Parenteral nutrition, a widely adopted nutritional therapy, is provided through intravenous administration of amino acids, glucose, lipids, electrolytes, vitamins and trace elements when patients cannot use the gastrointestinal tract or nutrition needs cannot be met through the gastrointestinal tract alone(Reference Baiu and Spain1). In response to major stress like abdominal surgery, the body shifts to a metabolic model of mixed energy supply based on glucose and lipids, particularly in the critical metabolic organs such as liver(Reference Finnerty, Mabvuure and Ali2). In clinical practice, patients undergoing abdominal surgery require fat emulsion-based early parenteral nutrition to meet or replenish their nutritional needs due to high nutritional risk, poor tolerance to enteral nutrition and post-operative fasting(Reference Gao, Liu and Zhang3). Significant efforts are still being made to develop a more appropriate strategy in early parenteral nutrition to provide the necessary nutritional support for patients undergoing abdominal surgery.
Hemihepatectomy, a radical curative procedure, is widely employed for treating hepatic malignancies and benign tumours(Reference Cai4). Previous preclinical studies have shown that peripheral-derived lipids rapidly accumulate in the liver after hepatectomy, and inhibiting this lipid accumulation delays hepatocyte proliferation and repair after hepatectomy(Reference Shteyer, Liao and Muglia5), which provides a theoretical basis for the use of fat emulsion-based early parenteral nutrition after hepatectomy. However, compared with partial hepatectomy, hemihepatectomy results in a smaller residual liver volume and an increased risk of small-for-size syndrome, impeding the regeneration of residual liver and the recovery of liver function(Reference van den Broek, Olde Damink and Dejong6,Reference Papamichail, Pizanias and Heaton7) . Furthermore, patients following hemihepatectomy generally have chronic liver diseases such as viral hepatitis and cirrhosis, which places their potential liver function in the vulnerable or decompensated states to exacerbate small-for-size syndrome even liver dysfunction after hemihepatectomy(Reference van den Broek, Olde Damink and Dejong6,Reference Papamichail, Pizanias and Heaton7) . Importantly, the liver, as a key metabolic organ, is involved in the synthesis and metabolism of various substances, particularly lipids(Reference Bechmann, Hannivoort and Gerken8). Post-hepatectomy liver dysfunction reduces the hepatic ability to consume and utilise lipids under stress conditions(Reference Huang, Gan and Mo9). The excessive accumulation of lipids in the liver leads to potential lipotoxicity, triggering inflammatory responses and metabolic disturbances, which further impairs liver function(Reference Neuschwander-Tetri10). Notably, due to the difficulty in obtaining clinical samples regarding regenerative liver, little is known about the impacts of fat emulsion-based early parenteral nutrition on lipid metabolism in regenerative liver. Therefore, exploring the effects of fat emulsion-based early parenteral nutrition on short-term recovery after hemihepatectomy could be a promising starting point.
Currently, clinical practice offers various formulations of fat emulsions, including long-chain TAG (LCT), physically mixed medium and long-chain TAG (MCT/LCT), structured TAG (STG) and n-3 fish oil emulsions. Given the differences in carbon chain length and structure among TAG, emerging studies suggest that carbon chain length and structure might affect the metabolic processes of different fat emulsion types in the body(Reference Hultin, Müllertz and Zundel11,Reference Wanten and Naber12) . Although previous studies have reported the effects of different types of fat emulsions on peri-operative outcomes in surgery(Reference Calder, Jensen and Koletzko13), it is also unclear whether short-term post-operative recovery was influenced by the different types of fat emulsion in patients following hemihepatectomy. This necessitates an in-depth analysis involving the effect of fat emulsions for patients undergoing hemihepatectomy.
In this study, we evaluated the effects of fat emulsion-based early parenteral nutrition for patients undergoing hemihepatectomy. Furthermore, we investigated the differences in short-term post-operative recovery in early parenteral nutrition with different fat emulsion formulations.
Methods
Data collection
Clinical data were retrospectively collected and analysed from 571 patients who underwent hemihepatectomy at the Division of Hepatobiliopancreatic Surgery, Department of General Surgery, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, China, between February 2010 and August 2020. The inclusion criteria for this study were as follows: (i) patients with indications for hemihepatectomy; (ii) patients who underwent either left or right hemihepatectomy; (iii) patients who received parenteral nutritional support from the day of surgery for at least 5 days post-operatively. Exclusion criteria included as follows: (i) patients with incomplete clinical data; (ii) patients with immunodeficiency disorders, hyperthyroidism, hyperlipidaemia, diabetes, severe jaundice, chronic renal disease, a history of acute myocardial infarction or stroke within the past 6 months or contraindications to fat emulsion use (e.g. fat malabsorption, allergy to fat emulsion components, etc.); (iii) patients with pre-operative malnutrition. The collected clinical data included demographic and peri-operative variables such as age, gender, BMI, surgical approach, Child-Pugh score, intra-operative blood loss, pathological findings, length of post-operative hospital stay and post-operative complications (including liver dysfunction, lung infection, abdominal infection, pleural effusion, ascites and biliary leakage). Additionally, peri-operative laboratory parameters were recorded, including RBC count, WBC count, platelet count (PLT), Hb, alanine aminotransferase, aspartate aminotransferase (AST), total bilirubin (TBIL), direct bilirubin (DBIL), indirect bilirubin (IBIL), albumin and C-reactive protein (CRP). This study was conducted in accordance with the ethical principles of the Declaration of Helsinki (as revised in 2013) and was approved by the Medical Ethics Committee of Nanfang Hospital, Southern Medical University (NFEC-2017-119).
Patients and treatment
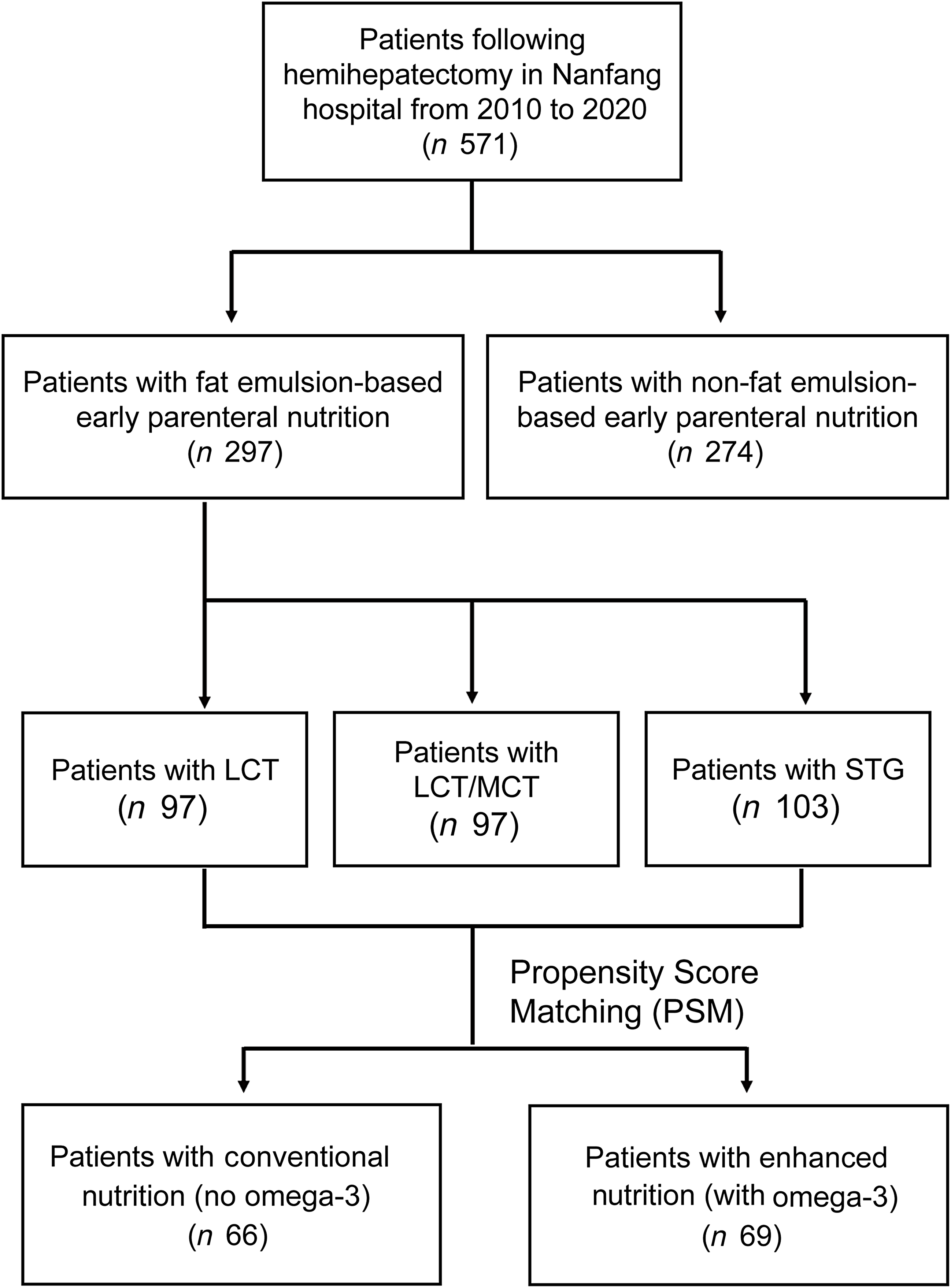
According to whether fat emulsion-based early parenteral nutrition was implemented during the patient’s previous treatment, patients were categorised into the non-fat emulsion-based early parenteral nutrition group (non-fatty Nutrition Group, n 274) and the fat emulsion-based early parenteral nutrition group (fatty Nutrition Group, n 297) (Figure 1). Demographic and clinical characteristics are summarised in online Supplementary Table S1. From the day of surgery to post-operative day (POD) 5, all patients received continuous parenteral nutritional therapy, which included glucose, amino acids, electrolytes, trace elements and vitamins. The nutritional regimens of both groups were isonitrogenous and isocaloric, with a nitrogen intake of 0·25 g/kg/d, a total caloric intake of 125.52 kJ/kg/d (30 kcal/kg/d) and non-protein calories ranging from 62.76 to 83.68 kJ/kg/d (from 15 to 20 kcal/kg/d). In the non-fat emulsion-based nutrition group, non-protein calories were exclusively derived from glucose, whereas in the fat emulsion-based nutrition group, non-protein calories were supplied by both glucose and fat emulsions, with an energy ratio of glucose to fat set at 6:4. Fat emulsions were administered at a dosage of 1·0–1·5 g lipid/kg/d to meet nutritional requirements. Based on the type of fat emulsion used, the fat emulsion-based nutrition group was further stratified into the LCT subgroup (n 97), the LCT/MCT subgroup (n 97) and the STG subgroup (n 103) (Figure 1). Additionally, using 1:1 propensity score matching, the fat emulsion-based nutrition group was further divided into the conventional nutrition subgroup (n 66) and the enhanced nutrition subgroup (n 69) (Figure 1). In the enhanced nutrition subgroup, n-3 fish oil fat emulsions (2 ml/kg/d) were continuously administered from the day of surgery to POD 5 in addition to the standard fat emulsion-based nutrition regimen. In this study, the sources of fat emulsions were as follows: LCT was provided by a fat emulsion–amino acids (17AA)-glucose (11 %) injection (1440 ml, Cavin, Fresenius Kabi AB, China); MCT/LCT was provided by Qiaoguang Kalu (Baxter, China) and STG was provided by a 250-ml Levin emulsion (Fresenius Kabi AB, China). n-3 fish oil emulsions were supplied as ω-3 fish oil fat emulsion injection (Fresenius Kabi Austria GmbH, Austria). The nutritional solutions consisted of mixtures of glucose, amino acids, fat emulsions, electrolytes and vitamins, all of which were infused via a central vein. All patients began oral intake following anal exhaust. In addition to nutritional support, comprehensive post-operative care was routinely provided.
The flow chart of the study. LCT subgroup, long chain subgroup; LCT/MCT subgroup, physically mixed medium and long chain; STG subgroup, structured TAG.

Assessment
Venous blood samples were collected from all patients preoperatively and in the early morning on POD 1, POD 3, POD 5 and POD 7. The effects of fat emulsion administration were evaluated based on laboratory parameters related to routine blood tests, liver function tests, inflammatory response and post-operative short-term outcomes. These parameters included alanine aminotransferase, AST, TBIL, DBIL, IBIL, albumin, RBC, WBC, Hb, PLT and CRP. Additionally, post-operative short-term outcomes included liver dysfunction, lung infection, abdominal infection, pleural effusion, ascites, biliary leakage, lengths of post-operative hospital stay (LOPOHS) and fasting durations. Biliary leakage was defined as a bilirubin concentration in the drainage fluid at least three times higher than that in the serum on POD 3(Reference Koch, Garden and Padbury14). Liver dysfunction following hepatectomy was defined as an international normalised ratio of prothrombin time > 1·5 or a TBIL level > 34·2 μmol/l on POD 5(Reference Rahbari, Garden and Padbury15). Post-hepatectomy liver dysfunction was further classified into three grades: Grade A: No changes in the patient’s clinical management were required. Grade B: The clinical course deviated from the standard post-operative trajectory but did not necessitate invasive intervention. Grade C: Invasive therapeutic interventions were required(Reference Rahbari, Garden and Padbury15). Lung infection was diagnosed based on positive post-operative sputum bacterial and/or fungal cultures or radiological evidence of pneumonia. Abdominal infection was confirmed by positive bacterial or fungal cultures from post-operative abdominal drainage fluid(Reference Ljubicic, Spajic and Vrkljan16). Pleural effusion was diagnosed via imaging findings of pulmonary effusion(Reference Ahmad, Krishnadas and Froeschle17). Ascites were identified using abdominal ultrasonography or computed tomography(Reference Hou and Sanyal18).
Statistical analysis
All statistical analyses were performed using SPSS Statistics 23·0 software (IBM, Armonk, NY, USA). A P-value < 0·05 was considered statistically significant. Quantitative data with a normal distribution were presented as mean (standard deviation (sd)), while data with a skewed distribution were expressed as the median and interquartile range. Differences between the two groups for normally distributed data were analysed using the Student’s t test. One-way analysis of variance (ANOVA) was applied for comparisons among multiple groups of normally distributed data, with post hoc pairwise comparisons conducted using the least significant difference (t test). The Mann–Whitney U test was used to compare skewed data between two groups, while the Kruskal–Wallis test was employed for comparisons among multiple groups of skewed data. Categorical variables were analysed using the Chi-square test or Fisher’s exact test, as appropriate. Propensity score matching was applied to balance confounding factors between the conventional nutrition subgroup and the enhanced nutrition subgroup.
Results
The effects of fat emulsion-based early parenteral nutrition in liver function and routine blood tests in patients following hemihepatectomy
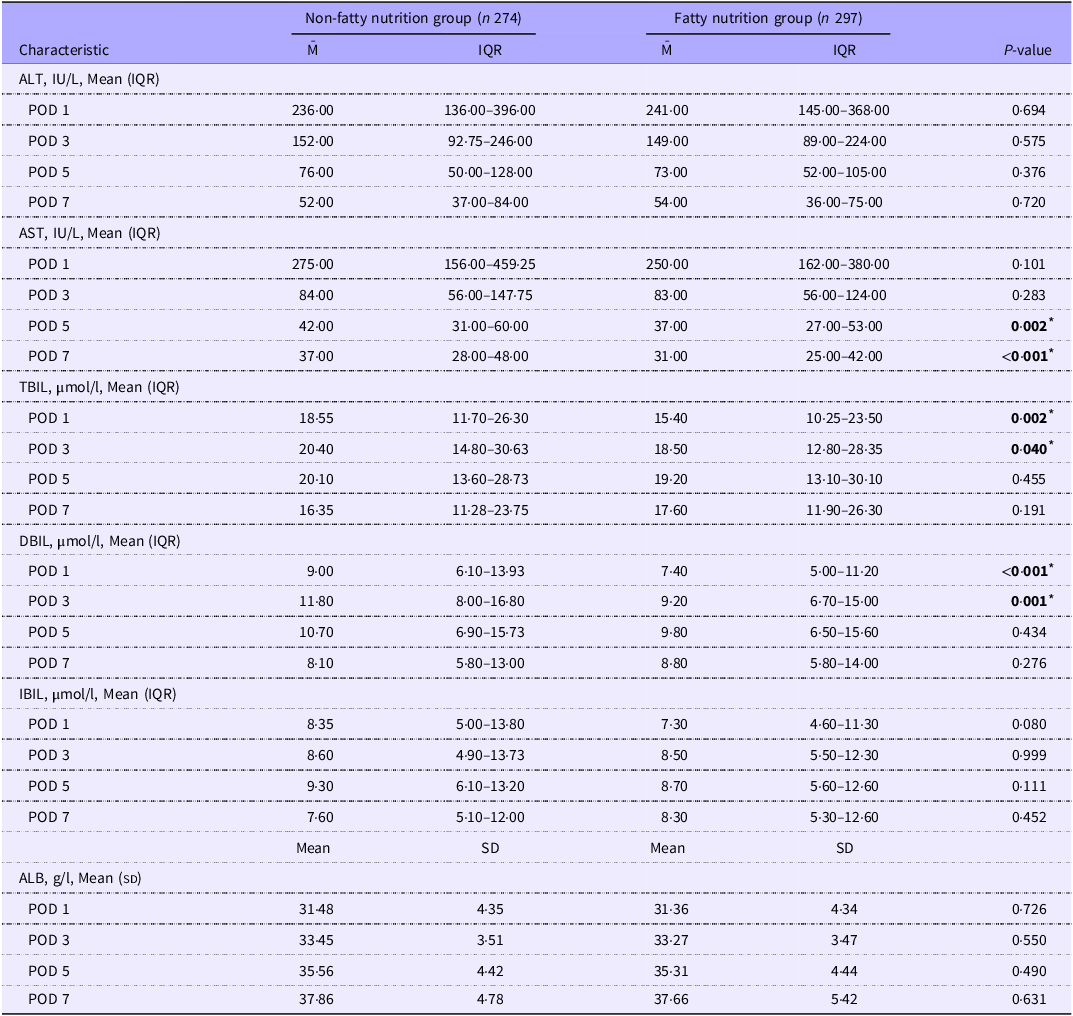
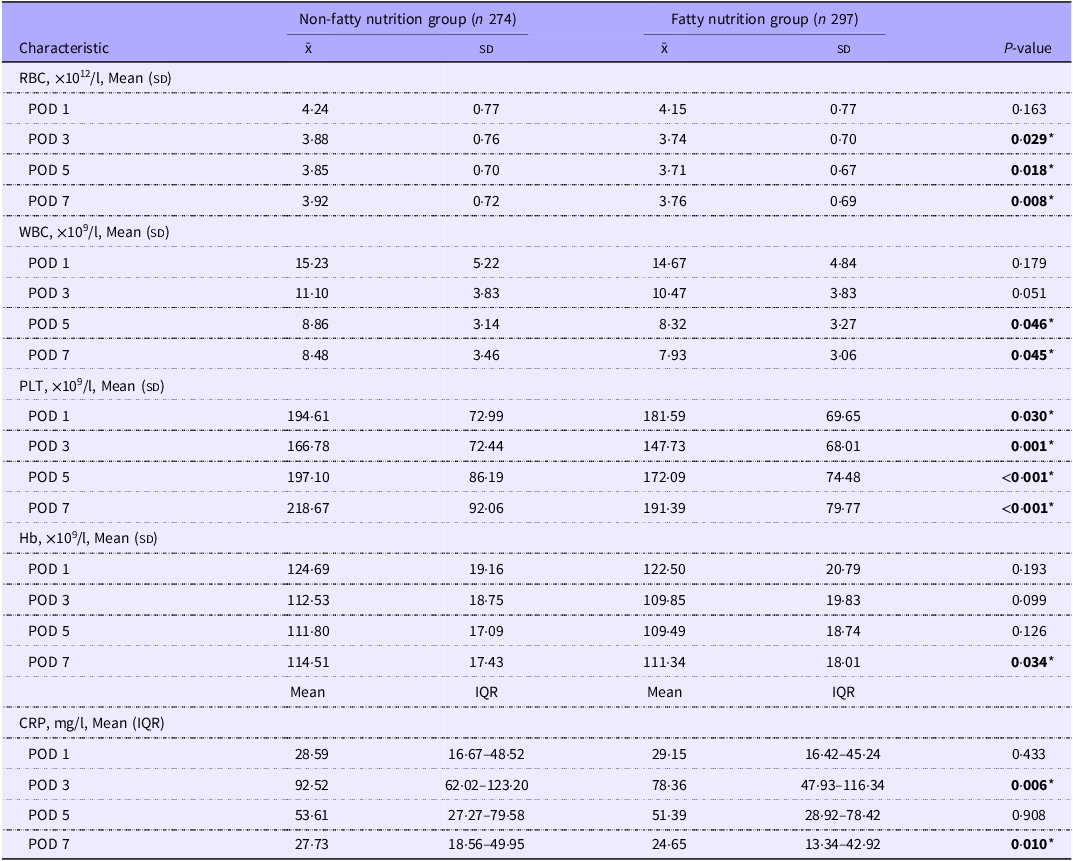
No significant differences were observed in the baseline characteristics between the non-fatty nutrition group and the fatty nutrition group, except for the pathological diagnosis of patients (online Supplementary Table S1). The fatty nutrition group showed significantly reduced levels of AST on POD5 and POD 7 compared with the non-fatty nutrition group (POD 5, 42·00 IU/L v. 37·00 IU/L, P < 0·05, POD 7, 37·00 IU/L v. 31·00 IU/L, P < 0·05) (Table 1). Moreover, in the fatty nutrition group, the levels of TBIL and DBIL on POD 1 and POD 3 were significantly decreased compared with the non-fatty nutrition group (TBIL POD 1, 18·55 μmol/l v. 15·40 μmol/l, P < 0·05, POD 3, 20·40 μmol/l v. 18·50 μmol/l, P < 0·05, DBIL POD 1, 9·00 μmol/l v. 7·40 μmol/l, P < 0·05, POD 3, 11·80 μmol/l v. 9·20 μmol/l, P < 0·05) (Table 1). We also found no significant differences in the other liver function parameters, including alanine aminotransferase, IBIL and albumin (Table 1). In the blood routine tests, from POD 3 to POD 7, RBC levels were significantly lower in the fatty nutrition group than those in the non-fatty nutrition group (POD 3, 3·88 × 1012/l v. 3·74 × 1012/l, P < 0·05, POD 5, 3·85 × 1012/l v. 3·71 × 1012/l, P < 0·05, POD 7, 3·92 × 1012/l v. 3·76 × 1012/l, P < 0·05) (Table 2). Notably, anaemia was not observed in either group, while the levels of Hb were significantly reduced in the fatty nutrition group on POD 7 (114·51 × 109/l v. 111·34 × 109/l, P < 0·05) (Table 2). Additionally, PLT levels from POD 1 to POD 7 were also significantly decreased in the fatty nutrition group compared with the non-fatty nutrition group (POD1, 194·61 × 109/l v. 181·59 × 109/l, P < 0·05, POD 3, 166·78 × 109/l v. 147·73 × 109/l, P < 0·05, POD 5, 197·10 × 109/l v. 172·09 × 109/l, P < 0·05, POD 7, 218·67 × 109/l v. 191·39 × 109/l, P < 0·05) (Table 2). Interestingly, we observed the significant reduced WBC levels on POD 5 and POD 7 in the fatty nutrition group (POD 5, 8·86 × 109/l v. 8·32 × 109/l, P < 0·05, POD 7, 8·48 × 109/l v. 7·93 × 109/l, P < 0·05), with the significant decrease of CRP levels on POD 3 and POD 7 in the fatty nutrition group (POD 3, 92·52 mg/l v. 78·36 mg/l, P < 0·05, POD 7, 27·73 mg/l v. 24·65 mg/l, P < 0·05) (Table 2). These results collectively suggest that while the reduced trends of hemogram exist in the fat emulsion-based early parenteral nutrition, fat emulsion-based early parenteral nutrition improves liver function and reduces inflammatory response in patients following hemihepatectomy.
Liver function of groups with or without early fatty nutrition (Mean values and standard deviations; median values and interquartile ranges)

POD, post-operative day; IQR, interquartile range; ALT, alanine aminotransferase; ALB, albumin; AST, aspartate aminotransferase; DBIL, direct bilirubin; IBIL, indirect bilirubin; TBIL, total bilirubin.
* P-value in boldface indicates statistical significance between Non-fatty nutrition group and Fatty nutrition group, P-value< 0·05.
Blood routine tests and CRP tests of groups with or without early fatty nutrition (Mean values and standard deviations; median values and interquartile ranges)

POD, post-operative day; PLT, platelet count; IQR, interquartile range; CRP, C-reactive protein.
* P-value in boldface indicates statistical significance between Non-fatty nutrition group and Fatty nutrition group, P-value < 0·05.
Fat emulsion-based early parenteral nutrition accelerates post-operative recovery without affecting post-operative short-term complications in hemihepatectomy
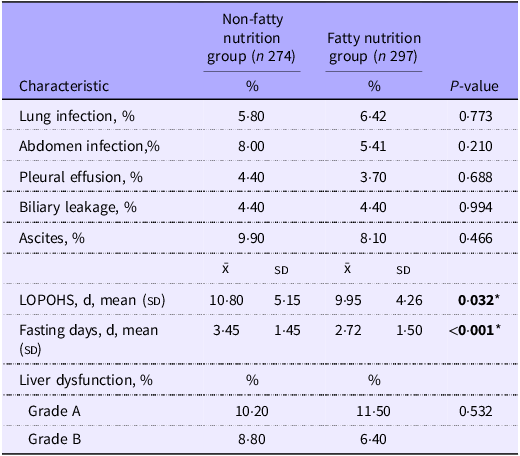
Post-operative complications and short-term recovery outcomes were evaluated in the non-fatty nutrition and fatty nutrition groups. As shown in Table 3, no significant differences were observed in the incidence of different classified post-operative liver dysfunction between the non-fatty nutrition group and fatty nutrition group. Moreover, fat-emulsion-based early parenteral nutrition had no impact on the incidence of short-term complications including lung infection, abdominal infection, pleural effusion, ascites and biliary leakage (Table 3). Notably, patients undergoing hemihepatectomy in the fatty nutrition group had significantly shorter LOPOHS and fasting durations compared to the non-fatty nutrition group (LOPOHS, 10·80 d v. 9·95 d, P < 0·05, fasting duration, 3·45 d v. 2·72 d, P < 0·05) (Table 3), suggesting that the fat emulsion-based early parenteral nutrition promotes short-term recovery after hemihepatectomy.
Post-operative recovery situations and complications in groups with or without early fatty nutrition (Percentages; median values and interquartile ranges)

LOPOHS, lengths of post-operative hospital stay.
* P-value in boldface indicates statistical significance between Non-fatty nutrition group and Fatty nutrition group, P-value < 0·05.
Different fat emulsion formulations have no impact on liver function tests, routine blood tests and post-operative short-term complications and recovery
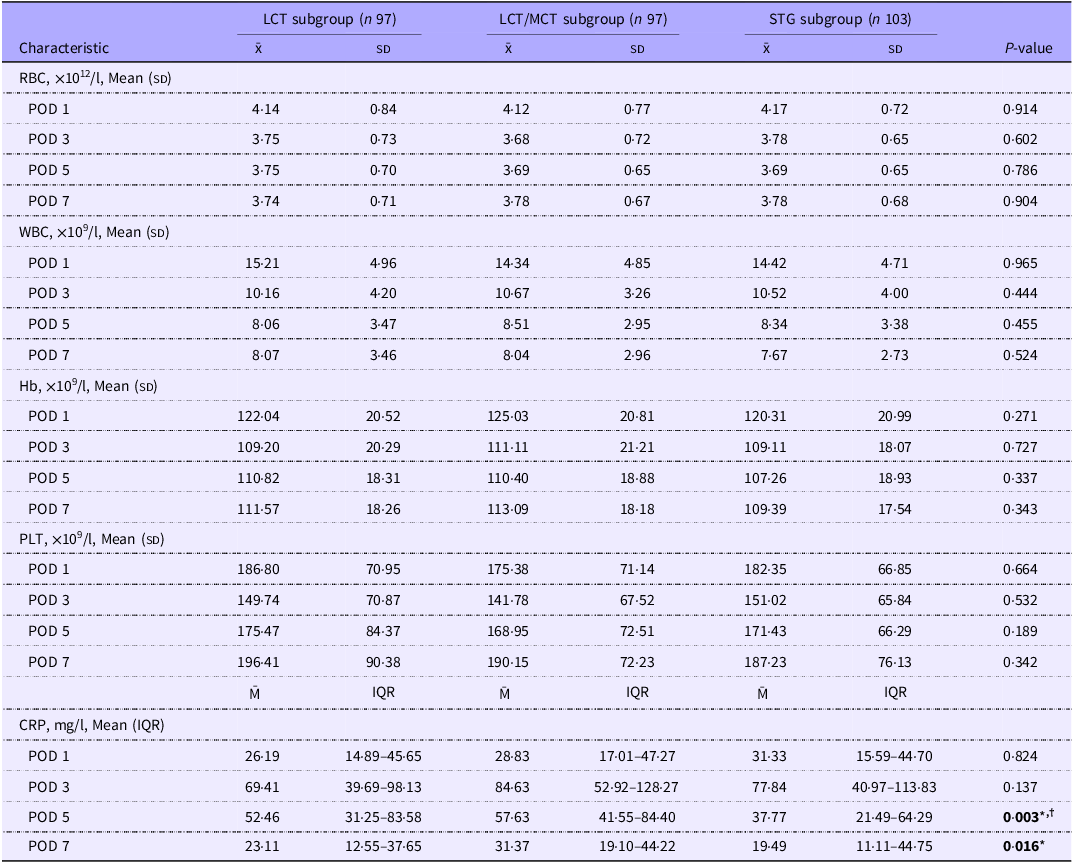
Among the LCT, LCT/MCT and STG subgroups, the baseline characteristics were comparable, including gender, age, BMI, HBsAg status, cirrhosis, Child-Pugh score, surgical approach, intra-operative blood transfusion, post-operative blood transfusion and post-operative choleretic medication (online Supplementary Table S2). No significant differences were found among these subgroups in liver function and routine blood tests, including alanine aminotransferase, AST, TBIL, DBIL, IBIL, albumin, RBC, WBC, PLT and Hb (Table 4 and online Supplementary Table S3). Interestingly, we found that the levels of CRP were significantly different among these subgroups on POD 5 and POD 7 (POD 5, 52·46 mg/l v. 57·63 mg/l v. 37·77 mg/l, P < 0·05, POD 7, 23·11 mg/l v. 31·37 mg/l v. 19·49 mg/l, P < 0·05, respectively) (Table 4). In the STG subgroup, CRP levels were significantly reduced on POD 5 compared with the LCT subgroup or the LCT/MCT subgroup (Table 4). Similarly, the levels of CRP on POD 7 in the STG subgroup were significantly decreased compared to the LCT/MCT subgroup (Table 4). Additionally, there were no significant differences in the incidence of post-hepatectomy liver dysfunction, post-operative complications, LOPOHS and fasting duration among the subgroups (online Supplementary Table S4). These findings collectively indicate that the early parenteral nutrition with different fat emulsion formulations has no marked effect on short-term recovery in patients following hemihepatectomy.
Blood routine tests and CRP test of LCT, LCT/MCT and STG subgroups (Mean values and standard deviations; median values and interquartile ranges)

LCT subgroup, long chain subgroup; LCT/MCT subgroup, physically mixed medium and long chain; STG subgroup, structured TAG. IQR, interquartile range; POD, post-operative day; PLT, platelet count; CRP, C-reactive protein.
* P-value in boldface indicates STG subgroup is significantly different from LCT/MCT subgroup (P-value < 0·05).
† P-value in boldface indicates STG subgroup is significantly different from LCT subgroup (P-value < 0·05).
Additional administration of n-3 fish oil emulsions reduces inflammation and the incidence of lung infections after hemihepatectomy
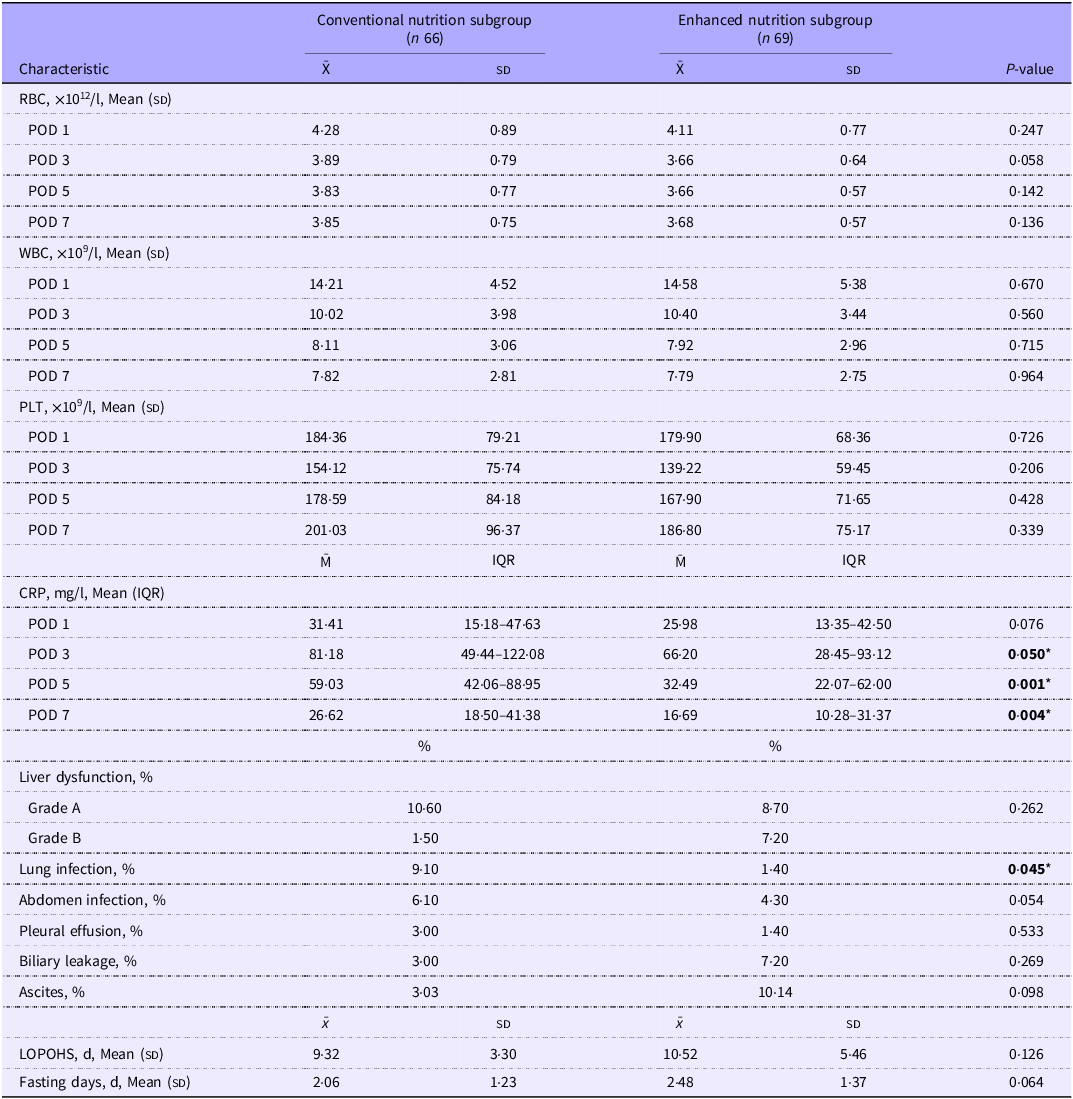
To explore the roles of additional administration of n-3 fish oil emulsions, patients in the fatty nutrition group were further classified into two groups: one receiving fat emulsion-based early parenteral nutrition with n-3 fish oil emulsions supplementation (Enhanced Nutrition Subgroup, n 69) and the other receiving fat emulsion-based early parenteral nutrition without n-3 fish oil emulsions supplementation (Conventional Nutrition Subgroup, n 228). We found that age, HBsAg status, surgical method, intra-operative blood transfusion, post-operative blood transfusion and post-operative choleretic medication were significantly different in the baseline characteristics between the enhanced nutrition subgroup and conventional nutrition subgroup (online Supplementary Table S5). To minimise the biases of baseline characteristics, 1:1 propensity score matching was performed using an allowable range of 0·10 and the predefined screening criteria including age, HBsAg status, surgical method, intra-operative blood transfusion, post-operative blood transfusion and post-operative choleretic medication. No significant differences were found in the baseline characteristics between the enhanced nutrition subgroup (n 69) and conventional nutrition subgroup (n 66) after propensity score matching (online Supplementary Table S6). Fat emulsion-based early parenteral nutrition supplemented with n-3 fish oil emulsions had no significant impact on liver function tests and routine blood tests (Table 5 and online Supplementary Table S7). Similarly, no significant differences between these two subgroups were observed in post-hepatectomy liver dysfunction, pleural effusion, ascites, biliary leakage, LOPOHS and fasting duration (Table 5). Notably, CRP levels were significantly reduced in the enhanced nutrition subgroup from POD 3 to POD 7 (POD 3, 81·18 mg/l v. 66·20 mg/l, P < 0·05, POD 5, 59·03 mg/l v. 32·49 mg/l, P < 0·05, POD 7, 26·62 mg/l v. 16·69 mg/l, P < 0·05) (Table 5). Consistently, fat emulsion-based early parenteral nutrition supplemented with n-3 fish oil emulsions significantly reduced the incidence of lung infection, with a decreasing trend in the incidence of abdomen infection (Table 5), indicating that the fat emulsion-based early parenteral nutrition with n-3 fish oil emulsions has a positive effect on controlling inflammatory response in patients following hemihepatectomy.
Blood routine tests, CRP test and post-operative recovery situations and complications between conventional nutrition subgroup and enhanced nutrition subgroup after propensity score matching (Mean values and standard deviations; median values and interquartile ranges; percentages)

POD, post-operative day; PLT, platelet count; IQR, interquartile range; CRP, C-reactive Protein; LOPOHS, lengths of post-operative hospital stay.
* P-value in boldface indicates statistical significance between Conventional nutrition subgroup and Enhanced nutrition subgroup, P-value< 0·05.
Discussion
This study presents the effects of fat emulsion-based early parenteral nutrition for patients undergoing hemihepatectomy. We found that fat emulsion-based early parenteral nutrition improves liver function and reduces LOPOHS and fasting duration in patients following hemihepatectomy, with a minor decrease in RBC and PLT. Moreover, the fat emulsion-based early parenteral nutrition with n-3 fish oil emulsions reduces inflammation after hemihepatectomy. These findings suggest that fat emulsion-based parenteral nutrition is feasible during the early recovery period of post-hemihepatectomy, serving as a conventional therapy of post-hemihepatectomy.
Appropriate therapies during post-hemihepatectomy are key to ensure early post-operative recovery(Reference Joliat, Kobayashi and Hasegawa19). Early parenteral nutrition provides adequate nutritional support to maintain physiological function under hepatectomy-induced stress(Reference Gao, Tian and Wang20). Given that peripheral-derived lipids rapidly accumulate in the liver after hepatectomy, fat emulsion-based early parenteral nutrition might further exacerbate lipid accumulation within the liver. Under normal physiological conditions, the liver can metabolise such lipids accumulation(Reference Bechmann, Hannivoort and Gerken8). However, due to the reduced number of functional hepatocytes, the hepatic ability to metabolise lipids is impaired after hemihepatectomy, leading to the excessive lipid accumulation(Reference Shteyer, Liao and Muglia5). These accumulated lipids damage hepatocytes by activating oxidative stress and inducing inflammatory responses, thereby exacerbating liver dysfunction(Reference Neuschwander-Tetri10,Reference Ferro, Baratta and Pastori21) . Therefore, it is crucial to assess the impact of fat emulsion-based early parenteral nutrition on the short-term outcomes of hemihepatectomy.
Fat emulsion-based early parenteral nutrition promotes post-operative short-term recovery in surgical patients(Reference Gao, Liu and Zhang3). We found that fat emulsion-based early parenteral nutrition significantly reduced the parameters of post-operative liver function tests, including AST, TBIL and DBIL, indicating that the use of fat emulsions decreases transaminase leakage and improves bilirubin metabolism. Similarly, previous research revealed that polyunsaturated fatty acids in fat emulsions alleviate cholestasis and decrease the morbidity of parenteral nutrition-related liver disease(Reference Raman, Almutairdi and Mulesa22). Additionally, our results showed that the early post-operative administration of parenteral nutrition with fat emulsions has no significant impact on the incidence of short-term post-operative complications after hemihepatectomy. Westvik et al. have reported that patients with chronic diseases are prone to occur post-operative malnutrition after major surgery, which is associated with a higher incidence of post-operative complications(Reference Westvik, Krause and Pradhan23). The European Society for Clinical Nutrition and Metabolism recommends the immediate nutritional intervention for malnourished patients following surgery, as it significantly adjusts their nutritional status to improve outcomes(Reference Wong, Praseedom and Liau24,Reference Braga, Ljungqvist and Soeters25) . Consistently, our findings showed that LOPOHS and fasting duration were markedly shortened in the fatty nutrition group, suggesting that the fat emulsion-based early parenteral nutrition accelerates short-term recovery in patients following hemihepatectomy. However, we found the levels of RBC, Hb and PLT were significantly reduced in the fatty nutrition group. Dahlan et al. pointed out that the infusion of fat emulsions alters the lipid composition of cell membranes to affect membrane stability, leading to hemolysis or blood cell damage(Reference Dahlan, Richelle and Kulapongse26), which potentially contributes to the reduction in RBC and Hb levels. The decrease in PLT may be attributed to the activation of platelets by fatty acids contained in the fat emulsion, resulting in platelet consumption(Reference Barrachina, Pernes and Becker27). Moreover, the metabolism of intravenous fat emulsions primarily relies on the liver. In patients with chronic liver diseases, the reduced hepatic metabolic and synthetic functions may affect hematopoiesis(Reference van Dievoet, Eeckhoudt and Stephenne28), potentially resulting in a decrease in RBC, PLT and Hb levels. Although RBC and PLT levels in the fatty nutrition group were significantly reduced compared with the non-fatty nutrition group, these values remained within the normal range and showed a trend of recovery. Given the major stress induced by hemihepatectomy, a more cautious approach is warranted. During the administration of fat emulsion-based early parenteral nutrition after hemihepatectomy, monitoring vital signs and laboratory parameters, such as routine blood tests, liver function tests and blood lipids, are essential to ensure safety and adjust therapeutic strategy.
The impacts on post-operative recovery are varied by using different types of fat emulsion(Reference Chambrier, Lauverjat and Bouletreau29). Traditional long-chain TAG is rich in n-6 polyunsaturated fatty acids, known to promote inflammation and suppress immune responses(Reference Larbi, Grenier and Frisch30,Reference Wu, Wang and Yang31) . The hydrolysis rate of medium-chain TAG and the production of ketone bodies are disturbed by the metabolism of the long-chain TAG, leading to metabolic dysregulation to increase the hepatic and renal burden(Reference Cotter, Johnson and Young32). In our study, we found no significant differences in the most laboratory parameters and clinical short-term outcomes among these three subgroups in patients undergoing hemihepatectomy. The relatively short duration of fat emulsion administration may contribute to the lack of significant differences among these three subgroups. Notably, we observed that CRP levels on POD 5 and POD 7 in the STG subgroup were significantly reduced compared with the LCT or LCT/MCT subgroups. STG, due to its faster clearance rate, is widely used in clinical practice(Reference Nordenström, Thörne and Aberg33). Previous studies have confirmed that the parenteral nutrition containing STG after hepatectomy reduces inflammation and improves immune function(Reference Zhao and Wang34). Furthermore, we evaluated the effects of fat-emulsion-based early parenteral nutrition supplemented with n-3 fish oil emulsions in patients following hemihepatectomy. Our results indicate that n-3 fish oil emulsions supplementation significantly reduced CRP levels and the incidence of lung infections after hemihepatectomy. Similarly, a decreased trend of abdomen infections was observed in the enhanced nutrition subgroup. n-3 fatty acids, riched in eicosapentaenoic acid and docosahexaenoic acid, have been reported to regulate immune function in monocytes, macrophages and endothelial cells(Reference Calder35,Reference Gong, Liu and Liao36) . Previous studies have suggested that n-3 fish oil emulsions are safe and effective in reducing post-operative inflammation(Reference Gong, Liu and Liao36–Reference Zhu, Wu and Qiu38). Although our study explored the effects of fat emulsion-based early parenteral nutrition in patients undergoing hemihepatectomy, due to the limited number of patients and single-centre study, our results still need to be validated in larger and multi-centre studies.
In conclusion, our findings indicate that fat emulsion-based early parenteral nutrition promotes short-term post-operative recovery in patients following hemihepatectomy, with a slight decrease in hemogram. The additional administration of n-3 fish oil emulsions in the fat emulsion-based early parenteral nutrition is associated with reduced inflammatory response and risk of post-operative infections. These findings provide evidence for the clinical practice of fat-emulsion-based early parenteral nutrition after hemihepatectomy.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525000613
Acknowledgements
We would like to acknowledge the data support provided by the Division of Hepatobiliopancreatic Surgery, Department of General Surgery, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, China.
Author Kai Wang was supported by grants from the National Natural Science Foundation of China (82170647). Author Chuanjiang Li was supported by grants from the National Natural Science Foundation of China (82270661) and the Guangdong Basic and Applied Basic Research Foundation (2023A1515010088). The funding source has no role in the design, practice or analysis of this study.
L. L. and Y. L.: study conception and design, acquisition of data, drafting of the manuscript, analysis and interpretation of data. Q. H. and H. L.: acquisition of data and revision of the manuscript. J. Z., K. W. and C. L.: study conception and design and critical revision of the manuscript.
All authors declare that they have no conflicts of interest to disclose.