


Small vulnerable newborns, including small for gestational age (SGA), low birth weight (LBW) and preterm birth, are primary causes of neonatal deaths and adversely affect long-term health outcomes(Reference Ashorn, Ashorn and Muthiani1), such as hypertension and diabetes in later life(Reference Crump, Sundquist and Sundquist2,Reference Crump, Sundquist and Sundquist3) . It is estimated that 26·2 % of live births were small vulnerable newborns in 2020(Reference Lawn, Ohuma and Bradley4). Therefore, early identification and interventions targeting risk factors for these adverse birth outcomes are of practical importance.
Maternal Hb is a potentially modifiable risk factor for adverse birth outcomes. Accumulated evidence suggests that physiological hemodilution from middle pregnancy may lead to trimester-specific associations between Hb levels and adverse birth outcomes(Reference Young, Oaks and Tandon5–Reference Burden, Smith and Sovio7). Specifically, a meta-analysis conducted in 2021 showed that low maternal Hb (< 110 g/l) in early pregnancy was associated with increased LBW risk, whereas this association was not observed in middle pregnancy(Reference Young, Oaks and Rogers6). For higher Hb levels (> 130 g/l), the meta-analysis reported that elevated Hb in middle pregnancy was associated with increased LBW risk, whereas in late pregnancy it was associated with reduced risk. However, this finding was based on a single study including more than 17 000 African American (46 %) and Caucasian (54 %) pregnant women(Reference Young, Oaks and Rogers6). In contrast, a 2023 meta-analysis pooling two large UK cohorts (over 11 000 pregnant women, more than 90 % White) reported inconsistent findings: low Hb in early pregnancy was not associated with LBW or preterm birth, whereas higher Hb in late pregnancy was associated with increased risks of LBW, preterm birth and SGA(Reference Burden, Smith and Sovio7). Differences in population characteristics and socio-economic status may explain the heterogeneity across studies. Given the inconsistent findings and limited evidence regarding the associations between higher Hb levels and birth outcomes, more studies using time-specific Hb measures in diverse populations are thus warranted to replicate the previous findings.
Moreover, maternal Hb levels are influenced by many factors such as physiological plasma volume expansion, health conditions, nutritional status or Fe supplements(Reference Vricella8–Reference Peña-Rosas, De-Regil and Garcia-Casal10). Therefore, Hb measurements at a single time point cannot fully capture the dynamic changes throughout pregnancy. However, studies to date have mainly focused on the association of Hb measurements at a single time point or Hb differences between two trimesters with birth outcome(Reference Young, Oaks and Tandon5,Reference Jung, Rahman and Rahman11) . In addition, there is a lack of studies on the dynamic changes of Hb levels on fetal growth parameters. A prospective study among 7317 pregnant women showed that elevated Hb levels were associated with fetal head circumference, length and weight growth restriction from the third trimester onwards; however, Hb levels were only measured in early pregnancy(Reference Gaillard, Eilers and Yassine12). Integrating repeated Hb measurements with longitudinal fetal ultrasound assessments may provide a more comprehensive understanding of the relationship between maternal Hb trajectories and birth outcomes.
To address the knowledge gap, we aimed to (1) investigate the associations of Hb trajectories with fetal growth parameters (based on ultrasound assessments) and birth outcomes and (2) assess the associations of time-specific Hb levels with similar health outcomes.
Methods
Study design and participants
The Tongji-Huaxi-Shuangliu Birth Cohort (THSBC) is an ongoing birth cohort launched between 2017 and 2020 in the Shuangliu Maternal and Child Health Hospital in China. Detailed information on the study design has been described elsewhere(Reference Wang, Huang and Wu13). In brief, 7281 pregnant women (aged 18–40 years; singleton pregnancy; and without infectious diseases or major chronic conditions) were recruited at 6–15 weeks of gestation. They were followed up regularly until the end of pregnancy. Maternal Hb measurements and fetal ultrasound examinations were obtained during routine antenatal visits(14). We further excluded pregnant women who (1) had no measurements of Hb during pregnancy (n 13), (2) had missing data for birth weight (n 392) and (3) had missing data for major covariates (n 32). Baseline characteristics were generally comparable between included participants and those excluded (online Supplementary Table 1). A total of 6844 participants met the eligibility criteria. A total of 6177 pregnant women who had Hb measurements in at least three of the four time periods of pregnancy were included in the trajectory analyses (online Supplementary Figure 1). The study was carried out in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Tongji Medical College, Huazhong University of Science and Technology (approval number: 2017-S225). All participants gave written informed consent before enrolment.
Hb measurements
Hb levels were measured by an automatic blood cell analyser (XN-10; SYSMEX) at the site hospital. Pregnancy was divided into four periods of pregnancy based on the distribution of gestational weeks of Hb measurements (early pregnancy: 6–12; middle pregnancy: 13–27; middle-late pregnancy: 28–32; and late pregnancy: 33–37 gestational weeks). Detailed information on the total number and the frequency of measurements during four periods is presented in online Supplementary Table 2. For pregnant women who had multiple measurements within any of the four periods, we used the mean value of Hb concentrations in subsequent analyses. According to the latest WHO criteria, anaemia was defined as Hb < 110 g/l in early pregnancy, < 105 g/l in middle pregnancy and < 110 g/l in late pregnancy(15). Based on prior literature(Reference Young, Oaks and Rogers6,Reference Burden, Smith and Sovio7) , 130 g/l was used as the cut-off for higher Hb. Hb concentrations between the anaemia threshold and 130 g/l were defined as the reference category.
Fetal ultrasound measures and adverse birth outcomes
Fetal growth parameters (head circumference, abdominal circumference (AC) and femur length) were measured by well-trained sonographers using standardised procedures. Meanwhile, the umbilical artery resistance index was measured by pulsed Doppler ultrasound to reflect placental function and placental vascular resistance(Reference Campbell, Diaz-Recasens and Griffin16). All fetal ultrasound measurements were done in three periods of pregnancy (middle pregnancy: 13–27; middle-late pregnancy: 28–32; and late pregnancy: 33–37 gestational weeks) (online Supplementary Table 3). Estimated fetal weight (EFW) was calculated based on AC, femur length and head circumference using the formula proposed by Hadlock et al(Reference Hadlock, Harrist and Sharman17). Birth weight was obtained from electronic medical records. SGA was defined as a birth weight that falls within the lowest 10th percentile according to the latest Chinese standards for sex- and gestational week-specific birth weights(Reference Dai, Deng and Li18). LBW was defined as birth weight < 2500 g. Preterm birth was defined as gestational week at delivery < 37 weeks.
Covariates
Maternal characteristics, including maternal age, education, parity, smoking, drinking and physical activity, were collected using a structured questionnaire at enrolment(Reference Wang, Huang and Wu13,Reference Xiang, Konishi and Hu19,Reference Wu, Wang and Ye20) . Education was divided into middle school or below, high school or equivalent and college or above. Parity was categorised into nullipara and multipara groups. Smoking and drinking in the past year were coded as never and ever/current. Physical activity was assessed by the Chinese version of the Pregnancy Physical Activity Questionnaire and expressed as metabolic equivalent of task-h/week (MET-h/week)(Reference Xiang, Konishi and Hu19). Infant sex was collected from electronic medical records. Pre-pregnancy BMI was calculated by the self-reported pre-pregnancy weight (kilograms) divided by the square of height (metres) measured in early pregnancy.
Statistical analysis
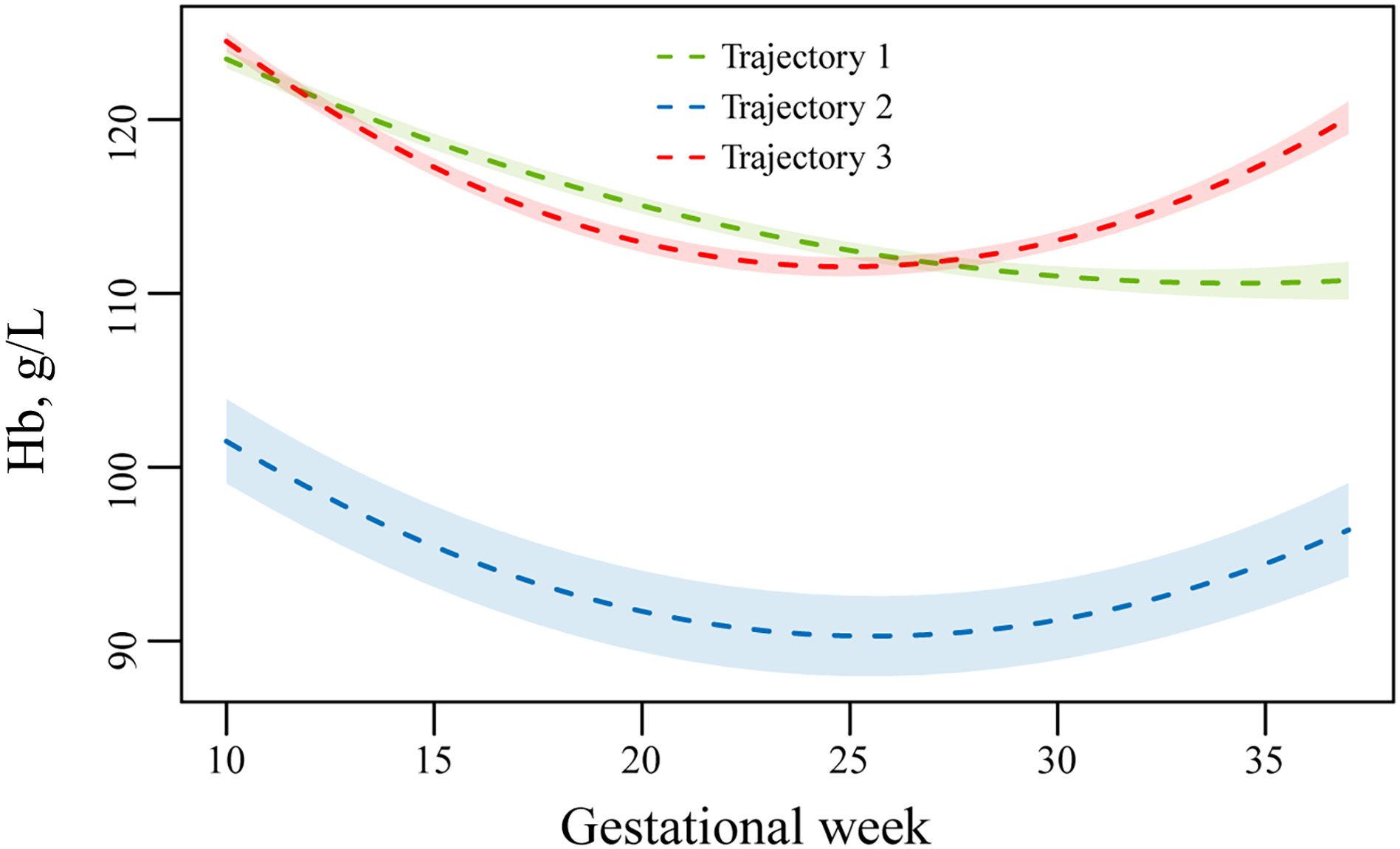
Latent class mixed models were used to identify trajectory groups among pregnant women who had at least three Hb measurements. The quadratic term of gestational weeks was included in the fixed effect to allow for non-linear change. In addition, gestational weeks were considered as a random effect to account for the variation between individuals. We fitted models with 1–5 classes and selected the best model based on the following principles(Reference Lennon, Kelly and Sperrin21): (1) the lowest Bayesian information criterion (online Supplementary Table 4); (2) the mean posterior probability of each class > 0·7; and (3) reasonable clinical significance. The model with three Hb trajectories was identified as the best fit: Trajectory 1 (consistent decline, n 3248; 52·6 %), Trajectory 2 (consistently low, n 152; 2·5 %) and Trajectory 3 (increase from the middle-late pregnancy, n 2777; 44·9 %) (Figure 1).
Hb trajectories in the Tongji-Huaxi-Shuangliu Birth Cohort. The dotted lines represent the class-specific mean predicted trajectory of Hb levels, and the shaded bands represent 95 % CI for the splines. Trajectory 1, consistent decline (n 3248; 52·6 %); Trajectory 2, consistently low (n 152; 2·5 %); Trajectory 3, increase from the middle-late pregnancy (n 2777; 44·9 %).

Fetal biometrics were log-transformed to normalise the distribution. Linear mixed models and linear regression models were used to examine the association between Hb trajectory groups and fetal biometrics in the whole pregnancy and in each specific period of pregnancy. In linear mixed models, all available fetal biometrics were included and regressed on trajectory groups, and variations within and between individuals were incorporated in the random effect. In linear regression models, to ensure that the gestational weeks for fetal measures were not earlier than the gestational weeks for Hb levels, the last fetal measure in each specific period of pregnancy was used to fit the models. The coefficients (β) and 95 % CI for fetal biometrics in all models were further converted using (e β − 1) × 100 % to explain the effect estimates for the log transformation of the dependent variable(Reference Zou, Wei and Shi22). These models were adjusted for age, education, infant sex, parity, smoking, drinking, physical activity, pre-pregnancy BMI, gestational weeks and the square of gestational weeks.
We also used multivariable generalised linear models to examine the associations of anaemia (< 110 g/l) and higher Hb levels (≥ 130 g/l) for each of four defined pregnancy periods, with fetal biometrics measurements and adverse birth outcomes, as compared with the reference group (110–129 g/l). Results were reported for each increase of 10 g/l when Hb was treated as a continuous variable. Modelling based on restricted cubic splines with three knots (10th, 50th and 90th percentiles) was used to explore the non-linearity.
To test the robustness of our results, we performed several sensitivity analyses. First, for women with multiple measurements within each pregnancy period, two sensitivity analyses were performed: Hb levels were defined as the maximum value or as the last measurement, instead of the mean value. Second, we excluded pregnant women who were diagnosed with gestational diabetes mellitus, gestational hypertension or pre-eclampsia during pregnancy since these diseases were related to fetal growth. Third, we also adjusted for the use of Fe supplements and folic acid during pregnancy. Fourth, we adjusted for BMI in early pregnancy instead of pre-pregnancy BMI. A two-sided P value < 0·05 was considered statistically significant. All analyses were conducted by R software version 4.1.0.
Results
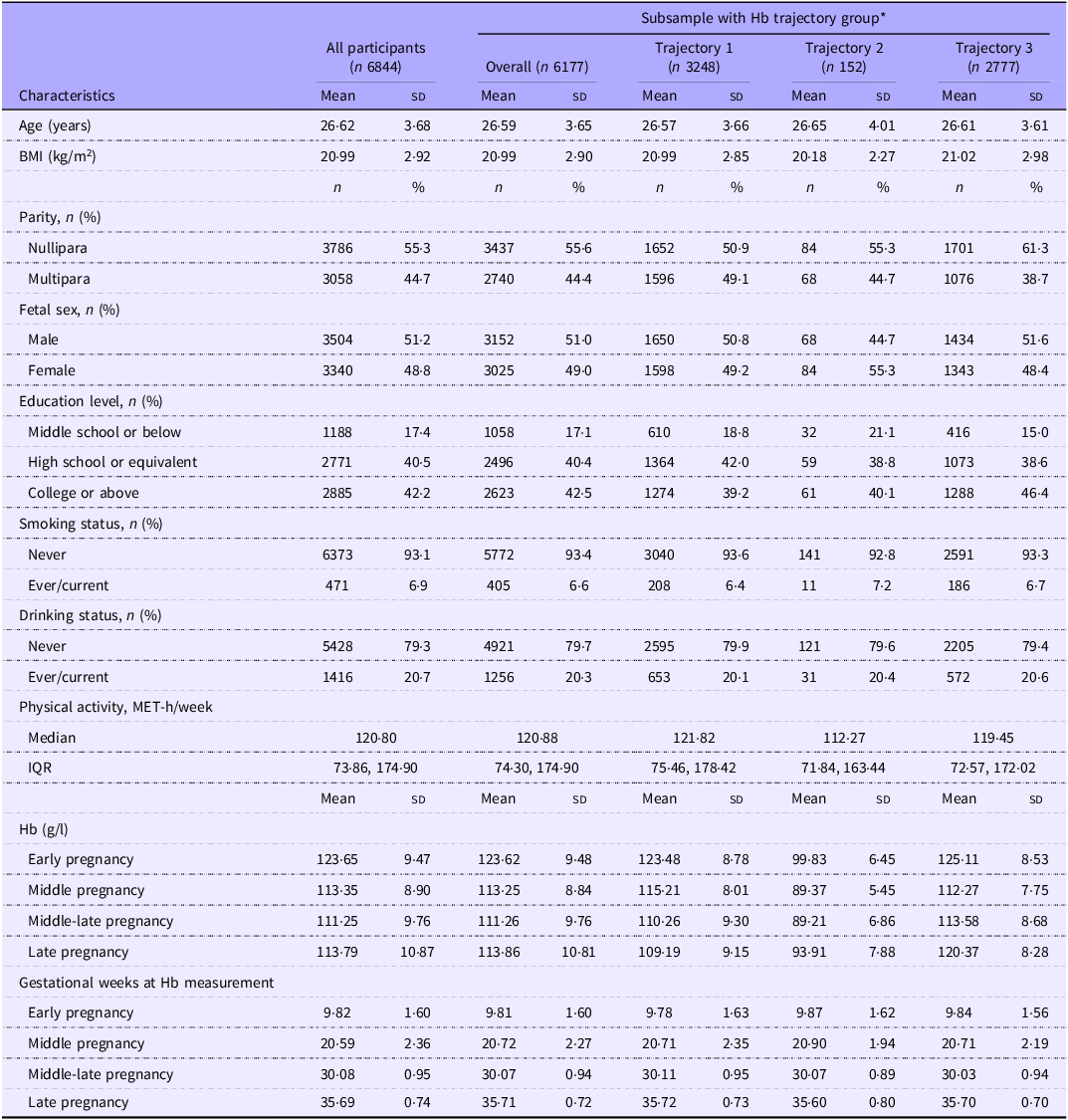
Of 6844 pregnant women, the mean age was 26·62 (sd, 3·68) years (Table 1). Study participants in the Trajectory 3 group of Hb were more likely to be nulliparous, well-educated and have higher pre-pregnancy BMI (Table 1). The prevalences of anaemia in the four periods of pregnancy were 6·8 %, 14·8 %, 41·8 % and 33·6 %, respectively (online Supplementary Table 5).
Characteristics of study participants from the Tongji-Huaxi-Shuangliu Birth Cohort

MET, metabolic equivalent of task; IQR, interquartile range.
* Trajectory 1, consistent decline; Trajectory 2, consistently low; Trajectory 3, increase from the middle-late pregnancy.
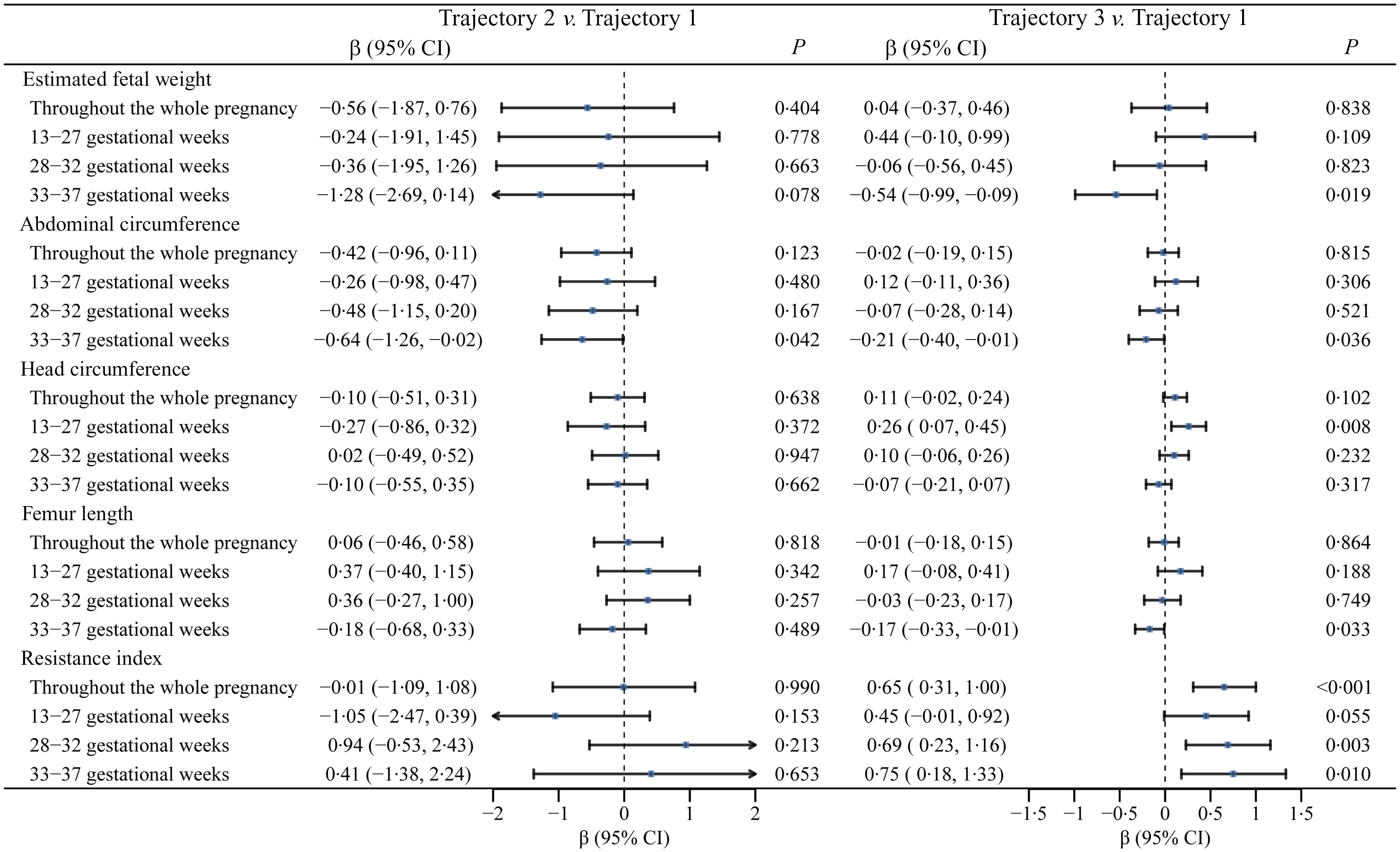
The associations between Hb trajectories and fetal biometrics are presented in Figure 2. Compared with Trajectory 1, Trajectory 2 was associated with lower AC in late pregnancy (β = −0·64; 95 % CI −1·26, −0·02). Trajectory 3 was associated with higher head circumference (β = 0·26; 95 % CI 0·07, 0·45) in middle pregnancy but lower EFW (β = −0·54; 95 % CI −0·99, −0·09), AC (β = −0·21; 95 % CI −0·40, −0·01) and femur length (β = −0·17; 95 % CI −0·33, −0·01) in late pregnancy. In addition, Trajectory 3 was also related to higher umbilical artery resistance index throughout pregnancy (β = 0·65; 95 % CI 0·31, 1·00). Compared with Trajectory 1, Trajectory 3 was associated with a higher risk of LBW (OR = 1·57; 95 % CI 1·09, 2·26; online Supplementary Table 6). Moreover, birth weight was 60·52 g lower (95 % CI −116·10, −4·95) in Trajectory 2 and 22·94 g lower (95 % CI −40·38, −5·50) in Trajectory 3 (online Supplementary Table 7).
Association of Hb trajectories with fetal biometrics. Linear mixed models were used for the whole pregnancy, and linear regression models were used for specific periods of pregnancy. Fetal biometrics were log-transformed. Trajectory 1, consistent decline; Trajectory 2, consistently low; Trajectory 3, increase from the middle-late pregnancy. Individuals in the Trajectory 1 group were set as the reference group. Models were adjusted for age, education, infant sex, parity, smoking, drinking, physical activity, pre-pregnancy BMI, gestational weeks at ultrasound measurements and the square of gestational weeks at ultrasound measurements.

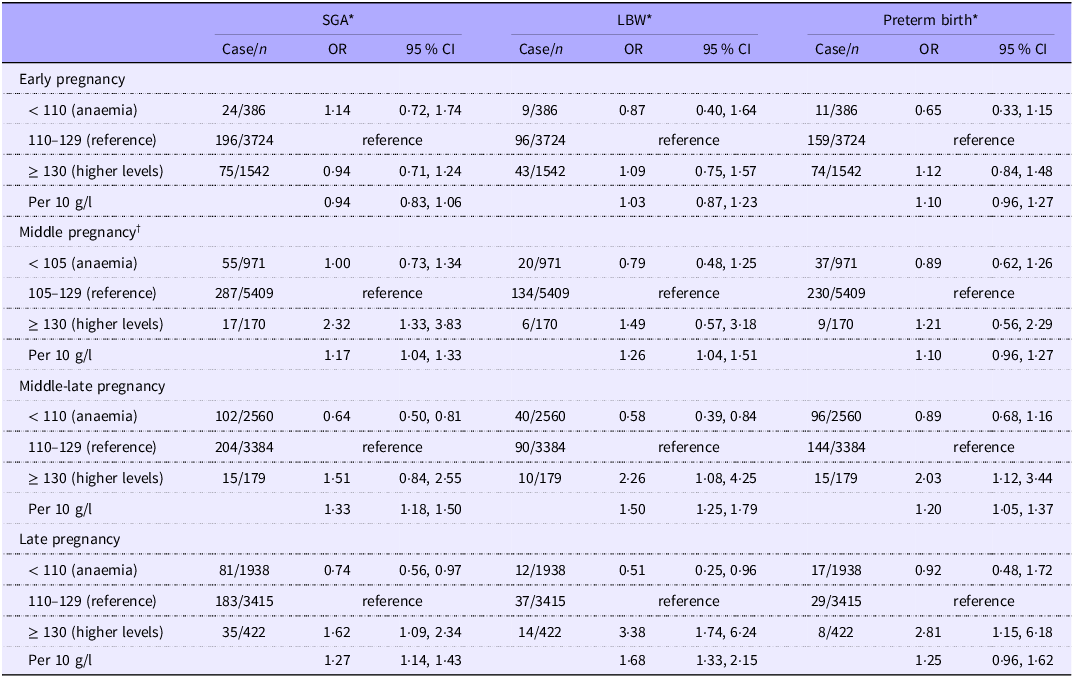
In early pregnancy, anaemia (< 110 g/l) and higher Hb levels (≥ 130 g/l) were not associated with SGA, LBW or preterm birth, compared with the reference group (110–129 g/l) (Table 2). In middle-late pregnancy, anaemia (< 110 g/l) was associated with lower risks of SGA (OR, 0·64; 95 % CI 0·50, 0·81) and LBW (OR, 0·58, 95 % CI 0·39, 0·84), while higher Hb levels (≥ 130 g/l) were associated with higher risks of LBW (OR, 2·26; 95 % CI 1·08, 4·25) and preterm birth (OR, 2·03, 95 % CI 1·12, 3·44), compared with the reference group (110–129 g/l). Higher Hb levels in middle-late pregnancy were associated with a lower birth weight (β, −31·51, 95 % CI −40·35, −22·68 for 10 g/l increase of Hb) (online Supplementary Table 8). A similar pattern of association of Hb levels with birth outcomes and birth weight was observed in late pregnancy (Table 2 and Supplementary Table 8). An increase of Hb levels was associated with lower EFW in middle, middle-late and late pregnancy, while anaemia (< 110 g/l) was associated with higher EFW in middle-late pregnancy (β, 0·95, 95 % CI 0·44, 1·47) and late pregnancy (β, 0·61, 95 % CI 0·12, 1·10), compared with the reference group (110–129 g/l) (online Supplementary Table 9). Restricted cubic splines showed non-linear associations of Hb levels in middle pregnancy with SGA and birth weight (online Supplementary Figure 2–3). In middle-late and late pregnancy, non-linear associations were noted for LBW and preterm birth (all P for non-linearity < 0·036; online Supplementary Figure 2).
Association of Hb levels in specific periods of pregnancy with adverse birth outcomes

SGA, small for gestational age; LBW, low birth weight.
* OR and 95 % CI were based on logistic regression models. Models were adjusted for age, education, infant sex, parity, smoking, drinking, physical activity, gestational weeks at Hb measurement and pre-pregnancy BMI.
† The cut-off of Hb levels of < 105 g/l in middle pregnancy was used to define anaemia as recommended by the WHO(15).
In all sensitivity analyses, the associations of Hb levels with birth outcomes and of trajectories with fetal biometrics were not substantially changed (online Supplementary Figure 4–6, Supplementary Table 10).
Discussion
Main findings
Compared with Trajectory 1 (consistent decline), Trajectory 3 (increase from the middle-late pregnancy) showed a positive association with fetal growth parameters in middle pregnancy, but a negative association in middle-late pregnancy and late pregnancy. In addition, Trajectory 3 was associated with a higher risk of LBW. Consistently, higher Hb levels were also associated with higher risks of LBW, SGA or preterm birth starting from middle pregnancy. Our findings highlight the importance of dynamic monitoring maternal Hb levels for reducing the risk of small vulnerable newborns.
Interpretation
To date, most studies have only examined the associations of trimester-specific Hb levels or differences between two trimesters with birth outcomes(Reference Young, Oaks and Tandon5,Reference Burden, Smith and Sovio7,Reference Xu, Wang and Li23) . A prospective study conducted in the Netherlands with 7317 participants showed that higher Hb levels in early pregnancy were significantly associated with lower EFW in late trimester(Reference Gaillard, Eilers and Yassine12). However, Hb levels and fetal growth parameters were only assessed at one time point. Considering the dynamic changes in Hb and fetal growth, we applied the trajectory model to identify three distinct Hb trajectories based on multiple Hb measurements and evaluated their relationships with repeatedly measured fetal growth parameters throughout pregnancy. Although these trajectories are data-driven and do not represent stable physiological phenotypes, they may provide complementary evidence by capturing overall patterns of Hb change at the population level. We observed positive coefficients for fetal growth parameters (EFW, AC and femur length) for Trajectory 3 (increase from the middle-late pregnancy) in middle pregnancy, compared with Trajectory 1 (consistent decline), despite a lack of statistical significance. However, the coefficients became negative in the middle-late pregnancy and reached statistical significance in late pregnancy. In addition, Trajectory 3 was related to higher umbilical resistance index starting from middle-late pregnancy. Increased umbilical resistance index is related to placental insufficiency, possibly because of impaired placentation(Reference Gaillard, Arends and Steegers24,Reference Baschat and Hecher25) . These findings suggest that fetal growth is closely related to fluctuation in Hb levels and that longitudinal Hb monitoring may help to identify pathological elevations and prevent fetal growth restriction. Moreover, Trajectory 2 (low-stable Hb) with 152 pregnant women was inversely related to birth weight compared with Trajectory 1. As Trajectory 2 only contained a small number of participants, these findings should be interpreted with caution, and prospective studies with larger sample sizes are needed to identify trajectory groups and replicate our findings in future.
In analyses restricted to each period of pregnancy, higher Hb levels measured in middle-late and late pregnancy were significantly associated with higher risks of LBW or SGA. Consistent with our work, several observational studies also linked higher Hb levels in the second or third trimester with adverse birth outcomes(Reference Young, Oaks and Tandon5,Reference Xu, Wang and Li23,Reference Steer, Alam and Wadsworth26,Reference Dewey and Oaks27) . It is hypothesised that higher Hb levels may reflect inadequate plasma volume expansion(Reference Dewey and Oaks27), which could compromise placental blood flow and lead to placental and fetal hypoxia(Reference Steer, Alam and Wadsworth26,Reference Stangret, Skoda and Wnuk28) . Relevant to harms of high Hb levels is the high intake of Fe supplements during pregnancy. A prospective study of 1196 non-anaemic pregnant women showed that infants of mothers in the highest tertile group of Fe supplements were at 89 % higher risk of term LBW and had lower birth weight (−72 g) and a shorter duration of gestation (−0·6 week)(Reference Shastri, Mishra and Dwarkanath29). In another clinical trial of 727 pregnant women with Hb ≥ 132 g/l in middle pregnancy, participants were randomised to receive either 50 mg of elemental Fe or placebo throughout pregnancy, and the incidence of SGA significantly increased in the intervention group (15·7 % v. 10·3 %)(Reference Ziaei, Norrozi and Faghihzadeh30). The WHO currently recommends daily Fe supplementation of 30–60 mg (plus 400 μg of folic acid) throughout pregnancy(31). The recommendation was based on a Cochrane review of sixty randomised controlled trials published in 2012, in which pregnant women who received daily Fe supplementation had a 70 % lower risk of anaemia at term and a 19 % lower risk of delivering infants with LBW(Reference Peña-Rosas, De-Regil and Dowswell32). However, when the review was updated in 2015(Reference Peña-Rosas, De-Regil and Garcia-Casal10), the reduction in the LBW risk did not reach statistical significance (relative risk: 0·84; 95 % CI 0·69, 1·03; 11 studies), and no significant effects on other birth outcomes were observed. The updated review thus concluded that the beneficial effect of Fe supplementation on infant outcomes is unclear and may vary depending on the initial Fe status(Reference Peña-Rosas, De-Regil and Garcia-Casal10). Thus, moderate Fe supplementation may be beneficial for individuals with low Fe status, while excessive supplementation could be potentially harmful for pregnant women who are Fe-replete(Reference Dewey and Oaks27). Taken together with the trajectory findings, our results suggest that regular monitoring of Hb during pregnancy, along with targeted Fe status assessment in women with abnormally elevated Hb levels, may have clinical relevance for guiding Fe intake and potentially reducing the risk of adverse birth outcomes.
Models based on restricted cubic splines predominantly showed a linear or a J-shaped association of Hb levels with adverse birth outcomes in our study, which was inconsistent with the reported U-shaped association in previous reports(Reference Dewey and Oaks27). In particular, anaemia in middle-late and late pregnancy was inversely associated with LBW and SGA, while we did not find significant associations for anaemia in early or middle pregnancy with adverse birth outcomes. Consistently, a pooled analysis from two UK pregnancy cohorts showed that anaemia in early pregnancy was associated with a 17 % lower risk of SGA but not LBW or preterm birth, while anaemia in late pregnancy was related to lower risks of LBW, SGA and preterm birth(Reference Burden, Smith and Sovio7). Differences in study design, sample size and primary causes of anaemia in different regions of the world may explain the inconsistent results(Reference Young, Oaks and Tandon5,Reference Burden, Smith and Sovio7,Reference Rahman, Abe and Rahman33) . Although both our study and previous research observed inverse associations between anaemia and adverse birth outcomes(Reference Burden, Smith and Sovio7,Reference Shi, Chen and Wang34) , these findings should not be interpreted as causal or protective, given the observational nature and the physiological plasma volume expansion during pregnancy. Future studies are needed to account for the causes of anaemia (physiologic or pathological) and evaluate the optimal cut-offs of Hb in different settings.
Strengths and limitations
The main strength of our study is the use of repeatedly measured Hb levels and fetal biometrics throughout pregnancy, which enabled us to conduct separate analyses by the timing of Hb measurements and investigate the association between the trajectories of Hb with intra-uterine growth and birth outcomes. However, we acknowledge several limitations in the study. First, Hb levels reflect both Fe status and physiological plasma volume expansion during pregnancy. However, we did not measure Fe status biomarkers, such as ferritin(Reference Auerbach, DeLoughery and Tirnauer35), which limits causal inference. Although we adjusted for self-reported use of Fe supplements and folic acid, residual confounding may remain. Second, measurement errors could not be avoided for fetal ultrasound measurements, although they were assessed by well-trained staff following standard procedures. Third, the trajectory models could not precisely differentiate physiological and pathological declines. Fourth, as lifestyle changes after anaemia diagnosis could affect birth outcomes, we could not exclude the possibility that the observed inverse associations between anaemia and adverse birth outcomes were driven by healthy lifestyle factors among individuals with anaemia after diagnosis. Fifth, the study sample size might not be sufficient for current analyses, and an a priori sample size calculation was not conducted. In particular, the number of individuals in the Trajectory 2 group was relatively small, which could lead to low statistical power. Sixth, since the study was conducted in southwestern China, the findings may not be necessarily generalisable to other populations.
Conclusions
Our findings suggested that fetal growth was related to fluctuations of Hb levels across pregnancy. In particular, higher maternal Hb levels starting from the middle-late pregnancy may be associated with lower EFW in late pregnancy and a higher risk of LBW.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107016
Acknowledgements
The authors thank all participants in the Tongji-Huaxi-Shuangliu Birth Cohort. The authors also thank the staff in the Shuangliu Maternal and Child Health Hospital and investigators from the Huazhong University of Science and Technology and Sichuan University.
X. F. P. was sponsored by the National Key R&D Program of China (2024YFC2707602) and the National Natural Science Foundation of China (82473646). A. P. was supported by grants from the National Natural Science Foundation of China (82325043). J. W. was supported by the Sichuan Science and Technology Program (2023ZYD0120).
X. F. P. and A. P. designed the research; Y. X. W., Y. W., P. W., Y. X. Y. and Y. W. L. conducted the research; Y. X. W. performed statistical analysis; Y. X. W. wrote the paper; Y. X. Y., Y. W., P. W., Y. W. L., Y. H. N. Y., Y. D. D., J. Y. Y., J. P. Z., L. X. H., Y. Y. H., J. W., G. L., X. F. P. and A. P. provided critical revision for important intellectual content of the manuscript. A. P. and X. F. P. are the guarantors of this work and, as such, have full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
All authors have disclosed that they have no financial relationships or conflicts of interest.
The study was carried out in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Tongji Medical College, Huazhong University of Science and Technology (approval number: 2017-S225). All participants gave written informed consent before enrolment.
Data described in the article, code book and analytic code are available upon reasonable request from the corresponding author.



 Open access
Open access