


The favourable evidence of effectiveness and cost-effectiveness of Early Intervention for Psychosis (EIP) services has motivated their implementation worldwide. Reference Csillag, Nordentoft, Mizuno, Jones, Killackey and Taylor1 Such evidence, however, comes almost entirely from high-income countries (HICs). Reference Correll, Galling, Pawar, Krivko, Bonetto and Ruggeri2–Reference Farooq, Fonseka, Ali, Milner, Hamid and Sheikh4 In low- and middle-income countries (LMICs) the duration of untreated psychosis (DUP) is longer and the treatment gap higher. Reference Farooq, Large, Nielssen and Waheed5 Therefore, it is crucial to generate local evidence to adequately implement this model of care. Reference Singh, Javed, Thara, Chadda, Iyer and Stefanis6
An adequate implementation should align service availability with people’s needs in a timely manner. Such services should be sensitive to the context, promoting recovery through engaging, collaborative rapport and continuity of care. Additionally, these services might require adaptation to the local culture, but keeping interventions as close as possible to the original protocols to secure fidelity. Reference Addington, Birchwood, Jones, Killackey, McDaid and Melau7 Finally, a sustainable scaling-up requires sufficient and continuous funding. Reference Saxena, Thornicroft, Knapp and Whiteford8
Because resources are limited, implementing a new intervention imposes an opportunity cost on those who do not receive care, on account of resources being invested elsewhere. Reference Drummond, Sculpher, Claxton, Stoddart and Torrance9 In this case, if EIP services are not cost-effective in the health systems where they are being implemented, such resources can be better used elsewhere. Furthermore, once services are established, disinvestment can be difficult and poorly managed changes may disrupt care pathways. On the other hand, not implementing interventions that are cost-effective is an inefficient use of resources and hinders people from receiving useful interventions. Reference Drummond, Sculpher, Claxton, Stoddart and Torrance9
Chile is a Latin American country with approximately 20.1 million inhabitants. Although considered a HIC since 2013 by the World Bank, the country presents high levels of inequality and poverty. Mental disorders are responsible for nearly 10% of the burden of diseases, 10 and a recent study estimated the incidence of first-episode of psychosis at 18.9 (CI: 18.7–19.1) per 100 000 person-years. Reference González-Valderrama, Jongsma, Mena, Castañeda, Nachar and Undurraga11 The treatment of schizophrenia is prioritised by an explicit health benefit plan known as Garantias Explícitas en Salud (GES). This includes pharmacological and psychosocial interventions provided by community mental health teams (CMHT) at secondary care. Although such a package of care is backed up by evidence of cost-effectiveness, Reference Chisholm, Gureje, Saldivia, Villalón Calderón, Wickremasinghe and Mendis12 in practice, patients attending CMHT receive medications but rarely other types of intervention. Reference Markkula, Alvarado and Minoletti13
This situation has motivated the development of services specially dedicated to help people in the early stages of psychosis. Reference Gaspar, Castillo, Maturana, Villar, Ulloa and González14 Such developments are similar to pioneering EIP initiatives in Australia and England, where these services are now provided nationwide. However, before expanding these services to the national level in Chile, local evidence is paramount. The importance of local evidence in LMICs has been highlighted by a recent review that found EIP interventions in only three LMICs (India, Iran and Uganda). Reference Farooq, Fonseka, Ali, Milner, Hamid and Sheikh4 The authors observed that no information about the cost-effectiveness of EIP services in LMICs could be found. Since that review was conducted, an economic evaluation of Brazilian EIP services has been published Reference Aceituno, Razzouk, Jin, Pennington, Gadelha and Bressan15 which, to the extent of our knowledge, is the only cost-effectiveness analysis of an EIP service in a LMIC.
Given the scarcity of economic evidence of EIP services derived from LMICs, despite the recognised importance of local evidence, our aim was to estimate the cost-effectiveness of implementing EIP services within the Chilean health system.
Method
Study design
We carried out an economic evaluation comparing EIP services against CMHT from the health system perspective following current methodological guidelines. Reference Kristensen, Husereau, Huić, Drummond, Berger and Bond16 This economic evaluation was a cost-utility analysis using a decision analytical model, following the guidance in the ISPOR-SMDM Task Force reports. Reference Caro, Briggs, Siebert and Kuntz17 This report also complies with the updated Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guidelines for economic evaluations. Reference Husereau, Drummond, Augustovski, de Bekker-Grob, Briggs and Carswell18
Study population
The population of interest was people aged 15–35 years with a first episode of psychosis (FEP). This includes the category of schizophrenia and other primary psychotic disorders according to ICD-10. Psychoses due to affective disorders (bipolar disorder and depression) are covered by other guidelines, and were excluded from this evaluation. Psychoses secondary to medical conditions or substance abuse were also excluded.
Interventions
The intervention consisted of an EIP service according to international consensus statements, implemented in an urban area of Santiago. Reference Bertolote and McGorry19 These services comprise a multidisciplinary team providing mental healthcare exclusively for people with a FEP, with a case-to-client ratio lower than that of standard care. The specific interventions include low-dose antipsychotics, psychological therapy, family psychoeducation and vocational support. Furthermore, the clinical teams implement internal audit and regular meetings as recommended by EIP fidelity scales. Reference Addington, Birchwood, Jones, Killackey, McDaid and Melau7 The comparator was treatment by CMHT. These services provide interventions for people with schizophrenia according to national guidelines, but they are not exclusively aimed at the early stages of psychosis and professionals must deliver care for people with other mental disorders.
Economic outcomes
Economic outcomes included the following: (a) costs measured in 2018 Chilean pesos (CLP); (b) benefits measured as quality-adjusted life-years (QALYs); and (c) incremental cost-effectiveness ratio (ICER) according to the following equation:
 $${\bf ICER}= {{\boldsymbol C}_{{\bf EIP}}-{\boldsymbol C}_{{\bf CMHT}} \over {\boldsymbol E}_{{\bf EIP}}-{\boldsymbol E}_{{\bf CMHT}}}$$
$${\bf ICER}= {{\boldsymbol C}_{{\bf EIP}}-{\boldsymbol C}_{{\bf CMHT}} \over {\boldsymbol E}_{{\bf EIP}}-{\boldsymbol E}_{{\bf CMHT}}}$$
where C EIP is mean costs of EIP, C CMHT is mean costs of CMHT, E EIP is mean effectiveness of EIP and E CMT is mean effectiveness of CMHT
Additionally, we used the net benefit approach to account for uncertainty in ICERs. The net benefit approach includes a theoretical (although unknown) value (λ) that society would place on one unit in improvement in the outcome of interest. Reference Stinnett and Mullahy20 This approach overcomes the limitations in the interpretation of ICER confidence intervals, and allows comparisons on the same scale:
 $${\bf NB}=\left(\Delta \boldsymbol{E} \times \boldsymbol{\lambda }\right)-\Delta \boldsymbol{C}$$
$${\bf NB}=\left(\Delta \boldsymbol{E} \times \boldsymbol{\lambda }\right)-\Delta \boldsymbol{C}$$
where NB is the net benefit approach, Δ E is differences in effects, Δ C is differences in costs and λ is willingness to pay.
At the moment, because Chile does not have an explicit cost-effectiveness threshold to specify λ , as a benchmark we utilised the World Health Organization (WHO) recommendation of using 1–3 times gross domestic product (GDP) per capita (USD 15 923). However, because such a threshold has been criticised for overestimating the cost-effectiveness of interventions, we tested lower values of λ in the sensitivity analysis.
A 10-year time horizon was considered appropriated in the base case analysis, because it is the longest follow-up from a randomised controlled trial registered in the literature. Reference Secher, Hjorthøj, Austin, Thorup, Jeppesen and Mors21 Longer time horizons, including 20 years, 30 years and lifetime horizon (considering an average life expectancy of 80 years in the Chilean population), were evaluated in the sensitivity analysis. Costs and effects were discounted at 3.0% to reflect time preference by valuing future costs and health outcomes slightly less than present ones, in line with standard methodological recommendations. Reference Kristensen, Husereau, Huić, Drummond, Berger and Bond16
Economic model
Model conceptualisation
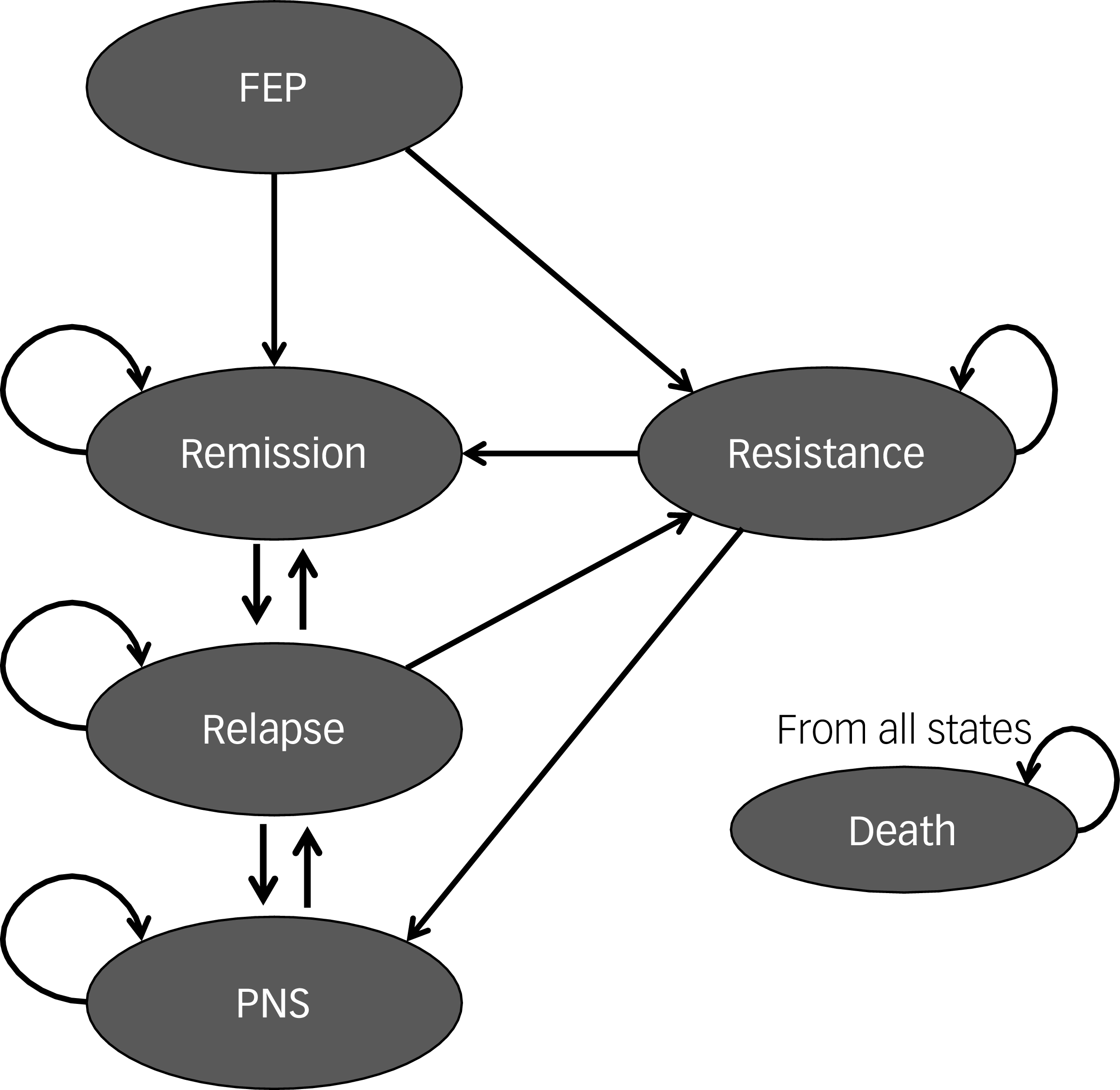
Model selection followed an iterative approach, including inputs from local stakeholders (clinicians and policy-makers), Chilean clinical guidelines and a systematic review of decision models covering the entire pathway of care for people with schizophrenia. Reference Jin, Tappenden, Robinson, Achilla, MacCabe and Aceituno22 The model comprised a transition model of six health states, also known as a Markov model, with 3-month cycles capturing states considered relevant to the decision context. Briefly, a Markov model is a mathematical model using transition probabilities that represents patients moving between mutually exclusive health states over time, to estimate long-term costs and health outcomes. Reference Caro, Briggs, Siebert and Kuntz17 A schematic representation can be found in Fig. 1.
Markov model conceptualisation. FEP, first-episode psychosis; PNS, persistent negative symptoms.

According to this model, a cohort of FEP patients moves between mutually exclusive health states defined by transition probabilities. People with a FEP experience variable degrees of symptom remission, which was defined by the Positive and Negative Syndrome Scale (PANSS) according to the Andreasen criteria. Reference Andreasen, Carpenter, Kane, Lasser, Marder and Weinberger23 Those who do not recover can develop treatment-resistant schizophrenia if they do not respond to two trials of antipsychotic medications at 600 mg equivalent of chlorpromazine, as recommended by consensus guidelines. Reference Howes, McCutcheon, Agid, de Bartolomeis, van Beveren and Birnbaum24 People achieving remission can either remain in such a state or suffer a symptomatic relapse, defined as worsening of symptoms requiring clinical care; Reference Emsley, Chiliza, Asmal and Harvey25 a proportion of these patients will require inpatient care to achieve symptom stability. Additionally, we added a health state to include patients with persistent negative symptoms; these have been recognised as an independent source of disability despite control of positive symptoms. Reference Galderisi, Mucci, Dollfus, Nordentoft, Falkai and Kaiser26 Finally, according to the model, people can die from every health state with a probability equal to their age-specific mortality rate (derived from Chilean life tables) multiplied by the hazard ratio associated with each health state.
As in any model, we excluded health states described in the natural history of the disease but deemed less relevant to the decision setting. For instance, the utility of services for people at clinical risk of psychosis remains controversial Reference Guloksuz and van Os27 and incipient only in Chile. A detailed list of assumptions and simplifications can be found in the Supplementary material.
Model parameters and data sources
The parameters used to populate the model were estimated from a Chilean cohort of FEP patients, published literature, local cost data and expert opinion.
The transition probabilities in the baseline natural history model (CMHT arm) were obtained by conducting a rapid review for each health state. Rapid reviews are structured evidence syntheses that intentionally abbreviate certain steps (e.g. narrower searches, single screening, prioritised study designs) while retaining prespecified methods and transparent reporting, consistent with Cochrane Rapid Reviews Methods Group guidance. Reference Garritty, Hamel, Trivella, Gartlehner, Nussbaumer-Streit and Devane28 When selecting a study to feed the model we followed published recommendations, favouring systematic reviews, then primary observational studies and then the control arm of randomised trials. Reference Dias, Welton, Sutton and Ades29 When no evidence for a certain parameter could be found, we elicited it from experts through a Delphi panel, as detailed in the supplementary materials.
The transition probabilities in the intervention arm were estimated from a cohort study taking place in the EIP service at the Psychiatric Institute Dr Jose Horwitz Barak in Santiago, Chile. Patients who agreed to participate were interviewed by research assistants certified in the standardised assessment of psychosis. Data collection took place between 2017 and 2019, and included assessments at baseline and 3-month follow-up. The data items included sociodemographic characteristics, anthropometric measures, ICD diagnosis, medications, substance abuse, PANSS scores, Hamilton Rating Scale for Depression, Young Mania Rating Scale and a cognitive evaluation using the MATRICS consensus battery. Reference August, Kiwanuka, McMahon and Gold30
Because of the observational nature of the sample, we pooled individual patient data with those from previously published meta-analyses using a Bayesian synthesis approach known as power prior. Reference Ibrahim, Chen, Gwon and Chen31 This method has been used when combining different sources of evidence to account for the higher risk of bias of observational evidence, while preserving its information relevant to the decision setting. Reference Ibrahim, Chen, Gwon and Chen31 We applied this method in a random-effects binomial model to account for the nested nature of the data. We assumed exchangeability of the studies, and the results were embedded in the Markov model using the log risk ratio scale. Details of the Bayesian analysis can be found in the Supplementary material.
In order to calculate the benefits associated with the interventions, each health state is associated with a specific health-related quality of life utility value (HSUV). HSUVs were extracted after conducting a systematic review. Reference Aceituno, Pennington, Iruretagoyena, Prina and McCrone32 The total number of QALYs gained by each strategy was obtained by multiplying non-dead health states by their respective HSUVs at each cycle and then summing these across the entire time horizon. The discount rate was applied to cycle length following previously suggested adjustment. Reference Drummond, Sculpher, Claxton, Stoddart and Torrance9
Finally, the cost parameters associated with each health state were estimated by multiplying local unit costs by their resource use. Chilean unit costs are published every 2 years by the Ministry of Health, and include all interventions and actions related to health problems included in the GES plan. 33 This includes hospitalisation costs, visits to emergency departments and appointments with professionals at different levels of care. Medication costs were obtained from the national supply centre for drugs (CENABAST). Given the absence of patient-level data in terms of resource use, identification and measurement of resource items was derived from published systematic reviews Reference Randall, Vokey, Loewen, Martens, Brownell and Katz34 and validated by local stakeholders (see Supplementary material). All costs are reported in 2018 Chilean currency (CLP). To facilitate international comparisons, we converted CLP to US dollars and UK pound sterling (GBP), adjusted for purchasing power parity (PPP) conversion rates provided by the Organisation for Economic Co-operation and Development.
A list of the model’s parameters, including point estimates, probability distributions and sources, is provided in the Supplementary material.
Sensitivity analysis
We conducted a series of deterministic and probabilistic sensitivity analyses (PSA) to assess the robustness of the model results. In PSA we ran the model for 5000 iterations using Monte Carlo simulation to account for uncertainty in the parameters.
Additionally, we conducted value of information (VOI) analysis to assess the potential value of additional research. Reference Fenwick, Steuten, Knies, Ghabri, Basu and Murray35 Briefly, given the uncertainty associated with the input parameters, there is always a possibility that the decision made with the current information is suboptimal. In theory, this uncertainty can be reduced by gathering more information. However, this process is also costly and uncertain. To deal with this situation, VOI analysis provides a formal assessment of the value of additional research, based on the extent to which the decision is improved by reducing uncertainty compared with the cost of new research. Following current methodological recommendations, Reference Fenwick, Steuten, Knies, Ghabri, Basu and Murray35 we calculated the expected value of perfect information (EVPI) for the population affected by the intervention using a recent estimation of the incidence of FEP in Chile. Reference González-Valderrama, Jongsma, Mena, Castañeda, Nachar and Undurraga11 Additionally, we calculated partial EVPI to assess which parameters were more influential on the decision.
Model implementation
The model was fully implemented in the programming language R, version 4.2.1 (2022) for MacOS (R Foundation for Statistical Computing, Vienna, Austria; https://cran.r-project.org/bin/macosx/), following coding good-practice recommendations. Reference Alarid-Escudero, Krijkamp, Pechlivanoglou, Jalal, Kao and Yang36 Bayesian analysis was implemented using the software Just Another Gibbs Sampling. We applied white- and black-box tests to verify and validate the internal results of the model. Reference Caro, Briggs, Siebert and Kuntz17 Face validity was provided by local stakeholders. Details of the verification tests are reported in the Supplementary material, and detailed code is available at https://github.com/david-aceituno.
Ethical standards
The primary study used to populate this model was conducted according to international ethical regulations, and was approved by the ethics committee of Pontificia Universidad Católica de Chile (approval no. 190603005). All adult participants (aged >18 years) signed an informed consent. For younger participants, patient and legal tutors’ consent was required.
Results
Study parameters
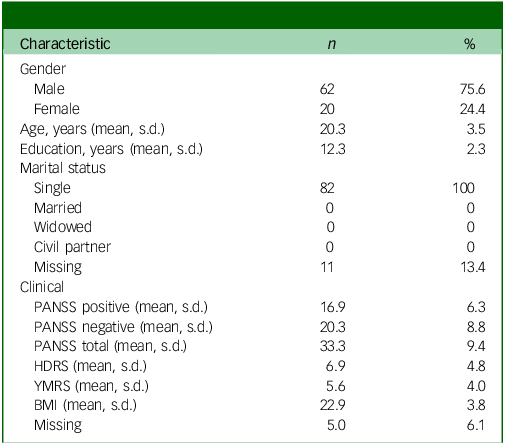
Individual-level data from the Chilean cohort study comprised 82 patients with FEP; most (78.5%) were male, with a mean (s.d.) age of 20.2 (3.49) years and 12.3 years of education. At baseline, the mean (s.d.) PANSS score was 33.26 (9.35) and the depression mean (s.d.) score measured by the Hamilton Rating Scale for Depression was 6.86 (4.76). Characteristics of the study participants can be found in Table 1.
Baseline characteristics of participants

PANSS, Positive and Negative Symptoms Scale; HDRS, Hamilton Depression Rating Scale; YMRS, Young Mania Rating Scale; BMI, body mass index.
The aggregate data included 7 studies with 2087 participants. Six studies evaluated the effectiveness of EIP services in achieving remission, and six assessed relapse prevention (five studies reported both outcomes). The effect of including cohort data is presented in Fig. 2. The results of the Bayesian model showed that people receiving EIP had a pooled risk ratio of 1.25 (95% credible interval (CrI): 1.05–1.58) of achieving remission when the observational evidence was fully incorporated. When the observational evidence was downweighted by 50%, the risk ratio changed slightly to 1.27 (95% CrI: 1.02–1.58); meanwhile, risk ratio was 1.33 (95% CrI: 0.93–2.06) when the observational data were discarded (power prior of 0). When the outcome assessed was relapse, the pooled risk ratio in the EIP group was 0.51 (95% CrI: 0.25–0.79) when the observational evidence was considered an additional trial. The risk ratio increased to 0.57 (95% CrI 0.28–0.88) when the individual-participant data were downweighted by 50%, and to 0.70 (95% CrI 0.36–1.13) when this type of evidence was excluded. Full details of the Bayesian synthesis, including model convergence diagnostics and forest plots, can be found in the Supplementary material.
Pooled risk ratios (RRs) at different levels of inclusion of observational evidence. Forest plots showing the effect of incorporating observational evidence within a meta-analysis of aggregate data. The y axis shows increasing weighting of the observational evidence from bottom to top, because the weighting factor is exponential. The x axis represents the estimated effect size (remission at left and relapse at right) in the RR scale. The blue point-and-range lines represent pooled effect sizes at different weightings of the observational evidence.

Base case analysis
The results of the base case analysis are shown in Table 2. According to this analysis, the implementation of EIP services resulted in a mean incremental cost of CLP 1 327 054 and a mean incremental benefit of 0.24 QALYs. The resulting ICER of CLP 5 550 044 (USD 13 742 or £9465 adjusted for PPP) per QALY was considered cost-effective at 1 GDP per capita of willingness-to-pay (WTP) (USD 15 923 or £10 968 PPP adjusted).
Results of base case analysis comparing early intervention for psychosis services against community mental health teams

CLP, Chilean peso; QALYs, quality-adjusted life-years; ICER, incremental cost-effectiveness ratio; CMHT, community mental health teams; EIP, Early Intervention for Psychosis; NA, not applicable.
Sensitivity analysis
The results of the 5000 simulations in PSA are plotted on the cost-effectiveness plane in Fig. 3. PSA showed that most (82.5%) of the simulation lay in the north-east quadrant followed by 9.6% in the south-east quadrant, where EIP dominates; 7.3% of the simulation lay in the north-west quadrant, where CMHT dominate.
Cost-effectiveness plan showing PSA simulations. The x axis represents the difference between EIP services and CMHT in terms of QALYs; the y axis represents the difference between EIP services and CMHT in terms of costs (CLP). PSA, probabilistic sensitivity analysis; EIP, Early Intervention in Psychosis; CMHT, community mental health teams; QALYs, quality-adjusted life-years; CLP, Chilean peso; ICER, incremental cost-effectiveness ratio.

Deterministic sensitivity analyses revealed that the model was sensitive to the following parameters: HSUVs of remission, HSUVs of resistance, probability of remission following an acute episode and probability of relapse given remission. However, EIP remained as the most cost-effective alternative compared with CMHT. Full details of the sensitivity analysis are presented in the Supplementary material.
Using the net benefit approach, EIP was associated with the highest expected net benefit at all WTP thresholds. In the base case analysis, at 1 GDP per capita (15 923 USD) of WTP, EIP had a probability of 0.85 of being the alternative with the highest expected net benefit. When the price that society is willing to pay for one increment in QALYs in people with FEP was halved, the probability of EIP being the most cost-effective alternative was 0.80. The cost-effectiveness acceptability curve shows the probability of EIP being cost-effective compared with CMHT at different thresholds of WTP (Fig. 4).
Cost-effectiveness acceptability curve showing the probability of EIP being cost-effective at different thresholds of WTP. The x axis shows WTP in Chilean peso (CLP), with the y axis representing the probability of cost-effectiveness. EIP, Early Intervention in Psychosis; WTP, willingness to pay; GDPpc, gross domestic product per capita.

VOI
The VOI analysis revealed that, in the base case analysis, the uncertainty surrounding cost-effectiveness translates into CLP 805 857 (£1374) of decision uncertainty. When the total population affected by the decision is taken into account (which included the annual incidence of FEP over a 10-year time horizon), the population EVPI reached CLP 26.1 billion (£44 532 358), indicating that further research might be valuable if costs are less than such an amount. Additionally, partial EVPI suggested that the effectiveness estimates and utility values of people in remission have the highest influence on this estimate. Furthermore, the expected value of partial perfect information analysis suggested that the parameters causing most of the decision uncertainty were the effectiveness of the intervention in reducing relapses, the costs of managing those relapses, the effectiveness of the intervention promoting remission and the costs associated with remission state. Further details of VOI analyses can be found in the Supplementary material.
Discussion
In this work we have evaluated the potential costs and benefits of implementing specialist services for people with FEP in the Chilean healthcare system. The results of this modelling exercise suggest that EIP services are a more efficient use of resources compared with standard care. Applying the commonly used WHO threshold of 1–3 GDP per capita (15 923–47 769 USD), EIP services had a chance of >80% of being more cost-effective than CMHT, according to the incremental analyses and net benefit approach.
Comparison with published literature
Comparisons between economic evaluations from different jurisdictions can be problematic due to differences in health system organisation, economic perspectives and study designs. Despite these differences, the results of our model are in alignment with published evidence of the cost-effectiveness of EIP. Reference Aceituno, Vera, Prina and McCrone3,Reference Shields, Buck, Varese, Yung, Thompson and Husain37 Several trial- and model-based economic evaluations have shown that implementation of EIP services is cost-effective.
However, as we previously highlighted, most of the evidence comes from HICs, with pioneering work in Australia and further evidence from Europe, North America and Asia. Reference Aceituno, Vera, Prina and McCrone3 Given that resources are even more limited in LMICs, having good cost-effectiveness estimates is crucial. However, producing local evidence in LMICs is difficult because of low investment in research, scarcity of reliable data and the cost of research itself. Reference Saxena, Thornicroft, Knapp and Whiteford8 In these situations, decision models can be used to support rational decision-making by simulating the potential benefits of alternative interventions. Reference Caro, Briggs, Siebert and Kuntz17 Furthermore, models allow quantification of the uncertainty of the decision and measure the value of additional research. In mental health, several recommendations have been made on the basis of modelling exercises (e.g. WHO-CHOICE research). Reference Hutubessy, Chisholm and Edejer38 Our group recently presented a model-based economic evaluation of EIP services in Brazil, with results similar to those for the Chilean case presented here.
Strengths and limitations
This study has both strengths and limitations. First, our model development followed a systematic and iterative approach to include the best published evidence, combined with Chilean data and opinions from local experts. We also conducted a wide range of sensitivity analyses, propagated uncertainty throughout the model, tested several scenarios and estimated the value of conducting further research. Second, we were able to use local cost data, which are updated regularly based on the schizophrenia GES benefit plan. Third, using a Bayesian approach allowed the inclusion of local cohort data in a rational and transparent manner. Cohort data have the potential of improving the applicability of findings, whereas their higher risk of bias can be downweighted using the power prior approach.
However, several limitations need to be acknowledged. First, the cohort sample size was small and with a short period of follow-up. This might partially explain the small impact of the observational data on the overall evidence. Second, the sample did not include a measure of DUP. It is, therefore, unclear whether such a variable might have changed the effectiveness of EIP services in Latin America, as suggested elsewhere. Reference Rosenheck, Leslie, Sint, Lin, Robinson and Schooler39 Third, our model was limited to participants with non-affective psychosis. In practice, people with bipolar disorder and/or depression with psychotic features might present to EIP services, but in the Chilean context they are covered by a separate GES package of care.
Fourth, although unit costs were available for most of the interventions included in EIP services, no patient-level data about service use could be found. As a result, we relied on administrative data and external literature to estimate service use. Despite using nationally validated unit costs, the measurement of service use in Chile is an area that requires further research.
Fifth, given the characteristics of the Chilean health system, it was not possible to measure private sector charges and therefore these results can be applied only to the public health sector. Although the public sector represents the majority of the healthcare system, at least 15% of the Chilean population have the private sector as their main provider of care, where price data are inaccessible to researchers and civil society.
Sixth, the model development includes only expert knowledge from clinicians and researchers. We did not include the inputs of experts by experience and/or their caregivers, which might have had relevant implications by changing the health states that matter most to those affected by psychosis.
Finally, restricting the perspective to the healthcare system has the limitation of underestimating the benefits of interventions with consequences outside the health system. This is especially relevant in mental health, where productivity loss, social care expenses and costs to caregivers are particularly relevant. Reference Aceituno, Vera, Prina and McCrone3
Policy implications and further research
The results of this cost-effectiveness analysis suggest that EIP services are cost-effective compared with CMHT. At the health policy level, these results have direct implications for the Chilean GES plan. For instance, the package of care currently provided by the GES plan would need to be expanded to closely align with those provided by EIP teams. Furthermore, our results suggest that treatments for people with FEP might be better implemented as a stand-alone service rather than within CMHT. Nevertheless, such implementation would require further examination of potential unintended consequences, such as the effect of including specialist services in the remainder of the mental health network, potential understaffing of CMHT and diversion of resources. A careful implementation is crucial to preserve the economic benefits of this intervention. Reference Csillag, Nordentoft, Mizuno, Jones, Killackey and Taylor1,Reference Shields, Buck, Varese, Yung, Thompson and Husain37
Additionally, the VOI analysis suggested that there is potential value in reducing uncertainty by collecting more data, particularly for certain parameters such as those related to the effectiveness of EIP programmes and the costs of remission. In addition to reducing this uncertainty regarding parameters, there is value in conducting further research prior to a wider implementation, despite evidence of cost-effectiveness. A recognised problem when moving from research to policy decisions is affordability. Reference Saxena, Thornicroft, Knapp and Whiteford8 Many LMICs face the problem of having good evidence of cost-effectiveness but with no budgets to set up new programmes or interventions. In such cases, a budget impact analysis would be useful to add information on the costs of implementation.
Similarly, no information about the impact of EIP services on health inequalities has been produced. There is consistent evidence of huge health disparities among people with mental health problems, especially psychosis. Reference Mangalore, Knapp and Jenkins40 However, to date no published study has examined the potential impact of implementing EIP services on such disparities.
Overall, our results suggest that implementing EIP services in Chile could be cost-effective, although further research incorporating patients’ point of view, measures of health inequalities and a societal perspective is warranted to ensure a sustainable scaling-up.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.11033
Data availability
The authors declare that all data supporting the findings of this study are available within the article, its supplementary information file and the GitHub repository.
Acknowledgements
We thank collaborators of the Red Andes for their inputs in model development and data availability. ANDES is a collaborative network focused on early psychosis in Latin America, supported by Programa Iberoamericano de Ciencia y Tecnología para el Desarrollo CYTED (no. 218RT0547).
Author contributions
D.A. participated in conception, analysis, interpretation of data, drafting and final approval. P.M., M.P., H.J. and M.W.P. participated in interpretation of data, drafting, revising and final approval. A.G.-V., C.B., E.A.U. and N.A.C. participated in drafting, revising and final approval.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. D.A. was fully funded by a National Commission for Scientific and Technological Research doctoral scholarship, which had no role in the conception or development of this project.
Declaration of interest
N.A.C. has received personal fees from Janssen outside of the submitted work. M.W.P. has received personal fees from Merck outside of the submitted work. The remaining co-authors declare no competing interests.







 Open access
Open access
eLetters
No eLetters have been published for this article.