


The global population aged 60 years and over is projected to reach 2 billion by 2050 which will be around 22 % of the people in the world(1). Brain ageing is associated with a decline in several cognitive functions, including memory, attention, speed of processing and executive function(Reference Harada, Natelson Love and Triebel2), changes that may result in mild incapacity even prior to the onset of dementia(Reference Phillips3). The speed of processing is an important domain of cognitive function and can be assessed by reaction time. Researchers have proposed that the speed of processing might be a fundamental component of individual differences in relation to cognitive ageing(Reference Deary, Johnson and Starr4). Some studies have suggested that diet, a modifiable lifestyle factor, may play a key role in cognitive ageing(Reference van de Rest, Berendsen and Haveman-Nies5); however, current evidence about associations of foods as well as their cooking methods, nutrient intakes and dietary patterns with processing speed is limited.
Nutrients may influence the loss of cognitive function with ageing(Reference Poulose, Miller and Scott6). Neuroprotective effects of PUFA and several vitamins, especially antioxidant vitamins (including vitamin E), are supported by cell and animal experiments in vitro and in vivo, observational studies and randomised control trials(Reference de Jager, Oulhaj and Jacoby7–Reference Masana, Koyanagi and Haro9). However, several clinical trials do not support the positive effects across all cognitive function measures(Reference Dangour, Allen and Elbourne10–Reference van de Rest, Geleijnse and Kok12). A systematic review and meta-analysis of supplementation trials with n-3 PUFA from infancy to old age showed that beneficial effects on cognition might happen only in infants but not in children, adults or the elderly(Reference Jiao, Li and Chu13), indicating that effects of nutrients on cognitive function may vary by age groups.
Cooking methods play an important role in dietary intake by modifying taste, palatability and nutrient composition of foods during the cooking process. For example, frying can reduce unsaturated fatty acids and antioxidant vitamins due to oxidation, but has little impact on protein and mineral content, whereas dietary fibre of potatoes can be increased by frying because of the formation of resistant starch(Reference Fillion and Henry14). Cooking can also influence fat content and fatty acid composition in meat. Gerber et al. showed considerable fat loss in several meat cuts cooked by grilling, broiling or pan-frying without fat being added, which affected the PUFA:SFA ratio(Reference Pereira and Vicente15). In addition, some hazardous compounds can be produced as a by-product during the cooking process. When high-protein containing food such as meat and fish is heated to high temperatures, polycyclic aromatic hydrocarbons can be produced, particularly benzo[a]pyrene(Reference Janoszka, Warzecha and Blaszczyk16). A cross-sectional study showed a 1 % increase of urinary 1-hydroxypyrene (a biomarker of polycyclic aromatic hydrocarbons) resulted in about 2 % poorer performance on cognitive function in individuals aged 60 years and older(Reference Best, Juarez-Colunga and James17). With regard to carbohydrate-rich food heated to high temperatures, acrylamide can be produced, a known neurotoxin and carcinogen(Reference Skog and Alexander18). Currently, evidence regarding effects of acrylamide on cognitive function is limited, but a study among non-smoking elderly Chinese men found that dietary acrylamide exposure was associated with mild cognitive decline(Reference Liu, Tse and Chen19). Both loss of nutrients and production of hazardous compounds can vary by cooking method, and at present, very little information exists regarding the possible influence of cooking methods on cognitive function.
In relation to dietary patterns, accumulating studies suggest that higher adherence to the Mediterranean diet (MeDi) may be associated with better cognitive performance(Reference Féart, Samieri and Rondeau20,Reference Calil, Brucki and Nitrini21) . Nevertheless, a recent systematic review suggested that there was a high level of heterogeneity among thirty-two articles studying associations between adherence to the MeDi, cognitive function and dementia, with almost half reporting that the MeDi was not associated with cognitive function or dementia(Reference Petersson and Philippou22), indicating that the protective effect of the MeDi on cognitive function remains inconsistent.
This longitudinal observational study aimed to investigate associations between midlife dietary factors, specifically foods, nutrients and MeDi pattern, with reaction time ability 10–15 years later. Potential associations between cooking methods and reaction time ability were also explored. In the present study, consumption of unsaturated fatty acids and fish, vitamins and vegetables, as well as adherence to the MeDi was hypothesised to be positively associated with reaction time ability, whereas consumption of SFA and meat was assumed to be negatively linked to reaction time ability.
Methods
Study design and participants
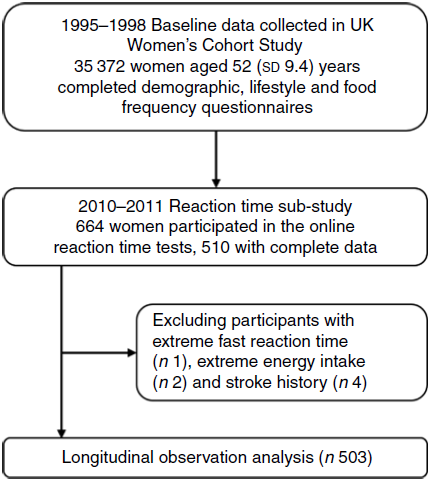
The UK Women’s Cohort Study(Reference Cade, Burley and Alwan23) was initiated in 1995 to explore potential associations between diet and chronic disease and recruited 35 372 women aged 52 (sd 9·4) years (1995–1998). At recruitment, the baseline survey collected FFQ, lifestyle as well as demographic and anthropometric information.
Sample size to investigate the impact of diet on reaction ability in the UK Women’s Cohort Study was estimated using the mean choice reaction time (CRT). A sample size of 530 women was computed from the estimation of the mean CRT using comparison of one mean to a reference value with the two-sided significance level of 0·05, marginal error of 15 ms and power of 0·8. This estimation was calculated using a reference mean CRT of 628 (sd 123) ms from a British study in which simple reaction time (SRT) and CRT were tested using the Deary–Liewald reaction time task for residents aged between 61 and 80 years in the City of Edinburgh(Reference Deary, Liewald and Nissan24). There were no previous studies of diet and reaction time on which to base a sample size calculation.
In 2010/2011, a subset of 664 women was involved in our pre-designed online reaction time tests. Among them, 510 women had complete dietary records and cognitive testing results. Exclusion criteria were applied among individuals with unlikely fast reaction times (SRT < 200 ms; CRT < 250 ms) prior to analyses as these were likely to represent accidental screen presses which were adapted from previous studies(Reference Bunce, Haynes and Lord25). We excluded participants if their reported energy intake was outside 1 % of the population distribution (<2 MJ/d (<500 kcal/d) and >25 MJ/d (>6000 kcal/d)) following previous studies(Reference Merchant, Vatanparast and Barlas26). We also excluded participants with stroke history because stroke could significantly impair cognitive function including the reaction time ability(Reference Kal, Winters and van der Kamp27).
Ethical approval was granted from National Research Ethics Service Committee for Yorkshire & the Humber – Leeds East (reference 15/YH/0027) at the cohort’s initiation in 1993, now covered by Health Research Authority REC reference: 17/YH/0144.
Reaction ability tests
The web-based cognitive measurement tasks (www.uk-wcs.co.uk) test participants’ reaction ability including SRT and CRT described previously(Reference Deary, Liewald and Nissan24,Reference Reimers and Stewart28) . The SRT task required participants to respond to a letter ‘Y’ appearing on a screen by pressing the ‘Y’ key on the keyboard as soon as it appeared for twenty trials. The CRT task required participants to respond to one of four numbers (5, 6, 7 or 8) appearing randomly on a screen by pressing the corresponding number on the keyboard as soon as it appeared for forty trials. The mean values of reaction times were analysed as the outcome to reflect participants’ cognitive ability. Each reaction time was grouped into two categories according to their median values, where the slow group was defined as less than the median and the fast group equal to or above the median. The median was used here to reduce the impact of outliers and skewed data.
Dietary measurement
Dietary information at baseline was obtained from self-administered FFQ with 217 British food items, which was based on the FFQ used in the UK for the European Prospective Investigation into Cancer and Nutrition study(Reference Riboli and Kaaks29). The baseline FFQ was compared against 4-d weighed food diaries and a second FFQ collected at the same time as the diary, on 283 women 3 years after baseline. Whilst accepting that each tool type is measuring different aspects of diet, correlations between the two dietary assessment methods were comparable to those found in other studies; for example, the correlation coefficients between the FFQ and the 4-d weighed food diaries were 0·39 for carbohydrate, 0·35 for fat, 0·43 for Ca and 0·62 for vitamin C(Reference Cade, Burley and Greenwood30,Reference Spence, Cade and Burley31) . Classification of food groups and derivation of nutrient intakes were detailed in previous studies(Reference Jones, Cade and Evans32,Reference Rada-Fernandez de Jauregui, Evans and Jones33) . Nutrients provided by supplements were not included in the nutritional analysis. The cooking methods of several common foods, including meat, fish, vegetables and potatoes, have been investigated by asking ‘How often do you eat foods cooked by the following methods?’ The specific cooking methods included roasting/baking, frying and barbecuing/grilling, and the consumption frequencies ranged from never to more than once a day containing eight categories. Participants with the frequencies of never and less than once a month were treated as non-consumers of specific cooked food item, while others with the frequencies of once a month or more were considered as consumers of that food item. The consumption frequency of each cooking method was treated as a dichotomous variable: non-consumers and consumers. This was included in the regression models with non-consumers as the reference group.
To quantify adherence to the MeDi, a variable of MeDi score was created based on the 217-item FFQ. The MeDi score was derived from a modified ten-point version of the MeDi(Reference Trichopoulou, Kouris-Blazos and Wahlqvist34,Reference Trichopoulou, Orfanos and Norat35) covering ten food/nutrient components consumed in g/d. Of the ten components, six traditionally consumed in the MeDi (vegetables, legumes, fruits and nuts, cereals, fish and fatty acid ratio of MUFA plus PUFA to SFA, namely, MUFA + PUFA: SFA) considered beneficial were assigned 1 if consumed at or above the median. Another three foods (meat, poultry and dairy products) considered detrimental were given a score of 1 for consumption below the median. For alcohol, a score of 1 was given to women who had intakes of between 5 and 25 g/d. Details are given in online Supplementary Table S1. Thus, the total MeDi score ranges from a minimal adherence score of 0 to a maximal adherence score of 10, with higher scores indicating greater dietary adherence. Further the total MeDi score was divided into three groups: scores 0–3 (low adherence), 4–6 (moderate adherence) and 7–10 (high adherence).
Covariate assessment
Baseline socio-demographic information, such as age, ethnicity, educational level, marital status, was undertaken by self-report. BMI was calculated from self-reported height and weight by formula of ‘weight/height2 (kg/m2)’. Sleep duration (h/d) was the weighted mean value calculated from self-reported sleep durations of weekdays and weekends. Socio-economic status was derived from the UK National Statistics-Socio-Economic Classification, where participants are classified into three categories (routine/manual, intermediate or managerial/professional)(36). Due to overlapping properties among socioeconomic indicators (education, social class, income or employment)(Reference Darin-Mattsson, Fors and Kareholt37), only socio-economic status was used as the adjustment factor in the present study. Physical activity was assessed as self-reported time spent on activities vigorous enough to cause sweating or a faster heartbeat (h/d).
A directed acyclic graph was constructed using the online DAGitty tool (http://www.dagitty.net) to determine the minimally sufficient set of confounding adjustments for the exposure–outcome relationship(Reference VanderWeele, Hernan and Robins38). Potential confounding variables including age, ethnicity (white, Asian, African and others), socio-economic status, BMI, physical activity, sleep duration, smoking status (current, former and non-smoker), alcohol consumption (g/d) and marital status (married or living as married, separated or divorced, single or widowed) were considered in the directed acyclic graph. Actual or likely relationships between variables were based on a priori knowledge from the literature, and the minimally sufficient adjustment set was age, ethnicity, marital status, physical activity, socio-economic status, sleep duration, BMI, smoking status and alcohol consumption (online Supplementary Fig. S1).
Statistical analysis
Characteristics such as demographics and dietary consumption were summarised. For continuous variables, means and standard deviations are displayed with Student’s t test for difference, while categorical variable characteristics are presented as percentages with the χ 2 test for difference. Nutrient intakes were adjusted for total energy using the nutrient density method(Reference Willett39) (for protein, carbohydrates and fat, the percentage of total energy derived from each one; for other nutrients, the ratio of selected nutrient intake to per 1000 kcal (4186 kJ) of total energy intake). Each energy-adjusted intake of foods and nutrients was entered in a multiple logistic regression model with total energy intake as a covariate using the multivariate nutrient density method recommended by Willett(Reference Willett39). Due to skewed distributions, the two reaction time variables were dichotomously categorised taking the median values as cut points; the fast groups (reaction time less than the median) were treated as the reference group, while the slow groups (reaction time equal to or above the median) were treated as the case group. Logistic regression models were conducted to identify potential associations between dietary intake, cooking methods and reaction ability. All analyses were conducted using Stata version 16.1 (StataCorp LLC). Values of P < 0·05 were considered to be statistically significant.
Results
Of 510 women with complete records, one participant with an unlikely fast CRT (64 ms), two individuals with extremely high energy intake (26 MJ/d (6293 kcal/d), and 33 MJ/d (7780 kcal/d)) and four participants with self-reported stroke history were excluded. Therefore, 503 women were considered eligible for analysis (Fig. 1).
Flow chart of reaction time study data collection and exclusion criteria.
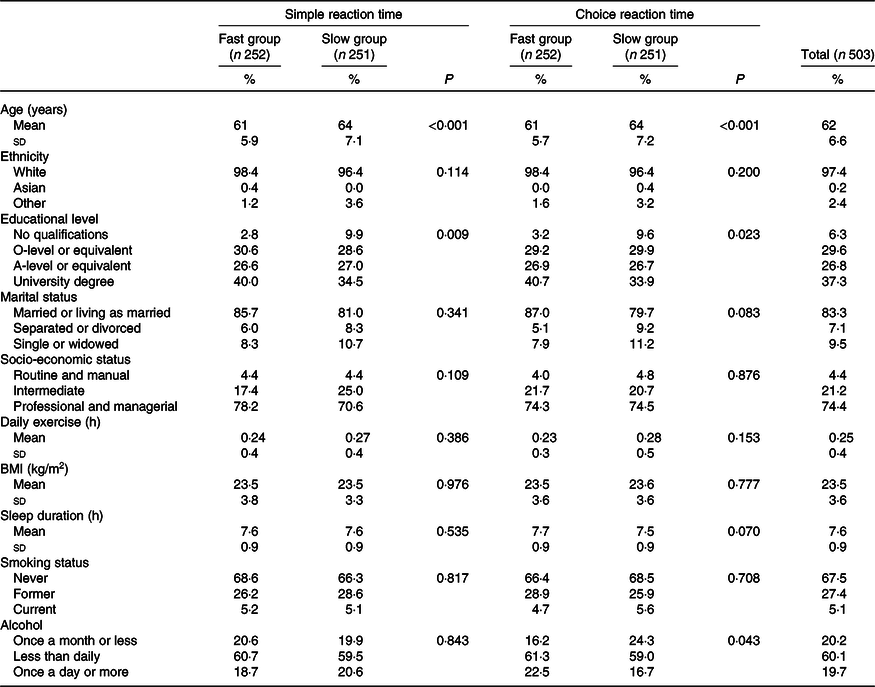
The characteristics of women who participated in the reaction time sub-study are summarised in Table 1. Participants who took part in reaction time tests had a mean age of 62 (sd 6·6) years. SRT and CRT were categorised into the ‘fast group’ and the ‘slow group’. Women in slow groups were significantly older and had lower educational levels than women in fast groups (64 v. 61 years old for both SRT and CRT; 35 v. 40 % university degree for SRT; 34 v. 41 % university degree for CRT). Among the women, 97 % were white, 83 % were married or living as married, 74 % had a higher level of social economic status (professional or managerial) and 67 % were non-smokers. The participants had a mean BMI of 23·5 kg/m2, a mean sleep duration of 7·6 h/d and 0·25 h/d of vigorous activities. With regard to alcohol consumption, 60 % of the women drank less than once a day but more than once a month, while 20 % consumed alcohol once a day or more and for the remaining 20 % consumption was once a month or less.
Demographic characteristics of participants between fast groups and slow groups for simple and choice reaction times
(Mean values and standard deviations; percentages)
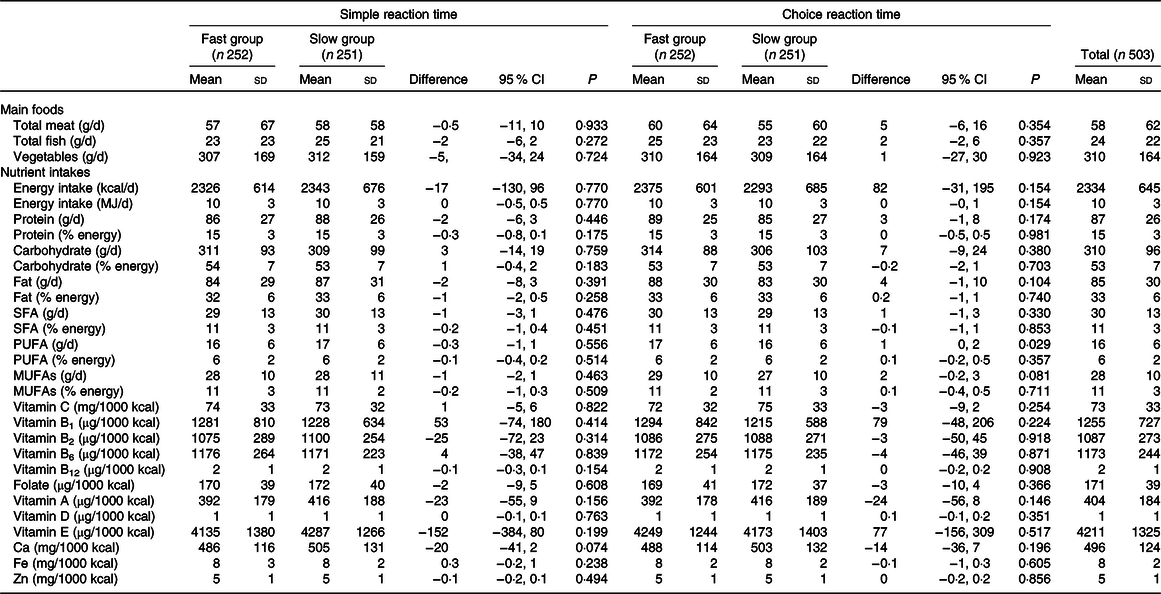
There was no significant difference in daily consumption of energy-adjusted total meat, total fish, vegetables and total energy intake, as well as energy-adjusted nutrients intake between fast groups and slow groups for both SRT and CRT (Table 2). In addition, multivariate logistic regressions showed that associations between these dietary exposures and reaction times were not statistically significant (Table 3).
Profiles of main foods and nutrient intakes comparing women with fast and slow reaction times
(Mean values and standard deviations; differences and 95 % confidence intervals)
Associations of main foods and energy-adjusted nutrient intakes with reaction times
(Odds ratios and 95 % confidence intervals)
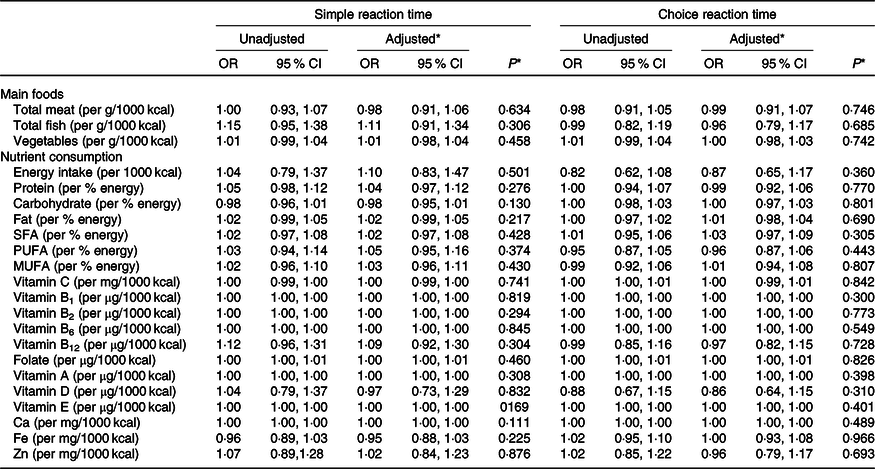
* Adjusted for age, ethnicity, marital status, socio-economic status, physical activity, BMI, sleep duration, smoking status, alcohol consumption and total energy intake.
As shown in Table 4, consumers of roasted/baked fish were 46 % more likely to be in the slow SRT group (adjusted OR 1·46, 95 % CI 1·00, 2·13). Consumers of fried vegetables were 64 % more likely to be in the slow SRT group (adjusted OR 1·64, 95 % CI 1·12, 2·39) with adjustment for confounding factors. However, the consumption of fish or vegetables cooked by any of these three methods did not change the risk of being in slow CRT groups. In addition, neither meat nor potato consumption cooked by any of these three methods changed the likelihood of being in slow groups for both SRT and CRT.
Comparison of reaction times between consumers and non-consumers of specific foods cooked by roasting/baking, frying and barbecuing/grilling
(Odds ratios and 95 % confidence intervals)
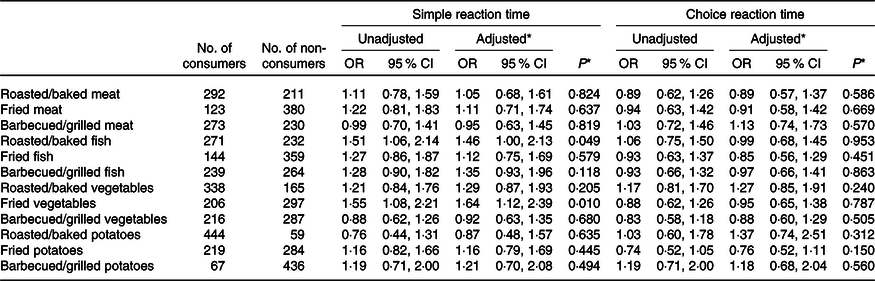
* Adjusted for age, ethnicity, marital status, socio-economic status, physical activity, BMI, sleep duration, smoking status, alcohol consumption and total energy intake.
Adherence to MeDi and its association with reaction ability is summarised in Table 5. Most women included in this analysis had moderate adherence to the MeDi (53 %), and the percentages of adherence among fast groups and slow groups for SRT and CRT were similar. Logistic regression results showed that SRT or CRT was not associated with adherence to the MeDi both in unadjusted and adjusted models.
Adherence to the Mediterranean diet and its associations with reaction times
(Numbers and percentages; odds ratios and 95 % confidence intervals)
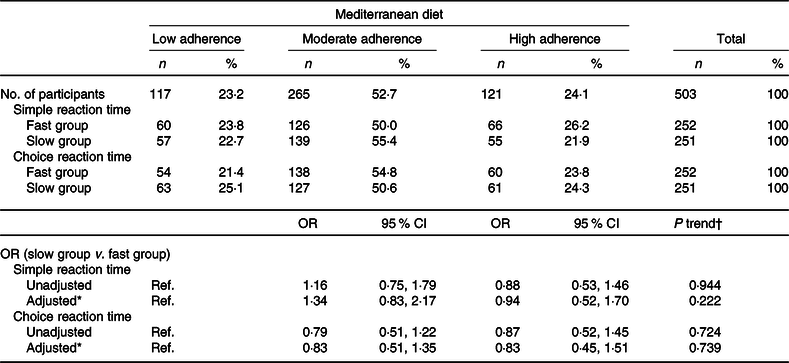
Ref., reference.
* Adjusted age, ethnicity, marital status, socio-economic status, physical activity, BMI, sleep duration, smoking status, alcohol consumption and total energy intake.
† Tests for linear trend of adherence to the Mediterranean diet in relation to reaction times.
Discussion
The prevalence of dementia in the general population aged 60 years and over is 5–8 %, and this figure is expected to rise in coming decades(40). There is an emerging awareness that women may disproportionately bear the burden of dementia almost globally compared with men(Reference Bamford and Walker41). Age is a strong risk factor for dementia and cognitive decline, and the average life expectancy worldwide is greater for women than men which makes dementia an important concern for women(42). There are also sex-specific biological mechanisms that could possibly result in increased susceptibility of women to Alzheimer’s dementia(Reference Mayeda43). The present longitudinal observational analysis was conducted in a female-only cohort study, allowing exploration of dietary exposures and subsequent reaction ability in women for the first time.
Our results showed that consumption of meat, fish, vegetables and nutrient intakes in middle-aged women were not associated with reaction ability 10–15 years later. Compared with low adherence to the MeDi, moderate and high adherence did not influence the risk of being in the slow reaction time groups. A similar longitudinal observational analysis, however, suggested that adherence to the MeDi assessed 22 years previously was positively associated with cognitive function in the Health Professionals Follow-up Study, a prospective cohort study initiated in 1986 among 51 529 US men aged 40–75 years(Reference Bhushan, Fondell and Ascherio44). Although some evidence shows that there is a protective effect of the MeDi against cognitive decline, most studies focus on memory and attention which tends to be assessed by the mini-mental state examination(Reference Loughrey, Lavecchia and Brennan45,Reference Martinez-Lapiscina, Clavero and Toledo46) . Few studies have been done on the associations between the MeDi and reaction time ability. A cross-sectional study involving ninety-three participants in Australia showed that the MeDi score did not differ significantly between the faster reaction time group and the slower reaction time group(Reference Hardman, Meyer and Kennedy47), consistent with our results.
Although in this study cooking methods of meat did not show effects on reaction times, the roasted/baked fish appeared to increase the risk of having a slow SRT with adjustment for confounding factors. However, since both non-consumers and consumers of roasted/baked fish were likely meddled with those who may also have selected different cooking methods for fish, confounding bias might have occurred with this association and some caution should be exercised when interpreting these significant results. Oily fish is high in unsaturated fatty acids which could be reduced during the long-lasting and high-temperature cooking process required for roasting/baking. Unsaturated fatty acids such as n-3 fatty acids are associated with better global cognition(Reference Masana, Koyanagi and Haro9). Therefore, oxidation of unsaturated fatty acids could be the potential reason that roasted/baked fish increased the risk of having a slow SRT. In addition, fried vegetables were also associated with a slower SRT. This could be due to acrylamide produced in carbohydrate-rich food during frying, another high-temperature cooking process(Reference Skog and Alexander18,Reference Liu, Tse and Chen19) . However, fried potatoes, a carbohydrate-rich food, did not show a similar negative association with reaction times. Potential mechanisms why only roasted/baked fish and fried vegetables had detrimental effects on SRT are unclear and similar studies are limited; more evidence needs be provided from other populations including cooking methods.
Strengths of this study include its novelty to explore effects of cooking methods on cognitive function, the longitudinal design and a fully adjusted regression model. The exploration of frequencies of cooking methods is novel in relation to health-related outcomes and has not been conducted in other studies to date. There is a possibility that these frequencies might be under- or over-reported. These potential measurement errors could reduce the power to detect real associations between dietary exposures and reaction ability; therefore, results should be interpreted with caution. Moreover, as an observational study, causality cannot be established, and potential confounding bias is always a possibility.
Our study is also limited that we did not include any assessment of nutritional supplement use resulting in underestimation of nutrient intakes; we have also not taken into account other diet quality indices apart from the MeDi in our analyses. It may be that combinations of nutrients and foods are more comprehensive than individual nutrients in relation to reaction times. In addition, most studies on the prevalence of dementia focus on people aged over 65 years; for those aged 45–64 years, the prevalence is relatively low at 98 per 100 000(Reference van der Flier and Scheltens48). The mean age of women who took part in the reaction time tests may be not old enough to show changes of reaction ability.
Overall, our study indicates no associations between reaction ability and consumption of total meat, fish, vegetables, energy-adjusted nutrient intakes and MeDi . However, there was a suggestion that foods cooked by specific methods may be related to reaction ability. This needs further exploration in additional studies.
Acknowledgements
The authors thank the participants of the UK Women’s Cohort Study for the provision of the data, the cohort team members who contributed to data collection, Mr Gareth Hagger-Johnson for carrying out reaction time tests and Mr Neil Hancock for his contributions to data management and technical assistance for the cohort.
H. Z. received funding from the China Council Scholarship (CSC ID: 201806010423). The UK Women’s Cohort was supported by funding from the World Cancer Research Fund (to J. C.). The funders of CSC and the World Cancer Research Fund had no role in the design, analysis or writing of this article.
The authors declare that this work had no commercial or not-for-profit sectors involved.
All authors were involved in the study conception and design. H. Z. contributed to the data analysis and wrote the manuscript. All authors interpreted the findings, and edited and approved the final manuscript.
The authors declare that there are no conflicts of interest.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114520002287








