



Children are considered the individuals most vulnerable in any humanitarian emergency and are disproportionately affected by the destruction, instability and violence that accompany prolonged conflict. Reference Rubenstein and Stark1 The effects of armed conflict and forced displacement on children’s health, development and overall well-being have been widely documented previously. Reference Bürgin, Anagnostopoulos, Vitiello, Sukale, Schmid and Fegert2,Reference Morina, Akhtar, Barth and Schnyder3 The United Nations Convention on the Rights of the Child affirms that all children are entitled to the rights to life, health and development. Reference Nicholl4 Armed conflicts continue to impact the psychological well-being of civilian populations, particularly children and adolescents. Ongoing large-scale humanitarian crises, such as those in Palestine and Ukraine, serve as a stark reminder of the severe mental health consequences of war and displacement. Approximately 1 in 5 people (22.1%) living in conflict-affected areas suffers from a mental health disorder, including depression, anxiety, post-traumatic stress disorder (PTSD), bipolar disorder or schizophrenia. Reference Charlson, van Ommeren, Flaxman, Cornett, Whiteford and Saxena5
The war in Ukraine, for example, triggered the largest displacement of refugees and internally displaced persons since the Second World War, with millions of children forced to abandon their homes. Reference Hodes6,Reference Cai, Bai, Zheng, Zhang, Cheung and Su7 Studies have reported high rates of psychological distress among Ukrainian adolescents, with one national study finding that 35.0% screened positive for PTSD symptoms, 32.0% for moderate to severe depression and 17.9% for moderate to severe anxiety. Reference Goto, Pinchuk, Kolodezhny, Pimenova, Kano and Skokauskas8 Another study found that nearly 70% of Ukrainian children in treatment-seeking settings met DSM-5 criteria for PTSD. Reference Pfeiffer, Garbade and Sachser9 These figures far exceed pre-war estimates, Reference Martsenkovskyi, Karatzias, Hyland, Shevlin, Ben-Ezra and McElroy10 reflecting the significant escalation in psychological trauma following the conflict.
Palestinian children have witnessed the killing of civilians, bombardment of residential areas and the mutilation of bodies, leading to significant and lasting mental health consequences. Reference Thabet, Abdulla, Elhelou and Vostanis11,Reference Dimitry12 Several studies have documented alarming rates of psychological disorders in this population, including PTSD, depression, anxiety and suicidal ideation. Reference Khoodoruth, Albobali, Selmi, Ouanes, Abdelkarim and Elhassan13,Reference Khan, Khan, Albobali and Alabdulla14 A systematic review found prevalence rates for PTSD and depression among Palestinians to be far higher than global averages, with an estimated 41% of Palestinian children affected by PTSD. Reference Shukri, Holmes, Shukri, Shukri and Saada15 Similarly, another study reported a pooled PTSD prevalence of 36% among children and adolescents in Gaza and the West Bank. Reference Agbaria, Petzold, Deckert, Henschke, Veronese and Dambach16 Girls were found to be disproportionately affected, especially when their mothers also suffered from PTSD, highlighting possible transgenerational epigenetic changes, as observed in cases of famine-related malnutrition and the associated increased risk of psychiatric conditions. Reference Qouta, Punamäki and El Sarraj17–Reference Khoodoruth and Khoodoruth19
Data suggest that up to 75% of Palestinian children have witnessed people being killed by rockets, and nearly all have experienced the shelling of their homes. Reference Dimitry12,Reference Agbaria, Petzold, Deckert, Henschke, Veronese and Dambach16 As of early 2025, over 62 000 Palestinian children had reportedly been killed and more than 110 000 injured since the escalation of violence on 7 October 2023. 20 Despite the scale of need, mental health services in Gaza remain fragmented and underfunded, Reference Dabbagh, Jaber, Raboczki, Tina and Al-Uzri21 highlighting the urgent need for a coordinated, trauma-informed and culturally appropriate mental health response, supported by international organisations. Palestinian children represent a highly minoritised and politically marginalised group, both within their homeland and in host countries, a reality that compounds the psychological impact of trauma and limits access to adequate care. This growing body of global research emphasises the enduring psychiatric consequences of armed conflict in young populations. Addressing these issues requires context-specific assessment tools, multidisciplinary interventions and sustainable mental health infrastructure.
On 9 December 2023, the first group of injured Palestinian children and their families arrived in Doha as part of a national programme aimed at sponsoring 3000 orphans and providing medical treatment to 1500 injured individuals. 22 This initiative builds on Qatar’s previous efforts in delivering comprehensive mental health and psychosocial support to displaced Afghan refugees. Reference Khan, Khan and Alabdulla23 The response includes primary medical care, trauma-informed psychiatric and psychological interventions and community-based psychosocial services, delivered by multidisciplinary teams. This type of host country initiative can be seen as a counter-model to systems that reinforce marginalisation, offering instead a culturally relevant and rights-based approach to care.
This pioneering cross-sectional study investigates the mental health status of displaced Palestinian children and adolescents now residing in Qatar. Specifically, it aims to estimate the prevalence of elevated post-traumatic stress symptoms among this population. By utilising validated assessment tools and involving parents and caregivers, this research further examines how key demographic and situational resilience factors, such as age, gender and perceived family support, may be associated with the severity of PTSD symptoms. The findings are intended to inform culturally sensitive, evidence-based interventions and policy responses. Moreover, this work contributes to the broader call for system-level reform by documenting how structural determinants, including displacement, political marginalisation and inequality, manifest in the mental health profiles of refugee children and adolescents
Method
Design, participants and setting
This cross-sectional study was carried out in the designated Palestinian refugee compound in Al Thumama, Qatar, established for individuals displaced from Gaza following initiation of the conflict. Participants were recruited exclusively from this setting. A total of 350 children were recruited using convenience sampling.
Eligible participants were Palestinian children and adolescents aged between 8 and 18 years and who had relocated to Qatar from Gaza following the events of 7 October 2023. Inclusion required that participants had the cognitive capacity to understand and complete the self-report questionnaires. Informed, written consent was obtained from parents or legal guardians, and written assent was obtained from the participants. Exclusion criteria included individuals outside the specified age range, non-Palestinian children, those residing in Qatar before the conflict, participants for whom informed consent was not granted and individuals with cognitive impairments preventing effective participation. As compensation, each participant received a grocery voucher for 50 Qatari Riyal (QAR, approximately US$13).
Measures
The study employed the following self-report instruments:
-
(a) The Child PTSD Symptom Scale – Self-Report Version for DSM-5 (CPSS-5-SR). This instrument is designed to assess PTSD symptoms in children and adolescents aged 8–18 years, based on DSM-5 diagnostic criteria. Reference Foa, Asnaani, Zang, Capaldi and Yeh24 It evaluates symptom frequency over the past month and includes three subscales reflecting cognitive, emotional/psychological and behavioural symptoms. CPSS-5-SR comprises 20 items that evaluate symptom frequency over the past month, aligning with DSM-5 criteria, and is an update of the original CPSS, Reference Foa, Johnson, Feeny and Treadwell25 which was based on DSM-IV and assessed symptoms over 2 weeks. Initial psychometric validation of CPSS was conducted among child survivors of the Northridge earthquake Reference Foa, Johnson, Feeny and Treadwell25 and adolescent survivors of sexual assault, Reference Gillihan, Aderka, Conklin, Capaldi and Foa26,Reference Rachamim, Helpman, Foa, Aderka and Gilboa-Schechtman27 demonstrating good internal consistency, test–retest reliability and convergent validity. CPSS-5-SR has similarly shown excellent internal consistency and test–retest reliability, as well as good convergent and discriminant validity in both interview and self-report formats. Reference Foa, Asnaani, Zang, Capaldi and Yeh24 The Arabic version used in this study has demonstrated acceptable internal consistency, with reliability coefficients of 0.73 for cognitive symptoms, 0.63 for emotional/psychological symptoms, 0.60 for behavioural symptoms and 0.78 for total score. Overall, the Arabic CPSS-5-SR is a valid and reliable instrument for assessment of PTSD symptoms among Arabic-speaking children and adolescents. Reference al-Ammar, Attal and Ismail28
-
(b) The Demographic and Resilience Questionnaire. The study utilised a structured Demographic and Resilience Questionnaire to gather essential background and contextual information from participants. This tool was designed to explore key demographic characteristics and situational factors related to displacement and trauma exposure, as well as potential indicators of resilience. The questionnaire was originally compiled in English by experienced Child and Adolescent Mental Health Services (UK) psychiatrists fluent in both English and Arabic. It was subsequently translated into Arabic and then reverse-translated by separate bilingual colleagues, to ensure linguistic accuracy and preserve contextual meaning. To confirm clarity and cultural appropriateness, the tool was piloted with five participants, and the results indicated no need for adjustments.
The questionnaire captured data on age, gender, educational background, displacement-related injuries, current living arrangements, pre-war social support and exposure to traumatic events such as being witness to death or bombings. These variables were selected specifically to examine potential associations with the severity of post-traumatic stress symptoms reported by participants. The format was structured to support systematic analysis, while also ensuring that the content remained culturally relevant and easily understood by Arabic-speaking children and adolescents.
Ethical standards
The study was reviewed and approved by the Institutional Review Board (IRB) of Hamad Medical Corporation (IRB no. MRC-01-24-256). The research was conducted in accordance with the ethical principles of the Declaration of Helsinki. Informed consent was obtained from the parents or legal guardians of all participants before enrolment. The nature and purpose of the research were explained in detail, including the voluntary nature of participation and the right to withdraw at any point without consequence. In addition to parental consent, age-appropriate assent was sought from each child participant according to ethical standards for research involving minors.
Participants were assured that their responses would remain confidential. No personally identifiable data were collected or linked to questionnaire responses. All data were anonymised using serial codes. These measures ensured that participants’ privacy and confidentiality were fully maintained throughout the study. Potential risks associated with participation, including psychological discomfort related to the trauma-related questions, were communicated to caregivers. Provisions were made to refer participants to mental health support services if distress arose during data collection.
Sample size determination and statistical analysis
Based on recent literature, Reference Agbaria, Petzold, Deckert, Henschke, Veronese and Dambach16 the reported prevalence of elevated symptoms of anxiety and PTSD among displaced children and adolescents ranged between 25 and 35%. For this study, an expected prevalence of 30% was used to determine sample size. With a precision level of 5% and a 95% confidence interval, the required sample size was calculated to be 350 participants.
Sample size was computed using the standard formula:
n = [Z 21 − α/2 × P(1 − P)]/d 2. In this formula, n represents the required sample size, Z is the z-statistic corresponding to the chosen confidence level (1.96 for 95%), α denotes the significance level (probability of a Type I error), P is the expected prevalence (0.30) and d is the desired precision (0.05). This sample size was considered sufficient to yield reliable estimates of the prevalence of elevated PTSD symptoms in the study population.
Statistical analysis was conducted using IBM SPSS Statistics version 26 for Windows (IBM Corp., Armonk, New York, USA; https://www.ibm.com/products/spss-statistics). Descriptive statistics were computed for all relevant variables. For categorical variables we reported absolute and relative frequencies as well as 95% confidence intervals (for the prevalence of PTSD). For continuous variables we calculated the mean, standard deviation and 95% confidence intervals of the mean.
To examine factors associated with PTSD symptoms, we conducted a multiple linear regression analysis using the CPSS-5 score as the dependent variable. Independent variables included age; gender; formal education; physical injury due to war; currently living with a parent; living with parents before the war; having witnessed the death of a first- or second-degree relative in Gaza; having witnessed the death of any person in Gaza; bombing in their local area; and length of exposure to the war in Gaza ≥3 months.
For each of these multiple linear regression models we determined the unstandardised regression coefficients (B), 95% confidence intervals, partial coefficients (r) and P-values. Multiple linear regression assumptions (including linearity, normality of residuals, homoscedasticity and the absence of multicollinearity) were checked.
The defined significance level α was 0.05.
Results
In this study, we found that children and adolescents exposed to the Gaza conflict had experienced extremely high rates of trauma exposure and PTSD symptoms, with intrusion and arousal symptoms most prominent. The presence of negative cognitive and mood alterations further emphasised the complexity and severity of their psychological distress.
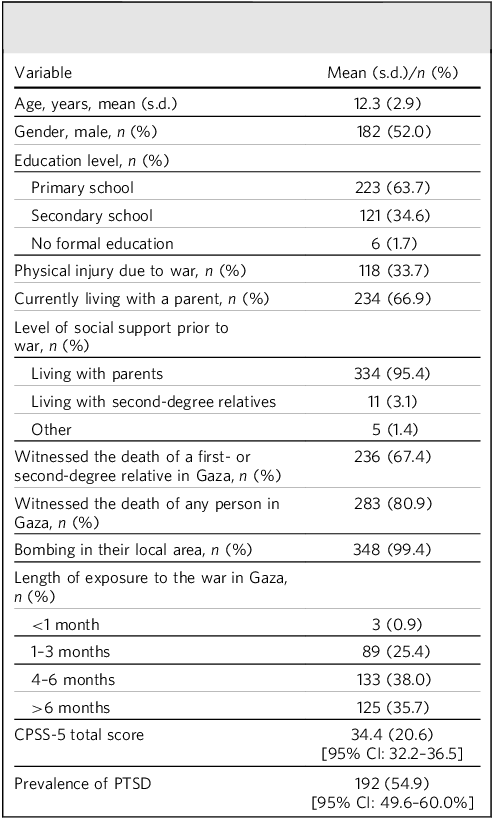
A total of 350 children and adolescents aged between 8 and 18 years were included in the study, with a mean age of 12.3 years (s.d. = 2.9). The gender distribution was nearly equal, with 52% males (n = 182) and 48% females (n = 168), indicating a well-balanced gender representation in the sample. The vast majority (98.3%, n = 344) had access to formal education before the conflict. Most children (95.4%, n = 334) lived with their parents before the war but, at the time of data collection, this figure had fallen to 66.9% (n = 234). A third of participants (33.7%, n = 118) had sustained a physical injury during the war.
War-related trauma exposure was near universal among the 350 participants. Almost all respondents (99.4%, n = 348) reported experiencing bombing in their local area. A large majority (80.9%, n = 283) had witnessed at least one death during the Gaza conflict, and 67.4% (n = 236) had specifically witnessed the death of a first- or second-degree relative. Most participants (>90%) had been exposed to war for longer than 1 month (Table 1).
Sociodemographic characteristics, PTSD scores and its prevalence among participants

PTSD, post-traumatic stress disorder; CPSS-5, Child PTSD Symptom Scale for DSM-5.
Scores on CPSS-5 ranged from 0 to 80, with a mean total symptom severity score of 34.4 (s.d. = 20.6). Using a clinical cut-off score of ≥31, 54.9% of participants (n = 192; 95% CI: 49.6–60.0%) met the threshold for probable PTSD. Analysis of CPSS-5 symptom clusters indicated that avoidance and intrusion had the highest average scores among participants, whereas changes in cognition and mood and increased arousal and reactivity had comparatively lower scores (Fig. 1).
Boxplots of Child PTSD Symptom Scale for DSM-5 (CPSS-5) subscale scores among war-displaced individuals. All scores are expressed in terms of percentage of the maximum possible score (to allow comparison between subscales with different theoretical maximum scores).

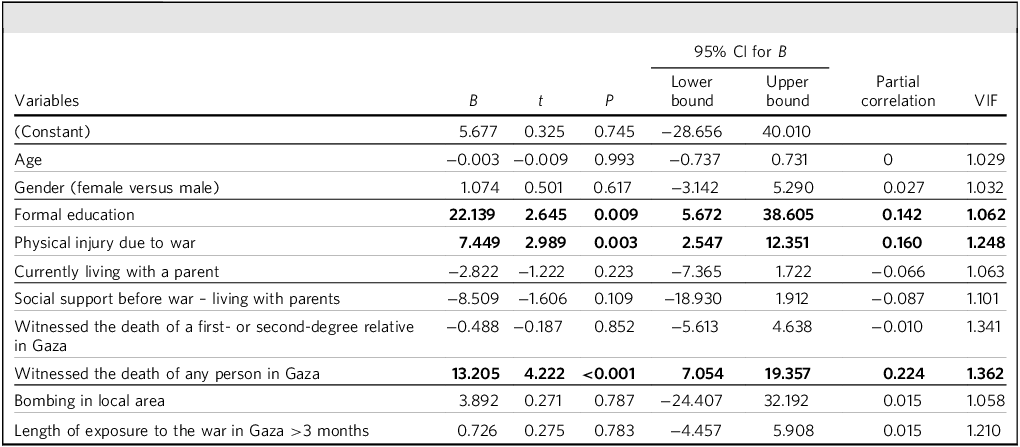
Further statistical analysis identified key factors associated with greater PTSD symptom severity (Table 2). Participants currently receiving formal education had significantly higher PTSD scores (B = 22.139, 95% CI: 5.672–38.605, P = 0.009, r = 0.142). Physical injury during the war was also linked to higher PTSD symptoms (B = 7.449, 95% CI: 2.547–12.351, P = 0.003, r = 0.160). Witnessing the death of any person in Gaza, particularly close relatives, was strongly associated with increased PTSD severity (B = 13.205, 95% CI: 7.054–19.357, P < 0.0001, r = 0.224).
Multiple linear regression analysis: factors associated with PTSD symptoms

PTSD, post-traumatic stress disorder; VIF, variance inflation factor.
Model: R 2 = 0.113, adjusted R 2 = 0.087, P < 0.001.
Bold type indicates statistically significant findings.
Discussion
Our findings reveal a high prevalence of PTSD symptoms among children and adolescents affected by the conflict in Gaza, with 54.9% of participants meeting the threshold. This rate is notably higher than the prevalence among youth in post-conflict populations. Reference Catani, Jacob, Schauer, Kohila and Neuner29,Reference Klasen, Oettingen, Daniels, Post, Hoyer and Adam30 This increased prevalence reflects the intense trauma exposure and limited access to psychological support in this conflict, pointing to the substantial mental health burden. These findings are consistent with previous research demonstrating that cumulative and prolonged trauma exposure is strongly associated with elevated PTSD risk in children and adolescents. Reference Thabet, Abed and Vostanis31,Reference Saltzman, Pynoos, Layne, Steinberg and Aisenberg32 Recent data from Ukraine, where similarly high rates of PTSD symptoms were identified among conflict-displaced adolescents, are comparable to our work. Reference Lushchak, Velykodna, Bolman, Strilbytska, Berezovskyi and Storey33 This highlights the growing global recognition that war trauma leads to complex and enduring psychiatric morbidity, even after children have been relocated to safer environments.
Intrusion levels and arousal symptoms were elevated, and this is in line with neurobiological models of PTSD demonstrating hyperactivation of fear circuits, leading to persistent re-experiencing, hypervigilance and sleep disturbances. Reference Perry, Pollard, Blakley, Baker and Vigilante34,Reference Carrion and Wong35 The high frequency of avoidance and negative cognitive symptoms, such as diminished interest and feelings of estrangement, indicates a broad impact on emotional regulation and social functioning of the affected children. These symptoms may impair developmental trajectories in social and academic domains in the future, Reference Cohen, Mannarino and Deblinger36 reinforcing the need for comprehensive interventions addressing not only core PTSD symptoms but also affective and cognitive sequelae, as well as future functioning levels.
Our analysis identified formal education, physical injury and being witness to death as key predictors of increased PTSD symptom severity. The relationship between education and PTSD symptoms may reflect the dual impact of disrupted schooling and increased psychosocial stressors associated with maintaining academic progress under conflict conditions. Pain and physical trauma may contribute to psychological symptoms beyond PTSD, with physical injury associated with elevated general distress and arousal. Reference Amir and Sol37 Being witness to the death of any person in Gaza was strongly associated with increased PTSD severity in this study. Whereas being witness to the death of a relative was not found to be statistically significant in this study, in contrast to some existing research, Reference Melhem, Porta, Shamseddeen, Payne and Brent38 the experience can lead to ‘traumatic bereavement’, in which trauma-related symptoms impede the natural grieving process, increasing vulnerability to both PTSD and prolonged grief disorder. Reference Cohen, Mannarino and Deblinger36,39
Although several predictors in the multiple linear regression analysis reached statistical significance (Table 2), the overall explained variance (R 2) remained modest. PTSD symptoms are influenced by certain factors that were outside the scope of this study, including previous mental health issues, coping styles, family circumstances and ongoing stressors. Because these influences were not measured, the regression model can account for only a limited share of the variability in symptom scores. The research population also had broadly similar levels of exposure, which reduces variability and makes strong predictive values less likely.
Growing research evidence confirms the positive role of psychological interventions in reducing PTSD symptoms in children and adolescents exposed to war-related trauma, particularly in developing countries. Teaching Recovery Techniques (TRT), a structured, cognitive–behavioural therapy (CBT)-informed, low-cost and scalable intervention, Reference Yule, Dyregrov, Raundalen and Smith40 can be delivered by trained non-specialists. TRT has been implemented in diverse settings including Gaza Reference Qouta, Palosaari, Diab and Punamäki41 and the West Bank Reference Barron, Abdallah and Heltne42 and has consistently shown clinical and statistical benefits. One systematic review found TRT to be the only programme yielding significant PTSD reduction in the Middle East, Reference Alzaghoul, McKinlay and Archer43 with another meta-analysis confirming its group-level benefits globally. Reference Davis, Meiser-Stedman, Afzal, Devaney, Halligan and Lofthouse44
Trauma-Focused Cognitive–Behavioural Therapy (TF-CBT) has been adapted to help children cope with a wide range of traumatic experiences, including physical or emotional abuse or neglect, domestic or community violence, traumatic loss, war and natural disasters. TF-CBT is a structured, conjoint parent–child intervention that employs cognitive–behavioural principles and exposure techniques to treat trauma-related conditions. A comprehensive review of studies performed between 1995 and 2013 found high-quality evidence from 10 randomised clinical trials supporting its effectiveness in reducing PTSD symptoms in children, although its impact on depression and behaviour problems was less consistent. Reference de Arellano, Lyman, Jobe-Shields, George, Dougherty and Daniels45
To mitigate the pervasive impact of bereavement, mental health interventions should also integrate group counselling and family support. Reference Alkhazaleh, Alharbi and Abojedi46 In parallel, trauma-/grief-focused group psychotherapy programmes, such as those used with war-exposed Bosnian adolescents, have shown promising results in reducing PTSD, depression and grief symptoms, and in improving psychosocial adaptation. Reference Layne, Pynoos, Saltzman, Arslanagić, Black and Savjak47 Similarly, community- and school-based programmes can offer scalable platforms for mental health promotion and resilience-building, especially when the availability of specialist services is limited. Reference Tol, Barbui, Galappatti, Silove, Betancourt and Souza48
Here, it must be pointed out that the prevalence of PTSD among children still resident in Gaza is probably much higher than that reported in this study. Children who are still living under the conflict face a longer duration of trauma exposure, ongoing unsafe environments and a continuous struggle to meet their basic needs. Furthermore, implementing any treatment modalities in Gaza currently poses significant challenges, including the risk of re-traumatisation, a severe lack of human resources and unreliable internet connectivity, which can make remote therapy or supervision even more challenging. These factors demonstrate the immense difficulties involved in providing adequate mental health support within the region.
Strengths and limitations
This study offers the most up-to-date insights into the psychological impact of the ongoing conflict on Palestinian children and adolescents and is, to our knowledge, the first and the largest clinical study of displaced Palestinian youth conducted during the current crisis. One of the major strengths of this work is that it focuses on a highly vulnerable and under-researched population. By targeting this specific group, the study addresses a significant gap in current mental health research and provides timely insights into the psychological impact of war and displacement on children and adolescents in the region. The use of validated, standardised questionnaires to assess symptoms of PTSD ensures that the data collected will be reliable and comparable with those from other studies around the globe.
Another strength of this research is its generalisability. Because it was conducted in a defined refugee setting, with focused recruitment and access to a representative sample of the displaced population, it allows for extension of the findings to similar contexts. The structured environment also reduces variation linked to external service differences, helping to ensure that the responses reflect the broader impact of conflict and displacement rather than features unique to the setting. Moreover, the participants shared key characteristics with displaced Palestinian children elsewhere, including comparable patterns of exposure, disruption and cultural background. The inclusion of a broad age range of children (aged 8–18 years) also enabled the exploration of symptoms in a developmentally wide range of children and young people. Furthermore, the study considers several demographic and situational variables, such as family support and gender, to explore their relationship with mental health outcomes. This comprehensive approach not only helps to identify risk factors but also shows potential protective factors that may be important for designing effective psychosocial support programmes.
Despite its many strengths, the study does have several limitations that are worth mentioning. The cross-sectional design restricts conclusions about symptom progression or long-term outcomes. Due to the reliance on self- or caregiver-report measures, there remains a risk of reporting bias. Although the study sample probably reflects the majority of displaced Palestinian children in Qatar, it may not capture the experiences of those outside this system. Furthermore, access to relatively stable living conditions, including healthcare, education, accommodation and nutrition, may itself be a mitigating factor against the psychological impact.
Conclusions about causality are hard to draw because there is no control group. Nevertheless, findings from a recent longitudinal study of war-affected Ukrainian adolescents Reference Skrypnyk, Martsenkovsky and Martsenkovska49 indicate that rates of PTSD and comorbid conditions can increase over time following trauma exposure. This highlights the need for continued monitoring and support, because initial presentations may underestimate the longer-term mental health burden. Future longitudinal research is required to provide deeper insight into symptom trajectories and protective factors.
Future directions
As shown by the high prevalence and severity of PTSD symptoms in this study, there is a clear need for further longitudinal research to better understand the long-term mental health trajectories of displaced Palestinian children and adolescents. Future studies could incorporate follow-up assessments at multiple time points to evaluate the persistence, fluctuation or resolution of symptoms over time. Longitudinal designs can also allow for the identification of predictive factors for recovery versus chronicity, providing crucial information for early identification of those at greatest risk. Such research can assess not only PTSD, but also the emergence of comorbid conditions such as depression, anxiety and functional impairment in academic and social settings. Besides, the inclusion of biological or psychophysiological markers of stress, where feasible, may further enrich our knowledge of trauma responses in this population.
Another important direction is in regard to intervention development and evaluation. Although the findings support the potential utility of existing evidence-based approaches such as TRT, TF-CBT and Eye Movement Desensitisation and Reprocessing, Reference Morena-Alcázar, Treen, Valiente-Gómez, Sio-Eroles, Perez and Amann50 culturally adapted and contextually relevant models of care are essential. Future work should explore how these interventions can be effectively integrated into community- and school-based settings within the host country, and whether hybrid models, i.e. combining elements of individual-, group- and family-based approaches, offer enhanced benefits. Research should also focus on implementation science aspects, including training of non-specialist providers, scalability, cost-effectiveness and engagement strategies tailored to refugee populations. It is also necessary that service models must be informed by the voices and preferences of children, families and frontline workers to ensure the involvement of all stakeholders. Finally, given the broader regional and global context, comparative studies involving other conflict-displaced youth populations could help delineate shared versus population-specific factors influencing PTSD outcomes. Cross-national collaborations could support the development of adaptable frameworks for early mental health intervention in humanitarian emergencies, with an emphasis on prevention, resilience-building and continuity of care for children and young people in prolonged displacement.
About the authors
Yasser Saeed Khan is a senior child and adolescent psychiatrist at Hamad Medical Corporation, Doha, Qatar, clinical associate professor at the College of Medicine, Qatar University, Qatar, and chair of the RCPsych Middle Eastern Division. Abdul Waheed Khan is an associate consultant psychiatrist at Hamad Medical Corporation, Doha, Qatar. Mohamed Adil Shah Khoodoruth was a clinical fellow at Hamad Medical Corporation at the time the work was carried out, and is currently affiliated with the Division of Child & Adolescent Psychiatry, Schulich School of Medicine and Dentistry, Western University, Canada. Olfa Selmi is a clinical fellow in child and adolescent psychiatry at Hamad Medical Corporation, Doha, Qatar. Sami Ouanes is a consultant psychiatrist at the MindWell Centre, Kuwait. Yahia Albobali is a specialist child and adolescent psychiatrist at Hamad Medical Corporation, Doha, Qatar, and clinical assistant professor at College of Medicine, Qatar University, Qatar. Marwan Abdelkarim Ali Abdelkarim is a physician assistant at Hamad Medical Corporation, Doha, Qatar. Areeg Hassan Mohamed Elhassan is a physician assistant at Hamad Medical Corporation, Doha, Qatar. Menatalla Abdelkader is a fellow in geriatric psychiatry at Hamad Medical Corporation, Doha, Qatar. Taieb Turki is a psychologist at Hamad Medical Corporation, Doha, Qatar. Ahmed Abdelhakim Ahmed Elzok is a charge nurse in the Mental Health Service, Hamad Medical Corporation, Doha, Qatar. Majid Alabdulla is chairman and senior consultant psychiatrist in the Mental Health Service, Hamad Medical Corporation, Doha, Qatar, and clinical professor of psychiatry at the College of Medicine, Qatar University.
Data availability
The data that support the findings of this study are not publicly available due to ethical and privacy restrictions. Anonymised data may be made available from the corresponding author subject to the necessary approvals.
Acknowledgements
We thank Fawziah Kassim Al-Ammar and Bothaina Ahmed Attal for kindly providing us with the Arabic version of the CPSS-5 questionnaire, and for granting permission for its use in our study. We thank all participants and their families for participating in this study.
Author contributions
Y.S.K.: conceptualisation, data curation, formal analysis, methodology, writing – original draft. A.W.K.: conceptualisation, data curation, methodology, writing – original draft. M.A.S.K.: methodology, data collection, writing – review and editing. O.S.: conceptualisation, data collection, methodology. S.O.: data curation, data analysis, writing – review and editing. Y.A.: conceptualisation, data collection, methodology. M.A.A.A.: data collection. A.H.M.E.: data collection. M. Abdelkader: data collection. T.T.: data collection. A.A.A.E.: data collection. M. Alabdulla: conceptualisation, supervision. All authors contributed to manuscript revision and have read and approved the submitted version.
Funding
We acknowledge the Medical Research Centre at Hamad Medical Corporation for providing funding to cover the cost of 50 QAR grocery vouchers given to each participant as a token of appreciation. Qatar National Library funded the open access publication of this article.
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.