Statement of Research Significance
Research Question(s) or Topic(s): Do anxiety/stress, depression, and posttraumatic stress disorder (PTSD) make unique contributions to negative metacognitive bias in cognitive abilities? Main Findings: In 601 veterans, greater negative metacognitive bias correlated with all three symptom domains, but only anxiety/stress (β = −.29) and depression (β = −.12) explained unique variance at time 1; PTSD did not. Over 2 years (n = 239), symptom changes in anxiety/stress (β = −.33) and PTSD (β = −.16) uniquely tracked changes in bias, whereas depressive symptom changes did not. Study Contributions: Anxiety/stress is the most consistent correlate of cognitive underconfidence, underscoring the need to assess both self-report and objective cognition and to consider their discrepancy in clinical decision-making. Next steps include testing whether metacognitive bias-targeted interventions (e.g., feedback-based cognitive training, metacognitive therapy) reduce bias and improve clinical outcomes. Also, future ecological momentary assessment studies would be useful to clarify temporal pathways between metacognitive bias and anxiety/stress.
Metacognition is broadly defined as thinking about one’s own thinking (Dunlosky & Metcalfe, Reference Dunlosky and Metcalfe2008) and one key aspect of metacognition is awareness of one’s abilities and performance (Schraw, Reference Schraw1998). Accurate metacognitive awareness can help with effectively navigating challenges and making the most of one’s abilities and is associated with improved outcomes (e.g., in adults with brain injury, Yeo et al., Reference Yeo, Pestell, Bucks, Allanson and Weinborn2021; in psychosis, Davies et al., Reference Davies, Fowler and Greenwood2017). Negative metacognitive bias, that is, underconfidence, has been associated with several types of clinical psychopathology, including depression (Fu et al., Reference Fu, Koutstaal, Poon and Cleare2012; Petersen et al., Reference Petersen, Porter and Miskowiak2019), anxiety (Hoven et al., Reference Hoven, Luigjes, Denys, Rouault and van Holst2023), and posttraumatic stress disorder (PTSD, Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023). For example, individuals with elevated depressive, anxiety, and PTSD symptoms have consistently shown to have more negative metacognitive bias as measured by the difference between subjective and objectiveFootnote 1 cognitive abilities. This has been found using both local, task-based measures (for a review, see Hoven et al., Reference Hoven, Lebreton, Engelmann, Denys, Luigjes and van Holst2019) and more global ability measures (Petersen et al., Reference Petersen, Porter and Miskowiak2019; Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023; Agnoli et al., Reference Agnoli, Mahncke, Grant, Goodman, Milberg, Esterman and DeGutis2024; Rouault et al., Reference Rouault, Will, Fleming and Dolan2022). It has been suggested that these deficits are either driven by a common anxious-depression factor (e.g., Rouault et al., Reference Rouault, Seow, Gillan and Fleming2018) or primarily by depressive symptoms (Petersen et al., Reference Petersen, Porter and Miskowiak2019; Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023; Agnoli et al., Reference Agnoli, Mahncke, Grant, Goodman, Milberg, Esterman and DeGutis2024), while the unique contribution of anxiety and stress has been largely overlooked (though see Culot, Corlazzoli et al., Reference Culot, Corlazzoli, Fantini-Hauwel and Gevers2021; Culot, Fantini-Hauwel et al., Reference Culot, Fantini-Hauwel and Gevers2021). The goal of the current study was to more thoroughly compare the unique contribution of anxiety/stress, depression, and PTSD to metacognitive bias using a relatively large sample of post-9/11 veterans.
Anxiety, depression, and PTSD commonly co-occur (Barbano et al., Reference Barbano, van der Mei, deRoon-Cassini, Grauer, Lowe and Matsuoka2019) and have several overlapping symptoms (e.g., negative affect, emotional dysregulation, difficulty concentrating, and avoidance behaviors). Regarding contributions to metacognition, an influential study by Rouault and colleagues (Reference Rouault, Seow, Gillan and Fleming2018) found that, in a large unselected population (N = 995), the transdiagnostic factor of anxious-depression best predicted more negative metacognitive bias (underconfidence) on a perceptual decision-making task. This common anxious-depression factor is proposed to reflect the overlapping symptoms between anxiety and mood disorders (e.g., tendency to avoid social situations and feelings of hopelessness, Eysenck & Fajkowska, Reference Eysenck and Fajkowska2018) along with increased fatigue and persistent negative thought patterns (Stavrakaki & Vargo, Reference Stavrakaki and Vargo1986). Several independent research groups have replicated the association between this anxious-depression factor and metacognitive bias. For example, Benwell et al. (Reference Benwell, Mohr, Wallberg, Kouadio and Ince2022) and Hoven et al. (Reference Hoven, Luigjes, Denys, Rouault and van Holst2023) showed that higher levels of anxious-depression predicted more negative metacognitive bias at both the local, trial-by-trial, and global levels. Further, Katyal et al. (Reference Katyal, Huys, Dolan and Fleming2025) showed that those with greater subclinical anxious-depression symptoms were less likely to update their more negative global confidence in response to higher local confidence.
Contrasting this transdiagnostic approach, evidence suggests that there may be unique aspects of depression and anxiety associated with metacognitive bias. Appreciating these unique contributions could have both important theoretical and clinical implications. Depressive symptoms may particularly lead to biases to attend to negative information when reflecting on past memories, that is, negative recall bias (Pyszczynski et al., Reference Pyszczynski, Hamilton, Herring and Greenberg1989). This may contribute to negative self-judgments such as repeatedly focusing on perceived past failures, losses, or inadequacies (Rimes & Watkins, Reference Rimes and Watkins2005), leading to negative metacognitive bias. Conversely, negative metacognitive bias may lead to or exacerbate depressive symptoms by feeding into negative self-schemas and stable, global attributions for perceived failures, reinforcing low self-esteem and hopelessness (Abramson et al., Reference Abramson, Seligman and Teasdale1978). Though the relationship may be bidirectional, a meta-analysis of studies of a related construct to global metacognitive bias, self-esteem, suggests that the effects of self-esteem on future depressive symptoms (vulnerability model, β = −.16) were stronger than the effects of depressive symptoms on future self-esteem (scar model, β = −.08, Sowislo & Orth, Reference Sowislo and Orth2013).
Anxiety and stress may also uniquely contribute to more negative metacognitive bias. Symptoms of anxiety, such as excessive worry, fear of failure, or apprehension about the future, may contribute to a belief that one’s abilities are inadequate to meet current demands. This in turn could lead to underconfidence (e.g., diminished perceived capacity to succeed; Lazarus & Folkman, Reference Lazarus and Folkman1984). Conversely, negative metacognitive bias may exacerbate anxiety symptoms by heightening worry and self-focused attention about one’s performance (Clauss et al., Reference Clauss, Bardeen, Thomas and Benfer2020; Hopkins et al., Reference Hopkins, Dolan, Button and Moutoussis2021; consistent with S-REF model, Wells & Matthews, Reference Wells and Matthews1996). Regarding the temporal causal pathways, one study found that more negative metacognitive beliefs temporally preceded increased anxiety symptoms in a lagged model across baseline, 1, and 2 months (Capobianco et al., Reference Capobianco, Heal, Bright and Wells2019). In contrast, Sowislo and Orth (Reference Sowislo and Orth2013) found that the effects between low self-esteem and anxiety were relatively balanced: self-esteem predicted anxiety (β = −.10) to a similar extent as anxiety predicted self-esteem (β = −.08). These studies indicate a need to further investigate the potential contributions of stress and anxiety to metacognition and confidence.
Compared to depression and anxiety, fewer studies have investigated the relationship between PTSD and metacognitive bias. Sacher et al. (Reference Sacher, Tudorache, Clarys, Boudjarane, Landré and El-Hage2018) found that individuals with PTSD significantly underestimated their memory performance, though they did not account for anxiety or depressive symptoms. Agnoli et al. (Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023) found that PTSD did not predict unique variance in metacognitive bias after accounting for depression, but PTSD symptom changes over time did uniquely predict changes in metacognitive bias. This suggests that PTSD-related cognitive self-evaluations may differ mechanistically from depression and anxiety. Depressive and anxious self-evaluations tend to be relatively stable, whereas PTSD-related self-evaluations may fluctuate with symptom severity and be more tightly linked to trauma-related disruptions (Kashdan et al., Reference Kashdan, Uswatte, Steger and Julian2006). While evidence for PTSD being an independent predictor has been inconsistent, its associations with changes in metacognitive bias warrants further investigation.
Despite these investigations associating depressive, anxiety/stress, and PTSD symptoms with metacognitive bias, few studies have directly compared their unique contributions, with recent studies emphasizing their common variance (Rouault et al., Reference Rouault, Seow, Gillan and Fleming2018; Seow et al., Reference Seow, Fleming and Hauser2025). The goal of the current study was to better characterize the separate contributions of depressive, anxiety/stress, and PTSD symptoms to metacognitive bias in cognition. We examined a well-characterized sample of 601 post-9/11 veterans who performed a validated, objective battery of cognitive assessments (memory, attention, and executive function) along with self-reported global cognition from the WHODAS II. Post-9/11 veterans often report experiencing cognitive impairments (e.g., 77.7% report moderate to very severe cognitive complaints, Seal et al., Reference Seal, Bertenthal, Samuelson, Maguen, Kumar and Vasterling2016) while demonstrating little-to-no objective cognitive deficits (35% have mild or major neurocognitive impairment, Riley et al., Reference Riley, Mitko, Stumps, Robinson, Milberg, McGlinchey and DeGutis2019), making them a good population to examine negative metacognitive bias. To assess depressive and anxiety/stress symptoms, we used the validated Depression, Anxiety, Stress Scales (Lovibond & Lovibond, Reference Lovibond and Lovibond1995). Anxiety and stress were combined since both subscales reflect anxiety symptoms (Rowland et al., Reference Rowland, Hamilton, Lino, Ly, Denny, Hwang and Green2013; Dodd et al., Reference Dodd, Lockwood, Mansell and Palmier-Claus2019). We used the clinician-administered PTSD scale for DSM-IV (CAPS-IV) to assess PTSD symptoms. To measure clinical symptom/metacognitive bias coupling beyond individual differences at time 1, we also examined how specific affective symptom fluctuations related to changes in metacognitive bias over a two-year period. Based on previous studies (Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023; Katyal & Fleming, Reference Katyal and Fleming2024; Katyal et al., Reference Katyal, Huys, Dolan and Fleming2025), we hypothesized that greater depressive and anxiety/stress but not PTSD symptoms would be uniquely associated with more negative metacognitive bias. Based on Agnoli et al. (Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023), we further predicted that changes in these symptoms over two years would relate to changes in metacognitive bias, particularly for depression.
Methods
Participants were drawn from a pool of 813 post-9/11 combat-deployed veterans recruited into the Translational Research Center for TBI and Stress Disorders (TRACTS; see McGlinchey et al., Reference McGlinchey, Milberg, Fonda and Fortier2017) who participated between 2010 and 2019. This study was approved by the VA Boston Healthcare System IRB (#2354). All participants provided written informed consent, and the study was carried out in accordance with the declaration of Helsinki.
We excluded participants who had moderate to severe traumatic brain injury (n = 38), a history of neurological/physical impairments (n = 5), psychiatric disorders (n = 9) including bipolar disorder and/or suicidal/homicidal ideation requiring crisis intervention at either assessment, or were not combat deployed (n = 18). Additional participants (n = 67) were removed due to evidence of reduced effort on the Medical Symptom Validity Test (Green, Reference Green2004) at either time point, and symptom overreporting on the Neurobehavioral Symptom Inventory Validity-10 Scale (n = 22). Finally, we excluded 53 participants who did not complete the WHODAS II or objective cognitive tests. Participants may have been excluded for more than one reason. This left a final sample of 601 participants at time 1 and 239 at time 2.
Clinical measures
PTSD symptom severity was assessed using the clinician-administered PTSD scale for the DSM-IV (CAPS-IV, Blake et al., Reference Blake, Weathers, Nagy, Kaloupek, Gusman, Charney and Keane1995; Weathers et al., Reference Weathers, Keane and Davidson2001). We used the total score, ranging from 0 to 136. The depression subscale from the 21-item Depression, Anxiety, and Stress Scale (DASS) was used to measure continuous depressive symptoms, with total scores ranging from 0 to 42 (Lovibond & Lovibond, Reference Lovibond and Lovibond1995). Additionally, in line with previous studies, we computed an anxiety/stress score from the DASS by summing anxiety and stress symptoms, with total scores ranging from 0 to 84.
Subjective cognition
The World Health Organization Disability Assessment Schedule II (WHODAS II, Federici et al., Reference Federici, Meloni, Mancini, Lauriola and Olivetti Belardinelli2009) is a validated 36-item self-report measure widely used in post-9/11 veterans (e.g., Bovin et al., Reference Bovin, Meyer, Kimbrel, Kleiman, Green, Morissette and Marx2019). There are six subscales: understanding and communicating, getting around, self-care, getting along with people, life activities, and participation in society. We used the understanding and communicating subscale to assess self-reported cognition: “In the past 30 days, how much difficulty did you have with…” (1) concentrating on doing something for 10 minutes; (2) remembering to do important things; (3) analyzing and finding solutions to problems in day-to-day life; (4) learning a new task, for example, learning how to get to a new place; (5) generally understanding what people say; and (6) starting and maintaining a conversation. Scores were reverse-scored and ranged from 0–30, with higher scores representing better self-reported cognition. The understanding and communicating subscale captures broad, everyday cognitive functioning rather than one-to-one correspondence with specific neuropsychological tasks (similar to previous studies, e.g., reviewed by Burmester et al., Reference Burmester, Leathem and Merrick2016); while some items map more directly onto objective tasks (e.g., sustained attention), others reflect more general cognitive demands. Items on the subscale showed small-to-moderate associations with the global objective cognition composite (r = .18−.30). Accordingly, metacognitive bias was operationalized at a global level as the discrepancy between subjective and objective cognition, making exact domain-level matching unnecessary.
Objective cognition
To assess objective cognition, we administered a validated battery of tests spanning executive function, memory, and attention domains (see Riley et al., Reference Riley, Mitko, Stumps, Robinson, Milberg, McGlinchey and DeGutis2019). Separate a priori-defined normed composites were created for each domain, which was guided by established theoretical and empirical frameworks (e.g., Miyake et al., Reference Miyake, Friedman, Emerson, Witzki, Howerter and Wager2000; Lezak, Reference Lezak2004; Strauss et al., Reference Strauss, Sherman and Spreen2006) and prior work using this battery (Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023), rather than by exploratory factor analysis. These composites were then averaged with equal weighting to create a global cognition composite. The executive function domain composite consisted of six measures: the Delis–Kaplan Executive Function System (D-KEFS) Trail Making Test Number/Letter Switching subtest, as a measure of working memory/switching (Delis et al., Reference Delis, Kaplan and Kramer2001), the D-KEFS letter fluency as a mixed executive function measure (FAS category switching and letter fluency subtests, Delis et al., Reference Delis, Kaplan and Kramer2001), the D-KEFS Color-Word Test, as a measure of inhibitory control (Delis et al., Reference Delis, Kaplan and Kramer2001), the CANTAB Intra-Extra Dimensional Set Shift Task (number of stages completed) as a measure of task-switching (De Luca et al., Reference De Luca, Wood, Anderson, Buchanan, Proffitt, Mahony and Pantelis2003), and the Auditory Consonant Trigrams as a measure of working memory (ACT, Shura et al., Reference Shura, Rowland and Miskey2016). The ACT was not administered to all participants at time 2; therefore, within-group changes were not examined with this measure. Verbal learning and memory were measured using the California Verbal Learning Test-Second Edition (Woods et al., Reference Woods, Delis, Scott, Kramer and Holdnack2006). The memory domain composite score measures encoding, recall, and recognition and consists of the mean age-adjusted z-scores of three measures: short-delay free recall, long-delay free recall, and long-delay recognition (see Riley et al., Reference Riley, Mitko, Stumps, Robinson, Milberg, McGlinchey and DeGutis2019). The attention domain composite consisted of three measures: the Test of Variables Attention (Henry, Reference Henry2005), the Digit Span Forward trials (WAIS-IV; Wechsler, Reference Wechsler2008), and the Trail Number-Sequencing subtest (Delis et al., Reference Delis, Kaplan and Kramer2001). The objective cognition composite consisted of the z-score average of executive function, attention, and memory domains, and reflects an average across standardized composite scores rather than equal numbers of component tests (Riley et al., Reference Riley, Mitko, Stumps, Robinson, Milberg, McGlinchey and DeGutis2019; Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023). Executive function was moderately correlated with attention (r = .52) and memory (r = .37), and attention and memory were more modestly correlated (r = .25).
Global metacognitive sensitivity and bias
Global metacognitive sensitivity, that is, accuracy, was calculated using Pearson correlations between self-reported and objective cognition measures at the group level. In calculating the metacognitive bias score for each participant, the objective cognition score was subtracted from self-reported cognition. Scores below 0 refer to a negative metacognitive bias relative to the sample, such that an individual reports more self-reported cognitive issues than are objectively measured. Self-reported cognition was z-scored within the total veteran sample for within-sample standardization given the absence of appropriate external normative data, while objective cognition was calculated based on normative data (see Riley et al., Reference Riley, Mitko, Stumps, Robinson, Milberg, McGlinchey and DeGutis2019). The objective cognition scores were then z-scored within the sample so that the mean and SD of both objective and self-reported measures were 0 and 1, respectively. As a result, metacognitive bias reflects a relative discrepancy within the deployed post-9/11 veteran sample rather than an absolute absence or presence of bias.
Time 1 analyses
We first quantified overall group metacognitive sensitivity as the Pearson correlation between self-reported and objective cognition scores. Metacognitive bias was defined as self-reported minus objective cognition, and its associations with depressive, anxiety/stress, and PTSD symptom severity were tested using Pearson correlations. Because these associations were hypothesized a priori based on prior work (e.g., Agnoli et al., Reference Agnoli, Zuberer, Nanni-Zepeda, McGlinchey, Milberg, Esterman and DeGutis2023), they were not corrected for multiple comparisons. To address clinical symptom overlap and identify unique predictors of metacognitive bias, we modeled shared variance among symptom domains using simultaneous regression and hierarchical models, rather than using item-level removal approaches that could alter validated scale structures and clinical interpretability. Variance inflation factors (VIFs) were examined to assess multicollinearity. To further delineate the unique contributions of each symptom domain, significant predictors were entered sequentially in hierarchical regressions to estimate incremental variance explained (ΔR 2). Given the substantial overlap among symptom domains, we conducted mediation analyses to examine whether the association between one symptom domain and metacognitive bias was significantly accounted for by another symptom domain. Mediation analyses were conducted in SPSS using the PROCESS macro (Hayes, Reference Hayes2012). Finally, to identify symptom features most strongly related to metacognitive bias, we conducted item-level Pearson correlations between DASS items and metacognitive bias scores, with FDR correction for multiple comparisons.
Longitudinal analyses
Longitudinal analyses included participants with complete time 1 and time 2 data (n = 239). Change scores (time 2–time 1) were computed for metacognitive bias and clinical symptoms, and Pearson correlations and multiple (including hierarchical) regressions were used to examine associations and test the unique and incremental contributions of depressive, anxiety/stress, and PTSD symptom changes to changes in metacognitive bias. Mediation analyses were conducted in SPSS using the PROCESS macro (Hayes, Reference Hayes2012) to examine whether the association between one symptom domain and metacognitive bias was significantly accounted for by another symptom domain.
Results
Demographics and clinical characteristics
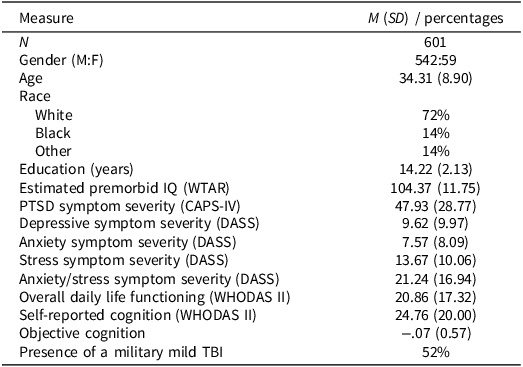
The veteran sample was 90% male, 72% white, with a mean age of 34.31 years (SD = 8.90), and 14.22 years of education (SD = 2.13), see Table 1. Participants generally scored in the subclinical range on all DASS subscales and overall exhibited moderate PTSD symptoms on the CAPS-IV; 15% of participants exceeded the moderate threshold for depressive symptoms on the DASS, 18% exceeded the moderate threshold for anxiety, and 53% met diagnostic criteria for PTSD on the CAPS-IV. Importantly, exclusion of participants meeting these clinical thresholds yielded highly similar results across all major findings (see Supplementary Materials). We found that affective measures were highly intercorrelated; anxiety/stress symptoms were strongly correlated with depressive symptoms (r = .77) and PTSD symptoms (r = .68), and depressive symptoms correlated with PTSD symptoms (r = .60).
Time 1 demographic, clinical, and cognitive characteristics

Table 1 Long description
The table presents demographic, clinical, and cognitive characteristics of a veteran sample. It includes measures such as the number of participants (601), gender distribution (542 male, 59 female), mean age (34.31 years with a standard deviation of 8.90), and years of education (14.22 years with a standard deviation of 2.13). The table also details race distribution (72% White, 14% Black, 14% Other), estimated premorbid IQ (104.37 with a standard deviation of 11.75), and various symptom severities including PTSD (47.93 with a standard deviation of 28.77), depressive symptoms (9.62 with a standard deviation of 9.97), anxiety symptoms (7.57 with a standard deviation of 8.09), stress symptoms (13.67 with a standard deviation of 10.06), and combined anxiety/stress symptoms (21.24 with a standard deviation of 16.94). Additionally, it covers overall daily life functioning (20.86 with a standard deviation of 17.32), self-reported cognition (24.76 with a standard deviation of 20.00), objective cognition (-0.07 with a standard deviation of 0.57), and the presence of a military mild TBI (52%).
Self-reported and objective cognition
The mean self-reported cognitive ability for the sample was 24.76, SD = 20.00, indicating mild-to-moderate impairment. Mean objective cognitive performance across the entire battery for the group was z-score = −.07, SD = .57, indicating little-to-no objective cognitive deficits. We found that worse self-reported cognition was significantly associated with increased depressive (r = −.64, p < .001), anxiety/stress (r = −.70, p < .001), and PTSD symptoms (r = −.57, p < .001), with all three variables predicting unique variance in self-reported cognition in a multiple regression (β = −.22, p < .001; β = −.44, p < .001; β = −.15, p < .001, respectively). Objective cognition was also significantly negatively associated with increased depressive (r = −.18, p < .001), anxiety/stress (r = −.20, p < .001), and PTSD symptoms (r = −.22, p < .001). In a simultaneous multiple regression only PTSD symptoms predicted unique variance in objective cognition (PTSD: β = −.13, p = .018; depression: β = −.08, p = .168; anxiety/stress: β = −.04, p = .542).
Global metacognitive sensitivity and bias
We next examined our measures of interest: global metacognitive sensitivity and bias. We assessed metacognitive sensitivity by correlating self-reported and objective cognition scores. Across the entire group, veterans had significant global metacognitive sensitivity, r = 0.25, p < .001, similar to other studies of global metacognition (e.g., Zell & Krizan, Reference Zell and Krizan2014; Agnoli et al., Reference Agnoli, Mahncke, Grant, Goodman, Milberg, Esterman and DeGutis2024). However, global metacognitive sensitivity did not significantly vary across anxiety/stress, depressive, or PTSD symptoms (all ps > .20, see supplemental Figure S1). When examining metacognitive bias, self-reported minus objective cognitive performance, we found it was significantly associated with increased anxiety/stress (r = −.41, p < .001), depressive (r = −.37, p < .001), and PTSD symptoms (r = −.31, p < .001; See Figure 1). These associations are notable when considering that we found the test–retest reliability of metacognitive bias over two years was only .52.
Associations of metacognitive bias with anxiety/stress, depressive, and PTSD symptoms.

Figure 1 Long description
A scatter plot with three sections, each showing the relationship between metacognitive bias and different symptoms. The first section, in purple, plots metacognitive bias against anxiety and stress symptoms, with a correlation coefficient of negative point four one. The second section, in blue, plots metacognitive bias against depressive symptoms, with a correlation coefficient of negative point three seven. The third section, in orange, plots metacognitive bias against PTSD symptoms, with a correlation coefficient of negative point three one. Each section contains hundreds of data points, with the x-axis representing symptom severity and the y-axis representing metacognitive bias. All values are approximated.
In a simultaneous multiple regression, depressive and anxiety/stress symptoms predicted unique variance in metacognitive bias (depression: β = −.12, p = .045, VIF = 2.55; anxiety/stress: β = −.29, p < .001, VIF = 3.00), though PTSD symptoms did not (β = −.03, p = .524, VIF = 1.90).
Hierarchical regressions clarified these relationships (Table S1). Depressive symptoms explained 14% of the variance in metacognitive bias and adding anxiety/stress symptoms accounted for an additional 3.9% (ΔR 2 = .039, p < .001). Conversely, anxiety/stress symptoms explained 17% of the variance, and adding depressive symptoms explained only an additional <1%. Thus, anxiety/stress symptoms show a stronger and more unique association with negative metacognitive bias, whereas depressive symptoms largely overlap with anxiety/stress.
To test whether anxiety/stress symptoms significantly mediated the effect of depressive symptoms on metacognitive bias, we conducted a mediation analysis using the PROCESS macro in SPSS. The indirect effect of depressive symptoms on metacognitive bias through anxiety/stress symptoms was significant (β = −.03, 95% CI: −.029, −.002), though the direct effect between depressive symptoms and metacognitive bias remained significant (β = −.02, p = .02), indicating that anxiety/stress symptoms partially mediated this association.
To further characterize symptom-specific associations with metacognitive bias, we conducted exploratory item-level correlations between DASS items and metacognitive bias, FDR-corrected for multiple comparisons (Figure 2). Stress items reflecting behavioral activation and distress (Q12, 8, 11, 14) and depressive items reflecting sadness and reduced initiative (Q5, 16, 13) showed the strongest associations (rs < −.30). Slightly stronger correlations for stress than anxiety may reflect the broader range of stress symptoms in this sample (Figure S2).
Item-level pearson correlations of DASS symptoms and metacognitive bias. Note. All items achieved significance after FDR correction.

Figure 2 Long description
The bar graph compares correlations of DASS symptoms and metacognitive bias. It features horizontal bars divided into three sections: Depression, Anxiety, and Stress. Each section lists specific DASS items with their corresponding correlation values. The Depression section includes items like 'I felt that life was meaningless' and 'I felt down-hearted and blue,' with correlations ranging from approximately -0.35 to -0.05. The Anxiety section lists items such as 'I experienced breathing difficulty' and 'I felt scared without any good reason,' with similar correlation ranges. The Stress section includes items like 'I felt that I was rather touchy' and 'I found it difficult to relax,' also with correlations ranging from approximately -0.35 to -0.05. The x-axis represents correlation values, while the y-axis lists the DASS items. The bars are color-coded: blue for Depression, purple for Anxiety, and dark purple for Stress. All values are approximated.
Associations between changes in metacognition and changes in depressive, anxiety/stress, and PTSD symptoms
To examine longitudinal coupling between metacognition and clinical symptoms, we analyzed change over ∼2 years in participants with complete data (n = 239). Metacognitive sensitivity was similar at time 1 (r = .25, p < .001) and time 2 (r = .20, p < .001; z = .82, p = .206), and metacognitive bias did not differ across time (time 1: M = .08, SD = .98; time 2: M = .01, SD = 1.04; t = 1.20, p = .231). Depressive (time 1: M = 9.57, SD = 9.95; time 2: M = 8.93, SD = 9.54; t = 1.56, p = .121) and anxiety/stress symptoms (time 1: M = 20.74, SD = 17.04; time 2: M = 20.73, SD = 16.71; t = .13, p = .895) showed nonsignificant reductions, whereas PTSD symptoms significantly decreased, albeit modestly (time 1: M = 47.25, SD = 28.80; time 2: M = 44.49, SD = 28.87; t = 2.85, p = .005). Changes in metacognitive bias were correlated with changes in depressive (r = −.35), anxiety/stress (r = −.46), and PTSD symptoms (r = −.34; all ps < .001), such that symptom improvement was associated with more positive metacognitive bias changes (Figure 3). The weaker association with depressive symptoms, despite its strong baseline association with metacognitive bias, may reflect lower change variance (SD = 7.89) relative to anxiety/stress (SD = 13.83) and PTSD (SD = 20.61). Results were unchanged or stronger after controlling for effects of regression to the mean (Table S2).
Associations between changes in metacognitive and changes in anxiety/stress, depressive, and PTSD symptoms.

Figure 3 Long description
A scatter plot with three panels showing the relationship between metacognitive bias and symptoms of anxiety, depression, and PTSD. The x-axes represent different symptom scales: DASS-21 Anxiety/Stress Symptoms, DASS-21 Depressive Symptoms, and CAPS-C PTSD Symptoms. The y-axes represent metacognitive bias. Each panel contains hundreds of data points. The first panel shows a negative correlation between anxiety/stress symptoms and metacognitive bias with a correlation coefficient of negative point four one. The second panel shows a negative correlation between depressive symptoms and metacognitive bias with a correlation coefficient of negative point three seven. The third panel shows a negative correlation between PTSD symptoms and metacognitive bias with a correlation coefficient of negative point three one. Each panel includes a trend line indicating the overall negative correlation. All values are approximated.
In a simultaneous multiple regression with changes in clinical symptoms predicting change in metacognitive bias, anxiety/stress symptoms, and PTSD symptoms explained unique variance (R2 = .25; anxiety/stress symptoms: β = −.33, p < .001, VIF = 2.85; PTSD symptoms: β = −.16, p = .001, VIF = 1.95), while changes in depressive symptoms were not a significant predictor (β = −.10; p = .137, VIF = 2.65). Hierarchical regressions confirmed anxiety/stress as the primary driver: PTSD explained 12% of the variance when entered first, with anxiety/stress accounting for an additional 12%, whereas anxiety/stress entered first explained 21% and PTSD added only 3% (ΔR 2 = .03; Table S3). Thus, across cross-sectional and longitudinal analyses, anxiety/stress symptoms were the most robust predictors of negative metacognitive bias and its change over time.
To test whether changes in anxiety/stress symptoms significantly mediated the association between PTSD symptom changes and changes in metacognitive bias, we conducted a mediation analysis using the PROCESS macro in SPSS. The indirect effect of PTSD symptom changes on metacognitive bias changes through anxiety/stress symptom changes was significant (β = −.008, 95% CI: −.012, −.006), though the direct effect between PTSD symptom changes and changes in metacognitive bias remained significant (β = −.008, p = .004), indicating that change in anxiety/stress symptoms partially mediated this association.
Discussion
The current study aimed to determine the unique contributions of anxiety/stress, depressive, and PTSD symptoms to global metacognitive bias in a large sample of post-9/11 veterans. Though studies have looked at the unique contribution of anxiety and depressive symptoms to self-reported cognitive complaints (e.g., Allott et al., Reference Allott, Gao, Hetrick, Filia, Menssink, Fisher and Cotton2020), the current study is the first to examine their separate contributions to metacognitive bias. At time 1, anxiety/stress symptoms showed the strongest correlation with metacognitive bias (anxiety/stress: r = −.41; depression: r = −.37; PTSD symptoms: r = −.31) and, in a multiple regression predicting metacognitive bias, only anxiety/stress (β = −.29) and depression (β = −.12) predicted unique variance. Hierarchical models further showed that entering anxiety/stress first explained 17% of variance, with depression adding <1%. Additionally, in terms of predicting changes in metacognitive bias over ∼2 years, changes in anxiety/stress symptoms and PTSD symptoms were significant unique predictors, whereas changes in depressive symptoms were not. Hierarchical models showed that entering anxiety/stress first explained 21% of variance in bias change, with PTSD adding 3%. Together, these findings point to anxiety and stress being the most consistent predictor of cognitive underconfidence. This distinct contribution of anxiety/stress to negative metacognitive bias has both important theoretical and clinical implications.
We observed robust relationships between metacognitive bias and anxiety/stress, depressive, and PTSD symptoms, along with strong intercorrelations among these affective symptom measures (r = .62–.77, similar to Kessler et al., Reference Kessler, Chiu, Demler and Walters2005; Ginzburg et al., Reference Ginzburg, Ein-Dor and Solomon2010; Rytwinski et al., Reference Rytwinski, Scur, Feeny and Youngstrom2013). Given this substantial overlap, it is understandable that previous metacognition studies have often treated anxiety and depression as a single anxious-depression transdiagnostic factor (e.g., Rouault et al., Reference Rouault, Seow, Gillan and Fleming2018; Benwell et al., Reference Benwell, Mohr, Wallberg, Kouadio and Ince2022; Hoven et al., Reference Hoven, Luigjes, Denys, Rouault and van Holst2023; Katyal et al., Reference Katyal, Huys, Dolan and Fleming2025). Moreover, many of these studies assessed local, trial-by-trial metacognition, which typically shows weaker associations with clinical symptoms than global metacognition (e.g., r = –.41, medium-to-large effect in the current study versus β = –.10, a small effect in Rouault et al., Reference Rouault, Seow, Gillan and Fleming2018). This combination of overlapping symptom variance and the smaller effect sizes for local metacognition likely left those studies underpowered to detect distinct contributions of specific symptom domains.
Building on this work, the current study isolates the specific contributions of each affective symptom domain to global metacognitive bias. Specifically, anxiety/stress symptoms emerged as the strongest unique predictor of metacognitive bias at time 1 and changes in metacognitive bias over time, surpassing depressive and PTSD symptoms. This pattern challenges the commonly held view that underconfidence is primarily a hallmark of depression (e.g., Beck, Reference Beck2008), and instead aligns with emerging evidence linking anxiety to metacognitive impairments (e.g., Katyal & Fleming, Reference Katyal and Fleming2024). Notably, this sample did not exhibit performance-based cognitive deficits relative to normative data, supporting the interpretation of negative metacognitive bias as reflecting underconfidence rather than unmeasured cognitive impairment. One potential explanation for this robust association is that anxiety/stress symptoms may make individuals feel they are unable to respond effectively to the current circumstances, that is, a belief that one’s abilities are inadequate to overcome current challenges (Lazarus & Folkman, Reference Lazarus and Folkman1984). This sense of inadequacy may be especially pronounced in cognitively demanding situations. Consistent with this, Vishwanathan et al. (Reference Vishwanathan, Kashyap, Reddy, Philip, Thippeswamy and Desai2022) found that individuals with anxiety disorders performed worse on a story-recall task, which many described as overwhelming, suggesting that anxiety may activate negative metacognitive beliefs in cognitively demanding contexts. Anxiety may particularly affect cognitive self-evaluations, given the link between anxiety and heightened self-monitoring of one’s thinking (e.g., thoughts and memory slips, Clark & McManus, Reference Clark and McManus2002). Taken together, these findings suggest that anxiety may distort metacognitive bias by amplifying perceived inadequacy, particularly in cognitively demanding situations.
An alternative to this anxiety/stress-driven explanation is that negative metacognitive bias may itself contribute to increased anxiety and stress (Hopkins et al., Reference Hopkins, Dolan, Button and Moutoussis2021; consistent with S-REF model, Wells & Matthews, Reference Wells and Matthews1996). Beyond our performance-based measure of bias, underconfidence can also manifest as broader, trait-like metacognitive beliefs about thinking, typically measured with the Metacognitions Questionnaire (MCQ). Fisher et al. (Reference Fisher, Reilly and Noble2018) found that, after accounting for demographics and other clinical variables, metacognitive beliefs on the MCQ explained an additional 31% of the variance in symptoms of anxiety and an additional 15% of the variance in depressive symptoms. Seow et al. (Reference Seow, Fleming and Hauser2025) also found that low general self-esteem, which can be associated with negative global metacognitive bias (Rouault et al., Reference Rouault, Will, Fleming and Dolan2022), was the biggest contributor to anxious-depression, followed by low-self efficacy, and low local task confidence. Extending these findings, the present results suggest that cognitive underconfidence may be especially linked to anxiety/stress, as confidence in one’s cognitive abilities is central to managing daily life challenges.
In terms of evidence for the temporal causal pathways between metacognitive bias and anxiety/stress, the findings are mixed. One study using the MCQ found that more negative metacognitive beliefs predicted subsequent increases in anxiety symptoms over 1–2 months in a lagged model (Capobianco et al., Reference Capobianco, Heal, Bright and Wells2019). In contrast, Sowislo and Orth (Reference Sowislo and Orth2013) reported a more reciprocal pattern between self-esteem and anxiety, with self-esteem predicting later anxiety (β = –.10) as well as anxiety predicting later self-esteem (β = –.08). Notably, interventions targeting metacognitive bias/cognitive confidence have shown to more reliably improve anxiety (e.g., Bowler et al., Reference Bowler, Mackintosh, Dunn, Mathews, Dalgleish and Hoppitt2012; Fodor et al., Reference Fodor, Georgescu, Cuijpers, Szamoskozi, David, Furukawa and Cristea2020) whereas there is less evidence that anxiety-focused interventions (e.g., cognitive behavioral therapy-CBT, selective serotonin reuptake inhibitors) robustly improve bias/cognitive confidence (though see modest effects in Fox et al., Reference Fox, Lee, Hanlon, Seow, Lynch, Harty, Richards, Palacios, O’Keane, Stephan and Gillan2023). Future research employing ecological momentary assessment to capture real-time changes in metacognitive bias and anxiety/stress may provide critical insights into their temporal causal dynamics.
From a clinical perspective, the current results suggest that anxiety and stress symptoms, even at subclinical levels, can be accompanied by significant negative metacognitive bias, matching or exceeding those seen in depression or PTSD. These findings underscore the importance of evaluating both self-reported and objective cognitive performance – and, critically, the discrepancy between them – when assessing patients and planning treatment, particularly in groups with elevated anxiety and stress such as post-9/11 veterans. Rather than dismissing cognitive complaints as functional or non-organic, subjective–objective discrepancies should be viewed as clinically informative and prompt evaluation of anxiety, depression, or PTSD that may distort self-evaluation of cognitive functioning. Beyond informing assessment, these findings suggest that metacognitive bias, in the cognitive domain or more broadly, could be an important treatment target. For example, in individuals with mild traumatic brain injury who exhibited negative metacognitive bias in cognition, a three-month program of cognitive training, using either structured “brain training” or entertainment games with performance feedback, significantly improved metacognitive bias and reduced depressive symptoms (anxiety measures were not administered; Agnoli et al., Reference Agnoli, Mahncke, Grant, Goodman, Milberg, Esterman and DeGutis2024). More broadly, metacognitive therapy, which targets thought processes about cognition (Rawat et al., Reference Rawat, Sangroula, Khan, Faisal, Chand, Yousaf and Yousaf2023), has been shown to be highly effective for anxiety, surpassing CBT in recovery rates (65% vs. 38% at two-year follow-up, Nordahl et al., Reference Nordahl, Borkovec, Hagen, Kennair, Hjemdal, Solem and Wells2018; 57% vs. 38% at nine-year follow-up, Solem et al., Reference Solem, Wells, Kennair, Hagen, Nordahl and Hjemdal2021). Together, these findings suggest that interventions that help to recalibrate self-evaluation, whether through feedback-based cognitive training or metacognitive therapy, may reduce metacognitive bias and particularly alleviate anxiety symptoms.
Despite the strengths of the findings, several limitations warrant consideration. The predominantly male post-9/11 veteran sample may limit generalizability to female or civilian populations. Self-reported cognition was assessed using only six items from the WHODAS II Understanding and Communicating subscale; more comprehensive instruments (e.g., the Cognitive Failures Questionnaire; Broadbent et al., Reference Broadbent, Cooper, FitzGerald and Parkes1982) may yield richer and more reliable estimates. Finally, the stronger associations with anxiety/stress relative to depression may partly reflect scaling or floor effects, as depressive symptoms were less frequently endorsed in this sample.
In summary, anxiety/stress symptoms were most consistently associated with negative metacognitive bias in post-9/11 veterans, surpassing both depression and PTSD. These findings suggest that higher anxiety/stress symptoms are uniquely associated with lower confidence in one’s cognitive abilities and underscore metacognitive bias as both a meaningful clinical outcome measure and a modifiable target for intervention.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1355617726101945.
Acknowledgments
None.
Funding statement
This work was supported by the US Department of Veterans Affairs through the Translational Research Center for TBI and Stress Disorders, a VA Rehabilitation Research & Development TBI National Research Center (B3001-C).
Competing interests
None.