


Intellectual and developmental disabilities (IDDs) refer to a group of conditions that occur during the developmental period, and are characterised by significant limitations in both intellectual functioning and adaptive behaviour. Reference Alnahdi and Schwab1 These limitations manifest themselves in conceptual, social and practical domains, and severely affect individuals’ daily functioning and long-term independence. According to the DSM-5, individuals with IDDs need ongoing support throughout their lives in performing basic life skills and social participation. The global prevalence of intellectual disabilities is estimated to be approximately 2–3%, and is even higher in low-income countries because of limited access to health services and inadequate preventive services. Reference Alnahdi and Schwab1
Families of individuals with IDDs, especially primary caregivers, face constant challenges in maintaining daily care routines, accessing adequate services and coping with the emotional and physical burden of caregiving. Research consistently shows that these mothers are at high risk of experiencing stress, anxiety and depression. Reference Anderson and Gerbing2,Reference Auberry3 As children transition into adulthood, difficulties in accessing appropriate services exacerbate family stress. Reference Auberry3 In addition, caregiving often coincides with the ageing of mothers, creating a dual burden that negatively affects family functioning.
Mothers take on a disproportionate share of caregiving responsibilities and become more vulnerable to negative health outcomes. Studies show that mothers with intellectual disabilities are at higher risk of experiencing health problems such as sleep disorders, musculoskeletal disorders and depression. Reference Borilli, Germano, de Avó, Pilotto and Melo4–Reference Eker and Arkar7 The decrease in the time that caregivers have for themselves negatively affects both their physical and emotional health, which leads to a decrease in quality of life and an increase in the burden of care. Reference Green8
The biopsychosocial model proposed by Engel Reference Engel9 provides a comprehensive theoretical framework for understanding human functioning through the dynamic interaction of biological, psychological and social systems. Within the context of IDDs, this model offers a useful lens to conceptualise how child-related characteristics (biological domain), maternal emotional and cognitive processes (psychological domain), and access to formal and informal support systems (social domain) interact to shape caregiver outcomes. Therefore, caregiving burden and maternal well-being should not be understood as isolated constructs, but rather as outcomes emerging from interconnected systemic influences.
Social support and caregiver well-being
Social support plays a critical role in the psychological adjustment processes of mothers caring for children with IDDs. Perceived social support refers to the emotional, informational or practical help that individuals perceive they receive from their social environment. Studies show that perceived social support alleviates the negative psychological effects of the care process by increasing coping skills and reducing emotional burden. Reference Hills and Argyle10 Low levels of social support were found to be associated with depressive symptoms, post-traumatic stress and negative parenting behaviours. Reference Hoffman, Marquis, Poston, Summers and Turnbull11,Reference Hosseini, Ramezani, Ashrafzadeh and Jamali12
The protective effect of social support is frequently emphasised in international literature. For example, Lunsky et al Reference Lunsky, Robinson, Blinkhorn and Ouellette-Kuntz13 found that social support is a preventive factor for burnout. Studies conducted in different cultural contexts show that strong social networks increase psychological resilience and increase life satisfaction in mothers of children with developmental disabilities. Reference Dimitrova-Radojichikj5,Reference Hosseini, Ramezani, Ashrafzadeh and Jamali14–Reference Sevgi and Ayran16 A study conducted in South Korea Reference Oh and Lee17 emphasised that social support reduces the burden of caregiving and promotes personal development, and a study conducted in the USA Reference Hoffman, Marquis, Poston, Summers and Turnbull11 found that higher levels of perceived social support were associated with more positive parenting outcomes and reduced family conflict.
In Turkey, because of the limited availability of formal support services, informal support – such as extended family, circle of friends or groups of mothers in similar situations – becomes much more decisive. Reference Kurt, Güneş Şan, Dinç and Uzun18 Recent studies Reference Jansen, Vissers and de Vries19,Reference Kay, Moulson, Vigod, Schoueri-Mychasiw and Singla20 highlight the importance of awareness-raising education programmes to empower families and reduce the burden of care. When families are informed and supported, they can develop more positive coping strategies and participate more actively in their children’s developmental processes.
Family quality of life, happiness and care burden
Family quality of life refers to the holistic well-being of family members, which is constituted by their level of satisfaction with various life domains such as health, emotional well-being, financial stability and social relationships. Reference Borilli, Germano, de Avó, Pilotto and Melo4,Reference Kurowska, Kózka and Majda21 In families with children with IDDs, family quality of life is affected by many variables such as the level of the child’s disability, the socioeconomic status of the family, access to services and the age, education and coping skills of the mothers. Reference Dimitrova-Radojichikj5,Reference Kurt, Güneş Şan, Dinç and Uzun18
As the child’s level of disability increases, mothers’ life satisfaction and psychological well-being have been found to decrease. Reference Alnahdi and Schwab1 It is stated that young mothers adapt to the care process more easily, and an increase in the level of education may differentiate the perception of quality of life depending on the context. In addition, emotional, economic and temporal care stress, defined as ‘family burden’, increases in the absence of adequate formal or informal support, and accordingly, happiness and perception of quality of life decrease. Reference Auberry3
Happiness, as a core component of subjective well-being, is frequently reported to be lower among mothers caring for individuals with IDDs. The ongoing demands of caregiving, restrictions in personal autonomy, and sustained physical and emotional strain may compromise psychological well-being in this population. In contrast, the presence of emotional support, opportunities for social participation and adequate economic resources have been associated with higher levels of happiness and overall well-being. Reference Lunsky, Robinson, Blinkhorn and Ouellette-Kuntz13
The biopsychosocial model proposed by Engel Reference Engel9 provides a comprehensive framework for understanding human functioning through the dynamic interaction of biological, psychological and social domains. Applied to the caregiving context, this model suggests that child-related disability characteristics (biological domain), maternal coping processes and emotional regulation (psychological domain), and access to formal and informal support systems (social domain) jointly shape caregiver outcomes. Accordingly, caregiving burden should not be conceptualised solely as an individual psychological experience; rather, it emerges from the interplay of multiple systemic influences. From a biopsychosocial perspective, these domains are inherently interdependent, and caregiving burden may operate both as a contextual stressor and as a mechanism indirectly influencing maternal happiness.
Studies in countries such as Canada, Australia and The Netherlands emphasise that increased family quality-of-life levels are positively associated with children’s developmental outcomes. Caregiver well-being is directly linked to the quality of parenting and the quality of the home environment. Reference Hoffman, Marquis, Poston, Summers and Turnbull11,Reference Meral and Cavkaytar22,Reference Granovetter, Sumrall, Lea, Gelles and Koehly23 Therefore, improving family quality of life and reducing the burden of caregiving are critical not only for mothers, but also for children’s long-term developmental outcomes.
Current study
In the existing literature, these variables have generally been examined independently. Reference Lunsky, Robinson, Blinkhorn and Ouellette-Kuntz13 However, studies that address these variables in a holistic manner for primary caregiver mothers are quite limited. A deeper understanding of the interactions between social support, family quality of life and happiness may enable the development of more effective interventions for care processes. Reference Hoffman, Marquis, Poston, Summers and Turnbull11,Reference Kurowska, Kózka and Majda21,Reference Perućica, Kalajdžić, Bakoč, Živanović and Škipina24 This study aims to examine the relationships between quality of life, happiness, perceived social support and family burden in mothers of individuals with IDDs from a correlational perspective. The study aims to contribute to the development of social support-based intervention strategies for mothers of individuals with IDDs. In this direction, the following questions were sought to be answered:
-
(a) Is there a mediating role of perceived social support between family burden and happiness of individuals with IDDs?
-
(b) Is there a mediating role of quality of life between family burden and happiness of individuals with IDDs?
-
(c) Is there a serial mediating role of quality of life and perceived social support between family burden and happiness of individuals with IDDs?
Method
Participants and procedure
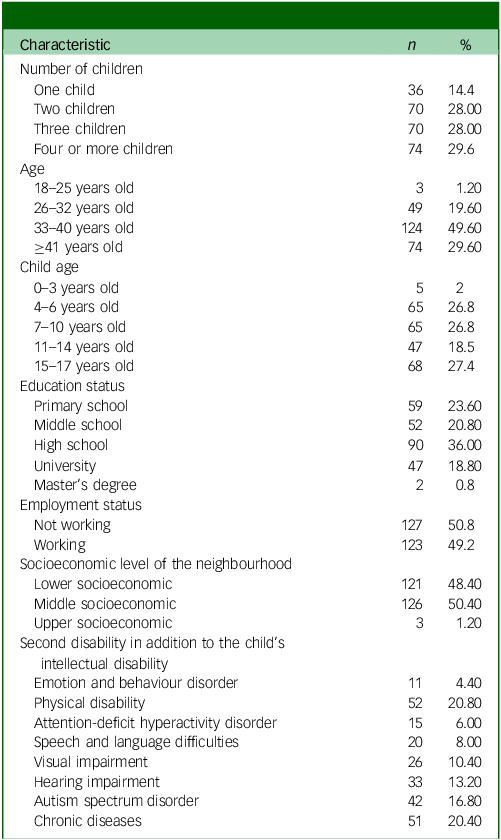
A total of 250 mothers of children with IDDs participated in this study. Participants were recruited through online parent networks and disability support groups, using a convenience sampling approach. Data were collected voluntarily via an online questionnaire. The obtained sample size surpassed the minimum requirements for structural equation modelling, and was deemed statistically sufficient for the analyses conducted. The demographic characteristics of the participants are detailed in Table 1.
Characteristics of the study group

Percentages exceed 100% because some children had more than one additional diagnosis.
Procedure
The data collection stages were carried out using tools created using Google Forms and accessible via a shareable link. In the informed consent form, families were asked not to share personal information and the purpose of the study was clearly stated. The duration of the questionnaire was set at 25–30 min, and mothers were given the right to withdraw if they did not participate in the study or felt uncomfortable after participating. The question ‘Do you want to participate in the study voluntarily?’ on the informed consent form were presented with yes or no options. When determining their participation preferences, participants were asked to check for yes or no boxes. The scales in Google Forms were designed to be accessible during the data collection period and then closed for data entry. As all form items were mandatory, no missing data occurred and no form was considered invalid. Participants were assured that their responses would remain confidential and anonymous and would only be used for research purposes. This study used a convenience sampling approach, as participants were recruited through online parent networks, disability support groups and social media platforms. Because participation was voluntary and depended on internet access and mothers’ willingness to engage, the sample may not fully represent all mothers of children with IDDs in Turkey.
Ethics statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human participants were approved by the Ethics Committee of Akdeniz University (approval number: 26.11.2024, 24/493).
Ethical approval was obtained before the data collection process. Informed consent was obtained from all participants before they took part in the study. Since the study involved mothers of children with IDDs and did not directly involve children, parental or guardian consent was not required for the children themselves. Participants were informed that their participation was voluntary, that they could withdraw at any time, and that their data would remain anonymous and confidential. Data collection from family for this study was conducted with the utmost consideration for ethical standards.
The study protocol was reviewed and approved by the appropriate educational authorities, ensuring that the research adhered to ethical guidelines and safeguarded the well-being of the participants. Participation in the study was entirely voluntary, and every effort was made to create a comfortable and supportive environment for the participants. Written informed consent was obtained from all participants by providing detailed information about the purpose, process, and possible effects of the study. During the consent process, it was clearly stated that the participants had the right to withdraw from the study at any stage, and that this decision would not lead to any negative consequences. In addition, all participants were assured that their data would be kept confidential and that the research results would be anonymised. This approach ensures that participants’ rights and privacy are protected and guarantees that the research is conducted in accordance with ethical principles.
Measures
Beach Center Family Quality of Life Scale
The Beach Center Family Quality of Life Scale is an instrument devised by the Beach Center on Disability at the University of Kansas, consisting of 25 questions organised into 5 domains; Reference Hoffman, Marquis, Poston, Summers and Turnbull11 the validity, reliability and adaptation study conducted by Meral and Cavkaytar Reference Meral and Cavkaytar22 produced the Turkish adaptation of the scale, which consists of five subdimensions: family interaction, parenting, emotional competence, physical/financial/material competence and support for disability. The highest score that can be obtained for the entire 5-point Likert-type scale consisting of a total of 25 items is 125, and the lowest score is 25. High scores indicate a high level of perception of family quality of life and low scores indicate a low level of perception of family quality of life. The internal consistency reliability coefficient of the scale was found to be 0.92.
The Oxford Happiness Questionnaire Short-Form
The Oxford Happiness Questionnaire was first developed by Argyle et al in 1989, as a 29-item structure. Later, it was revised by Hills and Argyle, Reference Hills and Argyle10 and the Oxford Happiness Questionnaire Short-Form was created. The adaptation, validity and reliability study of the scale into Turkish was conducted by Doğan and Akıncı Çötok. Reference Doğan and Akıncı Çötok6 The scale is a self-report-based, seven-item, five-point Likert-type scale (1 = strongly disagree, 5 = strongly agree) used to determine the subjective happiness levels of individuals. The total score that can be obtained from the scale varies between 7 and 35, and high scores indicate that the happiness level of the individual is high.
For the happiness construct, item parcelling was applied to improve model parsimony in the structural equation model, and two parcels (F1 and F2) were created using a balanced parcelling approach.
The Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MPSS) was developed by Zimet et al. Reference Zimet, Dahlem, Zimet and Farley25 to determine the adequacy of social support perceived by adolescents, and was adapted into Turkish by Eker et al. Reference Eker and Arkar7 The MPSS is a 12-item inventory that subjectively assesses the adequacy of social support received from 3 different sources: family, friends and an expert. The scale is a seven-point Likert-type inventory (scored between 1 and 7) ranging from ‘absolutely no’ to ‘absolutely yes’. The scale consists of three subdimensions: family subscale (includes items 3, 4, 8 and 11), friend subscale (includes items 6, 7, 9 and 12) and expert person subscale (includes items 1, 2, 5 and 10). Reference Zimet, Dahlem, Zimet and Farley25 The sum of the scores of each subscale (the lowest score is 4 and the highest score is 28) gives the score of the subscale, and the sum of the scores of all subscales (the lowest score is 12 and the highest score is 84) gives the total score of the scale.
A Family Burden Assessment Scale
A Family Burden Assessment Scale is a 5-point Likert-type measurement tool consisting of 6 sub-factors and 43 items, developed by Yıldırım Sarı, H. and Başbakkal, Reference Yıldırım-Sarı and Başbakkal26 to develop a valid and reliable family burden assessment scale for families with IDDs children. The subscales are economic, physical, emotional, social burden, perception of inadequacy and time requirement. The options are scored as ‘1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time/frequently, 5 = always’. High scores indicate that family burden is high. The cut-off point is nine points. The Cronbach’s α reliability coefficient of the scale is 0.92.
Data analysis
Before the main analyses, the data distribution was examined and found to be suitable for parametric analyses. Descriptive statistics, correlation analyses, reliability coefficients (Cronbach’s α, McDonald’s ω and Guttman’s λ), and convergent and discriminant validity analyses were conducted. All preliminary analyses were performed using IBM SPSS Statistics version 26.0 for Windows (IBM Corp., Armonk, New York, USA; https://www.ibm.com/products/spss) and JASP version 0.16.4 for Windows (JASP Team, Amsterdam, The Netherlands; https://jasp-stats.org/).
Structural equation modelling was employed to test the research questions following the two-stage approach proposed by Anderson and Gerbing. Reference Anderson and Gerbing2 First, the measurement model was evaluated, followed by testing of the structural model. Model fit was assessed with multiple indices, including the standardised root mean square residual (SRMR), root mean square error of approximation (RMSEA), comparative fit index (CFI), normalised fit index (NFI) and incremental fit index (IFI). In line with commonly accepted guidelines, SRMR and RMSEA values below 0.08, and CFI, TLI, NFI and IFI values close to or above 0.90, were considered indicative of acceptable model fit. Reference Hoyle, Panter and Hoyle27
Results
Preliminary analyses
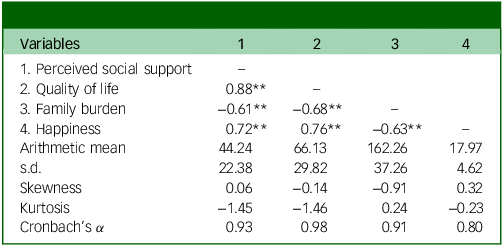
Table 1 presents the descriptive statistics and bivariate correlations among the study variables. Perceived social support was positively correlated with family quality of life (r = 0.88, p < 0.001) and happiness (r = 0.72, p < 0.001), and negatively correlated with family burden (r = −0.61, p < 0.001). Family quality of life was negatively associated with family burden (r = −0.68, p < 0.001) and positively associated with happiness (r = 0.76, p < 0.001). In addition, happiness was negatively correlated with family burden (r = −0.63, p < 0.001).
Preliminary analyses indicated that the data met the assumptions for parametric analyses. Skewness and kurtosis values were within acceptable ranges, internal consistency coefficients exceeded 0.80 for all scales and no evidence of multicollinearity was observed. Descriptive statistics and reliability coefficients for all study variables are presented in Table 2.
Relationships between variables and descriptive statistics

**p < 0.001.
Structural equation modelling
First, the measurement model including 4 latent and 16 observed variables was tested and demonstrated good model fit: χ 2(98, N = 250) = 508.00, χ 2/d.f. = 3.18, RMSEA = 0.065, SRMR = 0.058, TLI = 0.932, CFI = 0.944, NFI = 0.919 and IFI = 0.945. All indicators loaded significantly on their respective latent constructs, and reliability coefficients were high (α ≥ 0.80).
Following confirmation of the measurement model, the structural model was examined. In the partial mediation model, the direct path from family burden to happiness was not statistically significant (B = 0.10, p > 0.05). Although the NFI was slightly below the conventional 0.90 threshold (0.899), overall model fit was acceptable, consistent with recommendations for complex models in social science research. Reference Hoyle, Panter and Hoyle27
Consequently, the direct path was removed and the full mediation model was tested. The full mediation model showed good fit (χ 2(99, N = 250) = 525.20, χ 2/d.f. = 3.23, RMSEA = 0.061, SRMR = 0.061, TLI = 0.930, CFI = 0.942, NFI = 0.918, IFI = 0.943), and all structural paths were statistically significant.
Bootstrap analyses with 5000 resamples indicated that the indirect effect of family burden on happiness through perceived social support (B = −0.82, 95% bias-corrected and accelerated confidence interval (BCa CI) −1.18 to −0.55) and through family quality of life (B = −0.68, 95% BCa CI −0.91 to −0.47) were significant. Moreover, the sequential mediation of perceived social support and family quality of life fully accounted for the relationship between family burden and happiness (B = −0.059, 95% BCa CI −0.113 to −0.085). The final model is presented in Fig. 1.
Structural equation model of the serial mediation analysis. F1 and F2 indicate the two item parcels used to represent the happiness construct. **p < 0.01; F1–F2 parcel of happiness.

Discussion
This study adds to the growing body of research examining the well-being of mothers caring for children with IDDs, by integrating four key constructs – family burden, social support, family quality of life and happiness – into a single serial mediation model. This approach provides a clearer understanding of the mechanisms underlying caregivers’ well-being. By examining the relationships between quality of life, happiness, perceived social support and family burden in mothers of individuals with IDDs, this study provides a holistic perspective to understand the psychological well-being of caregiving mothers. Although the findings are consistent with both national and international literature, they also provide some unique contributions. Given the cross-sectional design, the study examines associations between variables rather than establishing causal relationships; therefore, expressions referring to ‘effects’ should be interpreted as statistical associations rather than causal pathways.
First, strong and positive relationships were found between perceived social support and both quality of life and happiness. This finding supports previous studies emphasising the importance of social support as a protective factor. Reference Borilli, Germano, de Avó, Pilotto and Melo4,Reference Engel9,Reference Šumskienė, Charenkova, Gvaldaitė, Seniutis, Gevorgianienė and Petružytė28 In particular, Lunsky et al Reference Lunsky, Robinson, Blinkhorn and Ouellette-Kuntz13 found that families with multiple care responsibilities experience high levels of stress and burnout, which increases the need for support. In the Turkish context, informal support networks (e.g. extended family, circle of friends, mothers with similar experiences) are known to be more decisive because of the limited availability of formal support services. Reference Jansen, Vissers and de Vries19,Reference Yıldırım-Sarı and Başbakkal26 In this context, in our study, it was observed that high perceived social support increased life satisfaction and decreased care burden. This reveals that not only the quantitative presence of social support, but also how it is perceived by the individual, is critical.
The finding of a negative relationship between perceived social support and family burden in the study points to the alleviating effect of supportive social relationships on care burden. This finding overlaps with the results of Oh and Lee, Reference Oh and Lee17 who emphasised the role of social support in reducing care burden in their study conducted in the South Korean context. Similarly, Kay et al’s Reference Kay, Moulson, Vigod, Schoueri-Mychasiw and Singla20 study in the USA shows that higher levels of perceived social support are associated with more positive parenting outcomes and reduced family conflict. These findings suggest that social support plays a universal protective role in different cultural contexts, and that it is even more decisive in countries with limited service infrastructure, such as Turkey.
Another important finding of the study was that there were significant negative correlations between family burden and quality of life and happiness. This result coincides with the work of Dimitrova-Radojichikj, Reference Dimitrova-Radojichikj5 who found that the perception of quality of life and happiness decreases when family burden is high. In addition, it has been emphasised in various studies that care burden is disproportionately distributed, especially for women, and that this is associated with negative health outcomes. Reference Eker and Arkar7,Reference Engel9,Reference Jansen, Vissers and de Vries19 This study shows that the negative effects on mothers’ health, psychological well-being and social lives are felt more intensely as the family burden increases. In fact, as Weiss et al Reference Weiss, Robinson, Fung, Tint, Chalmers and Lunsky29 stated, the decrease in the time that the caregiver has to spare for themselves leads to both physical and emotional burnout, which negatively affects life satisfaction.
Structural equation modelling findings show that the relationship between family burden and happiness is not direct, but indirect, through perceived social support and quality of life. This suggests that caregiver mothers’ happiness levels are not only related to the burden they are under, but also to how they cope with this burden and what kind of support systems they have access to. Although Engel Reference Engel9 stated that chronic stress, loss of autonomy and physical fatigue decrease levels of happiness, other studies have shown that social participation, emotional support and financial stability are associated with higher happiness and well-being. Reference Lunsky, Robinson, Blinkhorn and Ouellette-Kuntz13,Reference Šumskienė, Charenkova, Gvaldaitė, Seniutis, Gevorgianienė and Petružytė28,Reference Schworer, Ahmed, Hogenkamp, Moore and Esbensen30 Similarly, in this study, social support and quality of life stand out as determinants of mothers’ happiness. It should also be acknowledged that constructs such as family quality of life and perceived social support may partially overlap conceptually, as supportive family environments inherently contribute to both perceived social support and overall quality-of-life assessments. Future studies could employ alternative measurement models to further distinguish these dimensions.
Another noteworthy finding of the study is that quality of life is positively related to happiness and negatively related to family burden. This result shows that family quality of life is a multidimensional structure that affects not only individual satisfaction, but also the well-being of all family members. As Staunton et al Reference Staunton, Kehoe and Sharkey31 stated, family quality of life is not limited to health status or material conditions; it also includes elements such as social relationships, emotional competence and parenting roles. According to the findings of Alnahdi and Schwab, Reference Alnahdi and Schwab1 an increase in the child’s level of disability decreases the mother’s life satisfaction. Similarly, in this study, it was observed that quality-of-life scores decreased as care burden increased.
The impact of quality of life on mothers’ happiness is a frequently emphasised issue in the literature. For example, Kay et al Reference Kay, Moulson, Vigod, Schoueri-Mychasiw and Singla20 and Qian et al Reference Qian, Li, Xu, Ai, Li and Lei32 found that family quality of life is directly related to the quality of parenting and the quality of the home environment. Similarly, Jansen et al Reference Jansen, Vissers and de Vries19 reported that long-term developmental outcomes of children in families with high quality of life are also positively affected. In this context, improving quality of life is considered a critical goal not only for parental well-being, but also for children’s development.
Another important contribution of the study is the ability to fully explain the effect of family burden on happiness through the sequential mediation of social support and quality of life. This result supports the assumption that factors interact with each other and form a complex network of relationships based on the biopsychosocial model. In particular, it should be noted that stressors such as care burden are shaped by environmental and structural resources (social support, service access), as well as individual variables (coping strategies, self-efficacy). Reference Lunsky, Robinson, Blinkhorn and Ouellette-Kuntz13,Reference Granovetter, Sumrall, Lea, Gelles and Koehly23,Reference Weiss, Robinson, Fung, Tint, Chalmers and Lunsky29 These findings may also be associated with sociodemographic characteristics such as age, education level and employment status. As stated by Borilli et al, Reference Borilli, Germano, de Avó, Pilotto and Melo4 parental education, access to services and coping skills affect quality of life. In the current study, a significant portion of the sample was university graduates and came from a middle socioeconomic level, and that may have contributed to the high perception of social support and relatively positive quality-of-life scores.
When evaluated in the cultural context, it is seen that the care processes of individuals with IDDs in Turkey are generally based on women, public supports are insufficient and caregiving mothers have difficulty in benefiting from support systems. As emphasised by researchers such as Green Reference Green8 and Weiss et al, Reference Weiss, Robinson, Fung, Tint, Chalmers and Lunsky29 this care burden should be defined as a burden that has not only physical, but also emotional and social dimensions. The results of this study reveal that it is possible to alleviate the effects of this burden in the Turkish context through social support.
Limitations and suggestions
This study has several limitations that should be considered when interpreting the findings. First, its cross-sectional design precludes causal inferences among study variables. Although significant associations were identified, longitudinal studies are required to clarify the directionality of the relationships between family burdens, perceived social support, quality of life and happiness. Second, all data were collected using self-report measures, which may be subject to social desirability and response biases, particularly for subjective constructs such as happiness and quality of life. In addition, data collection was conducted online, and only mothers with internet access were able to participate, which may limit the representativeness of the sample. Finally, the sample primarily consisted of mothers from middle socioeconomic backgrounds. Therefore, the findings may not be generalisable to low-income, rural or less educated populations, whose access to support systems and caregiving experiences may differ.
Despite these limitations, our findings have important implications for research and practice. Strengthening informal and formal social support systems may improve the quality of life and well-being of mothers who care for individuals with IDDs. Psychoeducation and emotional support–based interventions developed in collaboration with public institutions and civil society organisations may help reduce caregiving burden and enhance coping skills, particularly when designed with cultural sensitivity.
Future research should include more diverse and representative samples and consider involving other family members, such as fathers, siblings or grandparents, to better understand role-sharing and burden distribution within families. Longitudinal and intervention-based studies are also valuable for examining causal mechanisms and evaluating the effectiveness of support-oriented programmes.
In conclusion, this study has made significant contributions to the literature by addressing the factors determining the psychological well-being of mothers caring for children with IDDs, in a multidimensional way. The main findings of the study show that social support and quality of life have direct and indirect effects on mothers’ well-being, and family burden plays a role as a critical variable in these relationships.
This study reveals that mothers with IDDs experience higher happiness levels when they perceive strong social support and maintain a high family quality of life. Conversely, caregiving burden negatively affects their well-being. A key finding is that caregiving burden does not directly reduce mothers’ happiness; instead, its impact is fully mediated by perceived social support and family quality of life. This highlights the pivotal buffering role of supportive social networks and a positive family environment in mitigating strain. For individuals with intellectual disabilities, the study underscores the indirect benefits of empowering caregivers through social support systems, as enhanced maternal well-being is associated with better caregiving outcomes and family functioning. For the research community, the study contributes a comprehensive model demonstrating the sequential mediation effect, offering empirical evidence to guide future intervention designs focused on improving both caregiver and care recipient outcomes within disability contexts.
This study makes two main contributions to the literature. First, by examining these variables within a serial mediation model, it presents a comprehensive framework that captures the complex mechanisms linking caregiving burden and well-being. Second, the results provide practical implications for the design of family-centred interventions. Strengthening informal and formal support systems, enhancing families’ access to psychosocial resources and developing culturally sensitive support programmes may substantially improve the well-being of caregiving mothers, and indirectly support positive developmental outcomes in children with IDDs.
Data availability
Researcher’s who wish to obtain additional data or conduct further analysis may contact the relevant authors to request supplementary information or materials. The corresponding author, A.E.S.Y., is willing to collaborate and provide the necessary information to support the results presented in the article.
Author contributions
A.E.S.Y. led the study design, conceptualisation, data collection and overall supervision of the research process; contributed substantially to data analysis and interpretation; and took the lead in writing the manuscript. Ö.A.K. contributed extensively to data analysis, literature review, interpretation of results and drafting major sections of the manuscript. H.M.S.D. contributed to the methodology section, data management and preliminary statistical analyses, and assisted in the organisation of the manuscript. M.A. provided support in advanced statistical analysis, assisted with the structural equation modelling procedures and contributed to the refinement of the Results section. Ş.D.D. contributed minimally by assisting with formatting, reference organisation and the final proofreading of the manuscript.
Funding
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.