


LEARNING OBJECTIVES
After reading this article you will be able to:
-
• understand the conceptual framework of formal thought disorder (FTD) as a collection of observable signs requiring specific elicitation procedures
-
• apply systematic conversational manoeuvres, including thought provocation, cognitive loading and inducing mental state talk, to reliably elicit FTD signs during clinical interviews
-
• implement a structured, phased approach to FTD assessment that integrates evidence-based techniques from validated rating scales into routine clinical practice.
‘I am the finest professorship […] This is again the highest activity – double – twenty-five francs – I am double polytechnic irretrievable’ (Babette S, in Jung’s Psychology of Dementia Praecox; Woods Reference Woods2011)
‘I love Russian songs. I love Russian speech. I know many Russians who are not Russians, because they speak a foreign language. I know that a Russian is a man who loves Russia. I love Russia. I love France. I love England. I love America. I love Switzerland, I love Spain, I love Italy, I love Japan, I love Australia, I love China, I love Africa, I love the Transvaal. I want to love everybody, and therefore I am God. I am not a Russian and not a Pole. I am a man, not a foreigner and not a cosmopolite. I love the Russian land. I will build a dam in Russia. I know that the Poles will curse me. I understand Gogol because he loved Russia’ (Vaslav Nijinsky; Nijinsky Reference Nijinsky2006)
‘ You know… I… when I came to England at eleven 102 road, I went to infant school at the time. I was eleven be tweven in December because you know, was still, I was so tiny for my age // … I’m them girl in Eastenders… Julie crabs’ skin and bone and starvation… I don’t know… school with that them… them people somehow, they look and the girl face look and I look like that…’ (Participant 26AR16 in the Discussing Abstract Ideas in Schizophrenia Corpus: https://reshare.ukdataservice.ac.uk/855021/; Delgaram-Nejad Reference Delgaram-Nejad, Archer and Chatzidamianos2023)
Spontaneous segments of speech like those above are rare in routine clinical practice. Yet these are the tell-tale signs of formal thought disorder (FTD) – a disruption in thought/language structure and coherence expressed through speech that represents a core diagnostic feature of severe mental illness (Kircher Reference Kircher, Bröhl and Meier2018). The central question facing time-pressed clinicians looking for FTD is: how can we increase the likelihood of eliciting such revealing speech patterns in the clinic?
The challenge of assessing FTD is fundamentally different from assessing many other psychiatric phenomena. Unlike hallucinations, depression or anxiety, which patients descriptively report, FTD must be actively drawn out to be observed during the clinical interview (Palaniyappan Reference Palaniyappan, Homan and Alonso2022). This requires clinicians to serve as architects of conversational conditions that reveal latent cognitive and linguistic vulnerabilities.
Over decades, a number of rating scales have demonstrated that FTD can be measured with high interrater reliability when specific elicitation procedures are followed (Voppel Reference Voppel, Ciampelli and Kircher2025). The authors of these rating scales (Singer Reference Singer and Wynne1965; Reilly Reference Reilly, Harrow and Tucker1975; Andreasen Reference Andreasen1979; Johnston Reference Johnston1979; Harrow Reference Harrow and Quinlan1985; Caplan Reference Caplan, Guthrie and Fish1989; Chen Reference Chen, Lam and Kan1996; Docherty Reference Docherty, DeRosa and Andreasen1996; Liddle Reference Liddle, Ngan and Caissie2002; Bazin Reference Bazin, Sarfati and Lefrère2005; Kircher Reference Kircher, Krug and Stratmann2014) universally acknowledge that standardisation of these procedures is essential to achieve good interrater reliability. Yet a paradox persists: despite their psychometric reliability, these scales remain unused in routine clinical practice (Zamperoni Reference Zamperoni, Tan and Sumner2024a). FTD remains what Sass & Parnas (Reference Sass and Parnas2017) described as ‘a grossly neglected concept’, with many psychiatrists in early career stages unfamiliar with its assessment.
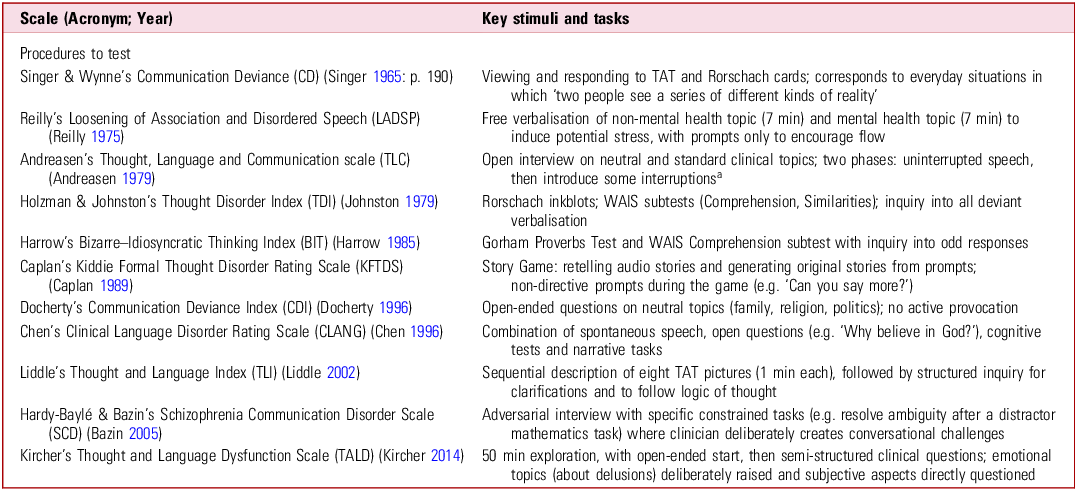
Multiple factors have contributed to this decline, including the bewildering array of overlapping terms (e.g. circumstantiality, tangentiality and derailment) used across scales (Sreeraj Reference Sreeraj, Voppel and Venkatasubramanian2025). Although theoretical clarification of FTD phenomenology and definitional ambiguities lies beyond the scope of this article (see Passby Reference Passby and Broome2017; Sreeraj Reference Sreeraj, Voppel and Venkatasubramanian2025), we address a more practical gap: bringing forth the reliable but implicit elicitation procedures exploited by these scales (Table 1) for regular clinical use. By extracting these methods, we make explicit a core set of conversational manoeuvres that can be synthesised and flexibly deployed in routine interviews. Our aim is to ground clinical artistry in measurement methodology, providing a practical manual for the FTD-focused interview (Box 1). We do not provide an exhaustive checklist of FTD items; for this, we refer readers to the appendix and supplement of another work (Sreeraj Reference Sreeraj, Voppel and Venkatasubramanian2025).
Overview of major formal thought disorder (FTD) rating scales and their elicitation procedures

TAT, Thematic Apperception Test; WAIS, Wechsler Adult Intelligence Scale.
a. Andreasen described a 50 min interview for scoring the TLC, but researchers have applied numerous variations, ranging from a set of 6 questions in a 5–10 min interview (Muralidharan Reference Muralidharan, Finch and Bowie2018) to using very brief recordings of free speech (∼1.5–3 min) (Tang Reference Tang, Hänsel and Cong2023) or snippets from videos of ∼1.9 min average length (Krell Reference Krell, Tang, Hänsel, Shaban-Nejad, Michalowski and Bianco2022).
Diagnosing formal thought disorder: key learning points
-
• Formal thought disorder (FTD) is a collection of observable signs that must be actively elicited through systematic conversational manoeuvres, not passively awaited.
-
• Seven key elicitation techniques can be derived from validated rating scales: free and open-ended discourse, thought provocation, cognitive loading, affective reactivity, inducing mental state talk (manipulation of perspectives), systematic targeted clarification and assessing subjective dimensions.
-
• A structured, phased approach to FTD assessment integrates these techniques across a 15–20 min interview: open discourse, structured provocation and social–cognitive–emotional challenge.
-
• The clarification technique is critical for differentiating occasional slips from genuine thought disorder – individuals without FTD can usually clarify their meaning or repair inconsistencies when prompted.
-
• Cultural context, linguistic factors and differential diagnoses (e.g. aphasia, intellectual disability, anxiety) must be carefully considered to avoid misidentifying normal variations or other conditions as FTD.
Core conceptual framework
The foundational insight for FTD assessment is deceptively simple: FTD comprises subtle but observable signs, not reported symptoms. This distinction has profound methodological implications. Just as eliciting a cardiac murmur requires dynamic auscultatory manoeuvres (e.g. handgrip, the Valsalva manoeuvre, squatting, breath holding or a treadmill stress), detecting FTD demands deliberate conversational techniques. Without proper technique, genuine pathology may go undetected, while improper technique may generate false positives.
Since FTD manifests through conversational speech, our elicitation procedures must themselves be conversational. The clinician becomes an active architect of discourse conditions, strategically varying communicative demands to stress-test linguistic cognition. Rating scale developers realised early that standard symptom-focused interviews are often insufficient. Patients may provide only brief utterances, without enough linguistic material to assess derailment, loosening or other phenomena. Successful scales solve this by systematically manipulating discourse conditions through seven key manoeuvres (Fig. 1 and Box 2). Employing these manoeuvres provides us with a ‘treadmill test’ for thought, language and communication processes.
Techniques to elicit formal thought disorder. This figure was generated using Google’s NotebookLM.

Good practice points in eliciting evidence of formal thought disorder (FTD)
-
• Allocate at least 15 min for dedicated FTD assessment, beginning with neutral, open-ended topics before progressing to more demanding tasks.
-
• Systematically request clarification for any unclear, illogical or tangential statements, and verify whether the patient has subjective experiences of disrupted thought flow and dynamics.
-
• When working with interpreters, brief them on the assessment goals and ensure they can convey speech structure and coherence, not just content.
-
• Balance assessment of observable FTD signs with direct inquiry about the patient’s subjective experience of their thinking processes.
-
• With the patient’s consent, consider recording verbatim (preferably via audio recording) portions of clinical interviews for more detailed analysis rather than simply noting ‘disorganised speech – present or absent’.
Seven key manoeuvres for eliciting FTD
Free and open-ended discourse
The rationale for open-ended discourse draws from a fundamental principle: reducing external guides for organising thoughts allows internal organisational deficits (i.e. mental disorganisation that constitutes FTD) to surface. As social dialogue imposes structure through topic cues, probes and joint attending, plenty of external support is available for organised discourse. In contrast, minimally directed or open-ended speech (soliloquies) strip away this scaffolding.
Associationist and psychodynamic theories that formed the basis of the ‘free association’ technique, i.e. saying whatever comes to mind freely or induced by a trigger word, have fallen from theoretical favour. But given the importance of observing aberrant semantic associations (Barrera Reference Barrera, McKenna and Berrios2005) and first-person narratives in FTD (Elleuch Reference Elleuch, Chen and Luo2025a), a modified form of this approach continues to be important for our purpose. Features such as derailment and perseveration emerge only when patients generate extended linguistic sequences with minimal external constraint. Phenomena like poverty of speech and increased latency become quantifiable through the amount, pacing and pausing of spontaneous output.
Instead of seeking complete Freudian-style free association, contemporary scales operationalise this principle through open-ended prompts. The Bizarre–Idiosyncratic Thinking (BIT) scale (Harrow Reference Harrow and Quinlan1985) makes this explicit: ‘more open-ended procedures better lend themselves to eliciting thought-disordered speech’ (Marengo Reference Marengo, Harrow and Lanin-Kettering1986: p. 499). The Schizophrenia Communication Disorder Scale (SCD) (Bazin Reference Bazin, Sarfati and Lefrère2005) focuses on everyday life topics – hobbies, family, television – that should elicit natural, elaborated responses. Some authors have resorted to the topic of dreams (Mota Reference Mota, Furtado and Maia2014). The Clinical Language Disorder Rating Scale (CLANG) (Chen Reference Chen, Lam and Kan1996) recommends neutral topics unrelated to psychopathology for this aspect of the interview.
Clinical application
Initiate the interview with 5–7 min of minimally constrained discourse, asking the patient to speak freely and telling them you will not interrupt. A prompt: ‘Tell me about your favourite TV show’ or ‘Thinking back, can you tell me a story about something important that happened to you in your life?’. The key is establishing permissive conditions to initiate the free-flowing thoughts with a first-person perspective.
Thought provocation through stimuli
Open-ended discourse removes external constraints, whereas thought provocation actively introduces interpretive demands. This procedure coincided with the shift from free association to projective techniques in the pre-DSM-III era, as ambiguous stimuli were seen as amplifying subtle cognitive aberrations. By requiring the patient to impose meaning on ambiguity, we can stress-test the integrity of their conceptual organisation.
FTD scales operationalise this strategy through a variety of complex stimuli with varying degrees of ambiguity in visual and auditory modalities. At the most ambiguous end, Rorschach inkblots, used in the Thought Disorder Index (TDI; Johnston Reference Johnston1979) and the test procedures to elicit Communication Deviance (Singer Reference Singer and Wynne1965), offer minimal perceptual structure. The Thematic Apperception Test (TAT; Murray Reference Murray1943), used by the Thought and Language Index (TLI) (Liddle Reference Liddle, Ngan and Caissie2002) and CLANG, provides recognisable scenes but leaves narrative connections unstated. Recorded stories (e.g. in the Kiddie Formal Thought Disorder Rating Scale, KFTDS; Caplan Reference Caplan, Guthrie and Fish1989) present less ambiguous content but require interpretive commentary.
Simple verbal provocation offers a more practical clinical approach. Abstract questions – ‘Why do you think some people believe in God?’ (CLANG) – demand sustained, organised argument. Proverb interpretation (CLANG, BIT) and comprehension items from the Wechsler Adult Intelligence Scale (Wechsler Reference Wechsler2008) used by the TDI and BIT (‘Why does land in the city cost more than land in the country?’) assess the ability to extract and articulate abstract meaning via monologues of extended utterances.
These tasks share a common feature: they require the patient to generate and sustain a coherent response to an interpretive challenge induced at abstract or metaphorical levels on neutral topics that a casual open-ended conversation might conceal. Although less abstract topics, such as ‘What would someone have to do if they wanted to smoke a cigarette/wash their hair/do their laundry?’ (Just Reference Just, Bröcker and Ryazanskaya2023) or ‘Tell me the story of Cinderella’ (Fradkin Reference Fradkin, Adams and Siegelman2024), can also serve as a prompt, abstract topics perform better in identifying features of FTD, without the need to wait for a full story to unfold.
Clinical application
Deploy prompts requiring extended interpretive responses in standard mental state examination tests: ‘What does it mean to say too many cooks spoil the broth?’. Follow with non-directive encouragement if the verbal output is insufficient, for example ‘Can you say more?’. Include complex visual stimuli (preferably featuring human figures as in the TAT; see ‘Inducing mental state talk’ below for the rationale) to provide interpretive challenge.
Cognitive loading
Executive dysfunction figures prominently in theoretical models of FTD, with cognitive disorganisation or dyscontrol representing a major factor across multiple analyses (Roche Reference Roche, Creed and MacMahon2015; Zamperoni Reference Zamperoni, Tan and Rossell2024b). Yet surprisingly few scales explicitly tax executive resources during assessment.
The SCD takes the most direct approach, embedding deliberate semantic ambiguity into prompts. Polysemic words such as tie, pumps and rags appear in contexts that activate multiple meanings, forcing executive systems to maintain appropriate semantic selection while suppressing competing interpretations. This dual-task demand can unmask subtle FTD. Of note, ambiguity can also increase the likelihood of expressing delusional ideas (for examples, see the Discussing Abstract Ideas in Schizophrenia Corpus (DAIS-C; Delgaram-Nejad Reference Delgaram-Nejad, Archer and Chatzidamianos2023); this has been the basis of Rorschach inkblots and other projective tests. Several models argue that delusions are formed to explain an experienced ambiguity (Denecke Reference Denecke, Schönig and Bott2024).
An alternative approach which introduces memory load was originally used by Bleuler (the story of a donkey that soaked its cotton load from Aesop’s fables (Bleuler Reference Bleuler1950)); this is also utilised by contemporary scales like the CLANG. Story recall taxes memory, executive control and narrative organisation simultaneously. This differs fundamentally from using stories as thought-provoking stimuli (as in the KFTDS), as the cognitive demand of recall creates the stress test, likely taxing the processes required for coherent retelling.
Clinical application
Ask the patient to read an 8–10 sentence short story and retell it in their own words. The resulting discourse reveals how cognitive demands tax organisation of thoughts.
Affective reactivity and emotional topics
Some people with psychosis show more pronounced symptoms when negative affect is aroused. This thought–affect interface has been observed for features of FTD (Docherty Reference Docherty, Evans and Sledge1994; Cohen Reference Cohen and Docherty2004). Some scales formalise this observation by deliberately introducing emotional arousal as a probe: for example the Thought and Language Disorder (TALD) scale (Kircher Reference Kircher, Krug and Stratmann2014) states ‘Since some phenomena occur solely under situational stress (delusions, hallucinations, emotional life events), emotional topics should be raised’. This procedure operates under the assumption that if capacity to organise thoughts is marginal, emotional arousal may precipitate decompensation into manifest FTD. For some, describing delusional or hallucinatory content may be the only context where FTD becomes manifest.
Of note, many healthy individuals show transient speech disorganisation when intensely emotional – a phenomenon that forms the basis for Main’s Adult Attachment Interview to identify disorganised attachment (George Reference George, Main and Kaplan1985). The SCD acknowledges this caveat and takes the approach of advocating ‘shielded’ assessment that avoids discussion of symptoms entirely. This methodological choice also addresses another concern – that of ‘symptom leakage’ or contamination, for example awareness of a patient’s bizarre delusions or hallucinations may bias an observer to rate speech as more illogical or loose than it actually is (Palaniyappan Reference Palaniyappan, Homan and Alonso2022). The ideal solution – although difficult in clinical practice – involves separate assessment contexts: one shielded from symptom content (early part), another deliberately engaging emotional reactivity (later part). Comparing discourse across contexts provides the most informative picture.
Clinical application
After establishing baseline patterns through neutral discourse (the first three manoeuvres above), gradually introduce personally relevant emotional topics, such as health-related topics (symptoms or treatment). Monitor for structural deterioration: Does logical sequencing fragment? Do referential connections become unclear? Does coherence collapse under emotional load and then recover?
Inducing mental state talk
A growing body of literature on social cognition and FTD indicates that issues with theory of mind (i.e. perspective-taking) may explain some of the features of FTD (Minor Reference Minor, Marggraf and Davis2015; Achim Reference Achim, Achim and Fossard2022; Hardy-Baylé Reference Hardy-Baylé, Sarfati and Passerieux2003). The closest approximation to testing this aspect appears in the SCD’s assessment of perspective-taking: ‘In your opinion, what does your father/mother/friend/doctor think about your problems?’. This requires modelling others’ mental states – a social cognitive demand revealed in ‘mental state talk’ (Kim Reference Kim, Dore and Cho2021)’ (e.g. ‘She knows that he is going to leave her’). Picture description tasks featuring human figures also involve implicit social demand modulation. Describing what characters are doing, thinking or feeling requires theory of mind operations that engage social cognition alongside language organisation. Furthermore, the need to generate syntactically more complex clauses (e.g. when describing who did what to whom) in stories also increases the likelihood of grammatical errors associated with FTD (Elleuch Reference Elleuch, Chen and Luo2025b). The integration of these demands can unmask deficits not apparent in non-social narratives.
Clinical application
Impose perspective-taking demands: ‘If I asked your colleague/best friend about you, what would they say?’. This requires adopting another’s perspective while maintaining narrative coherence. Use of TAT pictures with human characters or cartoon storyboards (Achim Reference Achim, Achim and Fossard2022; Alonso-Sánchez Reference Alonso-Sánchez, Alfaro-Faccio and Allende-Cid2022; Cho Reference Cho, Balles and Mackinley2026) may also enforce perspective-taking and mental state talk.
Targeted clarification
Of all the techniques derived from rating scales, seeking targeted clarification is one the most important for clinical judgement. When explicitly requesting clarification for an unclear or illogical statement, the patient’s response helps us to differentiate accidental slips or drifts (successfully clarified) from more pervasive thought disorder (further confabulation or tangentiality). This should be practised at all phases of the interview.
Many factors can produce unclear speech – anxiety, unfamiliarity with medical settings, limited education or simply the universal difficulty of converting complex thoughts into linear language. Seeking clarification involves asking patients to access and re-present the thought they just expressed. If the thought is intact but expression was poor, clarification succeeds. If the thought is disorganised, clarification may reveal further drift. Successful clarification after prompts indicates effective conversational scaffolding; the ability to repair unclear speech with clinician support may suggest milder FTD compared with cases where scaffolding fails to improve coherence.
Several scales incorporate this principle. The TDI instructs raters to ‘inquire into all deviant verbalizations, percepts, slips, and reasoning’ (Johnston Reference Johnston1979). The BIT requires inquiry into ‘all unclear or odd words or responses’ (Harrow Reference Harrow and Quinlan1985). The TLI structures this as systematic follow-up after picture descriptions (Liddle Reference Liddle, Ngan and Caissie2002). The SCD goes a step further and marks ‘the inability to clarify a speech corpus’ as a marker of deficit in the integration of contextual information (Bazin Reference Bazin, Sarfati and Lefrère2005). The consistency across scales reflects recognition that clarification requests are not optional add-ons but essential diagnostic manoeuvres.
Clinical application
When an unclear or illogical statement occurs, resist the urge to move on. Instead ask: ‘I want to make sure I understand – what did you mean by that?’ or ‘Can you explain that in a different way?’. Successful clarification weakens the case for FTD. Progressive confusion, tangential drift or bizarre elaboration strengthen it.
Assessing subjective dimensions
Formal thought disorder encompasses both observable signs and subjective experiences. Observable signs are the external manifestations of disrupted thought organisation, including disturbances in the structure of speech (e.g. derailment, tangentiality, incoherence) and in its dynamics (e.g. pressure of thought, flight of ideas); these are what clinicians directly observe, and what FTD rating scales such as the Thought, Language and Communication scale (TLC; Andreasen Reference Andreasen1979) and TALD (Kircher Reference Kircher, Krug and Stratmann2014) are designed to capture. Subjective experiences are patients’ first-person awareness of their own thinking processes, such as thoughts that feel blocked, racing or out of control (Kircher Reference Kircher, Krug and Stratmann2014). These two dimensions do not always correlate perfectly (Kircher Reference Kircher, Krug and Stratmann2014): many patients with profound objective disorganisation report minimal subjective awareness. Direct questions about patients’ internal experiences therefore complement, rather than substitute for, observational techniques (Box 3). Notably, subjective features of dysfunctional thought and language organisation may phenomenologically overlap with the cognitive/psychomotor slowing of a depressive episode (Palaniyappan Reference Palaniyappan and Wang2025), with common elicitation procedures as we describe here. A list of these, adapted from the TALD (Kircher Reference Kircher, Krug and Stratmann2014), is provided in Box 3 for clinical application.
Interview questions for assessing subjective aspects of formal thought disorder
-
1. Initiative: Is thinking too much of an effort for you these days? Do you feel that you have the mental energy you used to have?
-
2. Slowing: Does your thinking feel slowed down, as if it is a heavy drag?
-
3. Blocking/fading: Does your train of thought ever just suddenly stop mid-sentence, like hitting a wall? Do your thoughts sometimes just slowly fade away?
-
4. Poverty: Have you noticed fewer new ideas or thoughts coming to you than before?
-
5. Pressure: Have you experienced too many thoughts coming at once, like you can’t control them?
-
6. Interference: Do you find it hard to stay focused because other thoughts keep jumping in, or things around you keep pulling your attention away?
-
7. Rumination: Are there certain thoughts or worries that you can’t seem to stop thinking about, even when you try to move on to something else?
-
8. Reception: When people are talking to you, can you follow along and understand them as easily as before? Do you find some words or sentences confusing?
-
9. Expression: How about expressing yourself – do you feel that you can say what you mean as clearly as you used to? Do you find some words or phrases hard to come by?
The questions should be organised in a natural conversational flow, starting with energy and speed and moving through specific domains of thinking, attention and communication. These subjective items are modified from Kircher’s Thought and Language Disorder Scale (Kircher Reference Kircher, Krug and Stratmann2014).
An integrated clinical approach
A sensitive clinical assessment of formal thought disorder needs to follow a structured, phased approach, and we suggest the following (Fig. 2).
An integrated clinical approach to eliciting formal thought disorder. This figure was generated using Google’s NotebookLM.

Phase 1: Open discourse (5 min) – start with minimal restrictions to establish baseline patterns. Ask open-ended questions about neutral topics (hobbies, daily life, interests) to encourage natural speech without structure. This phase shows spontaneous organisation, speech quantity and pacing, and baseline coherence before introducing more demands.
Phase 2: Structured provocation (5 min) – introduce interpretive and narrative demands for more goal-directed thoughts. Story generation, proverb interpretation, abstract questions and complex picture descriptions all need organising around external prompts. This phase shows how organisational processes work when needed for specific communication goals.
Phase 3: Placing demands (3–5 min) – deliberately stress neural systems supporting linguistic cognition. Story recall increases memory load. Emotional content engages the thought–affect interface. Inducing mental state talk via perspective-taking taxes social cognition. Not all patients need this phase (e.g. someone with pressured speech in a manic episode does not) – but when earlier phases yield ambiguous results, stress-testing can be crucial.
Phase 4: Verification of subjective phenomena (5 min) – finally, enquire about subjective aspects of thought disorder. Throughout all phases of the interview, systematically seek clarification for any deviations, unclear statements or illogical connections noted.
Practical considerations and limitations
It is important to note that not all seven elicitation manoeuvres are equally specific for diagnosing FTD. Findings from affective provocation should be interpreted cautiously. Transient disorganisation can occur in healthy individuals under anxiety or strong emotion, in patients with limited formal education or familiarity with clinical settings and in those speaking a second language. Spontaneous disorganisation (phases 1 and 2) that worsens with cognitive loading or perspective-taking demands (phase 3), and disorganisation that cannot be repaired through targeted clarification (phase 4), provide stronger evidence for genuine FTD. Clinicians should seek convergent evidence across multiple manoeuvres and prioritise recurring instances over isolated findings from the various phases of the interview. Broader controversies and ongoing debates regarding interpretation and diagnostic thresholds are summarised in Box 4.
Controversial issues and ongoing debates regarding formal thought disorder (FTD)
-
• The theoretical basis of FTD remains debated: is it primarily a disorder of associations, executive control, semantic memory or communication pragmatics?
-
• The specificity of FTD to psychotic disorders is questioned, as similar phenomena occur in mania, dementia and even normal individuals under stress or fatigue.
-
• Whether FTD should be understood as a categorical sign (present/absent) or a dimensional phenomenon existing on a continuum remains unresolved.
-
• The role of the listener in identifying speech as ‘disordered’ is increasingly recognised, raising questions about the objectivity of FTD assessment.
-
• Emerging computational linguistics and natural language processing approaches may provide objective, automated FTD assessment, but their clinical utility and ecological validity remain to be established.
-
• The relationship between observable FTD and subjective experiences of thought disorder (racing thoughts, thought blocking) is complex and not fully understood.
Time constraints
Starting with free, open-ended discourse, followed by visual and abstract prompts to induce thoughts, increasing processing load via recall demands or emotional content, and finally inducing social complexity to elicit mental state talk provides an optimal set of approaches to elicit FTD in a clinical setting (Fig. 1). Although there are several other approaches (e.g. showing videos of emotional stimuli and then asking standardised questions (Huang Reference Huang, Xu and Zhao2026), clinical reality often complicates idealised assessment procedures. Individuals with negative symptoms may lack the motivation for extended discourse. Guarded individuals may resist procedures perceived as testing their sanity. Children may find formal assessment threatening. Assessing FTD in a gamified manner with picture descriptions, story-telling and collaborative exploration as laid out above (‘Inducing mental state talk’), or with playful word associations (that help assess semantic priming) shifts the focus from evaluation to shared activity with the clinician. Such gamification can reduce the Hawthorne effect on verbal behaviour and ensure engagement for the 15–20 min of discourse needed for a reliable assessment (Caplan Reference Caplan, Guthrie and Fish1989).
FTD may manifest in written material (letters, texts, emails) and does not always co-occur with spoken FTD. Clinicians should review written samples when available, although care is needed when interpreting FTD in text messaging, because of format-specific conventions.
Significant others
A growing body of evidence from individuals with lived experience of FTD highlights a crucial yet often overlooked dimension: the listener’s role in co-constructing what clinicians call disordered speech (Hodgins Reference Hodgins, O’Driscoll and Titone2022; also see Galletly Reference Galletly and Crichton2011). Communication is inherently dyadic: what one person finds incoherent may be understood by another. This insight challenges assumptions about the objectivity of FTD assessment and highlights the value of underutilised assessment strategies, such as systematic observation of conversations with others (third parties). But such strategies face practical constraints in a clinical setting. Enquiring about conversational difficulties encountered by people (significant others) who spend considerable time with the patient will be a valuable source of information.
Cultural and linguistic considerations
Assessing FTD across different cultural and linguistic contexts requires additional care. What appears to be loose associations or circumstantiality may reflect cultural narrative styles or translation difficulties. Some languages have features that complicate assessment. For instance, Tamil has no formal definite (the) or indefinite (a/an) articles, but relies on context and demonstratives. A native Tamil speaker may miss such nuances in English, and this needs to be accommodated in assessments. Another example is Cantonese, where the same phonetic sound can map onto multiple words; these frequent homophones and puns should not be considered pathological. Whenever possible, involve clinicians familiar with the patient’s cultural background and primary language. When using interpreters, ensure they understand the assessment goals and can convey not just content, but also the structure and coherence of the patient’s speech.
Documentation
Detailed documentation should specify the discourse context in which FTD was observed or absent (neutral concrete, neutral abstract, emotional, psychosis-related topics). Record verbatim examples whenever possible (e.g. using embedded dictation systems), including the elicitation method used (e.g. picture description, proverb interpretation) and whether clarification attempts were successful. This provides a richer source for longitudinal comparison and assessment of treatment effects and allows other clinicians to understand the basis for your assessment.
Implications for training
The impression of decline in FTD assessment skills among psychiatrists (Tucker Reference Tucker1998; Sass Reference Sass and Parnas2017) reflects, in part, inadequacies in current training (Zamperoni Reference Zamperoni, Tan and Sumner2024a). Traditional teaching often portrays FTD assessment as a passive observation rather than an active elicitation skill. Medical students and trainees can be explicitly taught the manoeuvres described here, with practice and feedback opportunities. Reviewing clinical interview recordings and discussing them provides valuable learning. Transcribing interview portions helps analyse speech patterns and sharpens observational skills. Workplace-based assessments could evaluate trainees’ ability to elicit FTD using these techniques. Exposure to validated rating scales, even if not used clinically, provides frameworks for understanding FTD phenomenology. The publicly available DAIS-C (Delgaram-Nejad Reference Delgaram-Nejad, Archer and Chatzidamianos2023) schizophrenia speech corpus, including participants with advanced FTD, and the interviewer being an expert with lived experience of psychosis (Delgaram-Nejad Reference Delgaram-Nejad2024, Reference Delgaram-Nejad2025) can be a useful training aid for clinicians reviewing recent interactions. FTD itself is not a single natural kind of psychiatric object; it is a clinical entity constituted for practical purposes (Palaniyappan Reference Palaniyappan, Sreeraj and Venkatasubramanian2026). Sharpening our training to reliably elicit all its constituents is key to its utility in the psychiatric clinic.
Conclusion
Babette’s ‘double polytechnic irretrievable’, Nijinsky’s stream of disconnected statements and the more recent example from participant 26AR16 from DAIS-C all represent the dramatic end of the FTD spectrum. But FTD exists on a continuum, from subtle loosening detectable only through systematic probing to profound disorganisation that overwhelms routine communication. Mastering the clinical skills of stress-testing, clarification and verification of individuals’ subjective experience of FTD will improve how we measure, document and understand thought disorder as it unfolds in front of us in our clinics.
MCQs
Select the single best option for each question stem
-
1 Which of the following best describes the conceptual basis for assessing formal thought disorder (FTD)?
-
a FTD is a subjective symptom that patients will spontaneously report if present
-
b FTD is a collection of observable signs that requires active elicitation
-
c FTD can only be reliably assessed using standardised rating scales
-
d FTD assessment should focus exclusively on the patient’s written communication
-
e FTD is best evaluated through passive observation during routine clinical conversation.
-
-
2 What is the primary purpose of requesting clarification when a patient makes an unclear or illogical statement?
-
a To demonstrate to the patient that their communication is problematic
-
b To fill time during the interview when uncertain how to proceed
-
c To differentiate between poor expression and genuine thought disorder
-
d To test the patient’s frustration tolerance and emotion regulation
-
e To allow the interviewer time to formulate their diagnostic impression.
-
-
3 Which of the following is an appropriate application of cognitive loading in FTD assessment?
-
a Asking rapid-fire questions without allowing time for responses
-
b Reading a brief story and asking the patient to retell it in their own words
-
c Conducting the interview in a noisy environment with multiple distractions
-
d Requiring the patient to write their responses rather than speaking to them
-
e Repeatedly interrupting the patient mid-sentence to test their frustration tolerance.
-
-
4 When assessing FTD across different cultural and linguistic contexts, which approach is most appropriate?
-
a Applying standardised Western assessment criteria uniformly across all cultural groups
-
b Avoiding assessing FTD in non-native speakers, as it cannot be done reliably
-
c Focusing only on non-verbal behaviours when working with interpreters
-
d Ensuring interpreters can convey speech structure, not just content
-
e Relying exclusively on self-report measures, to avoid cultural bias.
-
-
5 The recommended phased approach to FTD assessment typically requires what minimum duration?
-
a 3–5 min
-
b 7–10 min
-
c 15–20 min
-
d 30–45 min
-
e 60 min or more.
-
MCQ answers
-
1 b
-
2 c
-
3 b
-
4 d
-
5 c
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Acknowledgements
We thank the members of DISCOURSE in Psychosis consortium (https://discourseinpsychosis.org/) and DIALOG team (https://dialog.discourseinpsychosis.org/) for many conversations that shaped our thoughts on this topic.
Author contributions
L.P. conceived the article, wrote the first draft, provided overall supervision and critically revised the manuscript. O.D.-N. and E.Y.H.C. contributed to the conceptual development of the article and critically revised the manuscript. All authors approved the final version and agree to be accountable for all aspects of the work.
Funding
L.P. is supported by the Monique H. Bourgeois Chair in Developmental Disorders and a salary award from the Fonds de recherche du Québec – Santé (FRQS: 366934) and supported by the FRQS through a Research Centre Grant to Douglas Research Centre (https://doi.org/10.69777/5230). O.D.-N.’s work is supported by a Wellcome Trust Mental Health Award for the DIALOG consortium (314138/Z/24/Z).
Declaration of interest
L.P. reports personal fees for serving as chief editor of the Canadian Medical Association journals; speaker fees from Janssen Inc., Canada, Otsuka Canada Pharmaceutical Inc. and SPMM Course Limited, UK; participation in advisory boards for Bausch Health and Bristol-Myers Squibb Canada; book royalties from Oxford University Press; and investigator-initiated educational grants from Otsuka Canada outside the submitted work, in the past 5 years.



 Open access
Open access
eLetters
No eLetters have been published for this article.