


Background and rationale
One of the main challenges in mental health care is the marked clinical, biological, and functional heterogeneity of mental disorders [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1]. This heterogeneity limits prognostic accuracy and constrains the development and implementation of effective interventions [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1, Reference Williams, Carpenter, Carretta, Papanastasiou and Vaidyanathan2]. In many cases, individuals with distinct underlying biological alterations receive the same clinical diagnosis, while similar symptoms can result from different pathophysiological mechanisms [Reference Williams, Carpenter, Carretta, Papanastasiou and Vaidyanathan2–Reference Clark, Cuthbert, Lewis-Fernandez, Narrow and Reed7]. Consequently, patients grouped under the same diagnostic category often show highly variable responses to the same intervention, and conversely, similar responses can be observed across different diagnostic categories [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1].
Over the past decade, advances in precision medicine have led to the incorporation of advanced diagnostic tools and integrated analyses of biological, genetic, psychological, environmental, and social data. This integration supports a more accurate characterisation of the aetiological bases of mental disorders and opens the door to improved prediction, prevention, diagnosis, and treatment tailoring [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1, Reference Fernandes, Williams, Steiner, Leboyer, Carvalho and Berk8–Reference Scala, Ganz and Snyder10].
Although they share most principles and goals, precision approaches have some specificities in the fields of psychology and psychiatry, but this distinction may be questionable at different levels, as in both disciplines, a precision-based approach aims to use objective data to stratify patients into subgroups that share common etiopathophysiologies, have a similar prognosis, and respond to specific treatments with a given mechanism of action. In psychology, precision approaches are more focused on cognitive, affective, and behavioural processes to tailor non-pharmacological interventions to a patient’s functional and psychological profile [Reference Purgato, Singh, Acarturk and Cuijpers11, Reference Deisenhofer, Barkham, Beierl, Schwartz, Aafjes-van Doorn and Beevers12]. In psychiatry, precision approaches additionally support pharmacological treatment selection based on genetic, neurochemical, neurophysiological, or neuroimaging biomarkers, with the aim of optimising therapeutic response, minimising adverse effects, and considering medical comorbidities and differential diagnoses [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1, Reference Fernandes, Williams, Steiner, Leboyer, Carvalho and Berk8–Reference Scala, Ganz and Snyder10].
Within this scenario, precision psychiatry emerges from the premise that even when two individuals present similar symptoms, the underlying causes may differ. This is particularly relevant in mental health due to strong influences from genetic, neurobiological, and environmental factors. The overarching objective is to improve diagnostic precision, either through the development of new diagnostic systems based on objective and measurable criteria or through improving the precision of current diagnostic frameworks, while tailoring interventions to increase efficacy, improve adherence, and anticipate response, thereby reducing outcome variability. This requires considering both intrinsic factors (e.g., genetics, neuroplasticity, individual biology) and extrinsic factors (e.g., social and family environment, lifestyle, external conditions) [Reference Manchia, Pisanu, Squassina and Carpiniello13–Reference Lippard and Nemeroff17] as well as their interaction.
Overall, the development and implementation of precision medicine in mental health provides a robust foundation for a more comprehensive, evidence-based, and person-centred model of care, while also raising important clinical, ethical, health economic, and policy considerations that are central to contemporary mental health systems.
Although precision and personalised medicine are sometimes used indistinctively, we believe that “personalised medicine” is a broader term that includes care tailored to the individual patient, while precision psychiatry reflects an approach to care guided by measurable data to place patients into biologically or clinically meaningful subgroups.
Applications of precision medicine in mental health
Advances in biomedical research are improving the understanding of the biological mechanisms underpinning mental disorders and are accelerating the development and validation of more precise diagnostic and therapeutic tools [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1, Reference Fernandes, Williams, Steiner, Leboyer, Carvalho and Berk8].
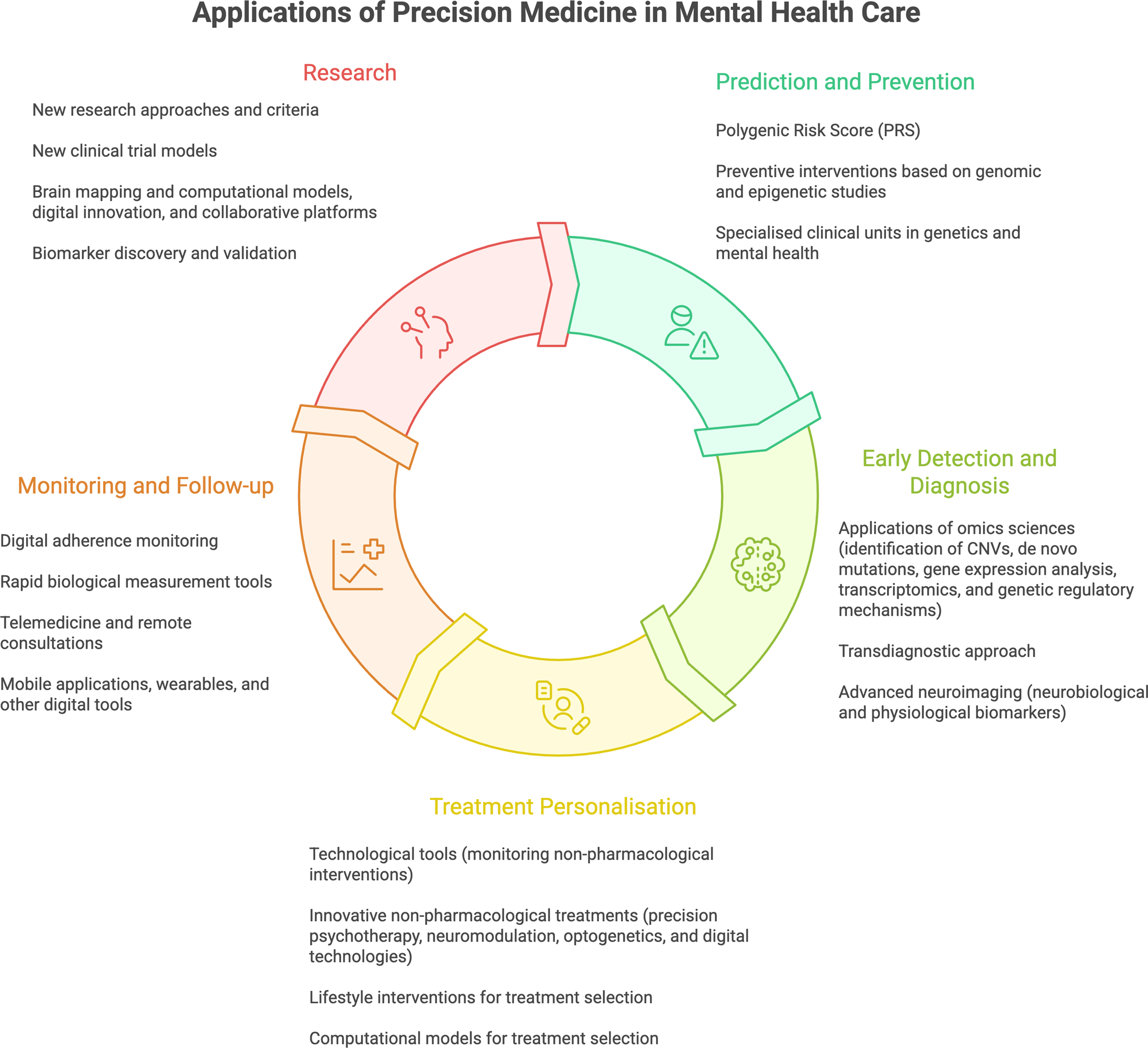
In clinical care, precision medicine has potential applications across the clinical pathway, including prediction and prevention, early detection and diagnosis, treatment personalisation, and monitoring and follow-up [Reference Williams, Carpenter, Carretta, Papanastasiou and Vaidyanathan2]. When implemented responsibly, it can support more targeted interventions aligned with an individual’s clinical and functional profile, in a context where the societal and economic burden of mental disorders remains a major challenge for healthcare systems [Reference Arango, Dragioti, Solmi, Cortese, Domschke and Murray15] (see Figure 1).
Applications of precision medicine in mental health care. This figure was created using Napkin (AI-assisted visualization tool) based on author-provided concepts and content.

Research
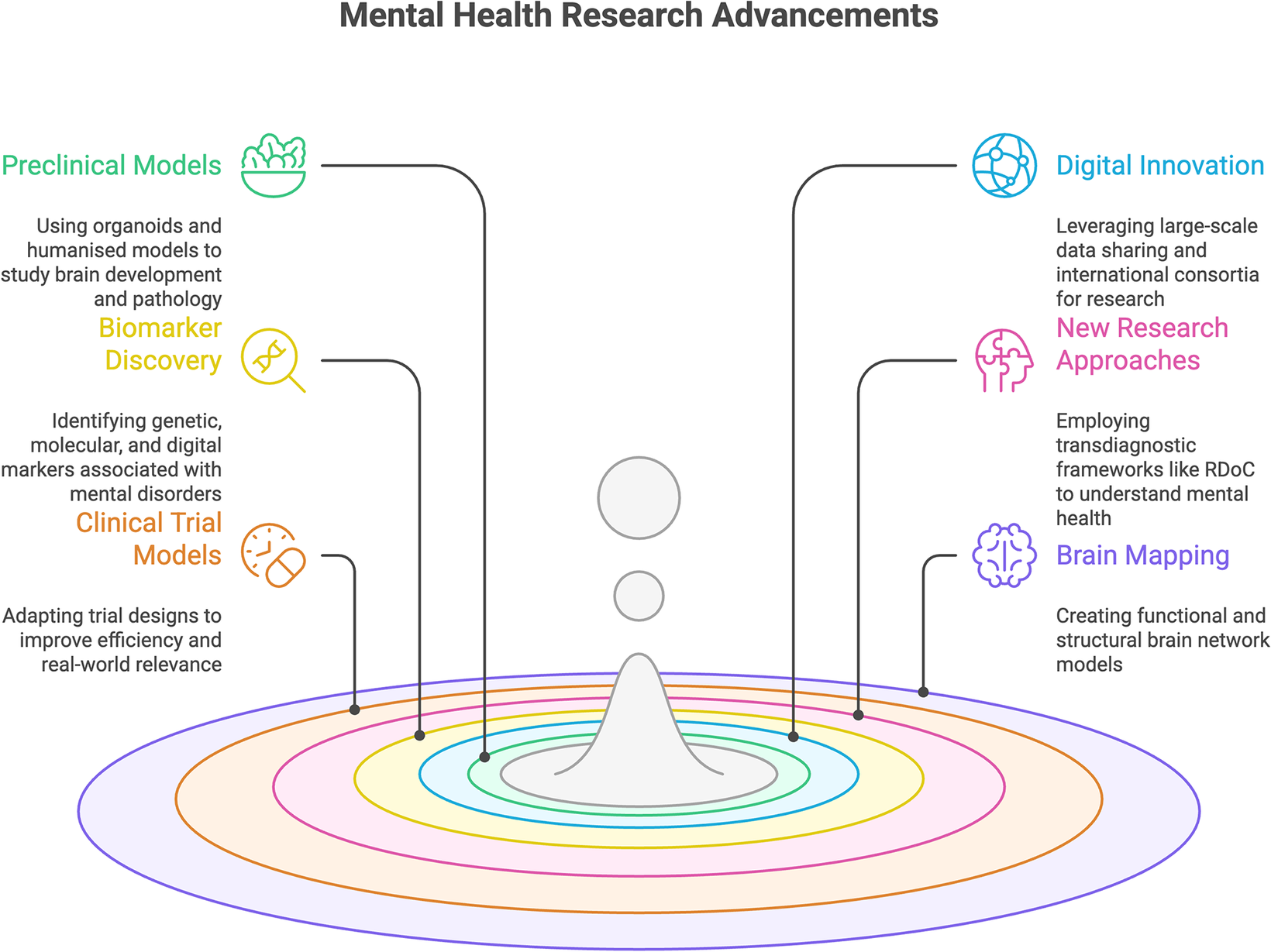
Recent advances in mental health research have generated new experimental, methodological, and collaborative approaches that underpin current developments in precision medicine (see Figure 2). These developments span research frameworks and technologies at different stages of validation and clinical translation.
Mental health research advancements. Note: This figure was created using Napkin (AI-assisted visualization tool) based on author-provided concepts and content.

Key research advances
-
• More precise preclinical studies of brain biology using human-relevant systems. Neuronal organoids and more complex brain region–specific organoids (“brain in a dish”) enable investigation of cellular and molecular mechanisms in environments closer to the human brain and facilitate evaluation of therapeutic interventions [Reference Zhang, Wang, Park, Song and Ming18–Reference Sloan, Andersen, Pasca, Birey and Pasca20].
-
• Humanised animal models, for example, implanting human neurons into genetically modified mice expressing human proteins, allow study of pathophysiological processes and treatment responses in systems closer to human biology [Reference Mansour, Goncalves, Bloyd, Li, Fernandes and Quang21, Reference Revah, Gore, Kelley, Andersen, Sakai and Chen22].
-
• Transdiagnostic research frameworks. The RDoC (Research Domain Criteria) approach promoted by the National Institute of Mental Health studies disorders through shared symptoms, processes, and mechanisms, supporting the identification of transdiagnostic biomarkers and more homogeneous clinical subgroups, improving clinical trial precision [Reference Williams, Carpenter, Carretta, Papanastasiou and Vaidyanathan2–Reference Etkin and Mathalon4]. Another current transdiagnostic approach is used in the HiTOP classification [Reference Kotov, Krueger, Watson, Achenbach, Althoff and Bagby23]. However, it must be stressed that both RDoC and HiTOP are meant to support research frameworks, but not to substitute clinical diagnostic systems such as DSM-5 or ICD-11.
-
• Expansion of transdiagnostic approaches to resistant depression, bipolar disorder, and schizophrenia, where shared mechanisms may be addressed through common strategies [Reference Cuthbert5–Reference Clark, Cuthbert, Lewis-Fernandez, Narrow and Reed7, Reference Kas, Penninx, Sommer, Serretti, Arango and Marston24, Reference Saris, Aghajani, Reus, Visser, Pijnenburg and van der Wee25].
-
• New clinical trial designs. Adaptive trials enable modification of parameters (dose, treatment, sample size) based on interim results that allow patient stratification and may be useful in the context of highly variable psychiatric treatment responses [Reference Lenze, Nicol, Barbour, Kannampallil, Wong and Piccirillo16]. N-of-1 studies evaluate treatment efficacy in single patients and support personalisation in complex cases [Reference Davidson, Silverstein, Cheung, Paluch and Epstein26]. Platform/basket trials evaluate multiple treatments across biological/clinical subgroups [Reference Joshi and Light27] which may aid in identifying theragnostic markers, that is biological markers that index response to a given treatment. Real‑world data and hybrid designs combine experimental evidence with digital registries and biomarkers [Reference Austin, Lobo, Samadbeik, Engstrom, Philip and Pole28]. Together, these designs support more flexible, efficient, and precise evaluation of interventions in mental health.
-
• Brain maps and computational modelling. Advances in neuroimaging, AI-based simulation, and genomic sequencing enable structural and functional models to understand circuits involved in cognition, emotion, and mood regulation. Initiatives such as the Human Brain Project and BRAIN Initiative support integrative neuroscience with translational potential [Reference Markram29, Reference Iyer, Maxson Jones, Robinson, Provenza, Duncan and Lazaro-Munoz30]. Human Cell Atlas efforts characterise brain cell types at the molecular level, enabling cellular-level insights [Reference Parums31].
-
• Biomarker discovery and validation. Consortia such as PSY-PGX [Reference van Westrhenen, Young, Heilbronner, Juruena, Ingelman-Sundberg and Jukic32], Psych-STRATA [Reference Baune, Fromme, Aberg, Adli, Afantitis and Akkouh33], and R-LiNK investigate genetic variants influencing treatment response, supporting biomarker targets for safer, more effective prescribing [Reference Scott, Hidalgo-Mazzei, Strawbridge, Young, Resche-Rigon and Etain34, Reference van Westrhenen, Young, Heilbronner, Juruena, Ingelman-Sundberg and Jukic35]. Projects such as PRISM, BD2, and CIBERSAM [Reference Arango and Vieta36] integrate neuroimaging, genetics, transcriptomics, epigenetics, and inflammation to define molecular/clinical profiles, with the aim of improving stratification and prediction of response, minimising adverse effects, and optimising adherence [Reference Kas, Penninx, Sommer, Serretti, Arango and Marston24, 37–40].
-
• Digital innovation and collaborative platforms. EIT Health promotes digital infrastructures, AI, and clinical decision support to accelerate reproducible research, harmonise methods, and increase representativeness – crucial for precision mental health [Reference Kelly and Young41].
-
• More advanced approaches to capture the impact of the environment. Exposome research integrates all environmental risk factors into a comprehensive, poly-environmental framework [Reference Barch42], while the growing body of Experience Sampling Method studies enables the examination of day-to-day environmental influences on mental health [Reference Guloksuz, van Os and Rutten43, Reference Myin-Germeys, Kasanova, Vaessen, Vachon, Kirtley and Viechtbauer44].
Prediction and prevention
Prediction and prevention in mental health require a clear distinction between approaches that support risk stratification and those that enable actionable preventive interventions. Advances in genomic research have improved the understanding of population-level vulnerability to mental disorders, showing that most psychiatric conditions are highly polygenic and reflect the cumulative effect of multiple genetic variants with small individual effects [Reference Mao, Lan, Liu, Guo, Wang and Lin45]. These findings have contributed to mapping shared genetic architecture across disorders, but their direct implications for prevention remain limited.
Whole genome sequencing and genome-wide association studies (GWAS) allow aggregation of genetic variants into polygenic risk scores (PRS), which estimate relative genetic liability [Reference Murray, Lin, Austin, McGrath, Hickie and Wray46]. PRS have shown potential in research settings for schizophrenia, bipolar disorder, major depressive disorder, ADHD, and autism spectrum disorders, particularly for risk stratification and the study of shared biological pathways [Reference Mao, Lan, Liu, Guo, Wang and Lin45, Reference Underwood and Hall47]. However, their clinical utility for prevention or treatment is constrained. Current PRS explain only a modest proportion of heritability (although meaningful PRS seem to emerge, for example, schizophrenia when the sample size approaches a critical size), show reduced predictive performance outside populations of European ancestry, and do not capture rare variants or dynamic biological, environmental, and social influences [Reference Murray, Lin, Austin, McGrath, Hickie and Wray46, Reference Bigdeli, Voloudakis, Barr, Gorman, Genovese and Peterson48]. Importantly, as PRS are derived from conventional diagnostic assessments (mainly DSM-based categories), which carry the heterogeneity problems mentioned above, they also capture this heterogeneity. Accordingly, PRS should be considered as complementary components of an integrated risk assessment rather than standalone tools for individual-level preventive decision-making. It remains to be established whether PRS have a larger role in prediction when diagnoses are biologically oriented rather than atheoretical.
Preventive strategies in mental health rely predominantly on identifying and modifying environmental and developmental risk factors. Environmental exposures can induce epigenetic changes affecting gene expression without altering the DNA sequence, particularly during sensitive periods of development. Perinatal hypoxia, prenatal nutrition, exposure to toxins, and stress during pregnancy have all been associated with increased risk for later mental disorders [Reference Lippard and Nemeroff17, Reference Anbalagan49, Reference Ho, Johnson, Tarapore, Janakiram, Zhang and Leung50]. These early-life factors represent critical windows for prevention, where timely interventions may reduce long-term vulnerability. High PRS might also identify individuals most susceptible to environmental risk in a stratified prevention paradigm.
Beyond early development, accumulating evidence highlights the influence of modifiable environmental and lifestyle factors across the life course. Research on the gut–brain axis suggests that alterations in microbiota composition are associated with depression and schizophrenia, implicating immune, metabolic, and neuroendocrine pathways in mental health risk [Reference Gupta, Dinesh and Sharma51]. Although causal mechanisms are still under investigation, these findings support preventive approaches targeting nutrition, physical activity, sleep, and other lifestyle-related factors [Reference Jin52, Reference Hernandez53].
Effective prevention, therefore, depends on integrating biological vulnerability with psychosocial and environmental context. Concrete prevention initiatives are already emerging within European health systems; for example, specialised clinical units integrating genetics and mental health care are now being established to support clinically healthy individuals with elevated genetic risk through tailored psychoeducation, monitoring, and early psychosocial and clinical interventions [54, 55]. Such initiatives illustrate how predictive information can be translated into proportionate, non-stigmatising preventive strategies embedded within routine healthcare.
Importantly, these integrated precision approaches are also directly relevant to suicide prevention, as suicidal behaviour often emerges from the convergence of psychiatric vulnerability, biological dysregulation (e.g., stress and inflammatory pathways), and cumulative psychosocial adversity, making it a paradigmatic outcome for multilevel risk stratification and targeted preventive interventions within a precision psychiatry paradigm [Reference Courtet and Saiz56].
Overall, prediction and prevention in precision mental health require a multilevel approach that prioritises modifiable risk factors while using genomic and biological information to inform, rather than replace, preventive action. Aligning these strategies with principles of the Precision Public Health may enable earlier identification of risk, targeted preventive interventions, and a reduction in the long-term clinical, social, and economic burden of mental disorders.
Early detection and diagnosis
Early detection is key to improving prognosis and optimising intervention effectiveness. However, current clinical practice still lacks sufficiently precise diagnostic tools for the early phases of mental disorders. Traditional classifications such as DSM-5-TR and ICD-11 are largely based on clinical observation and descriptive criteria, with limited specificity and ability to capture individual complexity, despite incremental improvements [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1, Reference Association57, 58].
In response to these limitations, transdiagnostic approaches propose studying mental disorders through shared processes and mechanisms (e.g., emotion dysregulation, impulsivity, cognitive deficits) rather than isolated diagnostic entities [Reference Oraki Kohshour and Heilbronner59]. In schizophrenia, for example, emerging approaches cluster patients using combinations of genetic, neurocognitive, and neuroimaging variables, identifying subgroups based on cognitive profiles, polygenic burden, or structural brain patterns [Reference Wolfers, Doan, Kaufmann, Alnaes, Moberget and Agartz60]. Such work supports reconceptualising schizophrenia as a set of syndromes with shared symptoms but distinct biological mechanisms. Large consortia such as ENIGMA [Reference Thompson, Stein, Medland, Hibar, Vasquez and Renteria61] and UK Biobank [Reference Sudlow, Gallacher, Allen, Beral, Burton and Danesh62] integrate genetic, clinical, and biological data from large populations to refine objective and functional diagnostic criteria, facilitating biomarker discovery and the development of more precise early detection tools [Reference González D, Alonso, Beltrán and Aparicio63].
Within this evolving diagnostic framework, advances in omics technologies are contributing to earlier detection by identifying biological signals associated with vulnerability and early disease stages. In genomics, copy number variants (CNVs), often arising from de novo mutations, affect genes critical to neurodevelopment and are more frequent in autism spectrum disorder (ASD), ADHD, and schizophrenia. Whole genome sequencing (WGS) can detect these variants even in the absence of a family history, supporting earlier diagnosis and improved phenotype characterisation. In neurodevelopmental disorders such as intellectual disability and ASD, whole exome sequencing (WES) has demonstrated a high diagnostic yield, approaching 30–40% in specialised settings, substantially exceeding that of most diagnostic tests used in other areas of medicine. De novo mutations have also been identified in adults with intellectual disability and may relate to additional psychiatric disorders [Reference Bass and Skuse64, 65]. Similarly, 22q11.2 deletion syndrome is associated with an increased risk of schizophrenia during adolescence, where early identification may enable preventive and tailored interventions [Reference Squarcione, Torti, Di Fabio and Biondi66].
Other molecular approaches are also being explored. Transcriptomic tools using peripheral blood mRNA are emerging, exemplified by the EDIT-B test, which combines RNA biomarkers and artificial intelligence algorithms to try to differentiate bipolar disorder from major depression, a clinically challenging but highly relevant diagnostic distinction [67, 68]. Epigenetic biomarkers are under investigation. BDNF gene methylation has been associated with mood disorders and response to antidepressant treatment (as prospectively studied in the P4D trial) [Reference Maier, Neyazi, Bundies, Meyer-Bockenkamp, Bleich and Pathak69], with hypermethylation linked to reduced BDNF protein levels, suggesting that methylation patterns may support early detection [Reference Alameda, Trotta, Quigley, Rodriguez, Gadelrab and Dwir70]. Methylome-wide association studies (MWAS) have preliminarily identified CpG methylation patterns that might be associated with major depression, including immune and inflammatory genes (e.g., MHC), and have enabled the development of methylation scores that, while not yet diagnostic, may represent progress toward blood-based epigenetic risk tools [Reference Shen, Barbu, Caramaschi, Arathimos, Czamara and David71].
Beyond molecular markers, functional and physiological biomarkers provide complementary information relevant to early detection. Blood lipidomic profiles and neuroimaging markers [Reference Williams72] have shown potential utility; machine-learning models (e.g., Elastic Net regression) have identified lipid-derived patterns in individuals with dual diagnoses of substance use disorder and ADHD, with a reported diagnostic capacity of approximately 72%. Structural and functional MRI studies have identified brain volume and connectivity alterations in depression, ADHD, and ASD. In depression, distinct connectivity patterns have been described between treatment-resistant depression (TRD) and non-resistant depression (nTRD), enabling more refined stratification and potentially more personalised treatment planning [Reference Sun, Lu, Shao, Han, Xia and Zheng73].
Electrophysiological methods, including EEG and MEG, can detect atypical neural activity patterns relevant to neurodevelopmental risk, particularly in preterm or low-birth-weight infants [Reference Courtet and Saiz56, Reference Association57]. Biochemical markers, such as neurotransmitters, inflammatory markers, and cortisol, may also show alterations before the onset of overt clinical symptoms [58]. In addition, eye-tracking tools can identify early attentional alterations associated with ASD risk, such as declining eye contact during infancy [Reference Jones and Klin74].
Finally, artificial intelligence is increasingly used as an integrative adjunct to early diagnosis by detecting subtle patterns across clinical, genomic, behavioural, and neurological data, including language use, sleep patterns, and daily behaviours. Natural language processing approaches can identify signals of psychological distress in clinical interviews even when symptoms are not explicitly reported, supporting earlier identification of depression, anxiety disorders, bipolar disorder, and ASD [Reference Malgaroli, Hull, Zech and Althoff75–Reference Ocando Parra77].
Treatment personalisation
Given heterogeneity, personalising both pharmacological and non-pharmacological treatments is a central pillar of precision mental health care. Individuals with the same diagnosis can respond differently to the same intervention; tailoring to genetic, neurobiological, psychological, and contextual features can increase efficacy and reduce adverse effects, advancing person-centred care. In this context, treatment personalisation aims to inform clinical decision-making by matching interventions to individual biological, psychological, and contextual profiles rather than relying on diagnosis alone.
Pharmacological treatments
A major advance in treatment personalisation is pharmacogenomics, which, in selected clinical contexts, identifies genetic profiles associated with efficacy and adverse effect risk, supporting safer and more informed prescribing decisions. Variants in cytochrome P450 genes (notably CYP2D6 and CYP2C19) influence antidepressant, antipsychotic, and mood stabiliser metabolism, determining poor/intermediate/normal/rapid/ultrarapid metaboliser phenotypes. Ultrarapid metabolisers may clear drugs before achieving therapeutic levels, while poor metabolisers may accumulate higher levels and risk-averse effects [Reference Milosavljevic, Bukvic, Pavlovic, Miljevic, Pesic and Molden78, Reference Petrovic, Pesic and Lauschke79]. Genotyping supports anticipating experience adverse reactions, optimising dosing, and selecting alternatives.
Variants affecting pharmacodynamic mechanisms are also relevant. In the serotonergic system, SLC6A4 (encoding the serotonin transporter, a target of SSRIs) polymorphisms, such as 5‑HTTLPR, influence expression and treatment response; HTR2A variants (e.g., rs6311, rs6313, rs7997012) may also influence SSRI response. Dopaminergic regulation variants, including COMT Val158Met, may affect antipsychotic response and side effects. BDNF Val66Met has also been associated with therapeutic response and clinical course. In any case, effect sizes are still too small to be individually predictive. Pharmacogenetic utility is especially relevant in complex cases with low response or unexplained side effects [Reference Fabbri and Serretti80]. However, the clinical effect sizes of most pharmacodynamic variants are modest, and their utility is greatest when integrated with clinical factors rather than used in isolation.
While many associations are not yet routine, pharmacogenetic testing is increasingly available. Inclusion of pharmacogenetic analyses has been approved in EU countries in the common service portfolio (2023), including psychiatric drugs such as tricyclic antidepressants and SSRIs [81].
Novel pathways beyond the monoamines (glutamatergic, cholinergic, endocannabinoid) are under investigation for novel treatments in schizophrenia, bipolar disorder, ADHD, and ASD [Reference Baird, Liu, Zheng, Sieberts, Perumal and Elsworth82–Reference Hill, Haney, Hillard, Karhson and Vecchiarelli86]. Precision approaches become particularly relevant when treatments with distinct mechanisms of action (MoA) are available (“when all you have is a hammer, everything looks like a nail”), and therefore, these advances call for precision prescribing to identify as soon as possible which patients may benefit most from a specific MoA [Reference Mas, Julia, Cuesta, Crespo-Facorro, Vazquez-Bourgon and Spuch87].
Inflammatory biomarkers are increasingly considered for treatment stratification. Low-grade inflammation and oxidative stress have been described in depression and first-episode psychosis, including reduced glutathione and elevated IL‑6, IL‑1β, TNF‑α, and CRP levels [Reference Fraguas, Diaz-Caneja, Ayora, Hernandez-Alvarez, Rodriguez-Quiroga and Recio39, Reference Catalan, Aymerich, Rodriguez-Sanchez, Pedruzo, Salazar de Pablo and Gil88, Reference Lindqvist, Dhabhar, James, Hough, Jain and Bersani89]. N‑acetylcysteine (a glutathione precursor) has been studied for neuroprotective effects after first-episode psychosis [Reference Romero-Miguel, Casquero-Veiga, Lamanna-Rama, Torres-Sanchez, MacDowell and Garcia-Partida90]. Meta-analyses suggest that anti-inflammatory agents (e.g., celecoxib, TNF‑α inhibitors) may improve symptoms in subgroups with elevated inflammation [Reference Gedek, Szular, Antosik, Mierzejewski and Dominiak91]. Integration of inflammatory biomarkers supports biologically informed treatment selection [Reference Carletti, Banaj, Piras and Bossu92].
Non‑pharmacological treatments
Precision approaches are also transforming non-pharmacological treatments. Precision psychotherapy aims to tailor interventions (CBT, psychoeducation, mindfulness) to personality, life history, context, social environment, and, when available, biological profiles. This collaborative model can improve efficacy, adherence, and patient experience. In obsessive-compulsive disorder, tailored CBT can achieve improvements comparable to pharmacological treatments [Reference Mathews93, Reference van der Straten, Bruin, van de Mortel, Ten Doesschate, Merkx and de Koning94].
Neuromodulation (e.g., transcranial magnetic stimulation, deep brain stimulation) targets specific circuits implicated in treatment-resistant depression, OCD, or chronic pain and can be combined with psychotherapy or pharmacological strategies to enhance individualization [Reference Krishna and Neuromodulation95].
Optogenetics, still experimental, combines genetic engineering with light stimulation to activate or inhibit neurons with high precision, enabling detailed study of circuits related to emotions, behaviour, memory, and mental illness, and potentially informing future targeted interventions [Reference Fakhoury96].
Digital technologies, virtual reality, and AI are expanding therapeutic options as adjuncts or alternatives to traditional psychotherapy, including apps, online therapy, therapeutic chats, and therapeutic videogames, which may be particularly useful for young people by matching digital habits, improving adherence, and targeting relevant psychological processes in the context where they matter [Reference Myin-Germeys, Schick, Ganslandt, Hajduk, Heretik and Van Hoyweghen97–Reference Torous, Linardon, Goldberg, Sun, Bell and Nicholas99] . Digital interventions show promise for anxiety, depression, and ADHD (including an FDA-approved therapeutic videogame). Virtual avatar-based interventions have shown effectiveness for eating disorders by addressing body image distortion in immersive environments [Reference Bruggers, Altizer, Kessler, Caldwell, Coppersmith and Warner100]. Many technologies still require rigorous validation, emphasising the need for robust studies and quality standards [Reference Marciano, Vocaj, Bekalu, La Tona, Rocchi and Viswanath101].
Lifestyle interventions are increasingly recognised as essential components of integrated mental health care. Evidence supports physical activity and nutrition as relevant adjuncts; physical activity can improve motivation, socialisation, and emotional health [Reference Hossain, Sultana, Shaik, Fan and Faizah102]. Nutrition and gut microbiota balance may influence mood and cognitive wellbeing [Reference Vernimmen103]. Lifestyle interventions should be designed and supervised by qualified professionals, may also be supported by digital and pharmacological interventions as well, and should be tailored to individual lifestyles and needs.
Treatment selection often remains trial-and-error. AI-enabled computational models using machine learning and causal inference integrate genetic, sociodemographic, brain function, and clinical data to support clinicians, predict response and adverse effects, and personalise dosing through pharmacokinetic data and patterns from electronic health records [Reference Sun, Lu, Shao, Han, Xia and Zheng73]. Clinical decision support systems are being implemented in some regions to assist prescribing and clinical management [Reference Garcia-Alonso, Almeda, Salinas-Perez, Gutierrez-Colosia, Iruin-Sanz and Salvador-Carulla104, Reference Almeda, García-Alonso and Salvador-Carulla105]. UpToDate also supports rapid access to evidence-based recommendations [106].
Monitoring and follow‑up
Technological advances support new monitoring and follow-up tools. Sensor-enabled “smart” medications can emit signals upon ingestion to objectively record dosing, supporting adherence and collaborative follow-up [107]. Rapid point-of-care biological tools can detect medication or substance presence in blood in real time, supporting dose adjustment and safety without external laboratories [Reference Torous, Linardon, Goldberg, Sun, Bell and Nicholas99].
Mobile apps, wearables, and digital tools enable continuous monitoring of behavioural, emotional, cognitive, and physiological variables (sleep, heart rate, stress), enabling early detection of decompensation, and allow for transdiagnostic clustering across individuals living with psychiatric or neurodegenerative disorders [Reference Kas, Jongs, Mennes, Penninx, Arango and van der Wee108]. Sleep alterations can anticipate relapse in bipolar disorder, depression, or psychosis. Platforms such as MONARCA integrate daily self-reports with passively collected smartphone data to support continuous monitoring in bipolar disorder [Reference Faurholt-Jepsen, Frost, Christensen, Bardram, Vinberg and Kessing109].
Telemedicine has improved follow-up by enabling video consultations, supporting adherence, early relapse detection, and access for rural or mobility-limited patients [Reference Torous, Linardon, Goldberg, Sun, Bell and Nicholas99, Reference Volpe, Eraslan, Orsolini, Fiorillo, Falkai and Gorwood110–Reference Stern, Micoulaud Franchi, Dumas, Moreira, Mouchabac and Maruani112]. Overall, these innovations support more precise and patient-centred follow-up.
Challenges
Despite substantial progress, the effective, safe, and equitable implementation of precision medicine in mental health faces persistent challenges across research, ethical and social governance, regulation, and routine clinical practice.
Research challenges
-
• Absence of comprehensive pathophysiological models. Brain complexity and marked disorder heterogeneity limit the development of valid, reproducible models that can reliably link biological mechanisms to clinical phenotypes. Emerging approaches such as organoids and humanised models represent important advances, but still cannot fully recapitulate the complexity of the human brain.
-
• Limited representativeness and diversity. Many genomic and biomarker findings are derived predominantly from populations of European ancestry, limiting generalisability and clinical applicability across diverse populations. Improving diversity in cohorts and ensuring longitudinal validation are essential for equitable translation into clinical practice.
-
• Limited sensitivity, reproducibility, and validation of biomarkers. Many proposed biomarkers show inconsistent performance across studies and populations, with modest diagnostic accuracy and limited external validation. These limitations, together with high costs and technical requirements, constrain their adoption in real-world clinical settings.
-
• Limited integration of biomarkers into conventional diagnostic systems. Current classifications, such as DSM-5-TR and ICD-11, remain largely descriptive and symptom-based, which limits the systematic incorporation of biological markers and constrains progress toward more objective and mechanism-informed diagnosis and treatment development.
-
• Insufficient research funding. Despite the high clinical, social, and economic burden of mental disorders, investment in mental health research – particularly in precision medicine – remains disproportionately low compared with other major disease areas, limiting innovation, large-scale validation, and translation into clinical practice.
-
• Equity is a central but often under-addressed challenge in precision medicine. Most biomarker, genomic, and digital psychiatry research has been conducted in high-income countries and predominantly in populations of European ancestry, limiting generalisability and potentially exacerbating existing health inequalities. Precision approaches risk benefiting primarily those populations with greater access to advanced diagnostics, digital infrastructures, and specialised care, while underserving socioeconomically disadvantaged groups and low- and middle-income settings. Ensuring equity, therefore, requires deliberate efforts to improve representativeness in research cohorts, adapt tools to diverse cultural and health-system contexts, and align precision psychiatry with principles of Precision Public Health, so that innovation contributes to reducing – rather than widening – mental health disparities.
Ethical and social challenges
-
• Persistent stigma and cultural barriers. Stigma and cultural factors continue to limit prevention, early diagnosis, and the development and uptake of innovative interventions, undermining help-seeking behaviour, research participation, and equitable access to advances in precision mental health.
-
• Risk of misinformation and pseudoscientific narratives. The spread of misleading or oversimplified information through social media and digital environments can generate confusion, trivialise mental suffering, and erode trust in scientific and clinical sources, thereby distorting public and professional perceptions of advances in precision mental health and hindering their responsible implementation.
-
• Technological development outpacing regulation. Rapid advances in artificial intelligence and digital mental health tools are exceeding existing regulatory frameworks, creating legal uncertainty, variability in standards of care, and potential inequities in access, safety, and accountability.
-
• Ethical dilemmas related to neurotechnologies. Emerging interventions such as neuromodulation, brain–computer interfaces, and optogenetics raise ethical questions regarding autonomy, informed consent, potential behaviour modification, and the boundaries of biomedical intervention, underscoring the need for transparent, proportionate, and participatory governance frameworks.
-
• Privacy and confidentiality risks. The use of genetic, clinical, and behavioural data in artificial intelligence systems raises significant challenges for data protection and confidentiality, including risks of re-identification even after pseudonymisation, which may undermine trust and limit acceptability in clinical and research settings.
Implementation challenges
-
• Limited routine implementation of genetic tools. The clinical uptake of pharmacogenomics and polygenic risk scores remains limited due to partial risk explanation, ancestry-related performance differences, and the need for specialised interpretation, infrastructure, and clinical workflows to support safe and scalable use.
-
• Limited population-level screening strategies for early detection. Beyond selected high-risk groups or advanced clinical presentations, validated screening approaches for early detection are scarce, highlighting the need for robust early markers, predictive algorithms, and evidence-based frameworks suitable for broader populations.
-
• Resistance to technology- and risk-based approaches. Hesitancy among clinicians and the public may arise from uncertainty about clinical utility, usability concerns, limited training, and fears of stigma or anxiety in asymptomatic populations, underscoring the importance of education, transparency, and ethical communication of risks and benefits.
-
• Insufficient multidisciplinary collaborative structures. Effective implementation of precision mental health is hindered by limited integration across psychiatry, clinical psychology, pharmacology, genetics, neurology, public health, bioinformatics, neuroscience, epidemiology, engineering, and social sciences, despite the inherently cross-disciplinary nature of precision approaches.
Conclusions and recommendations
Over the past decade, advances in precision medicine have begun to reshape mental health strategies across prevention, diagnosis, treatment, and follow-up, moving care toward more precise, comprehensive, and person-centred models. However, as outlined above, substantial scientific, ethical, regulatory, and implementation barriers continue to limit their safe, equitable, and large-scale integration into routine mental health care.
Ultimately, equitable implementation of precision psychiatry requires not only robust evidence and regulation but also clear and accessible communication that embeds these approaches within routine clinical care.
Addressing these challenges requires coordinated and sustained action involving clinicians, researchers, healthcare managers, policymakers, patients, caregivers, and society at large. In addition, international organisations should promote and coordinate the development of precision psychiatry initiatives. For instance, the ECNP has provided a roadmap for this [Reference Kas, Penninx, Knudsen, Cuthbert, Falkai and Sachs1], and the EPA [Reference Fiorillo113] and ECNP have decided to join forces in some of their activities in this area. Precision medicine in mental health should not be understood as a purely technological endeavour, but as a systemic transformation that integrates biological, psychological, social, and environmental dimensions of care within robust ethical and regulatory frameworks.
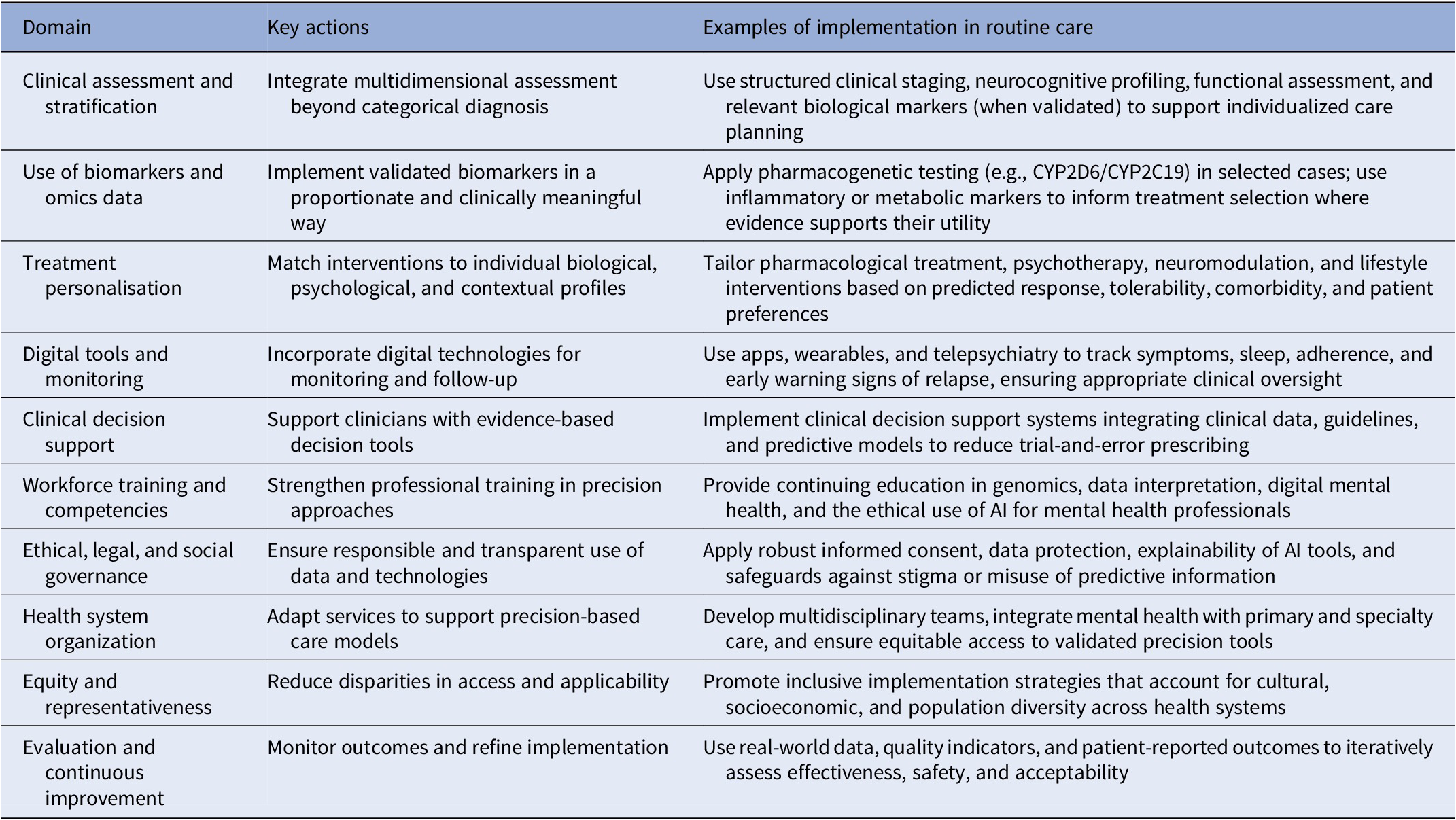
Based on the challenges identified, the following recommendations are proposed (Table 1):
-
• Increase investment in mental health research, particularly in precision medicine, to levels commensurate with the clinical, social, and economic burden of mental disorders and comparable to other major disease areas such as oncology or cardiovascular medicine.
-
• Strengthen translational research pipelines to improve understanding of brain function and the biological mechanisms underlying mental disorders, facilitating earlier detection, effective prevention, and the development of more precise and personalised therapeutic interventions, while also contributing to stigma reduction through improved biological understanding.
-
• Enhance biomarker research and clinical integration by prioritising sensitivity, reproducibility, and validation across diverse populations and care settings, and by promoting pathways for the responsible incorporation of validated biomarkers into existing diagnostic and clinical decision-making frameworks.
-
• Promote dissemination of evidence-based, accessible information for health professionals, policymakers, patients, and the public to counter misinformation, reduce stigma, and support informed and critical adoption of innovations in precision mental health.
-
• Update and harmonise ethical and regulatory frameworks governing emerging technologies in mental health, including artificial intelligence, digital tools, and neurotechnologies, ensuring robust protections for privacy and confidentiality, clear standards for informed consent, transparency in decision-making, and defined limits for biomedical intervention.
-
• Reinforce mental health as a public health priority through sustained national and regional strategies, coordination structures, and integrated action plans addressing mental health, addictions, suicide prevention, and associated social determinants.
-
• Strengthen mental health care services by supporting the implementation of validated advanced tools, including pharmacogenomics and polygenic risk scores where appropriate, and by scaling up evidence-based early detection, preventive, and predictive programmes within routine care.
-
• Expand and strengthen continuing education and training for mental health professionals in genomics, omics sciences, digital health technologies, data science, and personalised approaches, enabling critical appraisal, appropriate use, and reduced resistance to innovation.
-
• Promote multidisciplinary and cross-sector collaboration across psychiatry, clinical psychology, pharmacology, genetics, neuroscience, public health, bioinformatics, epidemiology, engineering, and social sciences to support integrated approaches spanning prediction, prevention, diagnosis, treatment, and follow-up.
Key actions for the implementation of precision psychiatry into routine clinical care

In conclusion, precision medicine offers a transformative opportunity to improve mental health care, but its potential will only be realised through deliberate, coordinated, and ethically grounded implementation. Aligning scientific innovation with clinical relevance, social responsibility, and health system readiness is essential to ensure that advances in precision mental health translate into tangible and equitable benefits for individuals and populations.
Acknowledgements
E.V. thanks the support of the Spanish Ministry of Science and Innovation (PI21/00787) integrated into the Plan Nacional de I + D + I and co-financed by the Instituto de Salud Carlos III - Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER); the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2021-SGR-01358), CERCA Programme, Generalitat de Catalunya; La Marató-TV3 Foundation grants 202234-30; the European Union Horizon 2020 research and innovation program (H2020-EU.3.1.1. – Understanding health, wellbeing and disease, H2020-EU.3.1.3. Treating and managing disease: Grant 945151, HORIZON.2.1.1 – Health throughout the Life Course: Grant 101057454 and EIT Health [EDIT-B project]).
Financial support
This work did not receive any specific funding.
Competing interests
C.A. has been a consultant to or has received honoraria or grants from Abbot, Acadia, Ambrosetti, Angelini, Biogen, BMS, Boehringer, Carnot, Gedeon Richter, Janssen Cilag, Lundbeck, Medscape, Menarini, Minerva, Otsuka, Pfizer, Roche, Rovi, Sage, Servier, Shire, Schering Plow, Sumitomo Dainippon Pharma, Sunovion, Takeda, and Teva. E.V. has received grants and served as consultant, advisor or CME speaker for the following entities: AB-Biotics, Abbott, AbbVie, Adamed, Adium, Alcediag, Angelini, Biogen, Beckley-Psytech, Biohaven, Boehringer-Ingelheim, Casen-Recordati, Celon Pharma, Compass, Dainippon Sumitomo Pharma, Esteve, Ethypharm, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, HMNC, Intra-Cellular therapies, Idorsia, Johnson & Johnson, LB pharmaceuthicals, Lundbeck, Luye Pharma, Medincell, Merck, Mitsubishi Tanabe Pharma, Newron, Novartis, Organon, Orion Corporation, Otsuka, Roche, Rovi, Sage, Sanofi-Aventis, Signant Health, Sunovion, Takeda, Teva, and Viatris, outside the submitted work. P.C. has been a consultant to or has received honoraria from Ethypharm Digital Therapy, Fondation Fondamental, Janssen Cilag, Novartis Pharma, Sothema, Viatris. L.P. reports honoraria for lectures from Johnson & Johnson and Boehringer Ingelheim, outside the submitted work. L.P. is a member of the Executive Committee of ECNP and chair of the ECNP Immuno-NeuroPsychiatry Network. A.F. has been a consultant to or has received honoraria or grants from Acadia, the Ambrosetti House, Angelini, Biogen, Boehringer, Bruno Farmaceutici, Fidia Pharmaceuticals, Johnson&Johnson, Lundbeck, Neopharmed Gentili, Neuraxpharm, Otsuka, Pfizer, Recordati, Rovi, Sage, Teva, and Viatris. A.R. has received honoraria for lectures and/or advisory boards from Janssen/Johnson & Johnson, Boehringer Ingelheim, Compass, GH Research, SAGE/Biogen, LivaNova, Medice, Shire/Takeda, Newron, MSD, AbbVie, cyclerion and Polpharma. Also, he has received research grants from Medice and Janssen. The preclinical research of M.J.H.K. is supported by a research grant from Boehringer Ingelheim. M.J.H.K. is shareholder and CSO of Behapp. P.M. has received consultation and/or speaker’s fee from Johnson&Johnson, Lundbeck, Richter Gedeon, Angelini, AstraZeneca, Teva, Krka, and Boehringer Ingelheim. B.W.J.H.P. has served on advisory panels for Johnson & Johnson, Boehringer Ingelheim, AbbVie, and Neurotorium. A.C. reports grants and personal fees from the Instituto de Salud Carlos III. She has also received research support from the Basque Government and honoraria from Janssen-Cilag, ROVI, Otsuka, Lundbeck, Viatris, and Neurotorium, all outside the submitted work. The remaining authors declare no conflicts of interest.
Use of artificial intelligence tools
Artificial intelligence–based tools were used to assist with drafting and linguistic refinement of the manuscript text (ChatGPT, OpenAI) and with the preparation of figures and graphical elements (Napkin). No data analysis, statistical modelling, or interpretation of results was performed using these tools. All content was generated, reviewed, and approved by the authors, who take full responsibility for the manuscript.

 Open access
Open access
Comments
No Comments have been published for this article.