Global dietary patterns increasingly favour the consumption of animal products and ultra-processed foods, accompanied by high intakes of sodium, sugar and fat( Reference Popkin, Adair and Ng 1 ). These dietary trends contribute to increased levels of obesity and diet-related diseases, especially in low- and middle-income countries, where increases are the most rapid( Reference Baker and Friel 2 ). The present paper addresses this situation by analysing one of the main tools to positively affect population eating behaviour: national dietary guidelines. This research contributes to tackling the pressing need to better address the burden of non-communicable, diet-related diseases through effective national policies that take a comprehensive, context-sensitive and multi-stakeholder approach to improve dietary quality and physical activity( Reference Lachat, Otchere and Roberfroid 3 ).
National dietary guidelines represent the nutrition policy and priorities of many countries. These are meant to be the result of consensus among food and nutrition experts, whose task is to translate scientific evidence into practical messages that encourage populations to select a healthy diet within their specific cultural and food context. While dietary guidelines can be useful as educational tools for local nutritionists and health providers, their effectiveness depends on how nutrition advice is framed( Reference Capra 4 ) and, ultimately, the public’s perceptions and interests concerning healthy eating behaviours( Reference Vandevijvere, De Vriese and Huybrechts 5 – Reference Nayga and Capps 8 ).
Comparative dietary guidelines research has mostly focused on their development, implementation( Reference Albert, Samuda and Molina 9 – Reference Aranceta and Serra-Majem 13 ) and pictorial representations( Reference Murphy and Barr 10 , Reference Painter, Rah and Lee 14 ). While there has been comparative research concerning overall guideline messages( Reference Sichieri, Chiuve and Pereira 15 ), there is a paucity of in-depth, cross-country comparative research on what the guidelines actually say and how nutrition messages are framed. The present study addresses this gap in the literature by engaging in a comparative content analysis of guidelines in the Spanish-speaking Caribbean (Cuba, Puerto Rico and the Dominican Republic), a region that shares a similar food culture, concerns over growing obesity rates and an increased consumption of energy-dense and ultra-processed foods, but differs in current economic and political conditions (Table 1).
Selected descriptive country indicators (from CIA World Fact Book( 39 ), unless otherwise noted)
CIA, Central Intelligence Agency; GDP, Gross Domestic Product; WHZ, weight-for-height Z-score; HAZ, height-for-age Z-score; ND, no data available.
* Figures represent 2011 data for Cuba and 2010 data for Puerto Rico and Dominican Republic( 40 ).
† 2005 statistic( 41 ).
‡ 2008 statistic( 39 ).
§ 2010 statistic( 25 ).
|| 2009 statistic( 25 ).
¶ 2007 statistic( 29 ).
Spanish-speaking Caribbean countries are characterized by traditional dietary patterns, where rice and beans are staples and meat is central in the plate. Accompanying foods include viandas (starchy roots such as yucca, taro and plantains), fried snacks (frituras) and preserved foods (such as salted dried codfish and sausages). Today, a variety of ultra-processed foods and drinks, including sugar-sweetened beverages, constitute add-ons to the traditional diets. Current diets tend towards energy-dense foods, an increase in the consumption of pre-prepared food products and foods away from home, and a low consumption of fruits and vegetables( Reference Colón-Ramos, Pérez-Cardona and Monge-Rojas 16 – Reference Porrata-Maury 18 ). While these changes go hand-in-hand with global dietary transitions, they are also influenced by circumstances unique to each context. Since the late 1950s, Puerto Rico has experienced a continued increase in fast-food restaurants. According to 2005 statistics, there were about 2000 fast-food restaurants, with a revenue of $US 1·0–1·3 billion per year and 77 % of the population visited these restaurants often( Reference Rosa 19 ). These fast-food restaurants coexist with street food stands, mostly selling fried snacks, as well as traditional meals. The foreign franchise food market started later in the Dominican Republic, in the late 1970s. In 2005 there were about 250 franchises, with 900 establishments, including non-food franchises( Reference Chacon Valverde 20 ), a considerably lower number compared with Puerto Rico, especially when accounting for the geographical size difference between the two countries (Table 1). While Cuba’s communist system and the US blockade have affected the country’s food supply stability( Reference Benjamin, Collins and Scott 21 ), there is local production of ultra-processed foods, including, for example, local brands of sugar-sweetened beverages (tuKola), among other similar products. In addition, access to foods away from home is increasing gradually with the recent upsurge in privately run restaurants (locally known as paladares) and the gradual opening of the country to foreign investment and food establishments( Reference Feinberg 22 , Reference Feinberg 23 ).
As a result of these changes, overweight and non-communicable diet-related diseases are present and increasing in the region. Puerto Rico shows the highest rate of adult obesity and childhood overweight (Table 1)( Reference Jimenez, Díaz and García 24 , 25 ). The Dominican Republic presents issues related to undernutrition, having a high level of childhood stunting, closely surpassing the percentage of childhood overweight (Table 1).
The present research focuses on how the national dietary guidelines address pressing local nutritional issues, contextualized in changing food environments and food culture similarities. The information provided by this comparative exercise can inform future public health nutrition initiatives in the region as well as those targeting migrant communities, including improvements in nutrition messaging and potential regional collaborations.
Dietary guidelines in the Spanish-speaking Caribbean
In the 1990s, the WHO and the FAO led a global effort to translate nutrient intake recommendations into food-based dietary guidelines( Reference Dwyer 11 ). However, guidelines have existed in the region since the late 1940s. As reviewed by Palacios and Anglero, the first Puerto Rican guidelines date back to 1946 and were based on the population nutrient needs and dietary patterns. However, since the 2000s, the island’s Food and Nutrition Commission of Puerto Rico (Comisión de Alimentación y Nutrición, CAN-PR) has been adapting the guidelines and icons from the US Department of Agriculture’s (USDA) Dietary Guidelines, starting with the Food Guide Pyramid for Puerto Rico( Reference Palacios and Angleró 26 ). The current Puerto Rican Dietary Guidelines (PR-DG), released in 2013, are based on the USDA 2005 and 2010 Dietary Guidelines. They include an adapted and translated version of MyPlate (MiPlato)( 27 ). The history of dietary guidelines in Cuba and the Dominican Republic is not well documented. Both countries published their current guidelines in 2009, following an internal process of review and consultation with local experts( 28 , 29 ). In Cuba, the guidelines were developed using a nationwide survey of food consumption and preferences, and included members of the culinary sector as part of the local experts consulted( Reference Porrata-Maury 18 , Reference Gorry 30 ). The current guidelines (Cuban-DG) are a revision of those published in 2000( 31 ). The current 2009 Dietary Guidelines in the Dominican Republic (DR-DG) seem to be the first in the country, developed with local and international actors, including the FAO and the Pan-American Health Organization( 31 ).
No information is available about the actual reach and use of these documents. They are disseminated through the usual channels, including schools, health providers and community-based nutrition education initiatives( 31 ).
Methodology
The present paper is based on a qualitative analysis of current dietary guidelines for each location. They were accessed electronically, through the official government agency responsible for their dissemination (Table 2). These guidelines include a long, complete policy document (targeting service providers), key recommendations (KR; targeting the general public) and the corresponding pictorial representation. The analysis was organized around the KR. These were summarized into main themes and categorized according to whether the recommendation was diet-based (addressing overall dietary patterns) or food-based (addressing specific food groups). Themes falling outside these main categories were classified as ‘other’ (e.g. exercise, weight control, breast-feeding and food safety) and excluded from the present food- and diet-centred analysis.
Selected characteristics of current dietary guidelines in the Spanish-speaking Caribbean
KR, key recommendation; INHA, Instituto de Nutrición e Higiene de los Alimentos; CAN-PR, Comisión de Alimentación y Nutrición; SESPAS, Secretaria de Estado de Salud Pública y Asistencia Social.
* Grains (granos) include beans and corn.
The policy documents were analysed using the qualitative analysis software, Atlas.ti version 7·5·2. Coding was organized around the KR themes, focusing on how the documents discussed each one, including the provision of practical advice, engagement with traditional dietary patterns and addressing local food availability and access, among other factors related to food selection.
Results and discussion
Overview of national dietary guideline policy documents
The different local procedures in the development of the national dietary guidelines included in the current analysis yielded documents that differ in organization, focus and the information presented. While the Cuban-DG and PR-DG share the stated emphasis on overnutrition and are directed at the healthy population over the age of 2 years, the DR-DG introduce the document with a food security emphasis, targeting all age groups, including children under 2 years of age. In this attempt, the DR-DG underscore the importance of infant feeding (lactation and complementary feeding) in a single document.
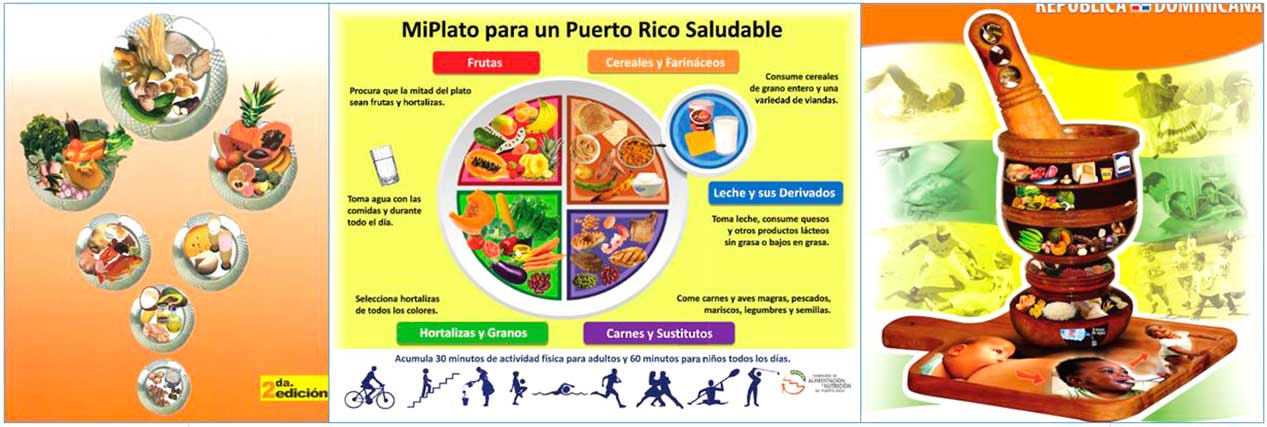
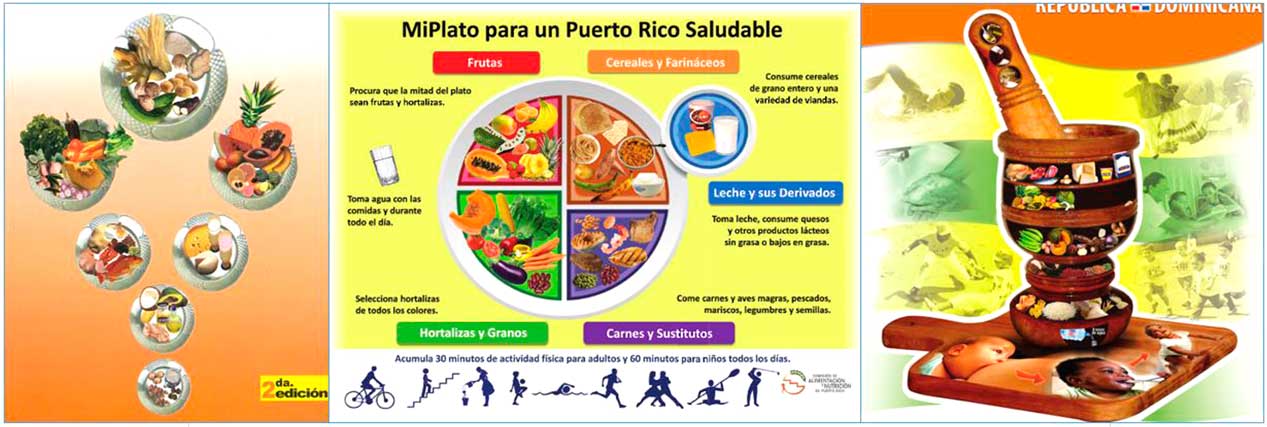
The guidelines also differ in the pictorial representations (Table 2, Fig. 1). While the illustrations agree on the relative importance or prominence of basic grains, fruits and vegetables, they differ in how proportionality is displayed. The Puerto Rican MyPlate is visually more fitting for meal-based food selection, while the Cuban Table and the Dominican Mortar and Pestle provide a more general guidance for daily overall dietary patterns (Fig. 1). While the Mortar and Pestle is an important culinary tool in the region, its use to display proportionality may not be as apparent when compared with the other two illustrations. Differences are also found in food groupings (Table 2) and how (and if) serving recommendations are specified (Table 3). The next section focuses on comparing the key recommendations for the public.
Comparison of daily food group recommendations for the reference group in current dietary guidelines in the Spanish-speaking Caribbean
NSp, not specified; c, cup; tbsp, tablespoon; tsp, teaspoon.
* 2500 kcal=10 460 kJ; 2000 kcal=8368 kJ.
Comparison of key recommendations
The guidelines varied in the number of KR for the public (Table 2). The coding process of these KR yielded sixteen distinct themes across the three documents (two diet-based, ten food-based and four ‘other’; Table 4). Only the Cuban-DG document addressed dietary patterns as part of the KR, by including diet variety and breakfast. The Cuban-DG link this meal to productivity and worker safety, underscoring the personal responsibility of eating breakfast. In contrast, the DR-DG indirectly include breakfast (as well as lunch and dinner) in the KR related to grains (Table 4), discussed further. Breakfast is not addressed in the PR-DG.
Key recommendations, organized by theme and country (author’s translations), in current dietary guidelines in the Spanish-speaking Caribbean
* The present analysis focuses on general population messages; therefore breast-feeding and child nutrition are included in the ‘other’ category.
† Víveres and viandas refer to starchy root crops such as potato, plantain, taro root, etc.
Of the ten food-based recommendations, only four themes overlapped across the three sets of guidelines: the encouragement of fruits and vegetables, encouraging low fat consumption and addressing protein sources. Other overlaps were found between Cuba and the Dominican Republic (sugar) and the Dominican Republic and Puerto Rico (dairy, grains/starches and water; Table 4). There were no unique KR overlaps between the Cuban-DG and the PR-DG. The Cuban KR are the only ones that include salt and the Dominican KR are unique in the inclusion of fortified foods (Table 4).
Commonalities in KR themes do not necessarily translate into how they are addressed. Some differences are small, as in the case of messages concerning fruits and vegetables (Table 4), while others are more noticeable. For instance, both the DR- and the PR-DG address grains and starches as part of the KR, but the DR-DG fail to make the distinction between whole and refined grains found in the PR-DG (also found in the Cuban document). In the Dominican KR, cereals and starches (víveres) are prescribed for all meal times, including breakfast, denoting differences in traditional eating patterns; in this case, the Dominican custom of eating mangú (boiled, mashed plantains) for breakfast.
The greatest differences within these guidelines lie in how they address protein sources, salt, sugar and fat, discussed next.
Eat your protein
Meat is an important part of meals in the Spanish-speaking Caribbean and this is addressed, albeit in different detail, throughout the three sets of KR and the policy documents. Messages concerning the consumption of meat are mostly based on nutritional content (saturated fat and cholesterol in the case of beef and chicken; n-3 fatty acids in the case of fish). However, while the Cuban- and PR-DG emphasize lean cuts of meat, the DR-DG do not make this distinction, encouraging red meat for the reduction of anaemia, along with beans and leafy greens.
Eggs are discussed as a protein source to a lesser extent than meat, with overall recommendations to limit their consumption in the Cuban-DG and PR-DG to avoid high cholesterol, a linkage disputed in recent research( Reference Rong, Chen and Zhu 32 ). Eggs are generally encouraged in the DR-DG, including the KR (Table 4), as a good source of protein, iron and other micronutrients.
Similar differences are found around messages concerning dairy. While the PR-DG encourage low-fat sources of dairy, this distinction is not present in the DR-DG (Table 4), where all dairy is recommended to promote ‘healthy bones and organs’. The Cuban KR do not include dairy, although the food guide illustrates this food group. The DR- and PR-DG encourage dairy consumption as the most important source of calcium, but the DR-DG also mention alternative sources for this mineral. These alternatives sources are also outlined in the Cuban document, where it is noted that ‘calcium requirements for adult men are lower and can be covered through a combination of alternative sources, such as cereals, beans, egg and fish’( 28 ). While not explicit in the Cuban-DG, this recommendation for non-dairy calcium sources is in line with emerging research linking dairy products and prostate cancer risk( Reference Aune, Navarro Rosenblatt and Chan 33 ). While eggs are mentioned as an ‘alternative source’, it is important to note that, except for the shells, they are not good sources of calcium. However, eggs’ vitamin D content can help in the absorption of the mineral.
The Cuban-DG document is the most detailed concerning discussions of animal and vegetable protein sources, including a direct criticism of the overconsumption and preference for meat as part of the traditional Cuban diet. It focuses on soya as an alternative to animal protein, lauding its benefits as a ‘superfood’:
The soybean is considered the most valuable of all beans [...] The phytochemical profile of soy is the most interesting of the plant kingdom and is credited with the greatest potential to reduce the risk of cancer( 28 ).
While the encouragement of vegetable protein sources and a reduction in meat consumption are in line with emerging public health and environmental concerns associated with eating meat( Reference Walker, Rhubart-Berg and McKenzie 34 ), this advice may be linked to the limited meat supply in the country. Additionally, the exaltation of soya is congruent with local strategies to address meat scarcity in the general Cuban population. Since the economic crisis of the 1990s (known as the Special Period in Times of Peace), the government has been mixing soya and ground meat in the food rations( Reference Shurtleff and Aoyagi 35 ). At the same time, it does not conform to the ongoing debates surrounding the science on the benefits and potential harms of this legume( Reference D’Adamo and Sahin 36 ).
The PR-DG also acknowledge plant sources of protein (legumes and seeds), providing some guidance for vegetarians. While legumes constitute an independent food group in the Dominican Republic food guide, these are not as explicitly presented as an alternative protein source for vegetarians.
Limit salt, sugar and fat
Spanish-speaking Caribbean diets are marked by high intakes of salt, sugar and fat( Reference Colón-Ramos, Pérez-Cardona and Monge-Rojas 16 – Reference Porrata-Maury 18 ). However, the three guidelines differ in the extent these pressing issues are addressed. For instance, they are mostly missing from the current Puerto Rican KR (except for the mention of low-fat protein and dairy sources), and only sugar and fat are addressed in the Dominican KR (Table 4). The Cuban-DG are consistently more specific in how they address these, using the results of the local consumption survey to frame their advice. This is accompanied with practical culinary tips to diminish the consumption of fats, sugar and salt during cooking and highlights ultra-processed industrial foods as hidden food sources for these, a message largely missing from the other two sets of guidelines.
While the Dominican KR include sugar and fat, no further discussion is found in the document, beyond asking the public to ‘avoid’ frying during food preparation. In the PR-DG, fats are mostly addressed as a condiment and nutrient (including trans fats). While sources of fats (i.e. fried foods) were included in previous guidelines( Reference Palacios and Angleró 26 ), the current document lacks this level of specificity, despite the high consumption of fried foods and fast foods on the island( Reference Colón-Ramos, Pérez-Cardona and Monge-Rojas 16 ). Sugar consumption is not directly addressed in the current PR-DG either.
The Cuban-DG are unique among the three in addressing salt as part of the KR (Table 4), advising against the use of salt at the table, a custom also present in Puerto Rico and the Dominican Republic. While not included in the KR, the three policy documents mention salt as a condiment to decrease. However, in the DR-DG salt is also indirectly encouraged as a source of iodine:
Always consume iodized salt and seafood […] limiting to the minimum needed for preparations or cooking foods( 29 ).
The emphasis on iodized salt corresponds to the inclusion of fortified foods in the KR (Table 4), absent from the other two sets of guidelines, and to a concurrent public health campaign, Consuma sal yodada, o nada (Consume iodized salt or nothing), established in collaboration with UNICEF to address the prevalent use of non-iodized salt in the country (despite its prohibition) and the persisting thyroid issues coming from the inadequate intake of this mineral at the time( 37 ). The underscoring of salt as a source of iodine could also be a potential source for confusion regarding dietary advice concerning this condiment, as one to decrease, but containing a nutrient that needs to be consumed. At the same time, a recent analysis has shown that actual intake of iodine is excessive, coming from the use of imported bouillon cubes and powder soups made with iodized salt( 38 ), calling for a change in messaging and a revision of the document taking these new data into consideration.
Water and liquid calories
The DR- and PR-DG encourage water as part of the KR (Table 4) and include it as part of the pictorial representations (Fig. 1). Water is encouraged over sugar-sweetened beverages, especially in the PR-DG. The Cuban-DG also discourage sugar-sweetened beverage and beer consumption, as part of messaging dissuading the consumption of industrially processed foods. However, water is not addressed in the Cuban guidelines as a beverage, but as part of cooking, ingredient substitution, hygiene, and food production.
Overview of results
The present comparison revealed differences that mirror the contrasting socio-economic and political situations in the region. The Spanish-speaking Caribbean region shares concerns over high intakes of fat, sugar and salt, a preference for animal sources of protein and a low intake of fruits and vegetables. The present analysis revealed that despite these important overlaps, the guidelines coincided only in the promotion of fruits and vegetables and the guidance (albeit different) concerning animal protein sources and fats (Fig. 2). There were discernible differences in level of specificity, especially when addressing issues of concern (salt, sugar and fat), as well as the different populations addressed.
Overlapping (a) food and nutrition issues and (b) key recommendation themes in dietary guidelines in the Spanish-speaking Caribbean (NCD, non-communicable diseases; F&V, fruit and vegetable; U5, under 5 years of age; MN, micronutrient; PA, physical activity)
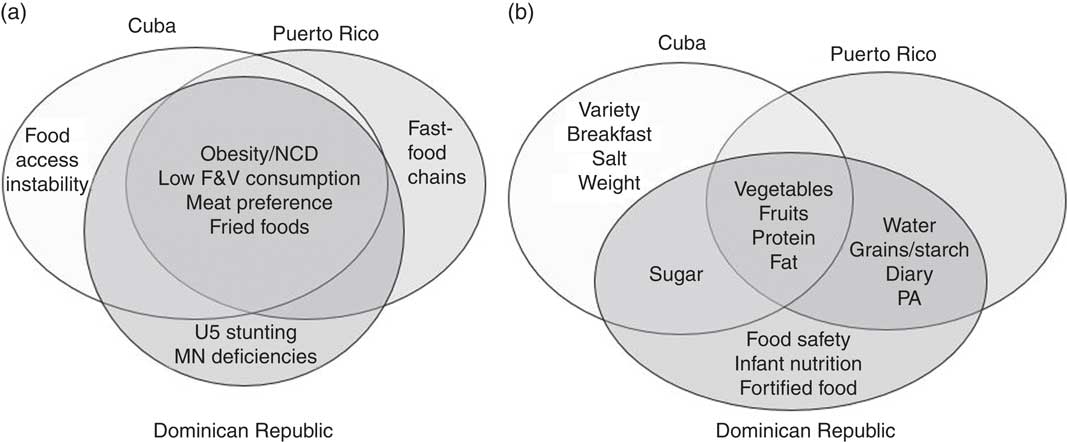
The DR- and Cuban-DG were more in tune with local food and nutrition issues. The DR-DG document reflected the country’s dual concern with issues of undernutrition and overnutrition. The Cuban-DG made active use of local consumption data and collaborations with the culinary sector, being the most specific of the three. These approaches differ greatly from the current PR-DG. As an adapted version of the USDA Dietary Guidelines, the PR-DG missed pressing issues of concern, namely the high consumption of fatty foods and fast foods( Reference Colón-Ramos, Pérez-Cardona and Monge-Rojas 16 ), despite being addressed in previous iterations of these guidelines( Reference Palacios and Angleró 26 ). This is an important, and perhaps unintended, consequence of the current political situation of the island, as a territory of the USA, and an example of how such status can affect local policy making and the framing of nutrition advice.
Lastly, the analysis revealed areas of improvement in light of emerging nutrition science. This was the case in advice concerning egg, meat and soya consumption. While the PR-DG will undergo a revision after the upcoming publication of the USDA 2015 Dietary Guidelines, no such process is currently planned for Cuba and the Dominican Republic.
Conclusion
The present study underscored the importance of context in the framing of dietary advice and the influence of national socio-economic and political situations on nutrition policy and education efforts. The results contribute to inform efforts to improve nutrition communication with the public in the Spanish-speaking Caribbean, including the importance of revising guidelines to account for current nutrition scientific advances. The commonalities in public health nutrition issues in the region present an opportunity for collaboration and resource sharing within these three countries. Moreover, it can also be applied to ameliorate health disparities among migrant communities from the Spanish-speaking Caribbean by gaining a better understanding on how experts frame and address these issues locally.
Future studies should address the information gap on the reach, use and effectiveness of the dietary guidelines included in the present analysis. This can include a comparative analysis evaluating the effectiveness of these documents, as well as the public reception and service provider use of the guidelines.
Acknowledgements
Acknowledgements: The author wishes to acknowledge valuable feedback from Marion Nestle, Professor of Nutrition, Food Studies and Public Health at New York University (NYU) and NYU Faculty Fellows Sophia Domokos and Natasha Wilson. Financial support: This work was supported by the NYU Postdoctoral and Transition Program for Academic Diversity. The funder had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: The author formulated the research question, designed the study, carried out the analysis and wrote the present manuscript. Ethics of human subject participation: Ethical approval was not required.