


Highlights
-
Lower CADS (≤3) post-EVT were linked to better 90-day outcomes, highlighting the role of imaging markers in BAO outcome prediction.
-
Younger age, lower NIHSS and successful reperfusion (mTICI 2b–3) were key factors for improved recovery.
-
BAO stroke outcomes are multifactorial, shaped by clinical, procedural and imaging factors.
Introduction
Intracranial large vessel occlusion is the most disabling cause of stroke accounting for 24–46% of acute ischemic strokes. Reference Rennert, Wali and Steinberg1 Among these, approximately 10% are caused by basilar artery occlusion (BAO), a condition with particularly poor outcomes. Reference Langezaal, van der Hoeven and Mont’Alverne2 Even with recent advances in the best medical treatment and endovascular therapy (EVT), 68–80% of patients with BAO die or are left severely disabled. Reference Solla, Argolo, Budohoski, Kolias, Caldas and Oliveira-Filho3,Reference Nguyen and Strbian4
The benefits of EVT for BAO remained unclear due to mixed evidence from earlier trials like BASICS and BEST, which failed to show a significant benefit. Nevertheless, these trials indicated potential EVT benefits for BAO patients with moderate-to-severe symptoms. Reference Solla, Argolo, Budohoski, Kolias, Caldas and Oliveira-Filho3–Reference Liu, Dai and Ye6 Recently, newer trials such as ATTENTION and BAOCHE demonstrated a clear benefit of EVT in reducing disability and mortality in BAO patients, further solidifying EVT’s role, particularly in those with moderate-to-severe symptoms. Reference Alemseged, Nguyen and Coutts7–Reference Pirson F.A., Boodt and Brouwer10 However, even in these studies, the mortality and disability rates following EVT remain high. In the ATTENTION trial, approximately 55% of patients in the EVT group had a significant disability (modified Rankin Scale, mRS > 3), and 35% died within 90 days. Similarly, in the BAOCHE trial, around 50% of EVT-treated patients experienced severe disability, with a 31% mortality rate. Reference Tao, Nogueira and Zhu5,Reference Jovin, Li and Wu8 This underscores the need for a deeper understanding of the factors that influence recovery trajectories and the critical importance of timely and effective reperfusion therapies.
Several studies have attempted to predict outcomes in BAO strokes. Reference Bouslama, Haussen and Aghaebrahim11–Reference Gory, Mazighi and Labreuche14 For instance, complete reperfusion (modified thrombolysis in cerebral infarction [mTICI] score 2b–3) has been identified as the strongest predictor of favorable recovery, surpassing factors like baseline National Institutes of Health Stroke Scale (NIHSS) scores and posterior circulation collateral flow. Reference Mahmoudi, Dargazanli and Cagnazzo15 Additionally, patient characteristics such as age, NIHSS score, diabetes and hypertension have been linked to outcomes. Reference Dornák, Herzig and Školoudík16 Cereda et al. Reference Cereda, Bianco and Mlynash17 introduced the Critical Area Perfusion Score (CAPS), an imaging marker that assesses the extent of brainstem hypoperfusion. They demonstrated that limited hypoperfusion (CAPS ≤ 3) before EVT strongly predicts favorable outcomes in patients with complete reperfusion. Recently, Karamchandani et al. Reference Karamchandani, Satyanarayana and Yang18 further validated the utility of pre-procedural perfusion imaging, including CAPS, for predicting final infarct volume after EVT in patients with BAO, reinforcing its prognostic value.
In parallel to their work, we utilized the Critical Area Diffusion Score (CADS) in diffusion-weighted MRI (DWI-MRI) post-EVT to evaluate its predictive accuracy for outcomes. Unlike the original CAPS, which assesses brainstem hypoperfusion, CADS does not measure perfusion but rather quantifies the extent and location of infarction within critical brainstem regions. The aim of our study is to identify predictors of favorable recovery including CADS.
Methods
Design and sample
This retrospective observational study aimed to collect data on BAO stroke patients who received EVT at our provincial comprehensive stroke center. Ethics approval was obtained from the University of Manitoba Health Research Ethics Board (REB number: HS22427 (H2018:506)).
The study included consecutive patients with acute ischemic stroke due to BAO who underwent EVT between January 1, 2015, and December 31, 2021. Patients were identified on admission and urgently assessed by the stroke team, including evaluations for thrombolysis and thrombectomy eligibility.
Inclusion criteria were (1) age ≥18 years; (2) pre-stroke modified Rankin Scale (mRS) 0–3; (3) no intracranial hemorrhage; (4) no well-established stroke on imaging; and (5) symptom onset within 24 hours.
Endovascular thrombectomy (EVT)
EVT was performed under conscious sedation or general anesthesia. Fellowship-trained interventional neuroradiologists and neurosurgeons conducted the EVT, with patients closely monitored in the high-observation unit for at least 24 hours post-procedure. Aspiration or stent retriever or a combination of the two were used, depending on the operators’ preference and the occlusion characteristics.
Data collection and imaging assessment
Clinical, demographic and imaging data were collected including age, gender, blood pressure, blood glucose, low-density lipoprotein, NIHSS, wake-up stroke status, thrombolysis administration and mTICI scores. Baseline, discharge and 90-day post-stroke mRS scores were retrieved from charts or by interviewing patients and families. Reperfusion was assessed using the TICI scale. Chart reviews were conducted in medical records department. Infarct size and location were quantified using the CADS, adapted from the original CAPS criteria Reference Cereda, Bianco and Mlynash17 and applied specifically to post-EVT diffusion-weighted MRI (DWI). The CADS assigns points based on the involvement of critical posterior circulation structures: one cerebellar hemisphere (1 point), bilateral cerebellar hemispheres (2 points), pons (2 points) and midbrain or thalamus (2 points) (Figure 1). A higher CADS indicates a more extensive infarction involving critical brainstem structures, potentially correlating with poorer clinical outcomes. Imaging analyses were conducted by a neurology resident (NF) under the direct supervision of a senior interventional neuroradiologist (JS).
Critical Area Diffusion Score (CADS). Illustrative examples of stroke infarcts (highlighted in blue) on diffusion-weighted imaging (DWI) for scoring CADS: involvement of a single cerebellar hemisphere (1 point), bilateral cerebellar hemispheres (2 points), pons (2 points) and midbrain or thalamus (2 points). Higher scores represent greater involvement of critical brainstem structures.

Outcome measures
Primary outcomes were mRS scores at discharge and 90 days, classified as favorable (0–3) or unfavorable (4–6). Secondary outcomes included infarct size and location using CADS.
Statistical analysis
All statistical analyses were conducted using R/RStudio version 4.3.2 and the tidyverse package. Patients were categorized into two groups based on their mRS and CADS scores (favorable outcomes [mRS 0–3] and unfavorable outcomes [mRS 4–6]). Continuous variables (e.g., age, NIHSS, treatment times) were reported as medians with interquartile ranges (IQR), and group comparisons were made using the Mann–Whitney U test. Pearson’s chi-square test was applied to compare nominal and ordinal variables between groups. A p < 0.05 was considered statistically significant.
Statistical analyses were conducted using ordinal logistic regression to assess the shift in mRS scores across different groups of TICI and CADS categories. Patients were divided into TICI 0–2a versus TICI 2b–3 groups and CADS ≤ 3 versus CADS > 3 groups. Odds ratios (OR) were calculated to estimate the likelihood of a shift toward more favorable outcomes (mRS 0–3) within each group. A 95% confidence interval (CI) and p-values were used to determine statistical significance. Data visualization included ordinal shift bar plots to display mRS distribution across TICI and CADS groups.
Results
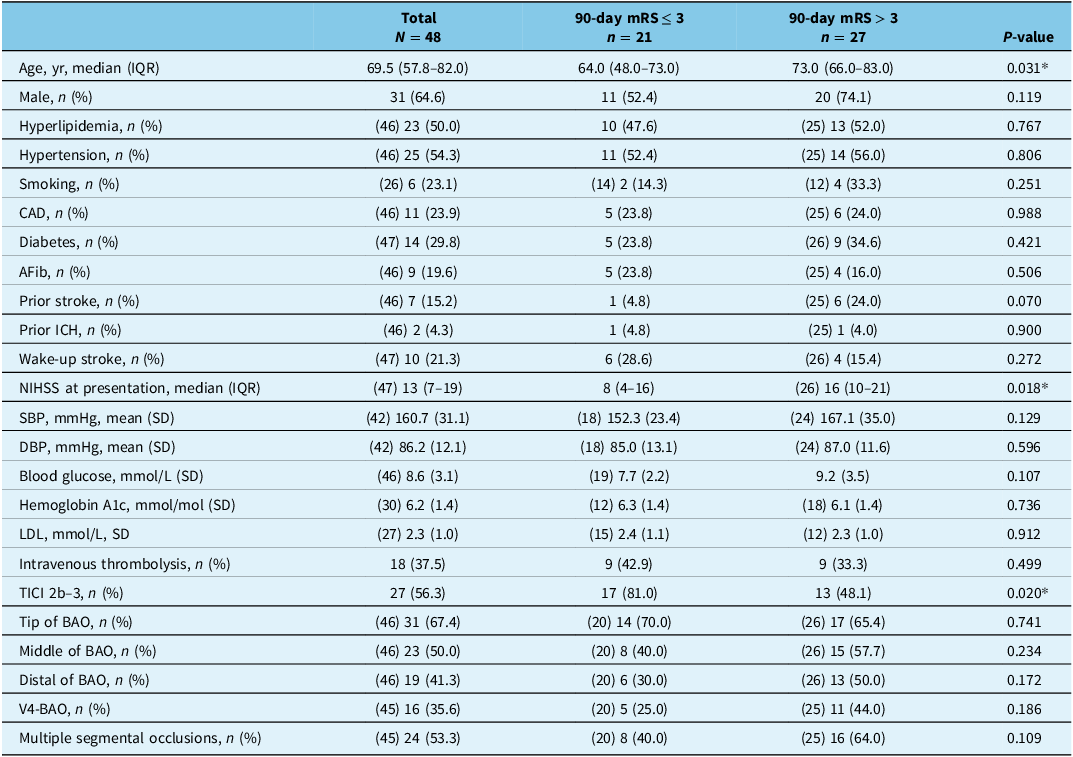
A total of 48 patients were included in the study, divided into two groups based on 90-day mRS scores: mRS ≤ 3 (n = 21, 43.8%) and mRS > 3 (n = 27, 56.3%). Demographic and baseline characteristics are summarized in Table 1.
Patient demographic, clinical characteristics and stroke presentation details by mRS

Table 1 Long description
The table presents data on 48 patients divided into two groups based on 90-day mRS scores: mRS 3 or less and mRS greater than 3. It includes columns for total patients, patients with 90-day mRS 3 or less, patients with 90-day mRS greater than 3, and P-values. The table has 25 rows with various demographic and clinical characteristics such as age, gender, medical conditions, stroke details, and treatment information. Each row provides specific data points for each group and the overall total. Notable trends include significant differences in age, NIHSS at presentation, and TICI 2b-3 percentages between the two groups.
*P<0.05; ** P <0.01; *** P <0.001; mRS = modified Rankin Scale; IQR = interquartile range; SD = standard deviation; CAD = coronary artery disease; AFib = atrial fibrillation; ICH = intracranial hemorrhage; NIHSS = National Institutes of Health Stroke Scale; SBP = systolic blood pressure; DBP = diastolic blood pressure; LDL = low-density lipoprotein; TICI score = thrombolysis in cerebral infarction score; BAO = basilar artery occlusion.
Patients in the mRS ≤ 3 group were significantly younger (median age 64.0 years, IQR 48.0–73.0) compared to those in the mRS > 3 group (median age 73.0 years, IQR 66.0–83.0; p = 0.031). They also had a lower NIHSS at presentation (median 8, IQR 4–16 vs. 16, IQR 10–21; p = 0.018) and a higher frequency of successful reperfusion (mTICI 2b–3 in 81.0% vs. 48.1%; p = 0.020).
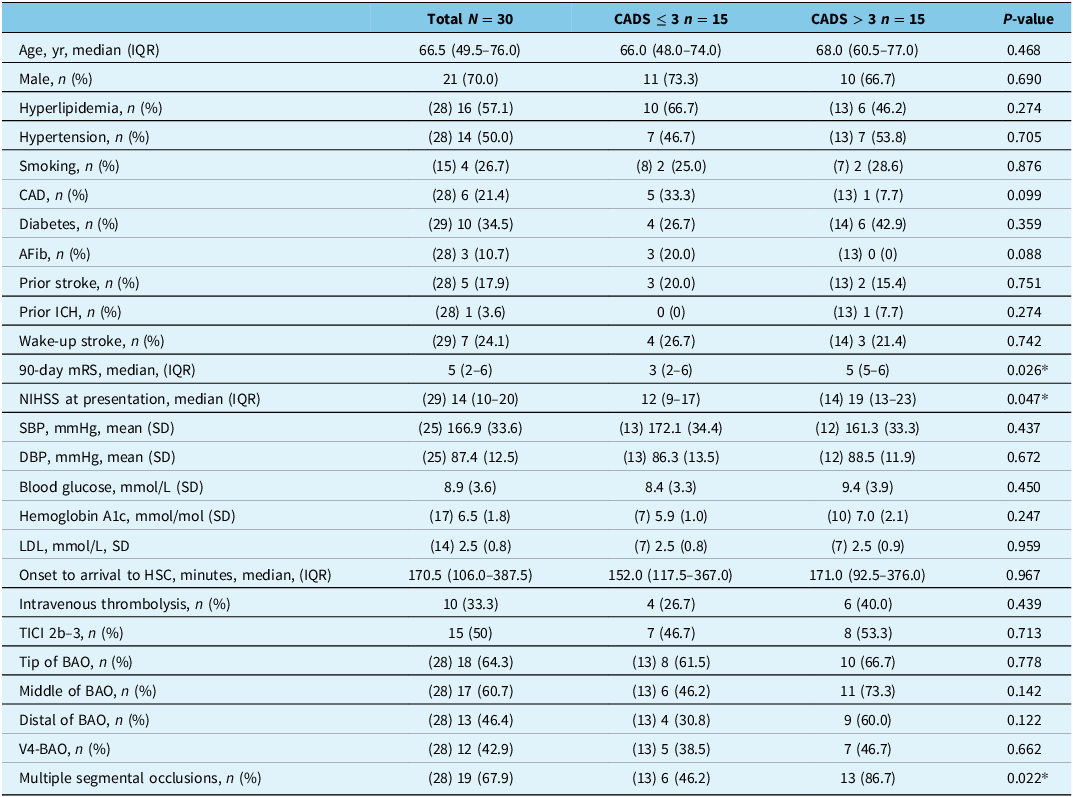
Thirty patients underwent follow-up DWI-MRI (Table 2). These patients were dichotomized into CADS ≤ 3 (n = 15) and CADS > 3 (n = 15). Patients with CADS ≤ 3 had significantly lower 90-day mRS scores (median 3, IQR 2–6 vs. 5, IQR 5–6; p = 0.026), lower NIHSS at presentation (median 12, IQR 9–17 vs. 19, IQR 13–23; p = 0.047) and fewer multiple segmental occlusions (46.2% vs. 86.7%).
Patient demographic, clinical characteristics and stroke presentation details by CADS

Table 2 Long description
The table compares patient demographics, clinical characteristics, and stroke presentation details by CADS, divided into two groups: CADS ≤ 3 and CADS > 3. The table has 30 rows and 15 columns. Column headers include Total N = 30, CADS ≤ 3 n = 15, CADS > 3 n = 15, and P-value. Row labels include Age, Male, Hyperlipidemia, Hypertension, Smoking, CAD, Diabetes, AFib, Prior stroke, Prior ICH, Wake-up stroke, 90-day mRS, NIHSS at presentation, SBP, DBP, Blood glucose, Hemoglobin A1c, LDL, Onset to arrival to HSC, Intravenous thrombolysis, TICI 2b–3, Tip of BAO, Middle of BAO, Distal of BAO, V4-BAO, and Multiple segmental occlusions. Each row provides specific values for each category. Notable trends include differences in 90-day mRS scores, NIHSS at presentation, and the presence of multiple segmental occlusions between the two groups.
*P<0.05; ** P <0.01; *** P <0.001; CADS = Critical Area Diffusion Score; IQR = interquartile range; SD = standard deviation; CAD = coronary artery disease; AFib = atrial fibrillation; ICH = intracranial hemorrhage; mRS = modified Rankin Scale; NIHSS = National Institute of Health Stroke Scale; SBP = systolic blood pressure; DBP = diastolic blood pressure; LDL = low-density lipoprotein; HSC = Health Sciences Centre (Winnipeg, Manitoba); TICI score = thrombolysis in cerebral infarction score; BAO = basilar artery occlusion.
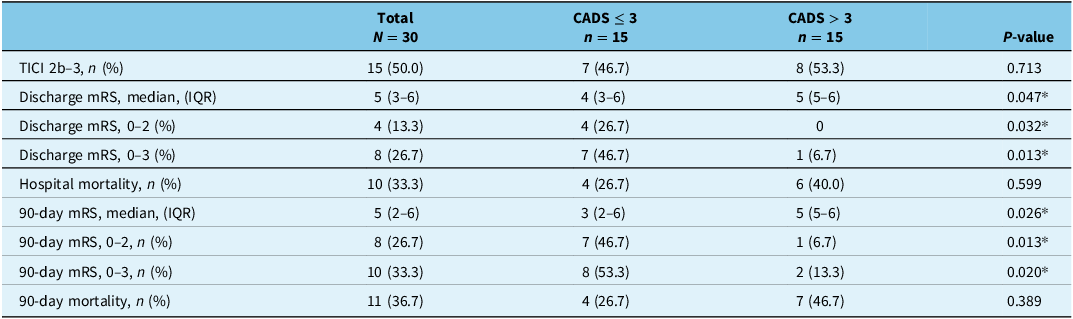
Table 3 compares clinical outcomes between patients with CADS > 3 and CADS ≤ 3. The results show significantly lower mRS scores at discharge (p = 0.013) and 90 days (p = 0.020) for CADS ≤ 3 patients.
Comparison of clinical outcomes of patients by CADS > 3 and CADS ≤ 3

Table 3 Long description
The table compares clinical outcomes of patients with CADS scores greater than 3 and CADS scores of 3 or less. It has 10 rows and 5 columns. The columns are labeled Total, CADS 3, CADS > 3, and P-value. The rows are labeled with different clinical outcomes and their respective values. Row 1: TICI 2b-3, n (%), Total 15 (50.0), CADS 3 7 (46.7), CADS > 3 8 (53.3), P-value 0.713. Row 2: Discharge mRS, median (IQR), Total 5 (3-6), CADS 3 4 (3-6), CADS > 3 5 (5-6), P-value 0.047. Row 3: Discharge mRS, 0-2, n (%), Total 4 (13.3), CADS 3 4 (26.7), CADS > 3 0 (0), P-value 0.032. Row 4: Discharge mRS, 0-3, n (%), Total 8 (26.7), CADS 3 7 (46.7), CADS > 3 1 (6.7), P-value 0.013. Row 5: Hospital mortality, n (%), Total 10 (33.3), CADS 3 4 (26.7), CADS > 3 6 (40.0), P-value 0.599. Row 6: 90-day mRS, median (IQR), Total 5 (2-6), CADS 3 3 (2-6), CADS > 3 5 (5-6), P-value 0.026. Row 7: 90-day mRS, 0-2, n (%), Total 8 (26.7), CADS 3 7 (46.7), CADS > 3 1 (6.7), P-value 0.013. Row 8: 90-day mRS, 0-3, n (%), Total 10 (33.3), CADS 3 8 (53.3), CADS > 3 2 (13.3), P-value 0.020. Row 9: 90-day mortality, n (%), Total 11 (36.7), CADS 3 4 (26.7), CADS > 3 7 (46.7), P-value 0.389.
*P<0.05; ** P <0.01; *** P <0.001; CADS = Critical Area Diffusion Score; TICI score = thrombolysis in cerebral infarction score; mRS = modified Rankin Scale.
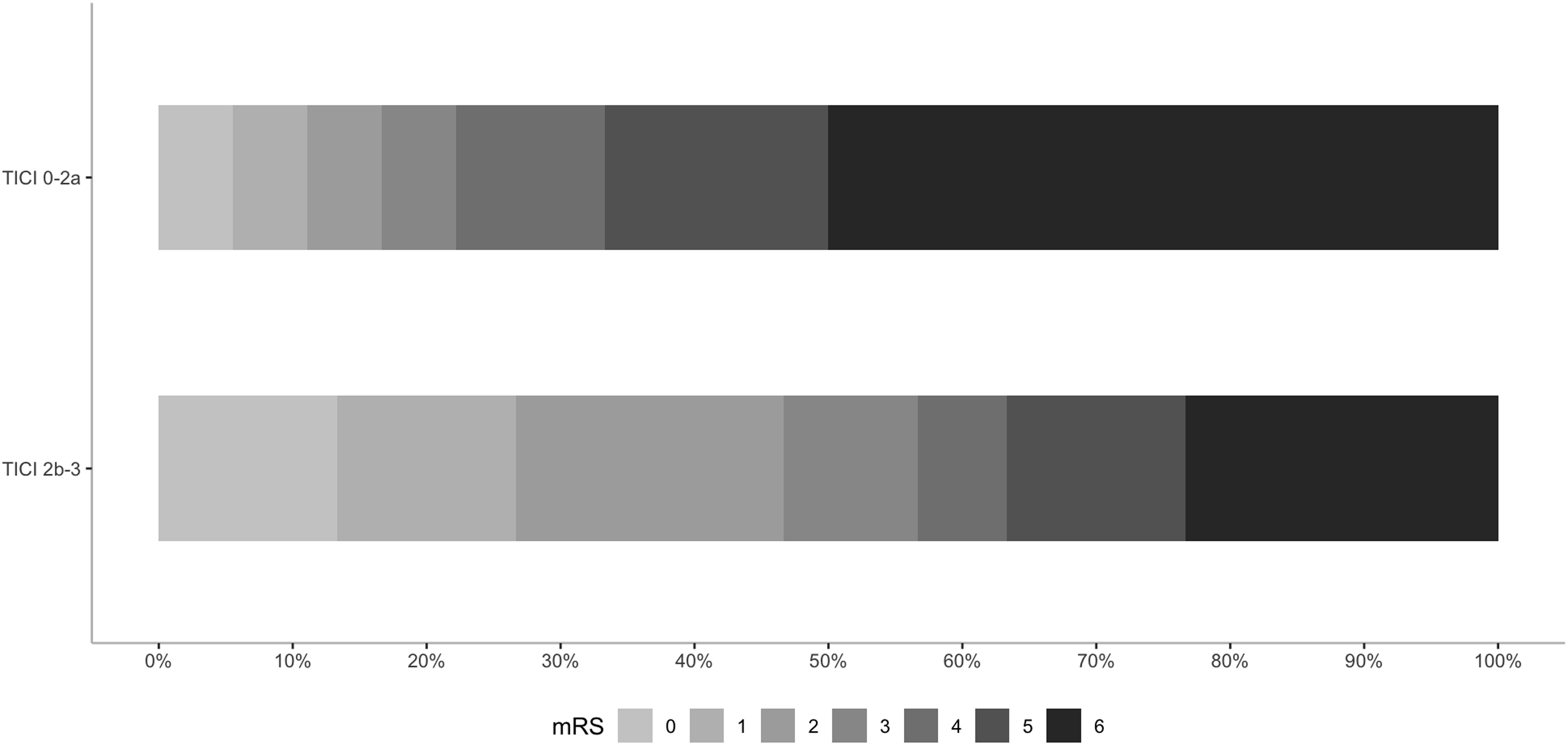
Figures 2 and 3 show an mRS ordinal shift analysis for CADS and TICI scores, respectively. Patients with CADS ≤ 3 had a significantly higher odds for favorable outcomes (mRS 0–3) compared to those with CADS > 3 (cOR = 5.2, 95% CI = 1.3–22.3, p = 0.022). Patients with TICI 2b–3 had significantly higher odds for favorable outcomes (mRS 0–3) compared to those with TICI 0–2a (cOR = 3.4, 95% CI = 1.1–11.3, p = 0.036).
Distribution of modified Rankin Scale scores by Critical Area Diffusion Score (CADS) > 3 and CADS ≤ 3.

Distribution of modified Rankin Scale scores by thrombolysis in cerebral infarction (TICI) 0–2a and TICI 2b–3.

The ROC curve analysis shows the predictive accuracy of CADS and TICI in determining favorable outcomes (mRS 0–3). The area under the curve (AUC) for CADS is 0.70, indicating a good ability to predict favorable outcomes. In contrast, the AUC for TICI is 0.66, which demonstrates similar predictive power.
When examined under a univariate logistic regression, CADS ≤ 3 is a strong predictor of favorable outcomes (OR = 10.89, 95% CI = 1.57–222.09, p = 0.038), and per-unit increases in baseline NIHSS highly predict slightly worse outcomes (OR = 0.86, 95% CI = 0.76–0.95, p = 0.007) (Table 4). In a multivariate logistic regression, successful reperfusion indicates considerably increased odds of favorable outcomes when controlling for CADS ≤ 3 and baseline NIHSS (OR = 18.8, 95% CI = 1.63–659.96, p = 0.044). Similarly, one-unit increases in baseline NIHSS decrease the odds of favorable outcomes by 18% (OR = 0.82, 95% CI = 0.65–0.98, p = 0.048) when controlling for CADS ≤ 3 and successful reperfusion. On multivariate analysis, CADS ≤ 3 was not found to be a significant predictor of favorable outcomes (OR = 9.05, 95% CI = 0.78–264.13, p = 0.113) (Tables 5 and 6).
Univariate and multivariate analysis of CADS and predictors of favorable outcomes in BAO patients

Table 4 Long description
A table comparing univariate and multivariate analysis of CADS and predictors of favorable outcomes in BAO patients. The table has 6 rows and 6 columns. Column headers are: Univariate OR, Univariate 95% CI, Univariate P-value, Multivariate OR, Multivariate 95% CI, Multivariate P-value. Row labels are: CADS ≤ 3, Reperfusion, Age scaled by 10 years, Gender, Baseline NIHSS. Row 1: Univariate OR, 10.89; Univariate 95% CI, 1.57–222.09; Univariate P-value, 0.038*; Multivariate OR, 7.94; Multivariate 95% CI, 0.65–245.34; Multivariate P-value, 0.144. Row 2: Univariate OR, 2.89; Univariate 95% CI, 0.74–14.53; Univariate P-value, 0.149; Multivariate OR, 12.45; Multivariate 95% CI, 0.77–670.48; Multivariate P-value, 0.124. Row 3: Univariate OR, 0.76; Univariate 95% CI, 0.52–1.09; Univariate P-value, 0.144; Multivariate OR, 0.78; Multivariate 95% CI, 0.26–2.19; Multivariate P-value, 0.643. Row 4: Univariate OR, 1.02; Univariate 95% CI, 0.26–3.68; Univariate P-value, 0.978; Multivariate OR, 0.65; Multivariate 95% CI, 0.01–45.09; Multivariate P-value, 0.834. Row 5: Univariate OR, 0.86; Univariate 95% CI, 0.76–0.95; Univariate P-value, 0.007**; Multivariate OR, 0.82; Multivariate 95% CI, 0.63–0.98; Multivariate P-value, 0.070.
*P<0.05; ** P <0.01; *** P <0.001; OR = odds ratio; CI = confidence interval; CADS = Critical Area Diffusion Score; NIHSS = National Institute of Health Stroke Scale.
Predictive power of CADS and reperfusion adjusted for baseline NIHSS and age

Table 5 Long description
A table comparing univariate and multivariate analysis of CADS, reperfusion, age, and baseline NIHSS. The table has 4 rows and 6 columns. Column headers are Univariate OR, Univariate 95% CI, Univariate P-value, Multivariate OR, Multivariate 95% CI, and Multivariate P-value. Row labels are CADS ≤ 3, Reperfusion, Age scaled by 10 years, and Baseline NIHSS. Row 1: Univariate OR, 10.89; Univariate 95% CI, 1.57–222.09; Univariate P-value, 0.038*; Multivariate OR, 7.83; Multivariate 95% CI, 0.65–237.58; Multivariate P-value, 0.144. Row 2: Univariate OR, 2.89; Univariate 95% CI, 0.74–14.53; Univariate P-value, 0.149; Multivariate OR, 13.72; Multivariate 95% CI, 0.88–602.48; Multivariate P-value, 0.102. Row 3: Univariate OR, 0.76; Univariate 95% CI, 0.52–1.09; Univariate P-value, 0.144; Multivariate OR, 0.85; Multivariate 95% CI, 0.39–1.83; Multivariate P-value, 0.658. Row 4: Univariate OR, 0.86; Univariate 95% CI, 0.76–0.95; Univariate P-value, 0.007**; Multivariate OR, 0.82; Multivariate 95% CI, 0.64–0.97; Multivariate P-value, 0.049*.
*P<0.05; ** P <0.01; *** P <0.001; OR = odds ratio; CI = confidence interval; CADS = Critical Area Diffusion Score; NIHSS = National Institute of Health Stroke Scale.
Impact of CADS, reperfusion and NIHSS on predicting favorable outcomes in BAO patients

Table 6 Long description
A table with two main sections: Univariate and Multivariate analysis. The table has three rows labeled CADS ≤ 3, Reperfusion, and Baseline NIHSS, and four columns labeled OR, 95% CI, and P-value under each section. Row 1: CADS ≤ 3, Univariate OR 10.89, 95% CI 1.57–222.09, P-value 0.038*, Multivariate OR 9.05, 95% CI 0.78–264.13, P-value 0.113. Row 2: Reperfusion, Univariate OR 2.89, 95% CI 0.74–14.53, P-value 0.149, Multivariate OR 18.8, 95% CI 1.63–659.96, P-value 0.044*. Row 3: Baseline NIHSS, Univariate OR 0.86, 95% CI 0.76–0.95, P-value 0.007**, Multivariate OR 0.82, 95% CI 0.65–0.98, P-value 0.048*.
*P<0.05; ** P <0.01; *** P <0.001; OR = odds ratio; CI = confidence interval; CADS = Critical Area Diffusion Score; NIHSS = National Institute of Health Stroke Scale.
Discussion
Our study identified several key factors influencing the outcomes of BAO stroke patients undergoing EVT, including age, NIHSS score at presentation, successful reperfusion as evidenced by TICI scores and the extent of infarction post-reperfusion assessed using the CADS. These factors collectively contribute to the diverse recovery trajectories observed in BAO patients.
Age and NIHSS at presentation
Patients who achieved a favorable outcome (mRS ≤ 3) at 90 days were significantly younger and presented with lower NIHSS scores compared to those with less favorable outcomes (mRS > 3). Specifically, the median age for the favorable outcome group was 64.0 years versus 73.0 years for the less favorable group (p = 0.031), and the median NIHSS scores were 8 versus 16, respectively (p = 0.018). These findings align with existing literature that identifies younger age and lower baseline NIHSS scores as critical predictors of better recovery in stroke patients. Reference Bouslama, Haussen and Aghaebrahim11,Reference Dornák, Herzig and Školoudík16 Younger patients may have better neuroplasticity and fewer comorbidities, contributing to improved outcomes. Reference Liew, Schweighofer and Cole19
Impact of successful reperfusion
Our results emphasize the significant role of successful reperfusion in functional recovery. Patients achieving TICI 2b–3 scores demonstrated higher rates of favorable outcomes compared to those with lower TICI scores (81.0% vs. 48.1%; p = 0.020). This underscores the importance of timely and effective reperfusion therapies in BAO stroke management. Previous trials, such as ATTENTION and BAOCHE, have demonstrated the benefits of achieving successful reperfusion in reducing disability and mortality among BAO patients. Reference Tao, Nogueira and Zhu5,Reference Alemseged, Nguyen and Coutts7,Reference Jovin, Li and Wu8 However, our findings also suggest that successful reperfusion alone may not guarantee favorable outcomes, as other factors like baseline stroke severity and patient age play significant roles.
Role of CADS
While age, NIHSS scores and TICI scores are established predictors of outcomes in BAO stroke, Reference Bouslama, Haussen and Aghaebrahim11,Reference Dornák, Herzig and Školoudík16 the role of imaging markers such as CAPS has been less explored. Cereda et al. Reference Cereda, Bianco and Mlynash17 introduced CAPS using CT and MR perfusion imaging before EVT to assess the severity of hypoperfusion and predict outcomes. In contrast, our CADS assesses infarct size and location based explicitly on DWI-MRI after EVT, focusing on confirmed infarct regions within predefined critical areas of the posterior circulation (cerebellum, pons, midbrain and/or thalamus). Figure 1 illustrates the scoring of CADS based on infarct distribution.
Another study from the same group demonstrated that pre-procedural cerebral perfusion imaging can effectively predict the final infarct volume in patients undergoing basilar artery thrombectomy. Reference Yuen, Mlynash and O’Riordan20 This study found that specific perfusion parameters correlated with the extent of irreversible brain damage after EVT, highlighting the importance of imaging in outcome prediction and individualized treatment planning.
Karamchandani et al. Reference Karamchandani, Satyanarayana and Yang18 demonstrated a correlation between pre-EVT perfusion parameters (original CAPS) and post-EVT infarct volume on DWI, validating pre-EVT imaging’s predictive role. Our study extends this by highlighting the clinical relevance of post-EVT imaging: identifying precise infarct locations within critical brainstem areas allows precise prognostic stratification for patients who have undergone successful reperfusion. While pre-EVT imaging is critical for guiding treatment decisions, post-EVT CADS adds significant value by providing an accurate prognosis for individual patients. The CADS score offers a structured, region-based approach to quantifying brainstem infarction, which can aid in prognostication, family counseling and rehabilitation planning.
Patients with CADS ≤ 3 exhibited significantly better median mRS scores at 90 days compared to those with CADS > 3 (median mRS 3 vs. 5; p = 0.020). This suggests that lower CADS scores correlate with better functional outcomes, supporting the potential utility of CADS in assessing recovery potential.
However, in our multivariate analysis, CADS did not remain an independent predictor of favorable outcomes when adjusted for successful reperfusion and baseline NIHSS scores (OR = 9.05; 95% CI = 0.78–264.13; p = 0.113). This may be due to the limited sample size and the possibility that CADS is interrelated with other clinical variables. This highlights the complexities in predicting stroke outcomes and suggests that while CADS is a useful tool, it should be considered alongside other significant factors like reperfusion success.
Our study aligns with the multifaceted approach to prognostication in BAO stroke suggested by recent research. For instance, the Charlotte Large Artery Occlusion Endovascular Therapy Outcome Score incorporates factors such as age, NIHSS score, glucose level and pre-thrombectomy imaging findings to predict outcomes. Reference Karamchandani, Satyanarayana and Yang18 This supports the notion that a combination of clinical and imaging markers, rather than a single factor, is crucial for accurate outcome prediction in BAO stroke.
Given these insights, our study not only reaffirms the multifactorial nature of stroke outcomes influenced by traditional clinical assessments but also introduces post-EVT DWI as a valuable tool in this predictive landscape. By integrating CADS with other established markers, we could potentially develop a more precise predictive model for long-term recovery.
Limitations
This study is constrained by its retrospective nature and the relatively small cohort size. A notable limitation is the application of the CADS post-EVT, differing from its original use pre-EVT, which may affect comparability. While demonstrating the utility of post-EVT DWI in predicting outcomes, future research should explore if a combined pre- and post-EVT imaging approach could further refine prediction accuracy.
Additionally, prospective trials are needed to validate CADS as a reliable predictor of long-term outcomes in BAO patients. Future research should investigate whether CADS, when combined with other markers such as NIHSS and collateral flow, could offer an even more accurate predictive model for long-term recovery.
Conclusion
Our study identifies age, NIHSS scores and successful reperfusion as significant predictors of recovery outcomes in patients with BAO. While lower post-EVT CADS scores were associated with better outcomes in univariate analysis, CADS did not remain an independent predictor when controlling for other factors. These findings suggest that while advanced imaging markers like CADS have potential utility, they should be interpreted alongside established clinical indicators.
Author contributions
NF collected the data, interpreted the imaging findings and drafted the manuscript. MA assisted with statistical analysis and data interpretation. SA contributed to data collection and ethics approval submission. JS provided conceptual guidance, oversaw all stages of the project development and offered critical revisions to the final manuscript.
Funding statement
No funding was received for the preparation of this review article.
Competing interests
The authors declare no competing interests.






 Open access
Open access
Target article
Evaluating the Role of Post-Thrombectomy MRI in Predicting Functional Recovery in Basilar Artery Occlusion
Related commentaries (1)
Reviewer Comment on Farhani et al. “Evaluating the Role of Post-Thrombectomy MRI in Predicting Functional Recovery in Basilar Artery Occlusion”