


Statement of Research Significance
Research Question(s) or Topic(s): How are parent-reported executive function difficulties linked to internalizing and externalizing problems in children with neurofibromatosis type 1 across ages and demographic subgroups? Main Findings: Greater executive function difficulties were consistently associated with higher levels of internalizing and externalizing symptoms across development, with notable age-specific patterns: emotional control and cognitive flexibility were more strongly linked to internalizing symptoms in adolescence; inhibitory control was more strongly associated with externalizing problems in childhood. The age-specific associations were generally similar across sex and parental education subgroups. Study Contributions: This study is the first to examine age-specific associations between executive function and mental health difficulties in children with neurofibromatosis type 1, offering preliminary insights into developmental patterns across multiple domains. Findings also highlight executive function as a potentially important area for future intervention research focused on emotional and behavioral challenges in neurofibromatosis type 1, particularly among higher-risk subgroups.
Mental health needs are frequently underrecognized in pediatric populations with rare diseases, often due to the diagnostic challenges these conditions present and the predominant focus on physical symptoms in clinical care (Nunn, Reference Nunn2017; Somanadhan et al., Reference Somanadhan, O’Donnell, Bracken, McNulty, Sweeney, O’Toole, Rogers, Flynn, Awan, Baker, O’Neill, McAneney, Gibbs, Larkin and Kroll2023). Consequently, affected children may go without timely psychological support, even though many rare diseases are now known to heighten the risk of cognitive, emotional, and behavioral difficulties (Dumbuya et al., Reference Dumbuya, Zeng, Deng, Li, Chen, Ahmad and Lu2025). Neurofibromatosis type 1 (NF1) is a well-documented example of such a condition. NF1 is a lifelong, autosomal dominant genetic condition with a global prevalence of approximately 1 in 3,000 individuals (Gutmann et al., Reference Gutmann, Ferner, Listernick, Korf, Wolters and Johnson2017). In addition to a range of physical manifestations, including tumors, skin pigmentation abnormalities, and skeletal issues (Gutmann et al., Reference Gutmann, Ferner, Listernick, Korf, Wolters and Johnson2017), NF1 is linked to an elevated risk of neurodevelopmental and psychiatric challenges across the lifespan (Gutmann et al., Reference Gutmann, Anastasaki, Gupta, Hou, Morris, Payne and Yohay2025; Vogel et al., Reference Vogel, Gutmann and Morris2017). Neuropsychological challenges in NF1 span multiple domains, including executive function (EF; Beaussart et al., Reference Beaussart, Barbarot, Mauger and Roy2018; Zong et al., Reference Zong, Liu, Wu, Wolters, Payne, Klein-Tasman, Walsh, Janusz, Pride, Morris, Bearden and Hou2026), social function and autism spectrum disorder (ASD; Chisholm et al., Reference Chisholm, Anderson, Pride, Malarbi, North and Payne2018), attention-deficit/hyperactivity disorder (ADHD; Hou et al., Reference Hou, Yu, Liu, Wilson-Lemoine, Wu, Moreira, Mujica, Mukhopadhyay, Novotney and Payne2025b), internalizing/externalizing behaviors (Liu et al., Reference Liu, Yu, Wu, Moreira, Mujica, Mukhopadhyay, Novotney, Rietman and Hou2025; Liu et al., Reference Liu, Zong, Payne, Stavinoha, Wolters, Walsh, Janusz, Klein-Tasman, Morris, Bearden, Pride and Hou2026), academic functioning (Yu et al., Reference Yu, Liu, Payne, Wu, Thompson, Moreira, Morey, Mujica and Hou2025a), and visual–spatial and visual–motor skills (Yu et al., Reference Yu, Liu, Payne, Zhang, Moreira, Mukhopadhyay, Novotney, Chown, Killam and Hou2025b). Despite this growing literature, research has largely examined these domains in isolation, providing limited insight into how neuropsychological difficulties co-occur or interact. This domain-specific focus constrains understanding of shared mechanisms and limits the development of integrated, developmentally informed intervention approaches.
Among children and adolescents with NF1, emotional and behavioral difficulties often co-occur with cognitive deficits (Huijbregts & de Sonneville, Reference Huijbregts and de Sonneville2011; Martin et al., Reference Martin, Wolters, Baldwin, Gillespie, Dombi, Walker and Widemann2012; Torres Nupan et al., Reference Torres Nupan, Velez Van Meerbeke, López Cabra and Herrera Gomez2017), affecting multiple areas of functioning and contributing to reduced quality of life (Barton et al., Reference Barton, Wolters, Walsh, Ullrich, Rosser, Tonsgard, Viskochil, Schorry, Klesse, Fisher, Gutmann, Packer, Korf, Acosta, North and Payne2025) and persistent psychiatric distress in adulthood (Domon-Archambault et al., Reference Domon-Archambault, Gagnon, Benoît and Perreault2018; Kenborg et al., Reference Kenborg, Andersen, Duun-Henriksen, Jepsen, Doser, Dalton, Bidstrup, Krøyer, Frederiksen, Johansen, Østergaard, Hove, Sørensen, Riccardi, Mulvihill and Winther2021). The current study examines whether EF skills are associated with two central domains of mental health – internalizing and externalizing problems – in children and adolescents with NF1, with the goal of informing future intervention research. In spite of growing awareness of cognitive, emotional, and behavioral challenges in this population (Torres Nupan et al., Reference Torres Nupan, Velez Van Meerbeke, López Cabra and Herrera Gomez2017), important gaps in the literature remain, which the current study aims to address.
First, it remains unclear how EFs are associated with internalizing and externalizing problems among children and adolescents with NF1 at different ages. In the general population, internalizing problems, such as anxiety, depression, and somatization, tend to increase from childhood through adolescence (Barreto et al., Reference Barreto, Teodoro, Ohno and Froeseler2018; Costello et al., Reference Costello, Mustillo, Erkanli, Keeler and Angold2003), while externalizing problems, such as aggression and delinquency, generally rise during childhood and decline in late adolescence (Petersen et al., Reference Petersen, Bates, Dodge, Lansford and Pettit2015; Steinberg Reference Steinberg2010). EFs, a set of higher-order cognitive skills including inhibitory control, emotional control, working memory, cognitive flexibility, and planning/organization, support goal-directed behavior and undergo protracted development across childhood into young adulthood, supported by maturation of prefrontal brain networks (Ferguson et al., Reference Ferguson, Brunsdon and Bradford2021).
In children from the general population, poorer EFs have been associated with greater internalizing and externalizing symptoms, with evidence suggesting that the strength of these associations may vary across ages (Freichel et al., Reference Freichel, Pfirrmann, de Jong, Cousijn, Franken, Oldehinkel, Veer and Wiers2024; Yang, Shields, et al., Reference Yang, Shields, Zhang, Wu, Chen and Romer2022). Interventions specifically targeting EF have been shown to enhance these cognitive skills (Diamond & Lee, Reference Diamond and Lee2011; Yamamoto & Imai-Matsumura, Reference Yamamoto and Imai-Matsumura2023) and, in some cases, to reduce internalizing and externalizing problems as well (Yamamoto & Imai-Matsumura, Reference Yamamoto and Imai-Matsumura2023). However, even though children with NF1 are at greater risk for both EF deficits (Beaussart et al., Reference Beaussart, Barbarot, Mauger and Roy2018; Zong et al., Reference Zong, Liu, Wu, Wolters, Payne, Klein-Tasman, Walsh, Janusz, Pride, Morris, Bearden and Hou2026) and mental health challenges (Domon-Archambault et al., Reference Domon-Archambault, Gagnon, Benoît and Perreault2018; Liu et al., Reference Liu, Yu, Wu, Moreira, Mujica, Mukhopadhyay, Novotney, Rietman and Hou2025), few interventions in this population have been developed with this dual vulnerability in mind (Domon-Archambault et al., Reference Domon-Archambault, Gagnon, Benoît and Perreault2018), partly due to a lack of relevant research. Identifying how associations between EF and mental health symptoms vary with age may inform developmentally sensitive hypotheses and future intervention research that target cognitive, emotional, and behavioral functioning in this population.
Furthermore, it remains unexplored whether demographic factors, including sex and parental education, moderate the age-specific associations between EF and internalizing and externalizing problems. Sex and parental education are related to both EF and mental health outcomes in the general population. Females tend to outperform males in some EF domains, such as inhibitory control (Raaijmakers et al., Reference Raaijmakers, Smidts, Sergeant, Maassen, Posthumus, van Engeland and Matthys2008; Rubia et al., Reference Rubia, Lim, Ecker, Halari, Giampietro, Simmons, Brammer and Smith2013), report more internalizing symptoms (de Sousa et al., Reference de Sousa, Peixoto and Cruz2021), and exhibit fewer externalizing behaviors (de Sousa et al., Reference de Sousa, Peixoto and Cruz2021). The associations between EF and behavioral problems may also differ by age and sex. A meta-analytic study found that better EF performance was correlated with lower levels of externalizing problems in preschool-aged children, particularly in studies with a higher percentage of males (Schoemaker et al., Reference Schoemaker, Mulder, DekoviÄ and Matthys2013), while another study found that in adolescence, poorer response inhibition was linked to greater affective problems among females but not males (van Deurzen et al., Reference van Deurzen, Buitelaar, Agnes Brunnekreef, Ormel, Minderaa, Hartman, Huizink, Speckens, Oldehinkel and Slaats-Willemse2012).
Similarly, higher parental education is typically associated with stronger EF skills (Halse et al., Reference Halse, Steinsbekk, Hammar, Belsky and Wichstrøm2019) and lower levels of internalizing and externalizing problems in children (Anderson et al., Reference Anderson, Siciliano, Henry, Watson, Gruhn, Kuhn, Ebert, Vreeland, Ciriegio, Guthrie and Compas2022). While research specifically examining parental education as a moderator of the EF–mental health link is limited, related evidence suggests such moderation is plausible. For instance, better academic achievement was only associated with higher life satisfaction among adolescents who reported higher (high school and above) versus lower maternal education (Crede et al., Reference Crede, Wirthwein, McElvany and Steinmayr2015). Although research on neurobehavioral differences by sex and parental education in children with NF1 is still emerging (Hou et al., Reference Hou, Yu, Jamnik, Liu, Wilson-Lemoine, Wu and Payne2025a), early findings suggest that similar patterns of demographic moderation may be present in this population. Specifically, females may be at greater risk for internalizing disorders (Kenborg et al., Reference Kenborg, Andersen, Duun-Henriksen, Jepsen, Doser, Dalton, Bidstrup, Krøyer, Frederiksen, Johansen, Østergaard, Hove, Sørensen, Riccardi, Mulvihill and Winther2021), and children from lower education households may experience greater EF challenges (Hou et al., Reference Hou, Allen, Wolters, Toledo-Tamula, Martin, Baldwin, Reda, Gillespie, Goodwin and Widemann2020) but, somewhat counterintuitively, greater decreases in internalizing problems (Hou et al., Reference Hou, Wu, Liu, Martin, Toledo-Tamula, Allen, Baldwin, Gillespie, Goodwin, Widemann and Wolters2022). Therefore, examining sex and parental education as moderators is important for determining whether the strength of age-related associations vary across subgroups. These analyses will help clarify how EF is related to internalizing and externalizing problems across different subgroups within the NF1 population and may help inform individualized intervention strategies.
Despite growing interest, prior research on EF and internalizing/externalizing problems in individuals with NF1 has been limited by small samples, over 90% of which have included fewer than 100 participants (Beaussart et al., Reference Beaussart, Barbarot, Mauger and Roy2018; Liu et al., Reference Liu, Yu, Wu, Moreira, Mujica, Mukhopadhyay, Novotney, Rietman and Hou2025). This limitation has made it difficult to address the gaps outlined above. Given the lack of large, longitudinal datasets in NF1 research, this study utilized a large and age-diverse sample (including 1,049 observations from 803 participants; ages 3–18) to pursue two primary aims: (1) to examine how EF is associated with internalizing and externalizing problems among children and adolescents with NF1 across ages, and (2) to explore whether these age-related associations are moderated by sex and parental education. To accomplish this, we employed an innovative analytic approach, namely time-varying effect modeling (TVEM), a flexible statistical method that allows for the estimation of how associations between variables change continuously across ages, even with cross-sectional data (Tan et al., Reference Tan, Shiyko, Li, Li and Dierker2012). This approach offers a nuanced, developmentally informed view of how the associations between EF and emotional or behavioral difficulties differ through childhood and adolescence. Findings from this study can help lay the groundwork for future longitudinal and intervention research, which will inform the development of age- and subgroup-tailored strategies to improve mental health outcomes in children and adolescents with NF1.
Method
Participants and procedure
This study analyzed cross-sectional data of 1,049 observations from 803 children and adolescents with NF1 collected across nine institutions in the United States and Australia. De-identified, individual-level data were pooled using integrative data analysis (IDA) (Curran & Hussong, Reference Curran and Hussong2009), a method that enhances statistical power and precision by combining data from multiple independent studies. IDA also improves sample diversity, representativeness, and coverage across age groups (Bainter & Curran, Reference Bainter and Curran2015). All analyses were conducted at the observation level; therefore, reported sample sizes (n) correspond to the number of observations unless otherwise noted. The merged dataset includes both clinical and community-based samples. The current study was completed in accordance with the Helsinki Declaration. Each participating site received approval from its institutional review board (IRB). Approximately half of the sites obtained written consent from participants or their guardians, while the others used retrospectively retrieved clinical data. The IDA protocol was approved by the IRBs at the University of Kentucky (ID 67,554) and the Florida State University (ID STUDY00003513).
Measures
Outcomes
Internalizing and externalizing problems were assessed with parent-rated composite scales from either the Behavior Assessment System for Children (BASC; n = 460, 44.9%) (Reynolds & Kamphaus, Reference Reynolds and Kamphaus2002, Reference Reynolds and Kamphaus2015) or the Child Behavior Checklist (CBCL; n = 589, 56.1%) (Achenbach Reference Achenbach2009), depending on the instrument administered at each site (see eTable 1). The internalizing composite included anxiety, depression, and somatization in BASC, and anxious/depressed, withdrawn/depressed, and somatic complaints in CBCL. The externalizing composite included hyperactivity, aggression, and conduct problems in BASC, and aggressive and rule-breaking behaviors in CBCL. For each participant, the standardized internalizing and externalizing composite scores provided by the administered instrument were used directly in analyses, without further aggregation or transformation. All scores were analyzed as T scores (M norm = 50, SD norm = 10), with higher values indicating greater symptom severity. BASC and CBCL are among the most widely used standardized measures of emotional and behavioral functioning in children, including those with NF1 (Allison Bender et al., Reference Allison Bender, Auciello, Morrison, MacAllister and Zaroff2008; Liu et al., Reference Liu, Yu, Wu, Moreira, Mujica, Mukhopadhyay, Novotney, Rietman and Hou2025). Both measures demonstrate good reliability and validity with high converging validity in internalizing and externalizing composites (Achenbach & Rescorla, Reference Achenbach and Rescorla2001; Allison Bender et al., Reference Allison Bender, Auciello, Morrison, MacAllister and Zaroff2008; Reynolds & Kamphaus, Reference Reynolds and Kamphaus2004).
Focal covariates
Parents rated EF difficulties with age-appropriate versions of Behavior Rating Inventory of Executive Function (BRIEF) (Gioia et al., Reference Gioia, lsquith, Guy and Kenworthy2000), a tool designed to evaluate real-world behavioral indicators of EF skills. Subscales used included Inhibit, Emotional Control, Shift, Working Memory, and Plan/Organize (reflecting inhibitory control, emotional control, cognitive flexibility, working memory, and planning/organization, respectively) from the preschool version (BRIEF-P; Gioia et al., Reference Gioia, Espy and Isquith2003), the original version (Gioia et al., Reference Gioia, lsquith, Guy and Kenworthy2000), and the second edition (BRIEF-2; Gioia et al., Reference Gioia, Isquith, Guy and Kenworthy2015) of BRIEF. eTable 1 presents the BRIEF versions used across sites. Standardized T scores (M norm = 50, SD norm = 10) of EF variables were used in analyses. Higher scores indicate greater EF difficulties. All subscales have shown good reliability and validity in children with NF1 (Payne et al., Reference Payne, Hearps, Walsh, Paltin, Barton, Ullrich, Haebich, Coghill, Gioia, Cantor, Cutter, Tonsgard, Viskochil, Rey-Casserly, Schorry, Ackerson, Klesse, Fisher and Gutmann2019).
Background information
Background information was either reported by parents or primary caregivers or retrieved from medical records (eTable 2). Participants’ age (in years), biological sex (categorized as male and female), and parental education were included in analyses. Parental education was initially coded into five categories based on information provided by each site: (1) less than high school; (2) high school or partial high school; (3) some college, community college, or associate degree; (4) college or university degree; and (5) graduate or professional training. When education levels were reported for both parents, values were averaged; when reported by a single parent, that value was used. For visualization in subgroup analysis, parental education was further categorized as low [i.e., lower than college] and high [i.e., some college or above]. Other available background information included whether NF1 was inherited from a parent or not (familial NF1 vs. sporadic NF1), whether plexiform neurofibromas were present (yes or no), whether they were diagnosed with ADHD (yes or no), depression (yes or no), anxiety (yes or no), ASD (yes or no), or specific learning disorder (SLD; yes or no).
Statistical analysis
TVEM with the P-spline approach was used to characterize how the associations between each EF domain and internalizing and externalizing problems varied across ages, following model fit practices outlined in Tan et al. (Reference Tan, Shiyko, Li, Li and Dierker2012). TVEM is a non-parametric technique particularly suitable for modeling processes that unfold over time or across ages (Tan Reference Tan, Shiyko, Li, Li and Dierker2012). It does not impose predefined functional forms (e.g., linear or quadratic) but assumes that changes occur smoothly and continuously over time. Originally developed for intensive longitudinal data analysis (Shiyko et al., Reference Shiyko, Burkhalter, Li and Park2014), this technique has been adapted to model age patterns in developmental studies using cross-sectional data (Hou et al., Reference Hou, Zong, Wu, Liu, Wolters, Janusz, Walsh, Morris, Payne, Pride, Garg, Robinson and Stavinoha2025c; Juang et al., Reference Juang, Hou, Bayless and Kim2018). In the current study, TVEM was applied to estimate coefficients flexibly, allowing for the delineation of smooth age patterns of the associations between EF domains and internalizing or externalizing problems. A participant-level random intercept was included to account for within-subject correlation due to repeated observations for some participants.
For Aim 1, we used TVEM to test the age-varying associations between each EF variable and internalizing or externalizing problems. For Aim 2, we explored the potential moderating effects of sex and parental education on the age-varying associations in two complementary sets of tests: First, an interaction term between each EF variable and sex or parental education was added along with the main effect of sex or parental education to TVEM models; second, when a significant interaction term was detected at any age point, we tested each TVEM model separately across moderator subgroups, to characterize the pattern and identify which subgroup showed stronger associations – analogous to probing simple slopes in traditional regression models. This approach is consistent with prior studies (Dermody et al., Reference Dermody, Thomas, Hopwood, Durbin and Wright2017; Juang et al., Reference Juang, Hou, Bayless and Kim2018).
TVEM estimates the intercepts and associations along with 95% confidence intervals (CIs) at each age point to create a smooth curve, which are summarized graphically. Statistically significant associations between EF variables or a product term and internalizing or externalizing problems are identified when the 95% CIs do not include 0. Significant differences across ages are indicated by non-overlapping 95% CIs between specific age points. Descriptive statistics were calculated and missingness checked using R (R Core Team, 2025). TVEM and subgroup analyses were performed using a SAS macro (Li et al., Reference Li, Dziak, Tan, Huang, Wagner and Yang2017), which automatically excludes cases with missing data on variables from the specific model analyses.
Results
Sample characteristics
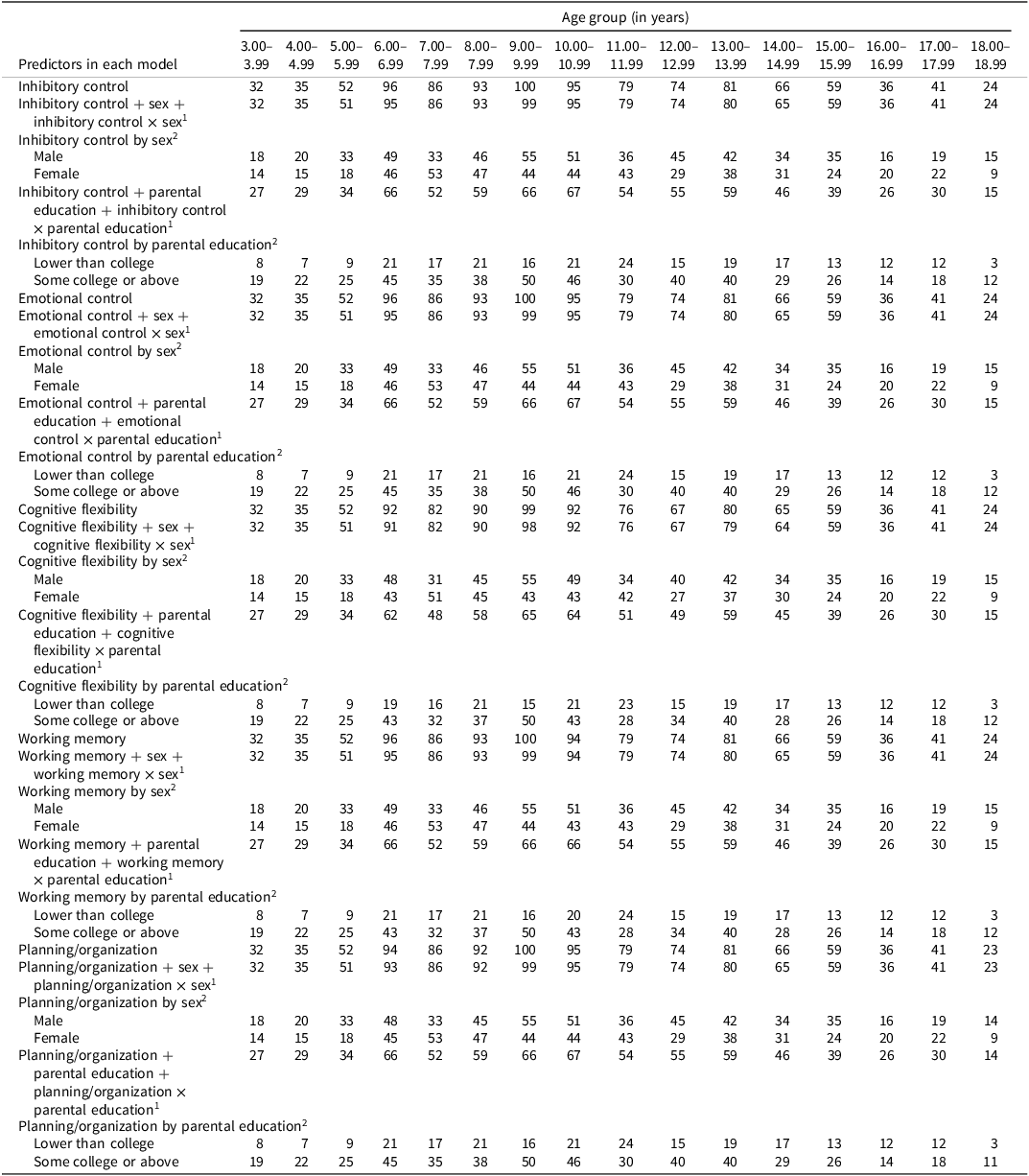
The combined sample included 1,049 observations from 803 children and adolescents with NF1, with a mean age of 10.58 years (SD = 3.84) ranging from 3 to18 years. The total sample size distribution by age for each association is presented in Tables 1–2. The sample size for each association in main analyses (not including Aim 2 subgroup analyses) was at least 15 for all age groups from 3 to 18, sufficient to yield reliable TVEM estimates. Among the observations who had background information available, 47.5% (n = 497/1044) were females, 67.5% (489/724) had parents with some college or above education, 36.6% (n = 273/746) had familial NF1, 48.6% (n = 268/551) had PNs, 41.5% (n = 319/775) had ADHD, 6.1% had depression (n = 47/767), 15.1% had anxiety (n = 117/775), 6.7% had ASD (n = 30/450), and 34.1% had SLD (n = 236/693). Detailed sample characteristics of each participating site and the combined sample are presented in eTable 1. Additional sample information is presented in eTable 2.
Sample size distribution by age for models estimating the age-specific associations between executive function domains and internalizing problems

1 In this model, the predictors include one executive function domain, one moderator, and the interaction term of the executive function variable and the moderator.
2 This model tests the age-varying association between one executive function variable and the outcome separately in each subgroup of the moderator; the executive function variable is the predictor, and the grouping variable is the moderator.
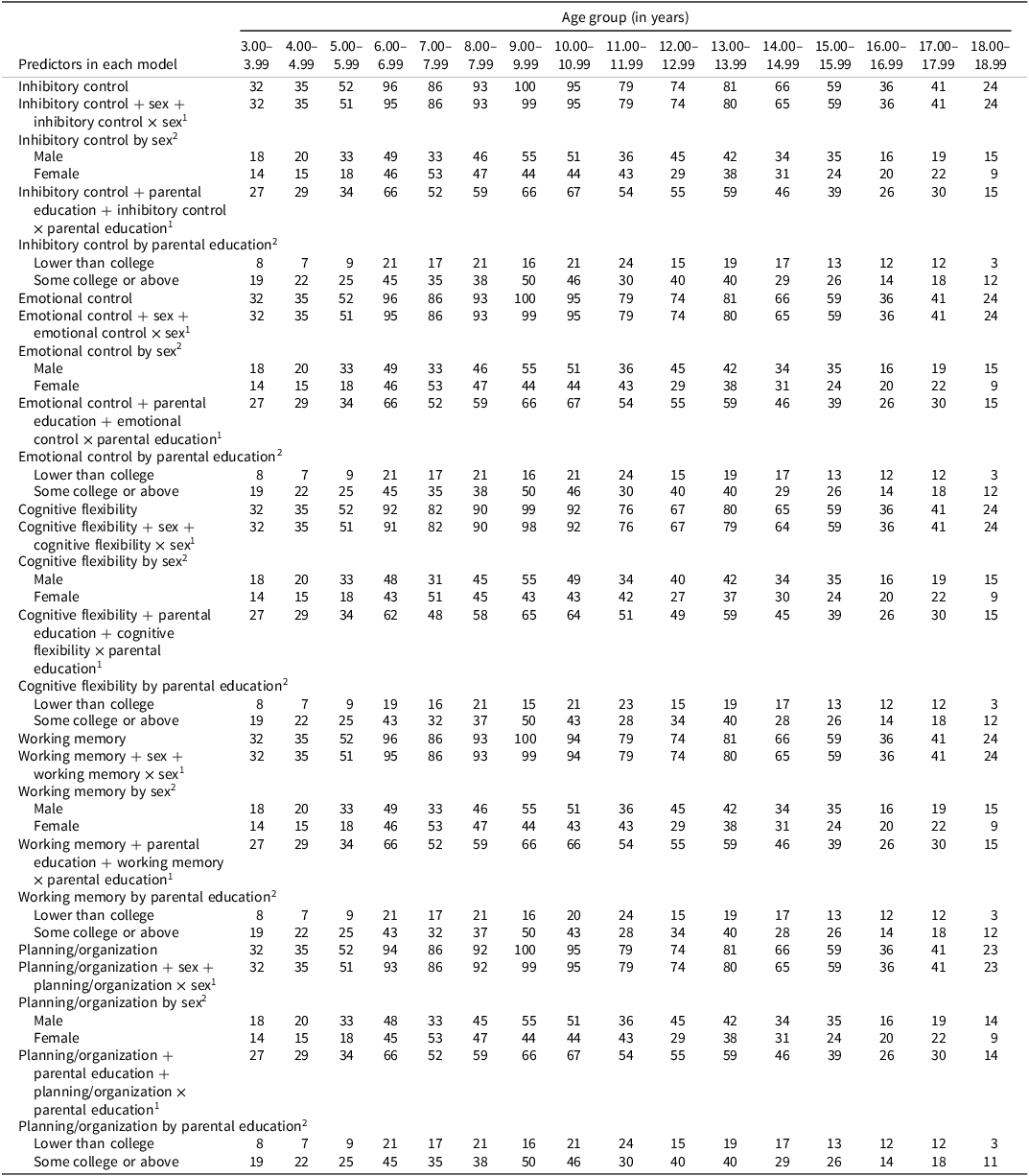
Sample size distribution by age for models estimating the age-specific associations between executive function domains and externalizing problems

1 In this model, the predictors include one executive function domain, one moderator, and the interaction term of the executive function variable and the moderator.
2 This model tests the age-varying association between one executive function variable and the outcome separately in each subgroup of the moderator; the executive function variable is the predictor, and the grouping variable is the moderator.
Descriptive statistics and correlations among study variables are presented in eTable 3, with score ranges by age group shown in eTable 4. Across the five EF domains, 22.6%–41.8% of observations scored in the clinically significant range (T ≥ 65), and 11.0%–15.3% scored in the at-risk range (T = 60–64). For internalizing and externalizing symptoms, clinically significant scores (T ≥ 65 for CBCL scores and T ≥ 70 for BASC scores) were reported for 19.7% and 13.1% of observations, respectively, while at-risk scores (T = 60–64 for CBCL scores and T = 60–69 for BASC scores) were reported for 17.0% and 12.5%, respectively. Substantial variability was observed across age groups for all focal study variables. Correlations among study variables are summarized in Supplementary Descriptive Statistics.
The amount of missing data for parental education was 30.98%, and 0.00% to 2.58% for other study variables (eTables 1 and 3). Results from the Little’s MCAR test suggested that the pattern of missingness was missing completely at random: χ 2(60) = 51.20, p = .783. The amount and pattern of missingness indicated that listwise deletion automatically implemented in the SAS macro for TVEM (Li et al., Reference Li, Dziak, Tan, Huang, Wagner and Yang2017) was acceptable.
Age-varying associations between executive function and internalizing/Externalizing problems
Parental complaints in all five EF domains, including inhibitory control (βs ranged from 0.26, 95% CI [0.16, 0.35] to 0.54, 95% CI [0.27, 0.81]), emotional control (βs ranged from 0.39, 95% CI [0.14, 0.63] to 0.90, 95% CI [0.63, 1.16]), cognitive flexibility (βs ranged from 0.41, 95% CI [0.34, 0.48] to 0.74, 95% CI [0.45, 1.02]), working memory (βs ranged from 0.31, 95% CI [0.23, 0.40] to 0.57, 95% [0.24, 0.91]), and planning/organization (βs ranged from 0.34, 95% CI [0.15, 0.43] to 0.45, 95% [0.11, 0.78]), were associated with greater internalizing problems across ages 3–18 (Figure 1; coefficient estimates presented in eTable 5). Parent-rated poorer functioning in the five EF domains, including inhibitory control (βs ranged from 0.42, 95% CI [0.34, 0.49] to 0.77, 95% CI [0.53, 1.01]), emotional control (βs ranged from 0.29, 95% CI [0.04, 0.54] to 0.84, 95% CI [0.55, 1.14]), cognitive flexibility (βs ranged from 0.38, 95% CI [0.04, 0.71] to 0.55, 95% CI [0.29, 0.82]), working memory (βs ranged from 0.26, 95% CI [0.03, 0.48] to 0.53, 95% CI [0.27, 0.80]), and planning/organization (βs ranged from 0.37, 95% CI [0.14, 0.61] to 0.48, 95% CI [0.39, 0.56]), were also associated with higher levels of externalizing problems across ages 3–18 (Figure 2; coefficient estimates presented in eTable 6). These findings suggest a potentially persistent association between poorer EF and greater internalizing and externalizing problems from early childhood to late adolescence.
Age-varying associations between executive function domains and internalizing problems. A. Inhibitory control – internalizing. B. Emotional control – internalizing. C. Cognitive flexibility – internalizing. D. Working memory – internalizing. E. Planning/organization – internalizing. Note. The x-axis represents age, and the y-axis represents standardized regression coefficient estimates based on T-score–scaled predictor and outcome variables (M = 50, SD = 10). A significant association is indicated by 95% confidence intervals (CIs) that do not include 0. Significant age differences are indicated by non-overlapping 95% CIs between specific age points.

Age-varying associations between executive function domains and externalizing problems. A. Inhibitory control – externalizing. B. Emotional control – externalizing. C. Cognitive flexibility – externalizing. D. Working memory – externalizing. E. Planning/organization – externalizing. Note. The x-axis represents age, and the y-axis represents standardized regression coefficient estimates based on T-score–scaled predictor and outcome variables (M = 50, SD = 10). A significant association is indicated by 95% confidence intervals (CIs) that do not include 0. Significant age differences are indicated by non-overlapping 95% CIs between specific age points.

Figure 2. Long description
The line graph presents the age-varying associations between various executive function domains and externalizing problems in children with Neurofibromatosis type 1. The x-axis represents age in years, ranging from 3 to 18 years. The y-axis represents standardized regression coefficient estimates based on T-score-scaled predictor and outcome variables, with a mean of 50 and a standard deviation of 10. The graph includes five subplots: A. Inhibitory control – externalizing, B. Emotional control – externalizing, C. Cognitive flexibility – externalizing, D. Working memory – externalizing, and E. Planning/organization – externalizing. Each subplot shows the estimate line and the 95% confidence interval (CIs). Significant associations are indicated by 95% CIs that do not include 0. Significant age differences are indicated by non-overlapping 95% CIs between specific age points. For example, in subplot A, ages 4.61 to 8.79 are stronger than ages 12.01 to 16.19. All values are approximated.
While most of the associations remained unchanged across ages, the strength of some associations varied significantly. Specifically, the associations between difficulties in emotional control and cognitive flexibility with internalizing problems were significantly stronger among middle-to-late adolescents than children. For example, the emotional control–internalizing association was stronger at ages 16.35–18.93 compared with ages 3.48–9.76, ages 15.23–18.93 compared with ages 4.77–6.06, and ages 17.32–18.93 compared with ages 3.00–11.53 (Figure 1B). Similarly, the cognitive flexibility–internalizing association was stronger at ages 16.51–17.16 compared with ages 6.38–11.85, ages 16.03–17.64 compared with ages 6.70–11.20, and ages 15.07–18.28 compared with ages 7.83–10.40 (Figure 1C), for instance. In contrast, the association between inhibitory control difficulties and externalizing problems was generally stronger among children than early-to-middle adolescents (e.g., ages 4.61–8.79 vs. ages 12.01–16.19, ages 5.57–6.86 vs. ages 10.56–16.84, and ages 8.95–9.92 vs. ages 13.94–14.90; Figure 2A). Coefficient estimates at each specific age are provided in eTables 5–6.
Moderation effects by sex and parental education
Sex significantly moderated the association between working memory difficulties and internalizing problems between ages 11.5 and 14, as the 95% CIs for the interaction term between working memory and sex did not include zero during this age range (Figure 3A). Follow-up subgroup analyses revealed a significantly stronger association between working memory difficulties and internalizing problems among males (vs. females) at these ages (Figure 3B).
Age-varying associations between working memory and internalizing problems moderated by sex. A. Interaction effects of working memory × sex on internalizing problems. B. Age-varying associations across sex subgroups. Note. The x-axis represents age, and the y-axis represents (A) regression coefficient estimates between the interaction term and the outcome; and (B) standardized regression coefficient estimates based on T-score–scaled predictor and outcome variables (M = 50, SD = 10). A significant association is indicated by 95% confidence intervals (CIs) that do not include 0. Significant age differences are indicated by non-overlapping 95% CIs between specific age points.

Figure 3. Long description
The line graph consists of two panels labeled A and B. Panel A shows the interaction effects of working memory and sex on internalizing problems. The x-axis represents age in years, ranging from 3 to 18, and the y-axis represents the regression coefficient. The black line represents the estimate, while the gray lines represent the 95% confidence interval. Panel B shows age-varying associations across sex subgroups. The x-axis represents age in years, ranging from 3 to 18, and the y-axis represents the regression coefficient. The solid black line represents males, and the dashed black line represents females. The gray lines represent the 95% confidence intervals for both males and females. All values are approximated.
Similarly, sex significantly moderated the association between planning/organization difficulties and internalizing problems between ages 12 and 14 (Figure 4A). Follow-up subgroup analyses suggested that the association was significantly stronger in males during this age range (Figure 4B). However, sex did not moderate the associations between difficulties in other EF domains (i.e., inhibitory control, emotional control, and cognitive flexibility) and internalizing problems, as the 95% CIs for their respective interaction terms included zero (eFigure 1).
Age-varying associations between planning/Organization and internalizing problems moderated by sex. A. Interaction effects of planning/organization × sex on internalizing problems. B. Age-specific associations across sex subgroups. Note. The x-axis represents age, and the y-axis represents (A) regression coefficient estimates between the interaction term and the outcome; and (B) standardized regression coefficient estimates based on T-score–scaled predictor and outcome variables (M = 50, SD = 10). A significant association is indicated by 95% confidence intervals (CIs) that do not include 0. Significant age differences are indicated by non-overlapping 95% CIs between specific age points.

Figure 4. Long description
The line graph consists of two panels. Panel A shows the interaction effects of planning/organization and sex on internalizing problems. The x-axis represents age in years, ranging from 3 to 18. The y-axis represents the regression coefficient, ranging from -0.50 to 0.50. The black line represents the estimate, and the gray lines represent the 95% confidence interval. Panel B shows age-specific associations across sex subgroups. The x-axis represents age in years, ranging from 3 to 18. The y-axis represents the regression coefficient, ranging from -0.50 to 1.50. The solid black line represents males, and the dashed black line represents females. The gray lines represent the 95% confidence intervals for both males and females. All values are approximated.
Parental education did not significantly moderate the association between difficulties in any EF domains and internalizing symptoms (eFigure 2). None of the EF domains interacted with sex or parental education in their associations with externalizing problems across ages. The graphs illustrating how the interaction terms were associated with externalizing problems are presented in eFigures 3 and 4, respectively.
Sensitivity analyses
Depression and anxiety
Because research suggests that EF may relate differently to depression and anxiety (Warren et al., Reference Warren, Heller and Miller2021), we conducted supplementary sensitivity analyses to examine age-specific associations between EF domains and these two internalizing subscales using TVEM with BASC and CBCL data separately. Overall, the patterns of associations were consistent with the main analyses of total internalizing problems. For BASC data (N = 589, ages 3–18; n ≥15 per age group, eTable 7), difficulties in all EF domains were linked to greater anxiety across most ages, but none varied in magnitude by age (eFigure 5). The associations with depression were also significant across ages (eFigure 6), and the link between emotional control and depression varied by age, being stronger at ages 16–18 than 4–6 (eFigure 6B). For CBCL data (N = 487, ages 6–16, eTable 8), EF difficulties were consistently associated with greater anxious/depressed and withdrawn/depressed symptoms, with no significant age variation (eFigures 7–8).
Intelligence
We also tested the EF-internalizing/externalizing links, while controlling for participants’ full intelligence scores assessed with the Wechsler Intelligence Tests (e.g., Wechsler Reference Wechsler2003, Reference Wechsler2008, Reference Wechsler2014, Reference Wechsler2014) and the Differential Ability Scales (Elliott Reference Elliott1990, Reference Elliott2007), given established associations between intelligence with EF (Arffa, Reference Arffa2007) and internalizing/externalizing problems (Kavish et al., Reference Kavish, Helton, Vaughn and Boutwell2020). Results remained largely unchanged after adjustment (see visualization of the results in eFigures 9–10; see coefficient estimates in eTables 9–10). Because models controlling for intelligence were based on a smaller subsample that had intelligence scores available, in addition to data on EF and internalizing/externalizing problems (ns = 963 to 965), we focus interpretations on results from the primary models without the intelligence covariate.
BRIEF response validity
Finally, we evaluated the robustness of findings to potential BRIEF response validity concerns. Validity indices were available from a subset of sites (n = 191), among which a small number of observations (n = 14; 7.3%) showed potential validity concerns (classified as elevated, questionable, or not acceptable). Excluding these cases did not alter the main findings regarding age-specific associations between EF and internalizing/externalizing symptoms, indicating that the results were robust to potential BRIEF response validity issues.
Discussion
This study examined the age-specific associations between EF difficulties and internalizing and externalizing problems in children and adolescents with NF1, based on parent report. Drawing on the largest multisite sample in NF1 to date and using an innovative statistical approach, we identified robust associations that varied in nuanced ways across ages, from early childhood to late adolescence. We also explored whether sex and parental education moderated these age-varying associations. The findings are discussed below.
Robust links between parental complaints of executive function difficulties and internalizing/externalizing symptoms across ages
Across all five parent-rated EF domains – inhibitory control, emotional control, cognitive flexibility, working memory, and planning/organization – greater EF difficulties were significantly associated with higher levels of both internalizing and externalizing symptoms in children and adolescents with NF1 from 3 to 18 years. The consistency of these associations across multiple, interrelated EF domains points to a robust and pervasive link between executive functioning and mental health in this population. These findings align with prior research in typically developing youth and in other neurodevelopmental conditions, where EF difficulties confer heightened vulnerability to emotional and behavioral problems (Freichel et al., Reference Freichel, Pfirrmann, de Jong, Cousijn, Franken, Oldehinkel, Veer and Wiers2024; Lei et al., Reference Lei, Charman, Leigh, Russell, Mohamed and Hollocks2022; Yang, Shields, et al., Reference Yang, Shields, Zhang, Wu, Chen and Romer2022). Importantly, the present study extends this literature to children and adolescents with NF1 – an underrepresented population in psychiatric and developmental research – highlighting EF difficulties as a potential transdiagnostic factor associated with the broad spectrum of emotional and behavioral challenges observed in this population.
From a clinical and translational perspective, these findings highlight executive functioning as a potentially important consideration when addressing emotional and behavioral symptoms in youth with NF1. Transdiagnostic approaches, such as cognitive behavioral therapy (CBT; Beck & Beck, Reference Beck2020) and acceptance and commitment therapy (Dindo et al., Reference Dindo, Van Liew and Arch2017), emphasize cognitive and emotional regulation processes and have demonstrated efficacy across a range of psychiatric and medical conditions (Aravind et al., Reference Aravind, Agarwal, Malhotra and Ayyub2024; Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012). Future research may explore whether adapting these interventions to more explicitly address EF-related processes – particularly emotion regulation and cognitive flexibility – could be relevant for children and adolescents with NF1. Longitudinal and intervention studies are needed to determine whether changes in EF skills are associated with subsequent improvements in mental health outcomes in this population.
Another important finding is that, while many of the EF-internalizing/externalizing associations did not vary across ages, notable age-related variations emerged for specific EF domains. In particular, the association between emotional control difficulties and internalizing problems was stronger in middle to late adolescence than in childhood. Adolescence is a period marked by increased emotional reactivity and evolving self-concept (Dahl & Gunnar, Reference Dahl and Gunnar2009), which may amplify the psychological impact of poor emotional control, especially in those with a rare disease like NF1, who may already experience heightened sensitivity or social stressors due to physical symptoms (Yang, Yoo, et al., Reference Yang, Yoo, Amin, Cheng, Sundaresan, Zhang and Duh2022) or learning difficulties (Torres Nupan et al., Reference Torres Nupan, Velez Van Meerbeke, López Cabra and Herrera Gomez2017; Vogel et al., Reference Vogel, Gutmann and Morris2017).
Similarly, the association between difficulties in cognitive flexibility and internalizing problems was also stronger during middle to late adolescence than during childhood. Cognitive flexibility, defined as the ability to shift thinking or behavior in response to changing rules, demands, or perspectives (Diamond, Reference Diamond2013), is a particularly important skill for navigating the increasing complexity of adolescent life, including peer relationships (Cheung et al., Reference Cheung, Wang, Monroy and Couch2016), academic pressures (Zheng et al., Reference Zheng, Akaliyski, Ma and Xu2024), and future planning (Thomsen, Reference Thomsen2016). Adolescents who struggle with this form of flexibility may find it difficult to cope with uncertainty, transitions, or perceived failures, potentially contributing to increased internal distress (Rademacher et al., Reference Rademacher, Kraft, Eckart and Fiebach2023). This may also be more salient for adolescents with chronic illnesses such as NF1, as they face more severe EF, socio-emotional, and behavioral challenges that start during early childhood and tend to worsen with age (Beaussart et al., Reference Beaussart, Barbarot, Mauger and Roy2018; Chisholm et al., Reference Chisholm, Anderson, Pride, Malarbi, North and Payne2018; Hou et al., Reference Hou, Yu, Liu, Wilson-Lemoine, Wu, Moreira, Mujica, Mukhopadhyay, Novotney and Payne2025b; Zong et al., Reference Zong, Liu, Wu, Wolters, Payne, Klein-Tasman, Walsh, Janusz, Pride, Morris, Bearden and Hou2026). Thus, the emotional impact of poor cognitive flexibility may be greater in adolescents with NF1 compared to children with NF1.
In contrast, the association between inhibitory control difficulties and externalizing problems was weaker in early to middle adolescence than in childhood. This pattern aligns with developmental models of behavioral regulation (Steinberg, Reference Steinberg2010). In early childhood, inhibitory control plays a central role in curbing aggression and rule-breaking behaviors, which are hallmarks of externalizing problems (Utendale & Hastings, Reference Utendale and Hastings2011). As children mature, however, behavioral self-regulation typically improves, and as a result, difficulties in inhibitory control may exert a diminishing influence on overt externalizing behaviors during adolescence, when other factors, such as peer influences, identity formation, and social norms, begin to shape behavior more strongly (Petersen et al., Reference Petersen, Bates, Dodge, Lansford and Pettit2015; Steinberg, Reference Steinberg2010). Together, these age-specific findings highlight the importance of considering developmental context when examining EF and mental health symptoms. The observed patterns suggest that future intervention research may benefit from developmentally sensitive and individually tailored approaches. For example, targeting emotional control and cognitive flexibility may be particularly relevant to examine during adolescence, whereas early interventions focusing on inhibitory control may be informative to evaluate in relation to externalizing problems during childhood.
Moderating roles of sex and parental education
Moderation analyses revealed largely consistent age-specific EF-internalizing/externalizing associations across demographic subgroups, alongside a small number of age-specific sex differences in association strength. Specifically, difficulties in working memory and planning/organization were more strongly associated with internalizing symptoms in males (vs. females) during early adolescence, although the associations were significant among both sex subgroups. These patterns may reflect males’ greater vulnerability during a time of increasing cognitive regulation demands such as in academics (especially in language and literacy; Hou et al., Reference Hou, Yu, Liu, Wilson-Lemoine, Wu, Moreira, Mujica, Mukhopadhyay, Novotney and Payne2025b; Oakley et al., Reference Oakley, Pekrun and Stoet2024) and social interactions (Wood-Downie et al., Reference Wood-Downie, Wong, Kovshoff, Cortese and Hadwin2021). Working memory supports emotional regulation by helping children manage complex thoughts and reappraise distressing situations (Diamond, Reference Diamond2013). Planning and organization, as a higher-order EF skill, may facilitate the implementation of adaptive coping strategies to manage stress (Diamond, Reference Diamond2013). Deficits in these domains may be especially disruptive for males, who face intensified sex norms during adolescence that discourage emotional expression (Smith et al., Reference Smith, Schacter, Enders and Juvonen2018). As a result, males may be less likely to recognize, reappraise, or effectively regulate emotional distress, increasing their risk for internalizing problems. Indeed, males conforming to social norms have been shown to exhibit greater depressive symptoms while this was not found in their female peers (Smith et al., Reference Smith, Schacter, Enders and Juvonen2018). Alternatively, because all measures were parent-reported, it is possible that parents of males with NF1 were more likely to notice EF-related struggles or interpret behavioral signs as emotional distress. Further research using multi-informant approaches is needed to clarify whether these patterns reflect true sex-based differences in vulnerability or differences in how symptoms are perceived and reported.
Notably, these significant moderation effects were the exception rather than the norm. Most associations between EF domains and internalizing/externalizing problems did not differ by sex or parental education. Sex did not significantly moderate the associations between difficulties in inhibitory control, emotional control, or cognitive flexibility and internalizing problems, nor did it moderate any associations with externalizing problems. Similarly, parental education did not moderate the links between any EF domains and internalizing or externalizing symptoms. Together, these findings suggest that the EF-internalizing/externalizing associations in children and adolescents with NF1 are largely robust across sex and parental education subgroups, despite potential mean-level differences in symptom severity (see correlations in eTable 3; see also Hou et al., Reference Hou, Allen, Wolters, Toledo-Tamula, Martin, Baldwin, Reda, Gillespie, Goodwin and Widemann2020; Kenborg et al., Reference Kenborg, Andersen, Duun-Henriksen, Jepsen, Doser, Dalton, Bidstrup, Krøyer, Frederiksen, Johansen, Østergaard, Hove, Sørensen, Riccardi, Mulvihill and Winther2021).
Overall, the moderation findings underscore consistency in the direction and presence of associations between EF and mental health across demographic subgroups, while acknowledging that minor variation in strength may arise depending on developmental stage and sex. These patterns highlight the importance of individualized and developmentally sensitive supports and simultaneously reaffirm the generalizability and robustness of EF difficulties as a potential risk factor for internalizing and externalizing problems in children and adolescents with NF1.
Limitations and future directions
While this study offers important insights into the age-varying associations between EF and mental health in children and adolescents with NF1, several limitations should be acknowledged. First, the predominantly cross-sectional design limits inferences about developmental change and causal or directional pathways between EF difficulties and internalizing/externalizing problems. Although TVEM allowed modeling age-varying associations at the population level, children of different ages may not be fully comparable in terms of comorbidities, cognitive resources, treatment exposure, or other unmeasured factors, which is particularly relevant given the marked phenotypic heterogeneity of NF1. Accordingly, age-related patterns should be interpreted as cross-sectional differences rather than within-person change. Moreover, although EF difficulties were analyzed as predictors in the current study, reverse or reciprocal associations are equally plausible, as mental health symptoms may also disrupt executive functioning (Bredemeier et al., Reference Bredemeier, Warren, Berenbaum, Miller and Heller2016; Zhou et al., Reference Zhou, Ma, Li, Bai, Ma, Li and Gong2025). Given that longitudinal datasets spanning childhood through adolescence remain rare, this large multisite sample provides a unique opportunity to characterize age-specific associations across a broad developmental span, informing hypothesis generation and future longitudinal and intervention studies.
Second, several measurement-related considerations should be taken into account when interpreting study findings. All focal study variables were based on parent-report measures, which may introduce shared method variance and potential reporting biases. Incorporating multi-informant data and objective, performance-based assessments in future research would strengthen the validity of findings. In addition, all questionnaires were scored using U.S.-derived normative data – the standard approach in both the United States and Australia – to ensure a consistent comparative framework across sites. Although Australian-specific norms are not available, the CBCL and BASC have demonstrated cross-cultural validity (Crijnen et al., Reference Crijnen, Achenbach and Verhulst1999; Heubeck, Reference Heubeck2000; Tan et al., Reference Tan, Kraska, Bell and Costello2021), and the BRIEF is widely used internationally. Nevertheless, cross-cultural measurement equivalence was not formally tested, particularly for the BASC and BRIEF. Future international studies would benefit from the development of country-specific norms or formal tests of measurement invariance. Lastly, parental education was reported by one or both parents. Future studies would benefit from systematically collecting maternal and paternal education separately, which would enable examination of potentially distinct contributions of each parent’s educational background to children’s EF and mental health outcomes.
Third, the generalizability of these findings beyond NF1 remains uncertain. Given NF1’s distinct cognitive and behavioral profile and the absence of a typically developing or clinical comparison group, it is unclear whether the observed associations and age-related patterns are specific to NF1 or reflect broader developmental processes. Future studies examining similar relationships in other neurogenetic or chronic conditions will be essential for distinguishing NF1-specific mechanisms from general adaptation processes and for informing both condition-specific and transdiagnostic intervention strategies.
Finally, limited and inconsistent diagnostic information for ADHD, ASD, depression, anxiety, learning disorder, and other neurodevelopmental disorders across sites constrained our ability to examine age-specific associations by comorbid status. More broadly, although this study focused on demographic moderators such as sex and parental education, future research would benefit from integrating harmonized diagnostic data with additional ecological (e.g., family stress, access to services), neurobiological (e.g., brain structure/function, types of NF1 mutations), and treatment-related factors (e.g., medication use, psychosocial interventions). Such integrative approaches will be critical for clarifying heterogeneity in EF–mental health associations in NF1 and for evaluating developmentally tailored interventions that account for contextual risk.
Conclusion
This study demonstrates that parental complaints of EF difficulties are consistently associated with higher levels of internalizing and externalizing problems in children and adolescents with NF1 from early childhood to late adolescence. Using a large, harmonized dataset, we found that while most associations were consistent across ages, some varied across developmental stages. Specifically, difficulties in emotional control and cognitive flexibility were more strongly associated with internalizing symptoms during middle to late adolescence, while poorer inhibitory control was more strongly related to externalizing problems in childhood. Moderation analyses indicated that the age-related associations were generally consistent across demographic subgroups, with a few exceptions: stronger links between certain EF difficulties and internalizing problems were observed among males at certain ages during early adolescence. Together, these findings highlight the value of monitoring EF difficulties as part of mental health assessment and care in children and adolescents with NF1. They also support the need for developmentally and contextually sensitive approaches to early identification and support. Future longitudinal and intervention research is needed to examine how EF difficulties and mental health outcomes are associated over time and to explore potential causal pathways in this high-risk population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1355617726102021.
Acknowledgments
From the National Cancer Institute (NCI), we thank Dr Brigitte Widemann, the principal investigator of the original NF natural history protocol (NCT00924196) from which the NCI test data were generated, Dr Staci Martin for collaborating on the development of the NCI test battery for this protocol and evaluating participants. From MD Anderson Cancer Center, we thank Grace Yang for database management and data preparation of the site’s data. We thank other staff, research assistants, and patients who contributed to the data. The first author used ChatGPT, an AI-based language model, to assist with polishing the language of the Introduction and Discussion sections. All content was reviewed and verified by the first author, who assumes full responsibility for the final manuscript.
Funding statement
This research was supported in part by (a) the Congressionally Directed Medical Research Programs, Neurofibromatosis Research Program [W81XWH2110504]; (b) the Intramural Research Program of the National Institutes of Health (NIH); (c) Florida State University Faculty Startup Funding; and (d) University of Kentucky Faculty Startup Funding. The contributions of the NIH authors were made as part of their official duties as NIH federal employees, are in compliance with agency policy requirements, and are considered Works of the United States Government. However, the findings and conclusions presented in this paper are those of the authors and do not necessarily reflect the views of the NIH or the U.S. Department of Health and Human Services. The study’s funders had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests
The authors have no conflicts of interest to disclose.







 Open access
Open access