Metabolic syndrome (MetS) is a disorder defined by a cluster of metabolic abnormalities encompassing hypertension, central obesity, insulin resistance and atherogenic dyslipidaemia(Reference Rochlani, Pothineni and Kovelamudi1). MetS is a major public health concern as a significant risk factor for cardiovascular atherosclerotic diseases and type 2 diabetes(Reference Grundy, Brewer and Cleeman2). Several definitions of the MetS exist with obesity, insulin resistance/hyperglycaemia and dyslipidaemias as common components differing in cut-off points for each component. The WHO definition was better suited as a research tool, whereas the National Cholesterol Education Program definition was more useful for clinical practice(Reference Deepa, Farooq and Datta3). The International Diabetes Federation produced a new set of criteria that can be used both epidemiologically and in clinical settings, compensating for differences in waist circumference and in regional adipose tissue distribution between different ethnic populations(Reference Zimmet, Alberti and Ríos4,Reference Mainuddin, Choudhury and Ahmed5) . Globally, the prevalence of MetS as defined by the WHO and the National Cholesterol Education Program varies widely among countries and ethnic groups, ranging from 1 to 39 %(Reference Zimmet, Alberti and Ríos4–Reference Laaksonen, Niskanen and Lakka6). Looking at the literature, the prevalence of MetS is higher using the International Diabetes Federation criteria followed by the WHO and then the National Cholesterol Education Program. This variation is probably due to the lower cutoff of the waist circumference (WC) and the fasting glycaemia established by them. Moreover, MetS is common in several rapidly developing countries in the Middle East, affecting about one in four individuals(Reference Sliem, Ahmed and Nemr7,Reference Saad, Cardoso and Martins8) .
Among its neighbouring countries, Lebanon, a small middle-income country in the Eastern Mediterranean Region, has a prevalence range of 31·2 % to 34·6 % of MetS among adults using the International Diabetes Federation criteria, with males presenting with a significantly higher rate than females(Reference Sibai, Obeid and Batal9). Consequently, cardiovascular diseases, diabetes and chronic disease risk factors, including obesity, have already emerged as the leading causes of morbidity and mortality in the country(Reference Sibai, Fletcher and Hills10).
Irritable bowel syndrome (IBS) is defined as a chronic disorder of the gastrointestinal tract that is diagnosed clinically and manifested by abdominal pain and shifts in bowel habits(Reference Horwitz and Fisher11). Individuals suffering from IBS struggle with the adverse effects that this condition imposes on their overall quality of life(Reference Weaver, Melkus and Fletcher12). There are three main types of IBS with either predominantly diarrhoea, constipation or both(Reference Manrique13). Depending on the diagnostic criteria employed, IBS affects around 11 % of the population globally, with variation by geographic region; the lowest occurring in South Asia (7·0 %) and the highest in South America (21·0 %)(Reference Lovell and Ford14). It is plausible that the underlying prevalence of symptoms in communities internationally is the same, but the variations reflect differences in access to health care(Reference Haas, Phillips and Sonneborn15), acceptability of the diagnosis(Reference Quigley, Bytzer and Jones16) and the significant stigma that is associated with it(Reference Jones, Keefer and Bratten17). Studies in the Arab world are relatively scarce but show comparable results to Western countries(Reference Almansour18). Furthermore, looking at the Middle East and specifically Lebanon, data reveal a prevalence of 20·1 % of IBS among adults and university students(Reference Costanian, Tamim and Assaad19,Reference Yazbeck, Malaeb and Shaaban20) .
Despite the rising prevalence of MetS and IBS, the evidence of their association remains inconsistent. IBS may affect dietary patterns, food digestion and nutrient absorption. These nutrition-related factors are closely related to MetS, implying that IBS may be a potential risk factor for MetS(Reference Guo, Niu and Momma21). On the other hand, IBS is independently related to a higher prevalence of MetS and elevated TAG that may be linked to the pathogenesis of gastrointestinal disorders(Reference Vich Vila, Imhann and Collij22). Gut dysbiosis is one of the significant factors in IBS that may influence the host’s immune responses and energy homeostasis in the body, causing an upstream regulation of inflammatory cascades, insulin resistance and impairment of the body’s metabolism(Reference Bayrak23), exacerbating MetS.
Research on this association of IBS with MetS within the Middle Eastern and Arab region, specifically Lebanon, is limited. The objective of this study is to investigate the association between MetS and IBS in a sample of Lebanese adults. Considering the unique socio-demographic and lifestyle characteristics of this population group, this study might help in highlighting some valuable insights into the relationship between these two prevalent conditions.
Materials and methods
Design
This was a cross-sectional study.
Subjects
Community announcements were used to invite Lebanese adults, aged 18–65 years, to participate in this study. Participants were asked to come to the data collection clinic fasting for at least 8 h. Additional inclusion criteria included being aged between 18 and 65 years of Lebanese nationality, free of self-reported active infections including COVID-19, not pregnant nor lactating and not on anti-tuberculosis drugs. The participants signed a written consent form after the study objectives and the right to withdraw at any time were explained.
Data collection – questionnaires
Socio-demographic characteristics and medical history information were collected through questionnaires and included sixteen questions related to age, sex, educational level, employment status and smoking status. Questions related to personal and family medical history of chronic diseases were also included.
Anthropometric measurements were collected and included height (cm) measured using a portable stadiometer, weight (kg) measured using a beam scale, BMI (kg/m2) calculated as the ratio of weight divided by the squared height in meters (m2) and WC (cm) measured to the nearest 0·1 cm at the mid-point, halfway between the right iliac crest and the lower costal region using standardised measuring tape.
Birmingham IBS scale
This self-administered eleven-item symptom questionnaire assesses IBS-related symptoms in the previous 4 weeks based on the Rome II criteria, with each question having a standard response scale. Symptoms are measured based on a six-point Likert scale (0–5) ranging from all of the time to none and converted to 100. The scale has three dimensions, including pain, constipation and diarrhoea, and is designed to enable assessment of symptom burden. This scale has a high internal validity (Cronbach’s α of 0·74 for pain, 0·79 for constipation and 0·90 for diarrhoea) and good external validity (r = −0·3 to −0·6) for pain and diarrhoea and moderate external validity (r = −0·2 to −0·3) for constipation, with all dimensions being reproducible (intraclass correlation coefficient 0·75 to 0·81)(Reference Roalfe, Roberts and Wilson24).
Mediterranean Diet Adherence Screener
Adapted from PREvencion con DIetaMEDiterranea (PREDIMED)(Reference Martínez-González, García-Arellano and Toledo25), this fourteen-item questionnaire aims to assess food intake or frequency of foods in favour of the Mediterranean diet. Responses that support the Mediterranean diet receive a score of 1, while those that do not receive a score of 0. The overall score is determined by adding up all the responses to the fourteen questions. The resulting score ranges from 0 to 14, with higher scores indicating a greater adherence to the Mediterranean diet. Mediterranean Diet Adherence Screener is a commonly used tool to assess adherence to the Mediterranean Diet that has been validated by several studies(Reference Bekar and Goktas26,Reference García-Conesa, Philippou and Pafilas27) .
The Birmingham IBS scale and Mediterranean Diet Adherence Screener were translated to Arabic following the best practices, i.e. forward translation to Arabic, then back translation to English by two independent translators. The translation also ensured that participants of all levels of literacy could respond(28). The questionnaire was pilot-tested on ten adults prior to data collection; feedback from the pilot was used to produce the final version of the questionnaire. In this study, the Cronbach alpha for the Birmingham IBS scale and Mediterranean Diet Adherence Screener were 0·794 and 0·218, respectively.
The International Physical Activity Questionnaire short form
The validated Arabic version of the questionnaire was used. International Physical Activity Questionnaire-Short Form includes seven questions regarding the duration and frequency of light, moderate and vigorous physical activity performed in the past week. The metabolic equivalent of tasks is calculated by multiplying the total minutes expended in a certain activity by the frequency (days) by the constants of 3·3, 4·0 and 8·0 for light, moderate and vigorous activity, respectively. The total metabolic equivalent of task values is calculated by totalling the respective metabolic equivalent of task values for all activities that were performed in periods that were more than 10 min in duration(Reference Craig, Marshall and Sjöström29). The International Physical Activity Questionnaire has been validated in Lebanon showing a high internal consistency (reliability) and intraclass correlation coefficient(Reference Helou, El Helou and Mahfouz30).
The Pittsburgh Sleep Quality Index
This questionnaire consists of nine questions, four of which assess sleep duration (hours), duration needed to fall asleep, amount of time required to wake up and time spent in bed while awake. The five other questions assess reasons for sleep troubles. A total score is computed using an algorithm adapted from the developers of the questionnaire. Higher scores (≥ 5) indicate poor sleep quality(Reference Buysse, Reynolds and Monk31). The Pittsburgh Sleep Quality Index was validated in Arabic, showing acceptable reliability and a high convergent validity with the Insomnia Severity Index(Reference Suleiman, Yates and Berger32). The Arabic version of Pittsburgh Sleep Quality Index which was culturally adapted by Haidar et al.(Reference Haidar, de Vries and Papandreou33) was used.
The ten-item Cohen Perceived Stress Scale
This ten-item questionnaire assesses stress levels in the previous month by investigating feelings for which respondents find their life situations unpredictable, uncontrollable or stressful. Answers use a five-point scale ranging from never (0) to very often (4), with a total score ranging from 0 to 40, with higher scores indicating higher perceived stress(Reference Cohen, Williamson, Spacapam and Oskamp34,Reference Roberti, Harrington and Storch35) . The Perceived Stress Scale shows satisfactory validity and reliability(Reference Lee36). The Arabic version of the questionnaire validated by Chaaya et al. (2010)(Reference Chaaya, Osman and Naassan37) was used.
Diagnosis of the metabolic syndrome
MetS was diagnosed using the International Diabetes Federation criteria(Reference Alberti, Zimmet and Shaw38). Participants were considered to have MetS if they had central obesity (≥ 94 cm males and ≥ 80 cm or BMI > 30 kg/m2) and two of the following factors: elevated TAG (≥ 150 mg/dl) or being treated for it; low HDL-cholesterol (< 40 mg/dl in males and < 50 mg/dl in females) or being treated for it; high BP (SBP ≥ 130 or DBP ≥ 85 mmHg) or being treated for hypertension and Fasting blood glucose (FBG) ≥ 100 mg/dl or were diagnosed with type 2 diabetes.
Statistical analysis
The data were analysed using SPSS, version 25. A descriptive analysis was done using the counts and percentages for categorical variables and mean and standard deviation for continuous measures. Normality distribution was checked using visual inspection of the histogram and verified by checking the normality line of the regression plot and the scatter plot of the residual. Independent-sample t test was used to compare the mean of the Birmingham IBS symptom questionnaire and subscales (pain, constipation and diarrhoea) between two groups, whereas ANOVA test was used to compare three or more means. Pearson correlation test was used to evaluate the association between continuous variables and the Birmingham IBS symptom questionnaire and each of the subscales (pain, constipation and diarrhoea). Four multivariable linear regression analyses using the Enter method were performed, taking respectively the Birmingham IBS symptom questionnaire total scale and each of the subscales (pain, constipation and diarrhoea) as the dependent variable. Covariates were informed by the literature and following a purposeful bivariate analysis, whereby variables showing a P-value less than 0·2 were included in the regression models as independent variables. Selecting variables with a P-value < 0·2 in the bivariate analysis for entry into the regression models was adopted to ensure potentially relevant variables were not prematurely excluded during the initial stages of model building. Those variables with modest associations (P-values between 0·05 and 0·2) in bivariate analysis might have higher associations when included in the multivariate model(Reference Bendel and Afifi39,Reference Mickey and Greenland40) . P-value less than 0·05 was considered significant.
Sample size calculation
Sample size calculation was performed using G * Power 3.1.9.7 software to detect a mean difference of IBS total score between those having or not having a MetS. Based on a medium effect size (Cohen’s d = 0·5), an α level of 0·05, and a power of 0·80, a minimum sample needed was 128 participants(Reference Cohen41,Reference Lakens42) .
Result
Sample description
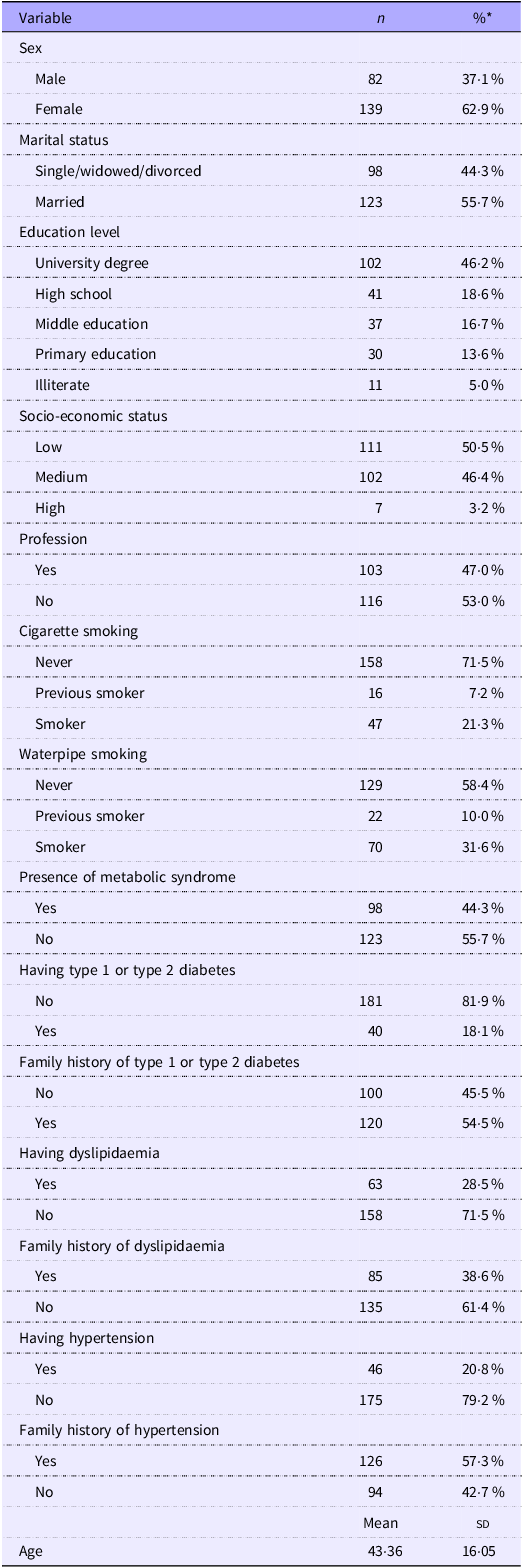
The socio-demographic and other characteristics of the participants are displayed in Table 1. A total of 230 participants were enrolled in the study. The majority of participants were female (62·9 %), and more than half of them were married (55·7 %), had a low socio-economic status (50·5 %), do not have any profession (53·0 %) and 46·2 % have a university degree. The majority of the participants do not smoke cigarettes (71·5 %) and 58·4 % of them do not smoke the water pipe. The presence of MetS was found in 44·3 % of the participants, and only 18·1 % have diabetes, 28·5 % have disorders of lipid metabolism and 20·8 % have hypertension. More than half of the participants have a family history of diabetes (54·5 %) and hypertension (57·3 %). The participants’ average age was 43·36 ± 16·05 years.
Socio-demographic and other characteristics of the participants (n 221) (Numbers and percentages; mean values and standard deviations)

* Valid percentages are presented.
Description of the visual analogue scale for irritable bowel syndrome
Table 2 describes the median, mean, sd and range of the scales used in this study. The mean Visual Analogue Scale (VAS)–IBS total scale was 16·98 ± 15·16 with a median of 14·54 and a range from 0 to 100.
Description of the VAS for irritable bowel syndrome (n 221) (Mean values and standard deviations)

VAS, Visual Analogue Scale; IBS, Irritable Bowel Syndrome.
Correlates of the IBS total scale and subscales
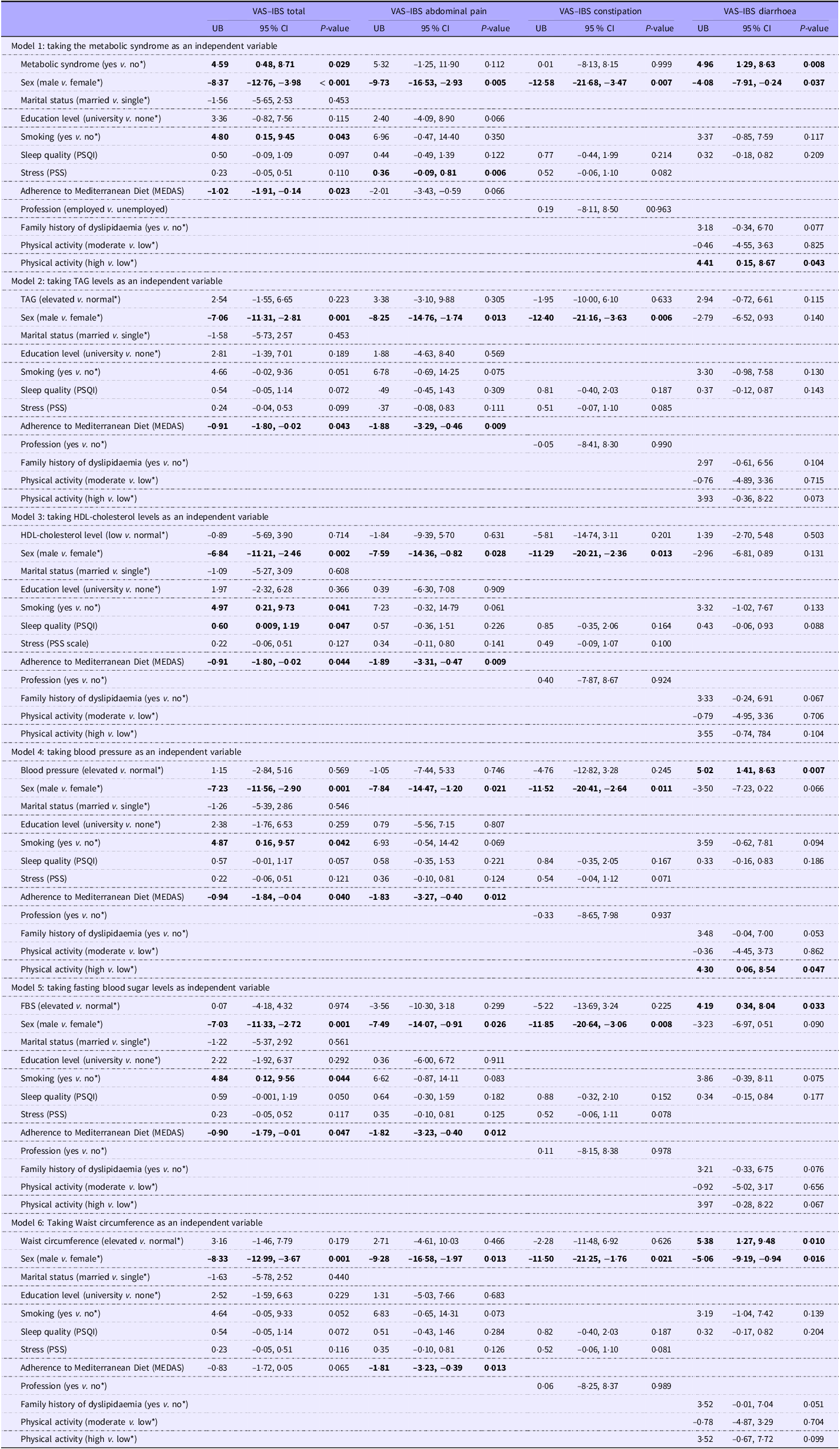
The bivariate analysis, using the IBS total scale and subscales as dependent variables, is displayed in Appendix 1. Linear regression models take the IBS total scale and subscales as the dependent variables. The analysis presented in Table 3 was adjusted over the following variables: sex, marital status, education level, profession, family history of dyslipidaemia, physical activity, smoking, sleep quality, stress and adherence to the Mediterranean diet.
Linear regression analysis taking irritable bowel syndrome as the dependent variables

VAS, Visual Analogue Scale; IBS, Irritable Bowel Syndrome; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale; MEDAS, Mediterranean Diet Adherence Screener; FBS, fasting blood glucose.
Numbers in bold indicate statistical significance.
* Reference category.
In the first model, considering MetS as the independent variable, MetS was positively associated with the VAS–IBS total scale (Beta = 4·59, P = 0·029) and the VAS–Diarrhoea subscale (Beta = 4·96, P = 0·008). Being a male was negatively associated with the VAS–IBS total scale and subscales. Being a smoker was positively associated with the VAS–IBS total scale (Beta = 4·80, P = 0·043); however, higher adherence to the Mediterranean diet was negatively associated with the VAS–IBS total scale (Beta = −1·02, P = 0·023). A significantly higher stress scale was positively associated with the VAS–abdominal pain subscale (Beta = 0·36, P = 0·006). Also, a high level of physical activity was positively associated with the VAS–Diarrhoea subscale (Beta = 4·41, P = 0·043) (Table 3, Model 1).
For model 2, considering TAG levels as an independent variable, male sex was negatively associated with the VAS–IBS total scale, the VAS–Abdominal pain and the VAS–constipation subscales. In addition, adherence to the Mediterranean diet was negatively associated with the VAS–IBS total scale and the VAS–Abdominal pain subscale (Table 3, Model 2).
In the third model, when considering HDL levels as the independent variable, male sex was negatively associated with the VAS–IBS total scale, the VAS–Abdominal pain and the VAS–Constipation subscales. Being a smoker (Beta = 4·97, P = 0·041) and having a lower sleep quality (Beta = 0·60, P = 0·047) were positively associated with the VAS–IBS total scale. Finally, higher adherence to the Mediterranean diet was negatively associated with the VAS–IBS total scale and the VAS–Abdominal pain subscale (Table 3, model 3).
In the fourth model, taking blood pressure as the independent variable, elevated blood pressure was positively associated with the VAS–IBS Diarrhoea subscale (Beta = 5·02, P = 0·007). Being a smoker (Beta = 4·87, P = 0·042) was positively associated with the VAS–IBS total scale, and high physical activity (Beta = 4·30, P = 0·047) was positively associated with the VAS-Diarrhoea subscale. In addition, higher adherence to the Mediterranean diet was negatively associated with the VAS–IBS total scale and the VAS–Abdominal pain subscale (Table 3, Model 4).
In the fifth model, considering fasting blood glucose as the independent variable, elevated fasting blood glucose (Beta = 4·19, P = 0·033) was positively associated with the VAS–Diarrhoea subscale. Male sex was positively associated with the VAS–IBS total scale, the VAS–Abdominal pain subscale, and the VAS–constipation subscale. Being a smoker (Beta = 4·84, P = 0·044) was positively associated with the VAS–IBS total scale; in contrast, higher adherence to the Mediterranean diet was negatively associated with the VAS–IBS total scale and the VAS–Abdominal pain subscale (Table 3, Model 5).
Finally, in the sixth model, taking WC as the independent variable, elevated WC (Beta = 5·38, P = 0·010) was positively associated with the VAS–Diarrhoea subscale. Male sex was positively associated with the VAS–IBS total scale and subscales. On the other hand, higher adherence to the Mediterranean diet (Beta = −1·81, P = 0·013) was negatively associated with a lower VAS–Abdominal pain subscale (Table 3, Model 6).
Discussion
Through this cross-sectional study, we explored the association between the MetS and IBS in a sample of the Lebanese adult population. Overall, we found a high prevalence of MetS (44·3 %), and after adjustment for potential confounding factors, we identified a significant positive association between MetS and IBS total score and with the IBS diarrhoea subscale and between elevated blood pressure, elevated fasting blood sugar and elevated WC and the IBS diarrhoea subscale.
Our findings are in line with previous research showing a significant positive association between MetS and its components and IBS(Reference Guo, Niu and Momma21,Reference Lee, Kim and Kim43,Reference Nozu and Okumura44) . Specifically, through a cohort study involving 5104 subjects and spanning 5 years, Wang et al. (2022)(Reference Wang, Feng and Shi45) reported more than twice the odds of developing IBS in patients with MetS. Furthermore, in line with our results, Wang et al. (2022)(Reference Wang, Feng and Shi45) reported higher odds of IBS with elevated WC levels, and Kumar et al. (2022)(Reference Kumar, Memon and Arshad46) reported higher fasting blood glucose and higher WC in patients with IBS. Finally, through a case-control study, Lee et al. (2015)(Reference Lee, Lee and Kang47) showed an independent positive association between elevated WC and higher visceral adiposity and IBS, especially, IBS diarrhoea.
Human studies stress the impact of hyperglycaemia, hyperinsulinaemia and MetS on painful neuropathy, whereas improved metabolic control in humans has led to the improvement of neuropathy. Moreover, there is a close relation between luminal and intracellular glucose concentrations, expression of glucose transporters and the release of gut hormones(Reference Ohlsson48). High levels of C-peptide, insulin, gastric inhibitory peptide and leptin increase the excitability of the hypersensitive nervous system often found in IBS and thereby lead to increased symptoms(Reference Nilholm, Roth and Ohlsson49,Reference Saidi, Nilholm and Roth50) .
Furthermore, looking at the mechanism behind the association between high obesity levels, specifically visceral obesity and high risk of diarrhoea, studies indicate accelerated small intestinal transit and distal colonic transit times in obese patients, leading to bile acid malabsorption and thus diarrhoea(Reference Xing and Chen51,Reference Fu, Li and Zhang52) . Visceral fat has also been found to increase the release of pro-inflammatory cytokines, which in turn alters intestinal permeability, leading to loose stools and increased stool frequency(Reference Lee, Lee and Kang47).
Finally, one potential mechanism for the relationship of hypertension with IBS may be that higher blood pressure could alter the tight junction proteins and gut permeability in the intestine, release proinflammatory cytokines and thereby, increase the risk of IBS(Reference Santisteban, Qi and Zubcevic53,Reference Fasano54) .
Although evidence hints at a prevailing positive trend between IBS and MetS, studies are still inconclusive. Javadeka et al. (2021)(Reference Javadekar, Oka and Joshi55) did not find an association between IBS and MetS among young adults. One explanation for this may be due to the exclusion of the patients with already known components of the MetS to nullify the confounding effects of change in lifestyle, diet and drugs on gut function.
While the exact mechanisms driving the positive correlation between IBS and MetS remain elusive, microbiota alterations emerge as a plausible explanation for this association(Reference Singh, Zogg and Wei56,Reference Posserud, Stotzer and Björnsson57) . Specifically, shifts in microbial composition and quantity, gut microbiota-mediated immune dysregulation and intestinal barrier dysfunction emerge as core pathophysiologies of gastrointestinal dysmotility and metabolic disease(Reference Singh, Zogg and Wei56). On one hand, microbial dysbiosis could lead to metabolic dysregulation. Suggested mechanisms include but are not limited to changes to gut barrier function and metabolic inflammation and effects on body weight regulation and insulin sensitivity(Reference Roberti, Harrington and Storch35,Reference Lee, Lee and Kang47) . On the other hand, metabolic abnormalities can cause gastrointestinal disturbances. For example, hyperglycaemia is associated with intestinal barrier dysfunction and increases the risk of enteric infection. In addition, visceral adiposity, for which WC is a proxy, increases the release of pro-inflammatory cytokines, and this in turn may alter intestinal permeability, leading to chronic diarrhoea(Reference Nozu and Okumura44). To date, it remains unclear whether gastrointestinal dysfunction or metabolic disorder comes first.
To better understand the pathophysiological interaction between the two diseases, the link at the molecular level should be further investigated. The pathology of these diseases shares common features, including adipose tissue dysregulation, inadequate immune response and inflammation(Reference Hyun58). As a central metabolic organ for integration and control of whole-body energy homeostasis, the adipose tissue has emerged as an important endocrine regulator that secretes cytokines and hormones, referred to as adipokines, which have pro- or anti-inflammatory activities. Moreover, changes in enteroendocrine functions have also been implicated in the pathogenesis of both diseases(Reference Zietek and Rath59). Glucagon-like peptide-1 has gained attention as a key player in the pathogenesis of metabolic and inflammatory diseases due to its function in modulating stress and promoting anti-inflammatory signalling. The insulinotropic and glucose-lowering effects of glucagon-like peptide-1 have long been shown to be impaired in obesity and type 2 diabetes.
Furthermore, the reason why sleep disorders are associated with IBS remains unclear. The gut–brain axis plays an important role in the pathogenesis of IBS. The central nervous system, autonomic nervous system, enteric nervous system and hypothalamic pituitary adrenal axis are thought to be involved(Reference Carabotti, Scirocco and Maselli60). Sleep deprivation led to modification of the autonomic nervous system activity and autonomic dysregulation(Reference Tobaldini, Costantino and Solbiati61). The hypothalamic pituitary adrenal axis has been reported to be inhibited by sleep and increased secretion of ACTH and cortisol(Reference Tobaldini, Costantino and Solbiati61,Reference Vgontzas and Chrousos62) . Moreover, chronic sleep disruption can also cause reversible changes in gut microbiota associated with IBS symptoms(Reference Poroyko, Carreras and Khalyfa63). Finally, elevated levels of dipeptidyl peptidase 4 seen in sleep deprivation can be an early indicator of metabolic disorders and are associated with increased inflammation in gastrointestinal disorders(Reference Montelongo-Rodríguez, Almendra-Pegueros and Valencia-Sánchez64).
Concerning sex variances, as found elsewhere(Reference Guo, Niu and Momma21,Reference Kim and Kim65) , females in our study exhibited a higher likelihood of having IBS in comparison with males(Reference Boeckxstaens, Drug and Dumitrascu66–Reference Chen, Mahurkar-Joshi and Liu68). This could be attributed to the impact of female sex hormones on gut motility. Noteworthy, we found that participants with higher adherence to the Mediterranean diet were less likely to report IBS symptoms; this is possibly due to the diet’s beneficial influence on gut microbiota and gut barrier(Reference Nozu and Okumura44). The Mediterranean diet boasts various attributes that can enhance gut health, including its rich phenol content that exhibits anti-inflammatory properties, leading to reduced expression of inflammatory molecules, and the higher presence of microbiota that produce short-chain fatty acids, aiding in the maintenance of intestinal epithelium function(Reference Chen, Mahurkar-Joshi and Liu68).
To the best of our knowledge, this study is the first to evaluate the relationship between IBS and MetS in a sample of Lebanese adults, using validated questionnaires and objective measurement of both biochemical and anthropometric indices. Furthermore, this study was sufficiently powered. Nevertheless, our results are limited by their cross-sectional design, which cannot be used to infer causality. Additionally, the sample was collected after the community announcement, which leads us to accept a possibility of self-selection bias; also, being free from infections was a self-reported inclusion criterion. Lastly, the percentage of female participants was much higher than that of males this limitation is common in such types of studies.
In this study, MetS and IBS were positively associated in a sample of the general Lebanese adult population. We suggest that it might be of value to screen for either condition if one of the syndromes exists to facilitate early detection and intervention. Future longitudinal studies are essential to establish a causal relationship between MetS and IBS, further understand the common pathogenesis and explore potential underlying mechanisms.
Acknowledgments
The authors declare no acknowledgements for this study.
This research was funded by the Zayed University RIF Grant R18030.
R.R. and M.A. contributed to the conceptualisation. M.A., S.H., N.M., D.P. and R.R. developed the methodology. T.M. and R.R. performed the formal analysis. S.H. and N.M. conducted the investigation. Data curation was handled by S.H. and N.M. The original draft was prepared by M.A., S.H., N.M., D.P. and R.R. T.M. reviewed and edited the manuscript. T.M. also handled visualisation. D.P. and R.R. provided supervision. Project administration was managed by S.H. and N.M. Funding was acquired by M.A., S.H., N.M. and R.R.
All authors have reviewed and approved the final version of the manuscript.
This research received ethical approval from the Institutional Review Board at the Lebanese International University (Ethical approval no: LIUIRB-220201-SH-111). The study’s objectives, protocol and the right to withdraw at any time were communicated to the participants prior to data collection. Subjects provided written consent, and only those consenting were included in the study.
All authors declare no conflict of interest.