


Depression is a common mental disorder that characterised by persistent low mood and anhedonia, often accompanied by changes in self-worth, concentration, energy, sleep, appetite and weight. Reference Harding, Pushpanathan, Whitworth, Nanthakumar, Bucks and Skinner1 It is highly prevalent, affects people across all age groups and is more prevalent in women compared with the general population. Reference Vos, Allen, Arora, Barber, Bhutta and Brown2 Depression carries significant personal, social and economic burden including increased expenditure on healthcare, reduced productivity and risk of depression complications, such as cardiovascular disease, social isolation, anxiety, diabetes, sleep disorder breathing and chronic obstructive lung disease. Reference Fallon, Davies, Silverio, Jackson, De Pascalis and Harrold3–Reference Mercedes, Nunes da Silva, Carregaro and Miasso5
The first-line treatments for mild to moderate depression often include pharmacological and psychological interventions, alone or in combination, and the most commonly used psychological intervention is cognitive–behavioural therapy (CBT). 6 CBT is an effective ‘talking’ therapy for treating depression, and requires intensive training, ongoing supervision and time commitments from trained and qualified mental health professionals. Reference Gautam, Tripathi, Deshmukh and Gaur7–Reference Richards, Rhodes, Ekers, McMillan, Taylor and Byford9 In Australia, access to CBT is particularly limited in rural and very remote communities, where shortages of trained mental health practitioners and geographic isolation restrict access to mental health services. These barriers contribute to delays in seeking care and greater unmet mental health needs, underscoring the need for more accessible treatment options. Reference Fennell, Hull, Jones and Dollman10,Reference Moody, Loi, Rock, Usher and Rice11
Behavioural activation has emerged as an alternative option to CBT, and is one of the psychological therapies recommended in several treatment guidelines for the treatment of subthreshold, mild or moderate depression in adults. 6,12,Reference Malhi, Bell, Bassett, Boyce, Bryant and Hazell13 Behavioural activation is a structured psychological intervention that focuses on increasing access to adaptive behaviours, reducing avoidance behaviours that inhibit access to positive reinforcement, and resolving barriers to activation. Reference Dimidjian, Goodman, Sherwood, Simon, Ludman and Gallop14 It is considered less complex than CBT and has demonstrated similar effectiveness in treating subthreshold, mild and moderate depression. Reference Richards, Rhodes, Ekers, McMillan, Taylor and Byford9 Several recent meta-analyses have reported that behavioural activation is effective in reducing depressive symptoms and can be applied across various conditions and target populations. Reference Cuijpers, Karyotaki, Harrer and Stikkelbroek15–Reference Yisma, Walsh, Steen, Gray, Dennis and Gillam19 For example, a systematic review targeting adults with comorbid non-communicable diseases concluded that behavioural activation may be a viable option for this population, highlighting its simplicity, adaptability and relevance for individuals whose physical health conditions may limit more complex therapeutic modalities. Reference Yisma, Muyambi, Walsh, Othman, Gray and Tan17 These findings suggest that behavioural activation is an evidence-based intervention whose core behavioural principles, such as engagement in meaningful activities and reinforcement of positive behaviours, can be adapted across diverse contexts. In addition, a recent Cochrane review of 53 randomised controlled trials (RCTs) involving 5495 participants found moderate certainty evidence that behavioural activation had greater short-term efficacy compared with treatment as usual for adults with depression, and found no significant differences in efficacy between behavioural activation and CBT. Reference Uphoff, Ekers, Robertson, Dawson, Sanger and South20
Mood monitoring and activity scheduling are common behavioural activation techniques and have been shown to be effective in helping individuals identify patterns in their mood, increase engagement in rewarding activities and reduce depressive symptoms. Reference Kanter, Manos, Bowe, Baruch, Busch and Rusch21 These techniques are simple to teach and implement, and suit delivery by non-specialist providers. Reference Kanter, Manos, Bowe, Baruch, Busch and Rusch21 Utilising behavioural activation in preventive interventions to manage and control early depressive symptoms may help mitigate the individual, family and societal costs associated with the burden of depression. Limited access to mental health professionals has led to a growing interest in whether non-specialist workers, such as lay workers, can deliver low-intensity mental health interventions like behavioural activation. Reference Barnett, Puffer, Ng and Jaguga22 According to the World Health Organization (WHO), lay workers are community members who have received some training to promote health or to perform some healthcare services, but are not healthcare professionals. 23 A previous Cochrane review, including 82 RCTs, examined the effect of interventions delivered by lay workers to improve maternal or child health or infectious disease management. Reference Lewin, Munabi-Babigumira, Glenton, Daniels, Bosch-Capblanch and van Wyk24 The review concluded that lay workers offer promising benefits in promoting immunisation uptake and breastfeeding, improving tuberculosis treatment outcomes and reducing child morbidity and mortality compared with usual care. For other health issues (e.g. HIV/AIDS prevention, malaria control), evidence was insufficient to draw conclusions about the effects of interventions delivered by lay workers. Reference Lewin, Munabi-Babigumira, Glenton, Daniels, Bosch-Capblanch and van Wyk24 Although the use of lay workers in the before mentioned health outcomes has been explored, there is currently no systematic reviews examining the effectiveness of behavioural activation when delivered by lay workers to adults with depression. Therefore, the aim of this systematic review was to examine the effectiveness of lay worker-delivered behavioural activation in reducing depressive symptoms in adults with depression.
In this review, we will use the definitions of non-specialist workers and lay workers as provided by the WHO and Uphoff et al. Reference Uphoff, Ekers, Robertson, Dawson, Sanger and South20 The term ‘non-specialist worker’ is heterogeneous, comprising two distinct groups: health professionals without specialist mental health training and lay workers with no clinical background. Reference Uphoff, Ekers, Robertson, Dawson, Sanger and South20,Reference Uphoff, Pires, Barbui, Barua, Churchill and Cristofalo25
Aims
In this review, we aimed to examine the effectiveness of behavioural activation in reducing depressive symptoms in adults when delivered by lay workers compared with any control group.
Method
The systematic review methodology was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow26 and followed a prespecified protocol registered in the International Prospective Register of Systematic Reviews protocol (PROSPERO identifier: CRD42024625620). The protocol was registered on 20 December 2024.
Inclusion criteria
Population
Adults aged ≥18 years diagnosed with depression or who report symptoms of mild to severe depression were included.
Intervention
The review focused on behavioural activation delivered by lay workers as the intervention. All RCTs evaluating treatment approaches for depression that were clearly described as ‘behavioural activation’, or treatments defined using the key components of behavioural activation, such as mood monitoring and activity scheduling, were included. Treatment approaches that incorporated elements of behavioural therapy, such as CBT or problem-solving therapy, were excluded.
Mode of delivery of behavioural activation
The mode of behavioural activation delivery could include face-to-face, online or group format by lay workers, including non-professional therapists, lay counsellors, lay workers, lay health workers, non-credential workers, voluntary workers or non-specialist persons. Lay counsellors who used psychological therapies targeting individuals or groups were eligible for inclusion without giving regard to the number of sessions. If behavioural activation was delivered by lay workers under the supervision of a therapist or psychiatrist, the study was included. However, if the lay worker was part of a team led by a psychiatrist or a psychotherapist who delivered the behavioural activation, the study was excluded.
Comparator intervention
Comparator interventions included waiting lists for treatment, usual care, comparative depression treatments or no treatments.
Outcome
The main outcome measure was the change in depressive symptoms, assessed by using scores from standard self-/clinician-/researcher-administered clinical rating scales from baseline to follow-up. Primary outcome measures included common depression scales such as the Patient Health Questionnaire-9 (PHQ-9) Reference Kroenke, Spitzer and Williams27 or Modified Beck Depression Inventory Version II (BDI-II). Reference Beck, Steer and Brown28 If a study included multiple scales for the same outcome, only the most used scale was selected.
Types of studies
Only RCTs were included. Other studies that were original and not RCT were excluded. All qualitative studies, study protocols, review protocols, commentaries, reports and systematic reviews were excluded. Other excluded studies include abstracts for conference proceedings or abstract with no full text or detailed results. Studies including participants with bipolar depression were also excluded.
Setting
This review included trials conducted in primary, secondary or community settings.
Search strategy
This systematic review adhered to the PRISMA guidelines. Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow26 Six databases were used to identify RCTs of behavioural activation for depression in adults, and included Ovid Medline, Ovid Embase, Ovid Emcare, Ovid PsycINFO, CINAHL and the Cochrane Library. Searches were also conducted in international trial registries, including the WHO International Clinical Trials Registry, the Australian New Zealand Clinical Trials Registry and ClinicalTrials.gov.
Reference lists of the included studies were checked to ensure all RCT trials were captured from the original electronic database searches. The first ten pages of Google Scholar were also searched. No restrictions on date, language or publication status was applied; however, unpublished data were not considered. All database searches were conducted between November and January 2025 (Supplementary Appendix 1: All databases search strategy).
Data collection and analysis
Study selection
All database search results were imported into Endnote reference management software version 2025 for Windows (The EndNote Team, Clarivate, London, UK; https://supportcenter.clarivate.com/s/article/Citing-the-EndNote-program-as-a-reference) and then uploaded into the Covidence systematic review management software for Windows (Veritas Health Innovation, Melbourne, Australia; www.covidence.org), where duplicates were identified and removed electronically. Two authors (A.A., M.J., I.N., S.O., N.M. or L.B.) independently screened each title and abstract of all records identified through the search strategy. Full-text articles of all identified trials were retrieved, and two authors (A.A., M.J., I.N., S.O., N.M. or L.B.) independently assessed the studies for eligibility based on the inclusion criteria. All disagreements for both title and abstract as well as full-text screening were resolved through team discussion, to reach a consensus based on percentages. Reasons for exclusion were recorded (Supplementary Appendix 2: list of excluded studies). A PRISMA flow diagram was used to present the study selection process. Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow26
Interrater reliability agreement assessment
Interrater agreement was evaluated using both the proportion of observed agreement and Cohen’s κ coefficient. Reference Cohen29 For title and abstract screening, reviewers demonstrated consistently high raw agreement (83–99%), but because ‘yes’ ratings were very rare, Cohen’s κ was reduced, with most pairs showing only slight to fair agreement, and one pair showed moderate agreement (κ = 0.53), some pairs had non-computable κ-values because of all ‘no’ ratings. For full-text screening, observed agreement was generally high, but the predominance of ‘exclude’ ratings limited the interpretability of Cohen’s κ. Among pairs with sufficient variation, agreement ranged from poor to moderate, with the highest at κ = 0.59. Overall, the reviewers were largely consistent in their decisions, indicating that Cohen’s κ underestimated the true level of agreement.
Data extraction and management
Data extraction was conducted independently by two review authors working in pairs (A.A., I.N., S.O., N.M. and L.B.). Each included study was independently extracted by two review authors, using a standardised data extraction sheet. The data extraction sheet was adapted from a template used in a previous study by the review authors. Reference Yisma, Muyambi, Walsh, Othman, Gray and Tan17,Reference Yisma, Walsh, Steen, Gray, Dennis and Gillam19 To ensure its suitability for the current review, the template was pre-tested for clarity and consistency. The extracted data included study characteristics such as study population, setting, recruitment method, treatment, outcome measures, randomisation, sample size calculation, measurements, effect size, risk of harm and reported adverse effect. All extracted data were compiled and cross-checked by a review author (S.O.) for completeness and accuracy. This additional verification step was undertaken to enhance consistency across the authors, minimise errors and ensure the overall reliability and transparency of the extracted data. Data extraction started on 4 March 2025.
Critical appraisal and risk of bias
Three review authors (S.O., M.J. and L.B.) independently assessed the risk of bias of each RCT by using version 2 of the Cochrane Risk-of-Bias Tool for randomised trials. Reference Higgins, Altman, Gøtzsche, Jüni, Moher and Oxman30 Consensus was reached through discussion among the review authors. Data from the risk of bias assessment were entered into robvis, a risk-of-bias data visualisation tool, to generate a summary figure. Reference McGuinness and Higgins31 Risk-of-bias assessments were used to critique the research evidence, but not as an exclusion criterion. The risk of bias across all domains was summarised to produce an overall risk of bias for each RCT.
Data synthesis and meta-analysis
The review included a narrative synthesis of the findings from the included studies. To estimate the overall effect of behavioural activation delivered by lay workers compared with any control group in reducing depressive symptoms in adults, a meta-analysis was conducted. The analysis focused on synthesising evidence on the effectiveness of behavioural activation interventions delivered by lay workers versus treatment as usual or enhanced usual care. A random-effects meta-analysis using inverse variance weighting was conducted to account for variability across studies. The results were reported as pooled effect sizes expressed as standardised mean difference (SMD) with corresponding 95% confidence intervals. Negative SMD values indicated a reduction in depressive symptoms and therefore favoured behavioural activation compared with control conditions. Statistical heterogeneity among the studies was assessed using the I 2-statistic, and findings were visually presented in a forest plot. All analyses were conducted in R for Windows, using the meta and metafor packages (R Core Team, R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/). Subgroup analysis was conducted to explore potential sources of heterogeneity in the pooled estimate of the effect of behavioural activation on depressive symptoms, based on comparator type (enhanced usual care versus active psychoeducation).
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence for the outcome. The GRADE framework considers five domains: risk of bias, inconsistency, indirectness, imprecision and publication bias. Certainty was rated as high, moderate, low or very low. GRADE assessments were performed using GRADEpro GDT software for Windows (McMaster University and Evidence Prime, Hamilton, Canada; gradepro.org).
Results
Study selection
A total of 9614 citation were identified and uploaded into Covidence systematic review software. A total of 1905 citation were removed electronically as duplicate. The title and abstracts of the remaining 7707 records were screened against the inclusion criteria. Of these 7644 records were excluded as irrelevant. The remaining 63 articles were eligible for full-text screening. Fifty-seven studies were excluded for the following reasons: study design was not RCT (n = 18), intervention was not delivered by lay workers (n = 14), the intervention was not behavioural activation (n = 13), different outcomes (n = 4), ongoing study (n = 3), duplicate (n = 2), wrong comparator (n = 2) and abstract with no full text available (n = 1). Six studies met the inclusion criteria and were included in the review and meta-analysis (Fig. 1). A list of excluded studies is presented in a Microsoft Excel sheet available in the Supplementary Material.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart.
Source: Page et alReference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow26. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/. RCT, randomised controlled trial.
a. Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers).
b. If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools.

Description of the included studies
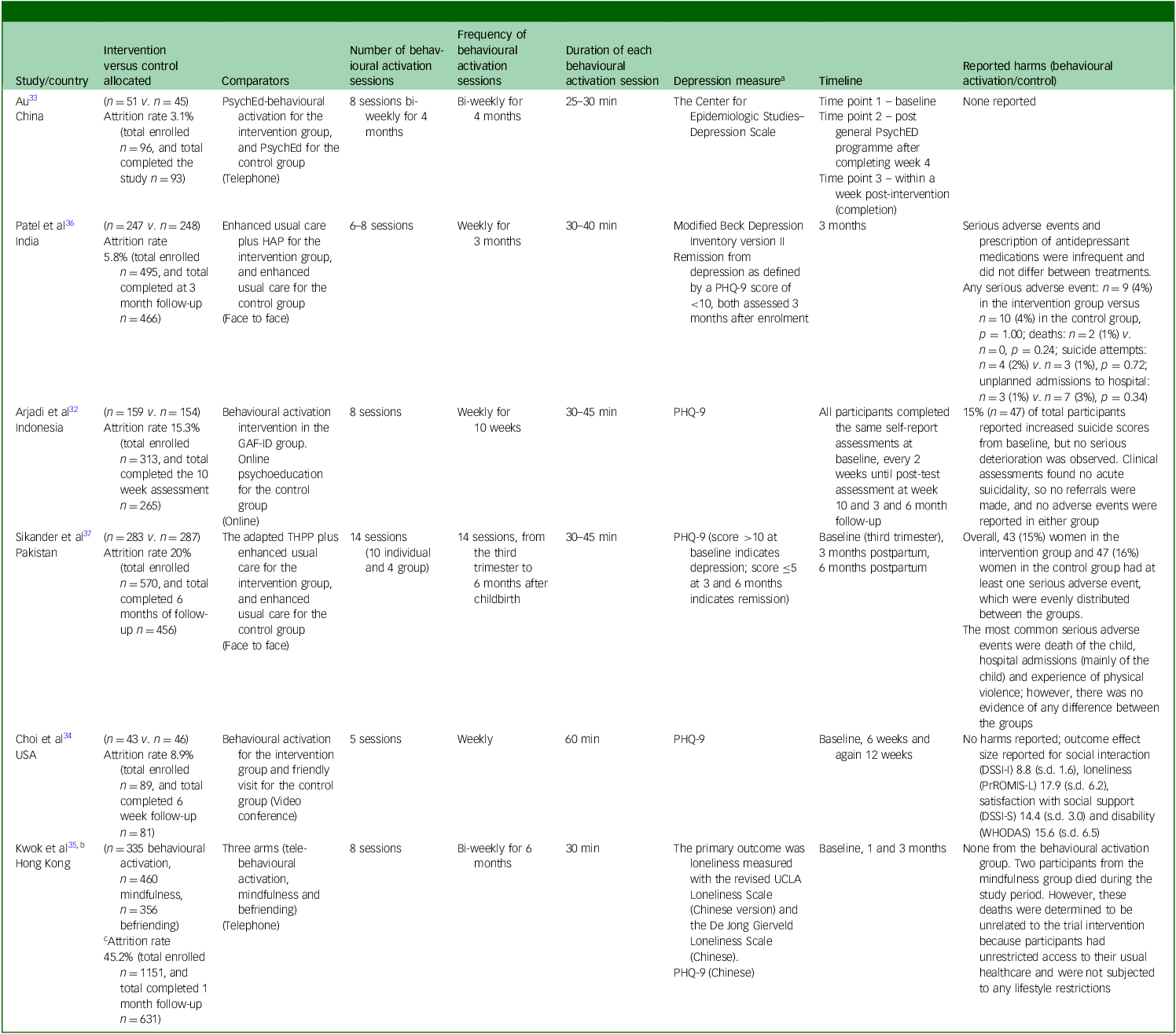
Six studies met the inclusion criteria and were included. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32–Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 These studies were conducted between 2015 and 2024 across various countries, including China, India, Indonesia, Pakistan, the USA and Hong Kong (Table 1).
Study characteristics

RCT, randomised controlled trial; PsychED, psychoeducation; HAP, Healthy Activity Program; PHQ-9, Patient Health Questionnaire-9; GAF-ID, Guided Act and Feel Indonesia; THPP, Thinking Healthy Programme peer-delivered; ENACT, ENhancing Assessment of Common Therapeutic factors rating scale; UCLA, University of California, Los Angeles.
These six included studies assessed the effectiveness of behavioural activation on depressive symptoms when delivered by lay workers. In terms of study design, four studies were two-arm RCTs, Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32–Reference Choi, Pepin, Marti, Stevens and Bruce34,Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 one study was a three-arm RCT Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 and one was a cluster RCT (Table 1). Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37
Study setting
Participants were recruited from various settings, including community-based settings, Reference Choi, Pepin, Marti, Stevens and Bruce34 their usual residences Reference Au33 and community dwellings. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 Recruitment also took place through primary healthcare centres Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 and in rural, village-based locations. Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 Additional settings included public housing estates primarily catering to solo-living older adults, community centres for older adults and older adult academies (Table 1). Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35
Participants
The inclusion criteria across the included studies varied based on the study aim and target populations. Five studies included adults aged 18 years and older with a diagnosis of depression or reported symptoms of mild to severe depression, except for one study that recruited participants aged 16 years and older. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 Two trials recruited older adults aged 50 years and older Reference Choi, Pepin, Marti, Stevens and Bruce34 or 65 years and older. Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 Across all included studies, a total of 1118 participants were recruited into the intervention groups, and 1596 into the control groups (Table 2).
Intervention and control group characteristics

PsychED, psychoeducation; HAP, Healthy Activity Program; PHQ-9, Patient Health Questionnaire-9; GAF-ID, Guided Act and Feel Indonesia; THPP, Thinking Healthy Programme peer-delivered; DSSI-I, Social Interaction Subscale of the Duke Social Support Index; DSSI-S, Social Satisfaction Subscale of the Duke Social Support Index; WHODAS, World Health Organization Disability Assessment Schedule; PROMIS-L, Patient-Reported Outcomes Measurement Information System, Social Isolation Scale; UCLA, University of California, Los Angeles.
a. Depression measure used for data analysis was the PHQ-9.
b. Kwok et alReference Kwok, Jiang, Yeung, Choi, Ho and Warner 35 used three comparators; only the behavioural activation and mindfulness data were included in the meta-analysis.
c. A total of 1151 participants were enrolled, and 631 completed the 1-month follow-up, corresponding to an attrition rate of 45.2%. The a priori sample size calculation indicated that 322 participants per group (644 total) were required after allowing for up to 10% loss to follow-up. Based on this sample size requirement, the attrition rate relative to the target follow-up sample was 2.0%.
All included studies reported attrition rates of less than 20%, and the reasons for loss to follow-up were clearly described in the Consolidated Standards of Reporting Trials diagrams of the primary studies. Five studies explicitly reported using an intention-to-treat approach to handle missing data. The total number of participants allocated to the intervention and control groups was 2714, of whom 2557 were included in the analysis (Table 2).
Intervention
All six included studies focused on providing behavioural activation for individuals who reported symptoms of mild to severe depression. The behavioural activation interventions ranged from 5 to 14 sessions, delivered weekly or bi-weekly over a period of 2 to 6 months. Session durations varied from 25 to 60 min. The mode of delivery differed across the studies, including face-to-face, telephone, video conference and online formats. Two studies delivered behavioural activation face to face with participants, Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36,Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 two studies delivered it via telephone, Reference Au33,Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 and the remaining two studies used either an online Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 or video conference Reference Choi, Pepin, Marti, Stevens and Bruce34 format.
All comparators were considered acceptable for inclusion if they did not fall under the category of behavioural activation. The comparators used in the included studies varied and included enhanced usual care, Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 online psychoeducation, Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32,Reference Au33 friendly visit, Reference Choi, Pepin, Marti, Stevens and Bruce34 mindfulness and befriending (Table 2). Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35
Lay workers characteristics and training
In the six included studies, lay workers were also known as lay counsellors, lay peer persons or paraprofessionals, and received varying types of training and supervision. In one study, lay workers completed a 42 h course and 20 h of group training on behavioural activation, delivered by social workers and clinical psychologists followed by weekly supervision. Reference Au33 In the study by Patel et al, Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 lay peer workers were provided with a 3-week participatory workshop on the healthy activity programme followed by a 6-month internship in primary healthcare clinics. Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 In addition, the lay peer workers received weekly group supervision and bi-monthly individual supervision. In another study, lay workers received 2 days of intensive training on internet-based behavioural activation, which included handling technical issues and clinical challenges. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 Lay workers also received printed materials and regular supervision. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 Another study reported that lay workers received six 2 h face-to-face group sessions weekly and were led by a social worker and a research assistant. Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 The remaining two studies Reference Choi, Pepin, Marti, Stevens and Bruce34,Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 did not report the exact duration of training, but reported that lay workers received training with regular supervision (Table 1).
Outcome measures
Outcomes were assessed across all included studies, using various depression scales. Three studies measured depression with the PHQ-9 scale as primary outcomes, Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32,Reference Choi, Pepin, Marti, Stevens and Bruce34,Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 whereas three studies used other scales, such as the Center for Epidemiologic Studies–Depression Scale Reference Au33 and the BDI-II, with remission defined using PHQ-9 scores, Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 the revised UCLA Loneliness Scale (Chinese version) and the PHQ-9 Chinese version. Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35
Four studies used PHQ-9 to determine the eligibility criteria based on the severity of depressive symptoms. In one study, participants were included if they scored >14 on the PHQ-9, indicating moderately severe to severe depression. Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 Another study included participants if they scored ≥10 on the PHQ-9 and had a clinical diagnosis of major depressive disorder or persistent depressive disorder as per the Structured Clinical Interview for DSM-5. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 Similarly, Sikander et al Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 included participants if they scored >10 on the PHQ-9; however, Choi et al Reference Choi, Pepin, Marti, Stevens and Bruce34 included participants if they scored <10 on the PHQ-9, indicating no to mild symptoms of depression (with a baseline mean score of 7.2) (Table 2).
Risk of bias and GRADE assessment
The six included studies were rated to have an overall high risk of bias. Across these studies, several sources of bias were identified. Patel et al Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 demonstrated high risk of bias in domains 3, 4 and 5 because of insufficient handling of missing outcome data, lack of blinding of outcome assessors, and indications of selective reporting. Kwok et al Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 raised some concerns regarding the randomisation process and lack of blinding of participants and people who delivered the intervention, whereas domain 5 was rated high risk because analyses did not follow a clearly prespecified plan and selective reporting was evident. Similarly, Choi et al Reference Choi, Pepin, Marti, Stevens and Bruce34 presented some concerns about randomisation, high risk in outcome assessment owing to lack of blinding, and insufficient information to judge adherence to a prespecified analysis plan.
High risk of bias was also observed in Arjadi et al Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 because of missing outcome data potentially related to true outcome values and unblinded outcome assessment, alongside evidence of selective reporting. Au Reference Au33 showed some concerns in domains 1 and 2 because of limited reporting on randomisation, lack of blinding and unclear deviations from intended interventions, whereas domain 5 was judged high risk due to the absence of a prespecified analysis plan and likely selective reporting. Sikander et al Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 was judged high risk for domain 1b because participants selection within clusters appeared to be influenced by awareness of intervention allocation, as well as high risk in domains 4 and 5 because of unblinded outcome assessment and indications of selective reporting and selective analysis (Fig. 2).
Risk of bias of the included studies. RCT, randomised controlled trial.

The certainty of evidence for the effect of behavioural activation delivered by lay workers to individuals diagnosed with depressive symptoms was rated as very low, downgraded because of a high risk of bias and imprecision, reflected by wide confidence intervals associated with high heterogeneity.
Reporting of adverse events and harms
All studies reported data on adverse events during trial implementation, except one study. Reference Au33 Two out of five studies reported no harm or adverse effects for the behavioural activation group. Reference Choi, Pepin, Marti, Stevens and Bruce34,Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 For the control group, Kwok et al Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 reported that two participants from the mindfulness group died during the study period. It was determined that these deaths were unrelated to the trial intervention as participants had unrestricted access to their usual healthcare and were not subjected to any lifestyle restrictions.
The remaining three studies reported serious adverse events; Patel et al Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 reported serious adverse events and prescription of antidepressant medications in both the intervention and the control group. These adverse events were similar in both the intervention and control group (n = 9 (4%) in the intervention group versus n = 10 [4%] in the control group). The reported serious adverse events included deaths, suicide attempt, and unplanned admissions to hospital from any cause. The authors noted that these events were not significantly different between groups and did not appear to be related to the intervention itself. Arjadi et al Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32 reported 15% (n = 47) of total participants increased suicide scores from baseline, but no serious deterioration was observed. Clinical assessments in this study found no acute suicidality, so no referrals were made, and no adverse events were reported in either group. Sikander et al Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 reported adverse events for 43 (15%) women in the intervention group and 47 (16%) women in the control group, with at least one serious adverse event in the control group. Serious adverse events reported included death of the child of the study participant, hospital admissions (mainly involving participants’ child) and experience of physical violence; however, there was no evidence of any difference between the groups. These events did not appear to be related to the intervention itself (Table 2).
Effectiveness of behavioural activation delivered by lay workers on reducing depression
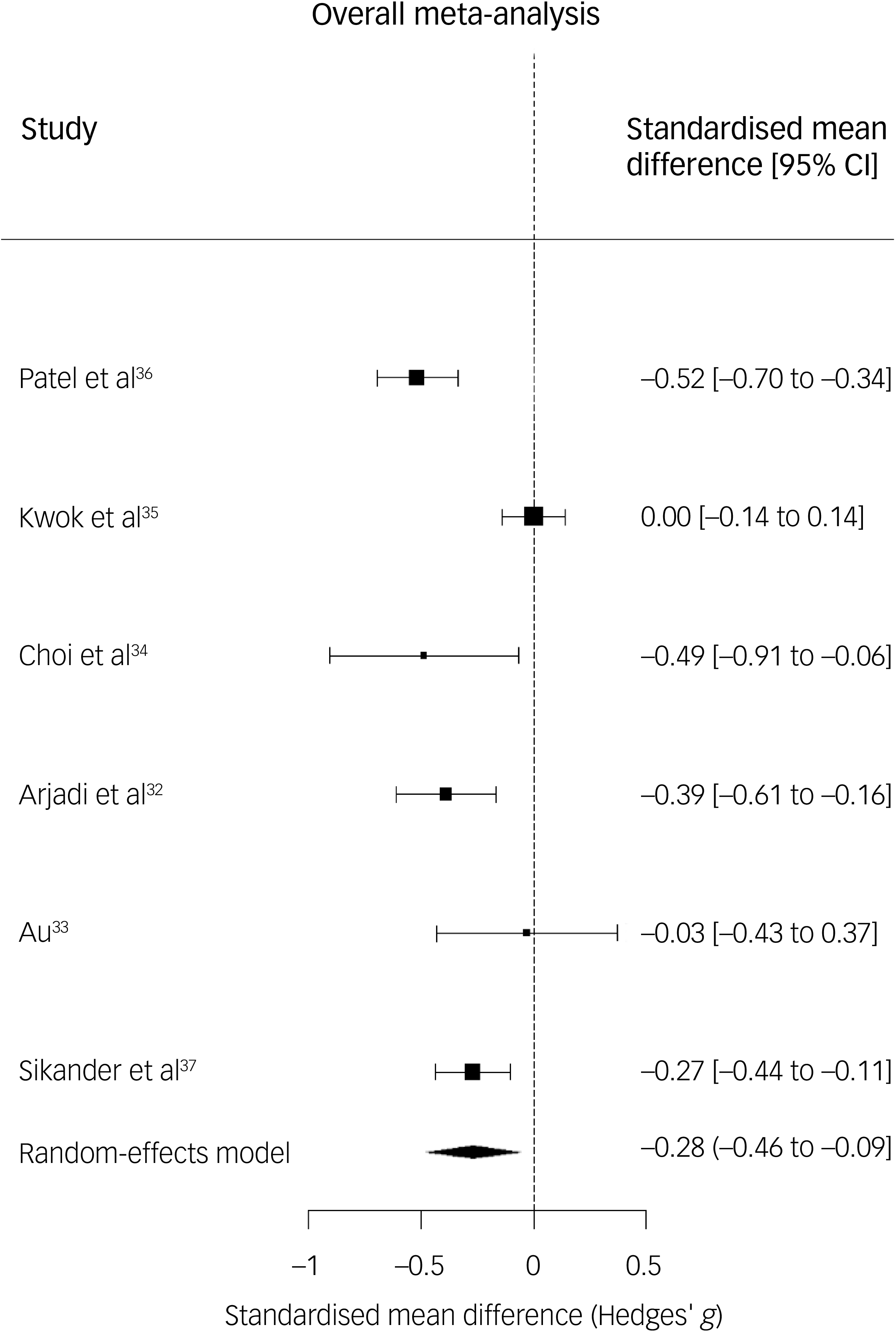
The meta-analysis included six RCTs assessing the effectiveness of lay workers delivered behavioural activation interventions for adults diagnosed with depression. The pooled SMD was −0.28 (95% CI −0.46 to −0.09; p = 0.0029), indicating a small but statistically significant effect in favour for the intervention group than the control group. There was evidence of statistically significant and substantial between study heterogeneity (I 2 = 76%; Cochran’s Q = 24.55, d.f. = 5, p = 0.0002) (Fig. 3).
Meta-analysis forest plot.

Findings from the meta-analysis suggest that behavioural activation may be effective in reducing depression in adults when delivered by lay workers. However, because of the high risk of bias in the included studies, these findings are based on low-quality evidence and should be interpreted with appropriate uncertainty about the effectiveness of behavioural activation delivered by lay workers for people diagnosed with depression.
Subgroup analysis
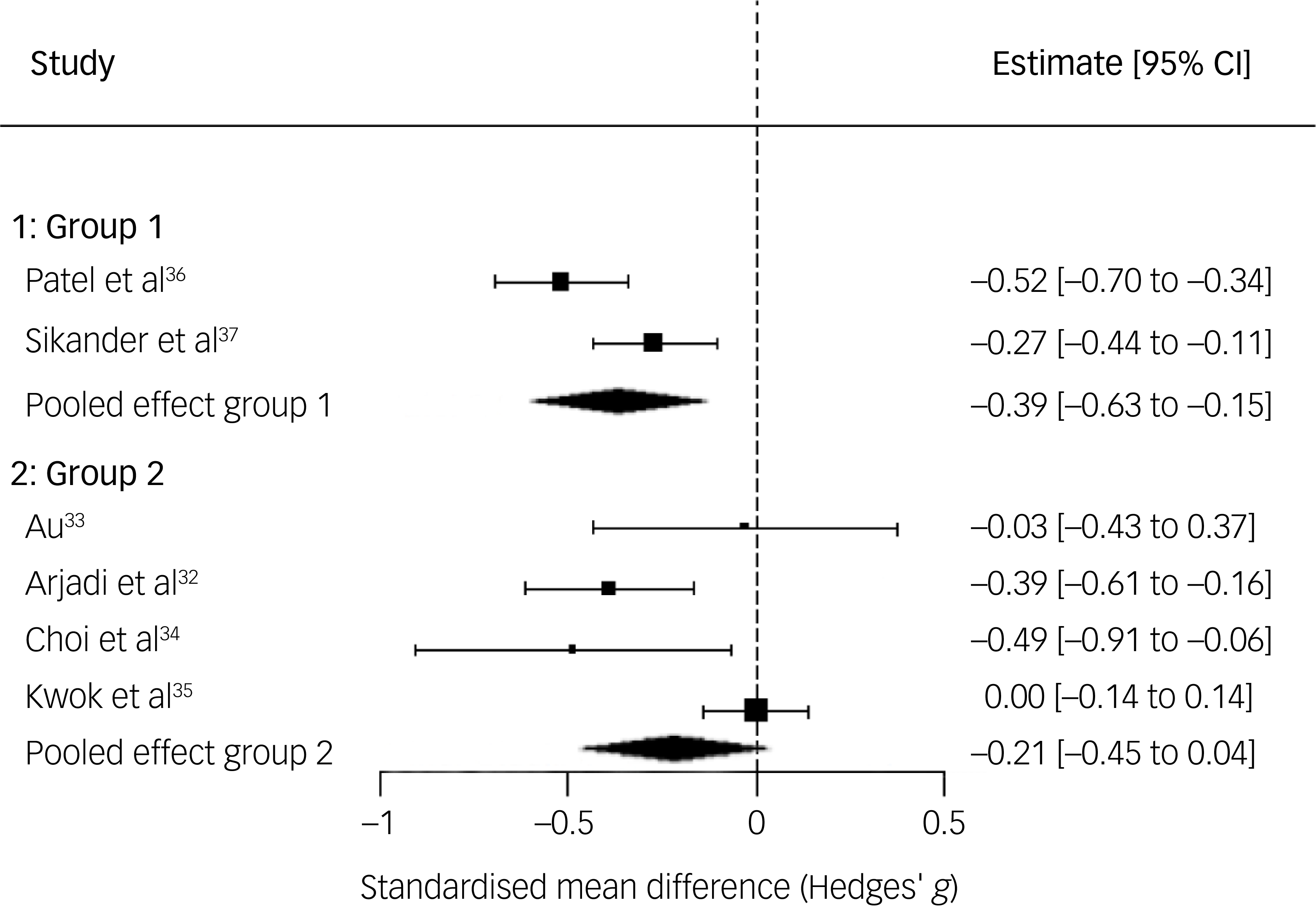
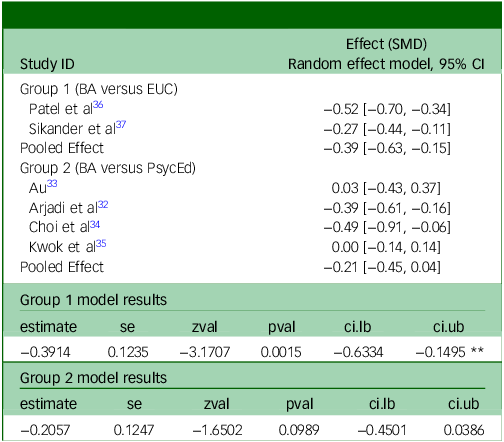
A subgroup analysis was conducted to explore potential sources of heterogeneity in the pooled estimate of the effect of behavioural activation on depressive symptoms, based on comparator type (enhanced usual care versus active psychoeducation). In group 1 (Patel et al Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 and Sikander et al Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 ), behavioural activation was associated with a statistically significant, moderate reduction in symptoms (g = −0.39). However, group 2 (the remaining four studies) demonstrated a smaller, non-significant effect (g = −0.21). These findings indicate that the effectiveness of behavioural activation may vary according to comparator type and study characteristics. The results of these subgroup analyses are presented in Fig. 4 and Table 3.
Subgroup analysis.

Subgroup analysis using R Metafor

Group 1: Random-Effects Model (k = 2; tau^2 estimator: REML). tau^2 (estimated amount of total heterogeneity): 0.0228 (SE = 0.0431). tau (square root of estimated tau^2 value): 0.1509. I^2 (total heterogeneity/total variability): 74.70%. H^2 (total variability/sampling variability): 3.95. Test for Heterogeneity: Q(df = 1) = 3.9518, p-val = 0.0468.
Group 2: Random-Effects Model (k = 4; tau^2 estimator: REML). tau^2 (estimated amount of total heterogeneity): 0.0404 (SE = 0.0508). tau (square root of estimated tau^2 value): 0.2011. I^2 (total heterogeneity/total variability): 70.26%. H^2 (total variability/sampling variability): 3.36. Test for Heterogeneity: Q(df = 3) = 11.3799, p-val = 0.0098. Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1. SMD = Standardized Mean Difference; CI = confidence interval; I 2 = proportion of heterogeneity; Q-test evaluates within-subgroup heterogeneity.
Discussion
The current systemic review and meta-analysis of RCTs assessed the effectiveness of behavioural activation interventions delivered by lay workers in reducing depressive symptoms in adults diagnosed with depression. Six RCTs met the inclusion criteria and were included in the meta-analysis. The pooled SMD was −0.28 (95% CI −0.46 to −0.09; p = 0.0029), indicating a small but statistically significant effect in favour for the intervention group than the control group. However, there was evidence of statistically significant and substantial between study heterogeneity (I 2 = 76%; Cochran’s Q = 24.55, d.f. = 5, p = 0.0002), suggests effectiveness may vary considerably across studies.
The included studies varied in various aspects, including participant demographics, behavioural activation duration and delivery, and type of comparators. Participants were randomly assigned, and the included studies reported that the attrition rate was <20% with a rational for lost to follow-up participants, which means participants were engaged with the behavioural activation intervention. Five of the included studies measured depressive symptoms as the primary outcome, with data collected and reported according to the study protocols. Although the intervention showed a small but statistically significant effect on depressive symptoms, the certainty of evidence was judged to be very low because of methodological limitations and a high risk of bias in the included studies. Therefore, these findings should be interpreted with caution and cannot be used to draw definitive conclusions about the effectiveness of behavioural activation delivered by lay workers for individuals with depression.
The behavioural activation interventions ranged from 5 to 14 sessions, delivered weekly or bi-weekly over a period of 2–6 months, with session durations varying from 25 to 60 min. Behavioural activation was effectively delivered using various modalities such as face-to-face, telephone, video conference and online formats. This flexibility in delivery format and structure highlights the adaptability of behavioural activation to diverse populations specially in low-resource and primary care settings. Although three studies reported moderate positive effects, Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32,Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36,Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 the remaining studies showed minimal to no effect. These studies Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32,Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36,Reference Sikander, Ahmad, Atif, Zaidi, Vanobberghen and Weiss37 shared several characteristics, including larger sample sizes, and were conducted in low- and middle-income countries, where access to mental health services is limited and shortages of mental health professionals are common. Reference Kakuma, Minas, van Ginneken, Dal Poz, Desiraju and Morris38,Reference Sørensen, Bæk, Kallestrup and Carlsson39 In contrast, the other three studies reported minimal to no effect of behavioural activation delivered by lay workers. Reference Au33–Reference Kwok, Jiang, Yeung, Choi, Ho and Warner35 These studies were different in several aspects; all were conducted in high-income countries, behavioural activation was delivered via telephone or video conference-based modalities, and sample size varied (although the study by Kwok et alReference Kwok, Jiang, Yeung, Choi, Ho and Warner 35 had a large sample). Differences in outcomes may reflect heterogeneity in population characteristics, intervention delivery mode, and fidelity of implementation, or context-specific effectiveness of behavioural activation, rather than indicating a uniformly effective intervention.
Overall, the evidence remains inconclusive regarding the effectiveness of behavioural activation when delivered by lay workers. Nevertheless, the pooled SMD across the included studies indicates a small but statistically significant reduction in depressive symptoms associated with lay worker-delivered behavioural activation. Importantly, despite growing evidence supporting the effectiveness of digital self-guided interventions, lay delivered behavioural activation approaches remain of interest because of lay workers’ potential to provide human support, enhance engagement in daily activities and adherence, and facilitate cultural and contextual tailoring. These features may be particularly relevant for individuals with limited digital literacy, restricted access to technology or more complex psychological needs, as well as in settings where digital infrastructure is insufficient.
Although all included studies evaluated the effectiveness of behavioural activation when delivered by lay workers, these studies varied in the extent and type of training and ongoing supervision allocated to lay workers. Effective outcomes appeared to correlate with more comprehensive training and ongoing supervision, which support the importance of adequate training preparation and ongoing support for lay workers. Reference Arjadi, Nauta, Scholte, Hollon, Chowdhary and Suryani32,Reference Au33,Reference Patel, Weobong, Weiss, Anand, Bhat and Katti36 These studies reported effective behavioural activation with weekly ongoing supervision. However, approaches to training and supporting lay workers differed across contexts, limiting the generalisability of any single model. As a result, our findings cannot specify a particular training approach for local implementation, which requires additional context-specific co-design and assessment based on the available resources, workforce capacity and cultural considerations.
No evidence of serious adverse events/harm directly related to the behavioural activation interventions were reported. Adverse events were unrelated to the behavioural activation intervention and were distributed roughly equally across both the intervention and control groups. These findings suggest that behavioural activation, when delivered by lay workers in similar contexts, may be a safe intervention to manage depression for adults, particularly in settings with limited access to specialist mental health professionals. Overall, behavioural activation delivered by lay workers appears to be a low-risk intervention that can be delivered across diverse settings.
Strengths and limitations
Our systematic review and meta-analysis have several strengths. The review was conducted by experienced researchers and guided by a prespecified protocol prospectively registered with PROSPERO and adhered to PRISMA statement guidelines.
A limitation and challenge across all the included studies was the inability to mask or blind participants because of the nature of the interventions. Another issue was the lack of detailed study descriptions, which led to insufficient information to verify whether any outcomes were selectively reported. The quality of the evidence in all included studies was poor because of high risk of bias. All studies were assessed as having a high risk of bias mainly arising from the measurement of outcomes and the selective reporting of results. These limitations affect the overall confidence in the review findings, and highlight the need for more rigorously designed trials in the future.
Limitations arising from the review process also need to be acknowledged. Although the search strategy was comprehensive and designed to capture all relevant study, there is a possibility that some eligible studies were missed during title and abstract screening. In cases where studies used multiple scales to measure the same outcome, only the most used scale was selected for analysis. Although no language restriction was planned, only studies with English-language abstracts were screened for inclusion. This may have introduced potential language bias, as studies without English abstracts could have been missed. This limitation should be considered when interpreting the findings.
Future research
The findings from this review and meta-analysis suggest that behavioural activation, when delivered by trained lay workers, may offer an effective approach for reducing depressive symptoms in adults. These findings are of importance, particularly in low- and middle-income settings with limited access to specialist mental healthcare professionals. Behavioural activation is a theory driven and empirically supported intervention that is grounded in behavioural models of depression. However, because of the high risk of bias and heterogeneity of the included studies, these findings should be interpreted with caution. Across the included studies, source of risk of bias included limitations in the randomisation process, lack of blinding of outcome assessors, incomplete or inadequate handling of outcome data, and selective reporting. These methodological weaknesses may have led to an overestimation of treatment effects and reduce confidence in the pooled estimates. In addition, based on a Cochrane review reporting moderate certainty that behavioural activation produces a moderate to large effect size, and our systematic review that has found no evidence of reported harm and demonstrated strong participants engagement, we propose that a well-designed implementation RCT and rigorous training protocols to train lay workers to deliver behavioural activation are needed, especially in low-resource and primary care and community settings.
Future research should prioritise well-designed, high-quality RCTs incorporating robust randomisation procedures, strategies to minimise occurrence and appropriate handling of missing data, and clearly predefined analysis plans, to evaluate the effectiveness of behavioural activation delivered by lay workers for individuals reported depressive symptoms. Greater harmonisation in the measurement of depressive symptoms across studies would also strengthen the evidence base and facilitate comparability and synthesis, although emerging resources such as harmonisation tools may help mitigate this challenge. Given the current evidence is very weak limited by high risk of bias and substantial heterogeneity, future studies should ensure rigorous methodological standards.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12018
Data availability
As this is a systematic review, it utilised data previously reported in the primary literature or in public domain. All summary data supporting the findings are provided in the text and the Supplementary Material.
Acknowledgements
We would like to acknowledge the academic librarian for her support during the development of the review search strategy.
Author contributions
All authors were involved in conceptualisation of the study. S.O. drafted the protocol, registered it with the PROSPERO, developed the search strategy and conducted database searches. A.A., M.J., I.N., S.O., N.M. and L.B. performed the title and abstract and full-text screening of retrieved papers. A.A., I.N., S.O., N.M. and L.B. performed data extraction. S.O., M.J. and L.B. conducted risk of bias. S.O. conducted meta-analysis and drafted the original manuscript. M.J. and L.B. reviewed the draft. A.K., E.A., M.H., K.M., M.C., R.G., E.J. and C.L. were involved in the study conceptualisation, reviewed the protocol and reviewed the final manuscript draft. All authors have read and agreed to the final version of the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.






 Open access
Open access
eLetters
No eLetters have been published for this article.