



Introduction
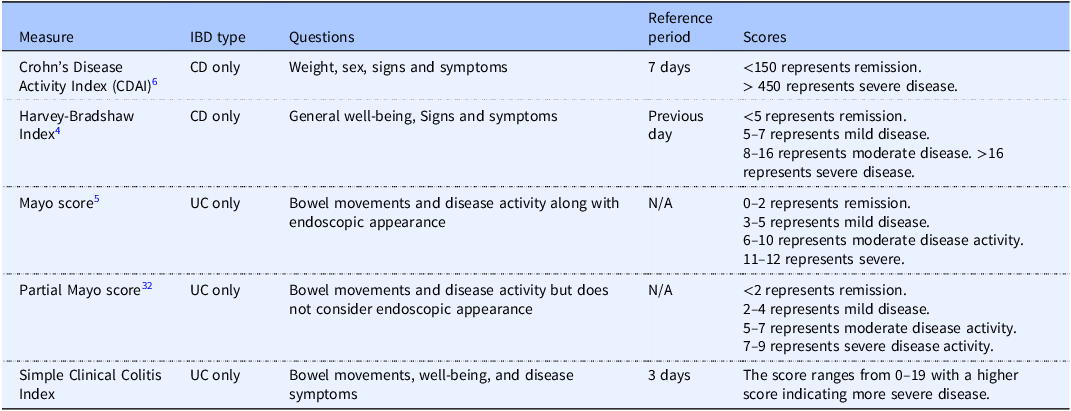
According to the Global Burden of Disease 2021, there were approximately 3.8 million cases of inflammatory bowel disease (IBD) worldwide.(Reference Ruan, Sun, Yu, Bai, Yang and Qian1) IBD, an autoimmune disease, causes chronic inflammation in the gastrointestinal (GI) tract.(2,3) IBD, including Crohn’s disease (CD) can occur as inflammatory patches anywhere between the mouth and anus, while ulcerative colitis (UC) is localized to the large intestine. Additionally, CD penetrates through many layers of the GI tract, whereas UC is localized to the surface of the intestinal wall. Tools such as the Mayo Score, for UC, and the Crohn’s Disease Activity Index (CDAI) and the Harvey-Bradshaw Index (HBI), for CD, are used to measure disease severity based on individual disease characteristics and symptoms (Table 1).(4–Reference Best, Becktel, Singleton and Kern6) IBD symptoms can include abdominal pain and cramping, frequent urgent bowel movements, blood or mucus in stool, and non-GI related symptoms such as joint pain and fatigue, all of which can impact quality of life (QOL).(7) Individuals with IBD can experience intermittent ranges of disease activity from remission with very mild or no symptoms to a flare, which occurs when symptoms and inflammation are severe. Changes in diet can potentially decrease symptoms and therefore increase QOL for these patients; however, the current dietary approaches may be difficult to manage or lead to stress and feelings of deprivation and therefore decrease QOL.(Reference Popa, Fadgyas Stanculete and Grad8) Many patients with IBD request diet information from providers.(Reference Holt, Strauss and Moore9) However, dietary advice varies for this population, likely reflecting a lack of evidence-based dietary guidelines for IBD.(Reference Limketkai, Godoy-Brewer and Parian10)
Measures of disease severity utilized in the included studies

CD, Crohn’s Disease.
UC, Ulcerative colitis.
Previous reviews have evaluated dietary interventions in adults with IBD, but the reporting of QOL within these reviews was not consistent. For example, four systematic reviews have explored the impact of dietary interventions on IBD.(Reference Limketkai, Godoy-Brewer and Parian10–Reference Gomes, Gomes and Braga13) In two of the reviews, by Limketkai et al.(Reference Limketkai, Godoy-Brewer and Parian10) and Nieva et al.(Reference Nieva, Pryor and Williams11) QOL was not the primary outcome of interest and was therefore missing from many included studies. Similarly, Abbas et al.(Reference Abbas, Shakil and Rana12) included studies with QOL as an outcome measure; however, they did not include both IBD types. Lastly, Gomes et al.(Reference Gomes, Gomes and Braga13) did not include QOL as an outcome measure. QOL can be negatively impacted by a variety of factors associated with IBD such as symptoms and treatments, thus it is important to consider for this population. As such, there is a further need to focus on QOL as the main outcome. Therefore, the purpose of this review is to explore clinical trials that focus on the impact of dietary interventions on disease specific, health-related QOL in adults with IBD.
Methods and materials
Study inclusion and exclusion criteria
Study inclusion criteria was based on study design, dietary pattern interventions, and outcomes. Randomized control trials and quasi-experimental studies with dietary pattern interventions that involved individuals with CD or UC, regardless of sex or ethnicity, were considered for review. Studies must have measured QOL using a health-related QOL questionnaire as an outcome. Time and language restrictions were not applied to these searches. Studies were excluded if the population consisted of children or adolescents under the age of 18 or had a nutrition support intervention, such as enteral or parenteral nutrition.
Literature search methods
This narrative review was developed using multiple databases to identify full-text, peer-reviewed articles. The EBSCOhost platform was utilized with eight chosen databases: Academic Search Premier, ALT Health Watch, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Health Source: Nursing/Academic Edition, CINAHL Ultimate, Cochrane Clinical Answers, and MEDLINE. Boolean search terms included ‘inflammatory bowel disease’ or ‘IBD’ or ‘ulcerative colitis’ or ‘Crohn’s disease’ AND ‘dietary interventions’ or ‘dietary advice’ or ‘dietary recommendations’. This search, completed in October 2024, resulted in 1054 total articles with 222 duplicates removed. The remaining 832 articles were screened for titles meeting inclusion criteria. Of these, 67 articles were eligible for retrieval. After reviewing abstracts, 24 articles met the eligibility for full text retrieval and screening. Seven of the 24 articles were eligible for this review based on the inclusion and exclusion criteria. Additionally, the PubMed database was searched using the original Boolean terms previously listed. PubMed was also set to filter for randomized controlled trials and clinical trials only, which resulted in 9 total studies; however, this did not add any new articles for this review. Lastly, hand searches of reference lists were completed and eight additional articles met inclusion criteria for a total of 15 articles, representing 15 studies to be included in this review. Titles and abstracts were screened and chosen by the first author (RM). Full text articles were then read and chosen for data extraction by the first author (RM). Information extracted included study design, participant demographics, IBD type, study duration, description of the intervention and control group diets, QOL measures, and changes in QOL. The second author (LK) then screened full text articles for the previously mentioned study criteria. Discussion between the authors (RM and LK) took place to resolve any disagreements in study eligibility or data extraction. Any conflicts were resolved after discussion with the third author (JD).
Results
Common dietary approaches used to reduce symptoms of IBD
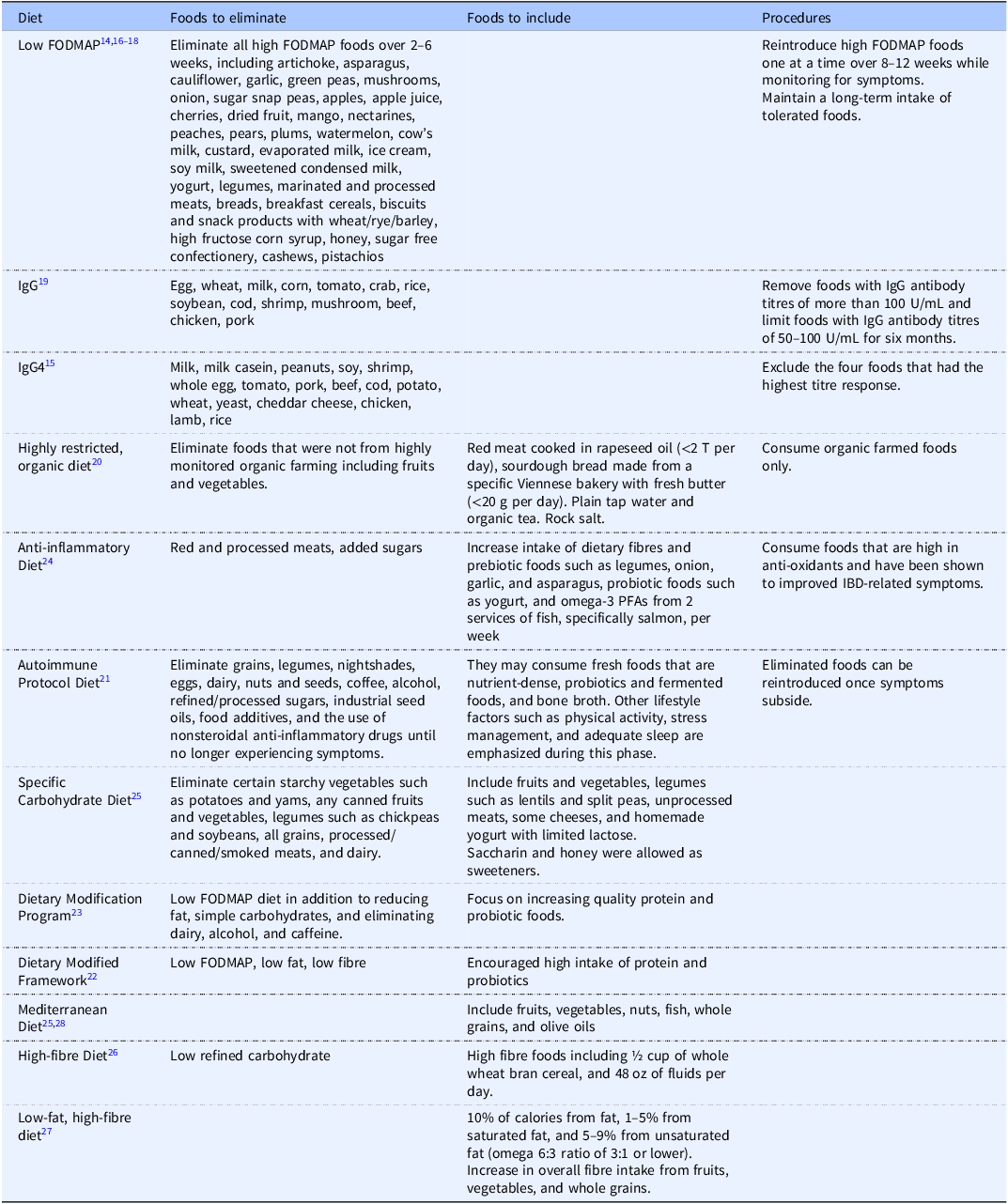
Selected studies include a variety of dietary approaches. The results will be grouped based on dietary intervention similarities (Table 2). For example, seven of the research teams used dietary approaches that focused on eliminating foods from the diet, such as the low FODMAP diet, a highly restricted organic diet, and the immunoglobulin-G (IgG) diet, which requires testing an individual’s serum for a response of IgG antibodies after exposure to certain food items.(Reference Bodini, Zanella and Crespi14–Reference Bartel, Weiss and Turetschek20) Other approaches, such as the Anti-Inflammatory Diet (AID), Autoimmune Protocol Diet (AIP), Dietary Modification Framework (DMF), and Dietary Modification Program (DMP) focused on eliminating specific foods associated with worsening symptoms while increasing intake of foods that may reduce GI inflammation, symptoms, and dysbiosis.(Reference Chandrasekaran, Groven and Lewis21–Reference Keshteli, Valcheva and Nickurak24) Although vegetarian or vegan dietary patterns were not identified specifically, the last group of dietary approaches used focused on specific foods or food groups that may reduce inflammation such as the Mediterranean diet (MD) and high fibre diets that focus on including foods or food groups that promote intake of anti-inflammatory foods, such as fruits and vegetables, and improved gut health.(Reference Lewis, Sandler and Brotherton25–Reference Chicco, Magrì and Cingolani28) Refer to Table 2 for descriptions of these diets.
Description of dietary approaches used across included studies
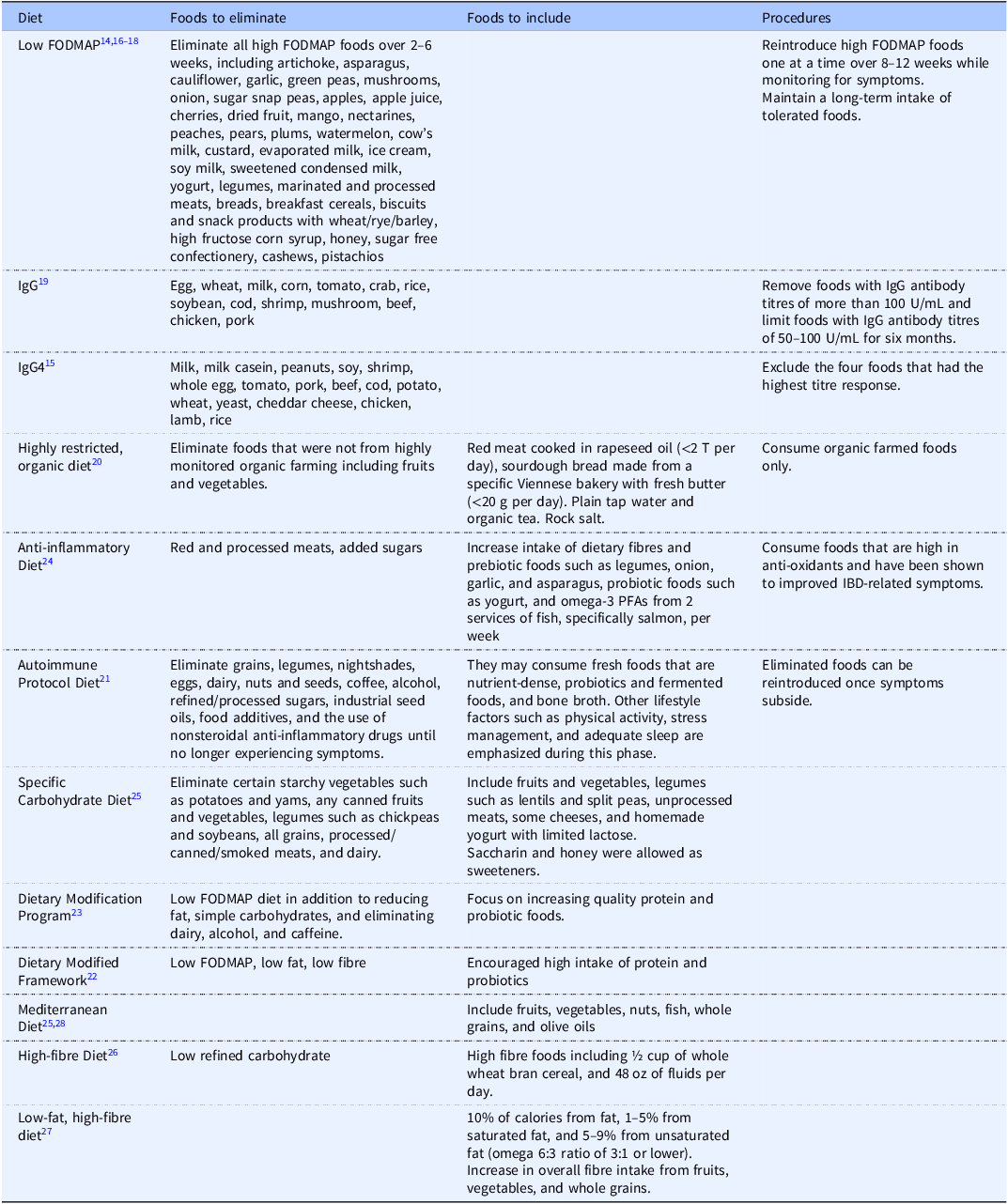
FODMAP, fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.
IgG, Immunoglobulin G.
Measures of quality of life use in studies
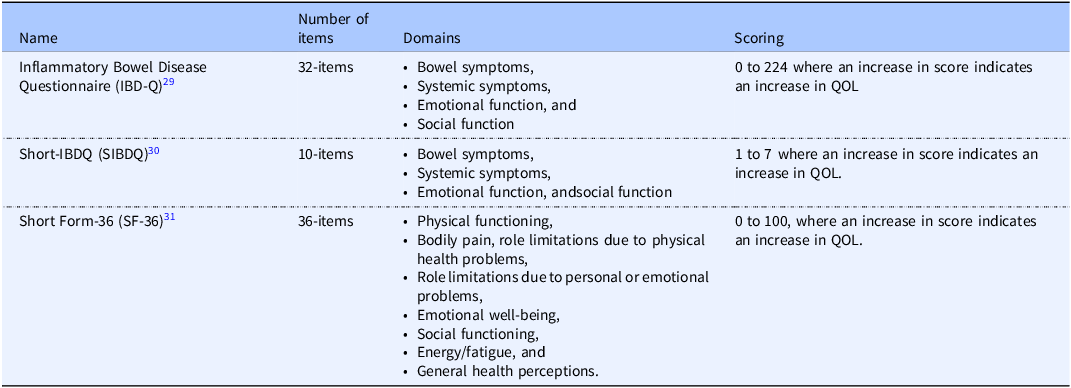
Each study met inclusion criteria by exploring QOL as either a primary or secondary outcome measure. This was observed using validated QOL measures, most of which were specific to IBD (Table 3). For example, the Inflammatory Bowel Disease Questionnaire (IBDQ) is a validated, 32-item questionnaire that assesses the disease-related QOL for individuals with IBD(Reference Guyatt, Mitchell and Irvine29) and was used most frequently within these studies.(Reference Bodini, Zanella and Crespi14,Reference Cox, Lindsay and Fromentin18,Reference Jian, Anqi and Gang19,Reference Bartel, Weiss and Turetschek20,Reference Kyaw, Moshkovska and Mayberry22,Reference Brotherton, Taylor and Bourguignon26,Reference Chicco, Magrì and Cingolani28) The short IBDQ (sIBDQ).(Reference Irvine, Zhou and Thompson30) is a shortened version of the IBDQ (containing 10 questions) and was utilized in six of the included studies.(Reference Gunasekeera, Mendall and Chan15,Reference Pedersen, Ankersen and Felding17,Reference Chandrasekaran, Groven and Lewis21,Reference Keshteli, Valcheva and Nickurak24,Reference Lewis, Sandler and Brotherton25,Reference Fritsch, Garces and Quintero27) Additionally, the Short Form 36 Health Survey (SF-36)(Reference Brazier, Harper and Jones31) is a validated questionnaire that assesses health-related QOL, though not specific to individuals with IBD, and was used in three studies.(Reference Melgaard, Sørensen and Riis16,Reference Tamizifar and Arab23,Reference Fritsch, Garces and Quintero27)
Measures of QOL utilized across included studies
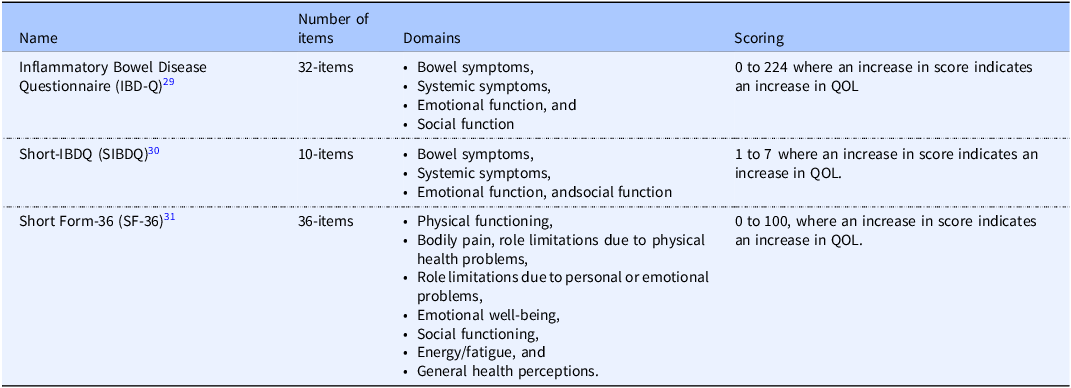
IBDQ, Inflammatory Bowel Disease Questionnaire.
QOL, quality of life.
Study design, setting, and duration
Of the 15 studies selected, 13 were randomized controlled trials (RCT).(Reference Bodini, Zanella and Crespi14–Reference Bartel, Weiss and Turetschek20,Reference Kyaw, Moshkovska and Mayberry22–Reference Fritsch, Garces and Quintero27) Six studies were unblinded,(Reference Pedersen, Ankersen and Felding17,Reference Jian, Anqi and Gang19,Reference Kyaw, Moshkovska and Mayberry22,Reference Keshteli, Valcheva and Nickurak24,Reference Lewis, Sandler and Brotherton25,Reference Fritsch, Garces and Quintero27) whereas three were double-blinded,(Reference Gunasekeera, Mendall and Chan15,Reference Melgaard, Sørensen and Riis16,Reference Bartel, Weiss and Turetschek20) three were single-blinded,(Reference Cox, Lindsay and Fromentin18,Reference Tamizifar and Arab23,Reference Brotherton, Taylor and Bourguignon26) and two were cross-over studies.(Reference Melgaard, Sørensen and Riis16,Reference Fritsch, Garces and Quintero27) In addition, two studies were uncontrolled trials.(Reference Chandrasekaran, Groven and Lewis21,Reference Chicco, Magrì and Cingolani28) These studies were conducted in multiple locations, globally (Tables 4–6). Duration of interventions ranged from four weeks to six months. Both crossover studies were 8 weeks with a 2-week washout period.(Reference Melgaard, Sørensen and Riis16,Reference Fritsch, Garces and Quintero27) Intervention delivery varied across different studies. Six of the studies provided some or all of the food items within the diet intervention.(Reference Melgaard, Sørensen and Riis16,Reference Bartel, Weiss and Turetschek20,Reference Tamizifar and Arab23,Reference Brotherton, Taylor and Bourguignon26–Reference Chicco, Magrì and Cingolani28) One cross-over study by Fritsch et al. provided participants with all meals based on menus created by a Registered Dietitian (RD).(Reference Fritsch, Garces and Quintero27) Twelve of the included studies provided in-person or personalized diet education from an RD or nutritionist on how to follow the designated diet.(Reference Bodini, Zanella and Crespi14,Reference Melgaard, Sørensen and Riis16–Reference Lewis, Sandler and Brotherton25,Reference Chicco, Magrì and Cingolani28) Additionally, two studies had access to online support while following the diets.(Reference Chandrasekaran, Groven and Lewis21,Reference Lewis, Sandler and Brotherton25) Alternatively, three studies provided diet education via handouts or other written material.(Reference Gunasekeera, Mendall and Chan15,Reference Brotherton, Taylor and Bourguignon26)
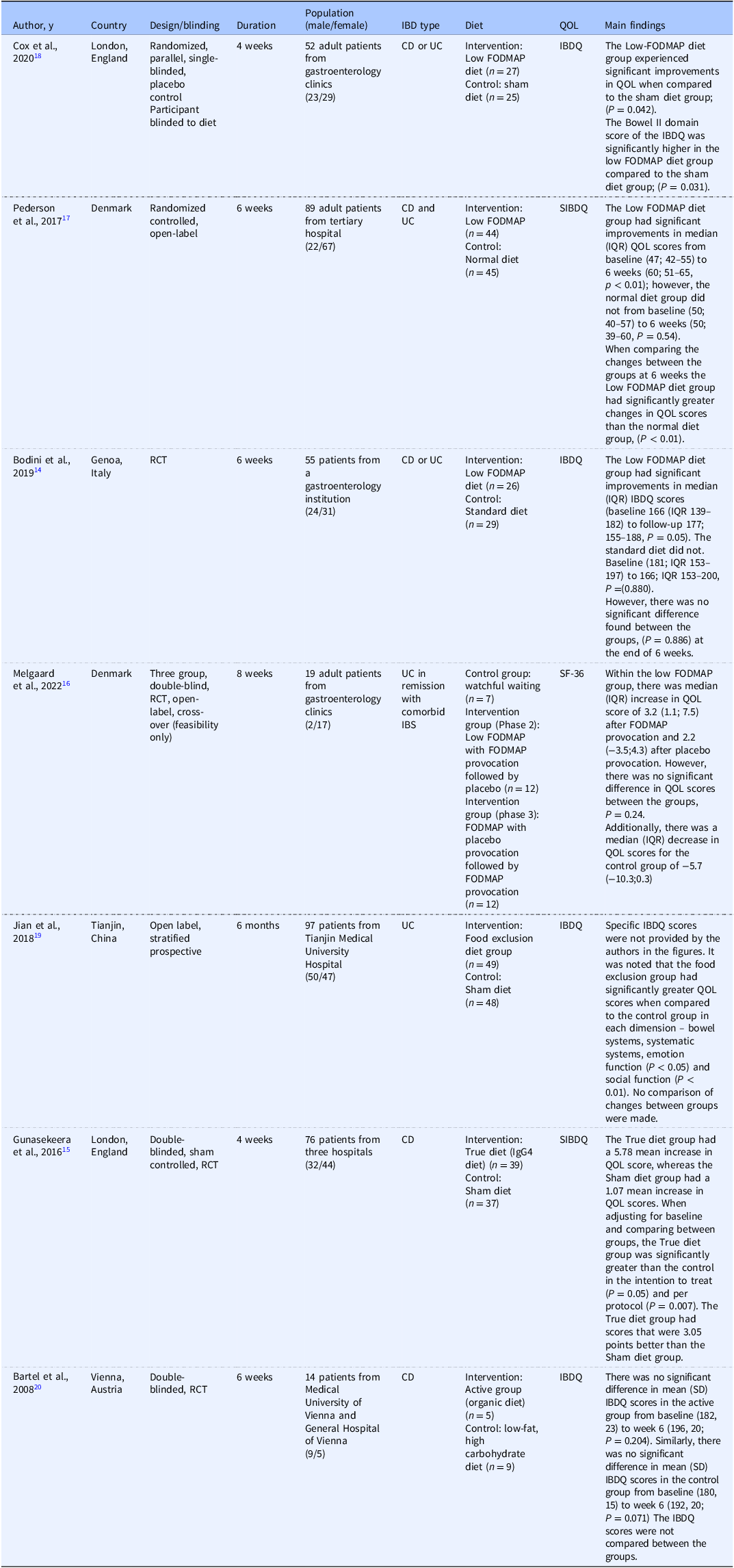
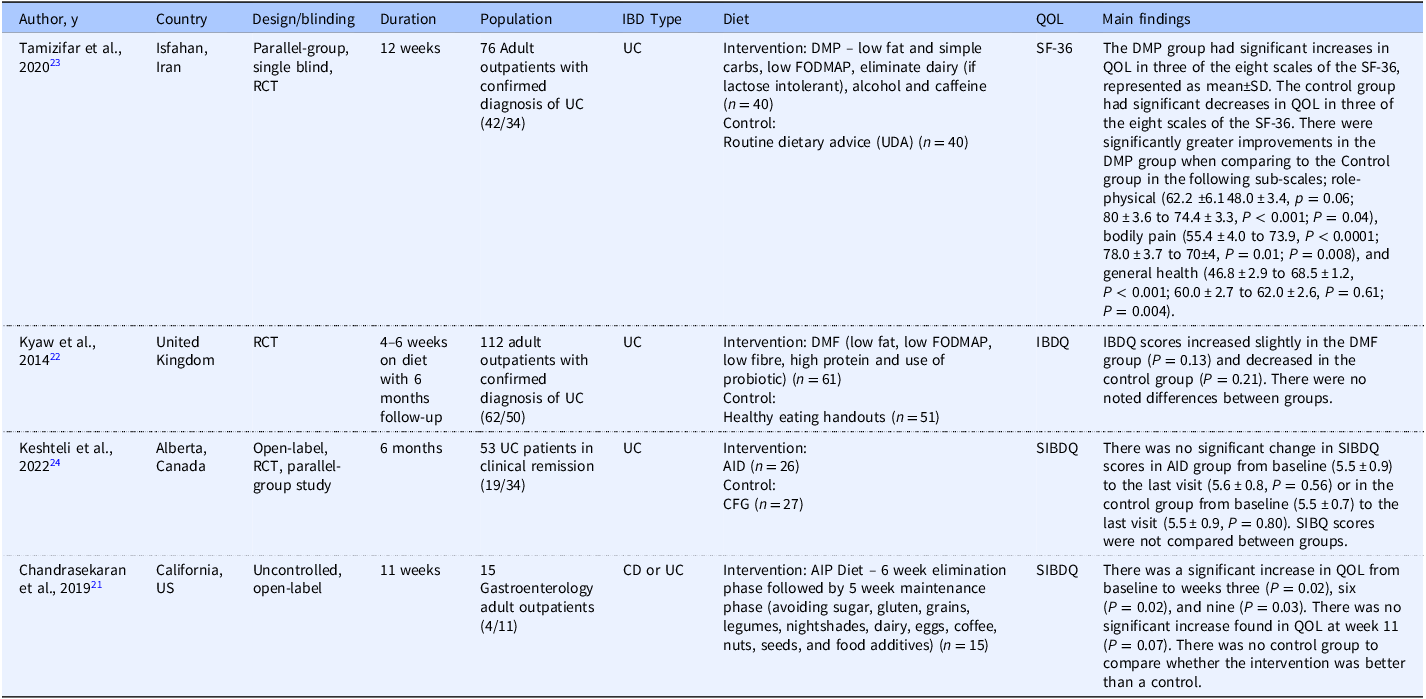
Characteristics and results of studies using elimination diets to improve quality of life among participants with IBD
CD, Crohn’s disease.
UC, Ulcerative colitis.
IBS, irritable bowel syndrome.
RCT, randomized controlled trial.
Short-form 36 (SF-36), An increase in the questionnaire score indicates an increase in Quality of Life (QOL).
Inflammatory Bowel Disease Questionnaire (IBDQ), The bowel II domain score of the IBDQ, measures GI symptoms impact on QOL.
Short Inflammatory Bowel Disease Questionnaire (SIBDQ), An increase in the questionnaire score indicates an increase in QOL.
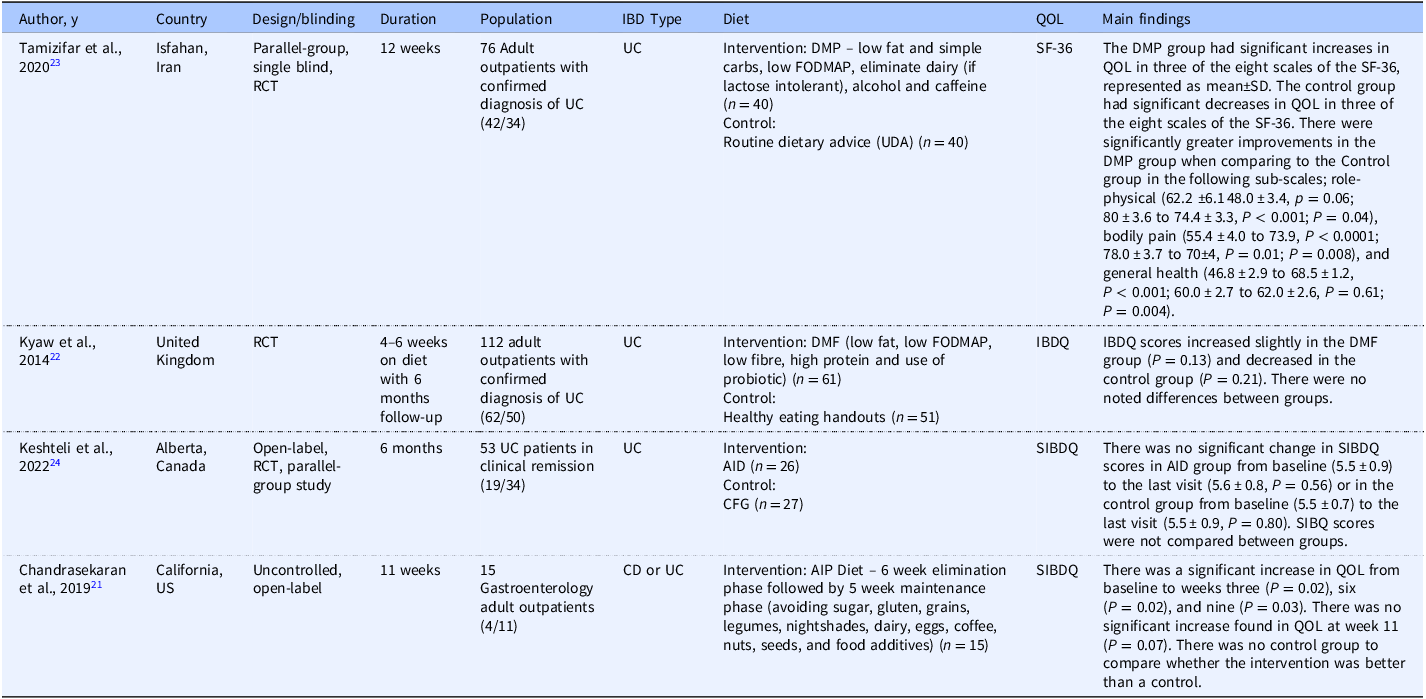
Characteristics and results of studies using an elimination diet that also increased specific foods among participants with IBD
CD, Crohn’s disease.
UC, ulcerative colitis.
RCT, randomized controlled trial.
DMP, Dietary Modification Program.
DMF, Dietary Modification Framework.
Short-form 36 (SF-36), An increase in the questionnaire score indicates an increase in Quality of Life (QOL).
Inflammatory Bowel Disease Questionnaire (IBDQ), The bowel II domain score of the IBDQ, measures GI symptoms impact on QOL.
Short Inflammatory Bowel Disease Questionnaire (SIBDQ), An increase in the questionnaire score indicates an increase in QOL.
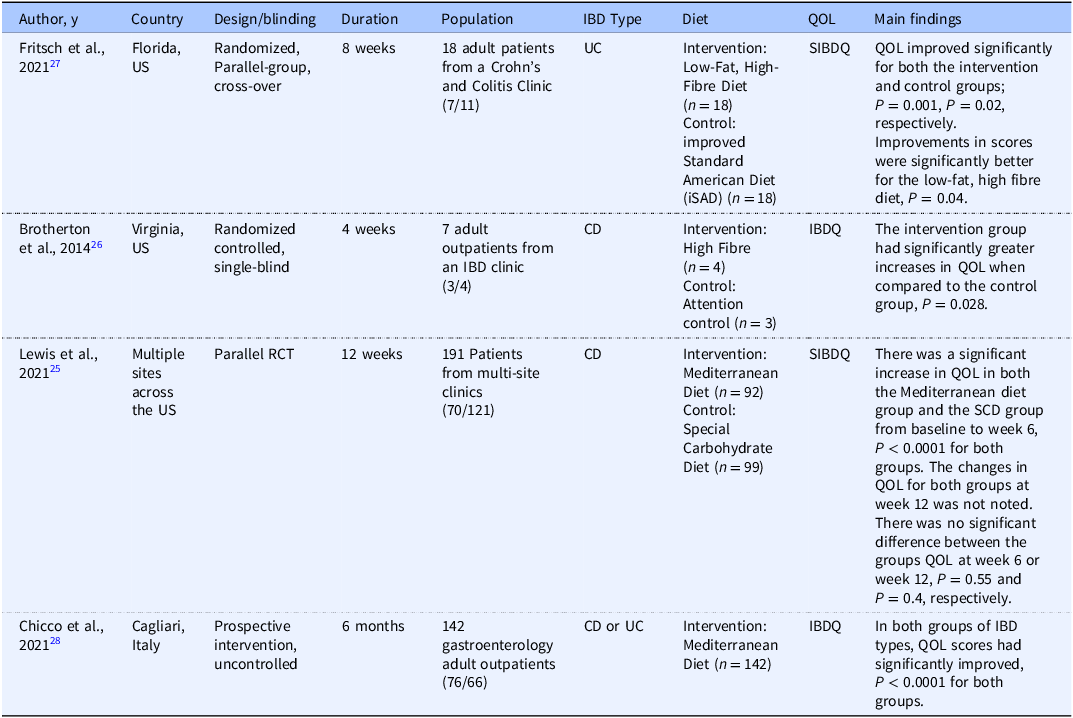
Characteristics and results of studies using dietary interventions that focus on increasing specific foods among participants with IBD
CD, Crohn’s disease.
UC, ulcerative colitis.
RCT, randomized controlled trial.
Short-form 36 (SF-36), An increase in the questionnaire score indicates an increase in Quality of Life (QOL).
Inflammatory Bowel Disease Questionnaire (IBDQ), The bowel II domain score of the IBDQ, measures GI symptoms impact on QOL.
Short Inflammatory Bowel Disease Questionnaire (SIBDQ), An increase in the questionnaire score indicates an increase in QOL.
Participant characteristics
Both sexes were included in all studies; however, more than half of the population studied were females. All studies included adult participants, 18 years and older, with a diagnosis of IBD. The IBD diagnosis was separated into subtypes: CD or UC. Where some studies included both subtypes,(Reference Bodini, Zanella and Crespi14,Reference Pedersen, Ankersen and Felding17,Reference Cox, Lindsay and Fromentin18,Reference Chandrasekaran, Groven and Lewis21,Reference Chicco, Magrì and Cingolani28) most studies did not. Crohn’s disease was studied independently within four studies, including the highly restricted organic diet, IgG4 diet, Mediterranean Diet, and high-fibre diet.(Reference Gunasekeera, Mendall and Chan15,Reference Bartel, Weiss and Turetschek20,Reference Lewis, Sandler and Brotherton25,Reference Brotherton, Taylor and Bourguignon26) Ulcerative colitis was studied independently in six studies including the low FODMAP diet, IgG diet, Dietary Modification Program, Dietary Modified Framework, and Anti-inflammatory diet interventions.(Reference Melgaard, Sørensen and Riis16,Reference Jian, Anqi and Gang19,Reference Kyaw, Moshkovska and Mayberry22,Reference Tamizifar and Arab23,Reference Keshteli, Valcheva and Nickurak24,Reference Fritsch, Garces and Quintero27)
Among the disease types, disease activity was assessed as an inclusion/exclusion criteria for each study. Most studies only included those in remission or with mild to moderate symptoms as defined by a disease severity tool (Table 1). Depending on IBD type, researchers used appropriate screening tools to select participants in either remission or with mild to moderate to severe symptoms. Tools used to screen for CD included the Harvey Bradshaw Index,(4,Reference Bodini, Zanella and Crespi14,Reference Gunasekeera, Mendall and Chan15,Reference Pedersen, Ankersen and Felding17,Reference Cox, Lindsay and Fromentin18,Reference Chandrasekaran, Groven and Lewis21) partial Harvey Bradshaw Index,(Reference Brotherton, Taylor and Bourguignon26) and the Crohn’s Disease Activity Index.(Reference Best, Becktel, Singleton and Kern6,Reference Gunasekeera, Mendall and Chan15,Reference Bartel, Weiss and Turetschek20,Reference Chicco, Magrì and Cingolani28) The Mayo Score,(Reference Bodini, Zanella and Crespi14,Reference Melgaard, Sørensen and Riis16,Reference Jian, Anqi and Gang19,Reference Chandrasekaran, Groven and Lewis21,Reference Fritsch, Garces and Quintero27) Partial Mayo score,(Reference Keshteli, Valcheva and Nickurak24) and Simple Clinical Colitis Index(Reference Pedersen, Ankersen and Felding17) were used to screen and classify participants with UC.
Medications and supplements
Treatments for IBD may include surgeries and medications all of which can be very costly and have serious or unwanted side effects.(2,Reference Holt, Strauss and Moore9) Medications are the most commonly used therapy when treating symptoms of IBD. The typical types include biologics, immunomodulators, aminosalicylate (5-ASA), corticosteroids, anti-TNF, and azathioprine.(2) Each study had different, specific inclusion and exclusion criteria for medication type, dosage, and time frame of use. Researchers in 14 of the 15 studies allowed medication use as a concomitant treatment yet required that participants remain on a stable dose throughout the study duration.(Reference Bodini, Zanella and Crespi14–Reference Cox, Lindsay and Fromentin18,Reference Bartel, Weiss and Turetschek20–Reference Chicco, Magrì and Cingolani28) Jian et al. did not report use of medication amongst participants, but they did report that changes in medical treatment would be considered for each participant.(Reference Jian, Anqi and Gang19) Although supplements such as vitamins, minerals, and probiotics may affect QOL in this population, only four studies discussed the use of supplements as inclusion and exclusion criteria. Cox et al.(Reference Cox, Lindsay and Fromentin18) and Tamizifar et al.(Reference Tamizifar and Arab23) excluded those who used or changed the dose of probiotics or prebiotics 8 weeks prior to the start of the study. Fritsch et al.(Reference Fritsch, Garces and Quintero27) excluded individuals who had used probiotics 4 weeks prior to the start of the study, whereas Bartel et al.(Reference Bartel, Weiss and Turetschek20) excluded anyone who had used probiotics. The remaining authors did not mention the use of supplements as an inclusion or exclusion criterion.
Changes in quality of life after following an elimination diet
Four studies used the low FODMAP diet for the intervention (Table 4).(Reference Bodini, Zanella and Crespi14,Reference Melgaard, Sørensen and Riis16–Reference Cox, Lindsay and Fromentin18) . Two of the four studies where the low FODMAP diet was compared to a sham or usual diet found significantly better and positive changes in QOL when compared to the control.(Reference Pedersen, Ankersen and Felding17,Reference Cox, Lindsay and Fromentin18) In a four-week randomized, parallel, single-blinded placebo control study, Cox et al. provided diet advice from an RD to 52 participants with either UC or CD.(Reference Cox, Lindsay and Fromentin18) At follow-up, the low FODMAP group experienced significantly greater IBDQ scores (81.9, SEM 1.2) compared to the sham diet group (78.3, SEM 1.2, P = 0.04). Pederson et al. also had nutritionists provide a one-hour counselling session on FODMAPs to the experimental group while the control group was asked to remain on the normal diet. After six weeks, the group following the low FODMAP intervention had a significantly greater increase in SIBDQ scores reported as median and interquartile ranges (IQR) compared to the normal diet group, (60, IQR 51–65 and 50, IQR 39–60, P < 0.01).(Reference Pedersen, Ankersen and Felding17) Additionally, scores were compared within groups from baseline to the end of the study, where the low FODMAP group had a significant increase in median scores (47, IQR 42–55 and 60, IQR 51 to 65, P < 0.01), but the normal diet group did not (50, IQR 40–57 and 50, IQR 39–60, P = 0.54), respectively. Similar to Pederson, Bodini et al. utilized a six-week low FODMAP diet intervention compared to a Standard Diet (SD) to evaluate changes in QOL.(Reference Bodini, Zanella and Crespi14) There was no significant difference between the scores reported as median and IQR from baseline to 6 weeks in the SD group (181, IQR 153–197 and 166, IQR 153–200, P = 0.88, respectively). However, there was a slight but significant increase in median survey scores in the low FODMAP diet group from baseline to 6 weeks (166, IQR 139–182; 177, IQR 155–188, P = 0.05, respectively). A positive outcome cannot be concluded as there was no significant difference found between groups at the end of 6 weeks (P = 0.88).
Lastly, in a three group, double blind RCT crossover study to test feasibility, Melgaard et al. examined changes in QOL in 19 adults with UC after completing three phases, including watchful waiting, low FODMAP with FODMAP provocation, and placebo provocation.(Reference Melgaard, Sørensen and Riis16) Provocation arms were used to provide participants with food containing FODMAPs that appeared and tasted similar to foods with low-FODMAPs. These provocation foods were made in the lab and provided to participants. They found no significant differences in changes in QOL scores over 4 weeks between the low FODMAP and placebo provocation groups, respectively (3.2, IQR 1.1–7.5; 2.2, IQR −3.5–4.3, P = 0.24). Additionally, the watchful waiting group had a decrease in QOL scores after 4 weeks although no significance level was provided (−5.7, IQR −10.3–0.3). There was no significant difference found between the groups and therefore a positive outcome cannot be concluded (P = 0.24).
Another elimination diet to consider is the IgG diet. Using a randomized, open label, stratified prospective study, Jian et al. recruited individuals previously admitted to a local hospital.(Reference Jian, Anqi and Gang19) Participants were assigned to follow the IgG diet intervention or the sham diet. Researchers examined changes in IBDQ scores in 97 participants with UC over a 6-month IgG diet intervention compared to a sham diet. There was no significant difference in the mean IBDQ scores between the groups at baseline (P > 0.05). Overall, the intervention group had significantly higher IBDQ scores compared to the sham diet group in all four dimensions; bowel symptoms, systemic symptoms, emotional function dimensions (P < 0.05), and the social function dimension (P < 0.01) after the 6-months. Similarly, Gunasekeera et al. studied an IgG4 diet, a subclass of the IgG diet, except only in those with CD.(Reference Gunasekeera, Mendall and Chan15) Individuals in the intervention group, known as the True diet, were to exclude the four foods with the highest titre response, indicating a greater immune response to those foods. The control group was instructed to exclude the four foods with the lowest titre response. Significant improvements were found in the intervention group when compared to the control after adjusting for baseline in both intention to treat and per protocol analyses, respectively (−3.05; IQR −6.11 to −0.01, P = 0.05 and −4.728; IQR −8.10 to −1.36, P = 0.007). Refer to Table 4 for details on the study results.
While the previously mentioned diets are commonly used elimination diets, Bartel et al. used a highly restricted organic diet (Table 2) in a double-blind randomized controlled trial.(Reference Bartel, Weiss and Turetschek20) Eighteen participants with mild-to-moderate CD were randomized to the active group (organic diet) or control group for six weeks with a follow-up at 24-weeks. The control group was instructed to eat a low-fat, high-carbohydrate diet while avoiding red meat and fibrous fruits and vegetables. Both groups received nutrition counselling by an RD at weeks 1, 3, and 6 of the intervention and weeks 12 and 24 of the follow-up period. The active group did not experience a significant change in IBDQ scores (reported as mean ± SD) from baseline to week 6, respectively (182 ± 23 and 196 ± 20; P = 0.204). Similarly, the control group did not experience a significant change in IBDQ scores from baseline to week 6 (180 ± 15 and 192 ± 20; P = 0.071). The changes in IBDQ scores were not compared between the intervention and control groups.
Changes in quality of life after following an elimination diet with increased specific foods
Research teams for four studies used an elimination diet paired with the addition of specific foods or nutrients (Table 5).(Reference Chandrasekaran, Groven and Lewis21–Reference Tamizifar and Arab23) In two of the four studies, research teams created similar dietary programmes for UC; however, only one found significant improvements in QOL following the intervention.(Reference Kyaw, Moshkovska and Mayberry22,Reference Tamizifar and Arab23) Tamizifar et al. created a 3-month Dietary Modification Program intervention (Table 2) for adults with UC, provided by RD instruction and an educational booklet.(Reference Tamizifar and Arab23) The control group received usual dietary advice (UDA). After adjusting for differences in baseline data, when compared to the control group, the Dietary Modification Program group had significantly greater improvements in three of the eight scales within the SF-36, including role-physical, bodily pain, and general health. Similarly, Kyaw et al. utilized the Dietary Modified Framework (Table 2) intervention in adults with UC.(Reference Kyaw, Moshkovska and Mayberry22) The diet advice was provided through an educational booklet over four to six weeks. Participants in the control group received healthy eating handouts. QOL was measured using the IBDQ, which was noted to increase slightly in the Dietary Modified Framework group with a mean difference of 7.173, yet this was not a significant change (P = 0.13). The control group was noted to have a decrease QOL scores with a mean difference of 3.454; however, this change was also not considered significant (P = 0.21). Between group changes were not noted.
In an open-label, randomized controlled, parallel study, Ketshteli et al. conducted a 6-month dietary intervention utilizing the Anti-Inflammatory Diet versus a control diet in adults with UC.(Reference Keshteli, Valcheva and Nickurak24) Twenty-six participants randomized to the Anti-Inflammatory Diet group received dietary counselling, including menus and recipes, once a month from an RD. Twenty-seven participants randomized to the control group were instructed to follow the Canada Food Guide (CFG) 2007.(Reference Canada34) There was no significant difference in SIBDQ scores reported as mean ± SD between the Anti-Inflammatory Diet group and the CFG group at baseline (5.5 ± 4.9–6.4 and 5.0 ± 5.0–6.0; P = 0.99). Furthermore, there was no significant difference in SIBDQ scores in the Anti-Inflammatory Diet group from baseline (5.5 ± 0.9) to the last visit (5.6 ± 0.8, P = 0.50) or in the CFG group from baseline (5.5 ± 0.7) to the last visit (5.5 ± 0.9, P = 0.80). There were no results reporting changes between the groups.
The Autoimmune Protocol Diet is an established diet used to reduce symptoms in autoimmune diseases. In an uncontrolled, open label study, Chandrasekaran et al. examined changes in QOL using the SIBDQ in 15 CD or UC participants after following the Autoimmune Protocol Diet over 12-weeks in an uncontrolled trial.(Reference Chandrasekaran, Groven and Lewis21) SIBDQ mean scores increased steadily at all time periods of the intervention as follows: baseline (46.5; SD 12.5) to week 3 (54.0; SD 7.7, P = 0.02); week 6 (53.3 SD 10.9, P = 0.02); and week 9 (62.0; SD 3.3, P = 0.03). However, from all participants that completed follow-up measures (n = 4), there was not a significant increase in SIBDQ scores from baseline to week 11 (46.5 to 61.5, P = 0.07). Differences in SIBDQ scores between CD and UC were also explored and there was no significant difference found between the IBD types (P = 0.77). Finally, there was no control group for comparison in this study. Refer to Table 5 for details on the study results.
Changes in quality of life while following dietary patterns with a focus on including specific foods
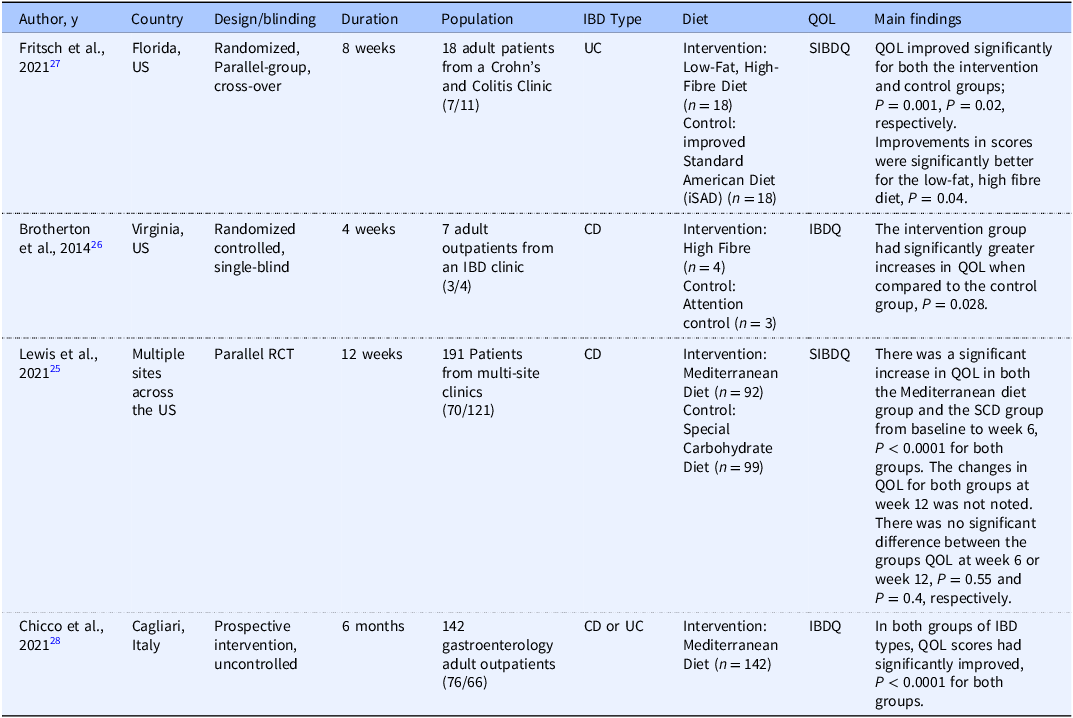
Four studies used dietary pattern interventions with a focus on including specific foods, such as the Mediterranean Diet or a high-fibre diet, to examine changes in QOL.(Reference Lewis, Sandler and Brotherton25–Reference Chicco, Magrì and Cingolani28) Control diets for three of the four studies varied, and one study was uncontrolled. All four studies had significant improvements in QOL following the intervention diets; however, not all results were compared between groups. Fritsch et al. used a randomized, parallel-group cross-over design in 18 adults with UC to examine changes in SIBQ scores following a low-fat, high-fibre diet (Table 6) and an improved standard American diet (iSAD) as the control.(Reference Fritsch, Garces and Quintero27) All meals were provided to the participants. SIBDQ scores increased significantly in both the intervention (P = 0.001) and control groups (P = 0.02) after 4 weeks on each diet. There were significant improvements in many of the scales within the SF-36 within both groups, including limitations due to physical health scores, role limitations due to emotional problems scores, social functioning scores, and bodily pain scores. Overall, the general health scores significantly improved from a baseline average of 48.5 in both the intervention and the control (59.1, P = 0.03 and 57.6, P = 0.04).
Similar to Fritsch, Brotherton et al. examined changes in QOL using a high fibre diet.(Reference Brotherton, Taylor and Bourguignon26) However, this was a randomized controlled, single-blinded study that used an attention control diet in 7 adults with CD over 4 weeks. The high fibre diet was not defined by the researchers; however, the intervention group received education on high-fibre, low-refined carbohydrate intake, and were encouraged to consume ½ cup of provided, whole wheat bran cereal and at least 48 oz of fluid per day, whereas the control group was instructed to avoid whole grains. They found that IBDQ scores significantly increased over time for the intervention group when compared to the control group, (P = 0.028). Clinical significance, defined by authors as a > 32-point increase, was also found in the high fibre diet group with a mean increase of 44.25-points in IBDQ scores whereas the control group had a mean increase of 19-points. This study collected additional data on diet adherence but did not report the findings. The small sample size of 7 should be considered when interpreting the results of this study.
Two studies explored changes in QOL after following the Mediterranean diet (MD).(Reference Lewis, Sandler and Brotherton25,Reference Chicco, Magrì and Cingolani28) However, Lewis et al.(Reference Lewis, Sandler and Brotherton25) used the Specific Carbohydrate diet (SCD), a diet commonly used within IBD, as the control diet in a parallel RCT with 194 participants with CD, whereas Chicco et al.(Reference Chicco, Magrì and Cingolani28) did not use a control diet and included 142 participants with either UC or CD. Lewis et al. found improvements in SIBDQ scores in the SCD group which was associated with an increase in standardized mean difference of SIBDQ scores from baseline to 6 weeks, (8.85 to 10.4, P < 0.0001); however, there was no report on the results from 6–12 weeks.(Reference Lewis, Sandler and Brotherton25) Additionally, the SCD did not have a significantly greater increase in median SIBDQ scores at week 6, (49.0, 39.0–58.0) compared to MD median scores at week 6, (49.5, 39.0–56.0, P = 0.55). Similarly, the SCD did not have a significantly greater increase in median SIBDQ scores at week 12, (50.0, 38.0–58.0) compared to MD median scores, (45.5, 36.0-57.0, P = 0.040). Chicco et al. found significantly improved IBDQ scores after the intervention (P < 0.0001) yet did not have a control group for comparison between groups. Reference Chicco, Magrì and Cingolani28 Refer to Table 6 for additional details on study results.
Discussion
Although this research is in its preliminary stages, it appears as if a wide range of dietary approaches have the potential to positively impact QOL in adults with IBD. Significant improvements in QOL were found in six of the 15 studies, including interventions using the low FODMAP,(Reference Pedersen, Ankersen and Felding17,Reference Cox, Lindsay and Fromentin18) IgG,(Reference Gunasekeera, Mendall and Chan15,Reference Jian, Anqi and Gang19) Dietary Modification Program,(Reference Tamizifar and Arab23) and high fibre diet.(Reference Fritsch, Garces and Quintero27) The Autoimmune Protocol,(Reference Chandrasekaran, Groven and Lewis21) Anti-inflammatory Diet,(Reference Keshteli, Valcheva and Nickurak24) highly restricted organic diet,(Reference Bartel, Weiss and Turetschek20) Dietary Modified Framework,(Reference Kyaw, Moshkovska and Mayberry22) and Mediterranean Diet(Reference Lewis, Sandler and Brotherton25,Reference Chicco, Magrì and Cingolani28) did not result in significantly improved QOL. Most of the dietary approaches were compared to a sham control diet or did not include a control, with one exception, where Lewis et al. compared the Mediterranean Diet to the Specific Carbohydrate Diet.(Reference Lewis, Sandler and Brotherton25) Thus, superiority of one dietary approach over another cannot be determined at this time.
Our results are similar to others using different search terms. Gomes et al. focused on dietary intake and gut microbiota in adults with IBD.(Reference Gomes, Gomes and Braga13) Similar to the findings of this review, Gomes et al. found that some of the same diets, including the MD, SCD, and low FODMAP diet may assist in reducing IBD symptoms, thus improving QOL.(Reference Gomes, Gomes and Braga13) However, this research team only focused on those with UC in remission. Lemketkai et al. conducted a systematic review and meta-analysis using 27 RCT studies to examine dietary interventions as a treatment for IBD.(Reference Limketkai, Godoy-Brewer and Parian10) Ten of the 27 studies measured QOL, of which six were included in this review. Although the purpose of their review was to focus on dietary interventions inducing remission, it was also noted that a diet high in fibre was not associated with reducing relapse despite increases in QOL in those with CD. Additionally, similar to this review, Limketkai et al. found that there were no improvements in QOL associated with the highly restricted organic diet or the AID. Furthermore, significant improvements in QOL were noted in other dietary intervention studies, such as a high-fibre diet, SCD, and MD diets. Yet only the high-fibre diet was found to have significant improvements in QOL when compared to the control group, whereas others were only compared within groups. The research team found that the MD and SCD may promote clinical remission for those with CD. However, there were no dietary interventions found to be associated with inducing remission in those with UC. Lemketkai et al. concluded a need for additional dietary intervention studies in IBD to increase the certainty of evidence that can help develop nutrition guidelines for IBD.(Reference Limketkai, Godoy-Brewer and Parian10)
Within all 15 studies reviewed, validated-specific questionnaires were used to assess health-related QOL. Despite these findings, it is difficult to determine if these diets should be recommended long-term as these studies had short study durations. Within the reviewed studies, three of the low FODMAP diet studies did not include the recommended reintroduction or maintenance phase of the diet. Thus, a conclusion cannot be drawn for the long-term impact of this diet. Elimination diets can be difficult to follow and could result in the restriction of foods if not followed correctly. Therefore, additional studies are needed to evaluate the long-term effects of these diets on QOL in addition to adequate nutrient intake. Dietary patterns such as the MD or high fibre diet may be more sustainable and easier to implement. Furthermore, the MD provides additional health benefits such as lowering the risk of cardiovascular disease and cancer, which are common comorbidities for those with IBD.(7,Reference Lewis, Sandler and Brotherton25)
The impact of these nine different diet interventions on QOL outcomes in adults with IBD requires further research. As noted, one limitation was the inclusion of only one subgroup, CD or UC. A reoccurring limitation amongst these studies is the small sample sizes; therefore, the reported changes in QOL were often underpowered. Additionally, most of these studies utilized a controlled sham diet that mimicked usual dietary intake rather than comparing dietary interventions. Thus, this design does not show the differences in changes in QOL across the different diet types, such as comparing an elimination dietary intervention to a dietary pattern intervention. However, these interventions ranged widely from elimination diets to inclusive, more sustainable diets. As mentioned previously, these dietary interventions were of short durations and did not always carry out all phases of the diets. Future research should focus on long-term benefits of dietary adherence. Additionally, the changes in QOL were not always reported clearly, making it difficult to draw conclusions. Because many of the study participants had mild to moderate symptoms, these diets cannot be generalized to all individuals with IBD.
Future research should compare the different dietary approaches and assess disease specific outcomes, diet adherence, adequacy of the diet long-term, sustainability of the diet long-term, other eating behaviours, and QOL. Similar to Lewis et al.(Reference Lewis, Sandler and Brotherton25) that compared the MD and SCD, researchers may consider comparing some of these dietary approaches to one another in a single study. It may be easier to highlight a superior dietary approach when they are compared side by side. For example, while elimination diets may be helpful in identifying foods and beverages that may be associated with symptoms, these diets are typically not appealing due to strict restrictions, nor are they meant to be followed long-term.(Reference Gunasekeera, Mendall and Chan15) Therefore, it should be noted that QOL may increase temporarily while strictly following an elimination diet due to changes in symptoms. Additionally, more studies are needed that include adequate numbers of both groups of CD and UC to understand the impact of dietary interventions in both groups. Results from dietary approaches may differ between the subgroups due to the previously mentioned differences between the disease location and inflammation. Larger sample sizes and longer study durations should also be a priority for future researchers to improve certainty of evidence.
Overall, dietary patterns that focus on specific foods or food groups showed the most consistent results, leading to increased QOL after the intervention diets. This is likely because they are more sustainable. Elimination diets, particularly the low FODMAP diet, showed mixed outcomes, with two studies reporting significant QOL improvements, likely due to the support from Registered Dietitians (RD) and nutrition counselling, which can improve sustainability. Conversely, studies with elimination diets that included specific foods had the fewest significant QOL increases after dietary changes, resulting in less consistent evidence.
Finally, the diversity of study designs and interventions can affect the interpretation of QOL outcomes when comparing studies. For example, in RCTs, the cross-over design may yield more robust results than double-or single-blinded designs because it allows participants to serve as their own controls. Similarly, the RCT studies will yield more reliable results than the uncontrolled trials because they allow comparison with a control group. Those with longer study durations demonstrate the sustainability of the dietary interventions and their long-term impact on QOL. Additionally, participants who received meals may have higher participation and lower attrition than those who did not, thereby influencing QOL outcomes.
Conclusion
Implications for practice
This review highlights the potential for several dietary interventions to positively impact QOL in adults with IBD. These diets are complex and require nutrition counselling from an RD. In 12 of the 15 studies, an RD was used to help explain the diet and counsel participants.(Reference Bodini, Zanella and Crespi14,Reference Melgaard, Sørensen and Riis16–Reference Chandrasekaran, Groven and Lewis21,Reference Tamizifar and Arab23–Reference Lewis, Sandler and Brotherton25,Reference Fritsch, Garces and Quintero27,Reference Chicco, Magrì and Cingolani28) For example, the low FODMAP diet should be carried out in three phases as opposed to remaining in the elimination phase long-term. Additionally, a high fibre diet is contraindicated for individuals with strictures. Therefore, an RD with experience in the treatment of IBD needs to be included as a member of the healthcare team to individualize diets to (1) reduce symptoms, (2) meet nutrient needs, and (3) accommodate preferences, resources, abilities, and lifestyles for adults with IBD. Based on the results from this study, these diets are likely most appropriate for adults with IBD in remission or with mild to moderate symptoms.
Acknowledgements
The authors have no acknowledgements to declare.
Author contributions
Rebekah McGuire contributed to the conceptualization and drafting of the work. Linda L. Knol and Joy W. Douglas equally contributed to reviewing and revising the work critically for important intellectual content. All authors agree to be accountable for all aspects of the work and read and approve the final manuscript.
Funding support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors declare none.


 Open access
Open access