


Within Public Health Nutrition targeting populations with much to gain from dietary improvement is a priority(Reference Aagaard-Hansen, Hindhede and Terkildsen Maindal1). In recent years there has been increasing focus on the preconception population. Preconception paternal and maternal risk factors such as obesity and unhealthy diet affect the metabolic and cardiovascular health of their offspring later in life(Reference Stephenson, Heslehurst and Hall2,Reference Eberle, Kirchner and Herden3) . These insights highlight the importance of diet and dietary behaviour in the years before parenthood, and with the convincing Lancet issue on preconception health Before the beginning (Reference Stephenson, Heslehurst and Hall2,Reference Barker, Dombrowski and Colbourn4) and Nature’s paper Adolescence and the next generation unpacking the importance of the preconception period, a new era on when to intervene started. Still, the question of timing is not straightforward. There is continuous discussion on what the preconception period is, spanning from fertile age to the time when couples plan to have a child(Reference Stephenson, Heslehurst and Hall2,Reference Hill, Hall and Skouteris5) .
Barker et al. (Reference Barker, Dombrowski and Colbourn4) suggested that there is a need for tailored interventions to different phases, depending on target group age and intention for parenthood. For adults with no immediate intention to become pregnant, interventions should aim to raise public awareness of preconception health and signpost to available evidence-based information resources. Barker and co-workers suggest web-based information platforms as suitable for this aim(Reference Barker, Dombrowski and Colbourn4). Digital interventions, like apps and websites, are often used within the Public Health Nutrition field and described as both feasible(Reference Steinberg, Kay and Svetkey6,Reference Melo, Santo and Mas Clavel7) and cost-effective(Reference Chen, Perez-Cueto and Giboreau8).
There are clear shortcomings in young adult’s diet(Reference Barker, Dombrowski and Colbourn4,Reference Valen, Engeset and Øverby9,Reference Parajuli and Prangthip10) and aiming to address the critical period raised above, we initiated an intervention study in 2018 – the PREPARED study – to improve diet in a broad preconception population (age 20–35 years)(Reference Øverby, Medin and Valen11), with a specific focus to recruit a fair share of men and lower socio-economic groups. During the project period we experienced difficulties and challenges in recruitment, retention, who we reached and unclear effects, as others have experienced before us(Reference Gul and Ali12,Reference Rodríguez-Torres, González-Pérez and Díaz-Pérez13) . These recurrent challenges need to be highlighted and discussed within the field of Public Health Nutrition, hopefully in this case to advance the way we work with the preconception population, the way we work to improve population diet and possibly to identify new ways of developing and evaluating interventions.
This review describes several digital interventions addressing preconception diet and discusses challenges in targeting this population with digital designs and in evaluation of intervention effect.
What do we know about digital dietary interventions targeting the preconception population?
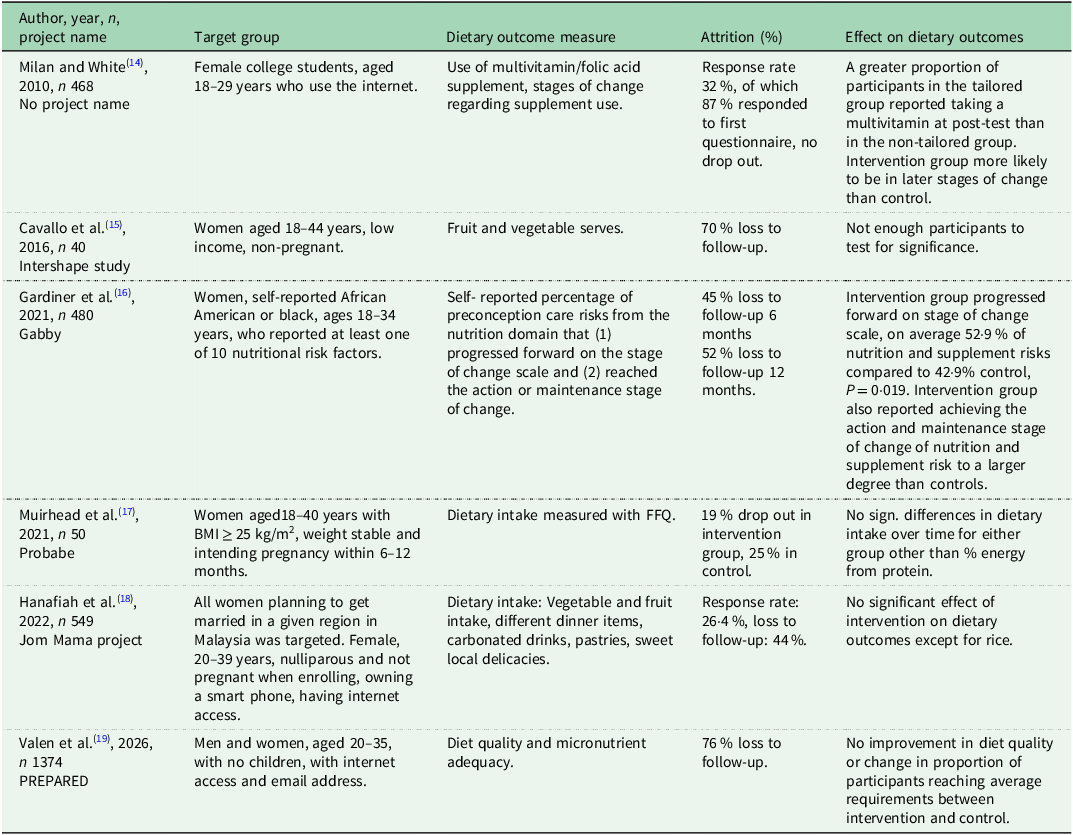
In the current review, we draw upon six digital interventions targeting diet the preconception population (Table 1). Five of these were identified though a review from O’Connor et al. from 2022(Reference O’Connor, Willcox and de Jersey20) targeting preconception phases but excluding early pregnancy and in vitro fertilisation treatment. The main aims of the interventions were to improve either weight gain, diet or physical activity, using different digital approaches with different dietary outcomes. This review focuses on dietary outcomes. Since that time, our study, PREPARED, has published results from a digital intervention aimed at promoting a healthy preconception diet in young people with no children(Reference Øverby, Medin and Valen11,Reference Valen, Wills and Medin19) . Below we present, for these six studies, the target population, type of digital intervention and participant engagement, effects and methodological issues and further discuss ways forward for this field.
Overview of digital interventions targeting preconception population with dietary outcomes

The preconception phase, the time before conception can be defined in many ways and includes both the female and male population(Reference Barker, Dombrowski and Colbourn4,Reference Hill, Hall and Skouteris5) .
Most studies to date have focused on women only, with varying age groups and variation in whether they had an intention to conceive or not. Cavallo et al. recruited low-income women aged 18–44 years from family planning clinics in USA(Reference Cavallo, Sisneros and Ronay15). Gardiner et al. recruited African American or Black women 18–34 years in USA and reported on those with at least one dietary risk factor(Reference Gardiner, Bickmore and Yinusa-Nyahkoon16). Hanafiah et al. recruited all nullipara women planning to get married in a specific region in Malysia aged 20–39(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18). Milan and White recruited female college students aged 18–29 years in USA(Reference Milan and White14), Muirhead et al. recruited female 18–40 years with BMI above 25 kg/m2 from clinical settings in Australia intending to become pregnant within 6–12 months(Reference Muirhead, Kizirian and Lal17).
Our study, PREPARED, is to the best of our knowledge, the first preconception dietary intervention to take the public health approach and target the general preconception population, and to approach both men and women(Reference Valen, Wills and Medin19). The field has had a large focus on women, however, aligned with increasing knowledge of the male contribution to pregnancy and offspring health(Reference Patton, Olsson and Skirbekk21,Reference Soubry22) , we wanted to include men. The preconception phase, when including the whole fertile range, is quite long (∼18–45 years for women and longer for men). The age range in our study was decided upon using two principles: (1) broad reach and (2) ‘do no harm’. With this broad approach, we first wanted to include 18–45-year-olds as this roughly corresponds to fertile age(Reference Øverby, Medin and Valen11). However, most 18–19-year-olds still attend public schools and live at home in Norway, and as we wanted to approach the young adults themselves (not their parents), we chose the lower age limit to be 20 years. The upper age limit was discussed with several people from the target population and with a professor in philosophy to avoid harm through potential stigma of not having children at age above 35 years. We concluded that being approached with a study focusing on your first child might seem difficult if you do not yet have, but truly want, children. We, therefore, chose 20–35 years of age as the most appropriate age group to target. Still, this age span includes participants in potentially very different phases of life. We also recruited participants individually, not as couples.
The type of digital interventions used, how it was developed and intervention group’s engagement with the resource
There has been mounting interest in digital interventions within public health as they seem easy to conduct and may have broad reach. Digital interventions might be, however, time-consuming to develop(Reference Bradbury, Watts and Arden-Close23) and recent research points at difficulties in engaging targeted populations in the resources(Reference Smith, Ward and Lambe24). The digital elements in the dietary preconception studies to date vary, as does the reported engagement with the resources during the intervention. Cavallo et al. used a blended approach in a web-based intervention with weekly email self-monitoring questionnaires and group sessions(Reference Cavallo, Sisneros and Ronay15). The intervention was a digital adaptation of a Weight-Wise programme which includes goal setting, self-monitoring, feedback and education to promote dietary and physical activity. It also included group sessions and a Facebook fan page where study staff made weekly comments to encourage participation. We have not been able to identify a description of how it was developed. The authors reported declines in activity in the self-monitoring questionnaire over time and a high loss to follow-up (70 %)(Reference Cavallo, Sisneros and Ronay15). Their qualitative analysis suggested that this group live busy lives and have work schedules that make behaviour change difficult(Reference Cavallo, Sisneros and Ronay15).
Gardiner et al.’s digital intervention Gabby was an online conversational agent(Reference Gardiner, Bickmore and Yinusa-Nyahkoon16). Based on risks identified from participant assessment, Gabby compiles a Health to do list, from which women can choose to discuss a topic that Gabby tracks over time. Gabby addresses issues like adequate intake of fruit and vegetables, unhealthy foods, how to uphold a healthy weight and more. Over the 12 months intervention Gabby tracks progress and provides feedback on actions taken. There is no description of how this was developed. The authors found that additional logins yielded better rates of achieving goals. They also report that 83 % logged in at least once, and that median duration of attendance in the sessions was quite high (14 min). They do not know the specific amount om minutes the women engaged in the nutrition and supplement domain(Reference Gardiner, Bickmore and Yinusa-Nyahkoon16).
Hanafiah et al.’s approach was also blended, and they used an app, phone calls and face- to-face approaches(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18). The intervention included six appointments with health promoters which encouraged healthy lifestyle changes for married couples. In addition, the couples had continuous access to a tailored mobile app. The app included a function with lifestyle challenges from which the couples could select, such as healthy foods, and then access to information on healthy lifestyles. All women in the intervention group downloaded the app. The app was developed based on extensive preparatory work, including engagement with stakeholders and young couples, identifying barriers and needs(Reference Sharif, Hanson and Chong25,Reference Norris, Ho and Rashed26) .
Milan and White used a study website and emails(Reference Milan and White14). During the 2–5 weeks the intervention lasted, the tailored intervention group got email messages regarding folic acid supplementation tailored to their stage of change for vitamin use. Those in the non-tailored group got more general information. The email messages included links to the website with relevant information. They did not report on engagement. Neither did they describe how the intervention was developed.
Muirhead et al. used a blended approach with face-to-face consultations, digital consultations and online forums(Reference Muirhead, Kizirian and Lal17). More than 80 % of the intervention group said the support they received was excellent. Muirhead et al.’s intervention was a meal replacement intervention with digital consultations, including an online forum support system not described in detail.
The PREPARED project included a website and regular emails. The PREPARED website included recipes of healthy dishes, articles and short texts and videos about topics worth knowing to improve or maintain a healthy diet. The articles included information about basic food items in a healthy diet, useful equipment for cooking and how good habits make everyday life easier, asserting that every meal counts(Reference Øverby, Medin and Valen11). The participants received regular email messages which were designed to be inspirational and educational at the same time. Participants had access to the digital content for 6 months and received weekly motivational emails during this period, 26 in total, leading directly to a new topic at the website. The intervention group used the digital resource for an average of two minutes every time they entered. We do not have data on how many times they entered the website. We evaluated how the intervention was experienced in a separate group than those included in the PREPARED study. Nine young adults were recruited to use the intervention for 3 months and were provided with information emails at double speed (twice weekly). The participants were interviewed afterwards and reported the intervention to be both inspiring and novel. They also thought the intervention made it easier to make healthy choices and provided a new justification for healthy eating. They specifically highlighted that it was refreshing that diet in this intervention was not only related to obesity and weight(Reference Øverby, Kr and ER27). We do not have qualitative data from the PREPARED participants.
The intervention PREPARED was informed by but not co-created with the target population. Before we started developing the PREPARED intervention, we explored young people’s thoughts and knowledge about preconception diet. We wanted to identify the needs of young people in general, and specifically male needs and needs of those from lower socio-economic background. We conducted short interviews with 33 young people(Reference Valen, Øverby and Hardy-Johnson28). To get information from the general preconception population and people who seldom participate in research, we recruited participants at different shopping malls(Reference Valen, Øverby and Hardy-Johnson28) for very short interviews. We ended up with more male than female participants and representation from a varied socio-economic background, as intended. In summary, findings from these interviews suggest that adults within the fertile age range are not intrinsically motivated to eat healthily. If they do so, it is because eating healthily is relevant to other goals like getting fit or looking good. The general impression was that the people interviewed did not have previous knowledge about the relevance of preconception, nor the importance of preconception health and nutrition for health in the next generation(Reference Valen, Øverby and Hardy-Johnson28). Based on these findings we developed a digital dietary intervention conveying the importance of a healthy diet for the individual’s health now, later in life and in the next generation. We applied self-determination theory to guide the development of promotional messages, videos and pictures, aiming to meet participants’ need for autonomy, competence and relatedness through the intervention content(Reference Øverby, Medin and Valen11). We were attentive to the fact that it should be relevant for men, and also that the texts and messages should be easy for everyone to understand.
Effects of the different digital interventions on dietary outcomes
Cavallo et al. did not test for significance due to low numbers of participants, however reported positive changes in fruit and vegetable intake(Reference Cavallo, Sisneros and Ronay15). Muirhead et al. did not find changes in diet, other than proportion of energy from protein(Reference Muirhead, Kizirian and Lal17). The PREPARED study did not find effect of the dietary intervention on the primary outcome diet quality, measured as a diet quality score(Reference Valen, Wills and Medin19). Hanafiah et al. did not find significant improvement in fruit and vegetables intake or any part of dietary aspects apart from rice consumption(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18). Gardiner et al. reported at 6 months that more women in the intervention group compared to control moved forward on the stage of change scale of the nutrition and supplement risks flagged, but this was not sustained at 12 months(Reference Gardiner, Bickmore and Yinusa-Nyahkoon16). Milan and White reported increased use of folic acid supplements in the intervention group, that intervention participants were more likely to be in later stages of change than controls, had increased self-efficacy and clearer perception of the importance of multivitamin use compared to controls(Reference Milan and White14). Summarising, four of the six studies did not report relevant effect, while two reported changes in motivation, in supplement use and dietary risk scores.
Methodological issues
Of the eligible participants in Cavallo et al.’s study (n 251), 170 were initially interested in participation, but after being contacted only 40 completed the baseline questionnaire and comprised the study sample (no statistical testing due to low numbers). Gardiner et al. recruited 528 subjects to the full randomised trial, with 480 flagged with at least one risk factor related to nutrition (eligible) resulting in 240 in both intervention and control arms. Complete outcome data was obtained from 116 intervention and 146 controls at 6 months and 105 intervention and 124 controls at 12 months. Hanafiah et al. approached 5053 women of which 2075 were eligible for the study. Of these only 548 were randomised, equal to a response rate of 26·4 %. Of these 305 completed the survey. The main loss to follow-up was pregnancy occurring. In Muirhead et al.’s study 132 were assessed for eligibility and 50 were randomised. There was a 75–81 % retention rate in completion of intervention in the two groups. A limitation with this study was that most of those recruited were highly educated, more than 85 %. Milan and White recruited university students, and from the 1450 women invited, 32 % expressed interest in the study. In total 408 responded to the first questionnaire, and 99 % completed the post-test survey.
In PREPARED, only 745 out of the recruited 1347 completed the self-administered digital baseline 24-hour recall and were subsequently randomised to either a control group or an intervention group, which was provided access to the digital intervention. Retention rate throughout the intervention was extremely low. Only 87 (23 %) from the intervention group and 99 (27 %) from the control group responded to questionnaires after 6 months, with slightly higher response rate at 12 months (n 122 (33 %) and n 128 (35 %) in intervention and control group, respectively). There were no differences between those included and lost to follow-up, except that those who were lost had somewhat lower education. It should be noted that the disappointingly low response rates directly following the intervention do not necessarily mean loss to follow-up over time, as we will keep sending invitations to yearly follow-ups with a short dietary screener and ask for permission to access birth data when they report having their first child.
How do we take the field forward?
In general, there seem to be limited effects from the digital interventions as presented above(Reference Milan and White14–Reference Valen, Wills and Medin19). The two that report some positive outcomes are approaching a risk-group (dietary risks) or have a one-message-intervention (supplements). There might be several reasons for these results, and they might be study specific. The findings do not necessarily show that digital interventions in the preconception phase do not work as there are methodological issues that hamper the findings. Below we discuss these, the target population, how an intervention is developed and recruitment. These are important issues that should be discussed before deciding to do more of the same.
Need to narrow the target population
The Lancet series on preconception health(Reference Stephenson, Heslehurst and Hall2), describe three different perspectives on preconception. The biological perspective, describing the days or week before conception, the individual perspective describing the time when the intention to conceive is present, and the public health perspective, including months or years before conception where risk factors can be addressed, including adolescence(Reference Stephenson, Heslehurst and Hall2). Following this series, Hill and co-workers have argued that there is no specific definition of the preconception population(Reference Hill, Hall and Skouteris5). In their paper elaborating on the preconception concept, they review what defines such population, describing four different preconception populations, where intentions to conceive and whether the population is sexually active or not are part of the definition. The first group, Intentional Preconception population, includes reproductive men and women, who are sexually active, the partner is not pregnant yet, however, they have a conscious decision to conceive. Muirhead’ s study(Reference Muirhead, Kizirian and Lal17) and Cavallo et al.’s study(Reference Cavallo, Sisneros and Ronay15) align with this definition. The second group, Potential Preconception population, resembles number one, but there is no decision to conceive. Hanafiah et al.’ s study(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18) is in this group targeting married couples. The third group is the Public Health group, being similar to the second group, however, not sexually active. The last group, the Lifecourse group, recognises the importance of preconception perspectives all through the lifecourse and includes adolescents and those pregnant. Hill and co-workers argue that such definitions will help researchers and policy makers in developing interventions and policy. Our PREPARED study(Reference Valen, Wills and Medin19) and Gardiner et al.’s(Reference Gardiner, Bickmore and Yinusa-Nyahkoon16) study are not easy to define in line with Hill’s definitions, as they focus on the reproductive age within a given age limit, were limited to a non-pregnant population and had no assessment of whether participants were planning children or were sexually active. It is difficult to use the definition in retrospect on the current studies, but this might be an important way forward, at least to specify the group. Our experience is that our target population represented a very wide age group and also a very varied group in general which makes it more difficult to meet individual needs of knowledge and skills(Reference Valen, Øverby and Hardy-Johnson28). Hanafiah et al. suggest that their results probably reflect that people preparing to start a family are either not motivated sufficiently by an intervention(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18,Reference Sharif, Hanson and Chong25) or simply not accessible, due to busy work schedules or to other priorities. The authors suggest that other phases of the lifecourse, perhaps before marriage, would be better. We do not know from the present studies, which phases are superior for intervention. Hill et al.’s suggestions to narrow the groups in relation to planning to have children seem relevant(Reference Hill, Hall and Skouteris5). Our own study points at the difficulties in reaching a wide age group with relevant messages(Reference Valen, Wills and Medin19), implying a need for a narrower age group when targeting individuals.
Need to find ways to involve the target population
Generally, there is an increasing understanding of the need to include users’ perspectives for interventions to be relevant to the target group(Reference Khubchandani, England-Kennedy and Wiblishauser29). Two of the studies presented describe how the intervention was developed with extensive user and stakeholder involvement and use of theory(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18,Reference Valen, Wills and Medin19,Reference Sharif, Hanson and Chong25,Reference Valen, Øverby and Hardy-Johnson28) . Both find no effects of their interventions. The other studies did not present how the intervention was developed.
The authors from the Jom Mama project report that it was clearly challenging to engage this group and ensure active participation in behaviour change in which they conclude that the intervention is unlikely to proceed to scale up(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18,Reference Sharif, Hanson and Chong25) . The authors suggest that the low involvement probably reflects that individuals preparing to start a family may not be sufficiently motivated or simply not accessible, due to busy work schedules or to other priorities. Most of the included studies report limited engagement with the digital resources. A recent overview of challenges with digital public health interventions, divided the challenges in technological and non-technological(Reference Iyamu, Gómez-Ramírez and Xu30). One of the non-technological issues was related to equity in using digital interventions. Digital interventions might disproportionately benefit already privileged groups in society and exclude marginalised populations. Several of the included interventions reached high socio-economic groups(Reference Muirhead, Kizirian and Lal17,Reference Valen, Wills and Medin19) and groups with good habits from the beginning, with less to gain from the intervention(Reference Sharif, Hanson and Chong25).
Need to improve recruitment and keeping participants in the trial
It is notoriously difficult to recruit young people to participate in research(Reference Jong, Stevenson and Winpenny31). Of the studies presented above, Hanafiah et al. struggled with recruitment(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18), as did Milan and White(Reference Milan and White14), Cavallo et al. (Reference Cavallo, Sisneros and Ronay15) and the PREPARED study(Reference Valen, Wills and Medin19). Muirhead et al. mostly recruited highly educated participants(Reference Muirhead, Kizirian and Lal17). In our PREPARED project we strove to identify the relevant settings to approach this widely defined group, as there is no preconception primary healthcare service in Norway, and no natural arena where all attends. Hanafiah et al. recruited from marriage registries, Cavallo et al. recruited from family clinical settings, Milan and White from universities, however these ways were not very successful either. This is not a new lesson learned, but a reoccurring issue in health and nutrition research threatening both the internal and the external validity of research findings(Reference Gul and Ali12). It is also a major reason for trial termination(Reference Desai32).
Hanafiah et al. note that despite considerable effort it was difficult to recruit(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18). The authors conducted a comprehensive process evaluation with focus group interviews and measurements of app use(Reference Sharif, Hanson and Chong25). It suggests that the reason for low recruitment might have been due to external factors like recruitment site, trouble with the app and length of the intervention. They state that those participating deemed themselves as healthy without need for health services, which may lead to lower level of completion of the intervention activities. Cavallo et al. recommend that future interventions targeting populations with high attrition develop a priori strategies for collecting data from non-returners to identify factors for non-participation(Reference Cavallo, Sisneros and Ronay15).
In the PREPARED study we tested recruitment through postal mail after having Statistics Norway draw a national representative sample of the selected age group. We managed to recruit 22 participants following invitation sent to 1000 recipients. We therefore left this strategy and recruited through social media, which had been successful in other groups(Reference Helle, Hillesund and Wills33). From recruitment through social media, 1347 agreed to participate, but attrition rate was high.
From our previous experience with mothers of infants, recruiting through social media has been successful(Reference Helle, Hillesund and Wills33), however, it turned out difficult to reach the number of participants planned for in the preconception group. It is possible that the age group 20–35 years are not interested in research participation, possibly due to a lack of engagement with the topic or insufficient awareness of its relevance(Reference Valen, Øverby and Hardy-Johnson28,Reference Salvesen, Valen and Wills34) . It might also be that the envisioned long-term follow-up and time-consuming dietary assessment methods were too labour intensive for the participants. A main reason for low recruitment, reported by several of the presented studies, may be that there is a general decline in participation in research(Reference Brintnall-Karabelas, Sung and Cadman35–Reference Galea and Tracy38). Reasons stated for declining participation seem to be inconvenience, time constraints, financial reasons or protocol issues(Reference Rodríguez-Torres, González-Pérez and Díaz-Pérez13,Reference Brintnall-Karabelas, Sung and Cadman35) , which may well be reasons why it was difficult to recruit from the preconception population in this study.
Attrition was very high in our study, as in Hanafiah et al. and others(Reference Cavallo, Sisneros and Ronay15,Reference Gardiner, Bickmore and Yinusa-Nyahkoon16,Reference Hanafiah, Aagaard-Hansen and Ch Cheah18,Reference Valen, Wills and Medin19) . This is a reoccurring limitation with digital interventions, with attrition rates as high as 75–99 %(Reference Wang, Mahe and Huo39). A recent systematic review focusing on attrition in digital dietary interventions, summarises that boosting and maintaining motivation throughout the study is important to keep participants in the study, as well as providing resources, which might be social support, personalised feedback and providing financial resources(Reference Wang, Mahe and Huo39). Similar results are found for digital diet interventions targeting adolescents(Reference Melo, Santo and Mas Clavel7). In the PREPARED study we did focus on motivation, but the resource did not include personalised feedback. Nor did we offer financial support or incentives, which might have reduced attrition.
Recruiting men proved to be particularly difficult in the PREPARED study. We interviewed men before the onset of the trial to understand what would make them interested in participating(Reference Valen, Øverby and Hardy-Johnson28). We also involved men when writing texts, selecting pictures with men to include in the messages and in the development of videos. Still, only 12 % of the final sample were men. Ryan et al. tried to identify what would enhance male participation in health research(Reference Ryan, Lopian and Le40), pointing to pictures when people exercise and with short captions. Still, Ryan et al. found that even if men clicked on the advertisements, they did not enrol in the study(Reference Ryan, Lopian and Le40). They found that a strategy of encouraging females to invite men boosted male participation. Hanafiah et al. found that including partners in the intervention (no outcomes on partners) did not improve effectiveness(Reference Hanafiah, Aagaard-Hansen and Ch Cheah18).
Recruitment of participants from low socio-economic position (SEP) groups was also largely unsuccessful in PREPARED as in other studies. Of those recruited, 23 % were from low SEP groups. We aimed at recruiting a broad sample using easy language and short texts and videos. In general, individuals with low SEP more often decline invitations to participate in research, up to 15 % more so than higher SEP groups(Reference Stuber, Middel and Mackenbach41). Reasons for low participation and retention rates may be due to the highly agentic nature of behaviour interventions, which do not align with lower resources and poor health literacy and less supportive environments often seen in these groups(Reference Lorenc, Petticrew and Welch42). Stuber et al. have suggested, after interviewing 11 experienced project coordinators, success factors in recruiting low SEP individuals. These include among others securing beneficial contextual and programme-related factors and establishing contact with the target group through existing networks(Reference Stuber, Middel and Mackenbach41). They also suggest making participation easier (e.g. providing transport) and providing different incentives.
Difficulties in recruitment and high attrition in intervention studies have implications for public health, as it leads to research questions being unanswered by underpowered studies and waste of resources. We do not know if the interventions are ineffective due to their content or lack of relevance or whether it relates methodological challenges. From the studies above, those finding effects addressed a specific behaviour (taking supplements), or focused on risk-groups which might be highly motivated, which leaves unanswered questions for the public health approach, targeting large parts of the population. Exploring new ways of conducting public health research remains an important issue to address. The researchers of the Jom Mama project comment in their process evaluation that the premise that individual interventions can provide behavioural change might be flawed and that more upstream structural interventions are needed to target underlying determinants such as low socioeconomic status, education, food and built environments(Reference Sharif, Hanson and Chong25).
Potential ways forward regarding recruitment and in developing interventions
There are some potential ways that should be explored regarding recruitment and making interventions relevant for the targeted group. Using citizen science and participatory action approaches (PAR)(Reference Cornish, Breton and Moreno-Tabarez43), like real world labs (RWL), to a larger extent may be a way of identifying better recruitment strategies and keeping participants in the studies. A RwL is an innovative research setting designed to address complex societal challenges, particularly those related to sustainability, through collaborative and experimental approaches(Reference Bergmann, Schäpke and Marg44). Actors in RWL are local government, members of the public (relevant target population) and academics from different research fields. RWL hold, great potential in co-understanding challenges and co-developing relevant and context-specific solutions. Regarding recruitment, one could use such a laboratory to identify existing networks as mentioned by Stuber et al. (Reference Stuber, Middel and Mackenbach41), or to a greater extent help understand the context of target populations. Interventions and actions should be culturally and socially acceptable(Reference Barrera, Castro and Strycker45). In an RWL, one could target the most relevant actions for the target group and develop interventions to align with their needs and skills. Representatives of the target group and other stakeholders should be included as co-researchers through all development.
Touched upon by Jom Mama researchers an important insight before developing interventions is that there seems to be limited effect of interventions focusing solely on individual behaviour change(Reference Sharif, Hanson and Chong25,Reference Bryant, Burton and Mahdi46) . Interventions targeting individual behaviour encompass risk of failure because they rely on the individual’s motivation and skills for it to be effective. In addition, such interventions may not adequately consider the complexity of dietary behaviours, which include systemic matters and influences(Reference Bryant, Burton and Mahdi46). There is a need for interventions targeting more upstream determinants and structural determinants of diet, targeting multiple layers of society, building capacity in communities, not just the individual, and taking a systems approach(Reference Waterlander, Ni Mhurchu and Eyles47).
Combining an RWL approach (where most stakeholders are present) with the systems approach might be a way forward for research within Public Health Nutrition when developing future interventions. Stakeholders should assist in defining the problems that an intervention intends to solve and together with researchers identify connections and relationships between factors contributing to the problem to identify leverage points pertinent to the aim of the intervention.
Along with changing the nature of interventions, new methods of effect evaluation will be needed. Most studies experienced large attrition likely due to the burdensome and time-consuming interventions and assessment methods used. In future work one could seek to develop alternative indicators for dietary health to reduce participant burden and also explore possibilities of developing data infrastructure related to already collected data and registries that can be used to evaluate effects of interventions. This is all ahead, but we need to discuss new ways of recruiting, developing interventions and evaluating intervention effectiveness more broadly.
Conclusion
There has been an increase in interventions targeting the preconception population aiming to improve diet for the benefit of the next generation. Digital interventions have been part of the approach. We identified six digital interventions reporting on dietary outcomes, however with different target populations. Two studies found the intervention to be effective in improving specific parts of diet, while the others reported no relevant effect. Effective interventions either targeted specific groups or one specific topic (supplement). Most projects faced considerable challenges with recruitment, particularly reaching individuals from lower socio-economic backgrounds and males. High attrition complicated the evaluation in all studies. In addition, there were difficulties in engaging participants in digital interventions. Challenges with lack of engagement, recruitment and attrition are not new insights, and we need to learn from these studies and acknowledge the need for new ways of recruiting, developing interventions and evaluating them. One should explore whether future studies could benefit from using citizen science and participatory action research possibly as part of a Real-world Lab approach, in which researchers work in close collaboration with the target population and other stakeholders during the whole process. Moreover, as current behavioural interventions mostly rely on individual agency and are largely unsuccessful, there should be an exploration of the possibility of targeting more upstream and structural determinants of diet rather than individual behaviour alone. In future reviews it might be easier to compare studies with stricter definition of the preconception population.
Acknowledgements
We thank the participants who have spent time taking part in the PREPARED study.
Author contributions
N.C.O., E.R.H. and F.N.V. conceived the main conceptual ideas and applied for funding. F.N.V. led the work on planning the recruitment strategy, assisted by E.N.V. E.R.H. led the work on the development of the intervention, assisted by E.N.V., N.C.O., A.M. and L.S. A.M. led the work on the choice of methods, developing questionnaires, assisted by E.N.V., L.S., N.C.O. N.C.O. led the work on developing the flow and system of the project and the data management, assisted by E.V., L.S., A.M. N.C.O. is the PI in collaboration with E.R.H. as co-PI. N.C.O. drafted this review paper, and all authors have critically reviewed, commented and revised it. All authors have approved the last version of the paper.
Financial support
The PREPARED study is funded by the University of Agder. The University of Agder had no role in the design, analysis or writing of the article.
Competing interests
All authors declare no conflicts of interest.

 Open access
Open access