


Recovery Colleges are adult education initiatives that use a personal recovery-oriented approach to support individuals with mental health difficulties. Unlike traditional clinical interventions focused on symptom reduction and relapse prevention, Recovery Colleges emphasise peer support, personal strengths and skills development. Courses are co-produced and co-facilitated by individuals with mental health lived experience alongside topic experts, helping to reduce stigma and avoiding the power imbalances in clinical settings. Single-site studies have identified that participation in Recovery Colleges is associated with improved self-esteem, identity, hope, social connections, lifestyle, quality of life and goal attainment.Reference Allard, Pollard, Laugharne, Coates, Wildfire-Roberts and Millward 1 – Reference Wilson, King and Russell 3 The first Recovery College opened in England in 2009 and, by 2022, there were around 221 Recovery Colleges across 28 countries.Reference Hayes, Hunter-Brown, Camacho, McPhilbin, Elliott and Ronaldson 4 England has the most Recovery Colleges, with 88 identified in a 2021 national survey, attended by roughly 36 000 students annually.Reference Hayes, Camacho, Ronaldson, Stepanian, McPhilbin and Elliott 5 Although most Recovery Colleges are open for all adults to attend, some of those affiliated with mental health trusts limit eligibility to current or recent trust service users, their carers and staff. ‘Service user students’ – college students who also use mental health services – can thus be found across all Recovery Colleges. The Recovery Colleges Characterisation and Testing 2 (RECOLLECT 2) research programmeReference Hayes, Henderson, Bakolis, Lawrence, Elliott and Ronaldson 6 aims to assess the effectiveness of Recovery Colleges for such service user students. The foundational research programme RECOLLECT 1 developed the 12-item, manager-rated RECOLLECT Fidelity Measure (RFM),Reference Toney, Knight, Hamill, Taylor, Henderson and Crowther 7 which was included in the national survey of Recovery Colleges in England.Reference Hayes, Camacho, Ronaldson, Stepanian, McPhilbin and Elliott 5 Cluster analysis, including RFM responses, organisational factors and student characteristics, identified three Recovery College types: strengths-oriented (located within National Health Service (NHS) Trusts, emphasising student strengths and structured recovery planning); community-oriented (operate in non-NHS settings, with a greater emphasis on social connection and community integration); and forensic, with the majority (>95%) of Recovery Colleges being either strengths- or community-oriented.Reference Hayes, Camacho, Ronaldson, Stepanian, McPhilbin and Elliott 5
The aims of this study were to (a) characterise a nationwide inception cohort of mental health service user students in relation to sociodemographic and clinical characteristics, health service use and student outcomes; and (b) evaluate differences across our two empirically identified main categories of Recovery College by comparing service user students attending strengths-oriented with those attending community-oriented Recovery Colleges.
Method
Participants and study design
In this study we present baseline data from a longitudinal pre–post observational study of Recovery Colleges in England that was conducted as part of the National Institute for Health and Care Research (NIHR) programme grant RECOLLECT 2 (www.researchintorecovery.com/recollect). A protocol for this study has been published elsewhere,Reference Hayes, Henderson, Bakolis, Lawrence, Elliott and Ronaldson 6 and details of the empirically identified Recovery College categories are available.Reference Hayes, Camacho, Ronaldson, Stepanian, McPhilbin and Elliott 5 Recovery Colleges were purposively sampled to maximise variation across Recovery College type and geographical region. We recruited from Recovery Colleges across the nine governmental regions of England: East of England, East Midlands, London, North-East, North-West, South-East, South-West, West Midlands, Yorkshire and the Humber.
Participants were adult (≥18 years) Recovery College students who were (a) current service users at local NHS mental health trusts and (b) newly registered at the Recovery College, defined as someone who had completed no more than one class or workshop at the time of providing consent. Participants completed survey assessments at baseline and at 4, 8 and 12 months. In this paper we describe the baseline cohort characteristics by Recovery College type. Because there was only one student from a forensic college in the sample, we compared students from strengths-oriented Recovery Colleges with those from community-oriented Recovery Colleges only. All participants provided informed written consent. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013. All procedures involving human subjects/patients were approved by Greater Manchester West Research Ethics Committee (no. 22/NW/0091, 15 May 2022).
Procedure
A bespoke recruitment plan to obtain an inception cohort of student participants was created with senior staff members at each participating Recovery College. All newly registering Recovery College students were made aware of the study by the Recovery College displaying information on their website, posters/leaflets by researchers attending the college and by Recovery College staff at the point of registration. If interested, their contact details were passed to the research team or, alternatively, students could contact the research team directly. Interested students met with the researcher, either face to face or via video call, telephone or email, who explained the study, established eligibility and provided a participant information sheet. After addressing any questions, students were asked to sign or verbally confirm the consent form. Research assistants used flexible, proactive engagement to facilitate involvement, conducting assessments through a variety of methods including emailed hyperlinks to online questionnaires, hardcopy, face to face and phone/video calls. All questionnaires were linked to a unique ID reference number. Additionally, students were asked to provide optional consent for the research team to access their electronic medical records, in order for the team to gather service use data for the preceding 4 months of each questionnaire time point. It was made clear to students that they could still participate in the study even if they did not allow access to their medical records.
Measures
Sociodemographic and clinical variables
Self-reported sociodemographic variables were age, gender, ethnicity, employment status, education/qualifications and housing status. Self-reported clinical variables were disability status, primary mental health diagnosis, time since contact with mental health services and whether the participant had ever been detained under the Mental Health Act. A copy of the study assessment can be found in the supplementary materials. Although detailed ethnicity data were collected, we report these data in aggregated categories due to the small sample sizes in some groups.
Self-rated student outcomes
The primary outcome was the 12-item Manchester Short Assessment (MANSA) to measure quality of life.Reference Priebe, Huxley, Knight and Evans 8 This comprises a 7-point Likert scale, with sum scores ranging from 12 (low quality of life) to 84 (high quality of life). MANSA has good psychometric properties, including internal consistency and validity. Secondary outcome measures were as follows: the 16-item Mental Health Confidence Scale (MHCS) to measure self-efficacy;Reference Carpinello, Knight, Markowitz and Pease 9 the 5-item Brief INSPIRE-O to measure personal recovery;Reference Moeller, Larsen, Austin, Slade, Arendt and Andersen 10 the 6-item Brief Resilience Scale to measure resilience;Reference Smith, Dalen, Wiggins, Tooley, Christopher and Bernard 11 the 12-item Herth Hope Index (HHI) to measure hope;Reference Herth 12 the 7-item Short Warwick–Edinburgh Mental Wellbeing Scale (SWEMWBS) to measure mental well-being;Reference Stewart-Brown, Tennant, Tennant, Platt, Parkinson and Weich 13 the 6-item Lubben Social Network Scale to measure social engagement,Reference Lubben, Blozik, Gillmann, Iliffe, von Renteln Kruse and Beck 14 modified to include 3 additional questions about acquaintances; the 16-item Social Inclusion Scale to measure social inclusion; Reference Secker, Hacking, Kent, Shenton and Spandler15 and EQ-5D-5L, including the visual analogue scale, to measure health status Reference Herdman, Gudex, Lloyd, Janssen, Kind and Parkin16 (mapped to the EQ-5D-3L value set, Reference Hernández-Alava and Pudney17 as required by the National Institute for Health and Care Excellence reference case, using an established mapping method Reference Dolan18 ). Because the current mapping method does not allow for the inclusion of gender other than male and female, EQ-5D-5L values were treated as missing where gender was recorded as non-binary or missing. All outcome measures have established psychometric properties.
Self-reported health service use
Health service use was assessed using a study-specific service use questionnaire modified from the Client Service Receipt Inventory. Reference Chisholm, Knapp, Knudsen, Amaddeo, Gaite and van Wijngaarden19 Participants were asked to fill in questions relating to their service use for the 4 months preceding the baseline assessment. The following aspects of service use were assessed: use of emergency departments, including whether transported by an ambulance and whether admitted or sent home; use of hospital in-patient services, including number of nights admitted; use of mental health services, including professional group seen and number of contacts; other hospital visits, including department/reason and number of visits; and primary care visits.
Analysis
Sociodemographic, clinical, student outcome and health service use variables were summarised as means and standard deviations, medians and interquartile ranges, and frequencies (%). We present results for the overall sample, as well as for students who registered at strengths- and community-oriented Recovery Colleges (forensic Recovery College students were excluded due to insufficient sample size). Complete case analysis was used to measure differences between strengths- and community-oriented Recovery College students on all outcomes. Due to the hierarchical nature of the data, with students nested in 34 different Recovery Colleges, multi-level analysis was used to assess differences in sociodemographic and clinical characteristics, self-rated student outcomes and self-reported health service use between Recovery College types. Specifically, we employed 2-level random intercept regression models, with students at level 1 and colleges at level 2. Depending on the distribution of the outcome variable, we used linear mixed-effects (mixed), binary logistic (melogit) and negative binomial (menbreg) regression models. As a sensitivity analysis to investigate whether missing data on student self-rated outcomes had introduced bias, we employed mean and median imputation where appropriate. This method involved substituting each missing value with the average (mean or median) of the observed values for that specific outcome. All analyses were performed using STATA 18.0 for Windows (Stata Corp LLP, College Station, Texas, USA).
Involvement of people with lived experience
The outcome measures for this study were selected using a two-stage process, each involving people with lived experience of, or providing informal support to someone with, mental ill health. Several also had been students or worked at a Recovery College. The first stage was the co-production of a change model for Recovery Colleges involving the RECOLLECT 2 Lived Experience Advisory Panel (LEAP) Reference Toney, Elton, Munday, Hamill, Crowther and Meddings20 that specified mechanisms of actions and outcomes for students. Reference Jennings, Slade, Bates, Munday and Toney21 The second stage comprised selection of a provisional set of outcome measures by the research team, which was then scrutinised by RECOLLECT 2 LEAP, membership of which comprised some from RECOLLECT 1 LEAP and some new members. Certain measures were then replaced, having been rejected by LEAP members as not having acceptable wording and/or not being a sufficiently close fit to outcomes in the change model. RECOLLECT 2 LEAP provided feedback on all Recovery College student-facing study documents, advised on student recruitment methods and supported student recruitment in some instances.
Results
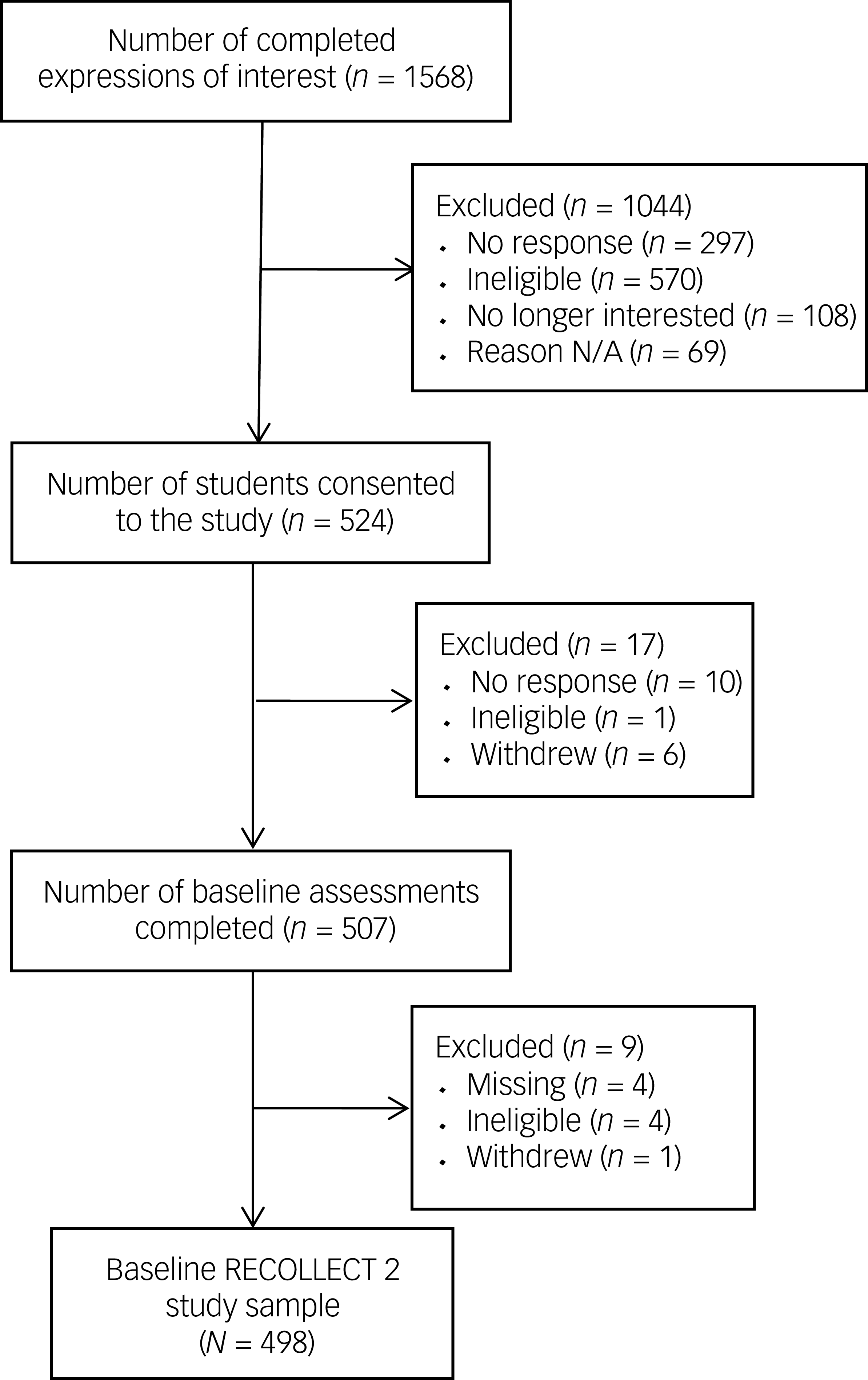
Recruitment of the RECOLLECT 2 cohort is shown in Fig. 1. Among the reasons for ineligibility at any stage of recruitment were identification as Recovery College staff, lack of current service user status and attendance at more than one Recovery College class prior to providing consent or completing the survey.
Recovery Colleges Characterisation and Testing 2 (RECOLLECT 2), recruitment and baseline data collection. N/A, not available.

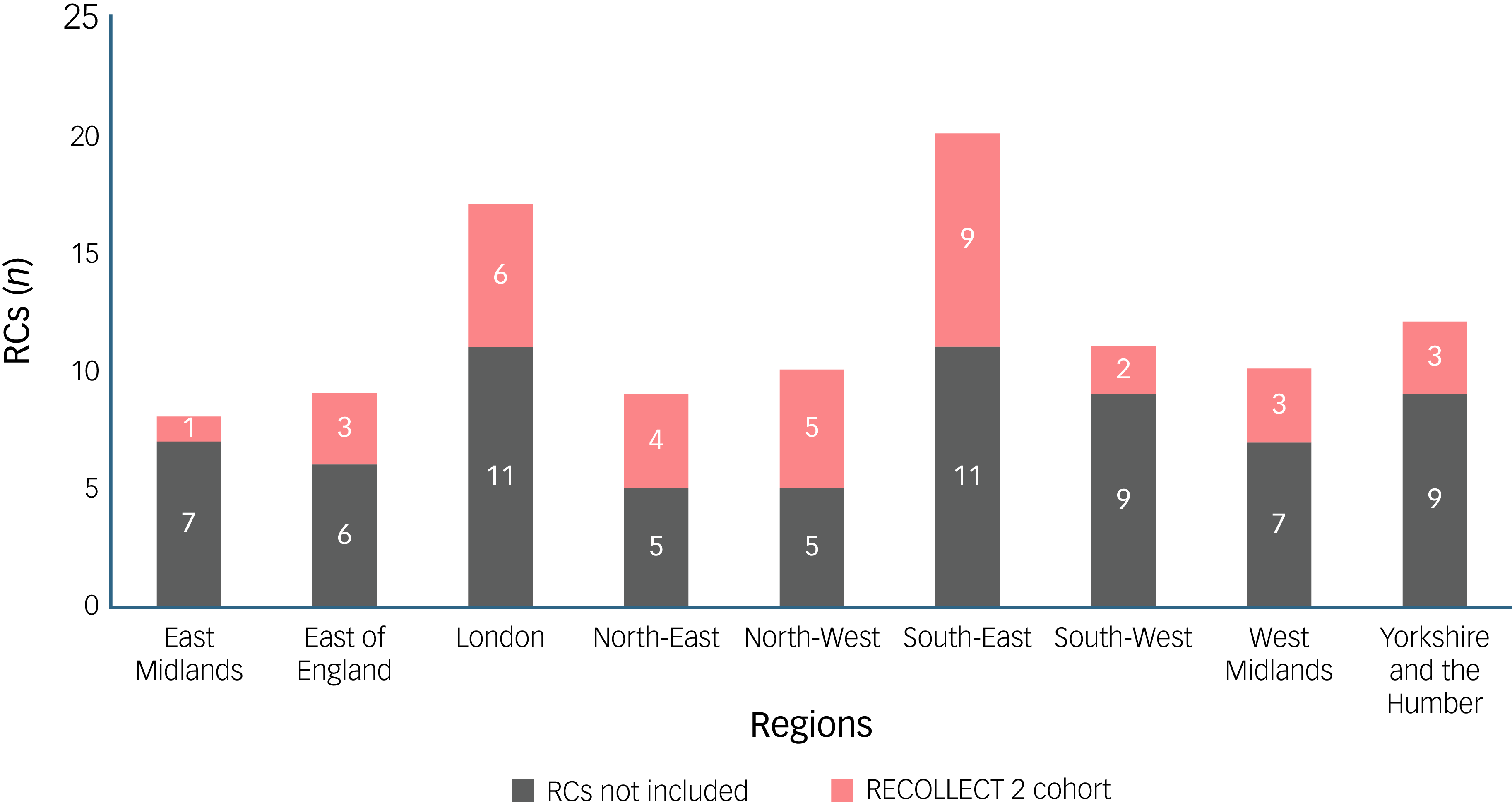
Of those who provided consent, 97% completed the baseline assessment, from which 98% were included in the RECOLLECT 2 cohort. The study sample comprised 498 newly enrolled students from 36 Recovery Colleges across all 9 governmental regions in England. The inclusion of Recovery Colleges in the RECOLLECT 2 cohort relative to the total number of Recovery Colleges in each governmental region is presented in Fig. 2.
Number of Recovery Colleges (RCs) by governmental region. RECOLLECT 2, Recovery Colleges Characterisation and Testing 2.

The geographical, sociodemographic and clinical characteristics of students are shown in Table 1. In relation to Recovery College type, 387 (77.7%) of students came from strengths-oriented colleges, 107 (21.5%) from community-oriented colleges and 1 (0.2%) from a forensic college. Three students (0.6%) came from a college not assigned to a Recovery College type (i.e. the Recovery College joined the study after the cluster analysis had been performed). Strengths- and community-oriented colleges differed in their distribution across government regions, with most community-oriented college students coming from the South-East (49.5%) or the North-East (43.0%).
Sociodemographic and clinical characteristics of the RECOLLECT 2 cohort

RECOLLECT 2, Recovery Colleges Characterisation and Testing 2; RC, Recovery College; GCSE, General Certificate of Secondary Education; A-level, advanced level.
A Bonferroni correction was applied for multiple comparisons, and statistical significance was thus set at P < 0.001; following application of this correction, there were no significant differences between RC types.
* P < 0.05.
Students across strengths- and community-oriented Recovery Colleges differed on two sociodemographic factors (Table 1); students from the latter were less likely to be unemployed and seeking work (odds ratio 0.41, 95% CI = 0.18–0.95) and were more likely to have entry-level/General Certificate of Secondary Education as their highest educational qualification (odds ratio 1.66, 95% CI = 1.00–2.75). However, these marginal differences were no longer significant following Bonferroni correction. Students from the two main Recovery College types did not differ significantly on any clinical factors, but no students from community-oriented Recovery Colleges had a primary diagnosis of a developmental disorder or substance use disorder. Only strengths-oriented Recovery Colleges included students who resided in long-stay or overnight facilities.
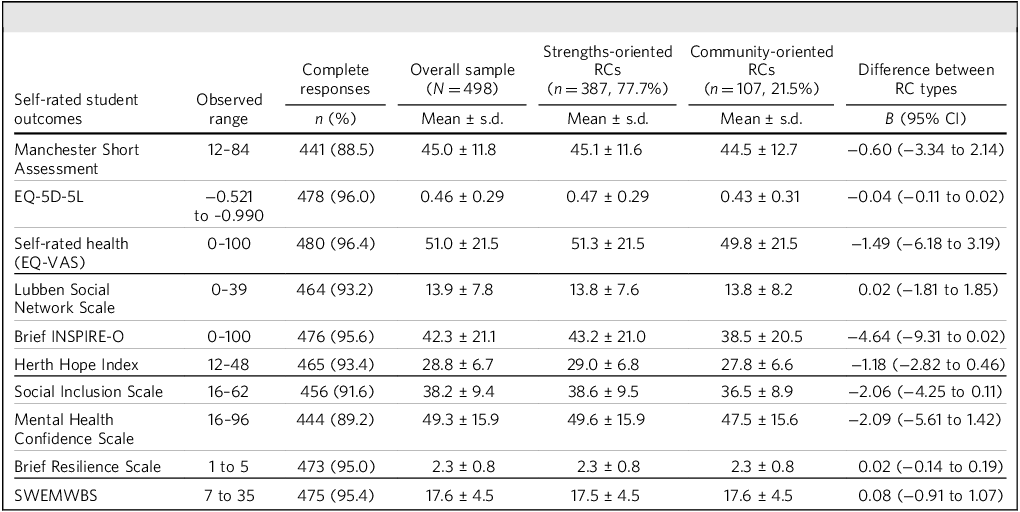
Mean baseline scores for all self-rated student outcomes are presented in Table 2. Students from strengths- versus community-oriented Recovery Colleges did not differ on any outcome. Baseline scores on imputed data are presented in Supplementary Table 1; it was also found that there were no differences indicating that missing data had not introduced bias.
Baseline scores for self-rated student outcomes in the RECOLLECT 2 cohort

RECOLLECT 2, Recovery Colleges Characterisation and Testing 2; RC, Recovery College; SWEMWBS, Short Warwick–Edinburgh Mental Wellbeing Scale.
A Bonferroni correction was applied for multiple comparisons, and statistical significance was thus set at P < 0.005. Following application of this correction, there were no significant differences between RC types. B-coefficients represent the estimated change in the outcome variable associated with a one-unit increase in the predictor.
*P < 0.05, **P < 0.001.
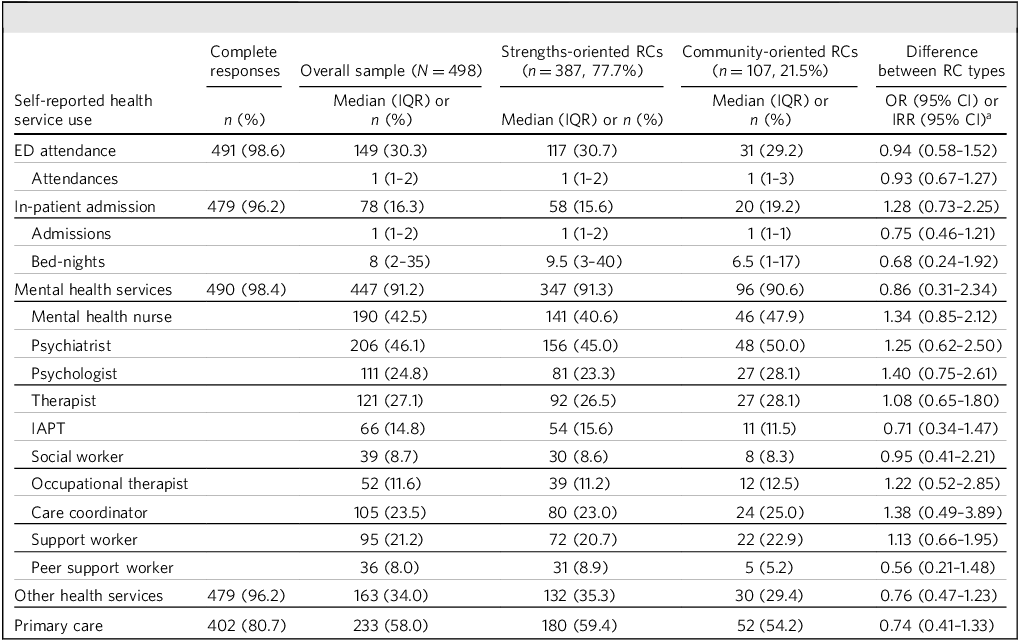
Self-reported health service use over the 4 months preceding completion of the baseline survey assessment for the overall cohort and Recovery College type is presented in Table 3. There were no differences between students attending strengths- versus community-oriented Recovery Colleges on any health service use outcome. Further detailed health service use data are provided in Supplementary Table 2.
RECOLLECT 2 self-reported health service use in the 4 months preceding baseline assessment

RECOLLECT 2, Recovery Colleges Characterisation and Testing 2; RC, Recovery College; IQR, interquartile range; ED, emergency department; IAPT, Improving Access to Psychological Therapies.
a Odds ratios are presented for categorical variables, and incidence rate ratios for count data.
*P < 0.05, **P < 0.001.
Discussion
Summary of key findings
This study provides the first nationwide characterisation of a large inception cohort of Recovery College students in England currently or recently using secondary mental health services. It offers insights into their sociodemographic and clinical profiles, as well as their engagement with health services. Although the cohort was diverse in certain sociodemographic aspects such as region, occupational status and educational background, most students were female and of White ethnicity. The majority self-reported having a disability, with the most frequently reported primary mental health diagnoses being mood, anxiety and personality disorders. Few students reported a diagnosis of a developmental disorder. Following correction for multiple comparisons, there were no significant differences in the sociodemographic or clinical characteristics of students attending strengths- versus community-oriented Recovery Colleges.
Interpretation in the context of previous research
Compared with national NHS mental health service users (MHSUs) (data from January 2025), 22 our cohort had a greater proportion of female students (72 versus 38%). This is consistent with a recent Recovery College study that found a significant difference in gender for two of three Recovery Colleges. Reference Bowness, Hayes, Stepanian, Anfossi, Taylor and Crowther23 This female skew may reflect either gender-specific engagement barriers or differing attitudes towards recovery-oriented education between male and female mental health service users. The age distribution of our sample – mostly aged 25–44 years – resembled that of the general MHSU population. Consistent with previous research, Reference Bowness, Hayes, Stepanian, Anfossi, Taylor and Crowther23–Reference Meddings, Walsh, Patmore, McKenzie and Holmes25 older adults (65+ years) were underrepresented (5%) despite increasing demand for mental health services in this group. Reference Pywell, Vijaykumar, Dodd and Coventry24
Ethnic minority representation was relatively lower than that of MHSUs nationally, particularly in Black populations (RECOLLECT, 3%; MHSUs, 11%). Previous studies reported mixed findings relating to ethnicity representative of Recovery College students compared with MHSU caseloads. Reference Bowness, Hayes, Stepanian, Anfossi, Taylor and Crowther23,Reference Meddings, Walsh, Patmore, McKenzie and Holmes25 In one recent Recovery College study, 92 out of 93 participants who responded to the question on ethnicity were White. Reference Allard, Pollard, Laugharne, Coates, Wildfire-Roberts and Millward1 In an earlier Recovery College study, 8–10% of those that completed follow-up were from Asian communities but there were no Black participants. Reference Wilson, King and Russell3 Our findings suggest potential systemic barriers to both Recovery College participation and research enrolment among ethnic minority groups. Reference Woodall, Morgan, Sloan and Howard26 Similarly, our cohort had a lower proportion of students reporting a disability (RECOLLECT, 58%; MHSUs, 84%) or a primary diagnosis of developmental disorder (RECOLLECT, 2.6%; MHSUs, 15%) than that of the national MHSU population. This may reflect either reduced accessibility of Recovery Colleges to people with learning disabilities or a lower relevance, as perceived by mental health staff, informal carers and/or the person with learning disabilities, of either recovery or education. Reference Slade, Amering, Farkas, Hamilton, O’Hagan and Panther27 However, because the survey asked participants to report their main mental health difficulty, it is possible that developmental disorders were under-identified. Students may have instead listed conditions such as anxiety, mood or personality disorders as their primary difficulty, viewing learning disabilities as separate to their mental health.
Self-rated student outcomes, including well-being and quality of life, were comparable to previous pre-intervention findings. For example, scores on measures such as MANSA, HHI, MHCS and EQ-5D-5L aligned closely with the NEON-O trial baseline data. Reference Slade, Rennick-Egglestone, Elliott, Newby, Robinson and Gavan28 Our SWEMWBS mean of 17.6 closely matched prior Recovery College findings, Reference Allard, Pollard, Laugharne, Coates, Wildfire-Roberts and Millward1 suggesting that these measures are robust indicators for Recovery College research.
RECOLLECT participants’ health service use appeared higher than that of MHSUs but in line with previous Recovery College research. For example, a greater proportion of RECOLLECT students had an in-patient admission in the past 4 months than the average MHSU in the past 12 months (RECOLLECT, 16.3%; MHSUs, 3.0%). 22 This suggests that our students may have had more severe or acute mental health difficulties. The RECOLLECT figure is more in line with a previous Recovery College study, which found that 20% of students had had an admission in the 18 months prior to enrolment. Reference Bourne, Meddings and Whittington30
The absence of significant differences between students enrolled at strengths- and community-oriented Recovery Colleges confirms that Recovery College type does not determine who accesses Recovery Colleges. Given the lack of Recovery Colleges available to potential students, instead, factors such as geographic location and accessibility may be more influential on enrolment. It remains unclear as to whether undertaking courses at a different type of Recovery College has an impact on outcomes, which RECOLLECT 2 aims to assess in the future. Indeed, this similarity between groups indicates the potential to examine the differential impact of Recovery College type on outcome measures, without student characteristics acting as a confounder.
Strengths and limitations
This study comprises the largest and most geographically representative cohort of Recovery College students to date, with participation from 36 Recovery Colleges across all 9 governmental regions in England, albeit with notable imbalances in regional sampling that should be considered when interpreting findings. It builds on previous studies limited to one or a small number of Recovery Colleges Reference Bowness, Hayes, Stepanian, Anfossi, Taylor and Crowther23,Reference Meddings, Walsh, Patmore, McKenzie and Holmes25,Reference Secker29 and often including only strengths-oriented Recovery Colleges. We also used a wider range of validated outcome measures compared with previous Recovery College research, Reference Allard, Pollard, Laugharne, Coates, Wildfire-Roberts and Millward1 allowing for robust comparisons with other longitudinal studies.
However, the sample may not be representative of all mental health service users using Recovery Colleges, because participants were limited to those willing to take part in longitudinal, quantitative research. This introduces potential bias, particularly because those less likely to participate in research – such as people with developmental disorders, certain disabilities or those from ethnic minority backgrounds – were underrepresented. Moreover, students from forensic Recovery Colleges were underrepresented in the current study, limiting the extent to which findings can be generalised to this group.
Clinical and policy implications
Our study suggests that certain groups of MHSUs may be underrepresented in Recovery Colleges and in Recovery College research, namely older adults, men, those with developmental disorder diagnoses and ethnic minority populations. Recovery Colleges could look at targeting enrolment processes towards these groups, diversity in staff recruitment and tailoring relevant course content. Researchers could share findings with global recovery networks to improve accessibility internationally. Despite our study having regular input from a LEAP, this is an area that requires ongoing effort.
The similarity in student profiles across Recovery College types, along with consistency in baseline well-being scores versus other intervention studies, suggest that our selected outcomes measures are suitable metrics to use for future evaluations of Recovery College effectiveness.
Future research
RECOLLECT 2 will provide the most comprehensive evidence to date on the effectiveness and implementation of Recovery Colleges in England. Reference Hayes, Henderson, Bakolis, Lawrence, Elliott and Ronaldson6 By conducting longitudinal analysis of a wide range of student outcome measures alongside Recovery College fidelity scores, this study will provide an empirical foundation for informing Recovery College policy. To improve representation, additional research could qualitatively explore why certain groups are underrepresented in Recovery Colleges and Recovery College research. Given the growing evidence that Recovery Colleges have significant potential in supporting people with mental health issues to live more fulfilled lives, Reference Anfossi2,Reference Bourne, Meddings and Whittington30,Reference Kay and Edgley31 our findings will maximise their impact and shape future service development.
About the authors
All authors are members of the RECOLLECT Study Team, members of the RECOLLECT International Advisory board and/or members of the RECOLLECT Lived Experience Advisory Panel. Joint first authors: Simon Lawrence is a trainee clinical psychologist at University College London; Amy Ronaldson is a research fellow at King’s College London. Joint last authors: Claire Henderson is a clinical professor of Public Mental Health at King’s College London and an honorary consultant psychiatrist at South London and Maudsley NHS Foundation Trust; Mike Slade is a professor of Mental Health Recovery and Social Inclusion at the University of Nottingham.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjb.2026.10220
Data availability
Once RECOLLECT 2 is completed, the data that support the findings of this study will be available on request from the UK Data Service repository. Once available, data access permission can be requested from Nottinghamshire Healthcare NHS Foundation Trust (research@nottshc.nhs.uk).
Acknowledgements
We thank all the individuals and organisations who contributed to the RECOLLECT study. M.S. acknowledges the support of NIHR Nottingham Biomedical Research Centre. For the purposes of open access, the author has applied a Creative Commons Attribution licence to any Accepted Author Manuscript version arising from this submission.
Author contributions
S.M., J.R., V.L., I.B., R.E., R.A.E., J.R., C.H. and M.S. conceptualised the study. All authors contributed to the study design. S.L., A.R., T.A., M.M., S.K.T., A.K., J.S., R.D., D.H., T.J., D.D., M.N., O.S., V.L., R.E., K.S., C.H. and M.S. facilitated the data collection. S.L., A.R., T.A., T.J., M.N., I.B., R.E., R.A.E., C.H. and M.S. analysed the data. K.B. and D.E. provided valuable context to the study. All authors contributed to data interpretation, and to drafting and critically revising the manuscript. All authors approved the final draft.
Funding
This work was supported by NIHR (grant reference no. 200605, 2020–2025). The views expressed are those of the authors and not necessarily those of NIHR or the Department of Health and Social Care.
Declaration of interest
None.
Transparency declaration
S.L., A.R., C.H. and M.S. affirm that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.




 Open access
Open access
eLetters
No eLetters have been published for this article.