits, reinforcing the importance of considering multiple environmental influences rather than focusing on any single context in isolation. A multi-contextual research approach is essential to develop a more complete understanding of the contextual risk and protective factors associated with behavioral health problems among system-involved youth.
The current study
Behavioral health research on system-involved youth has been constrained by limited consideration of co-occurring externalizing and internalizing problems and a lack of attention to developmental heterogeneity and environmental influences. To address these gaps, the current study investigated how externalizing (antisocial behavior, antagonistic traits, harmful substance use) and internalizing (distress) problems co-develop among system-involved male youth from the Crossroads Study (Cauffman et al., Reference Cauffman, Beardslee, Fine, Frick and Steinberg2021) during the three years following their first official arrest. This sample is notable for its racial, ethnic, and socioeconomic diversity, which allowed us to examine these processes among youth often underrepresented in developmental research but overrepresented in the legal system. On the other hand, the Crossroads sample includes only male youth. While this sampling approach impedes generalizability to female youth, it allows for a focused investigation of behavioral health development in system-involved male youth, who remain a relatively understudied developmental subgroup.
We employed group-based multi-trajectory modeling (GBMTM), a person-centered analytic approach designed to identify distinct subgroups of individuals following similar trajectories across multiple outcomes (Laursen & Hoff, Reference Laursen and Hoff2006; Nagin et al., Reference Nagin, Jones, Passos and Tremblay2018). Person-centered approaches are a valuable complement to more commonly utilized variable-centered approaches that describe relationships related to a single variable (Howard & Hoffman, Reference Howard and Hoffman2018). This approach allowed for a more comprehensive understanding of the heterogeneity in behavioral health trajectories among system-involved youth. Given the data-driven nature of GBMTM, the trajectory analyses in this study were exploratory, allowing us to identify naturally occurring subgroups of youth based on their co-occurring externalizing and internalizing trajectories without imposing predefined theoretical constraints.
In addition to characterizing the developmental trajectories of behavioral health problems, we investigated whether youth who followed different trajectories also varied in their likelihood of future rearrest in young adulthood. Rearrest is a critical metric of interest in the juvenile legal system, as it reflects the system’s effectiveness in addressing the risks and needs that contributed to youth being involved in the legal system in the first place. By linking adolescent symptom development to future young adult legal outcomes, we aimed to inform early identification and intervention efforts within the juvenile system. Although rearrest and self-reported offending are correlated, they differ conceptually and practically in ways that shaped our analytic approach (Huizinga & Elliott, Reference Huizinga and Elliott1986; Krohn et al., Reference Krohn, Thornberry, Gibson and Baldwin2010). Behavioral health trajectories were modeled using self-reported offending to capture a broad range of youth-reported antisocial behaviors. In contrast, rearrest reflects formal system responses and serves as a direct indicator of continued legal system involvement. In line with prior research (Commisso et al., Reference Commisso, Geoffroy, Temcheff, Scardera, Vergunst, Côté, Vitaro, Tremblay and Orri2024; Copeland et al., Reference Copeland, Miller-Johnson, Keeler, Angold and Costello2007), we hypothesized that subgroups characterized by elevated and increasing co-occurring internalizing and externalizing problems would demonstrate higher rearrest rates than subgroups with low or decreasing behavioral health problems. By linking developmental patterns of behavioral health to young adult rearrest outcomes, this study provided a clearer picture of which youth are most at risk for continued legal system involvement.
Finally, we explored multi-contextual risk and protective factors that distinguish high-risk trajectory groups. Youth development is shaped by interconnected social contexts – including families, peers, schools, and neighborhoods – which collectively influence behavioral health outcomes (Bronfenbrenner, Reference Bronfenbrenner1977). Importantly, many of the contextual predictors we examined, such as parental monitoring, peer deviance, and violence exposure, are especially relevant for system-involved youth, among whom these factors have been strongly linked to juvenile legal system outcomes (Chung & Steinberg, Reference Chung and Steinberg2006). Based on this, we hypothesized that youth in the high-risk trajectories would report greater exposure to contextual risk factors (e.g., lower parental monitoring, less supportive peer relationships, more neighborhood disorder). Identifying the specific environmental factors associated with elevated or lower risk for behavioral health problems provides a more comprehensive understanding of the relations between behavioral health trajectories and external influences. Altogether, this study aimed to provide a more comprehensive understanding of behavioral health development in system-involved youth and offer insights into potential prevention and intervention points.
Method
Participants
Data were drawn from the Crossroads Study (Cauffman et al., Reference Cauffman, Beardslee, Fine, Frick and Steinberg2021). The primary aim of the Crossroads study was to investigate how formally and informally processed youth differ in their rate of subsequent illegal behavior and legal system contact. However, it also examined a host of other developmentally relevant variables, including measures of behavioral health and environmental factors. The study tracked 1,216 male adolescents from three locations: Orange County, California; Jefferson Parish, Louisiana; and Philadelphia, Pennsylvania. Participants were between 13 and 18 years old (Mage = 15.29) at the baseline assessment. The sample was racially and ethnically diverse: 46% Latino or Hispanic, 37% Black or African American, 15% White, and 2% identifying as multiracial, multiethnic, or another racial/ethnic background. Youth were eligible if they had no prior arrests, were charged with specific offenses, and were being processed for the first time. Eligible offenses varied by site but included charges that resulted in formal processing for approximately half of first-time offenders (e.g., simple assault/battery, theft, criminal damage/mischief).
Recruitment involved collaboration with probation departments, district attorneys, and local courts. Eligible youth and their families were approached after case dispositions, and informed consent was obtained from parents or guardians, with youth providing assent. About 80% of eligible participants agreed to enroll in the study. Retention rates exceeded 85% for each assessment.
Procedure
Data collection included structured interviews conducted in participants’ homes or other private settings, with secure facilities utilized as needed. Baseline interviews occurred between July 2011 and June 2013, and follow-up interviews were conducted every six months for the first three years, followed by annual interviews until 9 years after baseline. Interviews covered a broad range of topics, including participants’ attitudes, behaviors, family dynamics, and peer influences. Sensitive questions (e.g., those addressing criminal behavior) were administered using anonymous keypad entry to enhance privacy and accuracy. To encourage participation and retention, youth were compensated for their time with payments that increased over the course of the study, and a specialized tracking system was employed to maintain contact with participants.
Measures
Behavioral health
Behavioral health indicators were chosen based on availability in the Crossroads Study and alignment with the HiTOP framework (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017). For externalizing, we retained three distinct indicators given their empirical and functional separation into subfactors in HiTOP and prior work (Frick & White, Reference Frick and White2008; Krueger et al., Reference Krueger, Hobbs, Conway, Dick, Dretsch and Eaton2021): antisocial behavior, harmful substance use, and antagonistic traits. Treating these domains separately allowed us to investigate whether they follow different developmental courses with distinct implications for risk. For internalizing symptoms, because anxiety and depression are highly comorbid and load on the HiTOP distress subfactor (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017), we combined the anxiety and depression subscales into a single distress composite.
Antisocial Behavior. Antisocial behavior, a subfactor of the externalizing psychopathology spectrum (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017; Krueger et al., Reference Krueger, Hobbs, Conway, Dick, Dretsch and Eaton2021), is broadly defined as actions that violate societal norms or infringe on the rights of others. Antisocial behavior is often operationalized through self-reported offending in research on youth development (Huizinga & Elliott, Reference Huizinga and Elliott1986; Krohn et al., Reference Krohn, Thornberry, Gibson and Baldwin2010). This approach is advantageous because it captures a wide range of behaviors, including those not detected by official systems, and minimizes systemic biases associated with differential enforcement practices.
Antisocial behavior was assessed using a modified version of the Self-Report of Offending scale (SRO; Huizinga et al., Reference Huizinga, Esbensen and Weiher1991). Offending variety was chosen as the primary measure because it correlates strongly with other metrics of offending (e.g., frequency and severity) while being less influenced by recall errors and the overrepresentation of minor offenses (Monahan & Piquero, Reference Monahan and Piquero2009; Osgood et al., Reference Osgood, McMorris and Potenza2002). At each assessment, youth indicated whether they had committed any of 24 specific illegal activities during the recall period (e.g., “In the past 6 months, have you taken something from another person by force, without using a weapon?”) Responses were recorded as “yes” (=1) or “no” (=0). A total offending score was calculated by summing the total number of affirmative responses, with higher scores indicating higher offending.
Harmful Substance Use. Harmful substance use, a subfactor of the externalizing psychopathology spectrum (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017; Krueger et al., Reference Krueger, Hobbs, Conway, Dick, Dretsch and Eaton2021), was measured using items adapted from the Substance Use/Abuse Inventory (Chassin et al., Reference Chassin, Rogosch and Barrera1991). Social consequences and dependency were chosen as the primary measure because they align with other measures of harmful or disordered substance use (e.g., DSM-5 substance use disorder) and better capture the clinical and functional impairments indicative of problematic use (Hasin et al., Reference Hasin, O’Brien, Auriacombe, Borges, Bucholz, Budney, Compton, Crowley, Ling, Petry, Schuckit and Grant2013). At each assessment, youth indicated whether they had incurred any of 17 social consequence items (e.g., “Have you ever had problems or arguments with family or friends before because of your alcohol or drug use?”) and 10 dependency items (e.g., “Have you ever wanted a drink or drugs so badly that you could not think of about anything else?”) during the recall period. Responses were recorded as “yes” (=1) or “no” (=0). A total harmful substance use score was calculated by summing the number of affirmative responses, with higher scores indicating more harmful substance use.
Antagonistic Traits. Antagonistic traits, a subfactor of externalizing psychopathology spectrum (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017; Krueger et al., Reference Krueger, Hobbs, Conway, Dick, Dretsch and Eaton2021), is characterized by navigating interpersonal situations using antipathy and conflict, hurting other people intentionally with little regard for their rights and feelings. Antagonistic traits encompass CU traits, which have been found to distinguish youth at risk for more severe and persistent antisocial behavior (Frick & White, 2008). CU traits have been linked to greater aggression, lower responsivity to punishment, and a higher likelihood of chronic offending, making them critical to understanding behavioral health trajectories in system-involved youth (Frick & White, 2008). CU traits were assessed using the 24-item Inventory of Callous-Unemotional Traits (ICU; Kimonis et al., Reference Kimonis, Frick, Skeem, Marsee, Cruise, Munoz and Morris2008). Participants were asked how well callous (e.g., “I do not feel remorseful when I do something wrong”), uncaring (e.g., “I do not care about doing things well”), and unemotional (e.g., “I do not show my emotions to others”) items reflected their thoughts and feelings. Participants responded on a 4-point Likert scale ranging from 0 (not at all true) to 3 (definitely true). CU trait scores were calculated by summing the items, with higher totals indicating greater CU traits.
Distress. Distress, a subfactor of the internalizing psychopathology spectrum (Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Zimmerman2017), encompasses both anxiety and depression, which have high comorbidity rates. Distress was assessed using the 16-item Revised Children’s Anxiety and Depression Scale (RCADS; Chorpita et al., Reference Chorpita, Yim, Moffitt, Umemoto and Francis2000). Youth reported how often they experienced symptoms of anxiety (e.g., “I worry that bad things will happen to me”) and depression (e.g., “Nothing is much fun anymore”). Participants responded on a 4-point scale ranging from 0 (Never) to 3 (Always). The total score was obtained by summing the items, with higher scores reflecting greater levels of distress symptoms.
Rearrest
Rearrest data were drawn from official records at four, five, seven, and nine years after baseline. Rearrest was measured dichotomously and cumulatively, meaning that if a participant was rearrested at any of these time points, they were coded as “yes” (=1) for having been rearrested. If they had no recorded rearrests across all time points, they were coded as “no” (=0).
Contextual factors
Family. Family risk factors included family criminality, parental deviance, and parental hostility. The family criminality measure assesses whether any family members have been involved in criminal activity, arrested, and/or jailed (M = 0.57, SD = 0.50). Parental deviance was assessed using a modified version of the association with deviant peers scale (Thornberry et al., Reference Thornberry, Lizotte, Krohn, Farnworth and Jang1994) with the word “parents” substituted for “peers” to assess parental antisocial behavior and antisocial influence. The 20-item questionnaire asked whether or not (yes = 1, 0=no) their parents had engaged in antisocial behavior (e.g., “Hit or threatened to hit someone?”) or suggested that the youth engage in antisocial behavior (e.g., “Suggest that you hit or beat someone up?”). A total parent deviance score was calculated as the proportion of deviant/antisocial behaviors endorsed, with a higher score indicating greater parent deviance (M = 0.05, SD = 0.07).
Parental hostility was assessed using an adapted version of the Quality of Parental Relationships Inventory (Conger & Conger, Reference Conger and Conger1994), which measures the affective qualities of the youth’s relationships with parents. Twelve items assessed hostility (e.g., “How often does your mother get angry at you?”). Participants responded on a 4-point Likert scale ranging from 1 (Never) to 4 (Always). Higher hostility scores indicated greater parental hostility.
Family protective factors included parental monitoring, parental warmth, and positive home environment. Parental monitoring was assessed using a 14-item questionnaire about household rules regarding supervision (Steinberg et al., Reference Steinberg, Lamborn, Dornbusch and Darling1992). Participants responded to items (e.g., “How often do you have a set time to be home on weekend nights?”) on a 4-point Likert scale ranging from 1 (Never) to 4 (Always). A total parental monitoring score was calculated by averaging the items, with higher scores indicating more parental monitoring (M = 3.15, SD = 0.58).
Parental warmth was assessed using an adapted version of the Quality of Parental Relationships Inventory (Conger & Conger, Reference Conger and Conger1994), which measures the affective qualities of the youth’s relationships with parents. Nine items assessed relationship warmth (e.g., “How often does your mother let you know she really cares about you?”). Participants responded on a 4-point Likert scale ranging from 1 (Never) to 4 (Always). Higher warmth scores indicated greater parental warmth.
Positive home environment was assessed using a 37-item scale adapted from a measure of living conditions in detention centers. The items assess participants’ level of comfort (e.g., “I enjoy being there,” “I am happy when I am there”) and feelings of safety at home (e.g., “When I’m there, I feel safe,” “Being there makes me feel nervous or worried”). Participants responded on a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). A total home environment score was calculated by averaging the items, with higher scores indicating a more positive home environment (M = 3.89, SD = 0.48).
Peer. Peer risk factors included peer deviance and peer hostility. Peer deviance was assessed using a modified version of the association with deviant peers scale (Thornberry et al., Reference Thornberry, Lizotte, Krohn, Farnworth and Jang1994). The 20-item questionnaire asked the number of participant’s friends who have engaged in antisocial behavior (e.g., “Sold drugs?”) as well as the number of friends a participant had who suggested they engage in antisocial behavior (“Suggested that you should sell drugs?”). Participants responded on a 5-point Likert scale ranging from 1 (none of them) to 5 (all of them). The total peer deviance score was calculated by averaging the items, with higher scores indicating greater peer deviance (M = 1.63, SD = 0.61). Peer hostility was assessed using an adapted version of the Quality of Parental Relationships Inventory (Conger & Conger, Reference Conger and Conger1994), which measures the affective qualities of the youth’s relationships. Twelve items assessed hostility (e.g., “How often do your friends get angry at you?”). Higher hostility scores indicated greater peer hostility.
Peer protective factors included peer warmth, assessed using an adapted version of the Quality of Parental Relationships Inventory (Conger & Conger, Reference Conger and Conger1994), which measures the affective qualities of the youth’s relationships. Nine items assessed relationship warmth (e.g., “How often do your friends let you know they really care about you?”). Participants responded on a 4-point Likert scale ranging from 1 (Never) to 4 (Always). Higher warmth scores indicated greater peer warmth.
Violence Exposure. Exposure to violence was assessed using 15 items adapted from the Exposure to Violence Inventory (Selner-O’Hagan et al., Reference Selner-O’Hagan, Kindlon, Buka, Raudenbush and Earls1998). Items documented seven witnesses (e.g., “Have you ever seen someone else being raped, an attempt made to rape someone, or any other type of sexual attack?”), six victimization (e.g., “Have you ever been chased where you thought you might seriously be hurt?”), and two exposure to death (e.g., “Has anyone close to you ever died?”) experiences. Participants responded to each item based on a dichotomous choice (yes = 1, no = 0). A total score was calculated using the sum of all items, with higher scores indicating higher violence exposure (M = 2.81, SD = 2.65).
Neighborhood. Neighborhood risk factors included neighborhood disorder, assessed using a 21-item questionnaire adapted from the Neighborhood Conditions Measure (Sampson & Raudenbush, Reference Sampson and Raudenbush1999). Items assessed how often youth witnessed both physical (e.g., “cigarettes on the street or in the gutters,” “graffiti or tags”) and social disorder (e.g., “adults fighting or arguing loudly,” “people using needles or syringes to take drugs”) in their neighborhood. Participants responded on a 4-point Likert scale ranging from 1 (Never) to 4 (Often). A total neighborhood disorder score was calculated by averaging the items, with higher scores indicating greater neighborhood disorder (M = 2.07, SD = 0.68).
School. School protective factors included teacher bonding and school orientation, which were assessed using 10 items based on the work of Cernkovich & Giordano (Reference Cernkovich and Giordano1992). Teacher bonding evaluates the degree to which students feel connected to and supported by their teachers (e.g., “Most of my teachers treat me fairly”). Participants responded on a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). A total teacher bonding score was calculated by averaging the items, with higher scores indicating a stronger bond with teachers (M = 3.46, SD = 0.82). School orientation assesses students’ attitudes toward their educational experience and the importance they place on schoolwork (e.g., ”Schoolwork is very important to me”). Participants responded on a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). A total school orientation score was calculated by averaging the items, with higher scores indicating a more positive orientation toward school (M = 3.91, SD = 0.63).
Individual Factors. Age at baseline was included as a covariate in the trajectory analyses to account for differences in youth’s developmental stage at the time of their initial arrest (ages 13–17). This adjustment helps control for potential variations in behavioral, social, and legal experiences that may be associated with entering the justice system at different ages. The nature of the index offense was included as a predictor of trajectory group membership to determine whether it may help distinguish youth who may be at risk for following high-risk trajectories of externalizing and internalizing symptoms. The nature of the index offense was drawn directly from official records and categorized dichotomously as either violent (=1) or nonviolent (=0) based on the charge (%violent = 18.17).
Analytic plan
Group-based multi-trajectory modeling (GBMTM) was employed to identify subgroups of youth with similar co-occurring trajectories of externalizing (antisocial behavior, antagonistic traits, harmful substance use) and internalizing (distress) symptoms. GBMTM is a person-centered analytic approach that identifies latent clusters of individuals following similar trajectories across multiple indicators of an outcome of interest (Nagin et al., Reference Nagin, Jones, Passos and Tremblay2018). The GBMTM approach is an extension of the dual-trajectory approach, which estimates the association between two variables by measuring the probability of a trajectory for the first variable given membership in a specific trajectory for the second variable. In contrast, the multi-trajectory approach examines the association by defining trajectory groups based on patterns of change for multiple variables simultaneously. The models were estimated using the Stata traj plugin (Jones & Nagin, Reference Jones and Nagin2013). Data from the baseline, 6-, 12-, 18-, 24-, 30-, and 36-month interviews were used in the trajectory analyses. For trajectory estimation, we used Full Information Maximum Likelihood to leverage all available repeated measures; 81.4% (n = 990) had complete data on the trajectory indicators. Descriptive statistics and missingness rates for trajectory model variables are provided in Supplemental Table 6.
We modeled the trajectories using the first three years to capture early postarrest changes at six-month intervals. Antisocial behavior, harmful substance use, antagonistic traits, and distress were included as the outcomes in the trajectories. Baseline age was included as a covariate. We followed guidelines for reporting on latent trajectory modeling (see Supplemental Materials, pp. 1–18). First, the optimal number of trajectory groups was selected by attempting to find model solutions in up to nine groups and comparing model fit across the model solutions that were found (Supplemental Table 1). Several model fit criteria were considered (Nagin, Reference Nagin2005). The Lo-Mendell-Rubin likelihood ratio test indicates whether a more complex model improves fit relative to a simpler model with a significance test. Entropy is a measure of classification uncertainty ranging from 0–1, with more certainty and class discrimination indicated with values approaching 1.0 and values greater than 0.8 considered acceptable (Celeux & Soromenho, Reference Celeux and Soromenho1996). Average posterior probability of trajectory group membership approximates the internal reliability for each trajectory ranging from 0–1, with values greater than 0.8 considered acceptable (Andruff et al., Reference Andruff, Carraro, Thompson, Gaudreau and Louvet2009). Odds of correct classification (with values above five being considered adequate) and trajectory size (i.e., greater than 5%) were also considered. Spaghetti plots of the optimal model solution (Supplemental Figure 1) and estimated mean trajectories for each solution (Supplemental Figure 2) are provided in the Supplemental Materials.
Differences in rearrest likelihood among the identified trajectory groups were examined using binomial logistic regression analyses, predicting rearrest during the five years following the last timepoint of the trajectory analyses. Age at baseline was included as a covariate. Missing data were handled via casewise deletion; complete rearrest data were available for 74.4% of the sample (n = 911). For rearrest prediction analyses, the trajectory group with the lowest externalizing and internalizing scores served as the reference group. Post hoc simple contrasts were conducted to compare trajectory groups that significantly differed from the reference group to each other. To examine how baseline contextual factors predicted high-risk group membership, we conducted separate bivariate logistic regression analyses for each high-risk trajectory group. Each model predicted binary group membership (1 = member of the target group; 0 = all others) from a single baseline predictor (i.e., 15 predictors per group). We applied a Bonferroni correction within each set of models to control for Type I error. Missing data were handled via casewise deletion; complete data on all antecedent predictors were available for 85.5% of the sample (n = 1040). Cumulative rearrest rates within the first three years for each trajectory group are provided in Supplemental Table 4. Descriptive statistics and missingness rates for all antecedent predictors are provided in Supplemental Table 5. A correlation matrix for antecedents assessed at baseline is provided in Supplemental Table 7. All statistical analyses were performed in Stata v18.
Missing data
We examined the pattern of missing data across all longitudinal behavioral health variables and rearrest outcomes. Little’s Missing Completely at Random (MCAR) test was nonsignificant (χ2(2462) = 2564.77, p = .073), indicating that the joint pattern of missingness did not depart from MCAR. We also examined demographic predictors of missingness, which revealed that Black youth had slightly higher odds of missing rearrest data compared with White youth (OR = 1.55, p = .024). No other differences in missingness were observed based on race, ethnicity, or age.
Results
Preliminary analyses
To evaluate whether the baseline behavioral health indicators aligned with the HiTOP framework, we estimated a four-factor confirmatory factor analysis using WLSMV. Model fit was acceptable (WLSMV: CFI = 0.93, TLI = 0.92, RMSEA = 0.046, SRMR = 0.109), and all items loaded significantly onto their intended factors, supporting the distinction among antisocial behavior, harmful substance use, antagonistic traits, and distress. Consistent with HiTOP, the two disinhibited externalizing subfactors (antisocial behavior and harmful substance use) were strongly correlated (r = 0.80). Antagonistic traits showed moderate correlations with both antisocial behavior (r = 0.38) and harmful substance use (r = 0.32), as expected for a separate subfactor within the broader externalizing spectrum. In contrast, correlations between all externalizing subfactors and distress were small (rs = 0.12–0.14), indicating clear separation between externalizing and internalizing spectra. This pattern provides strong evidence that the behavioral health indicators underlying the trajectory model reflect distinguishable, HiTOP-consistent psychopathology subfactors.
Model comparison
Model fit indices suggested that an eight-trajectory solution optimally characterized the sample (see Supplemental Tables 1 and 2). Figure 1 illustrates the eight trajectory groups, which differed in their initial values and rate of change in externalizing (antisocial behavior, harmful substance use, antagonistic traits) and internalizing (distress) subfactor symptoms. Low, moderate, and high classifications of baseline symptom levels for each trajectory group were designated based on sample statistics with a 0.5 SD cutoff (see Supplemental Table 8).
Group trajectory estimates for the optimal model solution. Note: Descriptive labels and sample sizes for each group are as follows: G1 (lowest symptoms – stable; n = 225), G2 (high substance use – improving; n = 133), G3 (moderate symptoms – improving; n = 329), G4 (high antagonistic traits – stable; n = 103), G5 (moderate symptoms – stable; n = 143), G6 (moderate symptoms – worsening; n = 114), G7 (high symptoms – rapidly improving; n = 98), and G8 (highest symptoms – partially improving; n = 71).

Figure 1 Long description
Panel A: The line graph shows the trajectory of antisocial behavior over 36 months following initial arrest. The x-axis represents months, and the y-axis represents the level of antisocial behavior. Different groups (G1 to G8) show varying trends, with some groups exhibiting stable behavior, while others show improvement or worsening over time. Panel B: The line graph illustrates harmful substance use over the same period. The x-axis represents months, and the y-axis represents the level of harmful substance use. Different groups show distinct patterns, with some groups reducing substance use and others increasing or maintaining their levels. Panel C: The line graph depicts antagonistic traits over 36 months. The x-axis represents months, and the y-axis represents the level of antagonistic traits. Groups show varying trends, with some remaining stable and others improving or worsening. Panel D: The line graph shows distress levels over 36 months. The x-axis represents months, and the y-axis represents the level of distress. Different groups exhibit different patterns, with some groups showing a decrease in distress and others showing an increase or stability.
Four groups demonstrated low to moderate externalizing and internalizing subfactor symptoms at baseline. The Lowest Symptoms – Stable group (Group 1 [G1]; 8.5% of the sample) was characterized by having the lowest symptom levels at baseline, which remained stable over time. The Moderate Symptoms – Improving group (Group 3 [G3]; 23.1%), the Moderate Symptoms – Stable group (Group 5 [G5]; 14.8%), and the Moderate Symptoms – Worsening group (Group 6 [G6]; 9.0%) all exhibited moderate symptoms across subfactors at baseline. However, they diverged substantially by their subsequent trajectories. The Moderate Symptoms – Improving (G3) group’s symptoms declined over time, while the Moderate Symptoms – Stable (G5) group’s symptoms remained largely unchanged. The Moderate Symptoms – Worsening (G6) group was unique in that it was the only group that displayed escalating symptoms across three subfactors – antisocial behavior, harmful substance use, and distress – while antagonistic traits remained stable.
Two groups started with elevations in a single externalizing subfactor alongside moderate distress. The High Substance Use – Improving group (Group 2 [G2]; 11.4%) and the High Antagonistic Traits – Stable group (Group 4 [G4]; 18.3%) each showed a distinct elevation at baseline – harmful substance use and antagonistic traits, respectively. However, the High Substance Use – Improving (G2) group exhibited symptom improvements over time across all factors, while the High Antagonistic Traits – Stable (G4) group showed persistently high antagonistic traits with little change apart from declining antisocial behavior.
Two groups exhibited elevated symptoms across all externalizing subfactors at baseline in combination with moderate distress. The High Symptoms – Rapidly Improving group (Group 7 [G7]; 9.5%) and the Highest Symptoms – Partially Improving group (Group 8 [G8]; 5.4%) both began with high levels of antisocial behavior, harmful substance use, and antagonistic traits. The High Symptoms – Rapidly Improving (G7) group showed sharp improvement over the three-year trajectory period across all externalizing and internalizing subfactors. The Highest Symptoms – Partially Improving (G8) group demonstrated improvement in the externalizing subfactors but experienced worsening distress that increased during the first six months and remained persistently high thereafter.
Young adulthood rearrest outcomes
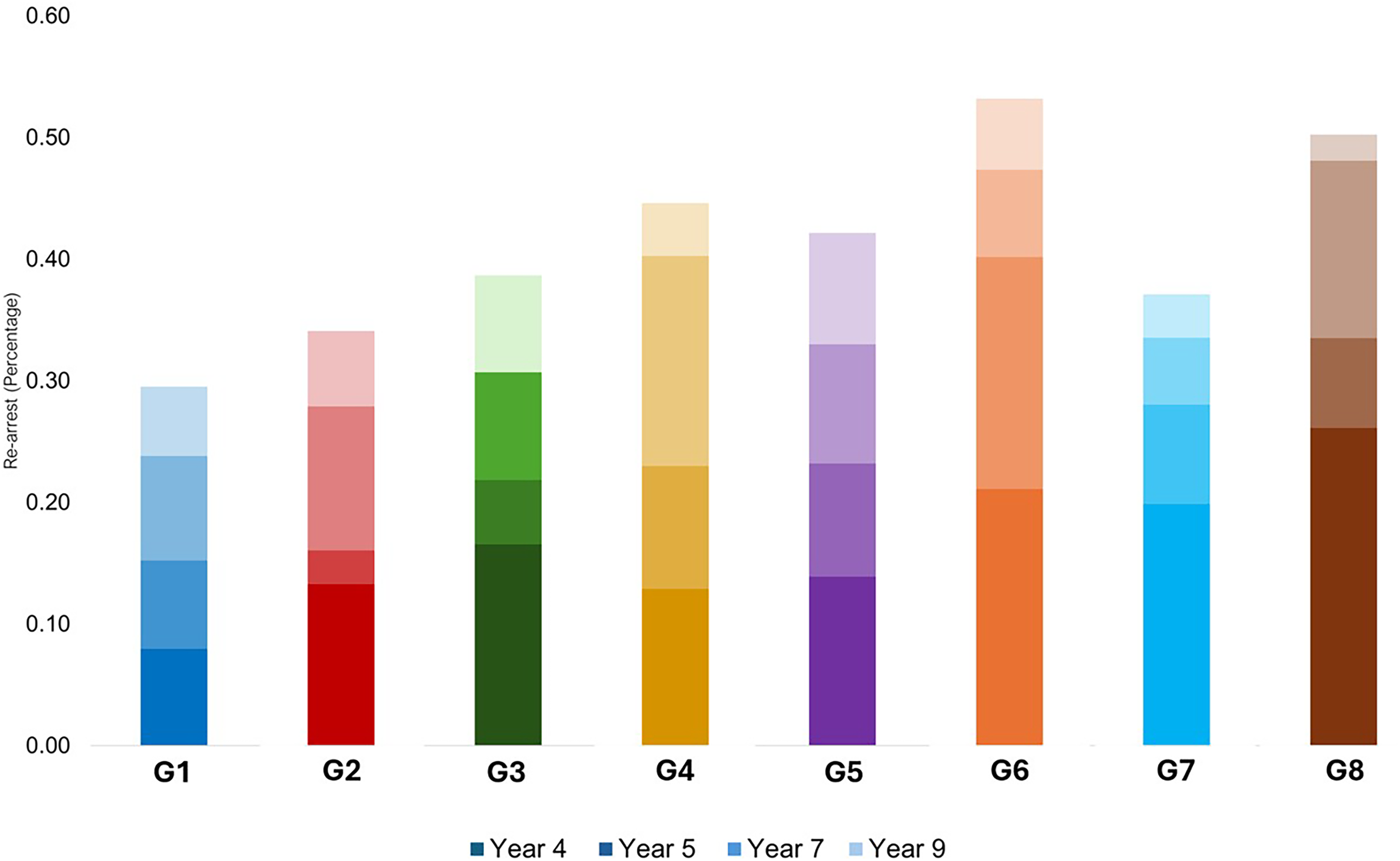
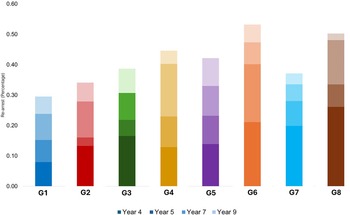
Figure 2 displays the cumulative rearrest likelihoods by group. The likelihood of rearrest substantially varied across the trajectory groups. The Lowest Symptoms – Stable group (G1) exhibited the lowest likelihood of rearrest (23.8% rearrested). Post hoc Sidak-corrected pairwise comparisons found that the High Antagonistic Traits – Stable group (G4; 40.3% rearrested), the Moderate Symptoms – Worsening group (G6; 47.3% rearrested), and the Highest Symptoms – Partially Improving group (G8; 48.1% rearrested) exhibited significantly higher probability (p < .05) of rearrest than those in the Lowest Symptoms – Stable (G1) group. No significant differences in rearrest were observed among any of the other groups. Of note, those in the High Symptoms – Rapidly Improving (G7) group, which began with elevated but rapidly improving externalizing and internalizing subfactor symptoms, demonstrated a relatively low rearrest rate (37.1%).
Cumulative rearrest rates by trajectory group. Note: Descriptive labels and sample sizes for each group are as follows: G1 (lowest symptoms – stable; n = 225), G2 (high substance use – improving; n = 133), G3 (moderate symptoms – improving; n = 329), G4 (high antagonistic traits – stable; n = 103), G5 (moderate symptoms – stable; n = 143), G6 (moderate symptoms – worsening; n = 114), G7 (high symptoms – rapidly improving; n = 98), and G8 (highest symptoms – partially improving; n = 71).
Contextual factors
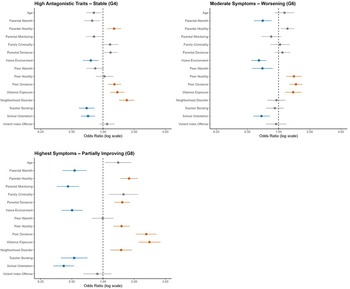
To identify baseline contextual risk and protective factors predicting membership in the three high-risk trajectory groups, we conducted separate bivariate logistic regressions for each of the 15 predictors within each group. Bonferroni correction was applied to control for Type I error. Figure 3 displays all predictors and indicates which were significant after correction; full model results are presented in Supplemental Table 3. Across the three high-risk trajectories, several predictors emerged as cross-cutting risk and protective factors. Peer deviance and violence exposure were consistently associated with membership in all high-risk trajectories, suggesting that they may reflect core developmental factors common to multiple high-risk pathways. Similarly, positive home environment and school orientation functioned as protective factors across groups, highlighting their broad relevance for behavioral health development.
Baseline contextual risk and protective factors associated with the three trajectory groups at highest risk for rearrest. Note: Odds ratios and 95% confidence intervals are displayed for each predictor. Bonferroni correction was applied to account for 15 comparisons per group. Red bars indicate predictors associated with a significantly higher likelihood of group membership after Bonferroni correction (adjusted p < .05); blue bars indicate predictors associated with a significantly lower likelihood of group membership after Bonferroni correction.
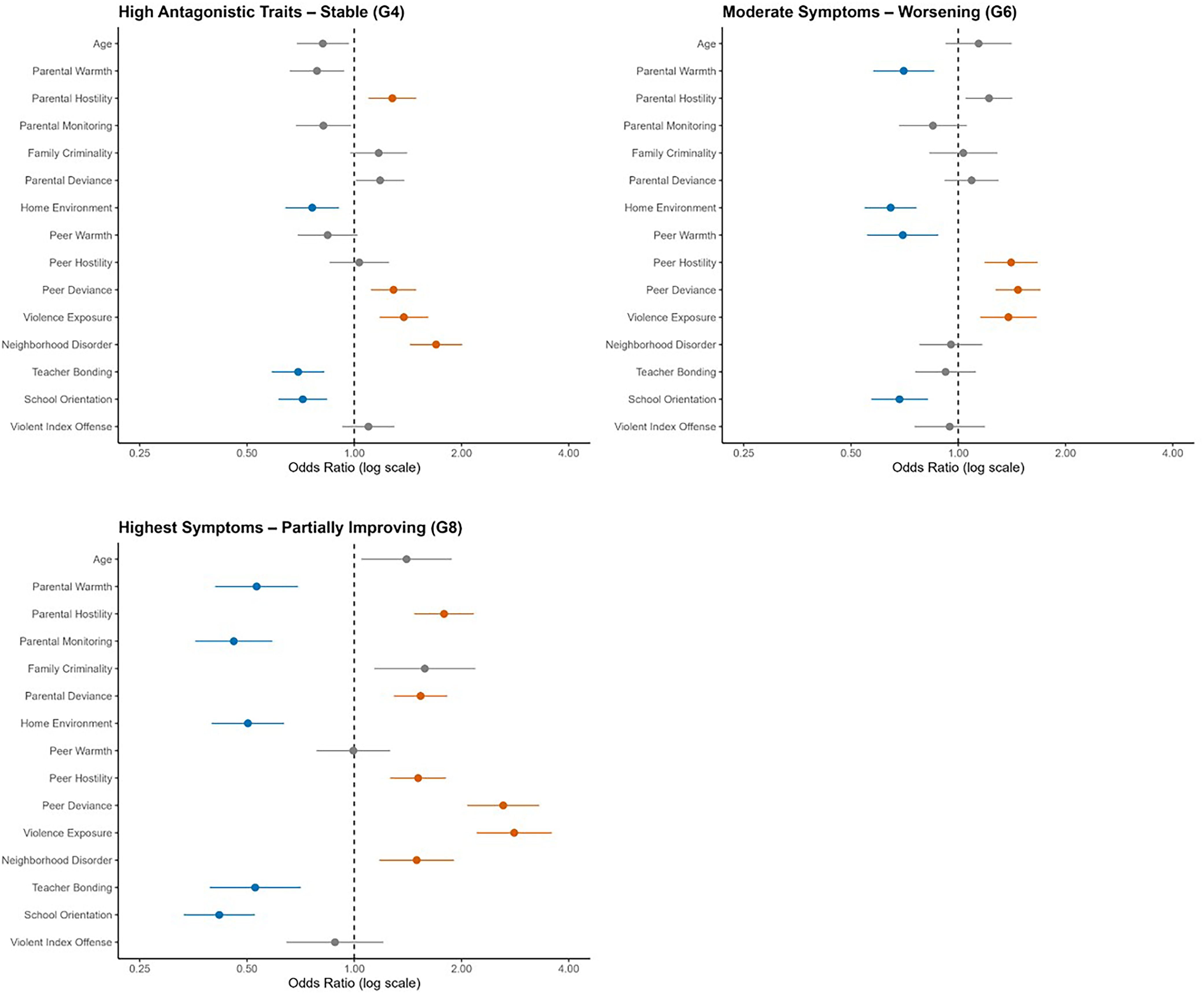
Several predictors were shared by two trajectory groups: neighborhood disorder and parental hostility predicted membership in the High Antagonistic Traits – Stable (G4) and Highest Symptoms – Partially Improving (G8) groups, whereas peer hostility predicted membership in the Moderate Symptoms – Worsening (G6) and Highest Symptoms – Partially Improving (G8) groups. Some protective factors were also partially overlapping across groups, with teacher bonding associated with the High Antagonistic Traits – Stable (G4) and Highest Symptoms – Partially Improving (G8) groups. Parental warmth was protective for the Moderate Symptoms – Worsening (G6) and Highest Symptoms – Partially Improving (G8) groups.
Two high-risk groups also had unique predictors. Membership in the Moderate Symptoms – Worsening (G6) group was uniquely associated with peer warmth as a protective factor. The Highest Symptoms – Partially Improving (G8) trajectory was the only group for which parental deviance emerged as a significant risk factor, and for which parental monitoring was an additional protective factor.
Discussion
This study aimed to enhance our understanding of the diverse behavioral health trajectories among system-involved youth. We identified eight distinct co-occurring trajectories of externalizing (antisocial behavior, harmful substance use, antagonistic traits) and internalizing (distress) problems, aligning with practitioner observations of the substantial heterogeneity in behavioral health needs among system-involved youth (Kapoor, Reference Kapoor, Peterson-Badali and Skilling2018). While most youth exhibited stable or decreasing externalizing and internalizing problems over time, some followed trajectories characterized by persistent or worsening problems. By incorporating four distinct indicators across externalizing and internalizing dimensions, this study provided a more comprehensive and nuanced assessment of youth behavioral health than studies examining one domain alone or those employing traditional categorical frameworks of psychopathology. Holistic and dimensional frameworks that consider internalizing problems may facilitate the identification of youth at the highest risk for continued legal system involvement and help differentiate between youth who present with similar externalizing behaviors. This level of specificity is critical for ensuring that appropriate resources are directed towards those most in need and interventions are addressing not only externalizing behaviors – which tend to be more visible and prioritized in legal contexts – but the fuller spectrum of behavioral health problems.
Compared with prior trajectory studies, which typically identify four to five unique trajectories, the larger number of groups identified in the current study likely reflects modeling four behavioral health indicators at once rather than one domain alone (e.g., Kjellstrand et al., Reference Kjellstrand, Yu and Eddy2019; Mulvey et al., Reference Mulvey, Steinberg, Piquero, Besana, Fagan, Schubert and Cauffman2010; Nivard et al., Reference Nivard, Lubke, Dolan, Evans, Pourcain, Munafò and Middeldorp2017). Even so, there are clear commonalities with the existing literature. For example, most youth showed low to moderate symptoms at baseline that stayed low or improved. We also identified a High Symptoms – Rapidly Improving (G7) group and a Moderate Symptoms – Worsening (G6) group, which echo patterns reported in prior work (Kjellstrand et al., Reference Kjellstrand, Yu and Eddy2019; Nivard et al., Reference Nivard, Lubke, Dolan, Evans, Pourcain, Munafò and Middeldorp2017). In contrast, we did not identify a “high-stable” group resembling the life-course persistent pathway, which has frequently emerged in previous studies (Kjellstrand et al., Reference Kjellstrand, Yu and Eddy2019; Mulvey et al., Reference Mulvey, Steinberg, Piquero, Besana, Fagan, Schubert and Cauffman2010; Nivard et al., Reference Nivard, Lubke, Dolan, Evans, Pourcain, Munafò and Middeldorp2017). This absence should be interpreted cautiously and may reflect limited power to detect a very small persistent class (e.g., 2.4% of the sample in Nivard et al., Reference Nivard, Lubke, Dolan, Evans, Pourcain, Munafò and Middeldorp2017).
Young adulthood rearrest outcomes
A central aim of this study was to identify not only how behavioral health trajectories differ across youth but also how these short-term adolescent trajectories relate to long-term legal outcomes in young adulthood. Rearrest is particularly important in this context because all youth in the sample were experiencing their first official arrest at baseline. Rearrest outcomes offer insight into which behavioral patterns signal risk for continued system involvement. Rearrest rates varied substantially across the eight trajectory groups, highlighting the differing long-term risks associated with distinct behavioral health trajectories. The Moderate Symptoms – Worsening (G6) and the Highest Symptoms – Partially Improving (G8) groups were the only two groups that exhibited worsening distress over time, and also exhibited the highest likelihood of rearrest. These findings align with research showing that co-escalating or chronic internalizing symptoms contribute meaningfully to long-term negative outcomes (Vergunst et al., Reference Vergunst, Commisso, Geoffroy, Orri, Bolanis, Vitaro, Tremblay and Côté2023), even when externalizing symptoms decline. Future research should explore potential mechanisms explaining how internalizing symptoms interact with system processes and supervision contexts to influence rearrest risk, such as reduced motivation to avoid detection of illegal behaviors or disengagement from helping services. These findings point to the importance of assessing and addressing internalizing problems like distress in system-involved youth.
However, increasing distress was not the only marker of risk. The High Antagonistic Traits – Stable (G4) group also had a high rearrest rate – third overall – despite relatively low levels of antisocial behavior and harmful substance use. The elevated rearrest outcomes among this group suggest that antagonistic traits may be a significant driver of long-term system involvement, even when antisocial behavior and substance use problems are not immediately prominent. These findings align with meta-analytic evidence showing that antagonistic traits are associated with more severe and persistent behavioral risk and often remain unchanged unless addressed directly (Frick & White, 2008; Perlstein et al., Reference Perlstein, Fair, Hong and Waller2023). Although youth with antagonistic traits may respond to behavioral interventions in terms of reduction in symptoms, they tend to begin and end treatment with more pronounced symptoms than their peers, and the traits themselves typically remain stable unless specifically targeted.
Interventions that address the specific socioemotional features associated with antagonistic traits may be especially important for these groups. Evidence-based strategies that include emotion-recognition and empathy-training modules – particularly those embedded within parenting-focused programs – have shown promise in reducing antagonistic traits when implemented under the right conditions (Perlstein et al., Reference Perlstein, Fair, Hong and Waller2023). Such strategies may foster improvements in emotional responsiveness and social connectedness, providing a crucial supplement to traditional behavior management approaches. Integrating antagonistic-specific components into legal system interventions could represent a key opportunity to reduce recidivism risk among youth with high antagonistic traits.
Contextual factors
Understanding how environmental contexts influence youth development is a core tenet of developmental theory, which emphasizes that behavioral outcomes are shaped by the dynamic interplay between youth and the multiple contexts they inhabit. Informed by the social-ecological model (Bronfenbrenner, Reference Bronfenbrenner1977), we investigated how baseline family, peer, school, and neighborhood contextual factors predicted trajectory group membership, focusing here on the three highest-risk groups: High Antagonistic Traits – Stable (G4), Moderate Symptoms – Worsening (G6), and Highest Symptoms – Partially Improving (G8). Four antecedents predicted membership in the three highest-risk groups – peer deviance and violence exposure (risk factors), and positive home environment and school orientation (protective factors) – highlighting core processes relevant across multiple pathways of risk.
Peer deviance and violence exposure are well-established predictors of future legal system involvement, operating through mechanisms such as behavioral modeling, social reinforcement, emotional dysregulation(Chung & Steinberg, Reference Chung and Steinberg2006; Low & Espelage, Reference Low and Espelage2014), and rejection from prosocial peers that can contribute to internalizing distress (Dishion & Tipsord, Reference Dishion and Tipsord2011). Consistent with prior work (Estrada & Baskin-Sommers, Reference Estrada and Baskin-Sommers2024; Estrada et al., Reference Estrada, Simmons and Baskin-Sommers2023; Moylan et al., Reference Moylan, Herrenkohl, Sousa, Tajima, Herrenkohl and Russo2010; Taylor et al., Reference Taylor, Grant, Zulauf, Fowler, Meyerson and Irsheid2018, the current findings suggest that violence exposure not only exacerbates antisocial behavior but also contributes to anxiety and depression, complicating intervention efforts. Addressing peer deviance and violence exposure early could help mitigate their long-term impacts on behavioral health and legal system involvement. Multisystemic and trauma-focused interventions are especially promising, particularly when they target both individual coping and the broader peer, family, and neighborhood environments that confer risk, thereby reducing violent behavior, internalizing symptoms, and recidivism (Baskin-Sommers et al., Reference Baskin-Sommers, Chang, Estrada and Chan2022).
School orientation and positive home environment emerged as robust buffers against membership in high-risk groups. Consistent with prior research, school engagement appears to reduce delinquency risk by fostering a sense of purpose, structure, and institutional connection (Monahan et al., Reference Monahan, VanDerhei, Bechtold and Cauffman2014), while supportive home environments promote emotional stability and buffer youth from external stressors (Chung & Steinberg, Reference Chung and Steinberg2006; Ryan et al., Reference Ryan, Williams and Courtney2013). Notably, these protective influences were evident even in a high-risk, system-involved sample, suggesting that positive school and family contexts can provide meaningful resilience even in the presence of other adversities. Future research should investigate these protective factors further, especially given their potential as accessible targets for prevention and intervention in system-involved youth.
Three predictors were uniquely associated with membership in a single high-risk trajectory group. Peer warmth was uniquely protective for the Moderate Symptoms – Worsening (G6) group, whose increasing externalizing and internalizing symptoms suggest vulnerability to escalating interpersonal strain. Developmental research shows that adolescents exposed to peer hostility or rejection are at elevated risk for both behavioral and emotional problems, as social exclusion erodes support, increases conflict, and heightens emotional distress (Cheek et al., Reference Cheek, Reiter-Lavery and Goldston2020; McDougall et al., Reference McDougall, Hymel, Vaillancourt and Mercer2001; Roach, Reference Roach2018). Dishion and Tipsord (Reference Dishion and Tipsord2011) further emphasize that peer rejection amplifies risk by increasing youth’s susceptibility to coercive interactions and deviant peer processes, which can contribute to both antisocial behavior and internalizing symptoms. Within this context, supportive peer relationships may be particularly impactful for this group by buffering the effects of hostility and negative peer influence.
In the Highest Symptoms – Partially Improving (G8) group, two family factors were uniquely associated with trajectory group membership: higher levels of parental deviance and lower levels of parental monitoring. This pattern is consistent with evidence that family processes are especially influential early in adolescence, when parental behavior shapes youths’ exposure to risk, coping strategies, and opportunities for supervision (Hoeve et al., Reference Hoeve, Dubas, Eichelsheim, Van der Laan, Smeenk and Gerris2009). Parental deviance may exacerbate vulnerability by modeling antisocial norms and reducing structure, whereas consistent monitoring provides a stabilizing scaffold that supports early behavioral improvement. Given this profile, family-focused intervention models, such as Multisystemic Therapy and Functional Family Therapy, may be particularly well suited for youth in this group, as they directly target parental behavior, monitoring practices, and broader family functioning (Baskin-Sommers et al., Reference Baskin-Sommers, Chang, Estrada and Chan2022).
Together, these findings suggest that while many contextual influences cut across multiple high-risk trajectories, certain peer and family processes may carry group-specific significance that warrants tailored intervention strategies. Consistent with developmental theory, our findings reinforce the importance of multi-contextual influences in understanding behavioral health development. Our results demonstrate that risk and protective factors across family, peer, school, and neighborhood domains significantly predicted membership in the highest-risk behavioral health trajectory groups. These patterns highlight the need for individualized interventions that are both developmentally informed and contextually responsive – approaches that address not only individual symptoms but also the ecological systems that shape youth pathways over time.
Trajectories of resilience
Though entering the legal system with behavioral health problems is often assumed to signal a heightened risk for continued system involvement, our findings challenge this notion. The majority of youth in our sample followed trajectories characterized by low and/or declining levels of externalizing and internalizing problems. This is noteworthy given that all participants had been arrested at baseline, an event that has the potential to disrupt developmental progress, stigmatize youth, and limit access to protective resources (Tolliver et al., Reference Tolliver, Abrams, Biely, Meza, Schickedanz, Guerrero, Jackson, Bath, Heard-Garris, Dudovitz and Barnert2023). That many youth maintained or returned to low symptom trajectories suggests that system contact does not inevitably lead to poor behavioral health outcomes or long-term system entrenchment.
Importantly, even among youth who entered the system with substantial behavioral health problems, not all remained on high-risk pathways. The High Symptoms – Rapidly Improving (G7) group offers the most salient illustration. These youth began with elevated behavioral health problems and higher exposure to peer deviance and violence, yet showed marked improvement and comparatively low rearrest in young adulthood. These patterns align with developmental theory, which emphasizes the plasticity of adolescence and the potential for behavioral and emotional adaptation following adversity (Masten & Cicchetti, Reference Masten and Cicchetti2010; Steinberg, Reference Steinberg2014). Resilience literature emphasizes that positive change is often facilitated by the presence of protective factors, such as supportive relationships, opportunities for autonomy, and skill-building environments (Zimmer-Gembeck & Skinner, Reference Zimmer-Gembeck, Skinner and Cicchetti2016). Identifying the factors that most strongly promote resilience among system-involved youth is a critical direction for future research, with the goal of informing interventions that both mitigate risk and build on strengths to support sustained positive development.
Implications for assessment
The diverse behavioral health trajectories observed in this study suggest that system-involved youth may not be optimally supported by a one-size-fits-all treatment approach. Rather, system-involved youth need tailored treatment strategies that assess and target both the severity and co-occurrence of externalizing and internalizing symptoms. As the juvenile legal system aims to expand and strengthen its rehabilitative approaches, integrating behavioral health considerations into risk assessment models has become increasingly critical (Taxman, Reference Taxman2014). Our findings highlight the value of adopting a dimensional conceptualization of behavioral health, consistent with frameworks such as HiTOP, for assessment in system-involved youth. The findings from this study support the movement toward assessment and rehabilitative approaches that consider both externalizing and internalizing symptoms, as well as the contexts in which they develop, when evaluating recidivism risk and intervention strategies. Policymakers and practitioners have increasingly sought to implement evidence-based frameworks, such as the risk-needs-responsivity (RNR) assessment model (Brogan et al., Reference Brogan, Haney-Caron, NeMoyer and DeMatteo2015), to guide these efforts.
The RNR model offers a promising assessment framework for matching interventions to individual youth. It emphasizes the importance of directing resources toward youth at the highest risk of recidivism (the risk principle) and targeting dynamic criminogenic needs (the needs principle) that are changeable and directly influence recidivism (Andrews & Bonta, Reference Andrews and Bonta2010). Externalizing behavioral health problems, such as antisocial behavior or harmful substance use, are classified as criminogenic needs because they often involve illegal behaviors and directly contribute to system involvement (Kapoor, Reference Kapoor, Peterson-Badali and Skilling2018). In contrast, internalizing problems like distress are considered specific responsivity factors – while they do not directly constitute criminal behavior, they can exacerbate externalizing behaviors or undermine intervention effectiveness (the responsivity principle) if left unaddressed (Kapoor, Reference Kapoor, Peterson-Badali and Skilling2018; Taxman & Caudy, Reference Taxman and Caudy2015).
In this study, youth with worsening internalizing and externalizing problems were at the highest risk for rearrest, reinforcing the importance of integrating both criminogenic needs and responsivity factors when evaluating one’s long-term risk for continued system involvement. These findings highlight the need for a more nuanced and dynamic approach to intervention in which internalizing problems are recognized as “risk amplifiers.” Moreover, the finding that specific contextual predictors differentiated high-risk trajectory groups reinforces their developmental relevance and supports integrating such factors into assessment and intervention planning. Moving forward, incorporating comprehensive behavioral health and contextual measures alongside traditional risk assessments may allow for more precise identification of youth most at risk for continued system involvement.
Limitations
Before concluding, several limitations of the analytic approach must be acknowledged. The exploratory nature of group-based multi-trajectory modeling introduces the potential for overfitting, as the trajectory groups identified are statistical abstractions that may not fully represent real-world patterns. Overfitting refers to models that capture noise in the data rather than true underlying patterns, which can limit generalizability (Nagin et al., Reference Nagin, Jones, Passos and Tremblay2018). This limitation was mitigated using several robust model fit criteria, including the Lo-Mendell-Rubin test, entropy, and average posterior probabilities. Another limitation of the analytic approach is that trajectories were modeled by study time point rather than chronological age. Modeling by age would allow for more direct developmental interpretation; however, the accelerated cohort design of the Crossroads Study poses challenges for age-based modeling due to increased missing data. Furthermore, our goal was to examine behavioral health development specifically in the years following a youth’s first arrest – an event that marks a key opportunity for system intervention and may catalyze developmental change.
Several sample-and data-related limitations should be noted. Because the sample includes only system-involved male youth, findings may not generalize to system-involved female youth. As female youth constitute a larger percentage of system-involved youth now than ever before, there is a great need for research investigating their development and behavioral health needs (Ehrmann et al., Reference Ehrmann, Hyland and Puzzanchera2019). Overall missingness was modest, but Black youth had somewhat higher odds of missingness compared to White youth. No other missingness differences were observed on the basis of race, ethnicity, or age. Additionally, some contextual predictors demonstrated strong positive skew or borderline reliability indices, which may reflect potential for measurement error and reduced power to detect effects (see Supplemental Table 5). While multiple regression is robust to non-normal predictors (Williams et al., Reference Williams, Grajales and Kurkiewicz2013), limited variability nonetheless reduces power to detect effects. Finally, because we considered only the contextual factors assessed at baseline (i.e., immediately after the first arrest), our ability to understand how changes in developmental context coincide with behavioral health trajectories was limited. Future research would benefit from longitudinal measurement of both symptoms and contextual influences to better model dynamic risk processes.
Conclusion
Altogether, this study provided a deeper understanding of the diverse behavioral health trajectories among system-involved youth, demonstrating that where youth start is not necessarily where they end. System-involved youth follow varied developmental pathways, with some exhibiting significant improvement despite early adversities, while others remain on high-risk trajectories marked by persistent externalizing and internalizing problems. These findings reinforce the need for individualized, developmentally informed assessment and strategies tailored to youths’ specific risks and needs. Implementing strategies that address both externalizing and internalizing problems – alongside the contextual risk and protective factors that shape them – can provide a more comprehensive foundation for promoting long-term well-being among system-involved youth.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0954579426101229.
Data availability statement
In accordance with the Transparency and Openness Promotion (TOP) Guidelines, we report that: (1) the data used in this study are from the Crossroads Study and are available to qualified researchers upon request and approval from the study team; (2) the analytic code used in this study are available upon request and approval from the corresponding author; (3) study measures and analytic procedures are described in the article and supplemental materials.
Acknowledgments
We are grateful to the Crossroads Study participants and the many individuals responsible for the data collection and preparation.
Funding statement
The Crossroads Study is supported by funding from the John D. and Catherine T. MacArthur Foundation, the Office of Juvenile Justice and Delinquency Prevention, the National Institute of Justice, the County of Orange, and the Fudge Family Foundation.
Competing interests
The authors declare no competing interests.
Pre-registration statement
This study was not pre-registered. The analytic approach was exploratory and data-driven.
AI statement
No artificial intelligence tools were used to create the intellectual content of this article.




 Open access
Open access