


The reintegration of people with severe mental illness (SMI) back into society following incarceration presents significant challenges for the people concerned, correctional systems, mental health service providers and society as a whole. Following their release, these individuals encounter many challenges including stigma, homelessness, unemployment and difficulty accessing adequate mental health services. Reference Lamb and Weinberger1,Reference Baillargeon, Hoge and Penn2 Without appropriate assistance, they are at an elevated risk of mental health deterioration, hospital admission, recidivism and re-incarceration. Reference Fazel and Yu3
Given the complexity of reintegration tasks (including a complex interplay of intrapersonal, interpersonal, institutional and community-level factors), specialised reintegration programmes have been developed that coordinate interventions across these domains to achieve successful outcomes. Reference Mourão, Sousa, Ferreira, Gonçalves, Caridade and Cunha4 Such programmes can contain facilitated access to healthcare and addiction services, assistance with social supports such as housing, financial support and employment. Reference Osher, Steadman and Barr5,Reference Abracen, Gallo, Looman and Goodwill6 However, the effectiveness of such interventions for people with SMI is unclear given the variability in interventions and mixed results reported in the literature.
A meta-analysis by Martin et al found that interventions targeting justice-involved individuals with mental disorders reduced criminal justice involvement, although the overall effect size was small with only modest improvements reported in mental health symptoms and functioning of participants. Reference Martin, Dorken, Wamboldt and Wootten7 Hopkin et al found that reintegration programmes can improve contact with mental health services, but the impact on re-incarceration is complex, and it can paradoxically lead to increased re-incarceration. Reference Hopkin, Evans-Lacko, Forrester, Shaw and Thornicroft8
Persons with SMI transitioning into the community face significant physical health challenges such as increased risk of hepatitis C, cirrhosis and diabetes. These conditions, combined with other issues such as accidental overdose and increased risk of suicide, make this population particularly vulnerable to adverse outcomes and heightened risk of death within the first 2 weeks after release. Reference Haas, Walter and Bailey9–Reference Brinkley-Rubinstein, Sivaraman, Rosen, Cloud, Junker and Proescholdbell11 Successful reintegration entails collaboration between several agencies to ensure continuous support during this critical transition juncture. Reference Hartwell and Orr12
This updated systematic review aims to provide a comprehensive synthesis of reintegration studies for individuals with SMI transitioning into the community from correctional settings. Unlike previous reviews that were limited in scope Reference Martin, Dorken, Wamboldt and Wootten7 or did not include the most recently published studies, Reference Hopkin, Evans-Lacko, Forrester, Shaw and Thornicroft8 this review broadens the search to include multiple academic databases and grey literature. This review attempts to identify effective practices, highlight existing knowledge gaps and inform future directions for research, policy and service development in correctional mental healthcare.
Method
This systematic review adheres to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Statement. Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow13 A protocol was developed and registered with PROSPERO (identifier: CRD42022299983) on 4 February 2022. Reference Adamo, Simpson, Jones, Gerritsen, Tagore and Groat14
Information sources and search strategy
A search strategy was developed in conjunction with a medical librarian (R.B.). We searched Ovid Medline, Ovid PsycINFO, Ovid EMBASE, Ebsco CINAHL, ProQuest’s Applied Social Sciences Index and Abstracts (ASSIA), Ebsco Criminal Justice Abstracts and Cochrane CENTRAL, from inception until the end of November 2025. No search filters or limits were applied to the search strategy. The complete search syntax for all databases searched is provided in Supplementary Appendix A. Grey literature – including dissertations and conference abstracts – was identified via database searches and targeted screening of key Canadian and American government agencies (federal, state and provincial) to capture emerging research. This search focused on organisations specialising in justice, corrections, public safety, social service, mental health and re-entry services. All identified materials were screened using the same inclusion and exclusion criteria applied to peer-reviewed literature.
Eligibility criteria
Inclusion and exclusion criteria for this review were structured using the Population, Intervention, Comparison, Outcome and Study (PICOS) Framework. The population of interest included adults (≥18 years) who were in a correctional environment (prisons, jails or detention centres), specifically those with an SMI who were released into the community under any conditions following any period or form of incarceration. Excluded populations were youth and adolescents, individuals found not criminally responsible or unfit to stand trial, those in psychiatric hospitals (including hospitals embedded within correctional systems) and populations without SMI symptoms, e.g. those with intellectual disabilities, sex offenders or those with only personality or substance misuse disorders.
Interventions considered were psychological, pharmacological, social work or other mental health interventions that commenced within correctional settings and aimed to improve mental health outcomes after release, such as reducing symptoms, improving functioning or lowering rates of re-incarceration. Interventions that commenced only after release were excluded. Those targeting concurrent disorders (e.g. substance use and mental health) were included if mental health outcomes were primary. Diversion programmes, like mental health courts, were also included. Comparisons included any design with or without a control group, such as pre–post studies, case-matched controls, or treatment-as-usual (TAU). Outcomes of interest were broad and included symptoms of SMI, psychological distress, well-being, healthcare utilisation, treatment adherence and motivation, social functioning, and rates of re-offence or re-incarceration, with any measures of effect accepted.
Eligible study designs included randomised controlled trials (RCTs), quasi-experimental, cohort, case–control, cross-sectional, case and brief reports with data, qualitative studies with data and opinion pieces with data, provided they were available in English or translated. Systematic reviews, meta-analyses, literature reviews and scoping reviews were excluded. Commentaries, editorials and opinion pieces without data were also excluded.
Study selection, data collection process and data synthesis
We imported references into Covidence (a web-based collaboration software platform that streamlines the production of systematic and other literature reviews) and duplicates were automatically removed. Two independent reviewers (V.A. and M.K.) screened titles and abstracts before full-text screening. Any conflicts between the two reviewers that arose were communicated to a senior scientist (A.I.F.S., C.G. or R.M.J.), who resolved these and provided the final decision. A fifth of all included studies, those that made it to the full-text review stage, were also reviewed by the senior scientists to ensure reliability; the scientists and reviewers were in agreement.
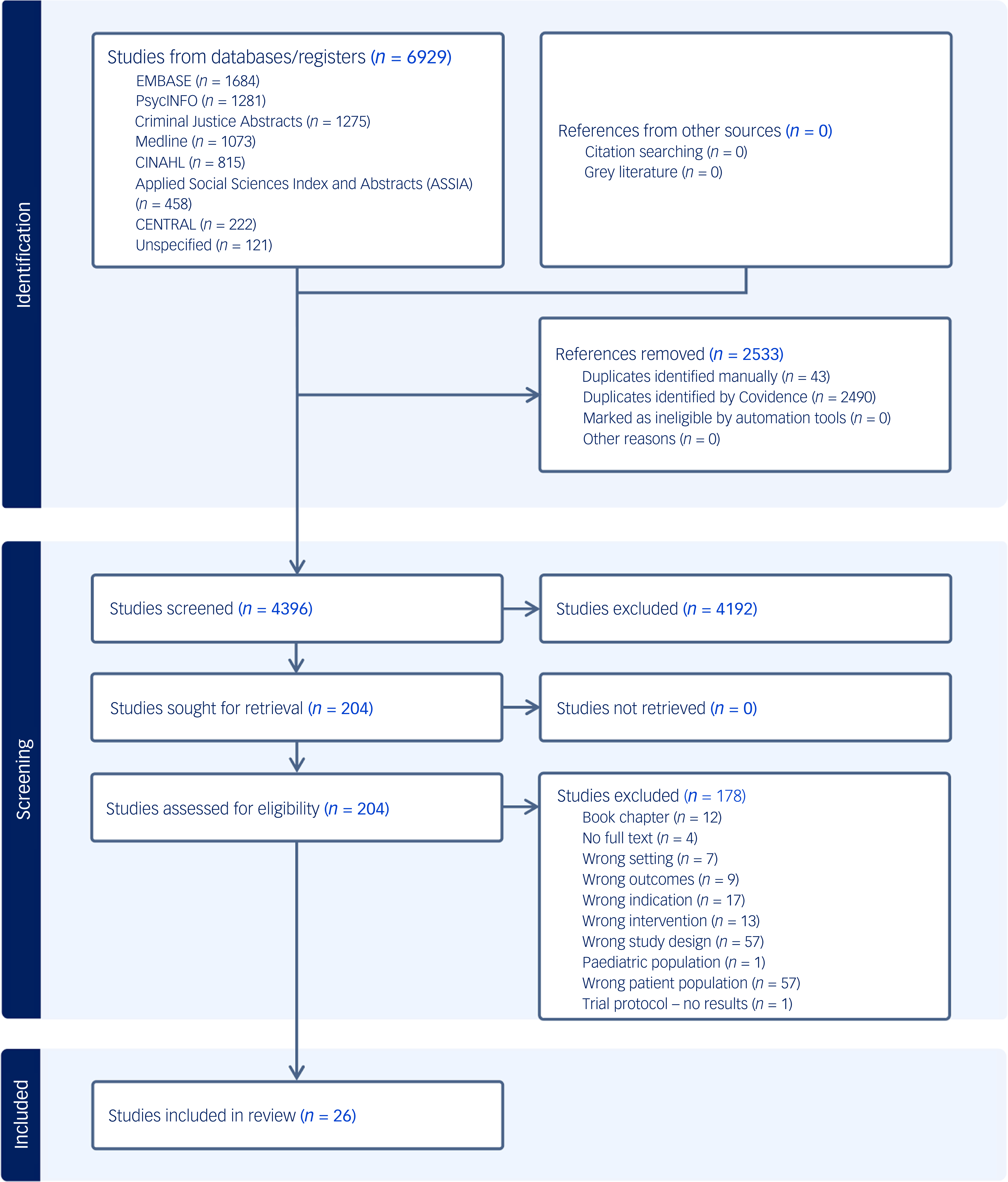
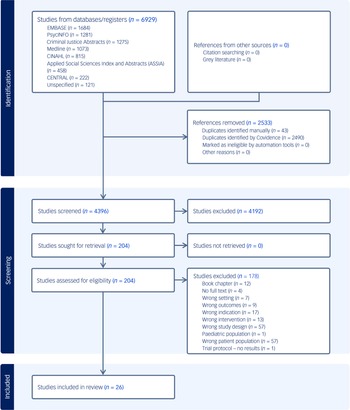
Full-text screening was independently conducted by two reviewers (V.A. and M.K.). Any conflicts that arose during this phase were resolved by a senior scientist (A.I.F.S., C.G. or R.M.J). After the full-text screening phase concluded, data extraction using standardised data extraction forms first commenced on 8 February 2024, after the original search. Data extraction was conducted independently, in duplicate, by two reviewers (V.A. and M.K.). Any conflicts that arose during the extraction process were resolved through discussion between the pair, and if consensus could not be reached, a senior scientist (A.I.F.S., C.G. or R.M.J.) was consulted to provide a final decision. An updated search was conducted through 10 January 2026. Title and abstract screening as well as full-text screening following the updated search was conducted by three reviewers (M.U.W., A.W. (independent reviewer) or C.P. (independent reviewer)), with two votes being needed for study inclusion or exclusion. Any conflicts that arose were resolved after discussion with a senior scientist (A.I.F.S. or R.M.J.). No new studies met the eligibility criteria to proceed to the data extraction phase following the updated search. The screening process is summarised in the PRISMA flow diagram (Fig. 1).
Preferred Reporting Items for Systematic Review and Meta-Analyses flow diagram.
Study risk-of-bias assessment
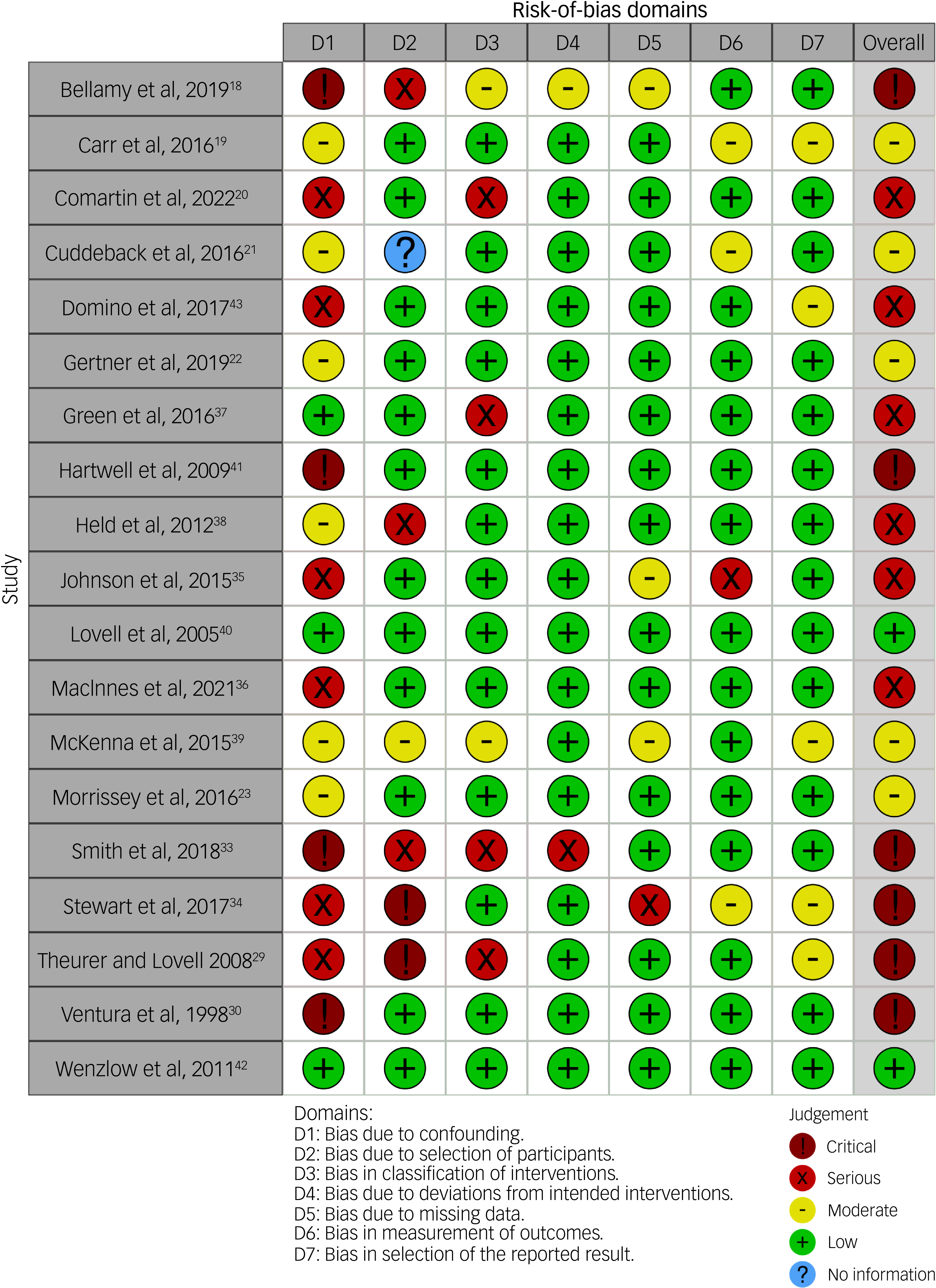
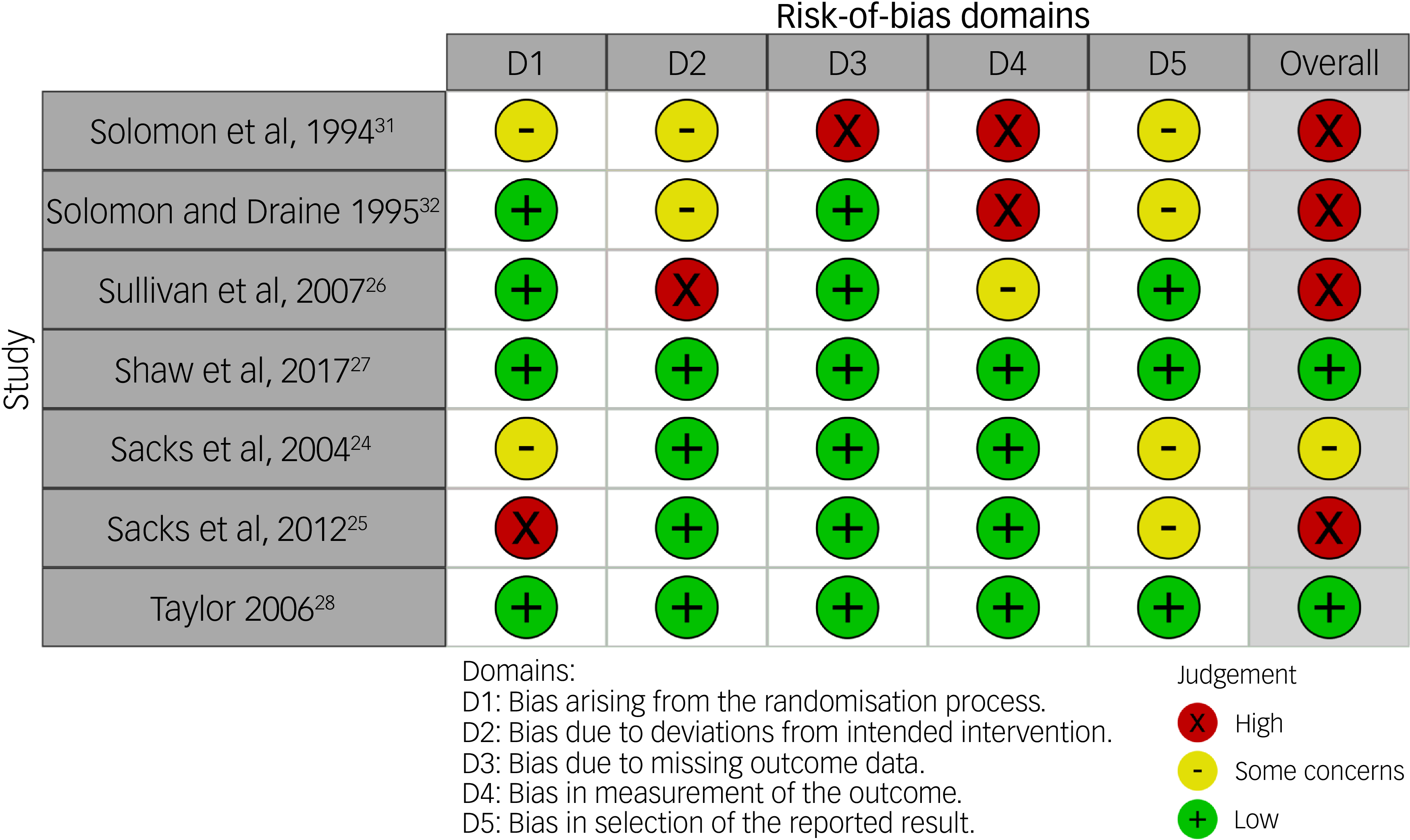
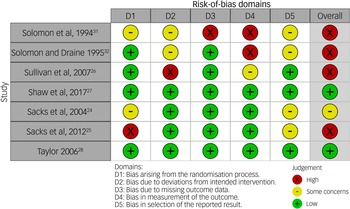
The Risk of Bias in Non-randomised Studies of Interventions (ROBINS-I) was used to evaluate risk of bias in non-randomised intervention studies; this tool has seven domains: confounding, participant selection, intervention classification, deviations from intended interventions, missing outcome data, outcome measurement and selective reporting of results. Reference Sterne, Hernan, Reeves, Savovic, Berkman and Viswanathan15 The Cochrane Risk of Bias Tool (RoB 2) was used to evaluate risk of bias in RCTs, and includes five domains: randomisation, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of the reported results. Reference Sterne, Savovic, Page, Elbers, Blencowe and Boutron16 Risk of bias was assessed for each article by one junior reviewer (V.A., M.K. or M.U.W.) and independently by one senior scientist (A.I.F.S., C.G. or R.M.J.); any differences that arose were resolved through discussion between the pair. Risk of bias plots were generated using the robvis tool. Reference McGuinness and Higgins17
Results
Study selection and characteristics
We identified 6929 studies, of which 2533 were duplicates, leaving 4396 studies. Following eligibility screening, 26 studies were deemed eligible for inclusion, from which we extracted data. Most of the included studies were from the USA (n = 21), followed by the UK (n = 2), and one each from Australia, Ireland and New Zealand. The median number of patients involved in these studies was 207 (range: 22–3086). Eleven studies were longitudinal, seven were RCTs, three had an AB design, two were quasi-experimental, two were retrospective and one was a brief report. Figures 2 and 3 report the risk of bias scores for each individual study. The results of the ROBINS-I tool assessments indicate varying levels of bias risk across non-RCT studies (Fig. 2); somewhat similar results were obtained using the RoB 2 tool for RCTs included in the review (Fig. 3).
Risk-of-bias assessments for non-randomised controlled trials, using the Risk of Bias in Non-randomised Studies of Interventions tool.
Risk of bias assessments for randomised controlled trials, using the Cochrane Risk of Bias Tool.
Study findings and outcomes
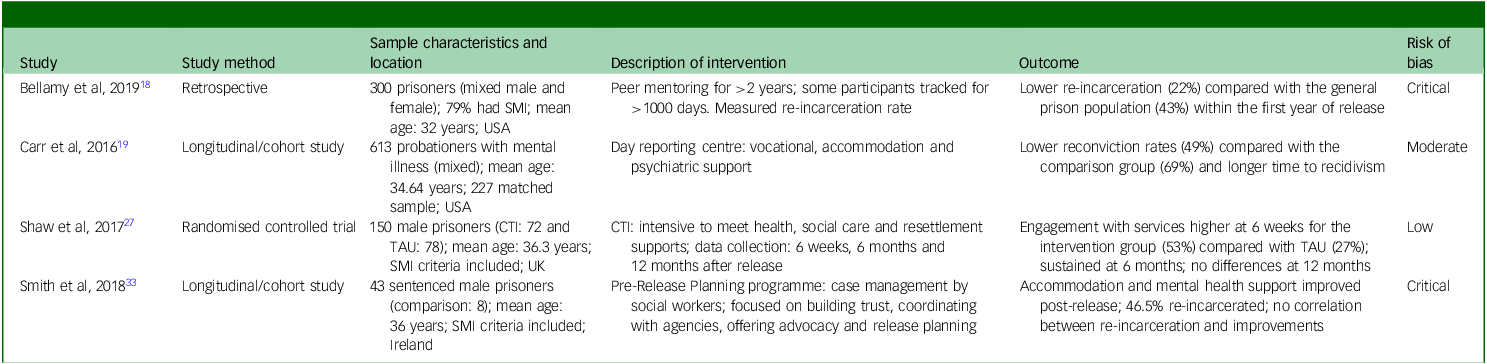
Tables 1–3 summarise the studies of community reintegration programmes for released prisoners with SMI. The interventions used encompassed peer support, Reference Bellamy, Kimmel, Costa, Tsai, Nulton and Nulton18 day reporting centres, Reference Carr, Baker and Cassidy19 pre- and post-release mental health services, Reference Comartin, Burgess-Proctor, Hicks, Putans and Kubiak20 expedited Medicaid enrolment, Reference Cuddeback, Morrissey and Domino21–Reference Morrissey, Domino and Cuddeback23 modified therapeutic communities, Reference Sacks, Sacks, McKendrick, Banks and Stommel24–Reference Sullivan, Sacks, McKendrick, Banks, Sacks and Stommel26 critical time intervention method, Reference Shaw, Conover, Herman, Jarrett, Leese and McCrone27 intensive case management Reference Taylor28,Reference Theurer and Lovell29 and community-based teams. Reference Ventura, Cassel, Jacoby and Huang30–Reference Smith, Harnett, Flanagan, Hennessy, Gill and Quigley33 Evaluations of different interventions highlighted variable degrees of success in terms of the outcomes measured, which were recidivism, enrolment in and engagement with mental health services, psychiatric symptoms and social functioning.
Community support service interventions
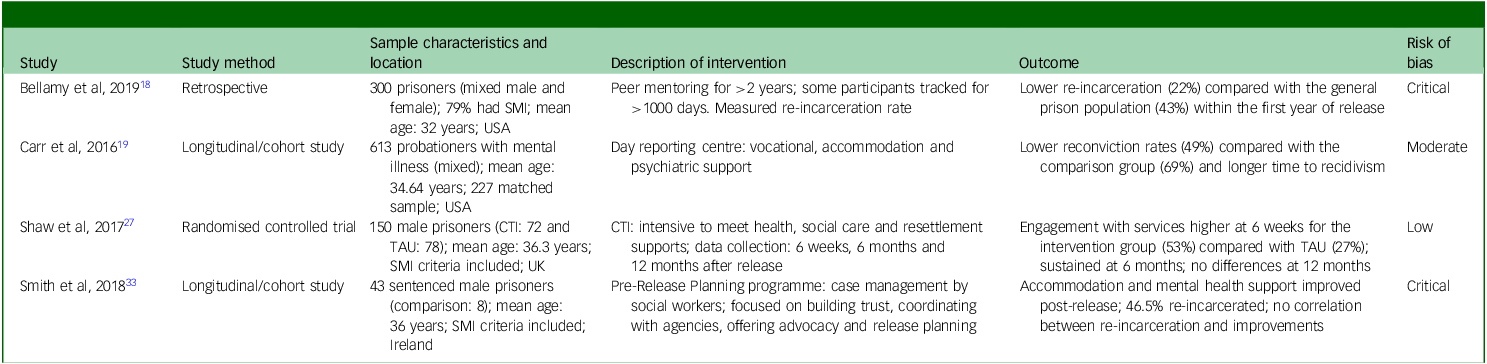
Table 1 Long description
A table summarizing studies on community reintegration programs for released prisoners with SMI. The table has 4 rows and 5 columns. Column headers are Study, Study method, Sample characteristics and location, Description of intervention, Outcome, and Risk of bias. Row 1: Study: Bellamy et al, 2019; Study method: Retrospective; Sample characteristics and location: 300 prisoners (mixed male and female); 79 percent had SMI; mean age: 32 years; USA; Description of intervention: Peer mentoring for greater than 2 years; some participants tracked for greater than 1000 days. Measured re-incarceration rate; Outcome: Lower re-incarceration (22 percent) compared with the general prison population (43 percent) within the first year of release; Risk of bias: Critical. Row 2: Study: Carr et al, 2016; Study method: Longitudinal/cohort study; Sample characteristics and location: 613 probationers with mental illness (mixed); mean age: 34.64 years; 227 matched sample; USA; Description of intervention: Day reporting centre; vocational, accommodation and psychiatric support; Outcome: Lower reconviction rates (49 percent) compared with the comparison group (69 percent) and longer time to recidivism; Risk of bias: Moderate. Row 3: Study: Shaw et al, 2017; Study method: Randomised controlled trial; Sample characteristics and location: 150 male prisoners (CTI: 72 and TAU: 78); mean age: 36.3 years; SMI criteria included; UK; Description of intervention: CTI: intensive to meet health, social care and resettlement supports; data collection: 6 weeks, 6 months and 12 months after release; Outcome: Engagement with services higher at 6 weeks for the intervention group (53 percent) compared with TAU (27 percent); sustained at 6 months; no differences at 12 months. Accommodation and mental health support improved post-release; 46.5 percent re-incarcerated, no correlation between re-incarceration and improvements; Risk of bias: Low. Row 4: Study: Smith et al, 2018; Study method: Longitudinal/cohort study; Sample characteristics and location: 43 sentenced male prisoners (intervention: 8; mean age: 36 years; SMI criteria included; Ireland; Description of intervention: Pre-Release Planning programme: case management by social workers; focused on building trust, coordinating with agencies, offering advocacy and release planning; Outcome: Not specified; Risk of bias: Critical.
SMI, severe mental illness; CTI, Critical time intervention; TAU, treatment as usual.
Community mental health service interventions
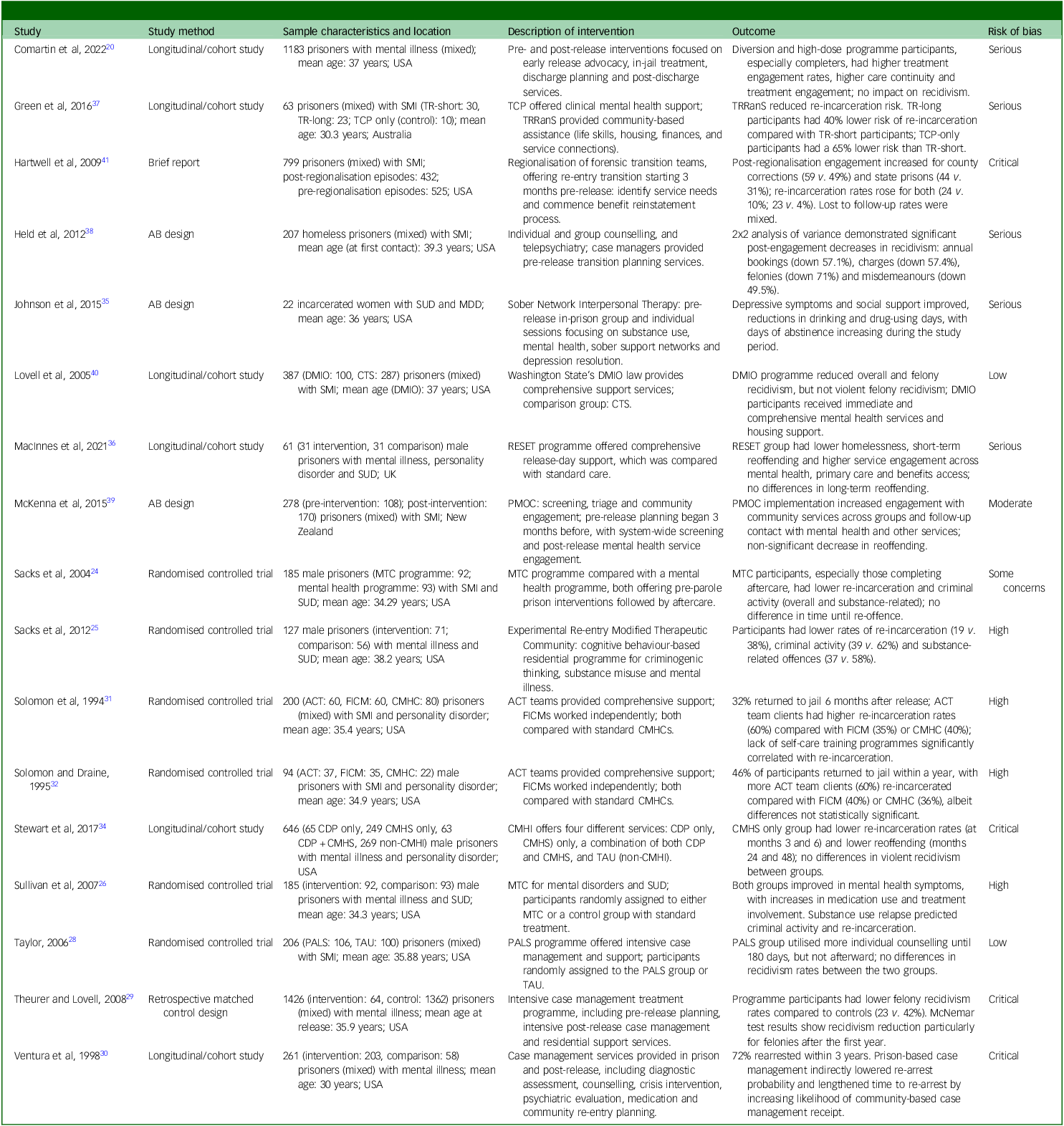
TR-short, short periods (<62 days); TR-long, longer periods (>62 days); SMI, severe mental illness; TCP, Transitional Coordination Programme; TRRanS, Transition Reintegration Recovery and Support; SUD, substance use disorder; MDD, major depressive disorder; DMIO, Dangerous Mentally Ill Offender; CTS, Community Transition Study; RESET, RESETle programme; PMOC, Prison Model of Care; MTC, Modified Therapeutic Community; ACT, assertive community treatment; FICM, forensic individual case manager; CMHC, community mental health centre; CDP, clinical discharge planning; CMHS, community mental health service; CMHI, Community Mental Health Initiative; TAU, treatment as usual; PALS, Providing Assistance with Linkage to Services.
Health insurance access-related interventions
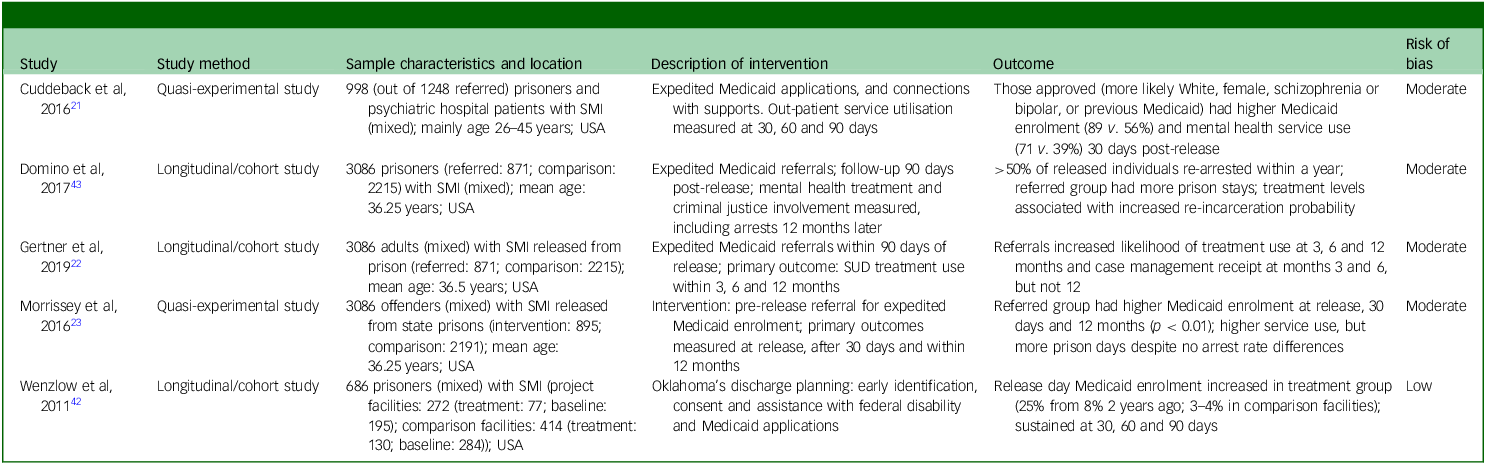
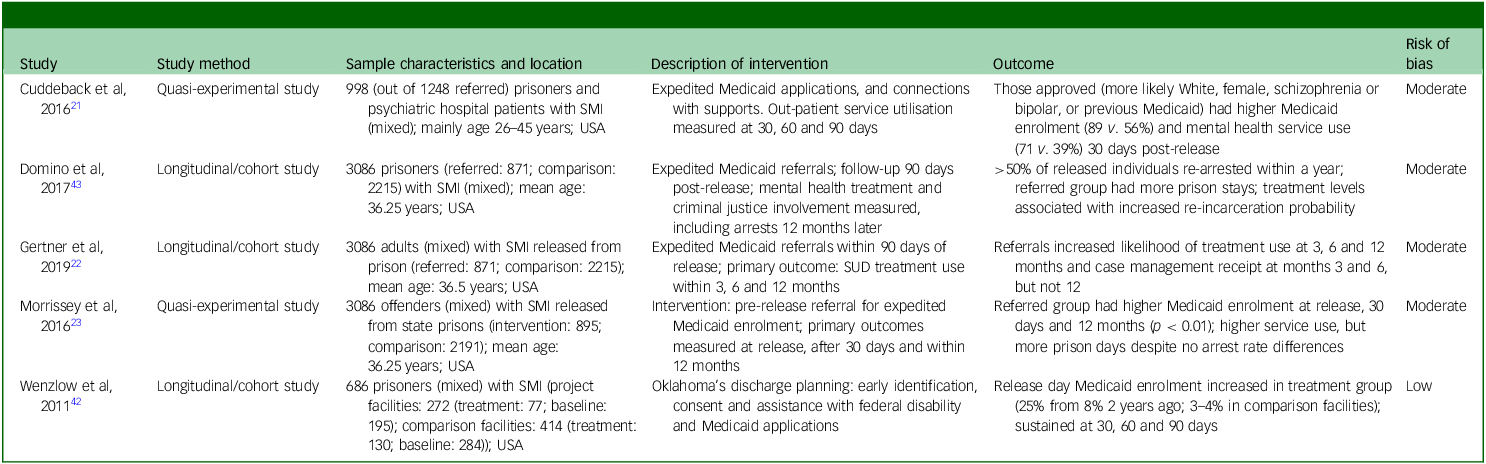
Table 3 Long description
A table summarizing studies on community reintegration programs for released prisoners with SMI. The table has six columns: Study, Study method, Sample characteristics and location, Description of intervention, Outcome, and Risk of bias. It contains multiple rows with specific details for each study. Row 1: Study: Cuddeback et al, 2016; Study method: Quasi-experimental study; Sample characteristics and location: 998 (out of 1248 referred) prisoners and psychiatric hospital patients with SMI (mixed); mainly age 26-45 years; USA; Description of intervention: Expected Medicaid applications, and connections with supports. Out-patient service utilisation measured at 30, 60 and 90 days; Outcome: Those approved (more likely White, female, schizophrenia or bipolar, or previous Medicaid) had higher Medicaid enrolment (89 vs. 56%) and mental health service use (71 vs. 39%) 30 days post-release; Risk of bias: Moderate. Row 2: Study: Domino et al, 2017; Study method: Longitudinal/cohort study; Sample characteristics and location: 3086 prisoners (referred: 871; comparison: 2215) with SMI (mixed); mean age: 36.25 years; USA; Description of intervention: Expedited Medicaid referrals; follow-up 90 days post-release; mental health treatment and criminal justice involvement measured, including arrest 12 months later; Outcome: >50% of released individuals re-arrested within a year; referred group had more prison stays; treatment levels associated with increased re-incarceration probability; Risk of bias: Moderate. Row 3: Study: Gernter et al, 2019; Study method: Longitudinal/cohort study; Sample characteristics and location: 3086 adults (mixed) with SMI released from prison (referred: 871; comparison: 2215); mean age: 36.5 years; USA; Description of intervention: Expedited Medicaid referrals within 90 days of release; primary outcome: SUD treatment use within 3, 6 and 12 months; Outcome: Referrals increased likelihood of treatment use at 3, 6 and 12 months and case management receipt at months 3 and 6, but not 12; Risk of bias: Moderate. Row 4: Study: Morrissey et al, 2016; Study method: Quasi-experimental study; Sample characteristics and location: 3086 offenders (mixed) with SMI released from state prisons (intervention: 895; comparison: 2191); mean age: 36.25 years; USA; Description of intervention: pre-release referral for expedited Medicaid enrolment; primary outcomes measured at release, after 30 days and within 12 months; Outcome: referred group had higher Medicaid enrolment at release, 30 days and 12 months (p < 0.01); higher service use, but more prison days despite no arrest rate differences; Risk of bias: Moderate. Row 5: Study: Wenzlow et al, 2011; Study method: Longitudinal/cohort study; Sample characteristics and location: 686 prisoners with SMI (project facilities: 272 (treatment: 193; baseline: 79); comparison facilities: 414 (treatment: 130; baseline: 284)); USA; Description of intervention: Oklahoma's discharge planning; early identification, consent and assistance with federal disability and Medicaid applications; Outcome: Release day Medicaid enrolment increased in treatment group (25% from 8% 2 years ago); 3-4% in comparison facilities; sustained at 30, 60 and 90 days; Risk of bias: Low.
SMI, severe mental illness; SUD, substance use disorder.
As detailed in Supplementary Appendix B, the operational definitions of both SMI and recidivism varied considerably across the studies reviewed. Diagnoses classified as SMI generally centred on schizophrenia and bipolar disorder, but frequently expanded to include others, depending on the study’s inclusion criteria. Recidivism was mainly defined as re-incarceration, although some studies included technical parole violations whereas others strictly measured new offences.
Studies can be broadly grouped into three categories based on the type of intervention employed: linkage to community support services, linkage or provision of community mental health services, and health insurance access interventions. We will discuss each in turn.
Community support services
Studies in this category aimed to link individuals to community support services. These include a single RCT, two longitudinal cohort studies and one retrospective study (see Table 1). Two studies had a critical risk of bias, Reference Bellamy, Kimmel, Costa, Tsai, Nulton and Nulton18,Reference Smith, Harnett, Flanagan, Hennessy, Gill and Quigley33 one had moderate risk Reference Carr, Baker and Cassidy19 and one RCT had a low risk. Reference Shaw, Conover, Herman, Jarrett, Leese and McCrone27 Four studies demonstrated generally positive impacts on service engagement and, in some cases, recidivism reduction. Bellamy et al found that peer mentoring commenced before release and continued in the community was associated with lower re-incarceration rates (22%) in the first year after release compared with the general prison population (43%). Reference Bellamy, Kimmel, Costa, Tsai, Nulton and Nulton18 Carr et al reported that participants in a day reporting centre with integrated vocational, accommodation and psychiatric support had lower reconviction rates (49%) and lower longer time to recidivism than matched controls (69%); completion status within the day reporting centre programme also predicted time to any conviction. Reference Carr, Baker and Cassidy19 Shaw et al conducted an RCT of a critical time intervention model and observed improved and more consistent contact with community mental health services after release, although the reduction in reoffending was not sustained at later follow-up. Reference Shaw, Conover, Herman, Jarrett, Leese and McCrone27 Smith et al, in a study on the Pre-Release Planning programme, found that a substantial number of participants (46.5%) were re-incarcerated during the study period, with no significant correlation between re-incarceration and improvements in mental health support or accommodation. Reference Smith, Harnett, Flanagan, Hennessy, Gill and Quigley33 These studies highlight that although case management and community support interventions can enhance continuity of care and initial service engagement, their effects on recidivism and long-term criminal justice outcomes remain mixed.
Community mental health services
Studies on linkages directly to community mental health service teams showed some positive results (see Table 2). The highest quality of evidence came from two RCTs, which investigated modified therapeutic communities and reported positive findings in terms of recidivism reduction. The modified therapeutic community group had lower re-incarceration rates (9%) than the comparison group (33%) in one study; in the other study, the experimental re-entry modified therapeutic community group had lower re-incarceration rates (19%) than the control parole supervision case management group (38%). Reference Sacks, Sacks, McKendrick, Banks and Stommel24,Reference Sacks, Chaple, Sacks, McKendrick and Cleland25 However, in terms of risk of bias, these studies had some concerns Reference Sacks, Sacks, McKendrick, Banks and Stommel24 or a high risk. Reference Sacks, Chaple, Sacks, McKendrick and Cleland25 On the other hand, two RCTs showed no significant difference in rate of re-incarceration among people under assertive community treatment, forensic individual case managers or the community mental health centre; both these RCTs had a critical risk of bias. Reference Solomon, Draine and Meyerson31,Reference Solomon and Draine32 Another two RCTs, one of a modified therapeutic community (high risk of bias) and another of a service-linkage programme (low risk of bias), reported mixed findings with periodic crisis stabilisation, increased service utilisation and some symptom improvement, but no significant differences were found in measures of symptom change and recidivism between groups. Reference Sullivan, Sacks, McKendrick, Banks, Sacks and Stommel26,Reference Taylor28
Non-RCT study methods in this category included longitudinal/cohort studies, AB design, retrospective matched control design and brief report. Four studies had a critical risk of bias, Reference Hartwell and Orr12,Reference Theurer and Lovell29,Reference Ventura, Cassel, Jacoby and Huang30,Reference Stewart, Farrell-MacDonald and Feeley34 five had a serious risk, Reference Comartin, Burgess-Proctor, Hicks, Putans and Kubiak20,Reference Johnson, Williams and Zlotnick35–Reference Held, Brown, Frost, Hickey and Buck38 one had a moderate risk Reference McKenna, Skipworth, Tapsell, Madell, Pillai and Simpson39 and one had a low risk. Reference Lovell, Gagliardi and Phipps40 The Sober Network cellphone-based intervention results suggested better social support and a reduction in depressive symptoms and substance use on community follow-up of women with substance use disorders and major depression. Reference Johnson, Williams and Zlotnick35 A study revealed that participants in an intensive case management treatment programme had a recidivism rate of 23%, which was just over half of the 42% rate observed in matched controls. Reference Theurer and Lovell29 In another study, men receiving only community mental health services had lower risk of recidivism and returning to custody. Reference Stewart, Farrell-MacDonald and Feeley34 Two of these had a critical risk of bias Reference Theurer and Lovell29,Reference Stewart, Farrell-MacDonald and Feeley34 and one had a serious risk. Reference Johnson, Williams and Zlotnick35 Another study, with a serious risk of bias, found no significant association between specific programme characteristics and recidivism. Reference Comartin, Burgess-Proctor, Hicks, Putans and Kubiak20 Additionally, increased return to the criminal justice system was observed after regionalisation of forensic transition teams in one study with a critical risk of bias. Reference Hartwell, Fisher and Deng41
With regard to service engagement and continuity of care, diversion participants, high-dose programme participant, and programme completers were more likely to engage in treatment both within 14 days and a year post-release, compared with non-diversion participants, low-/medium-dose programme participants and non-completers; Reference Comartin, Burgess-Proctor, Hicks, Putans and Kubiak20 this indicates that continuity of care was significantly influenced by programme dosage and completion. The Dangerous Mentally Ill Offender programme in the USA was noted to succeed in providing more comprehensive and consistent mental health services, and reducing overall and felony recidivism, but not violent felony recidivism; this study had a low risk of bias. Reference Lovell, Gagliardi and Phipps40 The development of a Prison Model of Care was studied using an AB design, which was focused on enhanced case detection, assessment and engagement of community mental health services before release in New Zealand. They found that men on remand achieved higher levels of engagement with general mental health services and observed a non-significant decrease in reoffending. Reference McKenna, Skipworth, Tapsell, Madell, Pillai and Simpson39 The risk of bias in this study was moderate.
Health insurance access-related interventions
Five studies fell into this category, which were either longitudinal cohort or quasi-experimental studies (see Table 3). Expedited Medicaid referrals were the most common intervention in this group. They are specific to jurisdictions with health insurance-based health services that require insurance enrolment to access healthcare follow-up and medication in the community. Such enrolment is frequently interrupted by incarceration. Four studies demonstrated that expedited Medicaid referrals were associated with higher enrolment rates and service utilisation post-release. Reference Cuddeback, Morrissey and Domino21–Reference Morrissey, Domino and Cuddeback23,Reference Wenzlow, Ireys, Mann, Irvin and Teich42 Referral to expedited Medicaid enrolment predicted a higher probability of accessing any substance use disorder treatment. Reference Gertner, Grabert, Domino, Cuddeback and Morrissey22 Also, Medicaid enrolment rates were significantly higher for approved individuals after 1 and 3 months following release. Reference Cuddeback, Morrissey and Domino21 However, two studies reported mixed findings. One showed that this intervention, despite increased enrolment and service utilisation, did not reduce criminal recidivism. Reference Morrissey, Domino and Cuddeback23 Another found that the group referred for expedited Medicaid had significantly more episodes of incarceration in the year following release. Reference Domino, Gertner, Grabet, Cuddeback and Morrisey43 Four studies had a moderate risk of bias Reference Cuddeback, Morrissey and Domino21–Reference Morrissey, Domino and Cuddeback23,Reference Domino, Gertner, Grabet, Cuddeback and Morrisey43 and one had a low risk of bias. Reference Wenzlow, Ireys, Mann, Irvin and Teich42
Discussion
We identified 26 studies that evaluated reintegration programmes for individuals with SMI transitioning from correctional institutions to the community. These varied widely in the type of interventions (e.g. peer support, transitional coordination, expedited Medicaid enrolment, integrated psychosocial interventions) and in outcomes measured (e.g. recidivism, treatment engagement, mental health symptoms, social functioning). Some programmes demonstrated efficacy in reducing recidivism and improving service engagement, the overall evidence base reflects a complex and rather mixed picture. Programmes addressing both mental health and social needs, such as those providing coordinated clinical care, housing and vocational support, were generally more effective in reducing recidivism and improving community engagement. For instance, peer mentoring and transitional coordination programmes consistently demonstrated lower rates of re-incarceration and higher treatment engagement rates compared with standard care; Reference Bellamy, Kimmel, Costa, Tsai, Nulton and Nulton18–Reference Comartin, Burgess-Proctor, Hicks, Putans and Kubiak20,Reference Green, Denton, Heffernan, Russell, Stapleton and Waterson37,Reference Held, Brown, Frost, Hickey and Buck38 however, three of these studies had a serious risk of bias, Reference Comartin, Burgess-Proctor, Hicks, Putans and Kubiak20,Reference Green, Denton, Heffernan, Russell, Stapleton and Waterson37,Reference Held, Brown, Frost, Hickey and Buck38 one had a moderate risk Reference Carr, Baker and Cassidy19 and one had a serious risk. Reference Bellamy, Kimmel, Costa, Tsai, Nulton and Nulton18 In contrast, programmes focusing solely on Medicaid enrolment or benefit reinstatement had mixed or even counterintuitive findings; Reference Gertner, Grabert, Domino, Cuddeback and Morrissey22,Reference Morrissey, Domino and Cuddeback23,Reference Domino, Gertner, Grabet, Cuddeback and Morrisey43 some studies reported increased re-incarceration when Medicaid enrolment was not paired with clinical engagement or case management, Reference Morrissey, Domino and Cuddeback23,Reference Domino, Gertner, Grabet, Cuddeback and Morrisey43 suggesting that multicomponent interventions are more effective than single-focus programmes. However, there may be jurisdiction specific reasons for this, and the goal of achieving access to health benefits is of itself vital in the tasks of reintegration.
The findings for case management and clinical engagement align with prior research, Reference Martin, Dorken, Wamboldt and Wootten7 demonstrating that interventions tackling both mental health-related factors and social determinants yield better outcomes than clinical or social interventions administered alone. The importance of addressing social determinants of health such as housing, financial support and employment alongside mental health treatment is well established in the literature. Reference Draine, Salzer, Culhane and Hadley44–Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones and Patalay46 Peer support models, in particular, have gained recognition for their role in fostering engagement and stigma reduction. Reference Davidson, Bellamy, Guy and Miller47 Integrated clinical and social support programmes are most consistent with existing evidence advocating for holistic approaches that address both mental health and social determinants. Although these programmes show promise, the evidence base is still limited, with small sample sizes and moderate-to-serious risk of bias in many studies.
Programmes focusing on expedited Medicaid enrolment or benefit reinstatement generally improved access to out-patient and substance use disorder treatment, Reference Cuddeback, Morrissey and Domino21,Reference Gertner, Grabert, Domino, Cuddeback and Morrissey22 but outcomes are mixed, especially with respect to re-incarceration. Reference Hopkin, Evans-Lacko, Forrester, Shaw and Thornicroft8 This may be because the programme was targeted too narrowly on health access alone, and not on a broad range of reintegration support. Instability may have been detected by health and probation services resulting in re-incarceration for breaches of release provision that might not otherwise have been detected. Reference Phelps48 Thus, it is an attempt to provide more, but incomplete or siloed services may increase the risk of re-incarceration. Similar findings have been noted in studies of Forensic Assertive Community Treatment models for persons with SMI with a history of criminal justice involvement. Reference Cuddeback, Morrissey and Cusack49,Reference Zhou and Ford50 Previous research indicates that, although insurance is necessary for access to care, coverage alone does not guarantee improved outcomes without coordinated clinical and social supports. Reference Binswanger, Stern, Yamashita, Mueller, Baggett and Blatchford10,Reference Winkelman, Kieffer, Goold, Morenoff, Cross and Ayanian51 Many programmes lacked randomised designs, thereby limiting causal inference.
Reintegration of prisoners with SMI into the community after release presents significant challenges that require comprehensive and coordinated approaches. This complex process involves addressing multiple interconnected factors, such as finances, employment, accommodation and mental healthcare continuity, to ensure successful outcomes for both the individuals and society at large. Reference Baillargeon, Hoge and Penn2,Reference Galletta, Fagan, Shapiro and Walker52 Studies are, therefore, understandably diverse and typically focus on a handful of issues; certain solutions also tend to be jurisdiction-specific (e.g. Medicaid in the USA). The availability and quality of mental health services and reintegration programmes varies greatly across jurisdictions, making it challenging to generalise findings. Conducting research into the reintegration of prisoners with SMI into the community presents several practical difficulties, which may include difficulties obtaining data because of privacy laws and bureaucratic obstacles, securing adequate funding for long-term studies, the logistical complexity of ensuring effective research collaboration between multi-disciplinary team staff and inconsistent definitions for ‘successful reintegration’ in different studies that make comparisons difficult. Reference Galletta, Fagan, Shapiro and Walker52,Reference Hunter, Lanza, Lawlor, Dyson and Gordon53
Traditional probation models usually focus on compliance instead of tackling underlying criminogenic needs or psychiatric symptomatology. This unidimensional approach can lead to higher recidivism rates compared with specialty models that integrate mental health treatment and supervision. Reference Lamberti54 Mental health service and probation linkages might initially appear to increase recidivism possibly as a result of increased detection of technical violations; Reference Skeem and Louden55 however, determining true effectiveness of these services in the community often takes up to a year to achieve, Reference Skeem, Manchak and Montoya56 complicating short-term evaluations. Although many included studies followed participants for a year or more, others focused on a much shorter duration, such as 3 months, Reference Cuddeback, Morrissey and Domino21 6 months Reference Solomon, Draine and Meyerson31,Reference McKenna, Skipworth, Tapsell, Madell, Pillai and Simpson39 and 9 months. Reference MacInnes, Khan, Tallent, Hove, Dyson and Grandi36
Sources in this review offer diverse study designs across various jurisdictions, providing insights from different mental health and criminal justice systems. Nevertheless, heterogeneity of interventions and outcomes is also a weakness of this review, making direct comparisons and synthesis of findings even more challenging. Most studies (19 out of 26) were non-RCTs, consequently increasing the risk of selection bias and confounding. Long-term programme impacts are obscured by the fact that more than half of the included studies (17 out of 26) tracked outcomes for a year or less. All studies were conducted exclusively in high-income countries, limiting their applicability to low- and middle-income countries. Furthermore, as detailed in Supplementary Appendix B, because of considerable heterogeneity in how SMI and recidivism were defined across the literature, direct comparability of outcomes becomes limited; the thresholds for reintegration failure measurement differed significantly – such as whether technical violations were included or a new criminal charge alone constituted recidivism. Another limitation of this review is that inter-rater agreement statistics were not calculated and a Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was not conducted, which could potentially affect the consistency of study inclusion decisions and evidence quality evaluation. In the present review, the included studies were highly heterogeneous in design, populations, interventions and outcome measures, and quantitative synthesis was not the primary objective; as such, applying GRADE would not have provided additional meaningful insight beyond the detailed risk-of-bias assessments performed already.
Successful reintegration of incarcerated individuals with SMI following release requires a multifaceted strategy that addresses both immediate and continued needs. The summarised studies reveal mixed outcomes, which highlights the complexity of addressing service engagement, social integration and recidivism among released prisoners with SMI. Although programme models and outcomes vary, interventions that offer sustained, coordinated support across clinical, social and structural domains, particularly those that integrate mental health care with housing, employment and peer support, tend to show the most promise in reducing recidivism and enhancing service engagement. In contrast, programmes narrowly focused on administrative tasks, such as expedited benefit enrolment without accompanying case management or therapeutic support, demonstrate limited or even counterintuitive impacts, including higher rates of re-incarceration likely linked to increased monitoring and detection of technical violations.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12034
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgements
The authors thank Andrew Whiteman (A.W.) and Corina Picco (C.P.) for their assistance during the screening phase of the review.
Author contributions
A.I.F.S., C.G. and R.M.J. contributed to study conception and design. V.A. and R.B. developed the search strategy and prepared the ‘Method’ section of the manuscript. V.A., M.K. and M.M. conducted the literature review, data extraction and risk-of-bias assessments, with decisions and ratings confirmed with A.I.F.S., C.G. or R.M.J. M.U.W. drafted the manuscript, with input from A.I.F.S. and R.M.J. All authors reviewed and approved the final manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
A.I.F.S. is a member of the BJPsych Open Editorial Board, but did not take part in the peer review or decision-making process of this paper.





 Open access
Open access
eLetters
No eLetters have been published for this article.