


I accidentally walked into a full length mirror in an office hallway because I didn’t realize it was my reflection and I expected that “guy” to move out of the way so we wouldn’t collide! It was embarrassing and funny all at the same time. I also raised my son from the time he was 3 weeks and I wouldn’t recognize him if I didn’t know he was supposed to be in the room. He is now 28 years old. (Subject BIOT2)
It is hard not to be fascinated by the amusing and sometimes poignant stories of patients with acquired prosopagnosia. How is it that a person who can see and remember most things suddenly finds that the faces of their family and friends have become strange and that they can now no more tell faces apart than they can stones on the beach? And, more to the point for neurologists and neuroscientists, what does the existence of this condition tell us about the organization of vision in the human brain? Or about how we achieve the seemingly effortless task of recognizing faces, despite their complex three-dimensional structures, shifts in viewpoint, fleeting changes of expression, long-term warping from age and the high degree of similarity between all human faces?
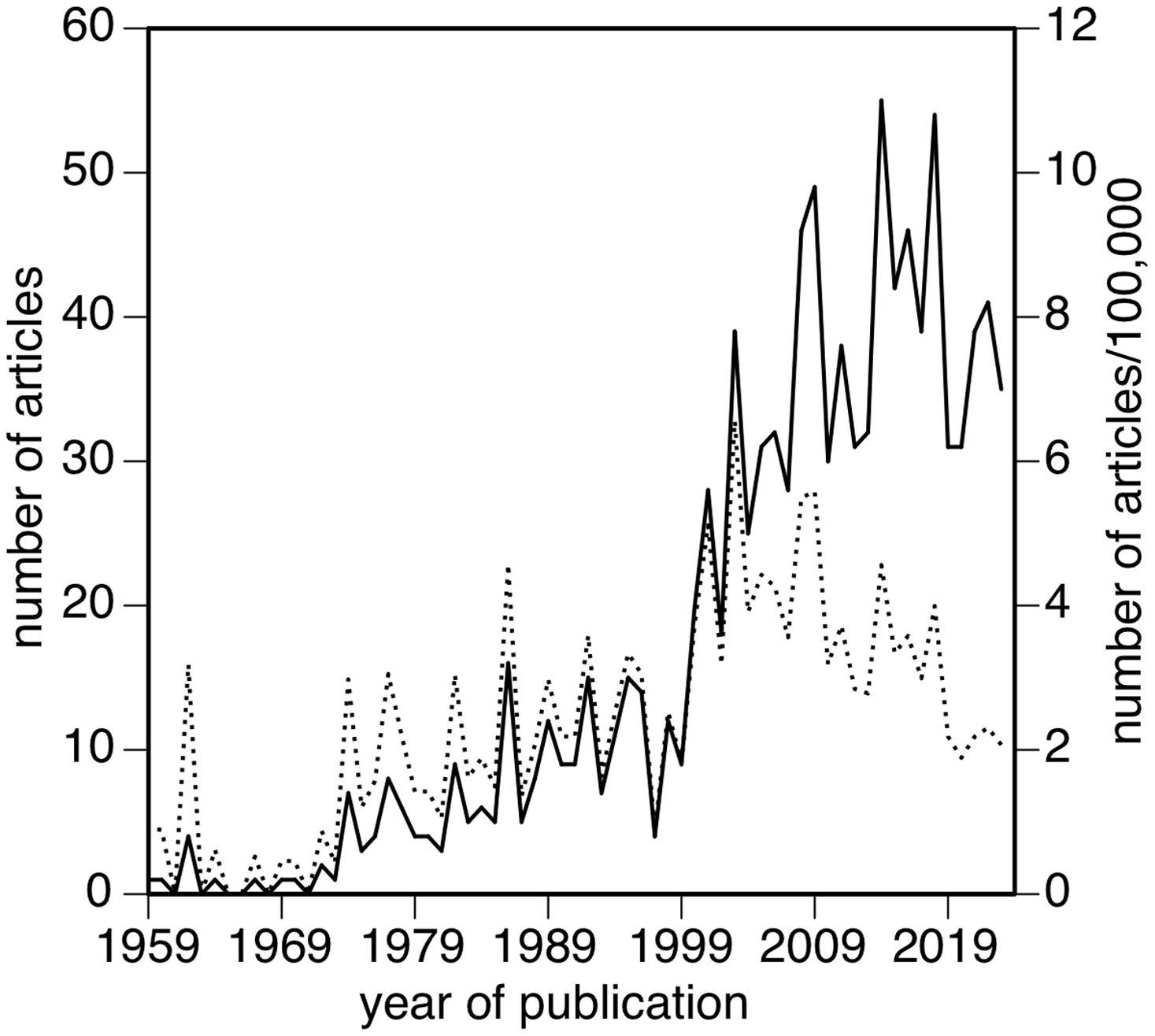
Acquired prosopagnosia has been part of the neurologic landscape for a long time. The term specifically refers to the loss of familiarity for the identity of the face, the lack of realization that it belongs to someone you have seen before. The first case was likely LL, who was reported 157 years ago by the Italian ophthalmologist Quaglino. Reference Quaglino and Borelli1,Reference Della Sala and Young2 It is a rare condition, with most neurologists unlikely to encounter more than one or two cases in their career. One or two also corresponded to the annual frequency of reports on prosopagnosia, until interest grew in the 1980s and then surged in the new century to about 40 papers a year, a 40-fold increase that exceeds the 10-fold growth in all scientific reports over this 60-year period (Figure 1).
Annual number of publications about prosopagnosia (solid line), also expressed as proportion of the scientific literature (dotted line).
Several factors have fueled the expansion of work in this unusual condition. In the 1980s, psychologists created cognitive models of face perception Reference Bruce and Young3,Reference Burton, Bruce and Johnston4 and were interested in how these applied to prosopagnosia. At the same time, structural imaging with CT and MRI scans permitted the in vivo demonstration of the lesions that caused prosopagnosia, Reference Damasio, Damasio and van Hoessen5–Reference de Renzi7 an advance over indirect inferences from homonymous field defects and the wait for pathologic data. Reference Meadows8 In the 1990s, functional MRI emerged as a tool and revealed the network of regions involved in the face perception of healthy subjects, Reference Haxby, Hoffman and Gobbini9 including first and foremost the fusiform face area. Reference Kanwisher, McDermott and Chun10 MRI techniques then expanded in several directions, allowing us to look at the structural and functional connectivity of this network Reference Davies-Thompson and Andrews11 and to explore the functions of cerebral regions using fMRI adaptation. Reference Grill-Spector and Malach12 For prosopagnosia, the development of face localizers robust enough to detect these networks in single subjects brought functional imaging to individual patients, Reference Fox, Iaria and Barton13 allowing the correlation of their functional defects with the structural impact of their lesions on the face network.
While these developments rapidly expanded our knowledge of the structural basis of face perception and prosopagnosia, advances in computerized image processing – some imported from the film industry – allowed more sophisticated means of measuring face perception. Instead of the simplistic Identikit drawings Reference Bradshaw and Wallace14,Reference Matthews15 used by police in the 1960s and 1970s, researchers could now morph faces between identities, ages and expressions, Reference Fox, Hanif, Iaria, Duchaine and Barton16 separate the texture and reflectance of a face from its shape, Reference O’Toole, Vetter and Blanz17,Reference Lai, Oruc and Barton18 manipulate the size and position of different features Reference Barton, Keenan and Bass19 and so on. These were used in adaptation studies to probe the nature of the face representations our brains store Reference Fox and Barton20,Reference Fox, Oruc and Barton21 and to generate concepts of how these representations might be organized, as, for example, norm-based coding models. Reference Leopold, O’Toole, Vetter and Blanz22
Finally, a major factor has been the discovery of developmental prosopagnosia. The first case was reported in 1976. Reference McConachie23 AB was a 12-year-old girl whose mother also had lifelong trouble recognizing faces. More cases were reported, leading to claims that as much as 2% of the population may have this condition, Reference Kennerknecht, Grueter and Welling24 though more recent estimates suggest the true incidence may be lower. Reference DeGutis, Bahierathan and Barahona25 Regardless, this has led to larger samples of “face-blind” subjects available for research, though the relation of the developmental to the acquired version is not clear. In particular, it is not known whether the developmental variant is simply the low end of the normal distribution of face perception abilities in the population or a pathologically distinct group. Reference Barton and Corrow26 Recent cluster analyses of 1500 subjects suggest the former, Reference DeGutis, Bahierathan and Barahona25 but more work with genetic and imaging biomarkers is needed to settle the issue.
This review focuses on acquired prosopagnosia. There are many intriguing aspects to this disorder, such as how patients with prosopagnosia scan faces, Reference Meadows8 whether they show covert recognition and what that means, Reference Barton, Barbeau, Felician and Joubert29 whether dissociations explain certain features Reference Fox, Iaria and Barton30 and the relation of face perception to other means of person recognition. Reference Barton and Corrow31 Here I will discuss five observations learned over 24 years of study.
Prosopagnosia is not a disorder but a family of disorders
People become prosopagnosic for different reasons, in both the structural and functional sense. The structural patterns of lesions in prosopagnosia are often complex but can be considered to differ mainly in two ways, whether they are (a) unilateral or bilateral or (b) anterior temporal or posterior occipitotemporal, though sometimes the latter occurs in combination.
Regarding laterality, a frequent association with left hemifield defects led to early beliefs that prosopagnosia resulted predominantly from right hemispheric damage. Reference Hecaen and Angelergues32 Bodamer, who coined the term “prosopagnosia,” inferred the presence of bilateral occipital damage from clinical signs, Reference Ellis and Florence33 and the seminal studies of Meadows Reference Meadows8 and Damasio Reference Damasio, Damasio and van Hoessen5 described bilateral lesions on imaging and/or autopsy. These were countered by an increasing number of imaging reports in the 1980s of patients with unilateral right hemispheric lesions. Reference Landis, Cummings, Christen, Bogen and Imbof6,Reference de Renzi7,Reference Michel, Perenin and Sieroff34–Reference Takahashi, Kawamura, Hirayama, Shiota and Isono37 On the other hand, prosopagnosia from a unilateral left hemispheric lesion is distinctly rare. Reference Barton38,Reference Papagno, Barvas, Tettamanti and Gainotti39 Subjects with this condition are often left-handed, and sometimes, their imaging reveals subtle right hemispheric changes as well. Reference Hills, Pancaroglu, Duchaine and Barton40
These clinical observations on lateralization are consistent with functional imaging studies in healthy subjects that show bilateral activation with a right hemispheric dominance during face processing. Reference Kanwisher, McDermott and Chun10,Reference Nestor, Behrmann and Plaut41 It is not clear if there is any qualitative difference in prosopagnosia between those with unilateral and those with bilateral lesions: the difference may be more quantitative, with slightly lower scores for face familiarity in those with bilateral lesions. Reference Barton42 The degree of lateralization of the face network likely varies on a continuum, and this may determine whether a right-sided lesion is sufficient to create prosopagnosia or if bilateral lesions are needed. Reference De Renzi, Perani, Carlesimo, Silveri and Fazio43 A rightward bias of this continuum can explain why prosopagnosia is rare after left hemispheric lesions.
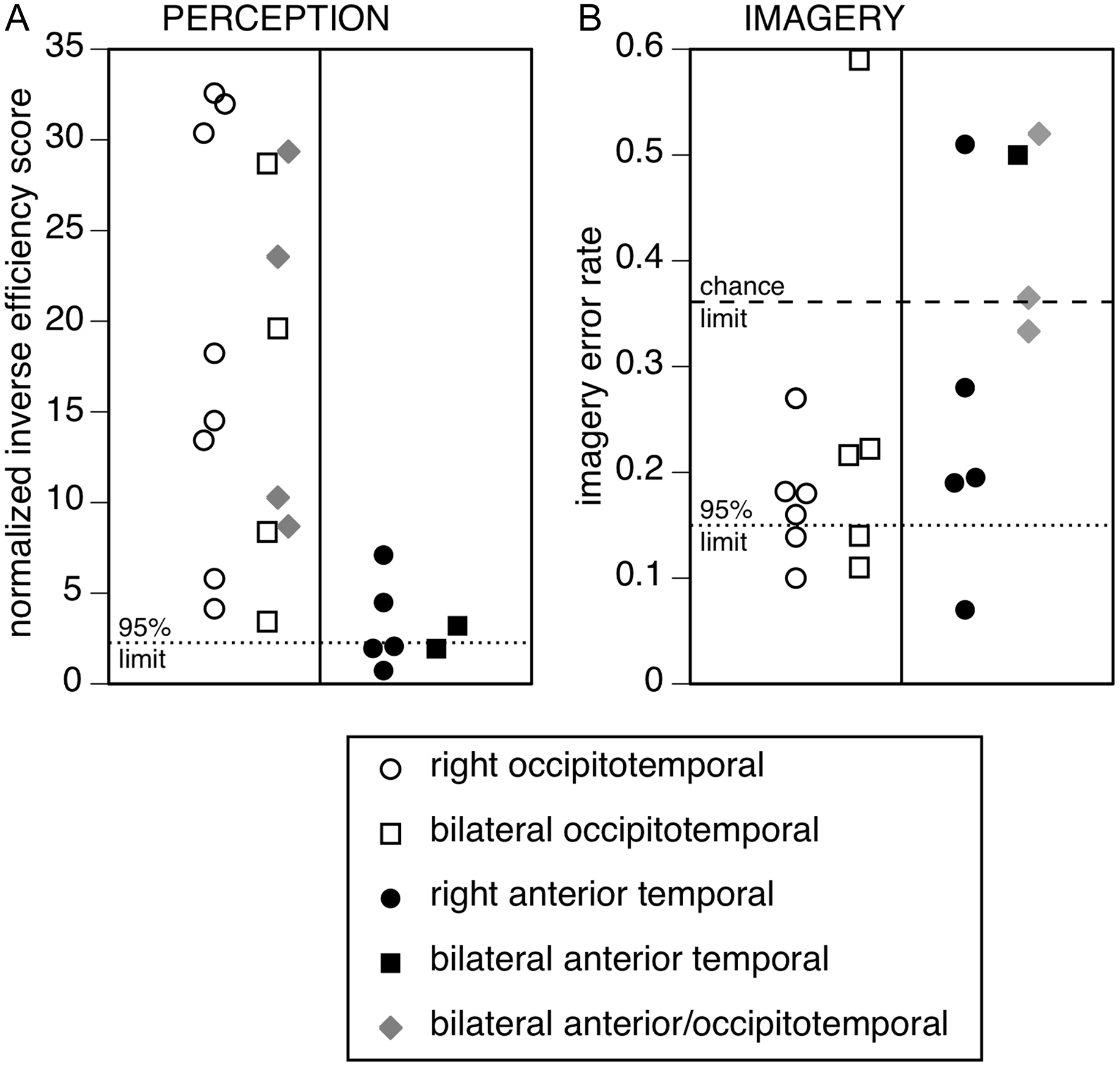
How about the second distinction, between posterior and anterior damage? The early cases also reported that damage was concentrated in the lingual and fusiform gyri. Reference Damasio, Damasio and van Hoessen5,Reference Meadows8 It is probable that such lesions affected the fusiform and/or occipital face areas that were later discovered with functional imaging. Reference Haxby, Hoffman and Gobbini9 This has been confirmed in modern studies that used functional MRI with single-subject methods to show loss of one or both of these areas in patients with such lesions. Reference Fox, Hanif, Iaria, Duchaine and Barton16,Reference Hills, Pancaroglu, Duchaine and Barton40,Reference Rossion, Caldara, Seghier, Schuller, Lazeyras and Mayer44 However, from the 1990s onward, reports of prosopagnosia with anterior temporal lesions emerged. Reference Evans, Heggs, Antoun and Hodges45–Reference Joubert, Felician and Barbeau47 While some reported no difference in the perceptual deficits between those with fusiform and those with anterior temporal lesions, Reference Busigny, Van Belle, Jemel, Hosein, Joubert and Rossion48 we found variations, as others had hypothesized. Reference Damasio, Tranel and Damasio49,Reference de Renzi, Faglioni, Grossi and Nichelli50 Those with fusiform lesions struggled to see the precise shape of faces, but this was less of a problem for those with anterior temporal lesions Reference Barton, Zhao and Keenan46 (Figure 2A). On the other hand, the latter had more trouble recalling the appearance of known faces on tests of imagery for famous faces. Reference Barton and Cherkasova51 In particular, those who performed no better than chance on imagery were more likely to have right anterior temporal lesions, often in combination with damage to bilateral occipitotemporal or left anterior temporal regions (Figure 2B). Conversely, those with normal imagery scores were more likely to have lesions limited to the occipitotemporal cortex.
Performance on face tests by 23 patients with acquired prosopagnosia, classified by lesion location. (A) Inverse efficiency scores, normalized by the performance of the control group, for the perception of face configuration (interocular distance and nose–mouth distance combined). (B) Error rate on the famous face imagery test. Both graphs are arranged so that worse performance corresponds to higher scores. The dotted lines show 95% prediction limits from the control group, while the dashed line in B shows the 95% limit for chance performance of 0.5: scores above this are no better than random guessing. Data compiled from Barton, 2008Reference Barton42 and Pancaroglu et al., 2016.Reference Pancaroglu, Hills, Sekunova, Viswanathan, Duchaine and Barton118
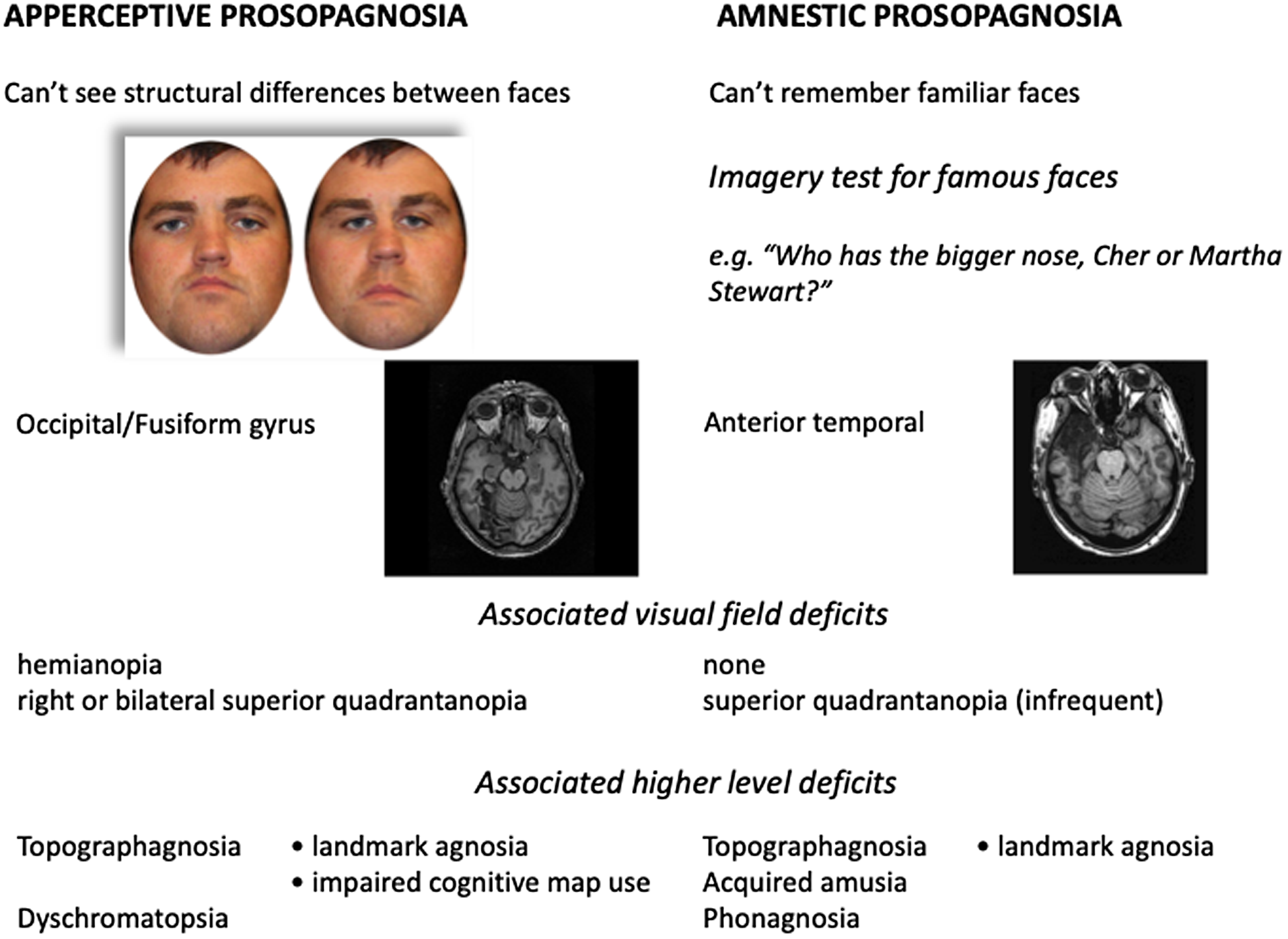
Hence, the structural distinction between fusiform and anterior temporal lesions maps reasonably to a functional distinction between apperceptive and amnestic variants of prosopagnosia (Figure 3). There is not a perfect correspondence, as mild imagery deficits are commonly seen in the former and mild perceptual inefficiencies in the latter. This is consistent with claims that apperceptive and amnestic deficits lie along a continuum Reference Damasio, Tranel and Damasio49 and that, as Lissauer originally noted for general visual agnosia, Reference Lissauer52 these distinctions are relative, not absolute. Reference Barton42 Nevertheless, the proposal that right anterior temporal lesions are required – though not always sufficient – for an amnestic variant implies that the representations of familiar faces are stored primarily in that structure. This has received support from recent work in rhesus monkeys that found cells that respond specifically to familiar faces in face-activated patches of the right temporal pole. Reference Landi, Viswanathan, Serene and Freiwald53
Summary of functional and structural differences for apperceptive and associative variants of prosopagnosia, including associated visual field defects and other high-level sensory deficits.
It has been argued that an associative form of prosopagnosia should have intact perception and intact memories yet fail to recognize faces because they cannot link the two. Reference Fox, Iaria and Barton30 As yet, we have not found a patient with acquired prosopagnosia who meets such strict criteria. However, a few patients with only right anterior temporal lesions come close, with only mild or no impairment in both perception and imagery.
Prosopagnosia is associated with other deficits in two syndromes
Human lesions are large. Vascular territories do not map onto the anatomic boundaries between one functional system and another, and tumors and infections do not respect sulcal or gyral divisions. It is no surprise that the damage that causes prosopagnosia will often affect adjacent neurologic circuits. The other functions that are impaired will be determined by this “neighbourhood principle.”
The tetrad of prosopagnosia, homonymous field defects, dyschromatopsia and topographic disorientation is well recognized. This was described even in the earliest cases Reference Della Sala and Young2,Reference Ellis and Florence33,Reference Pallis54 and later linked to bilateral fusiform damage. Reference Damasio, Damasio and van Hoessen5 It is a ventral occipitotemporal syndrome, in the same way that Bálint’s syndrome is a dorsal occipitoparietal syndrome. Both are syndromes in that not every patient will have all components of the syndrome – that will depend on variations in both individual anatomy and the location and size of the lesions. The frequent co-occurrence of these deficits is due to the anatomic proximity of the networks involved, not because one problem causes the others. This may seem obvious, but in Borelli’s commentary on Quaglino’s case, he speculated that impaired color vision was the reason why LL could not recognize faces or places. Reference Della Sala and Young2 Even now, one encounters prosopagnosic patients who erroneously assume that their struggles with face recognition are due to their hemianopia.
More details about this long-established tetrad have emerged. First, it is specific to the apperceptive variant of prosopagnosia, not surprising given that fusiform damage is involved. Second, the topographic disorientation has two components: poor place recognition and impaired cognitive map formation. Reference Corrow, Corrow and Lee55 Third, when the fusiform damage is bilateral, there may be a mild element of alexia, Reference Hills, Pancaroglu, Duchaine and Barton40 as indexed by an elevated word-length effect, the time needed to read a word as a function of the number of letters it contains. Reference Barton, Hanif, Eklinder Bjornstrom and Hills56 An occasional association with alexia is also consistent with earlier observations. Reference Ellis and Florence33
In contrast, anterior temporal lesions cause a different cluster of deficits (Figure 3). Dyschromatopsia is not a feature. Reference Moroz, Corrow, Corrow, Barton, Duchaine and Barton57 Field defects are less common despite the fact that Meyer’s loop is in the vicinity. Reference Barton, Hefter, Chang, Schomer and Drislane58 We found that only one of seven prosopagnosic patients with lesions limited to the anterior temporal lobes had an upper quadrantanopia – in contrast, only 1 of 12 patients with fusiform lesions alone had full visual fields. Patients with anterior temporal lesions get lost in familiar places too, but their topographic problems are due to place agnosia only, not impaired use of cognitive maps. Reference Corrow, Corrow and Lee55 A more distinctive difference is the presence of auditory deficits, reflecting the fact that the anterior temporal cortex is a multimodal sensory convergent zone. Those with bilateral lesions may be impaired in recognizing voices as well as faces, a deficit called “phonagnosia.” Reference Liu, Pancaroglu, Hills, Duchaine and Barton59 These patients still retain a store of biographic information about people, which distinguishes them from patients with a multimodal person recognition disorder, or “people-specific amnesia,” Reference Gainotti60–Reference Hanley, Young and Pearson62 Some also have acquired amusia, or tone deafness, with altered esthetic musical experiences, either musicophilia or its opposite, anhedonia. Reference Barton, Stubbs, Paquette, Duchaine, Schlaug and Corrow63 This may account for occasional reports from the pre-imaging era of patients who also lost the ability to sing or recognize music when they developed prosopagnosia. Reference Shuttleworth, Syring and Allen64 With our patients these auditory deficits were not mentioned spontaneously, and more sensory deficits may await characterization in this group – consider, for example, the description of an impairment in yet another modality, an agnosia for odors that accompanied prosopagnosia in a man with progressive bitemporal atrophy. Reference Mendez and Ghajarnia65
Not all agnosia in prosopagnosia is face-related
Unlike patients with general visual agnosia, prosopagnosic subjects do not mistake wives for hats. They know that a face is a face, a hat is a hat and a car is a car. What they cannot tell is whose face this is, and the natural question then is whether they can tell which hat and which car. For decades, people have argued about whether prosopagnosia is specific to faces – for a review, see.Reference Barton and Corrow66 For every report of a prosopagnosic patient who could recognize birds, dogs, butterflies, fruits, vegetables, cars or tools, there is a countering article about another whose recognition troubles included one or more of these other objects. This speaks to a larger issue, about whether visual processing in the human brain is modular or distributed. The modular view proposes that at least some components of the network involved in face recognition process faces alone, Reference Kanwisher67 whereas the distributed view argues that no region is dedicated to a single object. Reference Behrmann and Plaut68
The contribution of prosopagnosia to this debate is time-honored but complicated. The large scale of human pathology means that, if non-face object modules are close to face modules, there is a high chance that they will be damaged too. If so, problems with recognizing other objects will often accompany prosopagnosia, even if face processing is accomplished by a dedicated face module. One could argue that the discovery of a single patient with completely intact recognition of non-face objects would settle the argument, but exactly how does one show “completely intact recognition”?
A review of the studies of object recognition in developmental prosopagnosia Reference Geskin and Behrmann69 and its accompanying commentaries grappled with the difficulties involved. These were summarized later as 11 points that studies should consider, Reference Barton, Albonico, Susilo, Duchaine and Corrow70 such as firm diagnostic criteria, Reference Barton71 assessing reaction time as well as accuracy, showing putative classical dissociations, Reference Gerlach, Lissau and Hildebrandt72 testing equivalent processing stages, matching for test difficulty, Reference Campbell and Tanaka73 matching the number of exemplars in the decision space Reference Ramon74 and testing of at least three categories of objects.
One especially challenging task is accounting for variations in premorbid expertise for different types of objects. Recognition abilities depend not just on prior exposure but also on interest. While we assume that most humans have a similar interest in recognizing faces, this cannot be assumed for most other objects. Consider two hypothetical prosopagnosic patients: subject A, who has no interest in automobiles, and subject B, who is a car buff. Cars are a good category because all people in modern society are exposed to them on a daily basis. If we ask these subjects to name the car in Figure 4A, answering “Porsche” may be a sign of intact car recognition in subject A. However, we would expect subject B to do better, to say that it is a 911, perhaps more specifically the 964 variant, and judging by the wheels, a 1994 model. If subject B can only say “Porsche,” we would be concerned that something is amiss.
(A) What car is this? How precise an answer you can give depends on your perceptual expertise. (Answer: Porsche 911, 964 Targa variant, 1994 model year) (B) Expertise-indexed test of car recognition. The proportion of a set of 150 pictures of cars that were correctly named by a subject is plotted as a function of their score on a verbal semantic test, which asked them to match the manufacturer to a named model (e.g., Pinto, answer: “Ford”). In control subjects, these abilities are highly correlated (small gray dots, r = 0.91). With one exception, the nine prosopagnosic patients tested (large black discs) recognized fewer cars than predicted from their verbal semantic score. Data compiled from Barton et al., 2009Reference Barton, Hanif and Ashraf75 and Davies-Thompson et al., 2014.Reference Davies-Thompson, Pancaroglu and Barton119
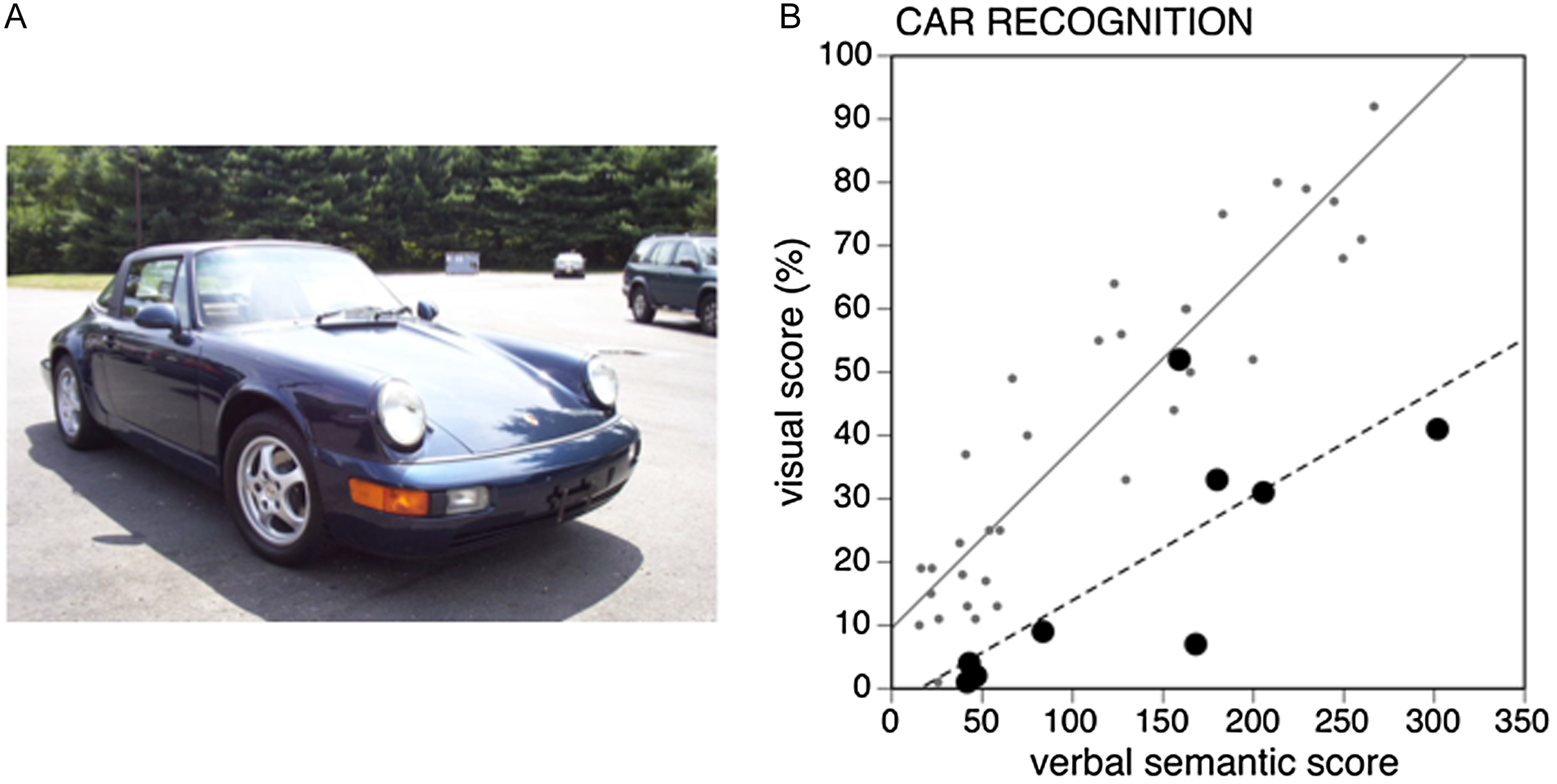
To take into account premorbid expertise, we devised a comparison between verbal semantic knowledge about cars – reasoning that semantic knowledge should be intact in prosopagnosia – and visual car recognition. Reference Barton, Hanif and Ashraf75 The two are highly correlated in healthy subjects, with an r of 0.91. This allowed us to predict how many of the 150 car images a given prosopagnosic patient should recognize on the basis of their verbal knowledge, knowing that the Pinto was made by Ford, for example. We found poorer car recognition than expected in almost all prosopagnosic patients, and this was particularly clear in those who were car experts. Reference Barton and Corrow66,Reference Barton, Albonico, Susilo, Duchaine and Corrow70,Reference Barton, Hanif and Ashraf75
However, the car is only one type of object. We supplemented this expertise-adjusted car test with two other probes, the Old/New Test, Reference Duchaine and Nakayama76 which includes subtests for cars, guns, horses and glasses, and the Cambridge Bicycle Memory Test, Reference Dalrymple, Garrido and Duchaine77 which uses the same format as the Cambridge Face Memory Test. We found that none of the 15 patients with acquired prosopagnosia (and only 1 of the 12 with developmental prosopagnosia) had conclusive evidence for intact non-face object recognition across all three tests. Reference Barton, Albonico, Susilo, Duchaine and Corrow70
One special class of objects is visual text. People in literate societies also have universal exposure to and interest in written words. Like face recognition, reading is considered an expert visual process. In fact, the bilateral networks for text and face perception overlap each other, Reference Nestor, Behrmann and Plaut41 with the key difference being that reading generates stronger activation in the left hemisphere while face recognition emphasizes the right. The left visual word form area occupies a region that is almost the mirror location of the right fusiform face area, underscoring the concept of the fusiform gyrus as a key structure in expert visual perception. Reference Weiner and Zilles78 Not surprisingly, prosopagnosic subjects with bilateral fusiform lesions have an elevated word-length effect, indicating a mild degree of alexia. However, prosopagnosic patients with right unilateral lesions – either anterior temporal or fusiform – do not show any difficulty in reading. Reference Hills, Pancaroglu, Duchaine and Barton40,Reference Duchaine, Susilo, Wright and Tree79 Rather, all but 1 of the 11 prosopagnosic patients in our study struggled to identify the handwriting or the font of the text. Reference Hills, Pancaroglu, Duchaine and Barton40,Reference Barton and Corrow66 Hence, the right hemisphere appears to contain a network that is important for decoding identity information in text, just as it has a network for identifying faces, but is less involved in reading text.
Not all face deficits are confined to prosopagnosia
If the recognition difficulties of many prosopagnosic patients extend to other objects besides faces, it is also true that these difficulties sometimes spare other types of facial information besides the identity of the person. Like many complex objects, faces convey a wide range of information, including gender, emotional state, age and attractiveness. Cognitive models of face perception proposed that dynamic information such as expression is processed separately from the static structural data upon which most judgments of face identity are based. Reference Bruce and Young3 However, a few early studies disagreed on (a) the type of anatomic damage that impaired the perception of facial expression Reference Kurucz, Soni, Feldmar and Slade80–Reference Adolphs, Damasio, Tranel and Damasio82 and (b) whether prosopagnosic patients were impaired in perceiving expression as well as identity – for review, see.Reference Fox, Hanif, Iaria, Duchaine and Barton16 New data from functional imaging then emerged, suggesting that the superior temporal sulcus played a key role in processing facial expression. Reference Haxby, Hoffman and Gobbini9,Reference Winston, Henson, Fine-Goulden and Dolan83,Reference Fox, Moon, Iaria and Barton84 A study using morphed faces as stimuli found intact perception of facial expression in four prosopagnosic patients, all of whom had preserved face-related activation of the right posterior superior temporal sulcus, while one patient with a lesion that eliminated this area – but spared the right occipital and fusiform face areas – was impaired in expression but not identity perception. Reference Fox, Hanif, Iaria, Duchaine and Barton16
Clearly, more work on expression deficits remains to be done. Studies of other social signals have yielded mixed results in prosopagnosic patients, with some finding variably preserved judgments of trustworthiness, attractiveness and aggression Reference Rezlescu, Susilo, Barton and Duchaine85 and others a reduced sense of facial attractiveness. Reference Iaria, Fox, Waite, Aharon and Barton86
Lip-reading is another task with faces that raises interesting questions about the lateralization of function. On the one hand, it involves faces, and faces have a network that is more active in the right hemisphere. On the other hand, it contributes to linguistic operations, which in most people are located in the left hemisphere. Lip-reading has been studied in a patient with prosopagnosia after a right posterior cerebral artery stroke and another with pure alexia after a left occipitotemporal stroke Reference Campbell, Landis and Regard87,Reference Campbell, Garwood, Franklin, Howard, Landis and Regard88 and, more recently, in four patients with pure alexia and one prosopagnosic patient, all with unilateral lesions. Reference Albonico and Barton89 Though small in number, the results are consistent. Neither of the two prosopagnosic patients had difficulty in lip-reading, while all five of the patients with pure alexia were impaired.
The poor lip-reading of alexic patients caused interesting anomalies in the McGurk effect. Reference McGurk and MacDonald90 This effect occurs when subjects see a face pronouncing one syllable while at the same time hearing a voice pronouncing a different one: subjects typically report perceiving a syllable that is a blend of the two. The pure alexic subjects failed to report either the blend or the visually presented syllable, but the subjects with acquired prosopagnosia performed normally.
From these observations, lip-reading appears to lateralize to the left. This is consistent with tachistoscopic reports of a right hemifield advantage for lip-reading Reference Campbell, De Gelder and De Haan91 and functional imaging studies showing that activity in the left superior temporal sulcus correlates with lip-reading proficiency Reference Hall, Fussell and Summerfield92 and the McGurk effect. Reference Nath and Beauchamp93
Both the results for lip-reading and those for handwriting and font identification make the same point: it is not the stimulus that is lateralized but the nature of the operation being performed. Prosopagnosic patients with right hemisphere lesions have trouble identifying not only faces but also handwriting and font, though they can read text and can lip-read with faces. Alexic patients with left fusiform lesions have almost the converse: they cannot do the linguistically directed tasks of reading text or lips, but they can identify faces. What we do not know yet is how they are with identifying handwriting or font.
Face recognition in prosopagnosia is malleable and can be trained
The preceding observations contribute to our understanding of neurologic structure and function, but on a practical level, can we fix prosopagnosia? With the exception of rare cases with resolution after small strokes or migraine Reference Martins and Sá94–Reference Koh96 – which admittedly may be underreported – most patients are likely to have prosopagnosia permanently. Most of the prosopagnosic patients studied have had the condition for months to years. While many are resourceful in finding strategies to work around their face recognition problems, they may still experience social difficulties. This has been studied best in subjects with developmental prosopagnosia, who report anxiety in social situations that can lead to avoidance behavior. Reference Yardley, McDermott, Pisarski, Duchaine and Nakayama97
Early studies of single cases or small series tried a variety of strategies, as recently summarized. Reference Dalrymple, Fletcher and Corrow98–Reference Bate and Bennetts100 These included creative approaches such as trying to convert covert into overt recognition, Reference Davies-Thompson, Fletcher, Hills, Pancaroglu, Corrow and Barton101 learning of face-name associations, Reference de Haan, Young and Newcombe102,Reference Powell, Letson, Davidoff, Valentine and Greenwood103 employing the tricks of professional mnemonists Reference Ellis and Young104 or emphasizing the recognition of facial features. Reference de Haan, Young and Newcombe102,Reference Francis, Riddoch and Humphreys105,Reference Beyn and Knyazeva106 The results have been mixed. Reference Bate and Bennetts100 The studies are also difficult to compare given the variations in training techniques and the means used to assess efficacy and because these studied single subjects for the most part.
To advance upon this situation, we performed a randomized online training study in a cohort of 10 patients with acquired prosopagnosia. Reference Bate and Bennetts100 The 10 were divided into 2 groups matched approximately for lesion location. One started with the training protocol and the other with a control condition, namely, watching British murder mysteries. We employed a perceptual learning technique. Reference Mayer, Rossion, Godefroy and Bogousslavsky107 This used a large volume of repetitive sensory training with feedback over 11 weeks. On each trial, a subject saw a target face, below which were two images, each made by morphing a variable degree between this target face and another face. The task was to choose which of the two was most similar to the target face. Initially, the difference between the two choice faces was set quite large, and the answer was obvious. With every correct response, the physical differences between the two choice faces were lessened until the subject was training at a level where they were getting about 85% correct. As training progressed, subjects began to perceive subtler differences. Once they achieved a learning criterion, they moved on to blocks with variable viewpoint, then variable expression, then variations in both viewpoint and expression, with the aim of learning the three-dimensional aspects of facial structure that would apply to real-life situations.
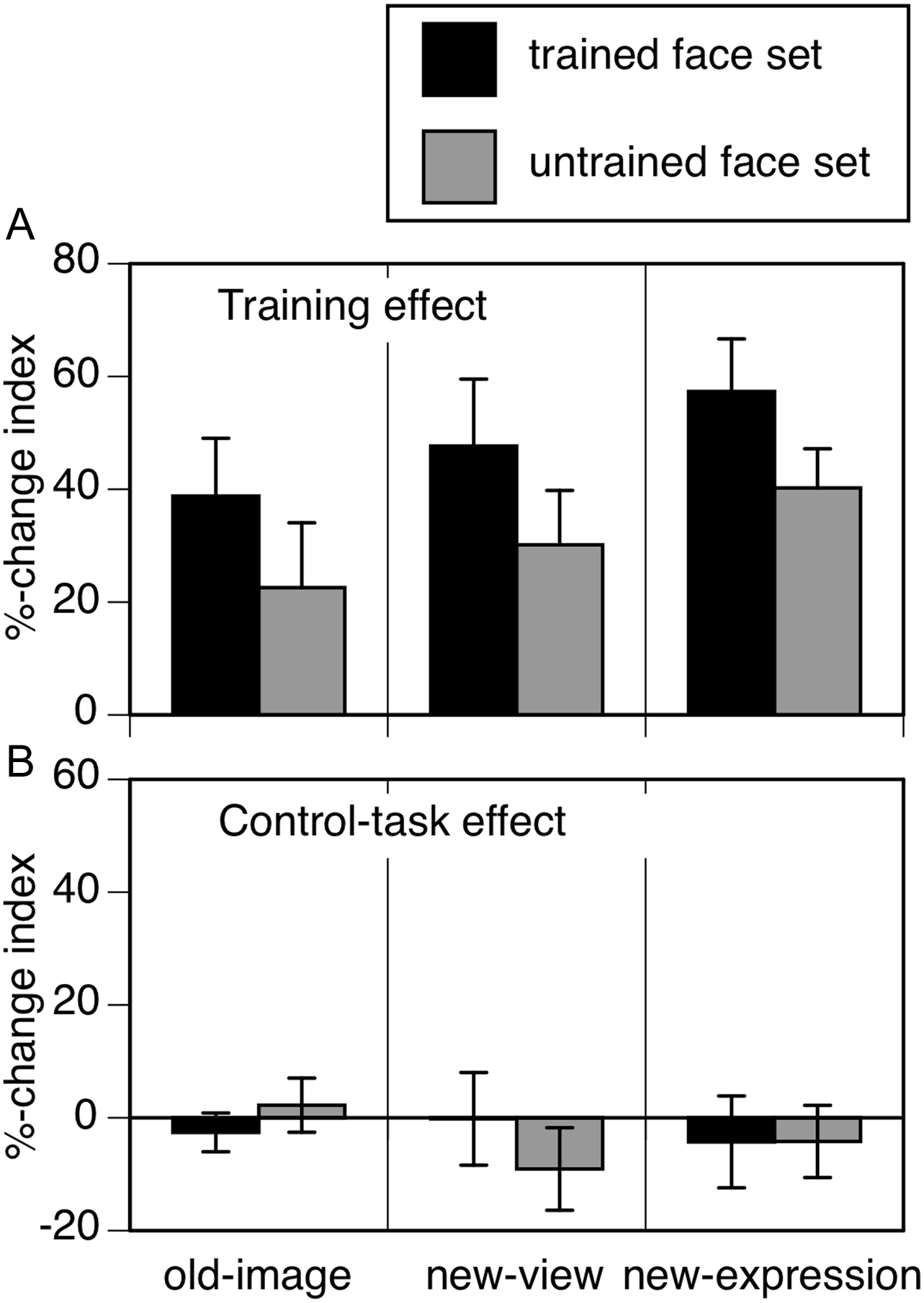
The result was a 39% improvement in subjects’ ability to see facial structure (Figure 5). Critically this improvement generalized to viewpoints and expressions that hadn’t been used in training. It also “transferred,” in that there was a 30% improvement for faces of new people not seen in training. Thus, subjects were not just doing better with a set of trained faces to which they had massive exposure, but they had learned a skill that could be applied to new faces. This effect was still apparent 3 months later. It is unclear how best to assess whether benefits from training impact face recognition in daily life, but some subjects related positive anecdotes about their experience with family and friends, though others did not.
Training the face perception of prosopagnosic patients. Subjects performed 11 weeks of daily work with a perceptual learning method. Graphs show the percent change from their test performance before training. After training (A), there is a nearly 40% improvement with the same types of images used in training (black bar in “old image”). The improvement does “generalize” to new views and new expressions of the same faces that had not been seen during training. Also, when tested on a set of faces from different people, there is “transfer” of benefit (gray bars, untrained face set). No benefit is seen after the control task (B), which provided exposure to faces but not feedback or a formal training structure. Data from Davies-Thompson et al., 2017.Reference Davies-Thompson, Fletcher, Hills, Pancaroglu, Corrow and Barton101
The same protocol improved face perception in a cohort of 10 subjects with developmental prosopagnosia, Reference Ahissar and Hochstein108 and other training studies have yielded positive results with the developmental variant. Reference Corrow, Davies-Thompson, Fletcher, Hills, Corrow and Barton109–Reference Bate, Adams and Bennetts111 Such findings indicate that face perception is malleable and can be improved in prosopagnosia. However, the current methods lead only to partial benefits and clearly do not “cure” the condition. In the future, refinements of these protocols and combination with techniques that promote cerebral network plasticity may yield even better results.
Summary
Reports of acquired prosopagnosia have been an invaluable complement to the studies of face perception in healthy subjects, investigations of the functional anatomy of the face network and electrophysiological work in nonhuman primates. As with any complex cognitive process, face recognition has component operations, and this fact is reflected in variants of prosopagnosia that correspond to lesions of different cerebral regions. These variants are marked clinically by associations with other perceptual deficits that form syndromes, one with occipitotemporal damage and one with anterior temporal lesions. Whether faces have a special modular status in visual processing continues to be debated. Acquired prosopagnosia is frequently accompanied by problems with recognition of other objects, particularly once the variability of human expertise with the latter is taken into account. On the other hand, the prosopagnosic deficit does not extend to all aspects of face perception. It is also not a fixed deficit but can be improved by training, which opens the possibility of rehabilitation.
Future directions promise interesting new developments. Most people are aware of the use of artificial intelligence to perform face recognition in forensic and commercial settings. More recent work in this area is starting to ask how well artificial neural networks can replicate the various properties of human face processing and provide insights into how our brains achieve this feat. Reference Bate, Dalrymple and Bennetts112–Reference O’Toole and Castillo114 While functional MRI was initially applied to human face networks, it is now being combined with electrophysiological techniques in nonhuman primates, where this has revealed a network of interconnected face patches extending from the posterior occipital to anterior temporal regions. Reference van Dyck and Gruber115,Reference Hesse and Tsao116 A major goal will be to understand the roles of these different patches and their interactions. Observations from these approaches will refine our understanding of prosopagnosia and clarify several theoretically important questions about its basis and the nature of visual processing in the human brain.
Acknowledgments
I thank the many students who performed the studies described and partnering colleagues, especially Brad Duchaine.
Author contributions
As the sole author, JB is responsible for all aspects of authorship of this manuscript.
Funding statement
I was supported by a Canada Research Chair (950-202111, 950-228984 and 950-232752) and the Marianne Koerner Chair in Brain Diseases. Over these years, the prosopagnosia project was supported by operating grants MOP-77615, MOP-85004, MOP-102567 and MOP-102567 from the Canadian Institutes of Health Research and 1R01 MH069898 from the National Institute of Mental Health, USA.
Competing interests
None.






 Open access
Open access