


Highlights
-
• Survivors of aSAH have a significantly higher risk of death by suicide compared to the general population.
-
• Suicide remains a rare outcome after aSAH despite an elevated risk.
-
• The evidence base exploring psychiatric conditions after aSAH is limited, and risk factors for suicide remain unclear.
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is a devastating disease with high morbidity and mortality. The incidence of aSAH is 6.1 per 100,000 person-years and case fatality rates vary between 27% and 44%. Reference Etminan, Chang and Hackenberg1,Reference Nieuwkamp, Setz, Algra, Linn, de Rooij and Rinkel2 Among survivors only 36–55% regain functional independence. Reference Nieuwkamp, Setz, Algra, Linn, de Rooij and Rinkel2 A systematic review found that one in four aSAH survivors report depression; however, some studies report rates up to 61.7%. Reference Tang, Wang and Kwok Chu Wong3 Depression following aSAH can persist for years and reduce overall quality of life. Reference Tang, Wang and Kwok Chu Wong3 Depression can also make individuals more prone to suicide and more likely to engage in substance abuse and other high-risk behaviors. Reference Orsolini, Latini and Pompili4,Reference Pozuelo, Desborough, Stein and Cipriani5 Many neurological diseases, such as traumatic brain injury, stroke, malignant brain tumors, amyotrophic lateral sclerosis, Huntington’s disease, multiple sclerosis, concussion and epilepsy, have been associated with increased risk of death by suicide. Reference Vyas, Wang, Gao and Hackam6–Reference Fralick, Sy, Hassan, Burke, Mostofsky and Karsies10
The aim of our study was to systematically review the published literature and perform a meta-analysis quantifying the extent, if any, that aSAH is associated with death by suicide. Our secondary objective was to determine whether any patient factors, such as patient demographics or comorbidities, were associated with suicide following aSAH. The findings of this study will inform practicing neurosurgeons, neuro-intensivists, stroke neurologists, general practitioners and other clinicians involved in the subacute and chronic management of these patients.
Methods
A systematic review and meta-analysis were carried out in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Reference Page, McKenzie and Bossuyt11 MEDLINE, Embase and PsychINFO were searched for primary sources from inception until April 1, 2025, using major search terms for non-traumatic (aneurysmal) subarachnoid hemorrhage (SAH), suicide and suicidal ideation. A medical librarian assisted in the search design. Studies meeting the following criteria were included: patient age ≥ 18 years, diagnosis of intracranial aSAH, reported suicide completion rate and/or suicide attempt rate and published in English. Exclusion criteria were diagnosis of traumatic SAH, aSAH secondary to spinal aneurysm, ischemic stroke and/or intracerebral hemorrhage, patient age < 18 years, patient diagnosed with concurrent malignant disease, case report or case series with ≤5 patients and non-English language article. The prespecified study protocol was registered on PROSPERO (CRD420251035409). Three authors independently reviewed all titles and abstracts to determine eligibility, with disagreements resolved by an additional author. Three authors independently completed full-text reviews to determine study inclusion.
The following variables were extracted from each included study: authors, year of publication, study country, study period, duration of patient follow-up, patient age, patient sex, sample size, count (%) patients with death by suicide, method used to diagnosis aSAH and suicide (including International Classification of Diseases [ICD] codes), medical comorbidities, method of suicide, timing of suicide following aSAH and reported risk factors for death by suicide.
Reported count data and adjusted estimates of relative risk (RR), including respective 95% confidence intervals (CIs), were extracted from source studies, though different formats were used to report estimates of association between studies (i.e., incidence rate ratio [IRR], standardized mortality ratio [SMR]). Given the occurrence of suicide is very low, reported estimates of association, specifically IRR and SMR, were considered equivalent. Pooled RR estimates of suicide were calculated using a random-effects model using the DerSimonian and Laird method. Reference DerSimonian and Laird12 We reported a simple model adjusting for patient age, sex and year of event and a comprehensively adjusted model adjusting for patient age, sex, year of event, living status, region, socioeconomic status, physical comorbidities and psychiatric hospitalizations. We reported model heterogeneity using the I 2 statistic. The Newcastle–Ottawa Scale was used to assess the risk of bias of included studies. Reference Wells, Shea and O’Connell13
Analyses were completed using R Statistical Software version 4.4.1 (R Core Team, 2021). Significance was set a priori at p < 0.05. Data extracted from the included studies are available upon request. Approval from the University of British Columbia Ethics Review Board was not required, and there was no requirement for patient consent as this study used publicly available deidentified data. The study was performed in accordance with the Declaration of Helsinki and all other relevant ethical guidelines.
Results
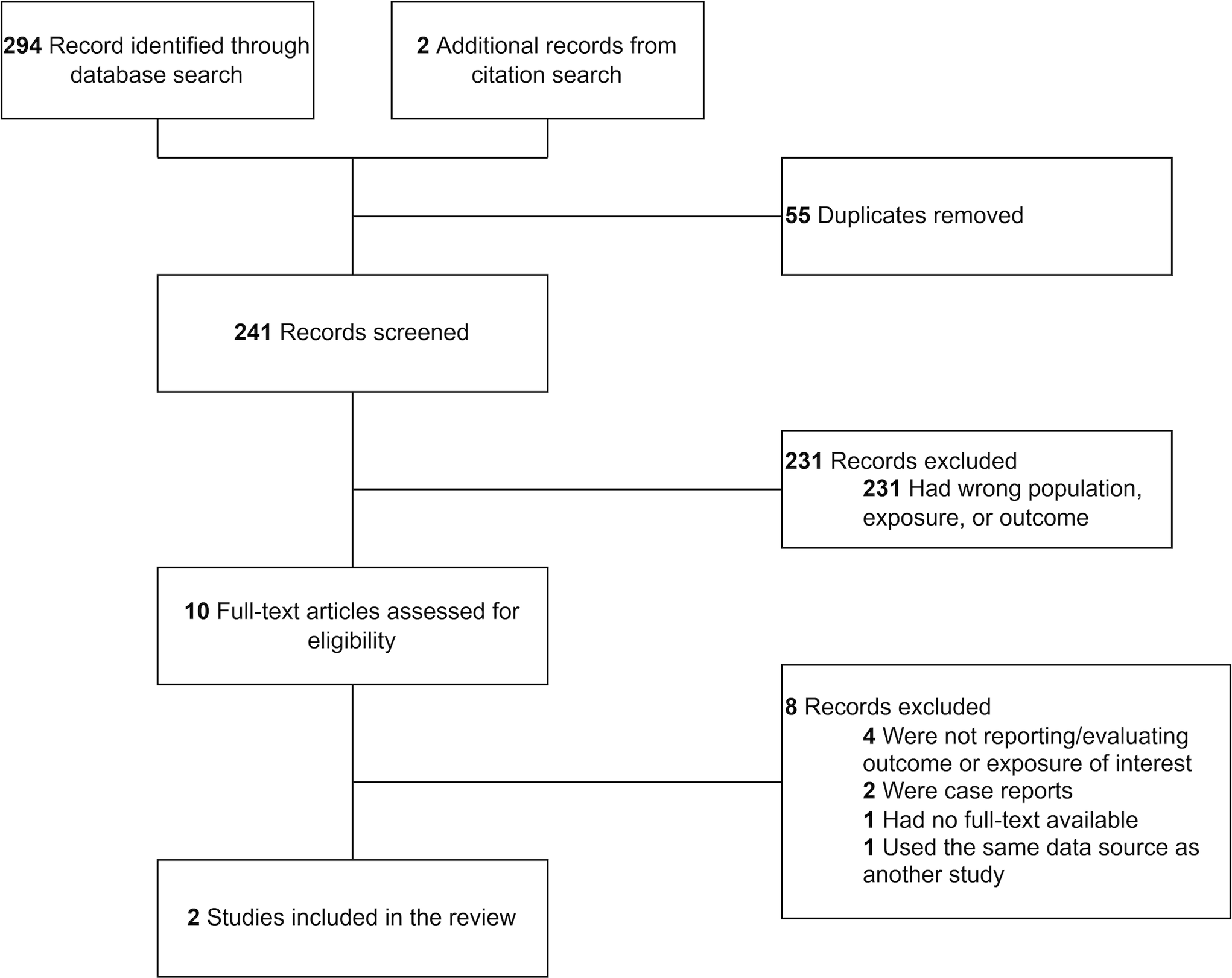
We identified 294 unique studies in our initial search, with an additional two relevant studies identified through backward and forward citation chaining (Figure 1). Once duplicates were removed, 241 abstracts were screened. Of these, 10 advanced to full-text review, and 2 studies were included in the meta-analysis. During full-text review, studies were removed for the following reasons: not reporting outcome of interest (n = 4), inappropriate study design (n = 2), source data from another study (n = 1) and no full text available (n = 1).
PRISMA diagram depicting study selection.

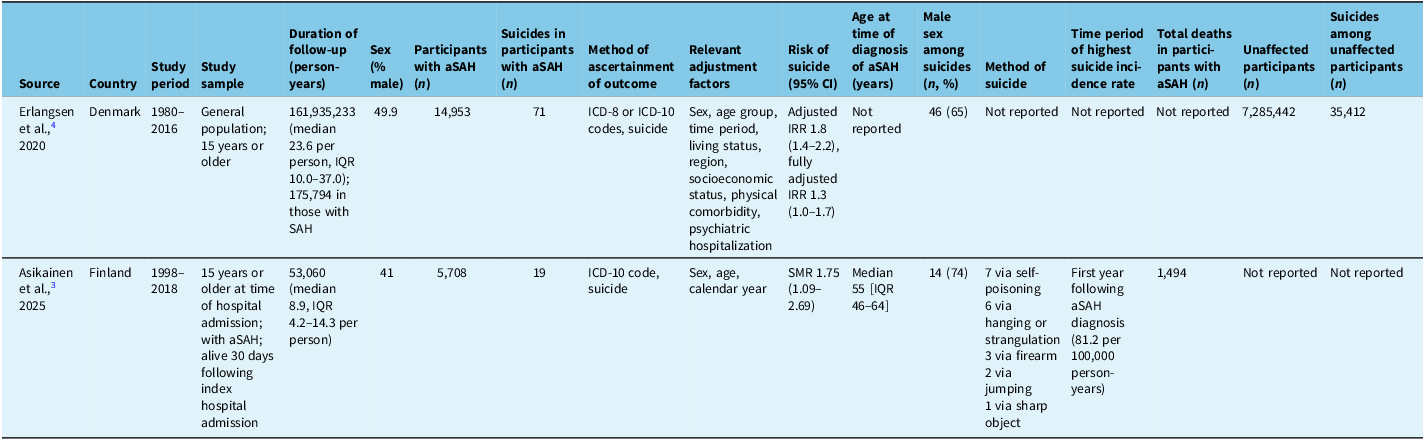
Our analysis included 20,661 aSAH survivors identified across 2 studies conducted between 1980 and 2018 in Denmark and Finland (Table 1). The median age was 55 years (IQR: 44–64) years, and 47.4% were male. Demographic data were limited to Asikainen et al.’s study. Reference Asikainen, Korja, Kaprio and Rautalin14 Total follow-up time was 228,854 person-years. Both studies were considered low bias using the revised Newcastle–Ottawa scale.
Characteristics of included studies

aSAH = aneurysmal subarachnoid hemorrhage; ICD = International Classification of Diseases; IRR = incidence rate ratio; SMR = standardized mortality ratio.
In this cohort, there were 90 deaths by suicide during the follow-up period. Suicide attempts were not reported. Suicide was more frequent in males (n = 60, 67%). Data on age at time of suicide were limited to Asikainen et al.’s study, which reported a median age at suicide of 45 years. Reference Asikainen, Korja, Kaprio and Rautalin14 In Asikainen et al.’s study, the most common reported method of suicide was self-poisoning (n = 7), followed by hanging or strangulation (n = 6) and by firearm (n = 3).
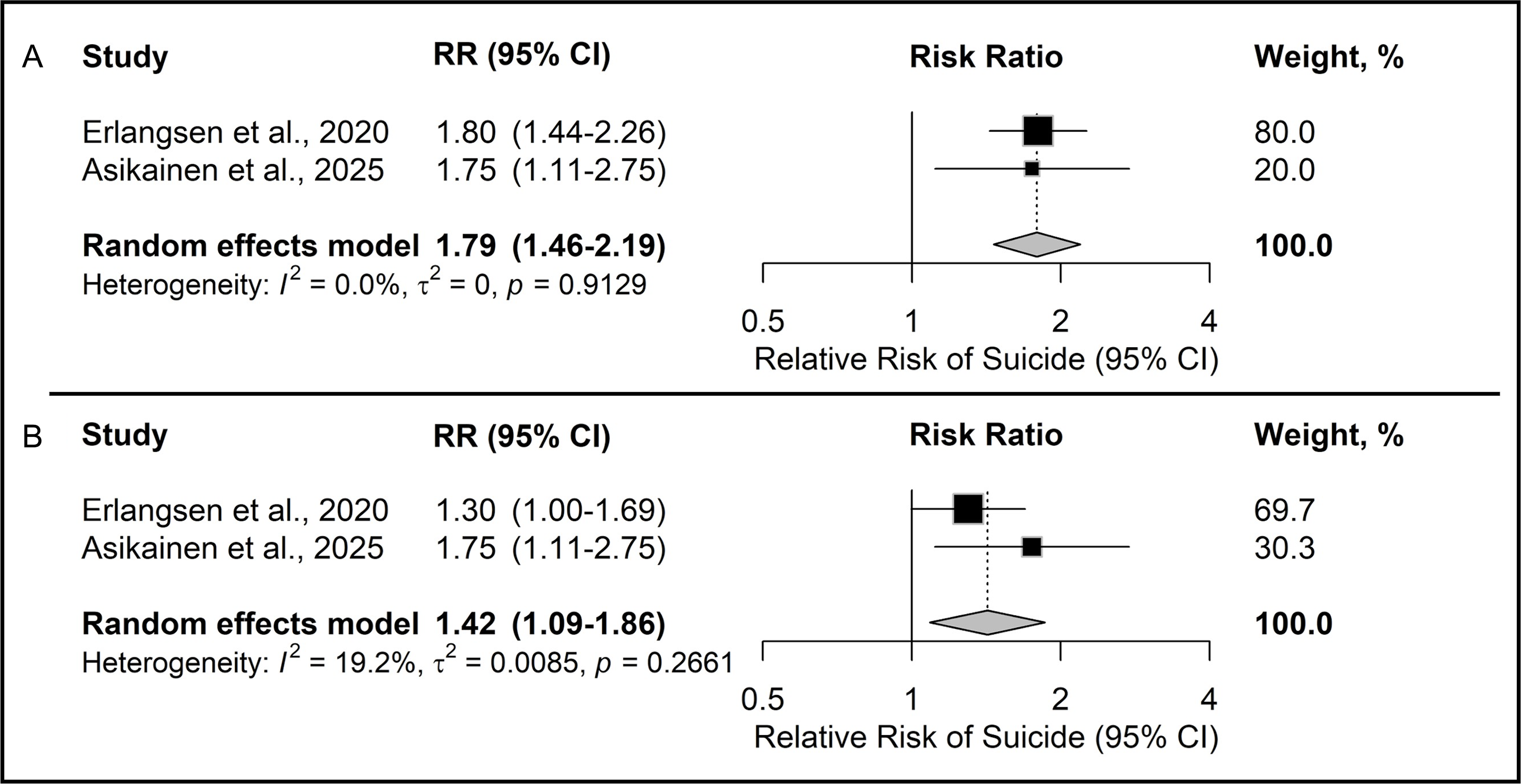
aSAH survivors had a higher risk of suicide compared to non-aSAH persons (RR = 1.79, 95% CI: 1.46–2.19, I 2 = 0%) in our simple model (p < 0.001, Figure 2A). This association persisted in the comprehensively adjusted model (RR = 1.42, 95% CI: 1.09–1.86, I 2 = 19.2%, p = 0.01, Figure 2B). Reference Erlangsen, Stenager and Conwell9 Given the limitations of the included studies, we were unable to identify any independent risk factors for suicide among aSAH patients dying by suicide. Further, rates of suicidal ideation were not reported in the included studies.
Forest plot of pooled relative risk (RR) for suicide in aneurysmal subarachnoid hemorrhage survivors after adjusting for age, sex and year of event in our simple model (A) and after adjusting for age, sex, year of event, living status, region, socioeconomic status, physical comorbidity and psychiatric hospitalization in our comprehensively adjusted model (B).

Discussion
In this systematic review and meta-analysis that included more than 20,000 aSAH survivors with over 225,000 person-years of patient follow-up, we observed that aSAH survivors are 1.8 times more likely to die by suicide than individuals without aSAH. These data were limited to two studies, reflecting a lack of literature on the topic. Despite the increased risk of suicide following aSAH, the vast majority of aSAH survivors do not die by suicide.
The magnitude of increased risk of suicide following aSAH in our study is similar to that described for other acute neurosurgical and neurological conditions such as ischemic stroke, intracerebral hemorrhage and traumatic brain injury. Reference Vyas, Wang, Gao and Hackam6,Reference Erlangsen, Stenager and Conwell9 Interestingly, higher magnitudes of relative risk of suicide are observed in degenerative neurological diseases such as Huntington’s disease, multiple sclerosis and amyotrophic lateral sclerosis. Reference Erlangsen, Stenager and Conwell9,Reference Fang, Valdimarsdóttir and Fürst15–Reference Brønnum-Hansen, Stenager, Stenager and Koch-Henriksen17 Patients with neurodegenerative diseases have a gradual decline in functional status and experience multiple losses as their disease progresses, which we postulate increases rates of depression and suicide. Reference Pinto, Geraghty, McLoughlin, Pagnini, Yardley and Dennison18 Conversely, following an acute but non-progressive life-changing event, such as aSAH, patients are more likely to accept a new life circumstance and demonstrate resilience. Nonetheless, some severely disabled stroke survivors, specifically those with modified Rankin scores of 5, report a quality of life worse than death. Reference Rebchuk, O’Neill, Szefer, Hill and Field19 We suspect that these patients have lower than expected rates of suicide because they are too functionally disabled, compared to patients with degenerative neurological diseases, to commit suicide.
Since aSAH is a form of stroke, it follows that our observed risk ratio of suicide following aSAH of 1.79 falls within the 95% CIs (RR = 1.73, 95% CI: 1.53–1.96) for suicide reported in a meta-analysis of over 2 million stroke survivors. Reference Vyas, Wang, Gao and Hackam6 The increased risk of suicide following stroke is attributed to unemployment, lost productivity and disability from the physical, cognitive and mental sequelae of stroke – all of which occur following aSAH. Reference Tang, Wang and Kwok Chu Wong3,Reference Vyas, Hackam, Silver, Laporte and Kapral20,Reference Terrill, Schwartz and Belagaje21 In both stroke and SAH, these sequelae are further compounded by depression, anxiety, fatigue and sleep disturbances. Reference Vyas, Hackam, Silver, Laporte and Kapral20,Reference Terrill, Schwartz and Belagaje21 Even young stroke survivors with excellent functional outcomes can have persistent cognitive deficits and depressive symptoms. Reference Rebchuk, Kuzmuk, Deptuck, Silverberg and Field22 Taken together, these impairments lead to an overall decreased quality of life and likely contribute to the increased risk of suicide following aSAH. Reference Tang, Wang and Kwok Chu Wong3,Reference Joundi, Adekanye and Leung23
Patients with unruptured intracranial aneurysm (UIA) also report reduced quality of life and increased psychological burden. Reference Kim, An, Kim, Lee and Yang24–Reference Ignacio, Pascual, Factor and Khu26 In patients who develop anxiety and depression following a UIA diagnosis, there is an increased rupture risk and mortality rate. Reference Essibayi, Azzam and Salim27 Patients with UIA and concurrent anxiety or mood disorders that undergo aneurysm treatment also have higher rates of perioperative morbidity and mortality, including perioperative stroke, compared to UIA patients without mood disorders. Reference Chen, Lakhani and Khunte28 In patients with mood disorders, activation of stress pathways (e.g., catecholamine surge and hypothalamic–pituitary–adrenal axis dysfunction) and elevated inflammatory markers may lead to increased rupture risk and worse clinical outcomes. Reference Emsley and Hopkins29 However, there may be a bidirectional effect wherein patients with worse outcomes have an increased risk of mood disorder. Reference Tang, Wang and Kwok Chu Wong3 Further research is necessary to better understand this complex interaction, including any potential association between UIA diagnosis and suicide.
It is important that neurosurgeons, neurologists, general practitioners and other medical practitioners involved in the care of aSAH survivors are aware of the increased risk of suicide in this population. Unfortunately, we lack a validated screening tool for depression in aSAH survivors. Reference Leung, Cartoon and Hammond30 Nonetheless, physicians involved in the care of aSAH survivors should screen for mood symptoms using a screening tool they are familiar and comfortable with. These patients may further benefit from multidisciplinary group-based support programs, which provide psychological support and facilitate rehabilitation. Reference Storey, Sheldrick, Dulhanty and Zarotti31 These multidisciplinary peer support groups can also be used to detect mood disorders in aSAH survivors. Reference Noble and Schenk32
Given the paucity of data studying the association between aSAH and suicide, future research should attempt to confirm or refute our observed association between aSAH and suicide in diverse populations. Unfortunately, answering this research question requires extensive population-level databases which are expensive to establish and maintain. Nordic countries have these databases, but this limits the external validity of their findings. Suicide does not appear to be more common in Nordic countries as data from the World Health Organization in 2024 ranks Finland’s suicide rate as 38th globally and Denmark’s as 107th. 33 Thus, it is unlikely that our observed association between suicide and aSAH is limited to Nordic countries. Future research should evaluate the effect of modifying factors like socioeconomic status, comorbidities and previous psychiatric illness on suicide rates following aSAH. Future research should also better identify the timing of suicide following aSAH to help develop targeted interventions for suicide prevention.
This study has several limitations. Given the stigma of mental health and suicide, it is possible that death by suicide was underreported. Data from included studies did not capture detailed information on potential risk factors, such as suicidal ideation, psychosocial context and temporal relationships between aSAH and suicide, making us unable to explore potential covariates on the risk of suicide following aSAH. One study reported non-traumatic SAH using ICD codes and did not subclassify based on etiology; however, we contacted the authors to verify the source data. Reference Erlangsen, Stenager and Conwell9 Lastly, our data were limited to Nordic countries with universal healthcare, limiting the external validity of our findings.
Conclusions
Compared to individuals with no history of aSAH, there is a small but significantly increased risk of suicide in aSAH survivors, yet suicide remains a rare cause of death following aSAH. There is a paucity of primary studies investigating this association, and our meta-analysis was restricted to two studies. Whether there are certain characteristics that make some patients more susceptible to the risk of suicide following aSAH remains unknown. Future research is necessary to assess modifying factors and identify the timing of suicide following aSAH to help develop targeted interventions for suicide prevention. It is important for clinicians to recognize the increased risk of suicide following aSAH and to screen appropriately for depression and suicidal ideation in these patients.
Acknowledgments
We appreciate the assistance of Dean Giustini with the research methodology.
Author contributions
ADR conceived the project, performed data analysis and interpretation and prepared and revised the original manuscript. CK performed data collection, analysis and interpretation and prepared and revised the original manuscript. MAR conceived the project and revised the original manuscript. CR performed data collection, analysis and interpretation and revised the original manuscript. BB performed data collection, analysis and interpretation and revised the original manuscript. CSH supervised the project and revised the original manuscript.
Funding statement
The authors did not receive funding or financial support for this study from any source.
Competing interests
The authors have no personal, financial or institutional interests to disclose. This study did not receive any funding or financial support.
Ethical standards
Human Ethics and Consent to Participate are not applicable given the nature of this work as a systematic review and meta-analysis. This study was performed in line with the principles of the Declaration of Helsinki. Ethics review was not required based on the policies set forth by the University of British Columbia Ethics Board. No formal consent process was required given the nature of the work.
Consent to publish
The requirement for consent ot publish was not required by the ERB due to lack of identifiable patient data.
Clinical trial number
Not applicable.

 Open access
Open access
Target article
Association Between Aneurysmal Subarachnoid Hemorrhage and Risk of Suicide: A Systematic Review and Meta-analysis
Related commentaries (1)
Reviewer Comment on Rebchuk et al. “Association Between Aneurysmal Subarachnoid Hemorrhage and Risk of Suicide: A Systematic Review and Meta-Analysis”