

Introduction
Naturally occurring retirement communities (NORCs) are geographic areas that have come to house a high proportion (≥30%) of older residents (Hunt & Gunter-Hunt, Reference Hunt and Gunter-Hunt1986). NORCs form as residents age in their building, neighbourhood, or as older adults relocate. Relocation can occur due to changes in finances, loss of their spouse, a desire to enhance their social network or be closer to family, and/or health changes that can make it hard to upkeep a house and necessitate proximity to services (Kloseck et al., Reference Kloseck, Crilly and Gutman2010; Li et al., Reference Li, Hu and Guo2022). NORC-based programs have the potential to facilitate ‘aging in place’, by bringing in health and social support resources from the surrounding community onsite to meet their unique needs (e.g., health services/assessments, fitness and nutrition programs; Parniak et al., Reference Parniak, DePaul, Frymire, DePaul and Donnelly2022). Pioneered in New York City, NORC supportive service programs (NORC-SSPs) have been found to delay long-term care home admission, decrease the likelihood of emergency department visits, improve social well-being, and prevent loneliness (Chum et al., Reference Chum, Fitzhenry, Robinson, Murphy, Phan, Alvarez, Hand, Laliberte Rudman and McGrath2022; Greenfield & Mauldin, Reference Greenfield and Mauldin2017; Kyriacou & Vladeck, Reference Kyriacou and Vladeck2011).
Canada has yet to fully realize the potential of NORCs to support its growing aging population (Women’s Age Lab, 2024). Advocates have called for investment into NORCs in Canada and research demonstrates a clear need for NORC-based programs. In Ontario, almost 1 in 10 older adults (~217,000) live in a NORC high-rise building and population-based data show that NORC residents have greater health needs (e.g., more emergency department visits, more chronic conditions) than older adults living in all other housing types in the community (Savage et al., Reference Savage, Huynh, Hahn-Goldberg, Matai, Boblitz, Altaf, Bronskill, Brown, Feng, Lewis-Fung, Sheth, Yu, Recknagel and Rochon2025). NORCs have been leveraged as a location to reach large numbers of older adults by implementing mobile on-site COVID-19 vaccination clinics in NORCs across the city of Toronto (Huynh et al., Reference Huynh, Sava, Hahn-Goldberg, Recknagel, Bogoch, Brown, Dubey, Isaacksz, Jün, Kouyoumdjian, Maltsev, Manuel, Martin, Matlow, McGreer, Mills, Niedra, Powis, Rochon and Brown2021). With that, it is vital to centre equity, to ensure such programming is reaching those in high-need communities (e.g., immigrants, low income, high health needs). Other equity-deserving locations to target can include seniors-designated social housing, whose residents experience economic, health, and social inequalities and face challenges such as housing conditions and barriers to accessing services (Sheppard et al., Reference Sheppard, Kwon, Yau, Rios, Austen and Hitzig2023).
As interest grows in spreading these programs across Canada, there is a need for a replicable and equitable process to identify potential sites that could benefit from such enhanced programming. A recent scoping review of NORCs found only six articles describing the process of identifying NORCs for enhanced programming (Aurand et al., Reference Aurand, Miles and Usher2014; Elbert & Neufeld, Reference Elbert and Neufeld2010; Hunt et al., Reference Hunt, Marshall and Merrill2002; Marshall & Hunt, Reference Marshall and Hunt1999; Morrison et al., Reference Morrison, Basnet, Budhathoki, Adhikari, Tumbahangphe, Manandhar, Costello and Groce2014; Parniak et al., Reference Parniak, DePaul, Frymire, DePaul and Donnelly2022; Rivera-Hernandez et al., Reference Rivera-Hernandez, Yamashita and Kinney2015). These methods involved leveraging relationships and partnerships with key informants and community organizations to identify NORCs in their local area (Parniak et al., Reference Parniak, DePaul, Frymire, DePaul and Donnelly2022). Furthermore, only two studies have used data-driven methods to identify NORCs (DePaul et al., Reference DePaul, Parniak, Nguyen, Hand, Letts, McGrath, Richardson, Rudman, Bayoumi, Cooper, Tranmer and Donnelly2022; Rivera-Hernandez et al., Reference Rivera-Hernandez, Yamashita and Kinney2015), pointing to the need for further research in this area. Both studies used census data to identify geographical areas with a high percentage of older adults, and DePaul et al. (Reference DePaul, Parniak, Nguyen, Hand, Letts, McGrath, Richardson, Rudman, Bayoumi, Cooper, Tranmer and Donnelly2022) additionally examined sociodemographic attributes of neighbourhoods (i.e., marginalization), as well as proximity and access to amenities, to further identify candidate sites. To date, no studies have integrated data on health and health care use into the selection process to identify potential NORC sites for intervention. While the leveraging of community partnerships in previous work is an important method, a data-driven approach can help ensure that sites who may not be well connected or networked within their communities have an opportunity to receive programming. Additionally, it allows for decision making to be based on evidence-backed measurable indicators, which is helpful in reducing bias. The objective of this study was to describe a systematic and iterative process taken to centre equity in the site selection process for a Canadian supportive service program delivered in NORCs and seniors-designated social housing.
Methods
Our method builds on the approach published by DePaul and colleagues (Reference DePaul, Parniak, Nguyen, Hand, Letts, McGrath, Richardson, Rudman, Bayoumi, Cooper, Tranmer and Donnelly2022) to select sites for the established and growing Oasis Senior Supportive Living, Inc. (Oasis) NORC-SSP in Canada. We expanded on their work to incorporate equity-driven perspectives for a demographically diverse population in Canada’s largest city – Toronto, as part of a larger implementation science research program aiming to understand the contextual determinants of NORC-SSP implementation to support the successful spread and scale to diverse settings.
UHN NORC program
The University Health Network’s NORC Innovation Centre’s (UHN NIC) NORC program (https://norcinnovationcentre.ca) aims to support residents to live independently and safely in their communities for as long as they choose. The UHN NORC program consists of recruiting a group of residents from NORC and seniors-designated social housing buildings, known as Ambassadors, to collaborate with program implementers (e.g., trained professional facilitators with backgrounds in community health) to co-facilitate programming specific to fulfilling the needs of their building. Programming examples include wellness activities (e.g., organizing community meals), social activities (e.g., book clubs or movie nights), and recreation activities (e.g., walking groups) and health activities (e.g., falls prevention program). The Ambassadors are given a microgrant to use to help organize resident-led programming in their building.
The UHN NORC program progresses through multiple stages. Initially, Ambassadors undergo facilitated training to build capacity in community development through a relational care approach. Sites with higher levels of need receive additional support, including an onsite NORC Connector – a staff member who assists residents in accessing health and social care resources and streamlining navigation. Some buildings may also receive support from an Integrated Care Lead (ICL), who assesses more complex needs, connects to primary care, facilitates timely referrals, and works to reduce avoidable emergency department visits in a model similar to those seen in traditional NORC-SSPs which bring services to residents through an on-site nurse or social worker (Vladeck & Altman, Reference Vladeck and Altman2015). Other sites are encouraged to continue as self-managed groups with the support of a NORC Connector who is on-call and continues to support them onsite and virtually through coaching and making connection to local social and health partners. The program emphasizes empowerment of older adults through their involvement in co-facilitating the program (Meschino et al., Reference Meschino, Recknagel, Bartleman, Dai and Hahn-Goldberg2024). By creating opportunities for meaningful social connection and inclusive communities, the program uses a preventive approach to produce positive health outcomes such as increased access to informal supports, life satisfaction, social connection, and increased access to timely care (Meschino et al., Reference Meschino, Recknagel, Bartleman, Dai and Hahn-Goldberg2024). This article describes the site selection process for the initial stage of this program.
Equity- and data-driven site selection process
Overview
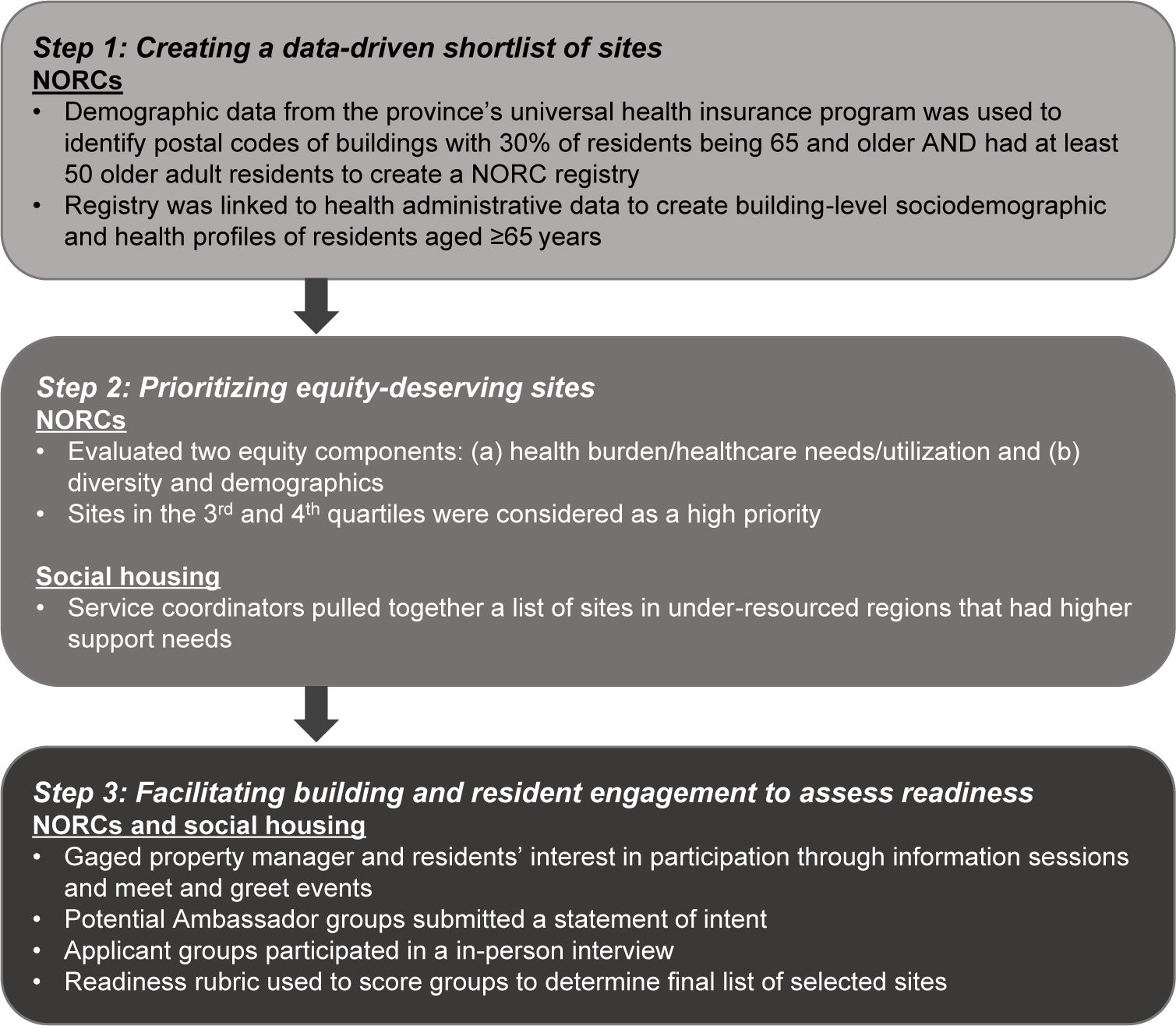
To select sites for the UHN NORC program, we (1) created a data-driven shortlist of NORC high-rise buildings in Toronto using census and health administrative data, (2) prioritized equity by targeting buildings with high health needs and diversity, and (3) facilitated building and resident engagement to assess interest, fit, and readiness for this program. University Health Network’s (UHN) Quality Improvement Review Committee (QI ID #23-0549) and Women’s College Hospital Assessment Process for Quality Improvement Projects (APQIP #2023-0026) reviewed and approved the proposed work. Sites included high-rise NORCs such as for-profit condominiums and apartments, co-operative housing sites, as well as seniors-designated social housing which provides subsidized housing for low- and moderate-income older adults. Although the latter are technically not NORCs, they were candidate sites for the UHN NORC program as they are places with a high density of equity-deserving older adults with high health needs, and high cultural diversity with lower English proficiency that can benefit from onsite programming tailored to their uniquely expressed needs. The three steps are summarized in Figure 1 and described next.
Summary of site selection steps.

Figure 1. Long description
At the top, Step 1 details creating a data-driven shortlist of sites for N O R Cs using provincial health insurance demographic data to identify buildings with at least 30 percent of residents aged 65 and older and at least 50 older adults, forming a registry linked to administrative data for building-level sociodemographic and health profiles of residents aged 65 years or older. A downward arrow leads to Step 2, prioritizing equity-deserving sites. For N O R Cs, two equity components were evaluated: health burden or healthcare needs or utilization and diversity and demographics, with sites in the third and fourth quartiles prioritized. For social housing, service coordinators compiled a list of sites in under-resourced regions with higher support needs. Another downward arrow leads to Step 3, facilitating building and resident engagement to assess readiness for both N O R Cs and social housing. This included gauging property manager and resident interest through information sessions and events, submission of intent statements by potential Ambassador groups, in-person interviews with applicant groups, and scoring with a readiness rubric to determine the final selected sites.
Step 1: Creating a data-driven shortlist of buildings
The site selection process started with Ontario’s first-ever NORC registry, created by University Health Network’s OpenLab, which identified all high-rise NORC buildings in the province (Huynh et al., Reference Huynh, Sava, Hahn-Goldberg, Recknagel, Bogoch, Brown, Dubey, Isaacksz, Jün, Kouyoumdjian, Maltsev, Manuel, Martin, Matlow, McGreer, Mills, Niedra, Powis, Rochon and Brown2021; Savage et al., Reference Savage, Huynh, Hahn-Goldberg, Matai, Boblitz, Altaf, Bronskill, Brown, Feng, Lewis-Fung, Sheth, Yu, Recknagel and Rochon2025). In early 2021, demographic data collected on registrants to the province’s universal health insurance program (RPDB) for the fiscal year 2019/2020 (the most recent data available at the time) was used to identify postal codes where 30% or more of residents were 65 years and older, and that had at least 50 older people living at that postal code. High-density buildings were then identified via postal codes using geospatial data sets for residential buildings, or Google searches (Sheth et al., Reference Sheth, Rochon, Altaf, Boblitz, Bronskill, Brown, Hahn-Goldberg, Huynh, Lewis-Fung, Feng and Savage2024). Postal codes corresponding with specific high-rise buildings were identified by cross referencing with Canada Post’s postal code-to-address database. Postal codes corresponding with multiple addresses were excluded as they represented a city block, neighbourhood, or broad area. Next, postal codes corresponding with those in databases for retirement homes and long-term care facilities were excluded because they were not considered to be ‘naturally occurring’. Google Maps was then used to verify that the final list of NORCs were in fact high-rise buildings. This registry was then linked, via six-digit postal code, with individual-level health administrative data at ICES to create building-level sociodemographic and health profiles of residents aged ≥65 years as of January 1, 2020. ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. These data sets were linked using unique encoded identifiers and analyzed at ICES. The use of this data is authorized under section 45 of Ontario’s Personal Health Information Protection Act (PHIPA) and does not require review by a Research Ethics Board. Site profiles were generated for NORCs in Toronto that had less than 80% of older adults as residents (to exclude long-term care homes, retirement homes, and seniors-exclusive buildings) and did not have listed supports already available (consultations with the provincial health authority were also held to determine this). These parameters were chosen with consideration to ensure a large enough population of older adults live in the building to benefit from the model and provide economies of scale, as well as to not over-saturate programming already existing in buildings with a high population of older adults.
Step 2: Prioritizing equity-deserving sites
Next, two major equity components were taken into consideration: (a) high health burden/health care utilization needs and (b) demographics and diversity. A number of health-related variables were measured using health administrative data that allowed for the assessment of the site’s needs levels. These variables were measured using either a 1- or 2-year lookback period from an index date of January 1, 2020. Variables assessed included health status (measured as the percentage of older residents with multimorbidity [at least two active chronic conditions]), health care utilization (measured as emergency department visits and long-stay home care use), and health care system access (measured as non-attachment to a primary care provider [PCP]). Health burden and health care utilization was used as an equity measure as it can illuminate equity-related issues such as dis/ability and financial status (e.g., costs associated with health issues). Research shows that primary care attachment is lower in areas with high residential instability and material deprivation, and in recent immigrants (Bayoumi et al., Reference Bayoumi, Glazier, Jaakkimainen, Premji, Kiran, Frymire, Khan and Green2023), and that lower socioeconomic status is associated with increased use of the emergency department (Khan et al., Reference Khan, Glazier, Moineddin and Schull2011), a higher multimorbidity risk (Álvarez-Gálvez et al., Reference Álvarez-Gálvez, Ortega-Martín, Carretero-Bravo, Pérez-Muñoz, Suárez-Lledó and Ramos-Fiol2023), and a higher propensity and intensity of home care use (Laporte et al., Reference Laporte, Croxford and Coyte2007). For demographics, factors that were taken into consideration included neighbourhood and building diversity in terms of the distribution of age, sex, immigrant status (permanent residents landing in Ontario between 1985 and 2020 were classified using the Immigration, Refugees and Citizenship Canada [IRCC] Permanent Resident database), and neighbourhood-level marginalization (using the Ontario Marginalization Index [ON-MARG] van Ingen & Matheson, Reference van Ingen and Matheson2002). For variable definitions, see Supplementary Table S1. These variables were chosen with consideration to replicability with other health administrative data sets for different contexts. Quartiles were calculated for each variable (very low, low, high, very high) to determine sites with high health and health care burden/utilization/needs, high ethnic diversity (measured using the ‘racialized and newcomer population’ dimension in ON-MARG), and were low income (high was measured as above average compared to other Toronto NORCs). Sites with higher levels of health burden and that were in lower income and high ethnic diversity neighbourhoods were designated as high need and prioritized for the shortlist. Having diversity in building types was also considered (e.g., condominium, apartments, co-operative housing). This was emphasized in this planning stage with consideration to making this program replicable and relevant across a variety of settings. An online review of common rooms within the building and inquiry of health services in the local area (in collaboration with the provincial health authority) was conducted to consider environmental and spatial suitability. The common room was required to ensure there was space for programming at the selected site.
Social housing sites under Toronto Senior’s Housing Corporation (TSHC) provide rent geared to income to support the needs of low- to moderate-income older adults. In conjunction with a data-driven approach to select a shortlist of social housing sites, UHN’s NIC consulted with Toronto’s largest older adult-designated social housing provider directly, who manually selected sites for their shortlist. They decided to focus on the regions and sites that were previously identified as needing greater levels of support in part because they had comparatively fewer services available in their neighbourhoods. Another consideration for selection involved on-site service coordinators who had identified a pre-existing level of autonomy and interest within tenants.
Step 3: Facilitating building and resident engagement to assess readiness
From January to March 2023, readiness criteria (non-physical, micro-level factors that impacted the decision to select a site) were assessed for the short-listed buildings. This step required communication with property managers and where indicated, the board of directors. Phone calls to property managers gave an overview of the program, requirements, and the potential benefits it could bring to its residents and building partners, as well as next steps for participation. These calls also assessed the level of engagement from the property managers and boards (e.g., their enthusiasm about the program) and confirmed any other necessary components for program implementation (e.g., approval by a board, ability to access the common room). This was important as the engagement of property managers and boards were important for the execution and sustainability of the program. In-person site visits were also conducted by the team to assess the physical space (e.g., conditions of the built structure).
After the distribution of promotional materials, online and in-person information sessions and meet and greets at each shortlisted site were held to engage with the residents to learn more about each site. These meet and greets were designed as drop-in, informal chats with residents. Residents were encouraged to form a potential Ambassador group (made up of 3–5 members) to facilitate the program if their site was selected and were asked to submit a statement of intent as a group. This document contained several questions for the group to fill out, covering Ambassador group information (e.g., how long they have lived in the building), site information (e.g., availability of common spaces, information sharing between residents, on-site staff, prominent cultural groups), the older adult population (e.g., any current resident run activities, social connectivity between residents), and motivations to joining this program. Potential Ambassador groups were then interviewed by program staff in person to assess readiness and strength of engagement. Interview questions assessed the skills and capacity of potential Ambassadors, resident culture in their site, alignment in program goals and values, and potential challenges (e.g., What does aging in place mean to you? What do you hope to accomplish with this project? How would you describe the quality of life for older adults in your building?). Based on the statement of intent and interview, each site was then scored on a 3-point scale (low, medium, high) in categories relating to the group’s ability to participate in this program using a readiness rubric created by the program’s team. These scores were discussed with the larger team, prior to final decisions being made. This decision was based on suitability for inclusion as well as the level of support needed for the site.
For social housing sites, a very similar process was followed. Rather than connecting with property managers, communication was made with their housing leadership. Existing building coordinators were responsible for distributing flyers and other promotional materials in the building to generate resident interest. The materials were printed and mailed directly to coordinators. Promotional material was distributed in the form of individual door drops of flyers to tenant units, as communication (particularly mode of communication) is critical in engagement with this population of older adults. The process to assess building readiness mirrored the steps taken to select the other NORC sites. Figure 1 provides a visual summary of this process.
Results
Creating a data-driven shortlist of buildings
Steps 1 and 2 took about 24 months to complete. The Ontario NORC registry was created in early 2021, taking about 2 months to complete. In April 2022, it was linked with health administrative data. Building-level profiles were then completed in August 2022. There were data integration, analysis, and oversight and management costs at ICES. The Ontario NORC registry identified 1941 sites (apartments, condos, co-ops, social housing) that were home to 217,000 older adults; 489 sites were located in Toronto. After excluding buildings with more than 80% of older adults as residents (excluded due to many having existing supports present), a total of 350 sites were identified to select from.
Prioritizing equity-deserving sites
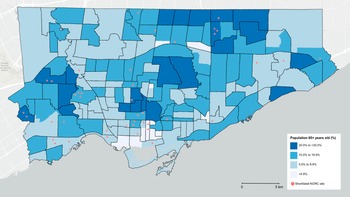
Shortlists were finalized at the end of 2022. With consideration for geographic diversity, the top two buildings in each geographic region of Toronto in terms of highest health needs, burden and health utilization were kept. We further added sites to the shortlist that had a lower percentage of older adults and/or a lower average age that also met our threshold for high health and social needs. Having a younger older adult demographic (i.e., approximately 65–75 years old) had been previously found to be a facilitator for programming in earlier iterations of the program. Sites that did not have common spaces to hold community programming or had existing health services were excluded, leaving a final shortlist of 28 sites. Figure 2 depicts where these shortlisted buildings were located, as well as the percentage of older adults in the surrounding neighbourhood. For the social housing sites, 13 sites (out of 83) were selected by staff that were determined to be of higher need and lower resourced, which were passed through to the next phase.
Map of the density of older adults (age 65+) by neighbourhood in Toronto (Statistics Canada, 2023; University of Toronto, 2023) overlayed with the locations of shortlisted sites.

Figure 2. Long description
Starting at the northwest, neighborhoods are shaded by percentage of adults age 65 and older: darkest blue for 20.0 to 30.0 percent, medium blue for 10.0 to 19.9 percent, light blue for 5.0 to 9.9 percent, and white for less than 4.9 percent. Higher densities cluster in the northwest, west, and northeast, with several medium-density zones in the central and eastern areas. Red dots, representing shortlisted N O R C sites, are scattered across the map, with concentrations in the west-central and central-south neighborhoods. The legend at the bottom right explains the color scale and red dot symbol. A scale bar at the bottom indicates distances up to 5 kilometers.
Assessing readiness
This stage took about 8 months to complete, from January 2023 to August 2023. Property managers or board of directors were the first point of contact. Overall, 57% (16/28) of management responded and expressed their support for the program. Most management contacted were supportive and curious about the program. Next, property managers or interested residents had to go to their board for approval and support as a partner of the program’s implementation. Communication materials were distributed to advertise meet and greet information sessions to residents in collaboration with property managers and boards. If sites had existing social committees, the team worked with the committee chair or lead after the property managers and board granted permission to procced with promotions.
Twelve meet and greets were held in total. Between 7 and 25 residents attended each of these sessions (number of older adult site residents: range = 73–357, mean = 188). Conversations were the first step to establish trust and rapport with residents and provided the history and context of the site (e.g., past programming, current needs). It was observed that attendance was higher at sites where there were positive relationships between residents and the property manager or where there was a pre-existing social committee. Social housing sites had higher turnout rates at information sessions with very enthusiastic and engaged residents. Social housing coordinators were observed to be eager to bring in this program for their residents and contributed a lot of work to advertise the meet and greet events. During these information sessions, team members also took note of whether or not there was a space (e.g., a common room) that could hold 25+ people, which factored into the final scoring for selection.
Statements of interest from 10 groups (out of a potential 12) were submitted. One group from a co-op site chose to not submit as they could not form an Ambassador group due to time commitment and capacity, despite the value they saw in the program and interest from their property manager and board. The other site was an apartment and while they had one resident who was enthusiastic, they were not able to establish a group due to lack of interest.
Following this, the 10 potential groups were each interviewed in-person. Intangible characteristics that stood out (but were not a requirement) for selected sites were residents who demonstrated the ability to self-organize, were confident in their abilities, had volunteers ready to help, were motivated to integrate more diversity and inclusion, valued neighbour and community connections, and/or had pre-existing leadership groups such as a social committee. However, some of these characteristics can be developed over time and sites were not required to have every single one to be selected.
The ability of the team to build trust and connect well with residents was also important for the selection process. It was observed that residents overall appreciated these in-person interviews for the NIC team to learn more about their communities and listen to their desires for improving them; they also appreciated the team’s support in the application process. However, there was dissatisfaction at times when residents felt confused regarding the program’s objectives and services for their community. Some residents also felt frustration in self-organizing (e.g., trying to gather interested peers, encountering language or technology barriers).
Final selection
Selected sites scored highly on criteria such as their ability to self-organize, commitment, and building culture. There were broader issues with some of the social housing sites regarding safety and/or physical infrastructure. Collaboration with property managers to address these issues was essential to having the building selected. Despite demonstrating high levels of need, there were too many risks to program participation in some buildings (e.g., safety concerns, lack of trust in property manager, lower ability to self-organize, incompatible building infrastructure), which led to them not being selected.
Ultimately, five sites (encompassing eight buildings) were selected, based on the capacity of the team to facilitate this program. Table 1 provides a summary of these selected sites’ characteristics. In alignment with our prioritization of equity and high-need communities, all sites had medium-to-high health needs and were in low-income neighbourhoods. Two sites were situated in highly ethnically diverse neighbourhoods (high racialized and newcomer populations). Additionally, we intentionally opted to select a diverse set of building types which included two condominiums, two social housing sites, and one co-operative housing site to allow for comparisons to be made in the evaluation process. The program finally launched in the fall of 2023.
Demographic characteristics of selected buildings

Table 1. Long description
The table has six rows and six columns. The header row lists: Characteristic, Site 1, Site 2, Site 3, Site 4, Site 5. For Region, Site 1 is West Toronto, Site 2 is Scarborough North, Site 3 is Downtown Toronto, Site 4 is West Toronto, Site 5 is East Toronto. For Building type, Sites 1 and 2 are Condominium, Site 3 is Co-operative housing, Sites 4 and 5 are Older adult-designated social housing. Proportion of residents 65 plus: Site 1 is 46 percent, Sites 2 and 3 are 41 percent, Site 4 is 83 percent, Site 5 is 93 percent. Neighbourhood income level: Sites 1 and 2 are Low income, Sites 3, 4, and 5 are Very low income. Neighbourhood diversity: Site 1 is Low diversity, Site 2 is Very high diversity, Site 3 is Very low diversity, Site 4 is Very high diversity, Site 5 is Low diversity. Health burden, utilization, and need: Site 1 is Medium, Site 2 is High, Site 3 is Medium, Site 4 is High, Site 5 is Medium.
Discussion
The changing population demographics in Canada suggest a need to focus on communities (i.e., buildings, neighbourhoods) with high proportions of older adults that would benefit from accessible resources to support aging in place. Programs like the UHN NORC program have the potential to fill this need. Considering the high diversity of Toronto and the older adult population in NORCs and social housing, equity was prioritized throughout this process with consideration for underserved populations (e.g., low-income, immigrant) and communities with greater health needs to target programs to where they could have greater benefit. This approach took an equity lens by prioritizing sites that demonstrated unmet and higher health needs (e.g., chronic conditions and service utilization) and diversity. The inclusion of social housing sites also emphasizes the equity focus of this process as many of these sites are under resourced and high need (Sheppard et al., Reference Sheppard, Kwon, Yau, Rios, Austen and Hitzig2023).
There is little published literature about the site selection process for NORC programming. The process we describe expands on the prior data-driven processes of Rivera-Hernandez et al. (Reference Rivera-Hernandez, Yamashita and Kinney2015) and DePaul et al. (Reference DePaul, Parniak, Nguyen, Hand, Letts, McGrath, Richardson, Rudman, Bayoumi, Cooper, Tranmer and Donnelly2022). Other adjacent community-based programs such as EMBOLDEN (Enhancing physical and community MoBility in OLDEr adults with health inequities using commuNity co-design intervention) in Hamilton, Ontario focused heavily on the surrounding environment to select intervention sites by using an environmental scan methodology that utilized census data, a review of existing services, organizational representative interviews, windshield surveys of selected high-priority neighbourhoods, and GIS mapping (Newbold et al., Reference Newbold, Valaitis, Phillips, Alvarez, Neil-Sztramko, Sihota, Tandon, Nadarajah, Wang, Moore, Orr and Ganann2023). What makes our process unique is the leveraging a novel province-wide Ontario NORC registry to identify potential sites and linking to health administrative data to reveal the health status and health needs of residents at a building level. This process allowed for the identification of equity-deserving older adult populations living in NORCs with key considerations for their health and health care needs, which was less of an emphasis in former site selection processes.
There is opportunity to use this methodology in other regional contexts. The creation of a NORC registry can be replicated in other urban regions with population-level data containing similar variables to the one used here. This could allow other regions to identify buildings housing large numbers of older adult residents and select interventions sites based on equity considerations and needs.
Strengths and limitations
There are a number of strengths and limitations related to this site selection process of the UHN NORC program. A novel strength is using data to identify diversity-level and health needs of NORC sites through the combination of census and health care records. Another strength was consideration for intangible characteristics including the ability of residents to self-organize and their confidence. While Ambassador groups did not necessarily have to hold mastery in these areas, the opportunity to cultivate and grow these skills throughout the program can contribute to the program’s success and sustainability. Finally, assessing both equity and readiness allowed us to identify NORCs that were diverse and high need, and understand how well the program would be suited for a site based on their residents and environment. Additional important considerations included the sites’ common space, adapting approaches for resident engagement, and characteristics of the residents to ensure the program’s sustainability.
There are several limitations to this process that should be acknowledged. This work focuses on vertical NORCs and social housing, excluding other sites such as horizontal NORCs. Future research that characterizes horizontal NORCs could help to determine where and how to best implement programming to support these residents. Another limitation is data availability. One variable that would be especially important to assess for equity is an indicator of the degree of social support (e.g., living alone, support from family members) of older residents, yet these data are not available in health administrative data. Additionally, as income and diversity data were collected on the neighbourhood level, it was not necessarily indicative of resident demographics at the site. With that, there is a possibility of this program not reaching certain communities due to neighbourhood-level data obscuring individual characteristics. To address this, future iterations may consider surveying residents to gage the individual-level characteristics of the specific site to understand if it is in alignment with the broader neighbourhood characteristics and better assess the level of need. Furthermore, while we aimed to select variables that are likely available across other data sets, there may still be a possibility that they are missing in some. We recommend selecting available variables that could be appropriately substituted. ICES has developed definitions to extrapolate ON-MARG variables from CENSUS data for other administrative data studies across Canada. For example, the ‘percentage below low income cut off (LICO)’ variable in CENSUS data corresponds to the ‘Material Resources’ variable in ON-MARG. Another limitation of this method is the need for engaged and willing property managers, who may have limited availability due to a variety of factors (e.g., time pressures, corporate priorities, burn out). While the responses from property managers were positive, there is a chance that there were high-need buildings that missed out on the opportunity to participate in the UHN NORC program due to the lack of response from their property manager. Finally, limitations related to equity emerged regarding common room space, language barriers, and computer literacy. Due to the need for a common room to hold events, sites without this in their infrastructure were not a good fit for this program. Additionally, some sites were noted to have barriers with language and computer use that impacted their ability to apply to and participate in this program. More support from program implementers would be needed for sites like these to overcome these barriers (e.g., making a greater effort to recruit bilingual Ambassadors or those with higher digital literacy).
Conclusion
As the number of NORCs and older adults residing in them grow, NORC SSPs programs can improve the health of older adult residents and help them age in place. We outlined three steps that take an equity- and data-driven approach to selecting NORC and social housing sites for program implementation. In describing this process, we outline a method for creating a registry of sites using population-level data, describe the use of equity to prioritize high-need sites, and identified key considerations including the assessment of the sites’ environment, adapting approaches for resident engagement, and resident characteristics. This method can be replicated and adapted to support the equitable selection of sites for future enhanced programing for NORCs or other sites with higher proportions of older adults across Canada.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0714980826100543.
Acknowledgements
We acknowledge and thank the current and past staff at Toronto Seniors Housing Corporation for their contributions to this process and their review of the manuscript including Joshua Graham, Jaipreet Kohli, and Arlene Howells. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from the Canadian Institutes of Health Research (HG1-185012) and the Public Health Agency of Canada. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI), and the Ontario Ministry of Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. This document is adapted from Statistics Canada, CENSUS, 2016. This does not constitute an endorsement by Statistics Canada of this product. Parts or whole of this material are based on data and/or information compiled and provided by Immigration, Refugees and Citizenship Canada (IRCC) current to September 2020. However, the analyses, conclusions, opinions, and statements expressed in the material are those of the author(s) and not necessarily those of IRCC. We thank IQVIA Solutions Canada, Inc. for use of their Drug Information File. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index.




 Open access
Open access