


Introduction
Infertility, as delineated by the World Health Organization (WHO), is characterized by the inability to achieve pregnancy following 12 months of regular, unprotected sexual intercourse. This condition affects approximately 15% of couples globally, with male factors contributing to 30–40% of cases. Recent global estimates continue to support this prevalence, underscoring infertility as a significant public health concern (WHO, 2023). The aetiology of male infertility is complex and multifactorial, involving oxidative stress, genetic predisposition, environmental exposures, endocrine disruption, metabolic disorders, and lifestyle factors. Growing evidence also highlights the contribution of pharmacological agents, including psychopharmacological drugs, as potential modulators of male reproductive function (Agarwal et al., Reference Agarwal, Mulgund, Hamada and Chyatte2015).
Over the past decades, mounting evidence has suggested a progressive decline in semen quality at the population level. A comprehensive meta-analysis by Levine et al. (Reference Levine, Jørgensen, Martino-Andrade, Mendiola, Weksler-Derri, Mindlis, Pinotti and Swan2023) reported significant temporal reductions in sperm concentration and total sperm count across multiple continents. While semen analysis standardized according to the WHO laboratory manual, 6th edition (2021) remains the cornerstone of fertility evaluation, conventional parameters such as concentration, motility, and morphology may not fully reflect sperm functional competence, particularly genomic integrity and chromatin organization.
Environmental and occupational exposures have been increasingly implicated in male reproductive pathology. Endocrine-disrupting chemicals (EDCs), including bisphenol A (BPA), phthalates, organophosphate pesticides, heavy metals, and persistent organic pollutants, can interfere with androgen receptor signalling, alter hypothalamic–pituitary–gonadal axis regulation, and induce oxidative stress–mediated testicular damage (Gore et al., Reference Gore, Chappell, Fenton, Flaws, Nadal, Prins, Toppari and Zoeller2022; Skakkebæk et al., Reference Skakkebæk, Lindahl-Jacobsen, Levine, Andersson, Jørgensen, Main, Liew, Priskorn, Holmboe, Bräuner, Almstrup, Franca, Znaor, Kortenkamp, Hart and Juul2022). Professional exposure in agriculture, plastics manufacturing, and chemical industries may therefore contribute to reproductive alterations observed at the population level.
Oxidative stress represents a central mechanistic pathway linking environmental, metabolic, and pharmacological exposures to sperm dysfunction. Due to their limited cytoplasmic antioxidant defences and high content of polyunsaturated fatty acids, spermatozoa are particularly susceptible to reactive oxygen species (ROS). Excess ROS leads to lipid peroxidation, mitochondrial impairment, DNA strand breaks, and defective chromatin condensation (Aitken and Baker, Reference Aitken and Baker2004; Venkatesh et al., Reference Venkatesh, Shamsi, Deka, Saxena, Kumar and Dada2011). These molecular alterations compromise fertilization capacity and are associated with impaired embryo development and adverse reproductive outcomes.
Beyond conventional semen parameters, SDF and abnormalities in chromatin packaging, including protamine deficiency, are now recognized as independent predictors of fertilization failure, recurrent pregnancy loss, and reduced success in assisted reproductive technologies (Agarwal et al., Reference Agarwal, Majzoub, Esteves, Ko, Ramasamy and Zini2016; Reference Agarwal, Mulgund, Hamada and Chyatte2015). Importantly, elevated SDF levels may be present even when standard semen parameters fall within reference ranges, highlighting the limitations of routine semen analysis.
Psychopharmacological agents such as selective serotonin reuptake inhibitors (SSRIs), antipsychotics, and mood stabilizers are widely prescribed globally. Recent systematic reviews and meta-analyses indicate that SSRIs may negatively affect sperm concentration, motility, morphology, and DNA integrity (Xu et al., Reference Xu, Liang, Chen, Li, Li, Hong and Xie2022; Alsabhan et al., Reference Alsabhan, Almalag, Alnuaim, Albaker and Alaseem2024). Proposed mechanisms include serotonergic modulation of the hypothalamic pituitary gonadal axis, mitochondrial dysfunction, oxidative stress induction, and interference with chromatin remodelling processes. Given the increasing prevalence of psychiatric disorders and long-term pharmacotherapy, elucidating the reproductive impact of these agents is of substantial clinical importance.
Taken together, these findings underscore the importance of evaluating not only classical semen characteristics but also advanced markers of sperm genomic integrity and chromatin organization. The present study therefore aims to assess the impact of psychopharmacological agents on sperm quality parameters, DNA integrity, and chromatin architecture, thereby providing mechanistic insight into drug-associated reproductive alterations relevant to fertilization potential.
Aim
The primary objective of this study is to elucidate the impact of psychopharmacological drugs on sperm parameters, DNA integrity, and chromatin structure, with a particular emphasis on the expression of PKA in sperm cells. This investigation seeks to enhance our understanding of the potential reproductive risks posed by these medications and to identify underlying mechanisms that could inform future therapeutic strategies.
Materials and methods
Study design and participants
This study was designed to investigate the effects of psychopharmacological drugs on reproductive health. The cohort was divided into two groups: 14 individuals undergoing treatment with psychopharmacological drugs (user group) and 15 individuals with no history of such drug use (non-user group). All participants were recruited from the general population, and eligibility criteria included males aged 20–40 years, with no underlying chronic illnesses or history of reproductive surgery.
Ethical considerations
Ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Istanbul Medipol University with decision number 508, dated 16.07.2019 (Appendix 9). Written informed consent was obtained from the patients. All procedures adhered to the Declaration of Helsinki. Informed consent was obtained from all participants, ensuring their voluntary participation and confidentiality of their data.
Sample collection
Semen samples were obtained by masturbation into sterile containers following 3–5 days of sexual abstinence. After liquefaction at room temperature, semen analysis was performed according to the WHO laboratory manual, 6th edition (2021). Sperm concentration, total count, motility, and morphology were assessed using standardized WHO criteria.
To ensure consistency and reduce inter-observer variability, all samples were analysed by trained personnel using standardized counting procedures. At least two independent microscopic evaluations were performed when necessary to confirm borderline results.
Sperm parameters analysis
Semen analysis was conducted to measure key parameters including volume, concentration, sperm count, motility, and morphology. Volume was measured using a graduated cylinder, while concentration and count were determined using a haemocytometer (World Health Organization 2021). Motility and morphology were assessed using light microscopy, following the WHO 2021 guidelines (World Health Organization 2021) (refer to Table 1).
Mean sperm parameters of patients drug users and non-users

Table 1. Long description
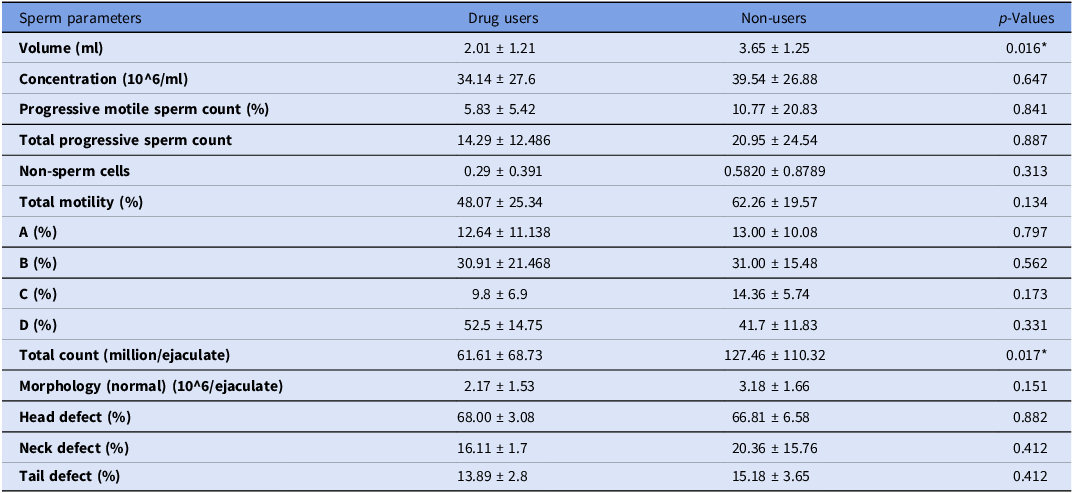
The table presents a comparison of sperm parameters between drug users and non-users, detailing volume, concentration, progressive motile sperm count, total progressive sperm count, non-sperm cells, total motility, and various motility percentages. It also includes total count, morphology, and defect percentages for head, neck, and tail. The table has 14 rows and 4 columns, with headers for sperm parameters, drug users, non-users, and p-values. Notable trends include significant differences in volume and total count, with drug users showing lower values. The p-values indicate statistical significance for volume and total count, marked by an asterisk.
Note: Data are presented as mean ± SD. p < 0.05 indicates statistical significance.
DNA fragmentation analysis
DNA fragmentation was evaluated using the TUNEL assay according to the manufacturer’s protocol. Spermatozoa were fixed in 4% paraformaldehyde (PFA) for 20 min at room temperature, washed three times with phosphate-buffered saline (PBS), and permeabilized as recommended by the kit instructions. Samples were then incubated with TUNEL reaction mixture at 37°C for 60 minin a humidified chamber protected from light. After washing, slides were counterstained and examined using fluorescence/confocal microscopy. For each subject, at least 100 spermatozoa were evaluated.
Definition of positivity
Spermatozoa exhibiting distinct nuclear fluorescence exceeding background signal were classified as TUNEL-positive. The percentage of DNA-fragmented spermatozoa was calculated by dividing the number of TUNEL-positive sperm by the total number of evaluated sperm cells and expressed as a percentage. Background fluorescence was assessed in control slides processed without the labelling enzyme to define baseline signal intensity.
Controls
Negative control slides were prepared by omitting the terminal deoxynucleotidyl transferase (TdT) enzyme during incubation to verify specificity of labelling and establish background fluorescence levels. All staining procedures were performed in parallel under identical conditions to minimize technical variability.
Troubleshooting and quality control
To prevent high background fluorescence, thorough PBS washing steps were performed, and slides were protected from drying during incubations. Samples with excessive cellular overlap or inadequate fixation were excluded from analysis. Fluorescence intensity settings were kept constant across samples to ensure comparability.
Chromatin structure analysis
(Toluidine Blue Staining)Chromatin structural integrity was evaluated using the Toluidine Blue staining method. Toluidine Blue dye binds to the phosphate groups of the DNA chain, indicating the chromatin condensation status of the sperm and indirectly reflecting DNA fragmentation. Air-dried sperm smear samples were fixed in 96% ethanol (Merck, Germany) and acetone (BDH Prolabo, France) at 4°C for 1 h. The samples were then hydrolysed in 0.1 Normal HCL (Merck K50227117 818, Germany) at + 4°C for 5 min to allow the dye to bind to the phosphate groups, followed by washing with distilled water. Subsequently, the samples were stained in 0.05% Toluidine Blue (Empire Genomics, USA) for 10 min. Pale blue sperm cells were considered unstained (with intact chromatin structure), while dark blue or purple sperm cells were considered stained (with abnormal chromatin structure). At least 100 cells were counted per sample, and the percentages of stained and unstained sperm were calculated. Stained samples were examined under a light microscope, and chromatin integrity was quantified based on the staining intensity and pattern (refer to Table 2).
Mean sperm parameters related to DNA fragmentation and chromatin structure integrity in patients using and not using medication

Table 2. Long description
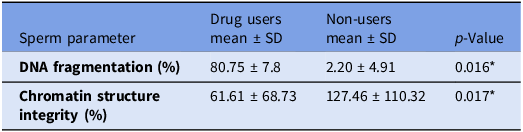
The table presents a comparison of sperm parameters between drug users and non-users, focusing on DNA fragmentation and chromatin structure integrity. It consists of three columns: Sperm parameter, Drug users mean ± SD, Non-users mean ± SD, and p-Value. The rows detail DNA fragmentation percentage and chromatin structure integrity percentage. Drug users show higher DNA fragmentation at 80.75 ± 7.8 percentage compared to non-users at 2.20 ± 4.91 percentage, with a p-value of 0.016 indicating statistical significance. Chromatin structure integrity is lower in drug users at 61.61 ± 68.73 percentage compared to non-users at 127.46 ± 110.32 percentage, with a p-value of 0.017 also indicating statistical significance.
Note: Data are presented as mean ± SD. p < 0.05 indicates statistical significance.
Definition of abnormal chromatin/decondensation
Spermatozoa exhibiting dark blue or purple metachromatic staining were classified as having abnormal chromatin condensation, whereas light blue staining was considered indicative of relatively normal chromatin packaging. Results were expressed as the percentage of sperm with abnormal staining.
Controls and standardization
All slides were processed simultaneously using identical fixation, hydrolysis, and staining times to ensure reproducibility. A reference slide with expected normal staining pattern was included in each staining batch to confirm staining consistency and dye performance.
Troubleshooting
To avoid overstaining or false-positive results, hydrolysis time and dye concentration were strictly standardized. Slides showing uneven staining, excessive debris, or technical artefacts were reprocessed when necessary.
PKA protein expression analysis
PKA protein expression in sperm cells was investigated through immunohistochemistry, following the methodology outlined by Dell’Acqua and Scott in “The Journal of Biological Chemistry” (Dell’Acqua and Scott, Reference Dell’Acqua and Scott1997). This method involved the use of specific antibodies to detect PKA within the sperm cells, followed by visualization using a secondary antibody conjugated with a fluorescent marker (Dell’Acqua and Scott, Reference Dell’Acqua and Scott1997). The distribution and intensity of PKA expression were analysed using fluorescence microscopy, with particular attention to potential differences between the user and non-user groups (Dell’Acqua and Scott, Reference Dell’Acqua and Scott1997). The prepared samples were fixed in 4% PFA at room temperature for 20 min. They were then washed three times for 5 min each with PBS (Phosphate Buffered Solution). A 3% H2O2 (Hydrogen Peroxide) solution in methanol was prepared (45 ml methanol + 5 ml 30% H2O2) and incubated at room temperature for 20 min. For antigen retrieval, a Citrate buffer solution (Bio Optica 15M-103, Italy) was prepared, and the samples were incubated in this Citrate buffer solution at 800 W until boiling, followed by 10 min of boiling in a 200-watt microwave (Samsung, Turkey). The samples were then allowed to cool for 30 min. The samples were analysed microscopically. Each slide was assessed based on the presence or absence of expression in specific regions of the spermatozoa, namely the head, acrosome, neck, and tail. The scoring system was as follows: a score of 1 indicated no expression, a score of 2 indicated expression in two regions, a score of 3 indicated expression in three regions, and a score of 4 indicated expression in all regions. In total, 100 spermatozoa were evaluated using this method.
Negative control slides were prepared by omitting the primary antibody to confirm staining specificity and assess background fluorescence. Imaging parameters were kept constant across all samples to ensure reliable comparison.
Statistical analysis
Data were subjected to rigorous statistical analysis using SPSS software (version 24.0). Descriptive statistics were calculated for all variables, and group comparisons were made using independent sample t-tests. Statistical significance was set at p < 0.05, and results were presented as mean ± standard deviation (SD).
Results
Comparison of conventional semen parameters between drug users and non-users
Conventional semen parameters for drug users (n = 14) and non-users (n = 15) are presented in Table 1.
Semen volume was significantly reduced in the drug-user group compared with non-users (2.01 ± 1.21 ml vs 3.65 ± 1.25 ml; p = 0.016). Total sperm count (million/ejaculate) was also significantly lower in drug users (61.61 ± 68.73 vs 127.46 ± 110.32; p = 0.017).
No statistically significant differences were observed between groups in sperm concentration (34.14 ± 27.6 vs 39.54 ± 26.88; p = 0.647). Similarly, progressive motile sperm count (%) did not differ significantly (5.83 ± 5.42 vs 10.77 ± 20.83; p = 0.841), nor did total progressive sperm count (14.29 ± 12.49 vs 20.95 ± 24.54; p = 0.887).
Total motility was lower in drug users (48.07 ± 25.34%) compared with non-users (62.26 ± 19.57%), although this difference did not reach statistical significance (p = 0.134). No statistically significant differences were detected in motility subclasses A (p = 0.797), B (p = 0.562), C (p = 0.173), or D (p = 0.331).
Morphological evaluation revealed no significant differences in normal morphology (2.17 ± 1.53 vs 3.18 ± 1.66; p = 0.151). Likewise, the prevalence of head defects (p = 0.882), neck defects (p = 0.412), and tail defects (p = 0.412) did not differ significantly between groups. Non-sperm cell counts were comparable (p = 0.313).
DNA fragmentation analysis
DNA fragmentation assessed by TUNEL assay is summarized in Table 2.
The percentage of TUNEL-positive spermatozoa was significantly higher in the drug-user group compared to non-users (80.75 ± 7.8% vs 2.20 ± 4.91%; p = 0.016) as illustrated in Figure 1.
(A). illustrates the detection of DNA fragmentation in human sperm utilizing the TUNEL assay. Panel a depicts the control group. Panel b shows the experimental group stained with DAPI. Panel c presents the experimental group with TUNEL (+) cells, Finally, panel d displays a merged image of panels b and c. Blue Arrow identifies sperm cells with positive TUNEL staining indicating DNA fragmentation. Red Arrow identifies sperm cells stained with DAPI. (B). The bar graph in Figure 1B depicts the percentage of DNA damage in human sperm across three groups: Control, AST (Asthenozoospermia), and OAT (Oligoasthenoteratozoospermia). The Control group has the lowest DNA damage, while the AST and OAT groups show higher levels, with OAT having the highest. Error bars represent the standard error of the mean.

The distribution of fragmentation values demonstrated markedly elevated DNA damage among individuals exposed to psychopharmacological medication.
Chromatin structure integrity
Chromatin integrity assessed by toluidine blue staining is presented in Table 2 and representative staining patterns are shown in Figure 2.
Chromatin structure in sperm cells stained with TOLUIDINE BLUE dye while (B) is drug users and (A) is non-users at a magnification of 100x. In Figure 3, we depict the chromatin structure within sperm cells, visualized using TOLUIDINE BLUE dye. Within the group of patients using the drug, the labelling is as follows. Black Arrow (tb+) denotes chromatin structures with positive TOLUIDINE BLUE staining. Red Arrow (tb−) denotes chromatin structures with negative TOLUIDINE BLUE staining.

Average chromatin integrity in drug users and non-users (Magnification: 100x).

A statistically significant difference in chromatin structure parameters was observed between drug users and non-users (p = 0.017). Drug users demonstrated altered chromatin integrity values compared with controls.
PKA immunostaining analysis
Alterations in PKA expression patterns were observed between drug users and non-users. Representative immunostaining images demonstrating PKA localization are presented in Figure 4.
Descriptive analysis of drug subgroups
Average semen parameters stratified by drug class are presented in Table 3. Due to the limited number of participants in several subgroups (n = 1 in some categories), no inferential statistical comparisons were performed at the individual drug level.
Average values of sperm parameters for drug groups

Table 3. Long description
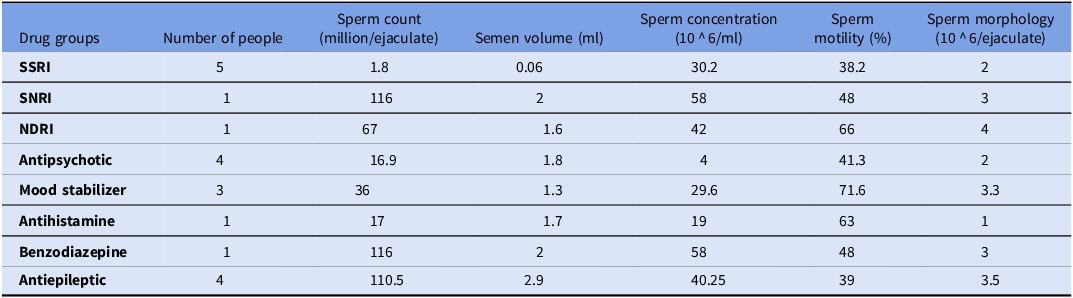
The table presents average semen parameters stratified by drug class, including the number of people, sperm count in millions per ejaculate, semen volume in milliliters, sperm concentration in millions per milliliter, sperm motility in percentage, and sperm morphology in millions per ejaculate. The drug groups listed are SSRI, SNRI, NDRI, Antipsychotic, Mood stabilizer, Antihistamine, Benzodiazepine, and Antiepileptic. Notable trends include the highest sperm count observed in the Antiepileptic group with 110.5 million per ejaculate and the lowest in the SSRI group with 1.8 million per ejaculate. Semen volume varies, with the highest being 2.9 milliliters in the Antiepileptic group and the lowest being 0.06 milliliters in the SSRI group. Sperm concentration is highest in the SNRI and Benzodiazepine groups at 58 million per milliliter, while it is lowest in the Antihistamine group at 19 million per milliliter. Sperm motility is highest in the Mood stabilizer group at 71.6 percentage and lowest in the SSRI group at 38.2 percentage. Sperm morphology is highest in the Antiepileptic group at 3.5 million per ejaculate and lowest in the Antihistamine group at 1 million per ejaculate.
Descriptive data indicate variability across drug categories in sperm count, semen volume, concentration, motility, and morphology. However, given the small subgroup sample sizes, these findings should be interpreted cautiously and are presented for descriptive purposes only.
Discussion
The present study investigated the impact of psychopharmacological drug use on conventional semen parameters, SDF, and chromatin structure integrity. The findings demonstrate that individuals exposed to psychopharmacological medications exhibited significantly reduced semen volume and total sperm count, alongside markedly elevated DNA fragmentation and altered chromatin integrity compared to non-users.
Conventional semen parameters
Although sperm concentration and motility did not reach statistical significance between groups, total sperm count and semen volume were significantly reduced in drug users. These findings are partially consistent with previous reports suggesting that certain psychotropic medications may negatively influence spermatogenesis and seminal fluid production (Xu et al., Reference Xu, Liang, Chen, Li, Li, Hong and Xie2022; Alsabhan et al., Reference Alsabhan, Almalag, Alnuaim, Albaker and Alaseem2024). Large-scale meta-analyses have highlighted that global declines in sperm count likely reflect multifactorial influences, including environmental exposures, metabolic factors, and pharmacological agents (Levine et al., Reference Levine, Jørgensen, Martino-Andrade, Mendiola, Weksler-Derri, Mindlis, Pinotti and Swan2023). Therefore, the reductions observed in the present cohort may represent part of a broader vulnerability of male reproductive physiology under long-term medication exposure.
DNA fragmentation and genomic integrity
One of the most prominent findings of this study is the markedly elevated SDF in drug users. SDF is increasingly recognized as an independent predictor of fertilization failure, impaired embryo development, and adverse reproductive outcomes (Agarwal et al., Reference Agarwal, Majzoub, Esteves, Ko, Ramasamy and Zini2016; Reference Agarwal, Mulgund, Hamada and Chyatte2015). Elevated SDF has been strongly associated with reduced blastocyst formation rates, lower implantation success, and increased miscarriage risk (Agarwal et al., Reference Agarwal, Panner Selvam, Baskaran and Cho2019). Moreover, oxidative stress–mediated DNA strand breaks and mitochondrial dysfunction are considered central mechanisms driving genomic instability in sperm cells (Aitken and Baker, Reference Aitken and Baker2004; Venkatesh et al., Reference Venkatesh, Shamsi, Deka, Saxena, Kumar and Dada2011).
These mechanisms provide biological plausibility for the significantly elevated DNA fragmentation observed among psychopharmacological drug users in the present study.
Chromatin structure alterations
Alterations in chromatin structure were also detected in drug users. Proper chromatin packaging, including adequate protamination and histone replacement, is essential for protecting paternal DNA during fertilization. Chromatin condensation defects have been associated with increased susceptibility to oxidative damage and impaired reproductive outcomes (Agarwal et al., Reference Agarwal, Mulgund, Hamada and Chyatte2015).
Furthermore, defective chromatin packaging may influence epigenetic regulation and early embryonic gene activation (Carrell and Hammoud, Reference Carrell and Hammoud2010). Environmental and pharmacological exposures have been shown to disrupt chromatin remodelling pathways, potentially contributing to persistent alterations in sperm genomic integrity (Skakkebæk et al., Reference Skakkebæk, Lindahl-Jacobsen, Levine, Andersson, Jørgensen, Main, Liew, Priskorn, Holmboe, Bräuner, Almstrup, Franca, Znaor, Kortenkamp, Hart and Juul2022). The findings of altered chromatin integrity in drug users therefore extend beyond structural abnormalities and may carry implications for embryo development.
Mechanistic considerations
The mechanisms underlying these findings are likely multifactorial. Psychopharmacological drugs may influence the hypothalamic–pituitary–gonadal axis, alter testosterone and prolactin levels, induce oxidative stress, and interfere with intracellular signalling pathways such as the cAMP–PKA axis. Additionally, oxidative and inflammatory pathways triggered by pharmacological exposure may exacerbate genomic instability (Gore et al., Reference Gore, Chappell, Fenton, Flaws, Nadal, Prins, Toppari and Zoeller2022;).
These overlapping mechanisms may explain the combined deterioration in sperm count, DNA integrity, and chromatin structure observed in the present study.
Clinical implications
From a clinical standpoint, the present findings highlight the importance of assessing advanced sperm quality markers in men undergoing long-term psychopharmacological treatment. Conventional semen analysis alone may underestimate reproductive risk. Incorporating DNA fragmentation assessment into fertility evaluation may provide additional prognostic value, particularly in cases of unexplained infertility (Agarwal et al., Reference Agarwal, Majzoub, Esteves, Ko, Ramasamy and Zini2016).
Given the increasing prevalence of psychiatric disorders and prolonged pharmacological management, fertility counselling should be considered for men of reproductive age initiating long-term psychotropic therapy.
Limitations
Several limitations should be acknowledged. The sample size was relatively small, particularly within individual drug subgroups, limiting statistical power for subgroup analyses. The cross-sectional design does not allow causal inference. Additionally, hormonal profiles, oxidative stress biomarkers, and inflammatory parameters were not assessed, restricting mechanistic interpretation.
Perspectives and future directions
Future studies should include larger, longitudinal cohorts to clarify dose-dependent and duration-dependent effects of psychopharmacological drugs on male reproductive health. Prospective investigations evaluating reversibility of sperm DNA damage following medication discontinuation would provide valuable clinical insight.
Further research should also explore epigenetic consequences of chronic psychopharmacological exposure, as accumulating evidence suggests that sperm epigenome alterations may have intergenerational implications (Donkin and Barrès, Reference Donkin and Barrès2020; Carrell and Hammoud, Reference Carrell and Hammoud2010). Evaluating assisted reproductive technology outcomes in exposed individuals may further clarify the clinical relevance of elevated DNA fragmentation and chromatin abnormalities.
Conclusion
The present study demonstrates that psychopharmacological drug exposure is associated with significant alterations in sperm genomic integrity and chromatin organization, alongside reductions in selected conventional semen parameters. Notably, the marked increase in SDF observed among drug users suggests that psychopharmacological treatment may compromise fertilization potential beyond what is detectable through routine semen analysis alone.
These findings reinforce the growing recognition that advanced sperm quality markers – particularly DNA fragmentation and chromatin condensation status – provide clinically meaningful information regarding male reproductive competence. The observed alterations in genomic integrity raise important considerations regarding embryo development, implantation potential, and possible long-term reproductive outcomes.
Given the increasing prevalence of psychiatric disorders and the widespread, often long-term use of psychotropic medications in reproductive-age men, the potential reproductive implications warrant careful clinical attention. Incorporating genomic integrity assessment into fertility evaluation protocols may improve risk stratification and patient counselling in this population.
Although the present study is limited by sample size and cross-sectional design, it provides important preliminary evidence supporting a biological association between psychopharmacological exposure and impaired sperm genomic stability. Future large-scale, longitudinal investigations are required to determine causality, dose–response relationships, reversibility following treatment modification, and potential epigenetic or intergenerational effects.
Overall, this study contributes to the evolving understanding of pharmacological influences on male reproductive health and underscores the need for integrated clinical and molecular approaches in the evaluation of drug-associated fertility alterations.
Immunohistochemical analysis of PKA protein in sperm from drug user group and non-user group (Magnification: 100x). In A and B panels, we present the results of an immunohistochemical analysis of PKA (Protein Kinase A) protein in the sperm of drug user group who was under the influence of the psychopharmacological drug. The black arrow points to the presence of PKA protein expression in the neck region of the sperm. Conversely, the Red arrow highlights PKA protein expression observed in the tail region of the sperm. In C and D panels, we present Immunohistochemical analysis of PKA protein in sperm from non-user group (Magnification: 100x). Black arrows points to presence of PKA protein presence neck and head regions.

Competing interests
The authors declare that they have no conflicts of interest.
Funding
None.





 Open access
Open access