


Cannabis is one of the most widely consumed psychoactive substances globally, with an estimated 219 million worldwide users as of 2021. 1 Globally, there has been an increase in the concentration of the primary psychoactive compound in cannabis: tetrahydrocannabinol (THC), especially in North America and Europe. Reference Cascini, Aiello and Tanna2
In the USA, the average THC concentration of federally seized cannabis increased from 8.9% in 2008 to 17.1% in 2017. Reference Chandra, Radwan, Majumdar, Church, Freeman and ElSohly3 Similar trends are reported by potency monitoring programmes in the European Union, which found that the average THC concentration of herbal cannabis increased from 5.0% in 2006 to 10.2% in 2016. Reference Freeman, Groshkova, Cunningham, Sedefov, Griffiths and Lynskey4 In Canada, the THC content of dried cannabis legally available has risen sharply in the past two decades, increasing from an average of 4% THC in the 2000s to 20% in 2023. Reference Li, Solmi, Myran and Fabiano5 The most frequently purchased cannabis products available at retailers across Canada often have a potency starting as high as 20–30% THC. Reference Brown6,Reference Lalonde7
Cannabis use has both acute and long-term impacts on mental health. Acute cannabis use is associated with transient cognitive impairment, Reference Dellazizzo, Potvin, Giguère and Dumais8 anxiety Reference Lowe, Sorkhou and George9–Reference Sharpe, Sinclair, Kramer, De Manincor and Sarris12 and psychotic-like experiences, Reference Mokrysz, Shaban, Freeman, Lawn, Pope and Hindocha13–Reference D’Souza, Perry, MacDougall, Ammerman, Cooper and Wu15 while chronic cannabis use is associated with other substance dependence. Reference Degenhardt, Hall and Lynskey16 Chronic cannabis use alone, as well as other co-occurring substance use, is associated with the development, or worsening, of mood and psychotic disorders. Reference Sideli, Quigley, La Cascia and Murray17 Further research suggests that these aforementioned effects could be moderated by cannabis potency, such that an increased THC content is associated with a greater magnitude of use consequences, such as cognitive deficits Reference Curran, Brignell, Fletcher, Middleton and Henry18,Reference Boggs, Cortes-Briones, Surti, Luddy, Ranganathan and Cahill19 and anxiety. Reference Sharpe, Sinclair, Kramer, De Manincor and Sarris12,Reference Childs, Lutz and de Wit20 Despite its importance, the influence of cannabis potency on mental health outcomes is often not explicitly examined, making its impact unclear.
Determining how cannabis potency affects users is especially important when considering adolescent and young adult (AYA) populations. Compared with older users, AYAs are at a higher risk of experiencing long-term consequences of substance use due to the critical neurodevelopmental time period coincident with this age range. Reference Konrad, Firk and Uhlhaas21 Cannabis use can cause disruptions to the brain’s endocannabinoid system, which has an important role in brain maturational processes during adolescence, Reference Haney22,Reference Meyer, Lee and Gee23 potentially resulting in a variety of mental health issues. Reference Meyer, Lee and Gee23 AYAs use cannabis more frequently than other age groups, 24 and use cannabis of a higher THC potency than previous generations. As such, a better understanding of high cannabis potency effects in AYAs is needed.
A recent scoping review by Bero et al assessed the health effects of high-potency cannabis (HPC) products across various age groups. Reference Bero, Lawrence, Oberste, Li, Leslie and Rittiphairoj25 The authors reported that studies assessing the mental health consequences of HPC were the most common in the literature; however, the specific consequences were not explicitly reported on. In addition, even though AYA made up a portion of their sample, Bero et al’s lack of focus on – or restriction to – an AYA age range makes their results less accessible to parties interested in determining how cannabis potency affects AYA mental health. Another existing review on the health impact of cannabis potency limited their focus to mental health disorders. Reference Petrilli, Ofori, Hines, Taylor, Adams and Freeman26 However, this review only discussed select mental disorders, and like Bero et al, Petrilli et al’s review did not specifically assess an AYA age range. Reference Bero, Lawrence, Oberste, Li, Leslie and Rittiphairoj25,Reference Petrilli, Ofori, Hines, Taylor, Adams and Freeman26 Consequently, while being effective explorations of their respective topics, these existing reviews are not best equipped to address the question of the effect of cannabis potency on cannabis-related mental health outcomes in AYA populations. Addressing this question is vital to understanding the impact of cannabis potency on a developmentally vulnerable age group. Understanding this relationship will also inform future cannabis-potency research and foster the subsequent development of public health strategies and targeted interventions. This gap in knowledge necessitates a precise yet thorough summary of the existing evidence.
To address this need, we conducted a scoping review to provide a broad overview of the literature, rather than attempting to answer a specific question. Reference Lockwood, dos Santos and Pap27 As such, our scoping review aimed to identify and summarise existing literature regarding the relationship between cannabis potency and the onset or progression of mental health conditions, with a focus on individuals aged 14–25. The present review also sought to explore potential differences in this relationship based on the gender and/or sex of the user.
Method
This review was conducted in accordance with the JBI methodology for scoping reviews and Lockwood et al’s scoping review methodological framework. Reference Lockwood, dos Santos and Pap27,Reference Peters, Godfrey, McInerney, Munn, Tricco, Khalil, Aromataris, Lockwood, Porritt, Pila and Jordan28 The protocol for this review was registered a priori in Open Science Framework 29,Reference Hambly Lapointe, Nosko, Crocker and Tibbo30 (https://doi.org/10.17605/OSF.IO/9R7QC).
Eligibility criteria
This review included peer-reviewed studies, preprints and theses/dissertations that reported the effect that cannabis of a specific potency had on the mental health outcomes of AYAs. We defined AYAs as individuals between the ages of 14 and 25. This age range was chosen due to its accordance with the World Health Organization’s definition of AYA Reference Lichenstein10–24,31 , and the age by which puberty usually begins. 32 Studies involving cohorts outside this age range were included only if the source could establish that the participants had used cannabis within the specified age range.
Reporting of cannabis potency included by percentage, mass and ratio of cannabinoids, and reported via self-report or laboratory-based analyses. Studies reporting exclusively on synthetic and medical-grade cannabis (i.e. dronabinol) were excluded. When author-given potency stratification was not used, we categorised cannabis as high potency if it contained 15% or more THC (15 mg/g) and as low potency if it contained less than this amount. Studies reporting on recreational and publicly available cannabis were included for this review. Studies exclusively reporting on epilepsy, somatic, motor or physical sensation related outcomes were excluded from the present review.
Search strategy
We conducted our searches of Ovid MEDLINE (NLM, Wolters Kluwer), CINAHL (EBSCO), PsycINFO (American Psychological Association) and Embase (Elsevier) on 3 June 2024, with a secondary search on 6 October 2025, to include eligible sources published since the primary search. The terms used in these searches are included in Appendix A. Sources derived from these searches were then collated and uploaded into Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Australia; www.covidence.org) for Windows. Duplicate sources were removed both automatically by the review software and manually by a reviewer (C.H.L.).
Study selection
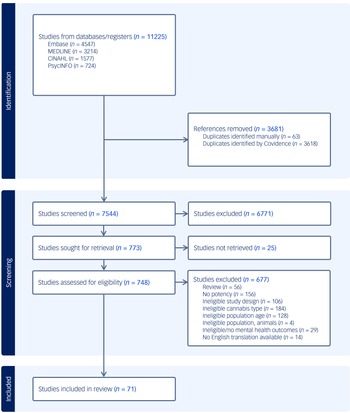
Once in Covidence, sources derived from the searches were screened twice. First, two independent reviewers screened the titles and abstracts of all sources (C.H.L. and L.N.). Sources which were found to meet the inclusion criteria at this point then had their entire text reviewed by the same two reviewers for further confirmation of the source’s suitability for the current review. Reference lists of reviews that made it to the full-text stage were manually screened for relevant sources. Any time a source was excluded from the review, the reason for doing so was recorded and are presented in the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) flow diagram (Fig. 1). If at any point there was confusion or a conflict between the reviewers that could not easily be resolved, a third reviewer would assess the source (C.E.C. or P.G.T.).
PRISMA-ScR diagram.

Fig. 1 Long description
The flowchart illustrates the process of screening and selecting studies for a review on cannabis. It begins with the identification phase, where studies from databases/ registers are listed, totaling 11225 studies. These databases include Embase (4547), MEDLINE (3214), CINAHL (1577), and PsycINFO (724). Next, references removed are shown, totaling 3681, with duplicates identified manually (63) and by Covidence (3618). The screening phase follows, where 7544 studies are screened, and 6771 studies are excluded. Studies sought for retrieval total 773, with 25 studies not retrieved. Studies assessed for eligibility total 748, with 677 studies excluded for various reasons such as review (56), no potency (156), ineligible study design (106), ineligible cannabis type (184), ineligible population age (128), ineligible population animals (4), ineligible/no mental health outcomes (29), and no English translation available (14). Finally, 71 studies are included in the review.
Data extraction
Data were extracted by two independent reviewers (C.H.L. and L.N.) using an extraction tool developed by C.H.L. in Covidence. A pilot test was conducted with five studies to ensure the data-extraction sheet included all necessary variables and outcomes. Ambiguities were resolved again through consultation with a third reviewer (C.E.C. or P.G.T.). The extraction sheet used included study design characteristics, aims, participant information, cannabis-use patterns and mental health outcomes.
Sex and gender considerations
Our secondary objective was to assess if gender and/or sex moderated the relationship between cannabis potency and AYA mental health outcomes. For the purposes of this review, we defined sex as being an individual’s biological characteristics present from birth, and gender as the roles and identities that an individual assumes regardless of biological characteristics. 33 Included studies which assessed gender and/or sex in relation to cannabis and AYA mental health outcomes had these additional findings extracted.
Results
Search results
In total, 11 225 studies were identified across our initial and updated searches and imported into Covidence, 7544 of which remained after duplicates were removed. Of these studies, 773 moved forward to full-text screening where a further 677 were excluded and 25 were unable to be retrieved due to having no available full-text manuscript. After this screening process and citation searching, 71 studies remained which had relevant data extracted. The screening process is illustrated in the PRISMA-ScR flow diagram (Fig. 1).
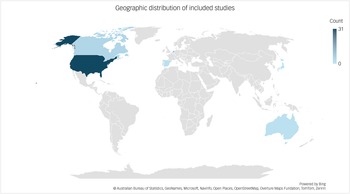
The studies included in this review encompass a broad time frame, with publication dates spanning from 1979 to 2025. However, analysis of the included studies reveals a geographical concentration, with approximately 44% of the included research being conducted in the USA, 21% in England and 11% in the Netherlands (see Fig. 2). Regarding regulatory contexts at the time of publication, 27% of the studies were carried out in nations where cannabis was only legal for medical use. In contrast, 18% of the research was conducted in areas where cannabis was legal for recreational use, and 53% in locations with a mixed regulatory status (i.e. legal in some jurisdictions within a country but not others).
Location of where the included studies were conducted, excluding studies conducted across multiple nations.

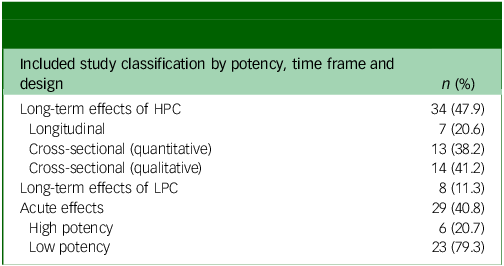
The results presented in this review are highly heterogeneous with respect to reported cannabis potency across studies. Studies were organised according to their classification by cannabis potency, focus on either long-term or acute effects and study design (Table 1). Of the total studies reviewed, 34 (47.9%) studies focused on the long-term effects of HPC with 7 (20.6%) utilising longitudinal designs (Table 2), 13 (38.2%) utilising a cross-sectional design with quantitative measures of potency (Table 3), and 14 (41.2%) utilising a cross-sectional design with qualitative measures of potency (Table 4). Eight (11.3%) included studies reported on the long-term effects of low-potency cannabis (LPC) (Table 5). The remaining, comprising 29 studies (40.8%; 6 HPC, 23 LPC), reported on the acute effects of cannabis (Table 6). The remainder of this review summarises this literature. Results regarding the acute effects of LPC use Reference Lane, Cherek, Tcheremissine, Lieving and Pietras34–Reference Wickens, Wright, Mann, Brands, Di Ciano and Stoduto56 are present in the Supplementary Table S1 available at https://doi.org/10.1192/bjo.2026.12023.
Distribution of included studies by potency, time frame and design categories

HPC, high-potency cannabis; LPC, low-potency cannabis.
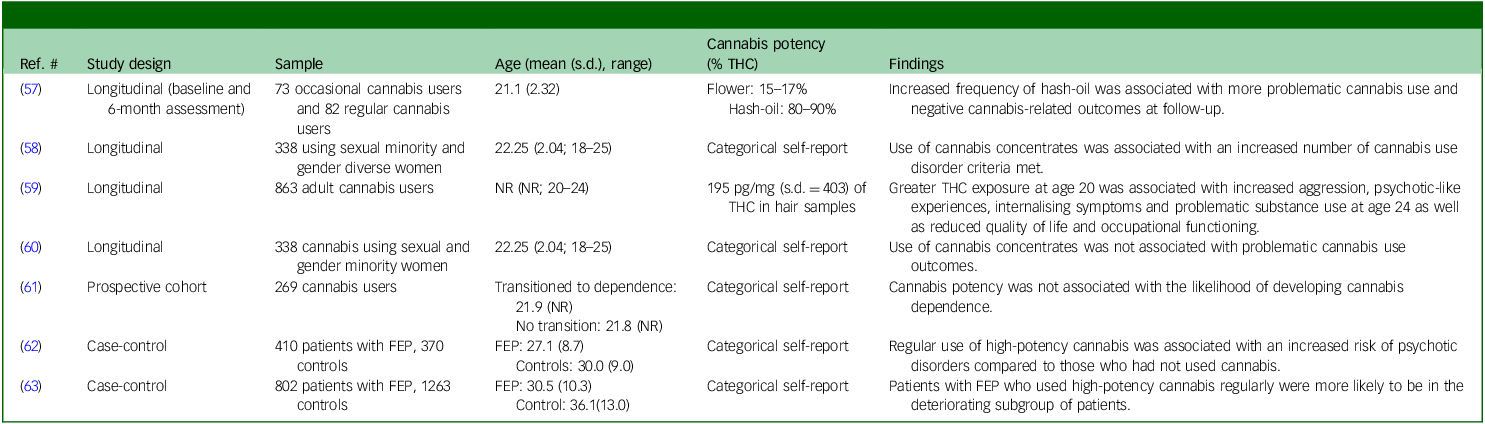
Findings from included studies with results regarding the long-term effects of high-potency cannabis (longitudinal)
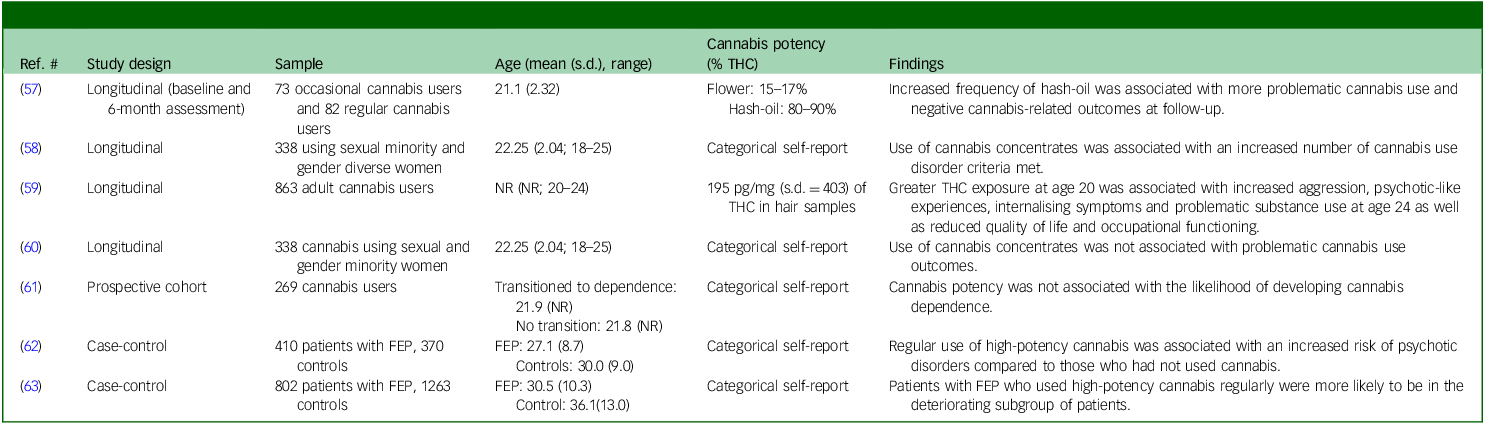
THC, tetrahydrocannabinol; NR, not reported; FEP, first episode of psychosis.
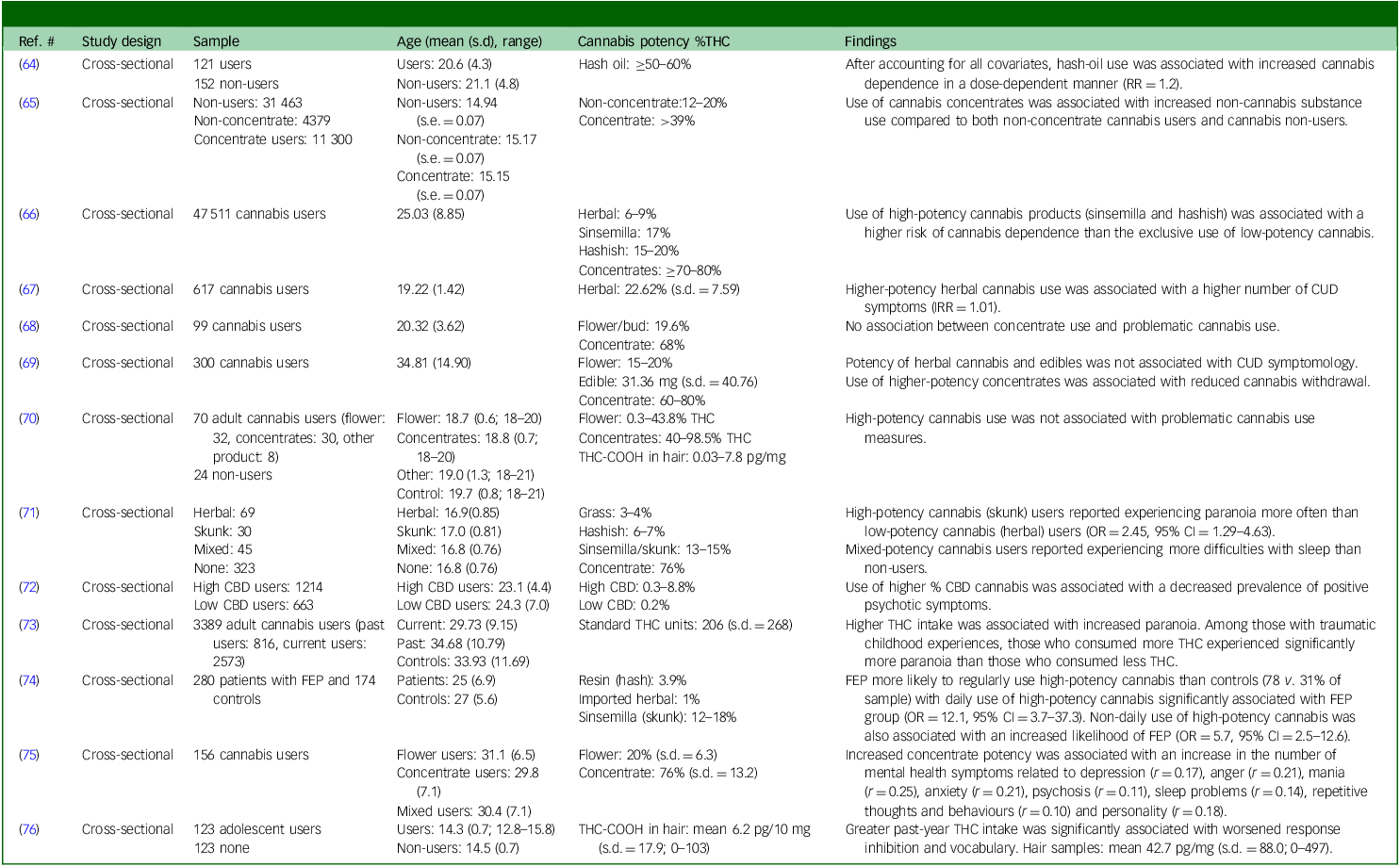
Findings from included studies with results regarding the long-term effects of high-potency cannabis (cross-sectional with quantitative potency)

THC, tetrahydrocannabinol; RR, rate ratio; CUD, cannabis use disorder; IRR, incidence rate ratio; THC-COOH, 11-nor-9-carboxy-THC; OR, odds ratio; CBD, cannabidiol; FEP, first episode of psychosis.
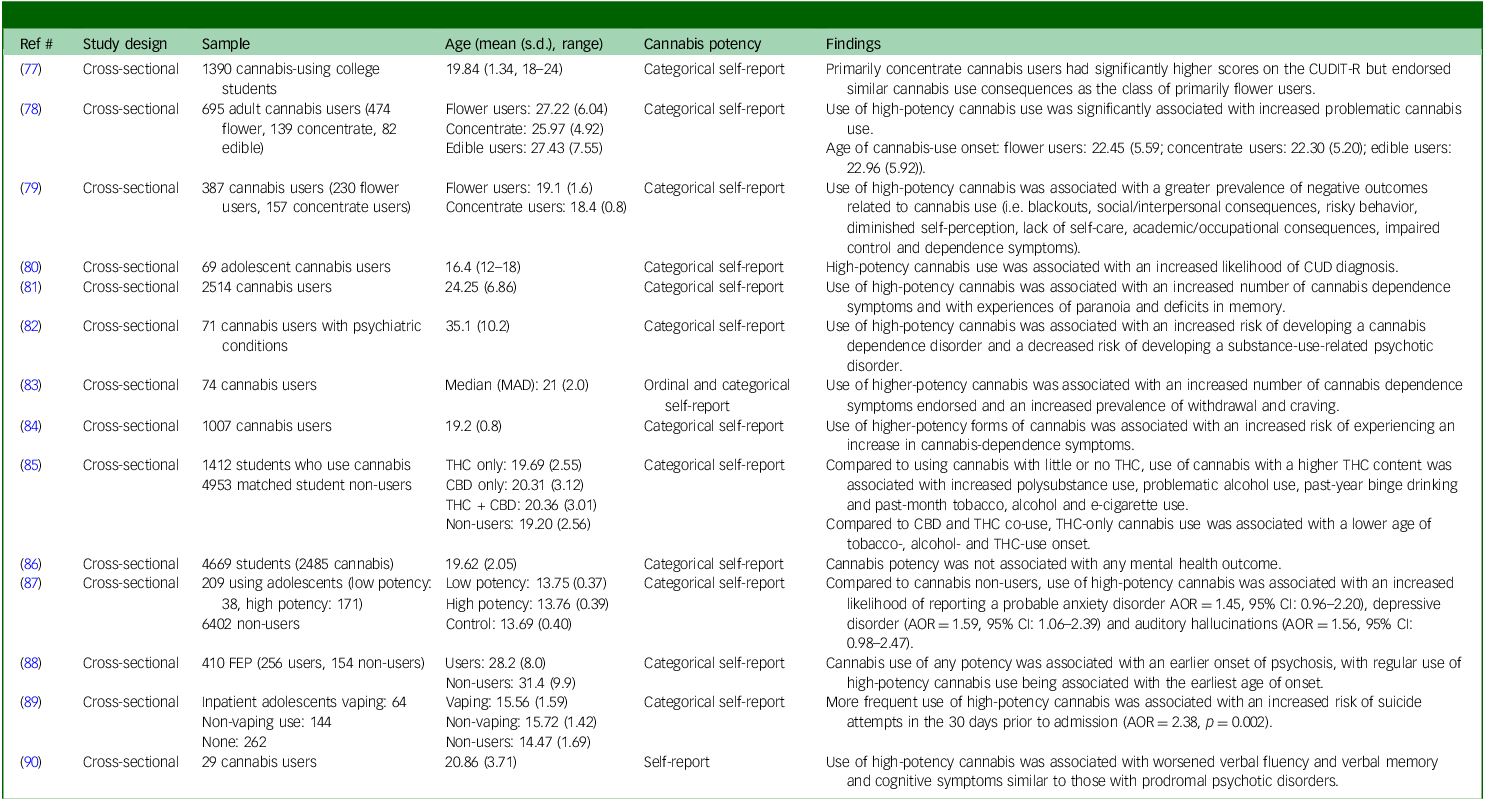
Findings from included studies with results regarding the long-term effects of high-potency cannabis (cross-sectional with qualitative potency)

Table 4 Long description
The table presents a detailed summary of studies focusing on the long-term effects of high potency cannabis. It includes 14 studies with a cross-sectional design and qualitative measures of potency. The table has 14 rows and 6 columns. Column headers are: Ref, Study design, Sample, Age (mean (s.d.), range), Cannabis potency, and Findings. Row 1: Ref: 37, Study design: Cross-sectional, Sample: 1390 cannabis-using college students, Age: 19.84 (1.34, 18-24), Cannabis potency: Categorical self-report, Findings: Primarily concentrate cannabis users had significantly higher scores on the CUDIT-R but endorsed similar cannabis consequences as the class of primarily flower users. Row 2: Ref: 38, Study design: Cross-sectional, Sample: 695 adult cannabis users (474 flower, 139 concentrate, 82 edible), Age: Flower users: 27.22 (6.04), Concentrate: 25.97 (4.92), Edible users: 27.43 (7.55), Cannabis potency: Categorical self-report, Findings: Use of high potency cannabis use was significantly associated with increased problematic cannabis use. Row 3: Ref: 39, Study design: Cross-sectional, Sample: 387 cannabis users (230 flower users, 157 concentrate users), Age: Flower users: 19.1 (1.6), Concentrate users: 18.4 (0.8), Cannabis potency: Categorical self-report, Findings: Use of high potency cannabis was associated with a greater prevalence of negative outcomes related to cannabis use (e.g., blackouts, social/interpersonal consequences, risky behavior, diminished self-perception, lack of self-care, academic/occupational consequences, impaired control and dependence symptoms). Row 4: Ref: 40, Study design: Cross-sectional, Sample: 69 adolescent cannabis users, Age: 16.4 (12-18), Cannabis potency: Categorical self-report, Findings: High potency cannabis use was associated with an increased likelihood of CUD diagnosis. Row 5: Ref: 41, Study design: Cross-sectional, Sample: 2514 cannabis users, Age: 24.25 (6.86), Cannabis potency: Categorical self-report, Findings: Use of high potency cannabis was associated with an increased number of cannabis dependence symptoms and with experiences of paranoia and delusions in memory. Row 6: Ref: 42, Study design: Cross-sectional, Sample: 71 cannabis users with psychiatric conditions, Age: 35.1 (10.2), Cannabis potency: Categorical self-report, Findings: Use of high potency cannabis was associated with an increased risk of developing a cannabis dependence disorder and a decreased risk of developing a substance-use-related psychotic disorder. Row 7: Ref: 43, Study design: Cross-sectional, Sample: 74 cannabis users, Age: Median (MAD): 21 (2.0), Cannabis potency: Ordinal and categorical self-report, Findings: Use of higher potency cannabis was associated with an increased number of cannabis dependence symptoms endorsed and an increased prevalence of withdrawal and craving. Row 8: Ref: 44, Study design: Cross-sectional, Sample: 1007 cannabis users, Age: 19.2 (0.8), Cannabis potency: Categorical self-report, Findings: Use of higher potency forms of cannabis was associated with an increased risk of experiencing an increase in cannabis dependence symptoms. Row 9: Ref: 45, Study design: Cross-sectional, Sample: 1412 students who use cannabis, Age: THC only: 19.69 (2.55), CBD only: 20.31 (3.12), THC + CBD: 20.36 (3.01), Non-users: 19.20 (2.56), Cannabis potency: Categorical self-report, Findings: Compared to using cannabis with little or no THC, use of cannabis with a higher THC content was associated with increased polysubstance use, problematic alcohol use, past-year binge drinking and past-month tobacco, alcohol and e-cigarette use. Compared to CBD and THC co-use, THC-only cannabis was associated with a lower age of tobacco, alcohol and THC use onset. Row 10: Ref: 46, Study design: Cross-sectional, Sample: 4669 students (2485 cannabis), Age: 19.62 (2.05), Cannabis potency: Categorical self-report, Findings: Cannabis potency was not associated with any mental health outcome. Row 11: Ref: 47, Study design: Cross-sectional, Sample: 209 adolescent users (low potency: 38, high potency: 171), Age: Low potency: 13.75 (0.37), High potency: 13.76 (0.39), Control: 13.69 (0.40), Cannabis potency: Categorical self-report, Findings: Compared to cannabis users, use of high potency cannabis was associated with an increased likelihood of reporting a probable anxiety disorder (AOR = 1.45, 95 percent CI: 0.96-2.20), depressive disorder (AOR = 1.59, 95 percent CI: 1.06-2.39), and auditory hallucinations (AOR = 1.56, 95 percent CI: 0.98-2.47). Row 12: Ref: 48, Study design: Cross-sectional, Sample: 410 FEP (256 users, 154 non-users), Age: Users: 28.2 (8.0), Non-users: 31.4 (9.9), Cannabis potency: Categorical self-report, Findings: Cannabis potency of any potency was associated with an earlier onset of psychosis, with regular use of high potency cannabis being associated with the earliest age of onset. Row 13: Ref: 49, Study design: Cross-sectional, Sample: 29 cannabis users, Age: 20.86 (3.71), Cannabis potency: Self-report, Findings: Use of high potency cannabis was associated with worsened verbal fluency and verbal memory and cognitive symptoms similar to those with prodromal psychotic disorders.
CUDIT-R, The Cannabis Use Disorder Identification Test – Revised; CUD, cannabis use disorder; MAD, median absolute deviation; THC, tetrahydrocannabinol; CBD, cannabidiol; AOR, adjusted odds ratio; FEP, first episode of psychosis.
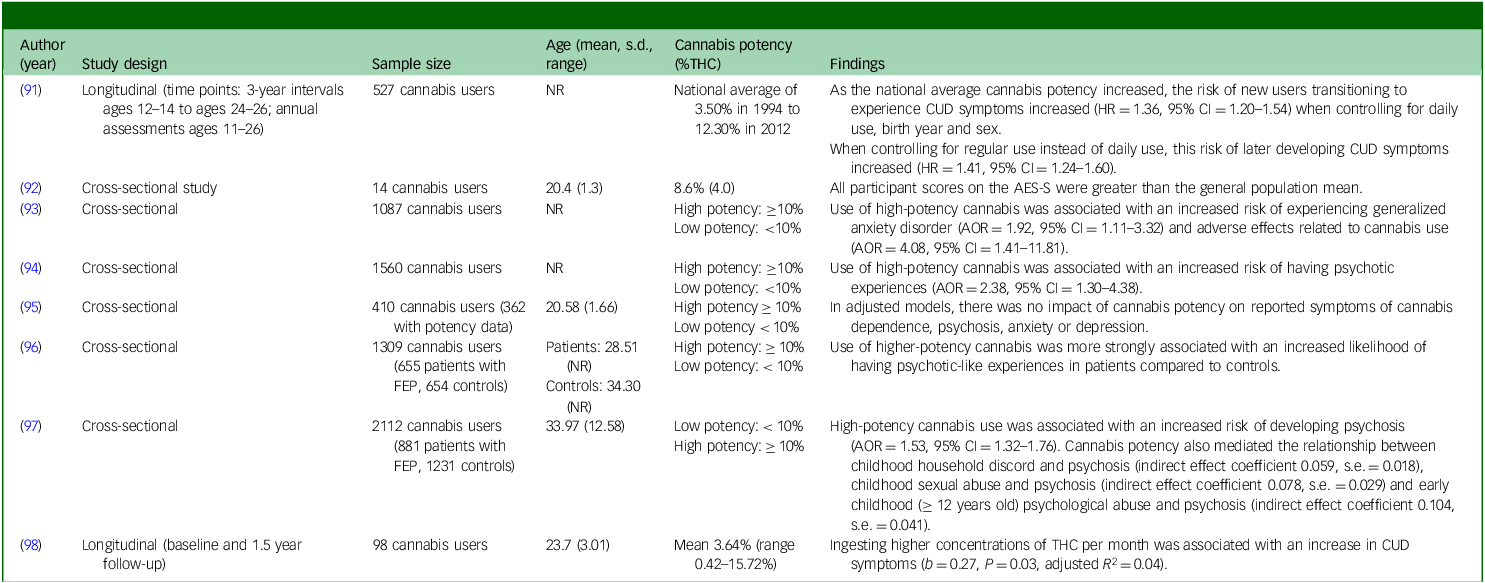
Findings from included studies with results regarding the long-term effects of low-potency cannabis

Table 5 Long description
The table presents data from studies on the long-term effects of low potency cannabis. It includes columns for author (year), study design, sample size, age (mean, standard deviation, range), cannabis potency (percent THC), and findings. The table has 8 rows and 6 columns. Row 1: Author (year): 85; Study design: Longitudinal (time points: 3-year intervals ages 12-14 to ages 24-26; annual assessments ages 11-26); Sample size: 527 cannabis users; Age: NR; Cannabis potency (% THC): National average of 3.50 percent in 1994 to 12.30 percent in 2012; Findings: As the national average cannabis potency increased, the risk of new users transitioning to experience CUD symptoms increased (HR = 1.36, 95% CI = 1.20-1.54) when controlling for daily use, birth year, and sex. When controlling for regular use instead of daily use, this risk of later developing CUD symptoms increased (HR = 1.41, 95% CI = 1.24-1.60). Row 2: Author (year): 86; Study design: Cross sectional study; Sample size: 14 cannabis users; Age: 20.4 (1.3); Cannabis potency (% THC): 8.6 percent (4.0); Findings: All participant scores on the AES-S were greater than the general population mean. Use of high-potency cannabis was associated with an increased risk of experiencing generalized anxiety disorder (AOR = 1.92, 95% CI = 1.11-3.32) and adverse effects related to cannabis use (AOR = 4.08, 95% CI = 1.41-11.81). Row 3: Author (year): 87; Study design: Cross-sectional; Sample size: 1087 cannabis users; Age: NR; Cannabis potency (% THC): High potency: ≥ 10 percent, Low potency: < 10 percent; Findings: Use of high-potency cannabis was associated with an increased risk of having psychotic experiences (AOR = 2.38, 95% CI = 1.30-4.38). Row 4: Author (year): 88; Study design: Cross-sectional; Sample size: 1560 cannabis users; Age: NR; Cannabis potency (% THC): High potency: ≥ 10 percent, Low potency: < 10 percent; Findings: In adjusted models, there was no impact of cannabis potency on reported symptoms of cannabis dependence, psychosis, anxiety, or depression. Row 5: Author (year): 89; Study design: Cross-sectional; Sample size: 410 cannabis users (362 with potency data); Age: 20.58 (1.66); Cannabis potency (% THC): High potency: ≥ 10 percent, Low potency: < 10 percent; Findings: Use of higher potency cannabis was more strongly associated with an increased likelihood of having psychotic-like experiences in patients compared to controls. Row 6: Author (year): 90; Study design: Cross-sectional; Sample size: 1309 cannabis users (655 patients with FEP, 654 controls); Age: Patients: 28.51 (NR), Controls: 34.30 (NR); Cannabis potency (% THC): High potency: >= 10 percent, Low potency: < 10 percent; Findings: High potency cannabis use was associated with an increased risk of developing psychosis (AOR = 1.53, 95% CI = 1.32-1.76). Cannabis potency also mediated the relationship between childhood household discord and psychosis (indirect effect coefficient 0.059, s.e. = 0.018), childhood sexual abuse and psychosis (indirect effect coefficient 0.078, s.e. = 0.029) and childhood (age < 12 years old) psychological abuse and psychosis (indirect effect coefficient 0.104, s.e. = 0.041). Row 7: Author (year): 91; Study design: Cross-sectional; Sample size: 2112 cannabis users (881 patients with FEP, 1231 controls); Age: 33.97 (12.58); Cannabis potency (% THC): Low potency: < 10 percent, High potency: ≥ 10 percent; Findings: High potency cannabis use was associated with an increased risk of developing psychosis (AOR = 1.53, 95% CI = 1.32-1.76). Cannabis potency also mediated the relationship between childhood household discord and psychosis (indirect effect coefficient 0.059, s.e. = 0.018), childhood sexual abuse and psychosis (indirect effect coefficient 0.078, s.e. = 0.029) and childhood (age < 12 years old) psychological abuse and psychosis (indirect effect coefficient 0.104, s.e. = 0.041). Row 8: Author (year): 92; Study design: Longitudinal (Baseline and 1.5 year follow-up); Sample size: 98 cannabis users; Age: 23.7 (3.01); Cannabis potency (% THC): Mean 3.64 percent (range 0.42-15.72 percent); Findings: Ingesting higher concentrations of THC per month was associated with an increase in CUD symptoms (b = 0.27, P = 0.03, adjusted R^2 = 0.04).
THC, tetrahydrocannabinol; NR, not reported; CUD, cannabis use disorder; HR, hazard ratio; AES-S, apathy evaluation scale; AOR, adjusted odds ratio; FEP, first-episode psychosis.
Characteristics of included studies with quantitative potency and acute effects of high-potency cannabis

THC, tetrahydrocannabinol; CBD, cannabidiol.
Long-term effects of HPC
We found that HPC use in the AYA population was most commonly associated with an increased risk and prevalence of cannabis dependence/misuse and an increased prevalence and earlier onset of psychotic disorders. Long-term HPC use was also associated with issues related to sleep quality, mood, cognition and personality, but these outcomes were less commonly reported on.
Problematic substance use and dependence
According to the examined literature, users of HPC, particularly concentrates and high-THC percentage dried flower, exhibit higher levels of cannabis dependence and problematic cannabis use. Studies included report that, when compared with users of LPC products, users of HPC products, such as butane hash oil (BHO), Reference Bedillion, Dharbhamulla and Ansell57,Reference Meier64 cannabis concentrates, Reference Dyar, Green and Rhew58,Reference Meier, Docherty, Leischow, Grimm and Pardini65,Reference Gunn, Aston, Sokolovsky, White and Jackson77–Reference Okey, Waddell and Corbin79 vapes Reference Kumar, Straton and Kaliamurthy80 or high-potency flower Reference Johnson-Ferguson, Loher, Bechtiger, Janousch, Baumgartner and Binz59,Reference Craft, Winstock, Ferris, Mackie, Lynskey and Freeman66,Reference Piercey, Mataczynski, Stallsmith, Emery and Karoly67,Reference Freeman and Winstock81–Reference González-Roz, Secades-Villa, Alemán-Moussa and Iza-Fernández85 are at a higher risk of reporting symptoms of cannabis dependence and/or other problematic substance use. Strong evidence for this relationship is provided by Bedillion et al. Using a longitudinal rather than cross-sectional design, these authors reported that individuals who used BHO at baseline were significantly more likely to develop cannabis dependence symptoms and have experienced negative outcomes related to their cannabis use, in a dose-dependent manner. Reference Bedillion, Dharbhamulla and Ansell57 However, some studies have reported that HPC use is not associated with cannabis dependence measures Reference Dyar, Green, Rhew and Lee60,Reference Van der Pol, Liebregts, de Graaf, Korf, Van den Brink and Van Laar61,Reference Pellegrino, Duck, Kriescher, Shrake, Phillips and Lalonde68–Reference Wade, Wallace, Baca, Andrade, Happer and Courtney70,Reference Schofield, Cuttler, Conner and Prince86 or that HPC use is associated with a decrease in cannabis dependence symptoms. Reference Steeger, Hitchcock, Bryan, Hutchison, Hill and Bidwell69
Psychotic symptoms and psychotic disorders
The second most commonly examined outcome among HPC AYA studies was psychosis/psychotic symptoms. Regarding psychotic symptoms, studies included report that regular use of HPC, such as skunk (16–20% THC 105 ) or cannabis concentrates is associated with having an increased number of psychotic symptoms. Reference Johnson-Ferguson, Loher, Bechtiger, Janousch, Baumgartner and Binz59,Reference Mackie, Wilson, Freeman, Craft, Escamilla De La Torre and Lynskey71–Reference Trotta, Spinazzola, Degen, Li, Austin-Zimmerman and Leung73,Reference Freeman and Winstock81,Reference Hines, Cannings-John, Hawkins, Bonell, Hickman and Zammit87 Regarding psychotic disorders, Di Forti et al found a strong association between HPC use and risk of psychosis. Out of a large sample of patients with first-episode psychosis (N = 280) and controls (N = 174), these authors found that daily users of skunk were significantly more likely to be a part of the patient group than those who used lower-potency cannabis products (odds ratio 12.1, 95% CI = 3.7–37.3 Reference Di Forti, Morgan, Dazzan, Pariante, Mondelli and Marques74 ). This same relationship was observed among non-daily users of HPC as well, albeit to a lower magnitude (odds ratio 5.7, 95% CI = 2.5–12.6 Reference Di Forti, Morgan, Dazzan, Pariante, Mondelli and Marques74 ). In later studies, Di Forti et al found that HPC use was associated with an increased risk of developing a psychotic disorder Reference Di Forti, Marconi, Carra, Fraietta, Trotta and Bonomo62 and that cannabis use of any potency was associated with an earlier onset of psychosis, with the earliest onsets being seen in those who used HPC. Reference Di Forti, Sallis, Allegri, Trotta, Ferraro and Stilo88 In individuals with already diagnosed psychotic disorders, one included study found that regular HPC use was associated with a decline in functioning. Reference Ferraro, Quattrone, La Barbera, La Cascia, Morgan and Kirkbride63 Contrary to these results, one study found that an increase in cannabis flower potency was associated with a decrease in psychotic symptoms, whereas increased concentrate potency was again associated with an increase in psychotic symptoms. Reference Prince and Conner75 Another study similarly found that HPC use was associated with a decreased risk of developing a substance-related psychotic disorder. Reference Matsumoto, Kawabata, Okita, Tanibuchi, Funada and Murakami82 Another reported that participants who regularly used cannabis with higher levels of cannabidiol (CBD) reported fewer psychotic symptoms than those who used HPC. Reference Schubart, Sommer, van Gastel, Goetgebuer, Kahn and Boks72
Other mental health outcomes
One study found that the potency of cannabis concentrates was positively associated with mood symptoms (anger, depression, mania and anxiety), sleep issues, personality disorder symptoms and repetitive thoughts and behaviours. Reference Prince and Conner75 However, this same study found that cannabis flower potency was negatively associated with memory issues, anger and repetitive thoughts and behaviours. Reference Prince and Conner75 Other studies have found that HPC use during AYA is associated with increased depressive and anxious symptoms, Reference Johnson-Ferguson, Loher, Bechtiger, Janousch, Baumgartner and Binz59,Reference Hines, Cannings-John, Hawkins, Bonell, Hickman and Zammit87 heightened aggression, Reference Johnson-Ferguson, Loher, Bechtiger, Janousch, Baumgartner and Binz59 increased risk of suicide, Reference Thomas, Thompson, Maron, Meisel, Spirito and Wolff89 worsened cognitive ability, Reference Wade, Wallace, Huestis, Lisdahl, Sullivan and Tapert76,Reference Freeman and Winstock81,Reference Morgan, Duffin, Hunt, Monaghan, Mason and Curran90 sleep quality degradation Reference Mackie, Wilson, Freeman, Craft, Escamilla De La Torre and Lynskey71 and deficits in occupational functioning. Reference Johnson-Ferguson, Loher, Bechtiger, Janousch, Baumgartner and Binz59 One of the included studies additionally compared the cognitive profile of HPC cannabis users with profiles of AYAs with known psychotic prodromes, finding them to be similar. Reference Morgan, Duffin, Hunt, Monaghan, Mason and Curran90
Acute effects of HPC use
Studies have reported that HPC administered acutely is associated with significant deficits in a number of cognitive domains including processing speed, memory, attention and executive functioning. Other less common outcomes included cannabis craving and mood.
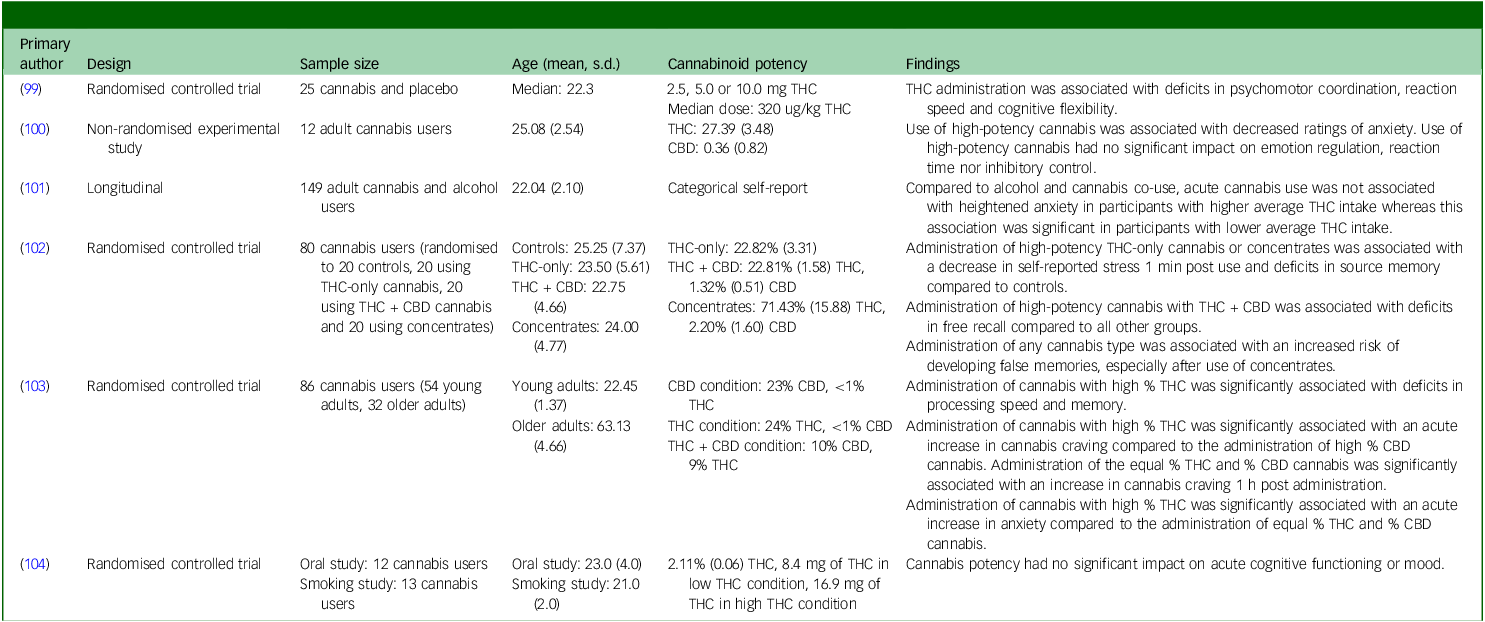
First, Belgrave et al observed that increasing THC doses (2.5, 5.0 and 10.0 mg) significantly impaired individuals’ psychomotor coordination, reaction speed and executive functioning, with effects lasting longer at higher doses. Reference Belgrave, Bird, Chesher, Jackson, Lubbe and Starmer99 Another study found that the administration of cannabis flower with high levels of THC and CBD led to poorer free recall and increased susceptibility to false memories compared with controls and lower-potency conditions. Reference Cuttler, LaFrance and Stueber102 Additionally, cannabis concentrates produced a greater risk of developing false memories. Reference Cuttler, LaFrance and Stueber102 Deficits in memory and processing speed because of increased THC concentrations were also found by another study. Reference Mueller, Ellingson, Cinnamon Bidwell, Bryan and Hutchison103 Regarding anxiety, findings suggest that acute HPC administration is associated with increased cannabis craving and anxiety, Reference Mueller, Ellingson, Cinnamon Bidwell, Bryan and Hutchison103 while other findings suggest that HPC administration is associated with reduced feelings of stress and anxiety. Reference Cavalli, Cuttler and Cservenka100,Reference Cuttler, LaFrance and Stueber102 Another study reported that, compared with alcohol and HPC co-use, acute HPC intake alone was only associated with heightened anxiety among users with a lower average THC intake, Reference Coelho, Hendershot and Wardell101 indicating that the effects of HPC on anxiety might be most pronounced among individuals who are light cannabis users. Null findings regarding the impact of acute HPC use were reported by multiple studies, specifically regarding changes in cognition and mood. Reference Cavalli, Cuttler and Cservenka100,Reference Wachtel, ElSohly, Ross, Ambre and De Wit104
Sex differences
The secondary aim of this review was to examine what evidence exists regarding sex and/or gender differences in the impact that cannabis potency has on AYA mental health outcomes. Unfortunately, sex and/or gender differences are highly underreported, with clear definitions of these constructs being even less common. Out of all included studies, only 14 explicitly assessed how sex could affect the relationship between cannabis potency and mental health outcomes in AYA, Reference Lane, Cherek, Tcheremissine, Lieving and Pietras34–Reference Metrik, Aston, Kahler, Rohsenow, McGeary and Knopik39,Reference Dyar, Green and Rhew58,Reference Dyar, Green, Rhew and Lee60,Reference Trotta, Spinazzola, Degen, Li, Austin-Zimmerman and Leung73,Reference Gunn, Aston, Sokolovsky, White and Jackson77,Reference Najera, Cavalli and Cservenka78,Reference Freeman and Winstock81,Reference Di Forti, Sallis, Allegri, Trotta, Ferraro and Stilo88,Reference Thomas, Thompson, Maron, Meisel, Spirito and Wolff89 with only one reporting a significant impact of sex and/or gender on HPC and mental health outcomes. This study found that females were more susceptible to paranoid symptom development than males. Reference Trotta, Spinazzola, Degen, Li, Austin-Zimmerman and Leung73
Discussion
The primary purpose of this scoping review was to summarise the existing literature regarding the impact of cannabis potency on AYA mental health outcomes. The summary provided here suggests that the use of HPC has both long-term and acute mental health effects. According to the studies reviewed here, the most common long-term effects of HPC use include: a higher risk of problematic cannabis use, Reference Bedillion, Dharbhamulla and Ansell57,Reference Meier64,Reference Craft, Winstock, Ferris, Mackie, Lynskey and Freeman66,Reference Piercey, Mataczynski, Stallsmith, Emery and Karoly67 a higher risk – and earlier onset – of psychosis and psychotic symptoms Reference Mackie, Wilson, Freeman, Craft, Escamilla De La Torre and Lynskey71,Reference Schubart, Sommer, van Gastel, Goetgebuer, Kahn and Boks72,Reference Di Forti, Morgan, Dazzan, Pariante, Mondelli and Marques74 and other adverse mental health outcomes, Reference Meier, Docherty, Leischow, Grimm and Pardini65,Reference Mackie, Wilson, Freeman, Craft, Escamilla De La Torre and Lynskey71,Reference Prince and Conner75 while common acute effects of HPC include: cognitive deficits, Reference Belgrave, Bird, Chesher, Jackson, Lubbe and Starmer99,Reference Cuttler, LaFrance and Stueber102,Reference Mueller, Ellingson, Cinnamon Bidwell, Bryan and Hutchison103,Reference Rudisill, Innes, Wen, Haggerty and Smith106 increased cannabis craving, Reference Mueller, Ellingson, Cinnamon Bidwell, Bryan and Hutchison103 increased anxiety Reference Mueller, Ellingson, Cinnamon Bidwell, Bryan and Hutchison103 and decreased stress levels. Reference Cuttler, LaFrance and Stueber102 However, there were a portion of studies which found that cannabis potency had no impact on mental health outcomes, Reference Van der Pol, Liebregts, de Graaf, Korf, Van den Brink and Van Laar61,Reference Pellegrino, Duck, Kriescher, Shrake, Phillips and Lalonde68,Reference Steeger, Hitchcock, Bryan, Hutchison, Hill and Bidwell69,Reference Schofield, Cuttler, Conner and Prince86,Reference Wachtel, ElSohly, Ross, Ambre and De Wit104 which invites caution when trying to make sweeping conclusions regarding the impact of AYA HPC use on these outcomes.
The secondary aim of this review was to collate information regarding the impact that sex and/or gender has on the relationship between cannabis potency and mental health outcomes in AYA. Unfortunately, only 14 of the studies discussed here explicitly assessed sex and/or gender effects. Reference Lane, Cherek, Tcheremissine, Lieving and Pietras34–Reference Metrik, Aston, Kahler, Rohsenow, McGeary and Knopik39,Reference Dyar, Green and Rhew58,Reference Dyar, Green, Rhew and Lee60,Reference Trotta, Spinazzola, Degen, Li, Austin-Zimmerman and Leung73,Reference Gunn, Aston, Sokolovsky, White and Jackson77,Reference Najera, Cavalli and Cservenka78,Reference Freeman and Winstock81,Reference Di Forti, Sallis, Allegri, Trotta, Ferraro and Stilo88,Reference Thomas, Thompson, Maron, Meisel, Spirito and Wolff89 Of this subset, only one found that the relationship between HPC use and AYA mental health outcomes was moderated by sex. Reference Trotta, Spinazzola, Degen, Li, Austin-Zimmerman and Leung73 Although these results could suggest that sex and/or gender has little impact on the relationship between cannabis potency and mental health outcomes in AYA, no strong conclusions can be made until further high-quality research on this topic is conducted. Apart from the lack of research examining sex and/or gender, what is additionally concerning is the fact that, despite having an explicit focus on sex and/or gender in their analyses, many of the aforementioned studies did not clearly define what the terms ‘sex’ and/or ‘gender’ meant in the context of their study. Delineating between these two constructs is important if we are ever to understand how someone’s sex and/or gender can impact AYA HPC use and outcomes.
The strengths of this scoping review include our search strategies, which were comprehensive and developed with the help of evidence synthesis librarians, and our use of two independent reviewers for the screening and extraction of sources. Together, we believe that these factors allow this review to provide a broad overview of existing research surrounding the effect that cannabis potency has on the mental health of AYA. However, our adherence to a scoping review methodology comes with inherent limitations. The first of which is that we did not assess the quality of included sources. While this would have provided information important for the purposes of making conclusions, such was not the goal of the current review. Our inclusion criteria were also quite lenient, introducing a great deal of heterogeneity to our results. Including assessments of sources and more strict inclusion criteria, both of which are common to systematic reviews, could have improved the interpretability and robustness of our results. However, the goal of the current review was not to answer the question of the effect of cannabis potency on the mental health of AYA, but to summarise the evidence that exists to address this question. Due to this aim, none of the conclusions made here are causal in nature.
Given the emerging evidence reviewed here and cannabis’ changing legal status in multiple jurisdictions, it would be suggested that researchers and governing bodies monitor product potency from a public health perspective. Currently, in Canada, the THC limit of edible cannabis is 10 mg per package while extracts can contain 1000 mg per package. 107 While these limits provide some control, they may not be sufficient to address concerns related to high-potency products. Considering that extracts can contain significantly higher amounts of THC, stricter limits or additional controls specifically targeting younger users may be warranted. Reducing access to HPC for younger populations could lead to the decreased incidence of cannabis-related cognitive and mental health issues. However, despite these quality control measures, a recent study found that one-third of cannabis products sold in Ontario, Canada had discrepancies between online cannabinoid potency descriptions and the potency of the actual product. Reference Doggett, Fein, Campbell, Henriquez, Busse and MacKillop108 This study reported that 16.7% of cannabis products in Ontario had physical labels that reported higher THC potency of the advertised product. Reference Doggett, Fein, Campbell, Henriquez, Busse and MacKillop108 Research such as this emphasises that governing bodies should ensure that cannabis distributors are accurately reporting the THC content of their products so that potency can be properly monitored and studied.
The increasing prevalence of cannabis use among youth, along with the significant rise in cannabis potency in recent years, calls for targeted research and education regarding its effects on mental health. As cannabis products become more potent, understanding their impact on developing brains and mental well-being is critical. There is a pressing need for enhanced investment in educational programmes tailored to different age groups, focusing on the risks associated with HPC and its potential effects on mental health. Such initiatives would help equip young people with the knowledge to make informed decisions and better navigate the potential risks associated with cannabis use. Considering that AYA can access HPC outside the legal market, it is also important for governments to implement measures to limit this exposure. Synthetic cannabinoids (i.e. spice, K2) must also be the focus of future research assessing the impact of AYA cannabinoid exposure on acute- and long-term mental health outcomes
In this review, our primary aim was to collate extant literature reporting the long-term and acute mental health effects of HPC use in AYA. Included studies most commonly reported that, compared with LPC use, HPC use in AYA is associated with an increased risk of psychosis/psychotic symptoms, problematic cannabis use and cognitive deficits. Our review also noted the almost complete lack of literature on the potential of sex and/or gender to moderate the relationship between cannabis potency and mental health outcomes in AYA, as well as the ambiguity with which researchers define sex and gender. We strongly recommend that future studies assessing the impact of cannabis on mental health also consider how the potency of products might influence their findings and include sex and/or gender-based analyses into their designs.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12023
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Acknowledgements
We would like to acknowledge the assistance of the reference librarians of Dalhousie University in the creation of our protocol and search terms.
Author contributions
C.H.L., C.E.C. and P.G.T. formulated the research question and protocol of the review. C.H.L. and L.N. equally contributed to the screening of all sources derived by the search and the extraction of relevant data, with C.E.C. or P.G.T. acting as a third reviewer when needed. C.H.L. wrote the initial draft of the manuscript based on the first literature search, with L.N., P.G.T. and C.E.C. making substantial edits to this manuscript and adding the data derived from the secondary search. The final version of the manuscript was approved and agreed upon by all authors.
Funding
This review was funded by a grant provided by the Government of Alberta, Canada.
Declaration of interest
None.
Appendix A
MEDLINE (Ovid) – 3 June 2024
-
1. adolescent/ OR ‘young adult’/ OR (teen* OR youth* OR adolescen* OR juvenile* OR (young ADJ2 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) ADJ2 (school* OR education))).kf,ti,ab.
-
2. exp cannabinoids/ OR exp cannabis/ OR exp ‘marijuana abuse’/ OR exp ‘marijuana use’/ OR exp ‘medical marijuana’/ OR (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*).kf,ti,ab.
-
3. (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’).kf,ti,ab.
-
4. exp mental disorders/ OR ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’).kf,ti,ab.
-
5. 1 AND 2 AND 3 AND 4
-
6. exp Animals/ NOT (exp Animals/AND Humans/)
-
7. (news OR comment OR editorial OR interview OR letter OR proceedings).pt.
-
8. 5 NOT 6 NOT 7
MEDLINE (Ovid) – 3 October 2025
-
1. adolescent/ OR ‘young adult’/ OR (teen* OR youth* OR adolescen* OR juvenile* OR (young ADJ2 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) ADJ2 (school* OR education))).kf,ti,ab.
-
2. exp cannabinoids/ OR exp cannabis/ OR exp ‘marijuana abuse’/ OR exp ‘marijuana use’/ OR exp ‘medical marijuana’/ OR (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*).kf,ti,ab.
-
3. (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’).kf,ti,ab.
-
4. exp mental disorders/ OR ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’).kf,ti,ab.
-
5. 1 AND 2 AND 3 AND 4
-
6. exp Animals/ NOT (exp Animals/ AND Humans/)
-
7. (news OR comment OR editorial OR interview OR letter OR proceedings).pt.
-
8. 5 NOT 6 NOT 7
-
9. limit 8 to yr=’2024 -Current’
Embase (Elsevier) – 3 June 2024
-
1. ‘adolescent’/exp OR ‘young adult’/exp OR (teen* OR youth* OR adolescen* OR juvenile* OR (young NEAR/1 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) NEAR/1(school* OR education))):kw,ti,ab
-
2. ‘cannabis’/exp OR ‘cannabinoid’/exp OR ‘cannabis use’/exp OR ‘cannabis addiction’/exp OR ‘cannabis sativa’/exp OR ‘medical cannabis’/exp OR (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*):kw,ti,ab
-
3. (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’):kw,ti,ab
-
4. ‘mental disease’/exp OR ((mental OR psych* OR cogniti* OR panic OR eating OR mood OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘substance use’ OR ‘Obsessive?Compulsive’) NEAR/1 (ill* OR disord* OR condition* OR disab*) OR bipolar OR anx* or depres* OR schizo* OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR phobia OR ‘substance abuse’ OR ‘substance misuse’ OR ‘panic attack*’ OR ‘gender dysphor*’):kw,ti,ab
-
5. 1 AND 2 AND 3 AND 4
-
6. (news OR comment OR editorial OR interview OR letter OR proceedings):it
-
7. ‘animal experiment’/de NOT (‘human experiment’/de OR ‘human’/de)
-
8. 5 NOT 6 NOT 7
Embase (Elsevier) – 3 October 2025
-
1. ‘adolescent’/exp OR ‘young adult’/exp OR (teen* OR youth* OR adolescen* OR juvenile* OR (young NEAR/1 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) NEAR/1(school* OR education))):kw,ti,ab
-
2. ‘cannabis’/exp OR ‘cannabinoid’/exp OR ‘cannabis use’/exp OR ‘cannabis addiction’/exp OR ‘cannabis sativa’/exp OR ‘medical cannabis’/exp OR (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*):kw,ti,ab
-
3. (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’):kw,ti,ab
-
4. ‘mental disease’/exp OR ((mental OR psych* OR cogniti* OR panic OR eating OR mood OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘substance use’ OR ‘Obsessive?Compulsive’) NEAR/1 (ill* OR disord* OR condition* OR disab*) OR bipolar OR anx* or depres* OR schizo* OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR phobia OR ‘substance abuse’ OR ‘substance misuse’ OR ‘panic attack*’ OR ‘gender dysphor*’):kw,ti,ab
-
5. 1 AND 2 AND 3 AND 4
-
6. (news OR comment OR editorial OR interview OR letter OR proceedings):it
-
7. ‘animal experiment’/de NOT (‘human experiment’/de OR ‘human’/de)
-
8. 5 NOT 6 NOT 7
-
9. #8 AND (2024:py OR 2025:py)
CINAHL (EBSCO) – 3 June 2024
-
1. (MH ‘Adolescence’) OR (MH ‘Young Adult’) OR TI (teen* OR youth* OR adolescen* OR juvenile* OR (young N1(adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) N1 (school* OR education))) OR AB (teen* OR youth* OR adolescen* OR juvenile* OR (young N1 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) N1 (school* OR education)))
-
2. (MH ‘Medical Marijuana’) OR (MH ‘Cannabidiol’) OR (MH ‘Cannabis+’) OR TI (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THCOR hemp* OR bhang*) OR AB (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THCOR hemp* OR bhang*)
-
3. TI (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’) OR AB (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’)
-
4. (MH ‘Behavioral and Mental Disorders+’) OR TI ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’) OR AB ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition*OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’)
-
5. 1 AND 2 AND 3 AND 4
-
6. PT (news OR comment OR editorial OR interview OR letter OR proceedings)
-
7. TI ((animal OR animals OR canine* OR dog OR dogs OR feline OR hamster* OR lamb OR lambs OR mice OR monkey OR monkeys OR mouse OR murine OR pig OR pigs OR piglet* OR porcine OR primate* OR rabbit* OR rats OR rat OR rodent* OR sheep*) NOT (human* OR patient*))
-
8. AB ((animal OR animals OR canine* OR dog OR dogs OR feline OR hamster* OR lamb OR lambs OR mice OR monkey OR monkeys OR mouse OR murine OR pig OR pigs OR piglet* OR porcine OR primate* OR rabbit* OR rats OR rat OR rodent* OR sheep*) NOT (human* OR patient*))
-
9. 5 NOT 6 NOT 7 NOT 8
CINAHL (EBSCO) – 3 October 2025
-
1. (MH ‘Adolescence’) OR (MH ‘Young Adult’) OR TI (teen* OR youth* OR adolescen* OR juvenile* OR (young N1(adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) N1 (school* OR education))) OR AB (teen* OR youth* OR adolescen* OR juvenile* OR (young N1 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) N1 (school* OR education)))
-
2. (MH ‘Medical Marijuana’) OR (MH ‘Cannabidiol’) OR (MH ‘Cannabis+’) OR TI (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THCOR hemp* OR bhang*) OR AB (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THCOR hemp* OR bhang*)
-
3. TI (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’) OR AB (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’)
-
4. (MH ‘Behavioral and Mental Disorders+’) OR TI ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’) OR AB ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition*OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’)
-
5. 1 AND 2 AND 3 AND 4
-
6. PT (news OR comment OR editorial OR interview OR letter OR proceedings)
-
7. TI ((animal OR animals OR canine* OR dog OR dogs OR feline OR hamster* OR lamb OR lambs OR mice OR monkey OR monkeys OR mouse OR murine OR pig OR pigs OR piglet* OR porcine OR primate* OR rabbit* OR rats OR rat OR rodent* OR sheep*) NOT (human* OR patient*))
-
8. AB ((animal OR animals OR canine* OR dog OR dogs OR feline OR hamster* OR lamb OR lambs OR mice OR monkey OR monkeys OR mouse OR murine OR pig OR pigs OR piglet* OR porcine OR primate* OR rabbit* OR rats OR rat OR rodent* OR sheep*) NOT (human* OR patient*))
-
9. 5 NOT 6 NOT 7 NOT 8
-
10. Limited publication date to: 20240601-20251231
PsycINFO (EBSCO) – 3 June 2024
-
1. DE ‘Emerging Adulthood’ OR DE ‘Adolescent Development’ OR DE ‘Adolescent Behavior’ OR DE ‘Adolescent Characteristics’ OR DE ‘Adolescent Health’ OR DE ‘Late Adolescence’ OR DE ‘Youth Mental Health’ OR TI ((teen* OR youth* OR adolescen* OR juvenile* OR (young N2 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) N2 (school* OR education)))) OR AB ((teen* OR youth* OR adolescen* OR juvenile* OR (young N2 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) N2 (school* OR education))))
-
2. DE ‘Cannabis’ OR DE ‘Cannabinoids’ OR DE ‘Hashish’ OR DE ‘Marijuana’ OR DE ‘Medical Marijuana’ OR TI (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*) OR AB (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*)
-
3. TI (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’) OR AB (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’)
-
4. DE ‘Mental Disorders’ OR DE ‘Affective Disorders’ OR DE ‘Anxiety Disorders’ OR DE ‘Behavior Disorders’ OR DE ‘Bipolar Disorder’ OR DE ‘Borderline States’ OR DE ‘Chronic Mental Illness’ OR DE ‘Dissociative Disorders’ OR DE ‘Eating Disorders’ OR DE ‘Gender Dysphoria’ OR DE ‘Mental Disorders due to General Medical Conditions’ OR DE ‘Neurocognitive Disorders’ OR DE ‘Neurodevelopmental Disorders’ OR DE ‘Neurosis’ OR DE ‘Obsessive Compulsive Disorder’ OR DE ‘Paraphilias’ OR DE ‘Personality Disorders’ OR DE ‘Psychosis’ OR DE ‘Serious Mental Illness’ OR DE ‘Sleep Wake Disorders’ OR DE ‘Somatoform Disorders’ OR DE ‘Stress and Trauma Related Disorders’ OR DE ‘Substance Related and Addictive Disorders’ OR DE ‘Thought Disorders’ OR DE ‘Youth Suicide’ OR DE ‘Abnormal Psychology’ OR DE ‘Attention Deficit Disorder’ OR DE ‘Attention Deficit Disorder with Hyperactivity’ OR DE ‘Suicide’ OR TI ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’) OR AB ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’)
-
5. 1 AND 2 AND 3 AND 4
-
6. PT (news OR comment OR editorial OR interview OR letter OR proceedings)
-
7. TI ((animal OR animals OR canine* OR dog OR dogs OR feline OR hamster* OR lamb OR lambs OR mice OR monkey OR monkeys OR mouse OR murine OR pig OR pigs OR piglet* OR porcine OR primate* OR rabbit* OR rats OR rat OR rodent* OR sheep*) NOT (human* OR patient*))
-
8. AB ((animal OR animals OR canine* OR dog OR dogs OR feline OR hamster* OR lamb OR lambs OR mice OR monkey OR monkeys OR mouse OR murine OR pig OR pigs OR piglet* OR porcine OR primate* OR rabbit* OR rats OR rat OR rodent* OR sheep*) NOT (human* OR patient*))
-
9. 5 NOT 6 NOT 7 NOT 8
PsycINFO (Ovid) – 3 October 2025
-
1. exp Adolescent Behavior/ or exp Adolescent Development/ or exp Adolescent Characteristics/ or exp Adolescent Health/ OR exp Emerging Adulthood/ OR exp Late Adolescence/ OR exp Youth Mental Health/ OR (teen* OR youth* OR adolescen* OR juvenile* OR (young ADJ2 (adult* OR person* OR individual* OR people* OR population* OR man OR men OR wom?n)) OR youngster* OR highschool* OR college* OR ((secondary OR high*) ADJ2 (school* OR education))).hw,ti,ab.
-
2. exp Cannabis/ OR exp Cannabinoids/ OR exp Hashish/ OR exp Marijuana/ OR exp Medical Marijuana/ OR (cannabi* OR dronabinol OR hash* OR mari?uana* OR tetrahydrocannabi* OR THC OR hemp* OR bhang*).hw,ti,ab.
-
3. (strength OR strong OR concentrat* OR mass OR potency OR potent OR ‘%THC’ OR ‘% THC’ OR percent* OR ‘mg THC’ OR ‘mgTHC’ OR ‘THC:CBD ratio’ OR quanti* OR content OR milligram* OR ‘mg’).hw,ti,ab.
-
4. exp Mental Disorders/ OR exp Affective Disorders/ OR exp Anxiety Disorders/ OR exp Behavior Disorders/ OR exp Bipolar Disorder/ OR exp Borderline States/ OR exp Chronic Mental Illness/ OR exp Dissociative Disorders/ OR exp Eating Disorders/ OR exp Gender Dysphoria/ OR exp Mental Disorders due to General Medical Conditions/ OR exp Neurocognitive Disorders/ OR exp Neurodevelopmental Disorders/ OR exp Neurosis/ OR exp Obsessive Compulsive Disorder/ OR exp Paraphilias/ OR exp Personality Disorders/ OR exp Psychosis/ OR exp Serious Mental Illness/ OR exp Sleep Wake Disorders/ OR exp Somatoform Disorders/ OR exp Stress and Trauma Related Disorders/ OR exp Substance Related and Addictive Disorders/ OR exp Thought Disorders/ OR exp Youth Suicide/ OR exp Abnormal Psychology/ OR exp Attention Deficit Disorder/ OR exp Attention Deficit Disorder with Hyperactivity/ OR exp Suicide/ OR ((psych* OR mental OR cogniti* OR panic OR eating OR mood OR ‘substance use’ OR conduct OR personality OR ‘attention?deficit?hyperactive’ OR ‘Obsessive?Compulsive’) ADJ1 (ill* OR disord* OR condition* OR disab*) OR anx* OR depres* OR schizo* OR bipolar OR suicid* OR anorex* OR agoraphob* OR PTSD OR post?traumatic?stress* OR bulimi* OR ADHD OR OCD OR delusions OR hallucinations OR ‘substance abuse’ OR ‘substance misuse’ OR phobia OR ‘panic attack*’ OR ‘gender dysphori*’).hw,ti,ab.
-
5. 1 AND 2 AND 3 AND 4
-
6. exp Animals/ NOT (exp Animals/ AND Humans/)
-
7. (news OR comment OR editorial OR interview OR letter OR proceedings).pt.
-
8. 5 NOT 6 NOT 7
-
9. limit 8 to yr=‘2024 -Current’



 Open access
Open access
eLetters
No eLetters have been published for this article.