


Breastfeeding is critical for child survival. Promotion of early initiation and exclusive breastfeeding for 6 months with continued breastfeeding for up to 24 months is one of ten interventions that, if implemented at 90 % coverage, could reduce child mortality by 15 %(Reference Bhutta, Das and Rizvi1). Breastfeeding prevents major causes of newborn and child mortality and may reduce the risk of childhood obesity and type 2 diabetes later in life(Reference Horta, Loret de Mola and Victora2–7). For mothers, breastfeeding protects against breast and ovarian carcinoma and reduces the risk of type 2 diabetes(Reference Chowdhury, Sinha and Sankar8). Furthermore, breastfeeding is associated with improved performance in intelligence tests among children(Reference Horta, Loret de Mola and Victora9), while breastfeeding is not associated with ‘economic losses of about $302 billion annually’(Reference Rollins, Bhandari and Hajeebhoy10).
Early initiation has been shown to improve exclusive breastfeeding rates(Reference Bégin, Maaike and White4). However, globally, less than half of all newborns are put to the breast within 1 h of birth, and only two out of five infants under 6 months of age are exclusively breastfed(Reference Bégin, Maaike and White4). In Kenya, 60 % of children are put to the breast within 1 h of birth, and 60 % of infants aged 0–5 months are exclusively breastfed(11). The prevalence of exclusive breastfeeding in Kenya has remained largely unchanged since 2014(11).
Breastfeeding education(Reference Admasu, Egata and Bassore12), counselling and support can improve breastfeeding practices(Reference Nguyen, Keithly and Nguyen13–Reference Haroon, Das and Salam15). It has been demonstrated that breastfeeding counselling (BFC) can result in a 90 % increase in exclusive breastfeeding of infants aged 0–5 months. A 2015 meta-analysis found that counselling or education increased the rates of early initiation, exclusive breastfeeding and continued breastfeeding, particularly in low- and middle-income countries(Reference Sinha, Chowdhury and Sankar16). In Kenya, 87 % of children whose mothers received BFC during antenatal care (ANC) visits were exclusively breastfed for the first 2 d compared with 27 % of children whose mothers did not receive BFC during ANC(11). While scaling BFC as part of routine ANC and postnatal care (PNC) could improve breastfeeding practices(Reference Menon, Nguyen and Saha17), BFC is not well integrated into the health system in Kenya(18).
Effective BFC requires skilled ANC and PNC providers. The 2018 WHO Guideline: Counselling of Women to Improve Breastfeeding Practices recommends that all pregnant women and mothers with young children receive BFC at least six times from the antenatal period through age 2(19). Step 2 of the Baby-Friendly Hospital Initiative (BFHI) Ten Steps focuses on ensuring staff have sufficient skills to support breastfeeding(7). One way to build health worker competencies is through the BFHI Training Course for Maternity Staff (BFHI training)(20).
The Kenya Ministry of Health (MoH) prioritised capacity strengthening for quality maternal, infant and young child nutrition service delivery(21). Mentoring interventions, in addition to training, have been found effective in strengthening the capacity of health workers and in improving the clinical management of infectious diseases among mothers, newborns and children(Reference Anatole, Magge and Redditt22–Reference Green, de Azevedo and Patten24). Mentoring interventions may also increase health workers’ adherence to guidelines, standards and protocols(Reference Feyissa, Balabanova and Woldie23). Additionally, mentorship programmes have been shown to strengthen health workers’ confidence and ability to implement a range of practices(Reference Melnyk, Fineout-Overholt and Feinstein25).
In 2022, stakeholders in Kenya proposed the development of a facility-based mentorship programme to strengthen health workers’ BFC competencies. The Division of Nutrition and Dietetics of the Kenya MoH; the BFHI Task Force of the Maternal, Infant and Young Child Nutrition technical working group and USAID Advancing Nutrition developed Implementation Guidance for a Facility-Based Breastfeeding Counselling Mentorship Program (26), leveraging global guidance and tools, including the BFHI training(20) and the Competency Verification Toolkit: Ensuring Competency of Direct Care Providers to Implement the BFHI (27) to design the facility-based implementation guidance. The Implementation Guidance provides a structured framework for establishing a facility-based BFC mentorship programme. It outlines specific roles and responsibilities for different stakeholders – from facility leadership to individual mentors and mentees – and provides adaptable tools such as mentee self-assessment tool, mentor observation checklists and mentor feedback forms. The Competency Verification Toolkit observation tools informed our verification approach for assessing knowledge and building health workers’ BFC skills across sixteen specific competencies necessary for implementing the Ten Steps to Successful Breastfeeding. Our study prioritised competencies in foundational skills; antenatal period, birth and immediate postpartum; essential issues for breastfeeding mothers and care at discharge. These resources were designed to be adaptable while maintaining fidelity to global BFHI standards, allowing for contextual implementation across different facility types and resource levels.
In 2023, the Kenya MoH and USAID Advancing Nutrition conducted this study to assess the feasibility of the BFC mentorship programme in the ANC and PNC departments of Mbagathi County Referral Hospital (Mbagathi Hospital). This study aimed to identify factors that enabled and hindered the programme’s implementation and measure its impact on health workers’ confidence and clients’ perceptions of BFC.
Methods
Study description
Study setting
The study was conducted in the ANC and PNC departments of Mbagathi Hospital, a level five public county referral hospital located in Kibra Sub-County, Nairobi, Kenya.
We selected this health facility in consultation with stakeholders for several reasons. First, the hospital has a high patient load; per day, it serves 75–80 pregnant women through the ANC clinic and has 25–30 live births(28). This large number of deliveries serves as an indicator of the high need for skilled BFC in the facility. Second, at the time, health facility staff had not been trained in the BFHI. This provided an opportunity for the study team to deliver the BFHI training pre-intervention as a prerequisite to the BFC mentorship programme. Finally, Mbagathi Hospital has maternal and child health programmes that complement the BFC mentorship programme, including a kangaroo mother care unit, staff trained on emergency obstetric and newborn care and continuous quality improvement teams.
The ANC and PNC departments were chosen as the focus of the study because of the importance of providing timely BFC during prenatal care and immediately after delivery. Additionally, it was important to ensure that our results would be useful in informing BFC implementation interventions within other public-level five referral hospitals in Kenya.
Description of the intervention
The intervention was a facility-based mentorship programme carried out from March to September 2023 in accordance with the implementation guidance for a facility-based BFC mentorship programme(26). This implementation guidance serves as a bridge between the BFHI Training Course and the BFHI Competency Verification Toolkit. It provides a comprehensive background on BFC, programme rationale and a programme management structure specifically designed for facility-based BFC mentorship, along with monitoring systems and adaptable tools for mentors and mentees.
For the study, we prioritised BFC competencies in foundational skills: communicating in a credible, effective way; antenatal, birth and immediate postpartum care; essential issues for breastfeeding mothers and care at discharge.
Prior to programme implementation, a comprehensive stakeholder sensitisation process was conducted. This included meetings with the Chief Executive Officer, Hospital Management Team, Reproductive Health department heads and Hospital administrator to secure institutional buy-in. The sensitisation emphasised the programme’s alignment with national breastfeeding promotion policies and its potential benefits for maternal and child health care, which was crucial for gaining administrative support and facilitating integration into existing hospital workflows.
After a 4-day training for ANC and PNC department health workers on the BFHI, implementation began with establishing the mentorship programme leadership structure at the facility. National BFHI training facilitators, the BFHI coordinator and the mentorship coordinator selected mentors (see Study Participants section below). Mentors, the facility BFHI coordinator and the facility mentorship coordinator participated in a 2-day Core Concepts in Mentorship Training for the Breastfeeding Counselling Mentorship Program (29) – an evidence-based curriculum grounded in adult learning principles that covers interpersonal communication, clinical teaching methodologies and contextual mentoring specific to BFC through participatory exercises aligned with BFHI standards to prepare them to support and guide mentees effectively throughout the programme.
Mentors supported mentees for 4 months. The mentoring involved demonstrations, mentor observations using competency assessment tools and weekly meetings. Meetings were both formal and informal, individual and in small groups. Mentors used clinical teaching, side-by-side mentoring and case presentations. Once per month, mentors, mentees, the BFHI coordinator, the mentorship coordinator and BFHI training facilitators met to review monthly activities, discuss areas for improvement and share experiences.
Study design
The study used a mixed-methods approach. The study aimed to identify factors that enabled and hindered the implementation of the facility-based BFC mentorship programme through health worker surveys at baseline and endline and focus group discussions (FGD) and key informant interviews (KII) at endline. We used health worker surveys (at baseline and endline) to measure the effect of the mentorship programme on mentees’ confidence related to BFC. We used client exit interviews (at endline) to determine the perceptions of pregnant and postpartum women related to their BFC experience. While the programme included competency assessments using standardised verification tools, this feasibility study focused primarily on self-reported confidence as a proximal indicator of programme impact. Data from mentors’ observations of counselling skills were collected but will be reported separately. This decision allowed us to prioritise implementation feasibility while maintaining a manageable assessment approach in the busy clinical setting.
Study participants and sampling methods
The study involved health workers, pregnant women and postpartum mothers in the ANC and PNC departments of Mbagathi Hospital, as well as health facility leadership. All doctors, nurses, nutritionists, clinical officers and midwives (eighty-seven total) from the ANC and PNC departments at Mbagathi Hospital were considered for participation in the study. Of these, eighty health workers participated in the BFHI training, and from this group, seven mentors and twenty-one mentees were selected for the study. The selection of mentors and mentees (see online supplementary material, Supplemental Material S4) was based on the criteria described in the implementation guidance(26), which includes designation as a doctor, nurse, nutritionist, clinical officer or midwife and at least 2 years of experience in maternal and newborn care. All pregnant women exiting the ANC department and all postpartum women exiting the PNC department on data collection days were screened for eligibility for the study. Eligible ANC clients were in the third trimester (≥ 29 weeks of gestation), had attended an ANC appointment and reported receiving BFC from a health worker during a visit in the prior 2 weeks. For PNC clients, eligibility criteria included having delivered a full-term infant and reported receiving BFC from staff. Enumerators interviewed sixty-two ANC clients at baseline and sixty at endline, and sixty-one PNC clients at baseline and sixty at endline (see Sample Size Calculation below). Health facility leaders purposively selected for KII included members of the health facility management team, the BFHI facility implementation team and the BFHI facility coordinator for Mbagathi Hospital.
Sample size calculation for client exit interviews
The required sample size for client exit interviews was calculated based on an estimated 18 live births per day, resulting in approximately 252 live births over each 2-week data collection period – baseline and endline. To achieve a 90 % confidence level with a 10 % margin of error, a sample size of fifty-two per time point per unit/clinic was required. Accounting for a 10 % nonresponse rate, the target sample size was adjusted to 60 per time point per unit/clinic.
The sample size (n) and margin of error (E) are given by
 $$n = {{N - x} \over {\left( {\left( {N - 1} \right){E^2}} \right) + x}}$$
$$n = {{N - x} \over {\left( {\left( {N - 1} \right){E^2}} \right) + x}}$$
 $$x = Z{\left( {{c \over {100}}} \right)^{2r\left( {100 - r} \right)}}$$
$$x = Z{\left( {{c \over {100}}} \right)^{2r\left( {100 - r} \right)}}$$
 $$E = \left[ {\sqrt {\left( {N - n} \right)x} /n\left( {N - 1} \right)} \right]$$
$$E = \left[ {\sqrt {\left( {N - n} \right)x} /n\left( {N - 1} \right)} \right]$$
where N is the population size, r is the fraction of responses of interest and Z(c/100) is the critical value for the confidence level c. The Raosoft sample size calculator was utilised for these calculations.
Data collection
Quantitative data
Health workers completed two online multiple-choice surveys (health worker post-training survey S5) in April 2023 at the start of the mentorship programme (baseline) and in September 2023 after the mentorship programme (endline).
Survey tools were developed based on the Competency Verification Toolkit(27).
Structured client exit interviews were administered by trained enumerators, either in person or by phone, immediately after determining eligibility and obtaining consent (Client Exit Interview Guide S6 and S7). We developed the interview guides in English, using questions in the most recent Service Provision Assessment tool, and had them translated into Kiswahili by a professional translator(11). Enumerators, fluent in both English and Kiswahili, asked clients how often certain actions occurred and how satisfied they were with the BFC services received.
Qualitative data
Qualitative data were collected at endline through FGD with mentors and mentees and KII with facility leadership. We conducted two FGD with mentees (one with PNC mentees and one with ANC mentees) and another with mentors. FGD included all mentors and mentees available (six out of seven and fourteen out of twenty-one, respectively). Trained research assistants facilitated FGD and KII using semi-structured guides that explored perceptions of the mentorship programme. FGD and KII were conducted in English. With participants’ consent, they were recorded and subsequently transcribed.
Study measures
Health worker surveys included twenty-one knowledge questions, which we computed into an overall test score (number) and percentage of questions answered correctly. Thirty-two questions assessed confidence in their ability to provide quality BFC using a Likert scale (not at all = 0, slightly = 1, somewhat = 2, quite = 3 and extremely = 4), which we converted to a binary outcome of extremely confident or not. We computed the percentage of BFC skills in which the health workers felt extremely confident all the time and also broken down as < 50 %, 50–79 %, and 80–100 % of the time.
Similarly, client exit interviews included twenty-six questions about health worker BFC practices during the ANC visit or postnatally using a Likert scale (no, never = 0; yes, some of the time = 1; yes, most of the time = 2 and yes, all of the time = 3).
Data analysis
Quantitative data
We used Stata v17 for management and analysis of quantitative data (StataCorp LP). We calculated descriptive statistics, numbers and percents for categorical variables and means, medians and interquartile range (IQR) for continuous variables. We conducted bivariate analysis to compare measures across time points, reporting P-values from Pearson’s chi-squared test for categorical variables and Wilcoxon rank sum test for continuous variables. For binary outcomes in the paired sample of health worker surveys, we used McNemar’s chi-square test to determine the statistical significance of differences in the proportions observed. We defined statistical significance of differences between time points as P < 0·05.
Qualitative data
We analysed and coded qualitative data collected during KII and FGD. We developed a coding framework iteratively through deductive and inductive approaches. Using the framework, two people independently coded all the transcripts. They compared results and discussed differences and generated a results matrix in Excel. Due to the limited number of transcripts, we used a rapid matrix-based analysis. The inductive process included familiarisation with data and development of broad codes and their definitions, as well as fine codes with illustrative quotes. All authors reviewed the coding framework and results matrix and helped identify themes. We refined themes through discussion and then interpreted and reported results.
Results
Quantitative findings from health worker surveys
Characteristics of health workers at baseline
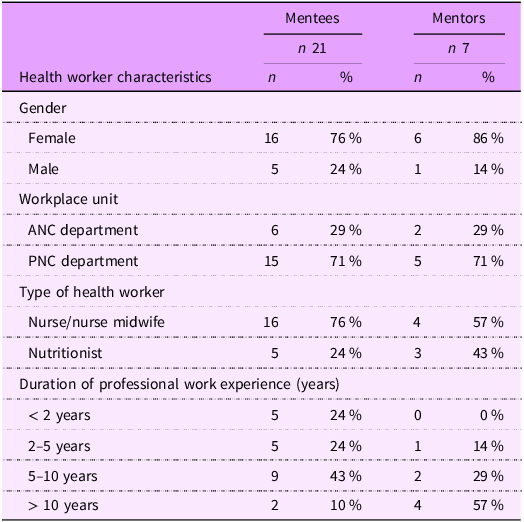
All twenty-one mentees and seven mentors completed the health worker survey at baseline, and nineteen mentees and seven mentors completed it at endline (Table 1). Most health workers were female (76 % of mentees and 86 % of mentors), and 71 % worked in the PNC department. Most mentors and mentees were nurses (76 % and 43 %, respectively). Approximately half of mentees (53 %) had 5 or more years of professional experience, 24 % had 2–4 years and 24 % had less than 2 years. More than half of mentors (57 %) had more than 10 years of experience. At baseline, all mentors and mentees reported having previously counselled clients on breastfeeding. Two mentees did not complete the endline survey. One had transferred to another facility midway through the programme, and the other was out of the country during the endline data collection period. Their baseline data were excluded from the comparative analysis.
Baseline characteristics of health workers

ANC, antenatal care; PNC, postnatal care.
Knowledge and confidence before and after mentorship
Knowledge and confidence related to BFC were high at the start of the programme. Knowledge was retained and confidence remained high throughout the programme (Table 2). On average, mentees answered 94 % of questions correctly at baseline and 92 % at endline. They were extremely confident in their ability to perform 72 % of actions related to BFC competencies at baseline and 75 % at endline. The percentage of mentees who felt extremely confident in their ability to conduct at least 50 % of the BFC actions increased from 71 % to 95 %. In addition, the percentage of mentees who were extremely confident in their ability to counsel women on breastfeeding and infant feeding increased from 67 % to 95 %. We did not observe statistically significant changes in confidence to perform other actions related to BFC. We combined data from multiple sources aligned with the WHO/UNICEF Competency Verification Toolkit. Table 3 presents this synthesis, showing how mentees’ knowledge (based on Annex E multiple-choice knowledge questions), self-reported confidence (aligned with thirty-two performance indicators from observation tools to verify competencies – Annex G) and client-reported experiences interconnect across key competency areas. While knowledge and overall confidence levels were high at baseline and remained stable, specific improvements were observed in counselling confidence, particularly in mentees’ ability to counsel women on breastfeeding and infant feeding, suggesting the mentorship programme reinforced practical application of existing knowledge.
Mentee knowledge and confidence for counselling pregnant and postpartum women on breastfeeding

BFC, breastfeeding counselling.
Summary of change in performance indicators by data source

Note: A successful mentorship programme for BFC is assured through knowledge, as the percent of the twenty-one knowledge questions answered correctly at baseline and endline confirms. The confidence levels to perform the thirty-two skills (measured by the thirty-two performance indicators) at baseline and endline stayed the same, indicating that the mentees have acquired and maintained the required attitude to provide quality BFC. This was verified using standardised detailed observation tools as shown in this table.
PNC, postnatal care, BFC, breastfeeding counselling.
Experiences with and perceptions of the mentorship programme
After the programme, all surveyed mentors and mentees said they would encourage others to join the programme (Table 4). The majority (89 %) of mentees indicated that the breastfeeding session observation job aid was the most helpful learning tool (Table 8 – see online supplementary material, Supplemental Material S2).
Mentors’ and mentees’ perceptions of the BFC mentorship programme at endline

BFC, breastfeeding counselling.
Most mentees (63 %) reported spending 4 or more hours per week with their mentor. Mentees felt that strong listening skills (95 %), counselling skills (89 %) and knowledge of breastfeeding (84 %) were important mentor qualifications, along with being supportive (89 %) and respectful (79 %) of mentees. Almost all mentees felt very respected by the mentors (95 %).
Six of the seven mentors felt very prepared for the BFC mentorship programme. All indicated that the mentor training was helpful, and they understood what was expected of them. All were satisfied with the support they received from health facility management – 43 % were very satisfied and 57 % were somewhat satisfied. The mentorship activities took a fair amount of time – 57 % of mentors reported spending 3–4 h per week per mentee. Mentors reported conducting an average of eight formal observations per mentee throughout the programme period, with most 63 % mentees spending 3 or more hours per week with their mentor.
Quantitative findings from client exit interviews
Client characteristics
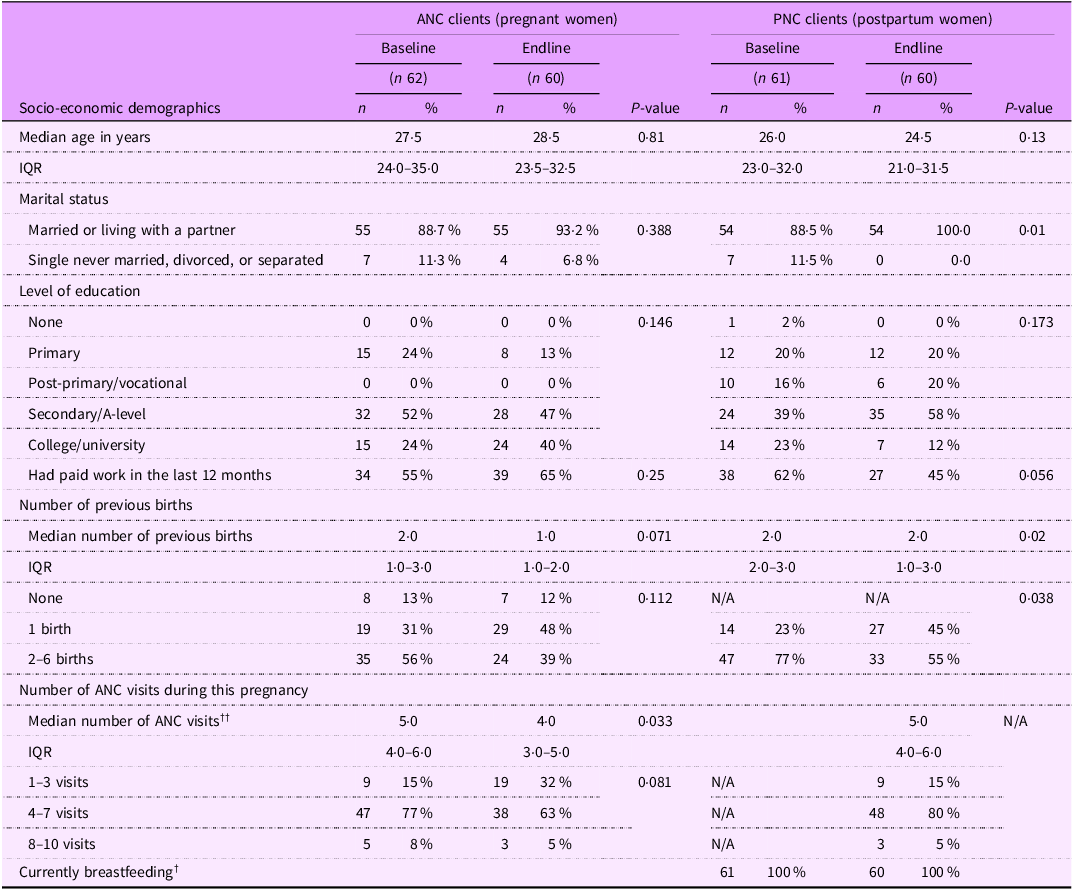
We interviewed 122 ANC clients (sixty-two at baseline, sixty at endline) and 121 PNC clients (sixty-one at baseline, sixty at endline) (Table 5). Most demographic characteristics were similar across time points for both groups. The median age of ANC clients was approximately 28 years, with most being married or cohabitating. For PNC clients, the percentage who were married or cohabitating increased from baseline to endline (88·5 % to 100 %, P = 0·01), and those with two or more previous births decreased (77 % to 55 %, P = 0·038). Other characteristics showed no statistically significant differences between time points.
Demographic characteristics of ANC and PNC clients who received BFC at Mbagathi hospital

The median number of births for the postpartum women at baseline was 2·0 (IQR 2·0–3·0) while at endline it was 2·0 (IQR 1·0–3·0). The IQR range at endline of 1·0–3·0 suggests that 50 % of women had between one and three births, showing a wider spread or greater variability in the number of births. This suggests that by the endline, there was a broader range of experiences regarding the number of births among the sampled population, with more women having fewer births (as low as one) compared with the baseline. ANC, antenatal care; PNC, postnatal care; BFC, breastfeeding counselling.
†PNC clients only; ††All clients excluding PNC pre-intervention.
Experiences and perceptions of breastfeeding counselling
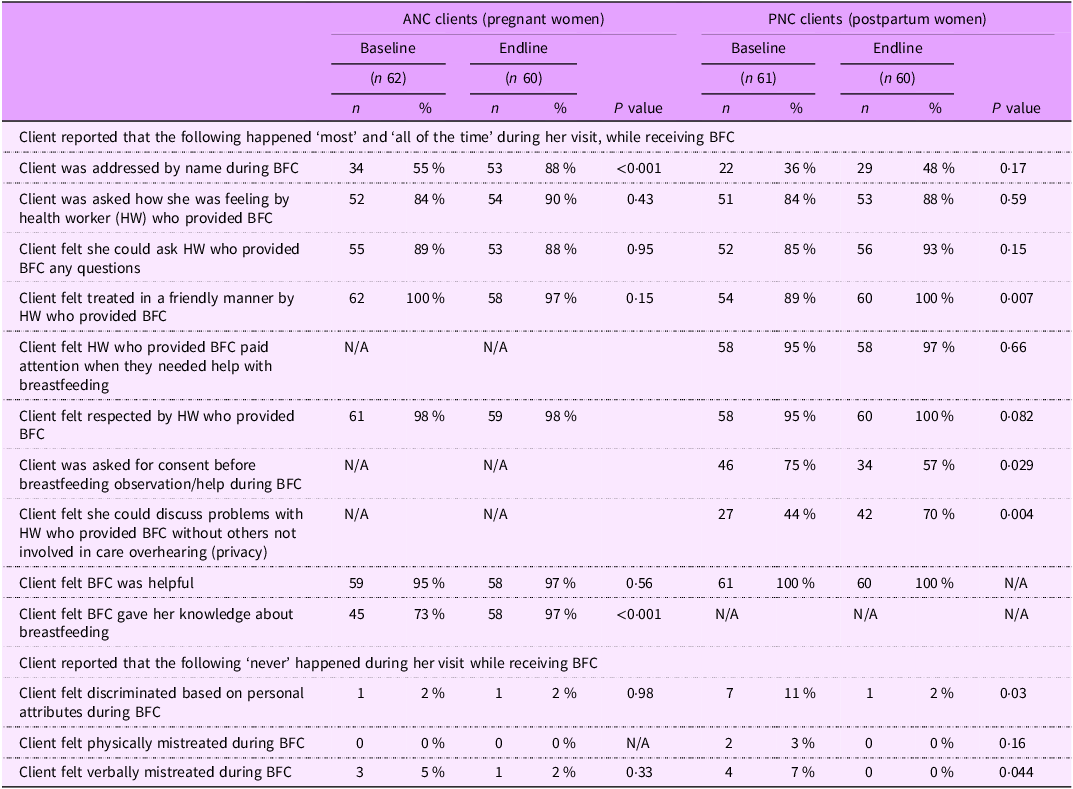
Most clients interviewed reported being treated in a friendly manner by the health worker(s) providing BFC and support at baseline and endline (Table 6). Among ANC clients, there was no statistically significant change; however, among PNC clients, the percentage increased from 89 % to 100 % (P = 0·007). Similarly, ANC and PNC clients reported feeling respected by the health workers providing BFC both before and after the programme. ANC clients were more likely to have been addressed by name at endline (88 %) than at baseline (55 %) (P < 0·001).
Pregnant and postpartum women’s perceptions of BFC, n (%)

Notes: We measured health worker practices during BFC, reported during client exit interviews using a Likert scale (no, never = 0; yes, some of the time = 1; yes, most of the time = 2; and yes, all of the time = 3) and converted into a binary outcome of either 1 = yes, all or most of time for positive statements or 1 = any yes for negative statements to simplify and reduce the response categories presented here. cccc PNC, postnatal care; BFC, breastfeeding counselling.
At baseline, only 3 % of PNC clients interviewed reported physical mistreatment by the health worker(s) providing BFC and support. None of the ANC or PNC clients reported physical mistreatment at endline. Among PNC clients, the percentage who reported verbal mistreatment declined (7 % baseline; 0 % endline, P = 0·04) as did the percentage who felt discriminated against based on personal attributes (from 11 % to 2 %, P = 0·03). More PNC clients indicated that they had privacy during BFC at endline (70 %) than at baseline (44 %) (P = 0·004). The percentage of PNC clients who reported health workers asking for consent before observing/helping with breastfeeding declined from 75 % at baseline to 57 % at endline (P = 0·029). Both ANC and PNC clients indicated that BFC was useful, and the percentage of ANC clients who felt that BFC gave them more knowledge increased from 73 % at baseline to 97 % at endline (P < 0·001).
Qualitative findings from focus group discussion and key informant interview
We identified several themes from the qualitative data collected through the FGD and KII. Key informants indicated that the mentorship programme was integrated with existing implementation of national guidelines on quality obstetrics and perinatal care(30) at the hospital, routine reporting, continuous medical education and continuous quality improvement. For example, strengthening monthly reporting on early initiation of breastfeeding by implementing skin-to-skin contact immediately after delivery aligns with mentorship programme goals to improve the quality of BFC and breastfeeding outcomes and immediate care of the newborn, a key action in the national guidelines.
Mentors and mentees were interested in participating to increase their knowledge and practices related to breastfeeding and improve maternal and child health. Mentors and mentees felt that gaining confidence to counsel caregivers on breastfeeding was one of the main positive outcomes. Health workers also mentioned strengthening foundational counselling skills, such as listening to and learning from the client. They perceived improvements in breastfeeding practices as well as maternal and child health outcomes and attributed them to the programme.
‘It has changed me. As I carry out my daily duties, I can assist a mother whose child is not breastfeeding well. The program has given me the ability to help such mothers, not only in the workplace but also outside my workplace. I can confidently implement the BFHI.’ (ANC Mentees FGD, health worker [HW] 2)
Mentees felt that mentors were well-qualified and could influence health workers.
‘[My mentor] was quite knowledgeable on what should be done. So whenever we faced some challenges, especially on the filling of the books and some scales, she could clarify how much is needed.’ (PNC Mentees FGD, HW 5)
They thought it was strategic to select departmental heads to serve as mentors.
‘Mentors were primarily chosen from among those who were already in charge of departments … this method was seen as strategic because it utilized existing hierarchies.’ (ANC Mentees FGD, HW 1)
Mentees generally viewed the selection and matching process positively, particularly the strategic use of existing leadership structures, merit-based selection and observations made during the trainings.
‘I think the process was strategic because by starting with the departmental heads those who were interacting with ANC and PNC, it gives them the leeway to spearhead the process and number two, when it comes to selecting the mentees the people working under them, I think it went well it is like trickling down effect down the chain.’ (ANC Mentees FGD, HW 2)
However, mentees noted that mentors’ other responsibilities made it hard to find time for mentoring and caused interruptions. Both mentors and mentees mentioned challenges scheduling meetings for debriefing, providing feedback or discussing issues. They noted that this was particularly challenging when mentors and mentees worked in different departments or had different work schedules.
‘A recurring issue was the lack of sufficient staff to handle the high volume of deliveries and have adequate time to provide breastfeeding counselling.’ (ANC Mentees FGD, HW 2)
‘My mentor is a nutritionist and I’m a nurse. The days that we’re supposed to meet, we find that we are in different shifts.’ (PNC Mentees FGD, HW 7)
Mentors and mentees were able to overcome these challenges by creating WhatsApp groups. The WhatsApp group served as a platform for ongoing support between face-to-face mentorship sessions, especially when scheduling conflicts arose due to different work shifts or departments. Mentees particularly valued the ability to receive real-time advice on complex cases through shared photos and descriptions. As one mentee noted.
‘For me I can say, it somehow went well. Despite the fact that we are different cadres, we were able to create a WhatsApp where we could do our meetings and communicate.’ (PNC Mentees FGD, HW 6)
Mentees appreciated the range of approaches used by mentors. Mentors expressed appreciation for the job aids guiding them, particularly when observing BFC sessions. Both mentees and mentors commented on the supportive approach that mentors took to providing feedback to mentees.
‘It was also helpful in that she would actually appreciate what you have done good, and later she would come up with what you could have done better. That encouraged us, gave us encouragement.’ (PNC Mentees FGD, HW 4)
Finally, mentees noted that the mentorship programme fostered relationships and teamwork across different cadres.
‘Teamwork, especially among health workers, nutritionists, nurses, and the administration, has really helped in the implementation of the program because if it was one cadre doing everything, it would not be successful as it is now. Because most of the cadres, we are now working together well.’ (PNC Mentees FGD, HW 1)
Factors that enabled and hindered implementation
Several factors enabled the implementation of the programme (Table 7). First and importantly, we designed the programme to be an integral part of health facility activities and implemented by staff. Second, health facility management had ownership of, support for and commitment to the study intervention. Leadership support for proposed changes in service delivery practices has been shown to be critical for engaging staff at all levels(Reference Wallen, Mitchell and Melnyk31). Third, conducting the BFHI training prior to the programme helped to ensure that mentees had the foundational knowledge of BFC prior to the programme. Fourth, mentors and mentees indicated they wanted to improve their knowledge and skills, women’s breastfeeding knowledge and practices and, ultimately, maternal and child health outcomes. Wallen and colleagues showed that believing in the importance of new practices contributes to their use. Mentors and mentees perceived improvements and attributed them to the programme, which seems to have motivated them to actively participate for the duration(Reference Wallen, Mitchell and Melnyk31). Fifth, mentors and mentees noted that mentors were well matched with mentees with whom they had a good rapport, who worked in the same department and/or were of the same cadre, thus ensuring compatibility, which is critical for successful implementation. Sixth, selecting trusted, well-respected and influential individuals as mentors and matching them with mentees with similar work schedules facilitated the implementation of the intervention and helped mentees be open to receiving feedback and suggestions for improvement. Seventh, mentors commented on the usefulness of the job aids, particularly the observation tools, which focussed on specific competencies related to mentees’ actions and skills and counselling checklists. Finally, mentors appreciated the programme’s versatility. Choosing the mentorship approach(es) that worked best for them and their mentees (i.e. in-person group, one-on-one, peer-to-peer or virtual meetings; demonstrations; observations; debriefs; teaching sessions and discussions) empowered mentors.
Enablers and barriers of the facility-based mentorship programme for BFC

BFC, breastfeeding counselling; ANC, antenatal care.
Nonetheless, there were challenges due to heavy workloads and conflicting work schedules. The former may be less of an issue in lower-level facilities not receiving a high number of referrals. The latter was mostly an issue when mentors were paired with mentees from different cadres.
Discussion
Mentorship programmes can improve the quality of maternal, neonatal and child healthcare services, including in resource-limited settings(Reference Anatole, Magge and Redditt22–Reference Green, de Azevedo and Patten24,Reference Manzi, Mugunga and Nyirazinyoye32) . Mentorship has also been found to influence mentee attitudes, interpersonal relations and motivation(Reference Melnyk, Fineout-Overholt and Feinstein25,Reference Wallen, Mitchell and Melnyk31,Reference Eby, Allen and Evans33) .
This feasibility study expands the evidence base by focusing on the feasibility of a mentorship programme for BFC. We determined whether the mentorship programme improved mentees’ knowledge and confidence to provide quality counselling and pregnant and postpartum women’s perceptions of BFC.
Mentees’ knowledge and confidence related to breastfeeding counselling
While mentees demonstrated high baseline knowledge (94 % correct) and confidence, which limited the potential for significant improvements across all indicators, it is noteworthy that significant change was observed specifically in mentees’ confidence in counselling women on breastfeeding and infant feeding (from 67 % at baseline to 95 % at endline, P = 0·014). The lack of statistically significant changes in other knowledge and confidence indicators should be interpreted in the context of already high baseline scores and the small sample size (n 21 at baseline, n 19 at endline). Rather than suggesting the programme had limited impact on knowledge(Reference Custers34–Reference Ventachalam, Kumar and Gupta36), these findings indicate that the mentorship approach may be most valuable for enhancing the capability to use a set of related knowledge, skills and behaviours to successfully provide BFC in a clinical setting.
Pregnant and postpartum women’s perceptions of breastfeeding counselling
Nearly all clients interviewed reported health workers treating them in a friendly manner and feeling respected before and after the mentorship programme. They did not report feeling discriminated against or experiencing physical or verbal mistreatment. Notably, we observed a significant decline among PNC clients who felt verbally mistreated and discriminated against based on personal attributes. This improvement in client treatment aligns with the FGD; mentees indicated increased empathy for clients. Finally, ANC and PNC clients’ perception of the usefulness of BFC increased over time.
A somewhat surprising finding was the decline in the percentage of PNC clients who reported health workers asking for consent before observing or helping with breastfeeding. This might have to do with (a) BFC becoming so integrated into services that health workers overlooked the need to ask each time and/or (b) enthusiasm to help women breastfeed might have led to health workers forgetting to ask for consent.
Study limitations
The study was conducted at a single health facility, limiting generalisability to other levels of care. Without a comparison group and purposive/convenient sampling, changes in mentee confidence and client-reported counselling cannot be definitively attributed to the mentorship programme. Our sample sizes were not large enough to detect moderate differences between baseline and endline. Exit interviews focused on satisfaction and measures of respective care rather than practices related to prioritised competencies. As a repeat cross-sectional design, there were some statistically significant differences between ANC and PNC client groups at baseline and endline. Overall, while suggestive, the lack of a comparison group limits definitive conclusions about the programme’s impact. A limitation of this feasibility study was the lack of data on breastfeeding outcomes such as initiation rates and exclusive breastfeeding rates at hospital discharge. Future evaluations of the facility-based BFC programme should include these metrics to assess the ultimate impact on breastfeeding practices.
Conclusions
The BFC mentorship programme was feasible when implemented as designed in a health facility with the requisite capacity to adapt it based on its existing infrastructure and supportive leadership.
As a next step, we recommend a series of carefully designed pilot studies implemented in a variety of settings (urban, rural), socio-economic environments and health facility types (public and private facilities, primary and secondary care facilities). These pilot studies will guide the next phase of implementation and enhance already existing efforts by respective county health departments implementing BFHI to achieve Step 2. Additionally, further research should assess the impact of the mentorship programme on breastfeeding practices among mothers in Kenya. This approach will provide valuable insights into the scalability and adaptability of the mentorship programme in different contexts and will ultimately contribute to improved BFC and breastfeeding outcomes.
Facility-based mentoring to strengthen BFC competencies is one potential approach for countries to achieve the second step of the BFHI ten steps. Based on study findings, implementation guidance(26) was revised to include: (1) updated BFHI competencies; (2) evidence of adaptability across facility levels; (3) enhanced mentor–mentee pairing and support mechanisms, including virtual options and (4) simplified competency assessment tools linked to various service points These evidence-informed refinements enhance the programme’s contextual adaptability whilst preserving fidelity to its foundational components, thus facilitating wider implementation across diverse healthcare settings.
Supplementary material
For supplementary material accompanying this paper, visit https://doi.org/10.1017/S1368980025100591
Authorship
The authors affirm that this manuscript titled ‘Breastfeeding counselling mentorship program feasibility: A mixed-methods study at Mbagathi County Referral Hospital, Nairobi, Kenya’ meets the authorship criteria set forth by the International Committee of Medical Journal Editors (ICMJE). All authors listed made contributions to the research and writing of the manuscript as follows: As the lead author, B.M.N. led the concept and design of the research, interpretation of data, drafting and revising the manuscript. Senior author: S.L. provided revisions to the data collection tools, review of analysis, summarising analysis data and revising the manuscript. Co-authors: Each co-author contributed to various aspects of the study, including research review, stakeholder engagement, data collection, data analysis, interpretation and preparation of the manuscript. All authors have participated sufficiently in this work to take responsibility for its content. Further, each author has reviewed and approved the final version of the manuscript and agrees to be accountable for all aspects of this work to ensure its integrity.
Financial support
The U.S. Agency for International Development (USAID) provided financial support for this article through its flagship multi-sectoral nutrition project, USAID Advancing Nutrition. It was prepared under the terms of contract 7200AA18C00070 awarded to JSI Research & Training Institute, Inc. (JSI). The contents are the responsibility of JSI and do not necessarily reflect the views of USAID or the U.S. Government. Additional support for this article is made possible by the generous support of the American people through USAID under the terms of the Cooperative Agreement #7200AA20CA00002, led by Jhpiego and partners.
Competing interests
The authors report no conflicts of interest.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Kenya Medical Research Institute Scientific Ethics Review Unit as Protocol Number – Non KEMRI 4607. Written and informed consent was obtained from all subjects/patients.







 Open access
Open access