


Since the onset of the COVID-19 pandemic in December 2019, millions of adults with a history of SARS-CoV-2 infection have developed a range of persistent, post-infection symptoms known as ‘long COVID’. Reference Chen, Haupert, Zimmermann, Shi, Fritsche and Mukherjee1,Reference OMahoney, Routen, Gillies, Ekezie, Welford and Zhang2 Also referred to as post-acute sequelae of COVID-19, long COVID is defined as the persistence or development of new symptoms within 3 months after the initial SARS-CoV-2 infection, with symptoms continuing for at least 2 months with no other alternative explanation. Reference Soriano, Murthy, Marshall, Relan and Diaz3 Long COVID is characterised by a diversity of neurological, cognitive, psychiatric and physical complications that may fluctuate and reappear overtime, and the condition is known to impact multiple organ systems with differing pathologies, resulting in a wide plethora of symptom profiles. Reference Davis, Assaf, McCorkell, Wei, Low and Reem4 Although the mechanisms of long COVID pathophysiology are unknown, current theories posit that viral persistence, immune dysregulation, microbial translocation, endothelial dysfunction, autoimmunity and dysregulated neurological signalling may contribute to its development and prognosis. Reference Davis, McCorkell, Vogel and Topol5 Given the novelty of this debilitating condition, the growing incidence of the condition and the lack of available treatment options at present, long COVID has emerged as a significant public health problem worldwide.
Growing research has highlighted the elevated prevalence and burden of psychiatric symptoms among adults living with long COVID. Recent findings from meta-analyses estimate that 16.2–23% of people with long COVID experience symptoms of depression, anxiety and/or post-traumatic stress; 13.5–45% experience sleep disturbances and 28.7–41% experience fatigue. Reference Poole-Wright, Guennouni, Sterry, Evans, Gaughran and Chalder6–Reference Zeng, Zhao, Yan, Li, Lu and Liu8 Large longitudinal studies have reported similar findings. For instance, a study of 797, 059 middle- to older-aged adults in the UK found elevated risk for incident and recurrent psychiatric disorders and psychotropic prescriptions 1 year after SARS-CoV-2 infection. Reference Wang, Su, Xie, Garcia-Rizo and Prieto-Alhambra9 Another study of adult patients in Colombia admitted to hospital for COVID-19 reported elevated prevalence rates of anxiety (16.6%), depression (21.8%), post-traumatic stress disorder (PTSD) (35.3%) and insomnia symptoms (23.9%) 2 years after discharge. Reference Guillen-Burgos, Galvez-Florez, Moreno-Lopez, Gonzalez, Guillen and Anaya10 Demographic factors including older age, female gender, lower socioeconomic status and clinical factors such as pre-existing mental health conditions, severity of initial COVID-19 infection, disease comorbidities, and hospital and intensive care unit admission have been identified as risk factors for psychiatric morbidity in adults with long COVID. Reference Zeng, Zhao, Yan, Li, Lu and Liu8,Reference Sudre, Murray, Varsavsky, Graham, Penfold and Bowyer11,Reference Taquet, Geddes, Husain, Luciano and Harrison12
Current literature suggests that symptom severity during the acute phase of SARS-CoV-2 infection may predict the prevalence and severity of psychiatric symptoms in long COVID. Reference Wang, Su, Xie, Garcia-Rizo and Prieto-Alhambra9,Reference Hastie, Lowe, McAuley, Winter, Mills and Black13 Adults with asymptomatic COVID-19 tend to report the lowest prevalence of long-term neuropsychiatric symptoms, whereas the highest prevalence of prolonged neuropsychiatric symptoms is seen in patients admitted to hospital and critically ill patients with COVID-19. Reference Zeng, Zhao, Yan, Li, Lu and Liu8 The number of acute symptoms in symptomatic patients may also be predictive of psychiatric symptoms of long COVID. Reference Sudre, Murray, Varsavsky, Graham, Penfold and Bowyer11,Reference Robineau, Zins, Touvier, Wiernik, Lemogne and de Lamballerie14 Symptom severity may lead to a greater likelihood of prolonged psychiatric morbidity in adults with long COVID for several reasons, including chronic neuroinflammation, post-intensive care syndrome, psychosocial stress and trauma associated with fear and uncertainty, and pathologic brain alterations. Reference Díez-Cirarda, Yus-Fuertes, Sanchez-Sanchez, Gonzalez-Rosa, Gonzalez-Escamilla and Gil-Martínez15,Reference Pandharipande, Roberson, Harrison, Wilson, Bastarache and Ely16 Studies have reported that COVID-19-induced psychiatric sequelae may persist for as long as 2 years after incident SARS-CoV-2 infection, which include symptoms of anxiety, depression and psychotic disorders. Reference Colizzi, Comacchio, De Martino, Peghin, Bontempo and Chiappinotto17–Reference Taquet, Sillett, Zhu, Mendel, Camplisson and Dercon19
Although research on long COVID has grown substantially in the past 4 years, most findings have come from Western and high-income countries. Reference OMahoney, Routen, Gillies, Ekezie, Welford and Zhang2,Reference Ferrari, Santomauro, Aali, Abate, Abbafati and Abbastabar20 Pooled prevalence estimates using SARS-CoV-2 seroprevalence data between 2020 and 2021 found that 65.1% of adults in Africa were previously exposed to the virus, among the highest globally at the time, and these rates only increased as new strains of the virus circulated. Reference Lewis, Ware, Whelan, Subissi, Li and Ma21 Using anti-nucleocapsid antibody data, researchers reported an 87% national seroprevalence rate in South Africa after the first Omicron wave between January 2021 and March 2022, whereas another study of unvaccinated adults in four African countries (Democratic Republic of Congo, Guinea, Libera, Mali) found a seroprevalence rate of 83% between August 2021 and June 2022, yet seroprevalence rates across the continent remain heterogenous. Reference Vermeulen, Mhlanga, Sykes, Cable, Coleman and Pietersen22,Reference Laverdure, Kazadi, Kone, Callier, Dabitao and Dennis23 A recent systematic review of 24 studies on long COVID in Africa reported a large range of long COVID prevalence rates, ranging from 2% in Ghana to 86% in Egypt, with several studies reporting prolonged psychiatric symptoms of depression, anxiety, PTSD and sleep disturbances. Reference Müller, Isaaka, Mumm, Scheidt-Nave, Heldt and Schuster24
Compared with high-income countries, low- and middle-income countries (LMICs) tend to experience greater structural constraints in their public healthcare systems that increase population-level long COVID risk, which include limited healthcare access, lower diagnostic capacity and poorer vaccine coverage. Reference Abel, Roope, Duch and Clarke25–Reference Zhou, Feng, Hu, Yang, Chen and Bastow27 Socioeconomic inequities in these settings further exacerbate risks for developing long COVID, because of adverse housing and employment conditions that may increase exposure to SARS-CoV-2; limited infrastructures for washing, sanitation and public health education; and psychosocial stress pathways that may compromise immune regulation and recovery. Reference Harris, Hart, Bhattacharya and Russell28,Reference Josephson, Kilic and Michler29 South African populations face a range of vulnerabilities to long COVID because of the country’s prolonged history of racial and social inequality under apartheid, overburdened public healthcare systems and elevated rates of comorbidities known to increase risk for long COVID, such as cardiometabolic conditions (e.g. diabetes, hypertension, obesity) and infectious diseases (e.g. HIV, tuberculosis). Reference Kim, Said Mohamed, Norris, Richter and Kuzawa30 By March 2023, South Africa’s National Institutes for Communicable Disease confirmed over 4.07 million cases of COVID-19. A small number of studies have reported elevated prevalence rates of long COVID in South Africa, which range from 35 to 66.7%. Reference Dryden, Mudara, Vika, Blumberg, Mayet and Cohen31,Reference Mendelsohn, Nath, De Sá and Von Pressentin32 Although LMICs have faced among the highest incidence rates and burden of COVID-19 and experience the greatest burden of physical and mental illnesses, Reference Hou, Gu, Ni, Shi, Ranney and Mukherjee33 little is known about the psychiatric symptoms of long COVID in LMICs, especially in Africa. Methodological shortcomings in long COVID studies have also compromised the comparison and generalisability of results, such as the lack of a control group. A recent systematic review found that only 11% of long COVID studies included a control group in their study design. Reference OMahoney, Routen, Gillies, Ekezie, Welford and Zhang2 To address this gap in the literature, we conducted a study in Johannesburg, South Africa with three groups of adults with confirmed SARS-CoV-2 infection and a vaccinated control group. This study had four aims:
-
(a) to estimate the prevalence of psychiatric symptoms, stratified by past COVID-19 severity;
-
(b) to estimate the associations between past COVID-19 severity (exposure) and current psychiatric symptoms (outcome);
-
(c) to estimate the association between current long COVID symptoms (exposure) and current psychiatric symptoms (outcome);
-
(d) to examine the possible mediating effect of current long COVID symptoms (mediator) in the association between past COVID-19 severity (exposure) and current psychiatric symptoms (outcome).
Method
Study design
This observational, case–control study took place at the Ezintsha Research Centre in Johannesburg, South Africa. Data collection took place between 16 August 2022 and 12 July 2023. Participants were identified based on previous enrolment in research studies at Ezintsha and partner study sites, and further recruited by using advertisements for study participation. Study staff obtained informed consent from potential participants before being screened for inclusion in one of four groups: group 1, previous asymptomatic SARS-CoV-2 infection confirmed by a documented positive polymerase chain reaction (PCR), antigen or antibody test during routine screening; group 2, previous symptomatic COVID-19 confirmed by a documented positive PCR or antigen test in the setting of out-patient management; group 3, previous symptomatic COVID-19 confirmed by a documented positive PCR or antigen test in the setting of in-patient hospital stay; and group 4, previous asymptomatic or symptomatic SARS-CoV-2 infection, confirmed through a documented positive PCR, antigen or antibody test, and receipt of a COVID-19 vaccine in a non-placebo arm of a COVID-19 vaccine study during 2020.
Group 1. Previous asymptomatic SARS-CoV-2 infection confirmed by a documented positive PCR/antigen/antibody test during routine screening.
Group 2. Previous symptomatic COVID-19 confirmed by a documented positive PCR or antigen test in the setting of outpatient management.
Group 3. Previous symptomatic COVID-19 confirmed by a documented positive PCR or antigen test in the setting of inpatient hospitalisation.
Group 4. Previous asymptomatic or symptomatic SARS-CoV-2 infection, confirmed through a documented positive PCR, antigen, or antibody test, and receipt of a COVID-19 vaccine in a non-placebo arm of a COVID-19 vaccine study during 2020.
All positive COVID-19 test results were required to have taken place at least 6 months before the initial visit. Additional inclusion criteria were as follows: ability to provide written or electronic informed consent, aged ≥18 years, willing to consent to verification of vaccination status in a national database and access to a telephone or digital communication device. Exclusion criteria included the following: a positive COVID-19 test within 3 months of the baseline visit; symptomatic SARS-CoV-2 infection at any stage before the study visit (for inclusion in group 1); SARS-CoV-2 infection, confirmed through a documented positive PCR, antigen or antibody test, before vaccination in a non-placebo arm of a COVID-19 vaccine study during 2020 (for inclusion in group 4); and any physical, mental or social condition that may interfere with the completion of baseline assessments. Group 4 served as the control group for this study as their participation in the first vaccine trials as non-placebo participants provided them the earliest protection against virus. Given that participants of the first vaccine trials were exposed to the first wave of COVID-19 infections in South Africa during which severe lockdown measures were in place, the probability of being infected with SARS-CoV-2 before vaccination was low.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. This study received ethical approval from the Human Research Ethics Committee at the University of the Witwatersrand (application #220304B) and the South African Health Products Regulatory Authority. The study protocol was registered with the South African National Clinical Trial Registry (www.sanctr.gov.za), National Human Research Ethics Committee (www.ethicsapp.co.za) and www.ClinicalTrials.gov (NCT05445713).
Study measures
A demographic questionnaire collected participant characteristics such as age, gender, employment status, income brackets and substance use history (tobacco and alcohol). Gender was assessed with a binary variable (male: 1, female: 2). Socioeconomic status was measured with a checklist of five different household assets (e.g. computer, electric stove, television, vehicle, washing machine), which were summed to create a total score ranging from 0 to 5. Employment status was assessed with a binary measure (unemployed: 0, employed: 1). Body mass index was calculated with anthropometric measures of height and weight.
Number of acute COVID-19 symptoms experienced during the incident infection were inventoried retrospectively, using a self-reported checklist of 14 key symptoms of SARS-CoV-2 infection, which included the following: fever, chills, headaches, myalgia, cough, difficulty breathing, dizziness, fatigue, sore throat, nausea/vomiting, diarrhoea, shortness of breath, ageusia and anosmia. COVID-19 infection history was measured by assessing the number of times the participant tested positive for SARS-CoV-2. An extensive medical history was collected to assess the presence of disease comorbidities. Number of days elapsed between incident COVID-19 infection, confirmed by a documented positive PCR, antigen or antibody test, and the date of data collection also was calculated. Finally, social support was assessed with the Multidimensional Scale of Perceived Social Support, a 12-item, seven-point Likert-based measure of perceived adequacy of social support from family, friends and significant other (α = 0.89).
Possible long COVID symptoms were collected with a survey that assessed 23 symptoms experienced within the past 4 weeks, which included the following: poor vision, ringing/buzzing in ear, stomach pain, back pain, pain in arms/legs/joints, headaches, chest pain, fever/chills, fainting, shortness of breath, pain or problems during sex, constipation or loose bowels, nausea/gas/indigestion, body numbness, tingling or pickling sensation in body, cough, loss of smell, loss of taste, diarrhoea, sore throat, hair loss, weight loss and runny nose. Participants were queried to what extent each of the symptoms bothered them from a scale of 1–3 (not bothered at all: 1, bothered a little: 2, bothered a lot: 3). A total score was created by summing all values (α = 0.88).
Mental health outcomes were assessed with a series of psychological symptom screeners. Depressive symptoms were assessed with the Patient Health Questionnaire-9 (PHQ-9), a nine-item battery that assesses key symptoms of depression, such as fatigue, irritability and melancholia (α = 0.84). The last question of the PHQ-9 queries thoughts of suicidal ideation, which was used separately to assess suicide risk. Anxiety symptoms were captured with the Generalised Anxiety Disorder-7 (GAD-7), a seven-item measure that assesses the severity of anxiety, including symptoms of nervousness, rumination and restlessness (α = 0.86). PTSD symptoms were measured with the PTSD Checklist – Civilian Version (PCL-C), which comprises 17 questions that assess major disease symptoms on a five-point Likert scale (α = 0.94). Although PTSD diagnoses typically query symptoms in response to a Criterion A event, the PCL-C assesses PTSD symptoms related to a set of ‘stressful experiences’ faced by the individual and can be viewed as a screening tool for PTSD symptoms. Bipolar disorder symptoms were measured with the Mood Disorder Questionnaire (MDQ), which assesses symptoms such as increased energy, grandiosity, decreased need for sleep and others. The first 13 items of the MDQ were summed to create a composite score of bipolar disorder symptoms (α = 0.83). Somatic symptoms were measured with the Patient Health Questionnaire-15 (PHQ-15), a 15-item survey that assesses symptoms of somatisation such as bodily pain, dizziness and heart palpitations (α = 0.85). The PHQ-15 was assessed shortly after the beginning of data collection and completed by a smaller number of participants. All participants completed 14 out of 15 questions of the PHQ-15 as the remaining question assessed the severity of menstrual cramps or problems with menstruation, which was not relevant for all participants. Data were summed to create a total score for the PHQ-14. A female-only subsample completed all 15 questions of the PHQ-15.
The following cut-off scores were used for the following measures, which were validated or previously used in past studies in South African adults: ≥10 (PHQ-9), ≥2 (question 9 on the PHQ-9), ≥10 (GAD-7), ≥44 (PCL-C), ≥7 (MDQ) and ≥10 (PHQ-15) Reference Kim, Swana and Sarma34,Reference Byansi, Galvin, Chiwaye, Luvuno, Kim and Sundararajan35 PHQ-14 scores were rescaled to fit a 0-30 range in order to calculate caseness using the ≥10 cutoff score in the full sample. The original ≥10 cut-off score was used for the female-only subsample that completed the full PHQ-15.
Statistical analysis
All analyses were conducted in Stata 16 (College Station, Texas, USA; https://www.stata.com/stata16/). COVID-19 severity group (i.e. placement in groups 1–4) and number of acute COVID-19 symptoms served as the exposure variables in two separate analyses. COVID-19 severity group was treated as a factor variable, and the vaccinated control group (group 4) served as the reference group. Number of acute COVID-19 symptoms was summed to create a total symptom score. Descriptive statistics were calculated to identify possible outliers and test for overdispersion. No major outliers were present in the data, and all mental health outcome variables were overdispersed. We estimated the bivariate correlations between COVID-19 severity group, number of acute symptoms, mental health outcomes and potential covariates. We fitted multivariable negative binomial regression models specifying current psychiatric symptoms as the outcome, with robust standard errors to account for overdispersion and heteroskedasticity. Demographic, behavioural, medical and social factors thought to potentially confound the relationship between COVID-19 severity group and mental health were included as covariates, which included age, gender, assets, employment status, income, body mass index, tobacco use, alcohol consumption, COVID-19 infection history, psychiatric diagnoses and medical comorbidities. Raw summed values were used for models predicting PHQ-14 and PHQ-15 scores.
We then examined the potential mediating role of long COVID symptoms by using the causal mediation framework proposed by Imai and colleagues. Reference Imai, Keele and Tingley36 Linear regression models were employed to estimate the average causal mediation effect (ACME), defined as the average change in current psychiatric symptoms associated with changes in long COVID symptoms under lower versus higher exposure to acute COVID-19 symptoms, as well as the average direct effect, capturing all remaining pathways linking acute COVID-19 symptoms to current psychiatric symptoms. All models controlled for the same demographic and socioeconomic covariates described above, and cluster-robust standard errors were applied.
Estimation of the ACME and average direct effect relied on the assumption of sequential ignorability, which requires that acute COVID-19 symptoms (the primary exposure) be independent of all potential outcomes and mediators, and that current long COVID symptoms (the mediator) be independent of current psychiatric symptoms after conditioning on acute COVID-19 symptoms and baseline covariates. To assess the sensitivity of the mediation results to potential violations of this assumption, we applied the sensitivity analysis developed by Imai et al. Reference Imai, Keele and Tingley36 This approach evaluates the extent to which unmeasured confounding – captured by the correlation between the error terms of the mediator and outcome models – would need to be present to render the estimated ACME null.
Results
Descriptive statistics
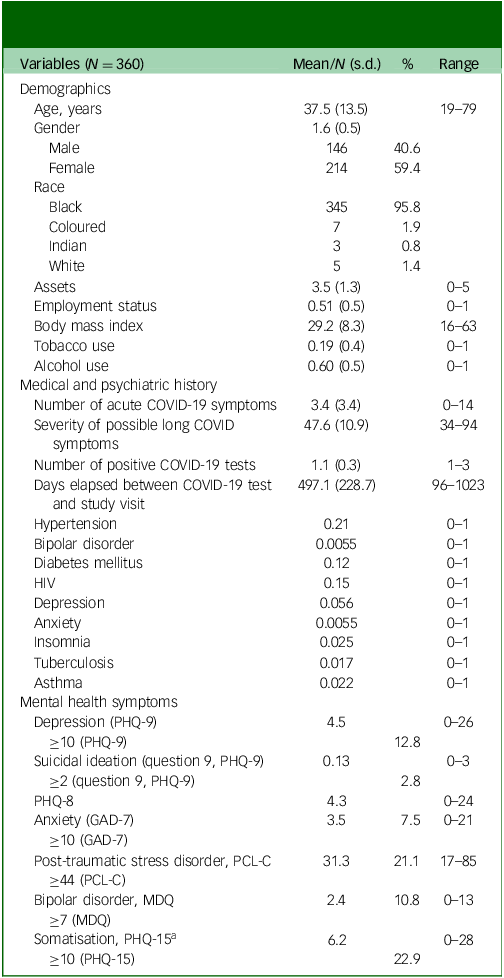
A total of 375 adults were enrolled in this study, and 360 adults were included in the analytic sample. Listwise deletion was used to address missing data, as <5% of all participants had missing data on focal variables. Table 1 describes the demographic characteristics of each group and the full sample. Total numbers of participants in each group were as follows: n = 96 for group 1, n = 100 for group 2, n = 98 for group 3 and n = 66 for group 4. The average age was 37.5 years and 59% identified as female. The average number of household assets was 3.5 out of a total of 5 items, and 51% were employed. The average number of acute COVID-19 symptoms was 3.4 (s.d. 3.4), and average number of days elapsed between incident COVID-19 infection and data collection was 497 days (s.d. 229). For medical comorbidities, 21% of participants reported a hypertension diagnosis, 15% of participants reported an HIV diagnosis and 12% of participants reported a diabetes diagnosis. For psychiatric comorbidities, 5.6% of participants reported a depression diagnosis and <1% reported diagnoses of bipolar disorder and/or anxiety. The prevalence rates of psychiatric ‘caseness’ determined by symptom screening scales were as follows: 12.8% for depression, 2.8% for suicidal ideation, 7.5% for anxiety, 21.1% for PTSD, 10.8% for bipolar disorder and 23.2% for somatisation.
Demographic characteristics, social experiences and mental health

Table 1 Long description
The table presents demographic characteristics, social experiences, and mental health data of 360 adults in a study. It includes variables such as age, gender, race, assets, employment status, body mass index, tobacco use, alcohol use, and medical and psychiatric history. The table also covers mental health symptoms like depression, suicidal ideation, anxiety, post-traumatic stress disorder, bipolar disorder, and somatization. The table has 8 rows and 4 columns. Column headers are Variables, n = 360 (s.d.), %, and Range. Row labels include Demographics, Age, Gender, Male, Female, Race, Black, Coloured, Indian, White, Assets, Employment status, Body mass index, Tobacco use, Alcohol use, Medical and psychiatric history, Number of acute COVID-19 symptoms, Severity of possible long COVID symptoms, Number of positive COVID-19 tests, Days elapsed between COVID-19 test and study visit, Hypertension, Bipolar disorder, Diabetes mellitus, HIV, Depression, Anxiety, Insomnia, Tuberculosis, Asthma, Mental health symptoms, Depression (PHQ-9), ≥10 (PHQ-9), Suicidal ideation (question 9, PHQ-9), ≥2 (question 9, PHQ-9), PHQ-8, Anxiety (GAD-7), ≥10 (GAD-7), Post-traumatic stress disorder, PCL-C, ≥44 (PCL-C), Bipolar disorder, MDQ, ≥7 (MDQ), Somatisation, PHQ-15, ≥10 (PHQ-15). Values are provided for each variable under the columns n = 360 (s.d.), %, and Range. Notable trends include the average age of 37.5 years, 59% identifying as female, and various prevalence rates of medical and psychiatric conditions.
PHQ-9, Patient Health Questionnaire-9; PHQ-8, Patient Health Questionnaire-8 (PHQ-9 total score calculated without Question 9 on self-farm/suicide risk); GAD-7, Generalised Anxiety Disorder-7; PCL-C, PTSD Checklist – Civilian Version; MDQ, Mood Disorder Questionnaire; PHQ-15, Patient Health Questionnaire-15.
a. Sample size for this measure is 306.
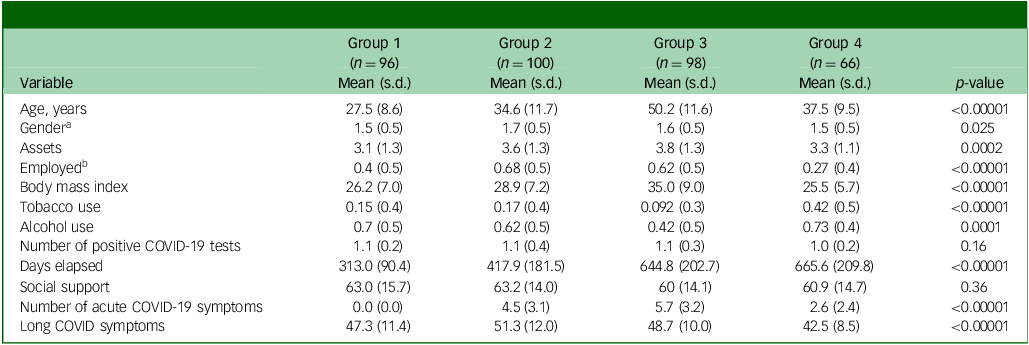
Unadjusted one-way analyses of variance found that the four COVID-19 severity groups varied significantly across demographic characteristics based on age, gender, assets, employment status, tobacco use, alcohol use, body mass index, days elapsed since acute COVID-19, number of acute COVID-19 symptoms and current long COVID symptoms, but not by COVID-19 infection history and social support (Table 2).
Group characteristics and comparisons

a. Male = 1, female = 2.
b. Unemployed = 0, employed = 1.
Regression analyses
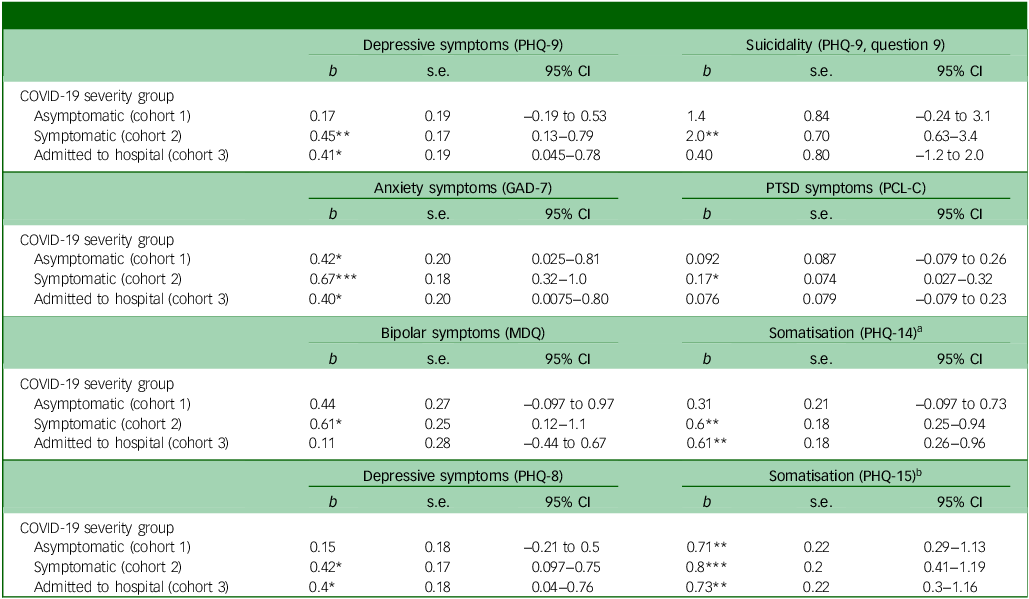
In fully adjusted models (Table 3), patients in the out-patient symptomatic COVID-19 severity group (group 2) exhibited the worst mental health outcomes out of all groups relative to vaccinated controls in nearly all models (group 4). Specifically, symptomatic patients reported elevated symptoms of depression (b = 0.45, p = 0.007, 95% CI 0.13–0.79), suicidal ideation (b = 2.0, p = 0.004, 95% CI 0.63–3.4), anxiety (b = 0.67, p < 0.001, 95% CI 0.32–1.0), PTSD (b = 0.17, p = 0.021, 95% CI 0.027–0.032), bipolar disorder (b = 0.61, p = 0.014, 95% CI 0.12–1.1), somatisation (b = 0.60, p = 0.001, 95% CI 0.25–0.94) and somatisation in the female subsample (b = 0.80, p < 0.0001, 95% CI 0.41–1.2). Asymptomatic patients and patients admitted to hospital also exhibited significantly elevated mental health symptoms relative to controls for certain conditions. Asymptomatic patients reported significantly heightened symptoms of anxiety, and female asymptomatic adults exhibited higher levels of somatisation. Patients who were admitted to hospital displayed significantly elevated symptoms of depression, anxiety and somatisation, both in the female subsample and the full sample. Female gender, tobacco use and depression diagnosis were common risk factors for elevated psychiatric morbidity, whereas social support was a protective factor against poor mental health in nearly all models.
Regression models predicting long-term mental health effects by COVID-19 severity group

Table 3 Long description
The table presents regression models predicting long-term mental health effects by COVID-19 severity group. It includes data on depressive symptoms (PHQ-9), suicidality (PHQ-9, question 9), anxiety symptoms (GAD-7), PTSD symptoms (PCL-C), bipolar symptoms (MDQ), and somatisation (PHQ-14 and PHQ-15). The table is divided into rows and columns, with each row representing a different COVID-19 severity group: Asymptomatic (cohort 1), Symptomatic (cohort 2), and Admitted to hospital (cohort 3). Each column represents different mental health outcomes and their respective statistical values: b, s.e., and 95% CI. Row 1: Depressive symptoms (PHQ-9): Asymptomatic (cohort 1) b 0.17, s.e. 0.19, 95% CI -0.19 to 0.53; Symptomatic (cohort 2) b 0.45, s.e. 0.17, 95% CI 0.13 to 0.79; Admitted to hospital (cohort 3) b 0.41, s.e. 0.19, 95% CI 0.045 to 0.78. Row 2: Suicidality (PHQ-9, question 9): Asymptomatic (cohort 1) b 1.4, s.e. 0.84, 95% CI -0.24 to 3.1; Symptomatic (cohort 2) b 2.0, s.e. 0.70, 95% CI 0.63 to 3.4; Admitted to hospital (cohort 3) b 0.40, s.e. 0.80, 95% CI -1.2 to 2.0. Row 3: Anxiety symptoms (GAD-7): Asymptomatic (cohort 1) b 0.42, s.e. 0.20, 95% CI 0.025 to 0.81; Symptomatic (cohort 2) b 0.67, s.e. 0.18, 95% CI 0.32 to 1.0; Admitted to hospital (cohort 3) b 0.40, s.e. 0.20, 95% CI 0.0075 to 0.80. Row 4: PTSD symptoms (PCL-C): Asymptomatic (cohort 1) b 0.092, s.e. 0.087, 95% CI -0.079 to 0.26; Symptomatic (cohort 2) b 0.17, s.e. 0.074, 95% CI 0.027 to 0.32; Admitted to hospital (cohort 3) b 0.076, s.e. 0.079, 95% CI -0.079 to 0.23. Row 5: Bipolar symptoms (MDQ): Asymptomatic (cohort 1) b 0.44, s.e. 0.27, 95% CI -0.097 to 0.97; Symptomatic (cohort 2) b 0.61, s.e. 0.25, 95% CI 0.12 to 1.1; Admitted to hospital (cohort 3) b 0.11, s.e. 0.28, 95% CI -0.44 to 0.67. Row 6: Somatisation (PHQ-14): Asymptomatic (cohort 1) b 0.31, s.e. 0.21, 95% CI -0.097 to 0.73; Symptomatic (cohort 2) b 0.60, s.e. 0.18, 95% CI 0.25 to 0.94; Admitted to hospital (cohort 3) b 0.61, s.e. 0.18, 95% CI 0.26 to 0.96. Row 7: Depressive symptoms (PHQ-8): Asymptomatic (cohort 1) b 0.15, s.e. 0.18, 95% CI -0.21 to 0.5; Symptomatic (cohort 2) b 0.42, s.e. 0.17, 95% CI 0.097 to 0.75; Admitted to hospital (cohort 3) b 0.4, s.e. 0.18, 95% CI 0.04 to 0.76. Row 8: Somatisation (PHQ-15): Asymptomatic (cohort 1) b 0.71, s.e. 0.22, 95% CI 0.29 to 1.13; Symptomatic (cohort 2) b 0.80, s.e. 0.2, 95% CI 0.41 to 1.2; Admitted to hospital (cohort 3) b 0.73, s.e. 0.22, 95% CI 0.3 to 1.16.
b, unstandardised regression weights; PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalised Anxiety Disorder-7; PCL-C, PTSD Checklist – Civilian Version; MDQ, Mood Disorder Questionnaire; PHQ-14, Patient Health Questionnaire-14; PHQ-8, Patient Health Questionnaire-8; PHQ-15, Patient Health Questionnaire-15.
*p < 0.05, **p < 0.01, ***p < 0.001.
a. This model includes the full sample and excludes the question on menstrual cramps (n = 306).
b. This model only includes women and includes the question on menstrual cramps (n = 184).
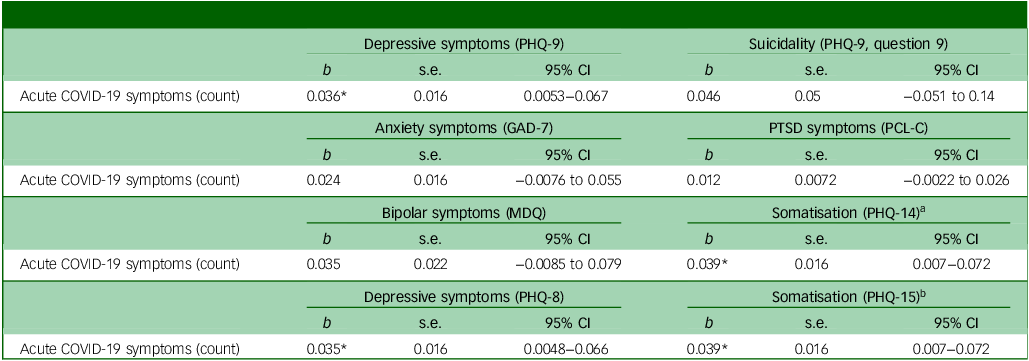
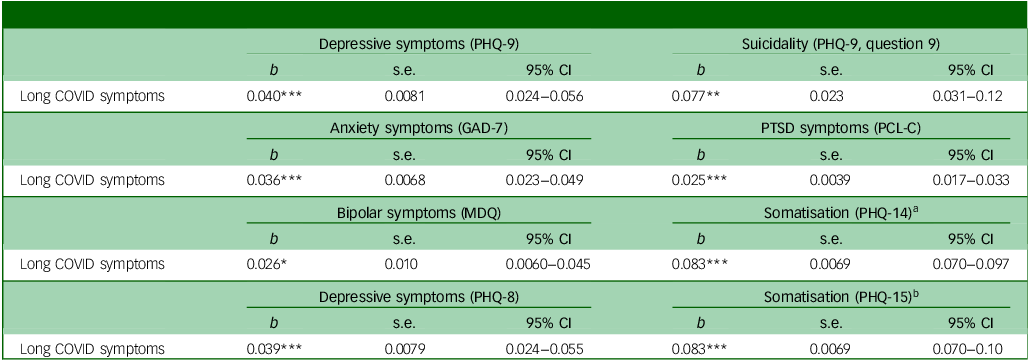
The number of COVID-19 symptoms was significantly associated with depression, somatisation and the female-only measure of somatisation (Table 4). Finally, the severity of current long COVID symptoms was directly associated with all measures of mental health, including depression, suicidal ideation, anxiety, PTSD, bipolar disorder and somatisation (p < 0.0001) (Table 5).
Regression models predicting associations between number of acute COVID-19 symptoms and long-term mental health effects

b, unstandardised regression weights; PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalised Anxiety Disorder-7; PCL-C, PTSD Checklist – Civilian Version; MDQ, Mood Disorder Questionnaire; PHQ-14, Patient Health Questionnaire-14; PHQ-8, Patient Health Questionnaire-8; PHQ-15, Patient Health Questionnaire-15.
*p < 0.05, **p < 0.01, ***p < 0.001.
a. This model includes the full sample and excludes the question on menstrual cramps (n = 306).
b. This model only includes women and includes the question on menstrual cramps (n = 184).
Regression models predicting associations between possible long COVID symptoms and long-term mental health effects

b, unstandardised regression weights; PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalised Anxiety Disorder-7; PCL-C, PTSD Checklist – Civilian Version; MDQ, Mood Disorder Questionnaire; PHQ-14, Patient Health Questionnaire-14; PHQ-8, Patient Health Questionnaire-8; PHQ-15, Patient Health Questionnaire-15.
*p < 0.05, **p < 0.01, ***p < 0.001.
a. This model includes the full sample and excludes the question on menstrual cramps (n = 306).
b. This model only includes women and includes the question on menstrual cramps (n = 184).
Mediation analyses
Current long COVID symptoms significantly mediated the association between acute COVID-19 symptoms and four mental health outcomes: depression, anxiety, PTSD and somatisation in the full sample (PHQ-14). In all four models, acute COVID-19 symptoms were positively associated with current long COVID symptoms, and current long COVID symptoms were positively associated with worse mental health symptoms.
Acute COVID-19 symptoms were associated with current long COVID symptoms (b = 0.4, 95% CI 0.03–0.7), and long COVID symptoms were correlated with depression scores (b = 0.17, 95% CI 0.1–0.2). In models predicting anxiety symptoms, acute COVID-19 symptoms were related to long COVID symptoms (b = 0.4, 95% CI 0.03–0.7), and long COVID symptoms were associated with anxiety scores (b = 0.14, 95% CI 0.09–0.2). Models predicting PTSD symptoms found that acute COVID-19 symptoms were associated with long COVID symptoms (b = 0.4, 95% CI 0.03–0.7), and long COVID symptoms were associated with PTSD scores (b = 0.9, 95% CI 0.6–1.2). Finally, in models predicting somatisation in the full sample, acute COVID-19 symptoms were correlated with current long COVID symptoms (b = 0.4, 95% CI 0.03–0.7), and long COVID symptoms were associated with somatisation scores (b = 0.71, 95% CI 0.7–0.8). In all mediation models, the direct and indirect effects were not significant. Furthermore, the proportions mediated were not interpreted because of the small and imprecisely estimated total effect, which rendered the proportion mediated unstable. Current long COVID symptoms did not mediate the association between acute COVID-19 symptoms and the following mental health outcomes: suicidality, bipolar disorder and somatisation in the female subsample.
Sensitivity analyses
The results of our sensitivity analysis showed that a correlation of ρ = 0.26 between the error terms of the mediator model and the outcome model for depression scores would be necessary for the ACME to equal zero. Thus, the product of the R 2-values for the mediator model and the outcome model would have to be 0.068 for the ACME to be zero. Such a pattern of correlations could be consistent with, for example, an omitted confounder explaining 26% of the remaining variance in long COVID symptoms and 26% of the remaining variance in depression scores (0.26 × 0.26 = 0.068).
We found similar results for our models specifying anxiety scores as the outcome. Sensitivity analysis for our anxiety scores model estimated that there would need to be a correlation of ρ = 0.27 between the mediator model error term and the outcome model error term for the ACME to equal zero. Results from our sensitivity analysis of PTSD scores model reported a ρ = 0.40, and a correlation of ρ = 0.93 for the somatisation scores model.
Discussion
In this observational, case–control cohort study of adults with a history of confirmed SARS-CoV-2 infection in Johannesburg, South Africa, adult patients with a history of out-patient-managed acute symptomatic COVID-19 exhibited the worst psychiatric outcomes relative to patients with a history of acute asymptomatic COVID-19, acute symptomatic COVID-19 requiring hospital admission and vaccinated controls. Female gender, tobacco use, depression diagnosis and low perceived social support were major risk factors for poor mental health. Patients with a history of symptomatic COVID-19 reported the worst mental health symptoms across all measures of depression, anxiety, suicidal ideation, PTSD, bipolar disorder and somatisation. Current long COVID symptom severity was associated with all mental health outcomes. Furthermore, our results suggest that long COVID symptoms mediated the association between acute COVID-19 symptoms and specific mental health outcomes (depression, anxiety, PTSD and somatisation), although the indirect effects of long COVID symptoms were modest. These findings contradicted our original hypothesis that adults with a history of hospital admission for COVID-19 would have exhibited the worst mental health problems as a function of symptom severity, number of acute COVID-19 symptoms and current long COVID symptoms, and across all groups.
All participants with a history of COVID-19 exhibited significantly elevated mental health symptoms relative to vaccinated controls, and patterns of COVID-19-related mental health trends varied by group. Patients with a history of acute symptomatic COVID-19 reported the worst overall mental health trends compared with all COVID-19 severity groups and controls. Furthermore, the number of acute COVID-19 symptoms was also associated with greater psychiatric symptom burden in this sample. These findings corroborate the broader literature, which suggests that symptomatic adult patients exhibit elevated and prolonged psychiatric morbidity when compared with asymptomatic patients and controls. Reference Taquet, Sillett, Zhu, Mendel, Camplisson and Dercon19 Considering the country’s elevated risk of psychiatric morbidity in South Africa, high SARS-CoV-2 seroprevalence rate and severe lack of public mental health resources, these data highlight a possible long-term risk factor for poor mental health in South Africa.
Prevalence rates of psychiatric caseness for most psychiatric disorders in this sample were lower than those reported in other studies, with the exception of PTSD and somatisation, which were 21.1% and 23.1% in this sample, respectively. For instance, studies based in Egypt (22%), Peru (31%) and Spain (19%) reported elevated levels of depression, and samples in India (24.8%), Poland (33.3%) and the USA (40%) have reported heightened rates of anxiety, Reference Seighali, Abdollahi, Shafiee, Amini, Teymouri Athar and Safari7,Reference Villarreal-Zegarra, Paredes-Angeles, Mayo-Puchoc, Vilela-Estada, Copez-Lonzoy and Huarcaya-Victoria37 although assessments of COVID-19 severity and mental health symptoms and the timing of these measurements vary considerably. The prevalence rate of PTSD symptoms was elevated in this sample and when compared with other studies. Previous studies based in India (15.5%), Italy (13%) and China (17.2%) reported lower rates of PTSD symptoms, whereas a small handful of studies reported elevated levels (Vietnam: 50%, Colombia: 35%). Reference Seighali, Abdollahi, Shafiee, Amini, Teymouri Athar and Safari7,Reference Vo, Dao, Van Duong, Nguyen, Do and Do38 Studies of symptoms of somatisation in patients with long COVID are limited, and recent findings have reported low rates of somatic symptoms (Peru: 2.2%, The Netherlands: 12.7%). Reference Seighali, Abdollahi, Shafiee, Amini, Teymouri Athar and Safari7 No studies on bipolar symptoms among patients with long COVID were found.
The result that patients with a history of acute symptomatic COVID-19 exhibited the highest levels of psychiatric morbidity out of all groups contrasts with the study hypothesis and broader findings that suggest that adult patients who were admitted to hospital for COVID-19 display the worst and most persistent psychiatric sequelae after SARS-CoV-2 infection. Reference Zeng, Zhao, Yan, Li, Lu and Liu8,Reference Hastie, Lowe, McAuley, Winter, Mills and Black13 Patients with a history of hospital admission in this study may have exhibited lower levels of psychiatric morbidity relative to the symptomatic COVID-19 group because of selection bias, as a greater proportion of adults who were admitted to hospital for severe COVID-19 may have died before study enrolment. Furthermore, adults with a history of hospital admission and severe long COVID symptoms may have also excluded themselves from study participation because of disease morbidity. The group with a history of hospital admission reported the greatest number of pre-existing diagnoses (e.g. HIV, hypertension, insomnia, tuberculosis) and was substantially older compared with the other study groups. Patients may have received additional clinical care and rehabilitation post-hospital admission, which recent studies have shown to be effective in improving physical and mental health compared with those receiving usual care. Reference Asimakos, Spetsioti, Mavronasou, Gounopoulos, Siousioura and Dima39,Reference McGregor, Sandhu, Bruce, Sheehan, McWilliams and Yeung40 Additionally, unmeasured socioeconomic and psychosocial factors specific to the symptomatic COVID-19 group, such as the stress of being a front-line worker or the financial strain of receiving out-patient care, may have contributed to their overall symptom burden.
We also found that current long COVID symptoms mediated the association between acute COVID-19 symptoms and certain adult psychiatric outcomes (depression, anxiety, PTSD, somatisation), although these results must be interpreted carefully. The indirect effects of long COVID symptoms were small, and neither the total nor the direct effects were statistically significant across all models. These results demonstrate that the associations between acute COVID-19 symptoms and mental health outcomes appear to operate through the mediating effects of long COVID symptoms, but the mediating effects were modest. Bias in our measures of acute COVID-19 infection and current long COVID symptoms may have affected the mediation analyses. Symptoms of acute COVID-19 infection were retrospectively reported in our study. Our assessment of long COVID severity may also have failed to capture other relevant symptoms, given the heterogeneity of the condition and the limited availability of validated measures at the time of data collection. Additionally, given the conceptual and measurement overlap between long COVID symptoms and somatisation, the mediation results may partially reflect shared symptom burden rather than a distinct causal pathway. Nevertheless, although past research has not examined the potential mediating role of long COVID severity on the mental health effects of COVID-19 infection, growing research has highlighted the psychiatric consequences of both acute SARS-CoV-2 infection and long COVID morbidity. Reference OMahoney, Routen, Gillies, Ekezie, Welford and Zhang2,Reference Seighali, Abdollahi, Shafiee, Amini, Teymouri Athar and Safari7–Reference Sudre, Murray, Varsavsky, Graham, Penfold and Bowyer11
Finally, these results contribute to a narrow literature on long COVID in Africa, particularly Sub-Saharan Africa, and suggest that the long-term psychiatric sequelae of SARS-CoV-2 infection may be prevalent in South Africa. Past studies suggest that elevated prevalence of disease comorbidities, limited public mental healthcare access, high mental health stigma and low vaccine coverage across many Sub-Saharan African settings pose major risks for COVID-19-related morbidity, including the psychiatric symptoms of long COVID. Reference Lewis, Ware, Whelan, Subissi, Li and Ma21 Furthermore, historical structural inequities in the continent further exacerbate socioeconomic conditions and public healthcare infrastructures, posing additional barriers to detection and treatment of chronic conditions. Findings from this study call for greater, long-term psychological screening among patients with SARS-CoV-2 infection, improving public healthcare services to adequately address increases in long COVID diagnoses and future research that traces longitudinal patterns of mental health in African communities.
This study was not without limitations. COVID-19 symptom data were collected retrospectively, introducing potential recall bias in the reporting of symptom profiles and infection history. The cross-sectional nature of this study prevented the ability to determine whether elevated psychiatric symptoms were attributed to pre-infection mental health rather than COVID-19 severity. Furthermore, we were unable to precisely determine the true number of SARS-CoV-2 infections after the initial infection, and all vaccination information was self-reported. Although the duration of time elapsed between initial SARS-CoV-2 infection and assessment of mental health symptoms was adjusted for in the models, the amount of time since the initial SARS-CoV-2 infection was not consistent across participants. Characteristics of hospital admission, such as ventilation use and intensive care unit admission, as well as biological markers of infection (e.g. viral load, inflammation, etc.), were not available in all participants. The demographic characteristics varied across the COVID-19 severity groups, limiting the comparability across groups. Our binary measure of employment status did not include an option for retired individuals, limiting our overall assessment of socioeconomic status. Although the mental health outcome variables exhibited some skewness and were better fit by a negative binomial model, we used linear regression in our mediation models to allow for interpretability and ensure compatibility with the causal mediation framework. As a result, estimates may be sensitive to model specification. The lack of accessible public mental healthcare and high mental health stigma in this context may have resulted in an underdiagnosis and underreporting of pre-existing psychiatric conditions, leading to a possible underestimation of psychiatric history. Finally, our control group mostly consisted of healthcare workers, who are more likely to be health conscious, have greater socioeconomic status and hold different risk perceptions compared with the general population. Although our comparison of demographic and clinical characteristics showed that the control group faced a range of risk and protective factors, the relatively privileged status of controls may have resulted in an underestimation of the effects across the experimental groups.
In conclusion, our observational case–control study of adults with confirmed SARS-CoV-2 infection in Johannesburg, South Africa, found that COVID-19 severity and number of acute symptoms were associated with worse psychiatric symptoms. Prevalence rates of PTSD and somatic symptoms were elevated in this sample. Adults with acute symptomatic COVID-19 exhibited the greatest psychiatric morbidity relative to vaccinated controls. Long COVID symptom severity was directly associated with worse psychiatric sequelae across all measures, and modestly mediated the association between acute COVID-19 infection and certain mental health outcomes (depression, anxiety, PTSD, somatisation). These results call attention to the long-term psychiatric sequelae of SARS-CoV-2 infection, and likely emergence of long COVID as a large public health concern in African countries widely affected by the COVID-19 pandemic.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12049
Data availability
Data are available upon reasonable request to the corresponding author.
Acknowledgement
We thank Sunsaara Shergill for her support on this study.
Author contributions
A.W.K. conceptualised the manuscript, oversaw data collection, and drafted and edited the manuscript. S. Swana conducted data collection and edited the manuscript. S. Sokhela managed data collection and obtained funding. S.L.-E. managed data collection, obtained funding and edited the manuscript. N.M. managed data collection. A.C.T. assisted in data analysis and edited the manuscript. W.D.F.V. conceptualised the project, managed data collection and obtained funding.
Funding
Funding from the Grants, Innovation and Product Development Award from the South African Medical Research Council supported this research. A.C.T. was supported by an award from the National Institutes of Health (number K24DA061696-01).
Declaration of interest
A.C.T. reports receiving a financial honorarium from Elsevier (for his work as Co-Editor in Chief of SSM – Mental Health) and from BMJ Publishing Group (for his work as Clinical Editorial Advisor for The BMJ).



 Open access
Open access
eLetters
No eLetters have been published for this article.