



Introduction
Malnutrition remains a major public health challenge, particularly in low- and middle-income countries (LMICs)(Reference Kerac, James, McGrath, Brennan, Cole and Opondo1), where it contributes to nearly half of all deaths in children under five years of age(2). The World Health Organization (WHO) categorises malnutrition as undernutrition (wasting, stunting, underweight), micronutrient deficiencies, and overnutrition(2). In 2023, an estimated 148 million children under five years were stunted and 45 million were wasted, with long-term consequences including impaired cognitive development(Reference Kirolos, Goyheneix, Kalmus Eliasz, Chisala, Lissauer and Gladstone3), reduced school performance, increased susceptibility to infections(Reference Al Amad, Al-Eryani, Al Serouri and Khader4–7), and later-life non-communicable disease risk(Reference Grey, Gonzales, Abera, Lelijveld, Thompson and Berhane8). Despite global commitments through the United Nations’ Sustainable Development Goals (SDGs) to end all forms of malnutrition by 2030, progress remains slow(Reference Al Amad, Al-Eryani, Al Serouri and Khader4).
Infants under six months (u6m) are especially vulnerable due to their dependence on breastfeeding, immature physiology, and susceptibility to infections. In LMICs, around 10.3 million children are underweight, including 4.1 million who are severely underweight; and 9.2 million are wasted, including 4.0 million who are severely wasted. Also, 11.8 million children are shorter than the standard height of similar age group children(Reference Kumar, Meiyappan, Rogers, Rogers, Daniel and Sinha9). Mortality risk is disproportionately higher in malnourished infants u6m compared with older children(Reference Kumar, Meiyappan, Rogers, Rogers, Daniel and Sinha9,Reference Grijalva-Eternod, Kerac, McGrath, Wilkinson, Hirsch and Delchevalerie10) , yet this group has historically been neglected in nutrition programmes and prevalence estimates(Reference McGrath11). Breastfeeding disruptions, poor maternal health, and sociocultural practices further exacerbate vulnerability(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12–Reference Rollins, Bhandari, Hajeebhoy, Horton, Lutter and Martines14).
Traditionally, infants with severe acute malnutrition (SAM) have been managed in inpatient settings. While effective for complicated cases, inpatient care is costly, inaccessible for many families, and often associated with low adherence(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference Kerac, Frison, Connell, Page and McGrath15,Reference Jibat, Rana, Negesse, Abera, Abdissa and Girma16) . In response, community-based management of acute malnutrition (CMAM) was developed, enabling outpatient care for clinically stable children without complications(Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13,Reference Grijalva-Eternod, Beaumont, Rana, Abate, Barthrop and McGrath17) . Recognising the need to include younger infants, the 2013 WHO guidelines were the first to include this age group(18), highlighting breastfeeding support, maternal care, and regular growth monitoring(Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13,Reference Grijalva-Eternod, Beaumont, Rana, Abate, Barthrop and McGrath17) . The updated 2023 WHO guidelines recommended greater emphasis on comprehensive, integrated, and flexible care of this age group, including early detection and structured management for inpatient and outpatient care depending on clinical need, to ensure survival, growth, and health development(2).
To address the unique needs of this age group, the Management of Acute Malnutrition in Infants under 6 Months (MAMI) initiative was launched in 2008(19), with the MAMI Care Pathway providing outpatient care strategies tailored to both mother and infant(19). This approach aims to bridge the gap between neonatal services and outpatient care for older children. However, evidence on the effectiveness, feasibility, and scalability of community-based interventions for infants u6m remains ‘low’ or ‘very low’, heterogeneous, and context-dependent, factors which are also acknowledged by the new 2023 WHO guidelines(2,Reference Munirul Islam, Arafat, Connell, Mothabbir, McGrath and Berkley5,Reference Moore, O’Mahony, Shevlin, Hyland, Barthorp and Vallières20) .
Given the scarcity of high-quality evidence and the vulnerability of this population, evidence syntheses are essential to guide policy and practice. While much research has focused on children over six months, comparatively little is known about outpatient and community-based care for younger infants.
This review maps existing research related to the outpatient and community-based management of malnourished infants u6m to identify knowledge gaps and inform practice and policy. The objectives guiding this scoping review are as follows:
-
• To describe the range and characteristics of existing literature on outpatient and community-based management approaches for this population.
-
• To summarise the reported interventions and strategies, including nutritional, breastfeeding, and maternal health support.
-
• To outline the available guidelines, tools, and resources to support outpatient and community-based management for practitioners and policymakers.
-
• To compile reported barriers, facilitators, and stakeholder perceptions related to implementing such interventions.
Methods
Study design
This scoping review synthesised evidence on outpatient and community-based management of malnutrition in infants u6m. The review followed the methodological framework of the Joanna Briggs Institute (JBI) for evidence synthesis(Reference Peters, Godfrey, McInerney, Munn, Tricco and Khalil21) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Review (PRISMA-ScR) guidelines(Reference Tricco, Lillie, Zarin, O’brien, Colquhoun and Levac22). A completed PRISMA-ScR checklist is provided as online Supplementary material 1. The protocol was prospectively registered in the Open Science Framework (https://osf.io/kq48y).
Eligibility criteria
This scoping review considered malnutrition as undernutrition, including wasting, stunting, and underweight, to maintain consistency with terminology across the included studies. Broader WHO terminology such as ‘at-risk of poor growth and development’ was not included to avoid reporting inconsistency and data limitation for this age group.
Studies were eligible if they:
-
• Included malnourished infants u6m or mother–infant dyads.
-
• Mentioned nutrition intervention set up in outpatient or community-based settings (e.g., nutritional screening and support, breastfeeding counselling, outpatient consultations); or included stakeholders’ perceptions and reflections about current outpatient or community-based treatment procedures, readily available tools, guidelines, or training materials to manage malnutrition of this age group.
-
• Were published between 2007 (just before the launch of the MAMI initiative in 2008) and August 2025.
-
• Were available in English.
Exclusion criteria were inpatient-only management, studies on infants older than six months, interventions not targeting malnutrition, or publications outside the defined time period and/or in a language other than English.
Search strategy
A comprehensive search was conducted in PubMed, Web of Science, CINAHL, and Google Scholar, supplemented by grey literature including institutional websites (WHO, UNICEF, ENN, CDC, FAO, and the Scaling Up Nutrition (SUN) network). Search terms included: ‘infants under six months’, ‘MAMI’, ‘CMAMI’, ‘outpatient management’, ‘community-based care’, ‘malnutrition’, and ‘undernutrition’. The updated search was conducted between 23 August 2025 and 31 August 2025. All suggested studies were also rescreened against our predefined eligibility criteria on 20 February 2026. Search strategies were adapted for each database and checked against reference lists of included papers. Both old and new search results for different databases have been provided as online Supplementary material 2.
Study selection
After the database searches, all the search records were managed with Rayyans Qatar Computing Research Institute (QCRI) software, a web-based online tool for managing and reporting systematic reviews and meta-analyses(Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid23) for duplicate removal and screening. After duplicate removal, two reviewers (M.H.A.M. and N.A.C.) independently screened titles and abstracts, followed by full-text review of potentially eligible studies against the inclusion criteria. Discrepancies were resolved by discussion with a third reviewer (R.C.-D.).
Data extraction
Data were extracted into a pre-piloted structured Microsoft Excel form, capturing study characteristics, design, population, intervention details (setting, admission/discharge criteria, feeding protocols), and reported outcomes (anthropometry, feeding practices, feasibility, and acceptability).
Data synthesis
As the eligible studies were heterogeneous in measurements of variables, study design, and reporting, we followed the descriptive and narrative synthesis method to report the key characteristics and findings of the included studies. We mapped the studies and structured the findings around the review objectives: (a) study design, (b) characteristics and scope of available literature, (c) setting or context, (d) geographic region, (e) admission and discharge criteria, (f) type of interventions or tool, (g) reported challenges or facilitators to implementation, and (h) policy and programmatic implementation.
Results
Study selection
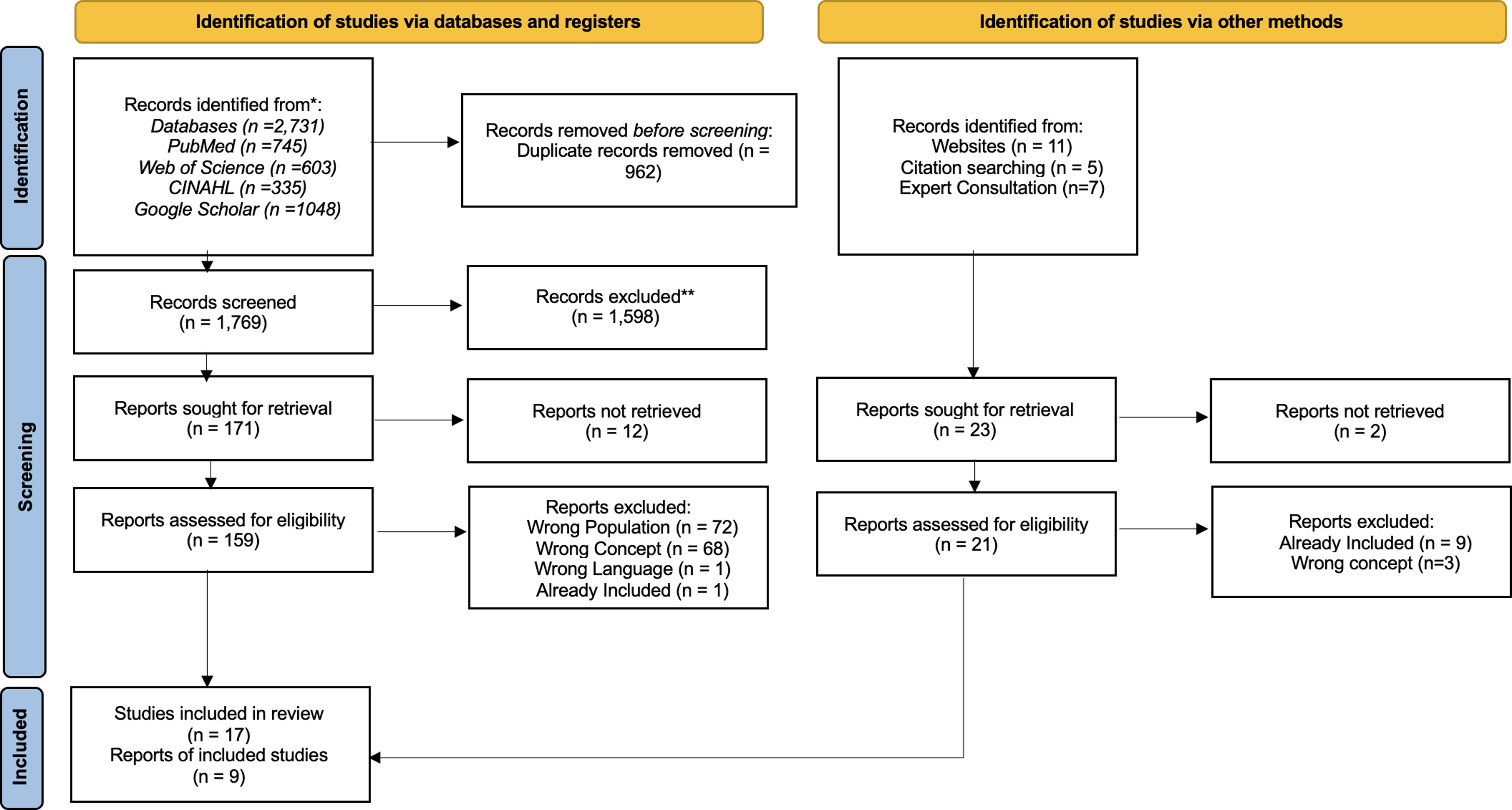
The search identified 2,754 records across databases, websites, expert consultation, and citation searching. After removal of 962 duplicates, 1,769 titles/abstract were screened, with 159 full texts assessed. Seventeen studies met inclusion criteria, and nine additional documents were retrieved from grey literature, including institutional websites and expert consultation, resulting in 26 studies included in the review. Fourteen potentially relevant papers could not be accessed in full. Reasons for exclusion were: wrong population (n = 72), wrong concept (n = 71), wrong language (n = 1), and duplication (n = 1). The PRISMA 2020 flow diagram summarises the process (Figure 1).
PRISMA flow diagram illustrating the study selection process for the review of outpatient and community-based management of malnourished infants under six months.

Characteristics of included studies
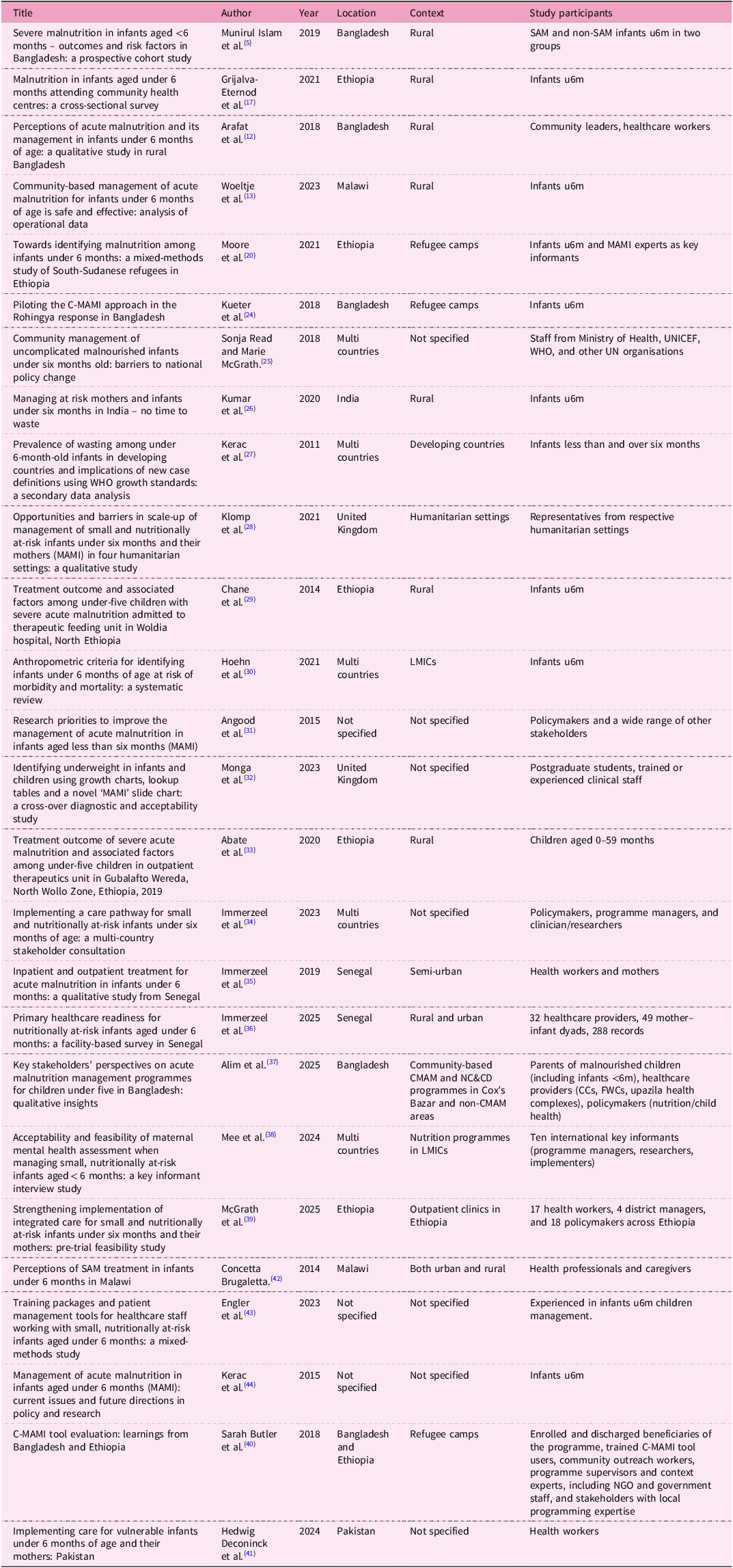
The included studies and reports were published between 2011 and 2025, with only four appearing after the latest 2023 WHO guidelines emphasising integrated management of infants u6m. Geographically, sub-Saharan Africa and South Asia dominated the evidence base, with limited data from Latin America, the Middle East, and Southeast Asia(Reference Munirul Islam, Arafat, Connell, Mothabbir, McGrath and Berkley5,Reference Grijalva-Eternod, Kerac, McGrath, Wilkinson, Hirsch and Delchevalerie10,Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13,Reference Moore, O’Mahony, Shevlin, Hyland, Barthorp and Vallières20,Reference Kueter, Burrell, Butler, Sarwar and Rahman24–Reference Kerac, Mwangome, McGrath, Haider and Berkley44) .
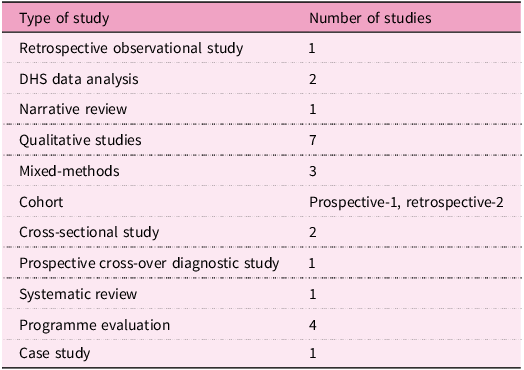
Study designs were heterogeneous. Qualitative studies (n = 7) were most common, followed by programme case studies (n = 4), mixed-methods (n = 3), and cohort studies (n = 3). Other designs included cross-sectional surveys, retrospective analyses, and systematic reviews (Table 1). This distribution highlights the limited availability of robust intervention trials. Table 2 illustrates the basic characteristics of included evidence, and details are presented in online Supplementary material 3.
Study designs represented in included literature

Basic features of included evidence

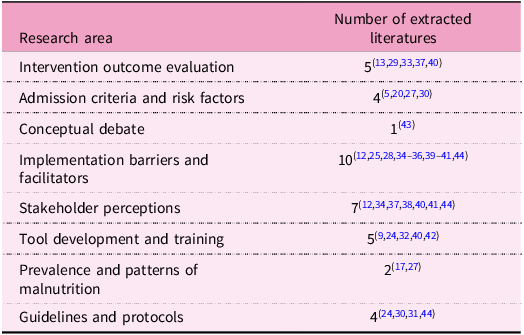
The included studies addressed a wide range of research foci, with the most common, almost half, being implementation challenges and stakeholder perceptions (n = 13), while relatively few evaluated intervention outcomes (n = 4) or examined admission criteria and risk identification (n = 4). A full thematic categorisation of study research foci is available in Table 3, where some studies contributed to more than one research focus category.
Distribution of included studies by research focus area

Intervention strategies and outcomes
Interventions are shifting away from hospitals toward outpatient and community settings, guided by protocols such as the MAMI Care Pathway, in line with the WHO’s 2023 recommendations(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36,Reference Mee, Abera and Kerac38,Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39) . The most common interventions were the provision of nutritional supplements, including ready-to-use therapeutic foods (RUTF), ready-to-use supplementary foods (RUSF), and fortified cereals, alongside breastfeeding support and maternal health. RUTF, RUSF, and fortified cereals were given to individual cases when no other feasible options were available and were considered a very special situation; exclusive breastfeeding is still the key public health recommendation for this age group(Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13). In Bangladesh and Senegal, health workers and caregivers believe re-lactation and the supplementary suckling technique (SST) were generally acceptable, although these findings are based on perceptions rather than direct measurement of outcomes(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference van Immerzeel, Camara, Deme Ly and de Jong35) . In Senegal, primary healthcare centres were moderately prepared to manage malnourished infants (overall 70%), but readiness for infants u6m was much lower (38%), according to the latest WHO 2023 guidelines recommendation. Assessment, classification, and treatment were limited, though routine visits such as postnatal checkups and immunisations provided opportunities to enhance care(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36).
Research across several countries included maternal mental health screenings, which were discussed as beneficial for maternal wellbeing and mother–infant interactions, and, indirectly, the baby’s growth(Reference Mee, Abera and Kerac38). In Bangladesh, community-based acute malnutrition management with nutrition counselling, child development support, and nutrient-rich foods were associated with reported improvements in recovery rate, weight gain, feeding habits, and growth(Reference Alim, Munirul Islam, Guesdon, Anik, Antoine and Marium37). Meanwhile, a study in Ethiopia reported that implementation of the MAMI Care Pathway was associated with improved breastfeeding, growth monitoring, and perceived reduction in hospital burden(Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39).
Some studies reported outpatient care as a potential viable therapeutic option for malnourished infants u6m. In Malawi, a 79% recovery rate was reported using nutritional supplements, though infant-specific doses were not detailed(Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13). In Ethiopia, Abate et al.(Reference Abate, Tilahun, Kassie and Kassaw33) saw a 65% recovery rate in outpatient settings, though coexisting illnesses made recovery harder(Reference Abate, Tilahun, Kassie and Kassaw33). A study in Bangladesh showed that 75% of infants reached catch-up growth with only minimal intervention, but a quarter still remained malnourished at six months(Reference Munirul Islam, Arafat, Connell, Mothabbir, McGrath and Berkley5). Online supplementary material 3 summarises the included literature.
Risk factors for malnutrition and recovery
Across various studies, several key risk factors for malnutrition were mentioned(Reference Kerac, Frison, Connell, Page and McGrath15,Reference Kerac, Ashorn, Berkley, Borg, Castro and Deconinck45) . Moore et al. reported that weight loss, faltering growth, and a mid-upper arm circumference (MUAC) under 115 mm were useful indicators for identifying malnutrition(Reference Moore, O’Mahony, Shevlin, Hyland, Barthorp and Vallières20). Similarly, Munirul Islam et al. highlighted the crucial role of maternal health, showing clear links between low maternal body mass index (BMI) and poor infant nutrition(Reference Munirul Islam, Arafat, Connell, Mothabbir, McGrath and Berkley5).
Challenges to appropriate treatment included poor identification and treatment of at-risk infants – only 15% were properly classified in Senegal, for example – and maternal mental health issues harming mother–infant interactions and growth. In Ethiopia, unmet maternal–infant needs and socioeconomic hardships made the situation worse(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36,Reference Mee, Abera and Kerac38,Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39) .
When it came to recovery, access to integrated nutrition counselling and micronutrient supplementation were identified as contributing factors in Bangladesh. Yet progress was often slowed by limited health services and hidden burdens of care(Reference Alim, Munirul Islam, Guesdon, Anik, Antoine and Marium37,Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39) . On the positive side, consistent monitoring, support for maternal mental health, and community-based follow-up were described to be associated with improved recovery rates and reduced caregivers’ burden in some settings(Reference Mee, Abera and Kerac38,Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39) .
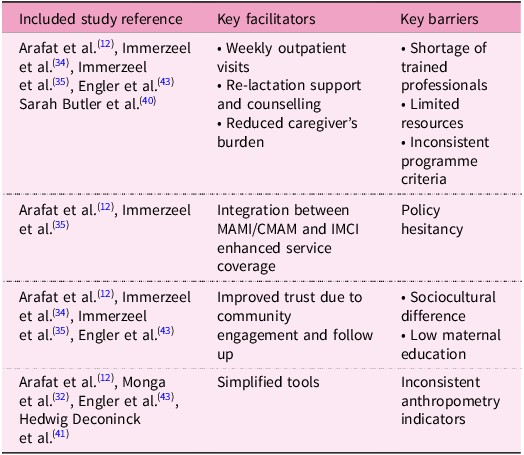
Facilitators and barriers
Reported enablers of successful outpatient care included the convenience of weekly visits, reduced caregiver costs, and integration with existing child health services(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference van Immerzeel, Diagne, Deme/Ly, Murungi, Diouf and Kerac34,Reference van Immerzeel, Camara, Deme Ly and de Jong35) . Community engagement and follow-up improved adherence, while re-lactation support and home-based breastfeeding counselling strengthened maternal–infant bonding(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference van Immerzeel, Diagne, Deme/Ly, Murungi, Diouf and Kerac34,Reference van Immerzeel, Camara, Deme Ly and de Jong35) . Integration of the MAMI Care Pathway with the Integrated Management of Childhood Illness (IMCI) framework was also considered a strategy to improve coverage(Reference van Immerzeel, Diagne, Deme/Ly, Murungi, Diouf and Kerac34). Additional facilitators included policy alignment (e.g., with national guidelines in Ethiopia), non-governmental organisation (NGO) support and incentives (in Bangladesh), task-shifting and community networks (multi-country), and strong infrastructure at routine contact points (in Senegal)(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36–Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39). Contextual adaptation and professional motivation were also noted as enablers(Reference Alim, Munirul Islam, Guesdon, Anik, Antoine and Marium37,Reference Mee, Abera and Kerac38) .
Reported barriers included limited availability of trained health workers, inconsistent admission and discharge criteria, high caseloads, and inadequate facility space and resources(Reference Kueter, Burrell, Butler, Sarwar and Rahman24,Reference Read and McGrath25,Reference Klomp, Kerac and Dyment28) . Sociocultural barriers, such as maternal education level, food-sharing practices, and gender dynamics, also hindered adherence(Reference Klomp, Kerac and Dyment28). Policymakers often hesitated to recognise differences between complicated and uncomplicated cases, limiting adoption of outpatient care and favouring inpatient treatment(Reference Read and McGrath25). Additional barriers encompassed workforce shortages, training deficits, inconsistent equipment/supplies, stigma around maternal mental health, time/financial constraints for families, and ethical issues such as screening without referral capacity(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36–Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39). Table 4 highlights the key facilitators and barriers.
Summary of described facilitators and barriers in outpatient/community management of infants u6m

Perceptions and acceptability
Caregivers and community members generally perceived outpatient care as more accessible and less costly than hospitalisation(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference Brugaletta42) . Mothers reported that home-based care strengthened maternal–infant bonding and improved acceptance of re-lactation techniques(Reference van Immerzeel, Camara, Deme Ly and de Jong35). Health workers acknowledged feasibility but expressed concerns about insufficient training, particularly in breastfeeding counselling and maternal psychosocial support(Reference Kueter, Burrell, Butler, Sarwar and Rahman24,Reference Kumar, Deb, de Wagt, Gupta, Bhandari and Sareen26) . Policymakers’ views were mixed; while many acknowledged the need for alternatives to inpatient management, reluctance stemmed from uncertainties around specific measurement cut-off points and resource shortages(Reference Read and McGrath25,Reference Klomp, Kerac and Dyment28) .
Tools, training, and protocols
Specialised tools gained focus, with the C-MAMI package being the only standardised tool for infants u6m described in a study, though its implementation varied across settings(Reference Engler, McGrath and Kerac43). Another study reported that the MAMI slide chart had 79% diagnostic accuracy, higher than traditional charts at 61%, and was preferred by health workers, though more real-world testing is needed(Reference Monga, Sikorski, de Silva, McGrath and Kerac32).
Protocols followed WHO 2023 guidelines and the MAMI clinical care pathway, often alongside plans such as IMNCI/ICCM in Ethiopia and CMAM plus nutrition programmes in Bangladesh(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36–Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39). The tools also included screenings for maternal mental health in multiple countries, alongside providing specialised foods and micronutrients(Reference Alim, Munirul Islam, Guesdon, Anik, Antoine and Marium37,Reference Mee, Abera and Kerac38) .
However, training gaps were a common issue, especially when it came to breastfeeding support and psychosocial care for mothers(Reference Kueter, Burrell, Butler, Sarwar and Rahman24,Reference Kumar, Deb, de Wagt, Gupta, Bhandari and Sareen26) . These shortages extended more broadly – for instance, in Senegal there was notably low readiness, highlighting an urgent need to build capacity in using equipment and enhancing the skills of health workers(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36). While task-shifting to less specialised staff and aid from NGOs helped to support implementation, challenges such as limited supplies and staffing shortages often made it hard to fully follow protocols(Reference Alim, Munirul Islam, Guesdon, Anik, Antoine and Marium37–Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39).
Guidelines and policy perspectives
Identified literature revealed ongoing discussions about the best criteria for admitting and discharging patients in malnutrition programmes. Although WHO growth standards and weight-for-length Z-scores (WLZ) are still widely used, some studies suggested that MUAC could be a simpler alternative, though it needs more validation(Reference Kerac, Blencowe, Grijalva-Eternod, McGrath, Shoham and Cole27,Reference Hoehn, Lelijveld, Mwangome, Berkley, McGrath and Kerac30,Reference Kerac, Mwangome, McGrath, Haider and Berkley44) . Moreover, weight-for-age Z-scores (WAZ) are also widely used as a criterion of interest because of their ability to identify high-risk infants compared to WLZ(Reference Hoehn, Lelijveld, Mwangome, Berkley, McGrath and Kerac30). In various settings, policymakers expressed concerns about whether outpatient care is practical without a clearer global consensus and stronger evidence to back it up(Reference Read and McGrath25,Reference Klomp, Kerac and Dyment28) .
The WHO 2023 guidelines and MAMI Care Pathway, supporting outpatient care and mother–infant pairs, align with policies in Ethiopia and offer cost-effective integration(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36–Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39). However, challenges include limited capacity in Senegal, governance issues in several countries, and workforce shortages requiring local adaptation in Bangladesh(Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36–Reference Mee, Abera and Kerac38). Policymakers stressed the importance of advocating for integrated strategies to address the unmet needs within routine health services(Reference Alim, Munirul Islam, Guesdon, Anik, Antoine and Marium37,Reference McGrath, Girma, Berhane, Abera, Hailu and Bathrop39) .
Synthesis of findings
Across diverse contexts, several consistent patterns emerged. Outpatient and community-based management was described as feasible and acceptable across different contexts. Breastfeeding support, maternal health, and culturally adapted interventions were frequently identified as important components of reported programmes. Tools such as the MAMI clinical care pathway, MUAC, and the MAMI slide chart (a WAZ look-up chart) showed promise for programmatic use, though further validation and contextual testing is needed. Persistent barriers included limited health system capacity, inconsistent protocols, and policy hesitancy. Collectively, the findings suggest that, while outpatient management of malnourished infants u6m is promising, broader adoption will require stronger evidence, standardised guidelines, and integration into national health systems.
Discussion
Principal findings
This review summarised 26 studies on outpatient and community-based care for malnourished infants u6m. Despite more research following the WHO 2023 guidelines, there is still insufficient evidence to establish specific treatment protocols or clear admission and discharge criteria. Key details like feeding doses, follow-up schedules, and intervention outcomes remain underreported, limiting broad acceptance across contexts. Despite methodological heterogeneity, consistent themes emerged across identified literature. Outpatient care was described as feasible and acceptable to caregivers in multiple contexts(Reference Munirul Islam, Arafat, Connell, Mothabbir, McGrath and Berkley5,Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13,Reference Chane, Oljira and Atomesa29,Reference Abate, Tilahun, Kassie and Kassaw33,Reference van Immerzeel, Camara, Deme Ly and de Jong35,Reference Alim, Marium, Guesdon, Islam, Antoine and Anik46) . Breastfeeding support, maternal health interventions, and culturally tailored strategies were frequently highlighted as vital components of reported programmes(Reference Arafat, Islam, Connell, Mothabbir, McGrath and Berkley12,Reference Kumar, Deb, de Wagt, Gupta, Bhandari and Sareen26,Reference van Immerzeel, Diagne, Deme/Ly, Murungi, Diouf and Kerac34,Reference van Immerzeel, Camara, Deme Ly and de Jong35,Reference Mee, Abera and Kerac38,Reference Alim, Marium, Guesdon, Islam, Antoine and Anik46) . While re-lactation and SST are often conveyed as acceptable, the available evidence is largely based on caregiver and health worker views rather than direct evaluation of practice outcomes. Implementation in real-world settings may be more challenging, as mentioned in previous studies(Reference Lelijveld, Mahebere-Chirambo and Kerac47). Innovative tools such as the MAMI clinical care pathway, MUAC, and the MAMI slide chart were reported as potentially useful for detecting at-risk infants; MUAC and WAZ are both recognised by the WHO 2023 guidelines, though further validation and contextual testing is required(2,Reference Moore, O’Mahony, Shevlin, Hyland, Barthorp and Vallières20,Reference Kerac, Blencowe, Grijalva-Eternod, McGrath, Shoham and Cole27,Reference Hoehn, Lelijveld, Mwangome, Berkley, McGrath and Kerac30,Reference Monga, Sikorski, de Silva, McGrath and Kerac32) . Also, a new clinical care pathway for the management of small and nutritionally at-risk infants aged under six months and their mothers is currently being tested in a randomised controlled trial (RCT)(Reference Kerac48). However, major barriers included weak health system capacity, inconsistent admission/discharge protocols, and policy hesitancy, particularly in resource-constrained settings(Reference Kueter, Burrell, Butler, Sarwar and Rahman24,Reference Read and McGrath25,Reference Klomp, Kerac and Dyment28,Reference Van Immerzeel, Deme-Ly, Diagne-Camara, Penzias, Seck and Diallo36) .
Comparison with existing literature
These findings align with previous evidence that highlighted the vulnerability of infants u6m and the historical neglect of this age group in nutrition programming(2,Reference McGrath11,Reference Kerac, Mwangome, McGrath, Haider and Berkley44) . The 2023 WHO guidelines highlight that infants u6m remain a vulnerable group, with limited evidence on outpatient and community-based management(Reference Kerac, Ashorn, Berkley, Borg, Castro and Deconinck45). Our review complements these findings by mapping current interventions, tools, and stakeholder perspectives, and similarly identifies gaps in implementation, standardisation, and geographic coverage. The central role of breastfeeding support echoes WHO recommendations, which emphasise exclusive breastfeeding and maternal wellbeing as first-line interventions(2,Reference Woeltje, Evanoff, Helmink, Culbertson, Maleta and Manary13,Reference Grijalva-Eternod, Beaumont, Rana, Abate, Barthrop and McGrath17) . At the same time, the debate over anthropometric indicators remains unresolved. While WLZ continues to be widely used to predict the mortality at infant and child level, multiple studies argued for WAZ and MUAC as simpler alternatives(Reference Moore, O’Mahony, Shevlin, Hyland, Barthorp and Vallières20,Reference Kerac, Blencowe, Grijalva-Eternod, McGrath, Shoham and Cole27,Reference Hoehn, Lelijveld, Mwangome, Berkley, McGrath and Kerac30,Reference Kerac, Mwangome, McGrath, Haider and Berkley44,Reference Ahmed, Ali, Argaw, Bahl, Bailey and Baqui49) . This reflects broader discussions in the global nutrition community and addressed the 2023 WHO guidelines about how best to identify infants at highest risk of mortality(2). A recent study also highlights key evidence gaps in the management of infants u6m, reinforcing the need for further research on interventions, tools, and implementation strategies.
While CMAM is well applied for older children, evidence for infants u6m is limited and mostly from Africa and South Asia, leaving gaps in Latin America, the Middle East, and Southeast Asia that affect global guidance.
Strengths and limitations
This is, to our knowledge, the first review to consolidate global evidence on outpatient and community-based care for malnourished infants u6m. Strengths include a comprehensive search strategy across a wide range of databases and grey literature, protocol registration, and adherence to PRISMA standards. Inclusion of diverse study types also allowed mapping of both implementation experiences and policy perspectives.
Several limitations should be acknowledged. The search strategy focused on ‘malnutrition’ and ‘undernutrition’, which may have resulted in the potential exclusion of infants classified as at-risk according to the new, broader WHO definition. Also, the possibility of missing studies addressing early risk factors and the findings should be interpreted within the context of clinically endorsed malnutrition. Restricting to English-language publications may have excluded relevant evidence from francophone Africa, Latin America, and Asia. The lack of critical appraisal of study quality, consistent with scoping methodology, means that the strength of evidence could not be assessed. Considerable heterogeneity in interventions, outcomes, and reporting limited comparability and precluded meta-analysis. Finally, several potentially relevant documents could not be accessed in full.
Policy and practice implications
Despite these limitations, the review highlights several important lessons. First, outpatient and community-based management were repeatedly described as more accessible and acceptable to the caregivers, provided adequate support is in place. Integrating breastfeeding counselling, maternal health services, and psychosocial support into outpatient care is essential to optimise outcomes. Second, tools such as MUAC and the MAMI slide chart may offer opportunities to simplify case identification; however, the WHO 2023 guidelines renamed this age group as ‘infants at risk of poor growth and development’ and advised considering various indicators besides anthropometry such as WAZ < 2SD, WLZ < 2SD, and MUAC < 110 from six weeks to six months old for identification(2). Third, programmatic implementation may benefit from clear admission/discharge criteria, sufficient training for frontline workers, and adaptation to cultural contexts.
From a policy perspective, reluctance among some governments to adopt outpatient management underscores the need for stronger evidence and clearer global consensus. Alignment between WHO guidelines, national policies, and field implementation will be critical. In particular, recent 2023 WHO recommendations on managing ‘at-risk’ infants u6m provide a timely opportunity to harmonise protocols, build confidence among policymakers, and scale up proven approaches(Reference McGrath11).
Research priorities
Future research should focus on robust implementation studies and pragmatic trials to generate high-quality evidence. Context-specific validation and testing of MUAC cut-offs and diagnostic tools are urgently needed, particularly in humanitarian settings. Development and testing of specialised nutritional products for infants u6m may also be warranted. Equally important are policy-focused studies that address barriers to scale up and explore strategies for integrating MAMI pathways into routine health systems. These priorities align with recent WHO guidance, which emphasises implementation research to explore feasibility, acceptability, and stakeholder perspectives in this vulnerable population.
Conclusions
Outpatient and community-based care for malnourished infants u6m is a promising alternative to inpatient treatment. Evidence to date suggests it is feasible and acceptable in several contexts, although robust evidence on effectiveness remains limited, particularly when breastfeeding and maternal health are prioritised. However, widespread adoption requires stronger evidence, validated diagnostic tools, and integration into national policies and health systems. Addressing these gaps will be essential to reduce mortality and improve long-term outcomes for this highly vulnerable population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954422426100419.
Acknowledgements
The authors thank the University of Oviedo and Karolinska Institute for academic support during the conduct of this review, especially the experienced librarians for helping to finalise the search strategy. The authors used LLM for ensuring linguistic clarity and overall structure buildup.
Financial support
This work was supported by an Erasmus Mundus scholarship awarded to M.H.A.M. by the European Education and Culture Executive Agency (European Commission) for the Erasmus Mundus Master’s Course in Public Health and Disasters at the University of Oviedo.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Authorship
All authors contributed to the ideation and design. Conceptualisation, methodology, screening, and data extraction were performed by M.H.A.M. and N.A.C. Formal analysis, visualisation, and the first draft of the manuscript were undertaken by M.H.A.M. All authors wrote, reviewed, and edited the manuscript, with R.C.-D. in overall supervision.
Ethical standards
As a scoping review, this study considers secondary data already published, and therefore ethical approval was not necessary for its completion.
Patient and public involvement statement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.



 Open access
Open access