


Introduction
Malnutrition remains a leading contributor to global morbidity and mortality, surpassing the burden of many other major health concerns. According to the Global Nutrition Report(1) over 820 million individuals, approximately one in nine people globally, suffer from hunger or undernutrition, with the highest prevalence reported in sub-Saharan Africa, West Asia, and Latin America.(1) In developing countries, malnutrition during early childhood is not only life-threatening but also has long-term implications on educational performance, health status, and economic productivity later in life(Reference Black, Victora and Walker2,3) In Nigeria, according to 2018 surveys and reports, child malnutrition remains a significant issue with both undernutrition and overweight affecting children’s growth and development,(Reference Ekholuenetale, Okonji, Nzoputam and Barrow4) Some factors such as poor maternal nutrition, limited access to health services, inadequate infant feeding practices, and poverty are significant contributors to malnutrition in form of stunting, wasting, and obesity in children. In the northern part of Nigeria, the rate of wasting is highest in children between the ages of 6 and 24 months, which is compounded by conflict, displacement, and poor health systems.(Reference Ojeleke, Groot and Pavlova5) This problem in the early stages of life can increase the risk of infections, morbidity, and mortality, together with decreased mental and cognitive development, most especially in rural and orphanage homes. The global incidence of orphaned children resulting from parental loss has escalated in recent years. Approximately 153 million children globally are orphans, with approximately 17.8 million being double orphans,(Reference Sewnet, Derseh and Desyibelew6) with over one in seven children orphaned in sub-Saharan Africa.(Reference Deters7)
Nigeria is known to have highest populations of orphans and vulnerable children in the world today because of the effect of HIV/AIDS on its large population.(Reference Embleton, Ayuku and Kamanda8) These children are susceptible to a number of dangers, such as a higher chance of unfulfilled fundamental needs, such as schooling(Reference John, Poh and Jalaludin9) and necessary medical treatment,(Reference Akeredolu10) as well as child labor and abuse,(Reference Akeredolu10,Reference Mohammed, Musa and Fage11) which can result in malnutrition.(Reference Guthold, White Johansson and Mathers12,Reference Agugo, Asinobi and Afam-Anene13) In an orphanage home, caregivers are primarily responsible for food choices, which are often influenced by cultural practices, food availability, cost, and time constraints. Diets in institutional settings may be monotonous, with limited food variety and nutrient density, thereby increasing the risk of micronutrient deficiencies and energy imbalance.(Reference Osei, Pandey and Spiro14) Furthermore, poor food preparation methods can contribute to the degradation of essential nutrients, exacerbating the risk of undernutrition. Children in orphanages had a significantly higher rate of undernutrition than non-orphanages. Orphaned and institutionalised children may experience one or several micronutrient deficiencies due to poor nutritional status and are vulnerable to infections since they are at risk for a variety of complications, putting their health and development in great trouble.(Reference Obasohan, Walters and Jacques15) Since the early years of life are critical for proper growth and development, the nutritional condition of children under five is especially concerning. Their nutritional well-being is a reflection of national, local, and domestic investments in family health, which both directly and indirectly support the growth of the nation as a whole and, more specifically, the development of people. Studies have shown that children living in orphanages are far more likely to suffer from malnutrition than children living in families.(Reference Karam, Sahu and Rajaa16,Reference Nwaneri and Omuemu17)
A study conducted by Adeomi et al. (Reference Adeomi, Aliyu and Sabageh18) in Lagos found that orphans had a significantly higher prevalence of malnutrition among the children living in orphanages, despite the reported healthy eating patterns and high dietary diversity. In Nigeria, very little data exists on the eating patterns, anthropometry, and nutritional status of children living in orphanages, and no data have been published for Kogi State. This study set out to quantify the eating pattern, nutrient intake, and nutritional status, and extent of malnutrition of children residing in orphanages in Kogi State, Nigeria. The data from this study is expected to assist health policy makers, educators, and other stakeholders in planning appropriate intervention programs targeting children in orphanages in Kogi State and other parts of Nigeria.
Specific objectives of this study.
The specific objectives of this study are to:
-
1. To access the food consumption pattern of the orphanage children in Kogi State
-
2. To determine their nutritional status using indices like anthropometry and mid-upper arm circumference.
-
3. To evaluate their nutrient intake using weighed food intake assessment for macro and some micronutrients.
Material and methods
Study design and population and location
The study used cross sectional research design. The study was conducted on selected orphanage homes both in rural setting and urban setting in Kogi State. Fifteen recognised orphanage homes spread among the state’s Eastern and Western senatorial districts of Kogi State served as the study’s location. The research population consisted of every child living in the orphanages between the ages of 2–5 years located at Lokoja, Ugwalawo, Anyiba, Otutulu, Okura, Odu-gegeli, Lsanlu, Egbe, Kabba, and Ogidi. The study lasted for two weeks. Kogi State came into existence in 1991, as one of the 36 States in Nigeria, and was created out of the defunct Kebba province of the defunct Northern region. It is located in the north-central zone of Nigeria referred as the middle belt region. It is bounded by ten states; to the east by Nassarawa State, to the South by Enugu, Anambra and Edo States, to the West by Ondo, Ekiti, and Kwara States and to the North by Niger, Abuja, and Nassarawa States. It is the only State in Nigeria boarded by ten other States. The majority of the people are farmers growing crops such as yams, maize, beans, cassava, cocoyam, cashew, mango, and oil palm.
Eligibility criteria: A total of 15 orphanage homes were used for the study. The orphanages were selected based on the consent approval signed by the manager and owners of the orphanage homes. The inclusion criterion of having lived in the orphanage for at least three months led to the enrollment of the children 2 to 5 years old in the study.
Study population: All the children between the age of 2–5 years in the orphanges located in the Eastern and Western part were used for the study. In compliance with dietary intake study procedures,(Reference Gibson and Ferguson19) a sub-sample of 23 children was chosen from this cohort using systematic random selection for a 3-day weighted food consumption evaluation.
Ethical clearance: In accordance with the Declaration of Helsinki(20) this cross-sectional study obtained approval from Research Ethics Committee of Department of Nutrition and Dietetics, Faculty of Agriculture, University of, Nigeria, Nsukka.
Informed Consent: Formal approval permission was obtained from the Ministry of Women Affairs and Social Development, Kogi State to carry out the studies in orphanage homes. After approval of this study by the Ethics Committee, and the Ministry of Women Affairs and Social Development, Kogi State, the orphanage administrative and caregivers was met and informed of the objectives of our study in order to obtain their consent and assistance.
Data collection
Questionnaire
Data were collected through a structured questionnaire validated for content by 5 lecturers in the Department of Nutrition and Dietetics, University of Nigeria, Nsukka was used to collect information. The questionnaire gathered information on socio-demographic characteristics of the children and that of the caregiver, diet inquiry of food and snack commonly consumed at school, and frequently consumed foods for carbohydrate food intake, protein food intake and fruit and vegetable consumption practices in the orphanage homes.
Anthropometric assessment
Anthropometric measurements were conducted following WHO standard protocols.(21)
Weight measurement
The children were weighted with minimal clothing, no foot wear, before meal and with an empty bladder, they were told to stand at the centre of the calibrated digital scale, body weight was measured to the nearest 0.1 kg. For active children, the caregivers were weighted alone first and then the caregiver were weigh again carrying the child. The actual weight of the child was subtracted from the caregiver’s weight. The weight of the children was expressed as a percentage of that expected for his or her age in terms of standard deviation. Weight of the children were plotted on the growth chart to determine the number of children that were wasted (<−2 z score), severely wasted (<−3 z scores), mildly wasted (between −2 to −3 z scores), overweight (+1), and obese (+2 and +3).
Height measurement
Height is stable measure that shows the total increase in size of an individual at the moment it is determined. In this study, height was recorded to the nearest 0.1 cm using a measuring tape fixed to a ruler. The height of the children was measured standing on a flat floor, barefoot and with feet together, their head was held erect with arms by the sides, the head piece was lowered until it came in contact with the head. The height of the children was expressed as percentage of that expected for his or her age or in terms of standard deviation. The index height for age was used to classify shortness or stunting, which is a linear growth that has failed to reach genetic potential as a result of poor diet or disease. Height for age of the children was plotted on the growth chart to determine the number of children that were stunted (<−2 z score), severely stunted (<−3 z scores), and normal (<−1).
BMI calculation
Body mass index was calculated from the results obtained using the following formula; BMI (kg/m2) = weight (kg)/ height (m2) and classified based on age-, sex-, and height-specific percentiles into these categories: Overweight (17.1–18.8), Underweight (14.2 to 12.9), Thin (<12.9–12.0), Normal (15.3–15.7), and Severe Thinness (<12.0).
Mid-upper arm circumference
This is the measurements of the muscle in the arm. Muscle wasting or poor muscle development is a feature of all the spectra of protein energy malnutrition. Mid-upper arm circumference (MUAC) was measured using a non-stretchable measuring tape. All measurements were taken in duplicate and the average was used in analysis. With the following procedures, the measurement was taken on the left arm with the hand hanging freely, the tape was placed on the left upper arm midway between the acromion process of the scapula and the olecranon process of the elbow. The reading was then set at the nearest 0.1cm and recorded. The result was then compared with the reference standard, >13.5 cm (normal), <12 cm (severe malnutrition), and 12–13.5 cm (moderate malnutrition).
Dietary intake assessment
A 3-day weighed food intake study was carried out among the 23 sub-sampled children, including two weekdays and one weekend day to estimate the nutrient intake of the children from the consumed food. It involved weighing all the food ingredients used in the food preparation during the period and snacks consumed. The cooked food, quantity served, plate waste and discarded food was weighed throughout the survey period using a digital kitchen scale with 1 g sensitivity. Standard food models and local utensils were used to ensure accurate estimation of portion sizes. The meals were weighed after cooking as well as the quantity served to each child before feeding. Plate wastes were weighed and subtracted from the quantity served to determine the actual food intake of the child. The snacks consumed throughout the period by each child were also weighed. The amount of food consumed was expressed as raw food weight and estimated from the proportion of the different ingredients in the recipe. The water conversion factors were determined by averaging repeated measurements of raw and cooked foods. Nutrient intake data were analysed using the West African Food Composition Table and WHO/FAO food composition data.(22)
Procedure for nutrient intake using food composition tables was assessed as follows;
-
each raw ingredient used in preparing the meal was weighed = a
-
total weight of cooked meal excluding the weight of pot were weighted = b
-
Weight of food consumed excluding the plate wastes were recorded = c
-
Conversion factor was used to find the amount of each raw ingredient consumed =
 $\;{c \over b}$
$\;{c \over b}$
-
The amount of each raw food ingredient consumed was calculated =
${c \over b}\;*a$
-
The process was repeated for all the meals consumed per day for breakfast, lunch, dinner and snacks.
-
The total of the amount of raw ingredient consumed (
${c \over b}\;*a$
) in breakfast, lunch, dinner snacks was calculated to get the amount of that particular ingredient consumed for the day (d) -
Therefore, nutrient consumed from each raw ingredient was calculated as follows: 100 g of each raw ingredient= x nutrient
-
$n = {d \over {100}}*x$
-
This process was repeated for all the nutrients in each raw ingredient of all the meals.
-
Nutrients from the different ingredients was added to know the amount of each nutrient consumed from the meals for day 1
-
All the process was repeated for days 2 and 3
-
The amount of nutrient consumed in days 1, 2 and 3 was calculated for mean to get the average daily intake of the nutrient.




The estimated nutrient intakes were compared with the Recommended Nutrient Intakes (RNIs) based on age and sex as outlined by WHO/FAO (2004) to assess adequacy(23) using the calculation below;
 $Intake\;as\;\% \;RNI = {{{\rm{Actual}}\;{\rm{intake}}\; \times 100} \over {{\rm{Requirement}}\;{\rm{for}}\;{\rm{Age}}/{\rm{sex}}/{\rm{wt}}}}$
$Intake\;as\;\% \;RNI = {{{\rm{Actual}}\;{\rm{intake}}\; \times 100} \over {{\rm{Requirement}}\;{\rm{for}}\;{\rm{Age}}/{\rm{sex}}/{\rm{wt}}}}$
Statistical analysis
Data were analysed using the Statistical Package for the Social Sciences (SPSS), version 21. Descriptive statistics including means, frequencies, and percentages were used to summarise the data. Date from anthropometry measurement were plotted on the growth chart (z scores) and compared to the reference standard for each sex. The analysis was then presented in frequencies and percentage for the number of children in each categories. Nutrient intake adequacy was assessed by comparing observed intake with age-specific RNIs, and the percentage contribution of each nutrient to the recommended intake was calculated.
Results
The socio-demographic data of the children
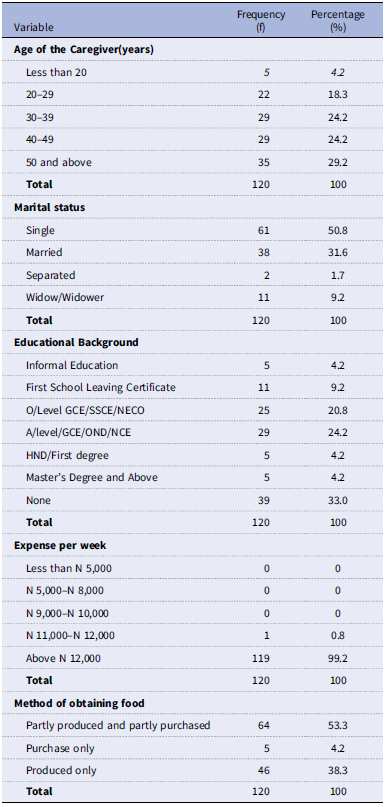
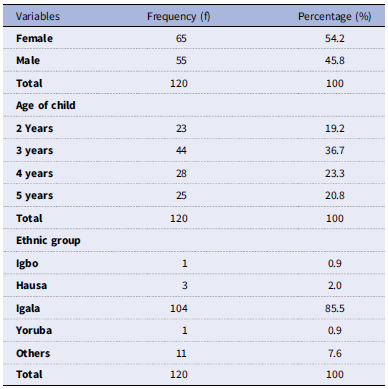
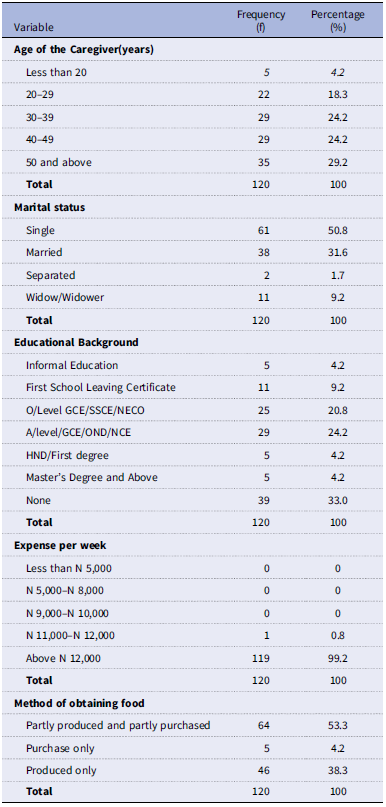
Table 1 present the socio-demographic data of the children in the orphanage homes. They were 120 orphanage children between the ages of 2–5 years, which consisted of more girls (54.2 %) than boys (45.8%). Children from the ages of 3years (36.7%) were more populated in the study. Most of the orphanage children (85.5%) where basically from Kogi State, native of Igala ascent.
The socio- demographic data of the children

N = 120.
The socio-economic characteristics of the caregivers
The data on Table 2 represent the self-reported questions from the caregivers; the majority, 29.2% of the caregivers, were 50 years and above, with the majority of them single (50.8%), 24.2% held qualifications at the A/Level, GCE, OND, or NCE levels, while 33.3% had no formal education. Weekly household expenditures by caregivers in the orphanages ranged from ₦12,000 and above. Food sources were primarily from market purchase, and farm produce cultivated among the older children in the orphanage homes, accounting for 53.3% of reported procurement methods, while only 38.3% of some orphanages depended only on farm produce, and a few (4.2%) purchased all their food from the market.
The socio-economic characteristics of the caregivers
Food consumption pattern of the children
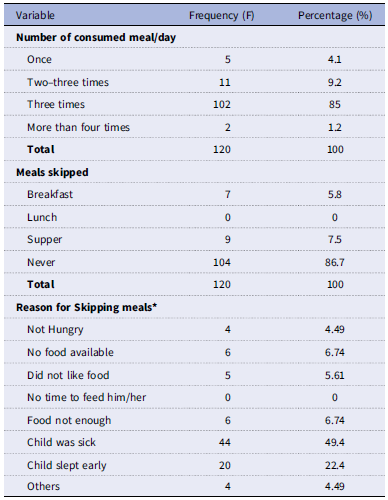
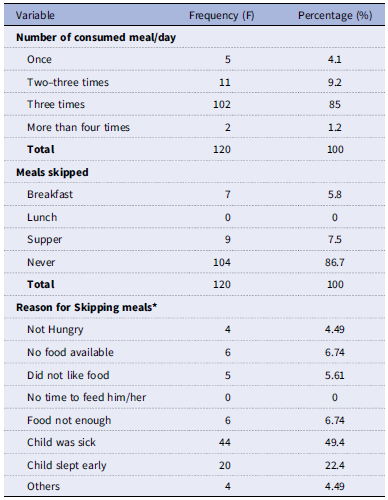
Food consumption patterns were gathered using a questionnaire completed by caregivers on behalf of the children. Table 3 shows the food consumption patterns of the children in the orphanage. Most children (85%) consumed meals three times a day, while 9.2% ate twice a day, and 1.2% reported eating more than four times a day. A small number of children skipped breakfast (5.8%), and 7.5% skipped dinner regularly. The reasons for skipping meals included difficulties accessing available food (6.74%), a dislike for the provided food (5.61%), and a lack of appetite (4. 49%).daily. Reasons were inability to access available foods (6.74%), 5.61% indicated a dislike for the food provided, and 4.49% reported a lack of appetite.
Food consumption patter of the orphan children
*multiple response.
Meal consumed in school
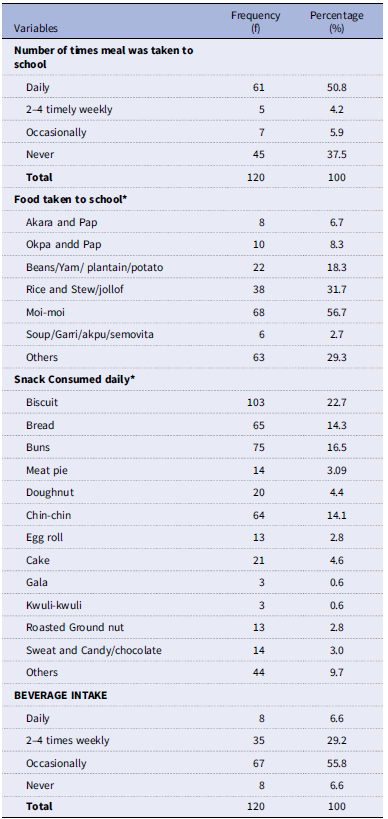
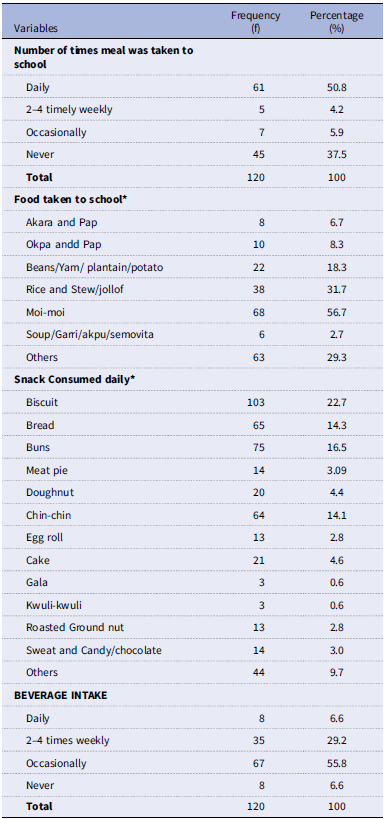
We visited some schools where some of the children were enrolled near the orphanage. The food and snacks consumed were recorded, as shown in Table 4. Among the children surveyed, 37.5% carried food to school, while 50.8% did not. Among those who brought food, rice and stew were the most commonly consumed items (31.7%), followed by moi-moi (56.7%), and beans, yam, plantain, or potatoes (18.3%). Common snacks included biscuits (22.7%) and bread (16.7%), while roasted groundnuts were consumed by 0.6%. Beverages such as Bobo, Zoba, Ribena, and Coca-Cola were consumed daily by 6.6% of the children, with 55.8% consuming these beverages occasionally.
Meal consumed in school by the orphan children
N = 120.
Food consumption pattern of the orphanage children
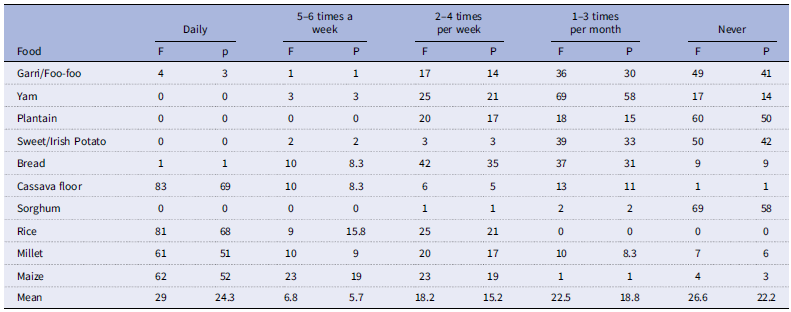
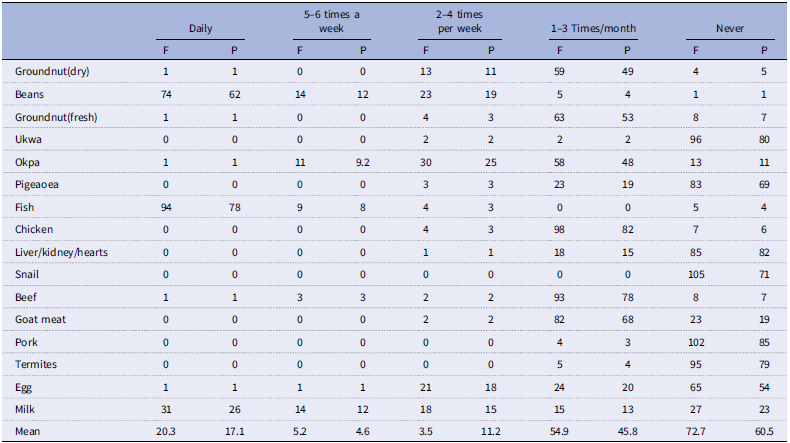
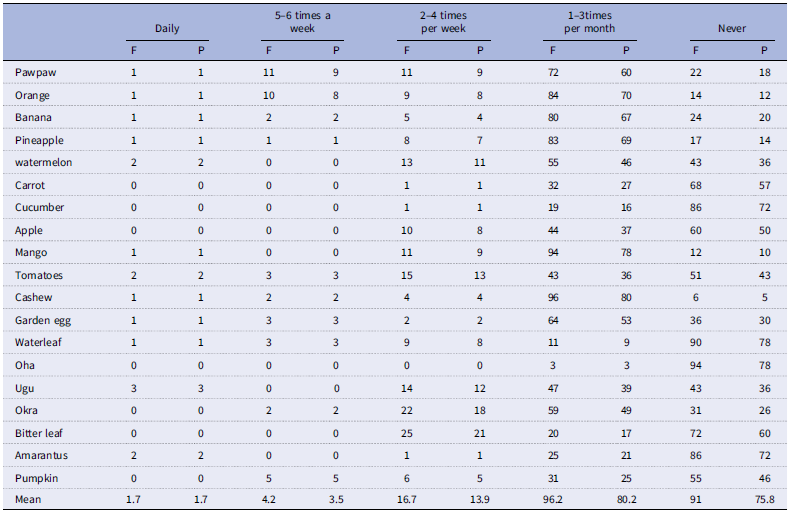
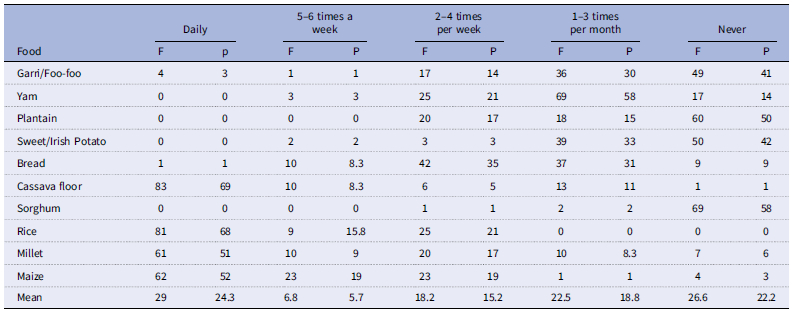
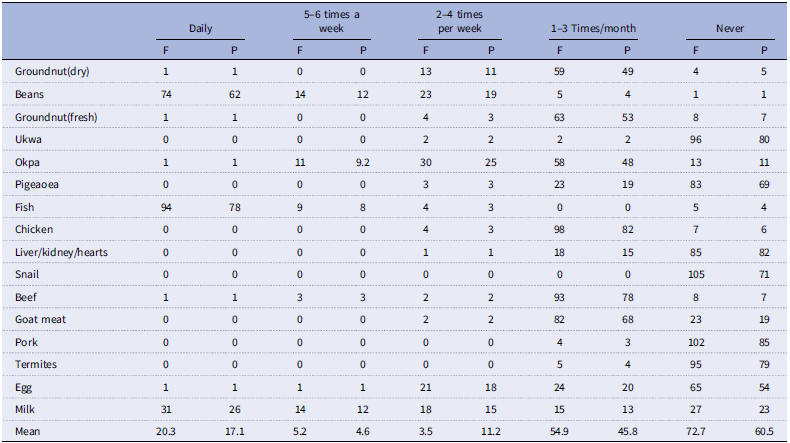
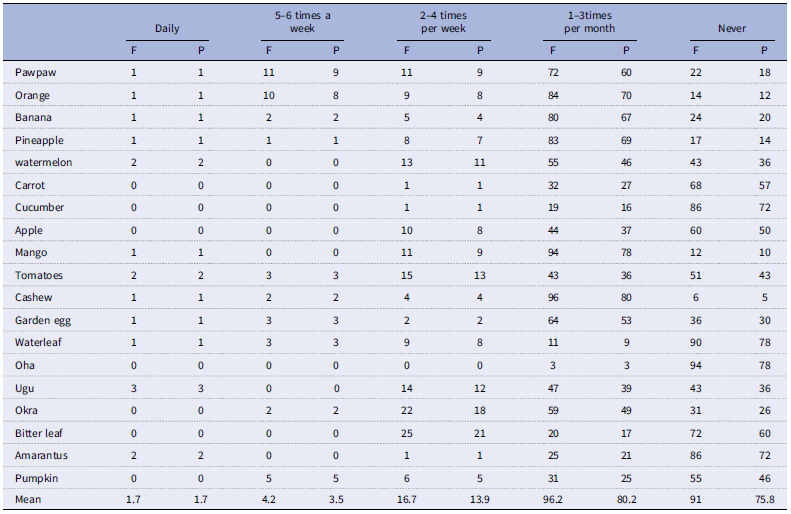
Frequency of consumption of three food groups for carbohydrate, protein, fruits, and vegetable food sources, were reported on Tables 5, 6, and 7. According to Table 5, cassava flour (83%), rice (81%), millet (61%), and maize (62%) were frequently consumed on a daily basis, with a combined total of 24.3% of responses indicating this. In contrast, sorghum (58%) and garri or fufu (41%) were reported as never being consumed. Table 6 presents the frequency of protein source consumption. Beans (62%), fish slices (78%), and milk (26%) were consumed daily. However, ukwa (80%), cowpeas (69%), liver (82%), and snails (71%) were never consumed, accounting for 60.5% of total responses. As for fruit and vegetable (Table 7) they were rarely consumed daily, with only 1.7% of respondents indicating daily consumption. Conversely, 80.2% reported consuming fruits and vegetables 1 to 3 times a month, while 75.8% indicated that they never consumed them at all.
Frequency consumption of carbohydrate rich foods
Frequency of consumption of protein food source
Frequency of consumption of fruit and vegetables rich food source
Anthropometric indices of children according to sex
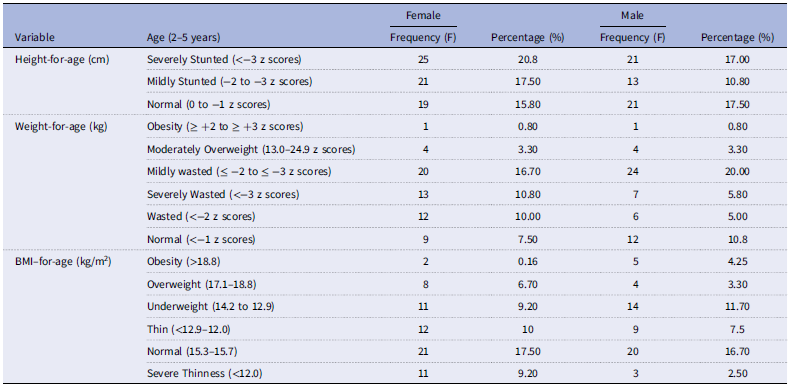
Table 8 presents the anthropometric indices of the children disaggregated by sex. The data revealed that girls exhibited higher rates of severe stunting (20.8%), wasting (10.8%), overweight (6.7%), and severe thinness (9.2%) compared to boys, who recorded 17.0% for severe stunting, 5.8% for severe wasting, 3.3% for overweight, and 2.5% for severe thinness. However, the prevalence of underweight was higher among boys (11.7%) than among girls.
Anthropometric indices of children
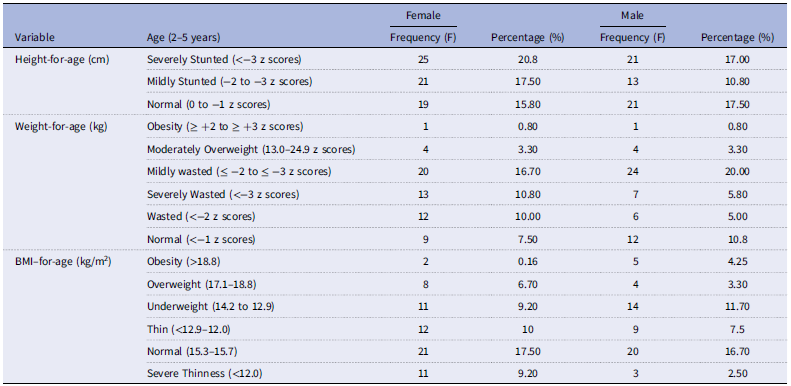
BMI: Body mass index.
Mid-upper arm circumference of the children
Prevalence of malnutrition seemed to increase with increase in number of female children (Table 9). Mid upper arm circumference showed that severe malnutrition was more observed in the female children (15.05%).
Mid-upper arm circumference of the children

Energy and nutrient intake of children
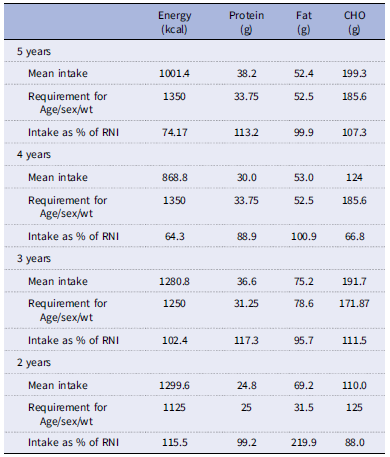
Table 10 presents the energy, protein, fat, and carbohydrate intake of the orphanage children categorised by age groups, from the weighted food intake, categorised by age group. Children need macronutrients to grow, maintain body functions, and remain physically active. The average daily energy among the children was as follows: 1001.4 kcal for 5 years of age, 868.8 kcal for 4 years of age, 1280.8 kcal for 3 years of age and 1299.6 kcal for 2 years of age. The mean values for 4–5 years old was inadequate as compared to the estimated average requirement (1350 kcal, 1350 kcal, 1250 kcal, 1125 kcal). Protein intake is important as it provides essential amino acids required for protein synthesis and growth in children. The data on the protein intake reported that the protein intake was 38.2 g for 5 years of age, 30.0 g for 4 years of age, 36.6 g for 3 years of age and 24.8 g/day for 2 years of age. Subjects in all age group met the daily protein recommendation respectively. The total fat intake of the children (2–5 years) was 69.2 g, 75.2 g, 53.0 g, 52.4 g respectively, with age 2 years exceeding the recommendation. Carbohydrates are the preferred fuel for the active brain and growing muscles. They are found in a variety of foods. The data on carbohydrates content presented shows that consumption of carbohydrates exceeded the recommended intake of 185.6 g/day in 4–5 years’ age groups. Specifically, carbohydrates intake was 174.73 ± 45.39 g in the 7–9 age group, 190.60 ± 76.55 g in the 10–12 years’ age group and 250.13 ± 46.33 g in the 13–15 years of age.
Energy, protein, fat and carbohydrate intake of children according to age as percentages of recommended nutrient intake

RNI: Recommended nutrient intake.
CHO: carbohydrate.
Vitamins and mineral intake of children according to age
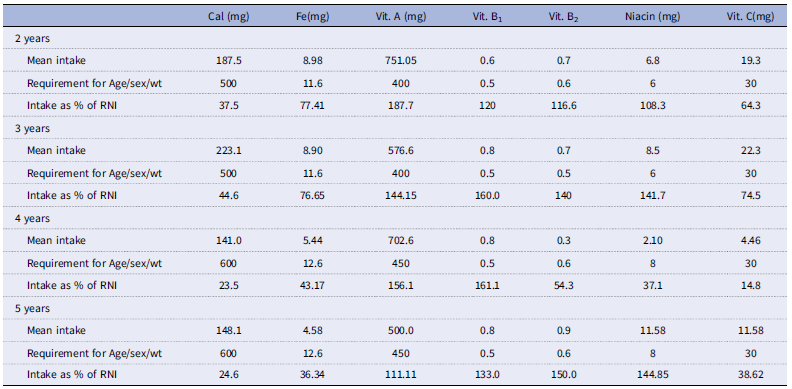
Table 11 presents the total intake of selected vitamins and minerals among the orphanage children, compared with the RDA for each age group. Calcium intake was recorded as 187.7 mg and 223.1 mg for the 2-year and 3-year age groups. In contrast, the 4- and 5-year-olds had lower intakes of 141.0 mg and 148.1 mg reapectively. The data depicts that the mean intake of iron was 8.98 mg in the 2 years age group, 8.90 mg in the 3 years age group and 5.44 mg in 4, 4.58mg in the 5 years age group. None of these iron averages met the recommended intake for their respective age groups. Vitamin A intake was 751.05 µg for 2-year-olds and 576.6 µg for 3-year-olds, while 4- and 5-year-olds had intakes of 702.6 µg and 500.0 µg, respectively, all the age groups exceeded the daily recommendation for Vitamin A. The daily mean intake of Vitamin B1 was adequate compared to the recommended dietary intake of 0.5 mg across all age group. For Vitamin B2, the mean daily intake was 0.6 mg for 2 years of age, 0.8 mg for 3 years, 0.8mg for 4 years and 0.8 mg for 5 years of age. However, the 3-year-olds did not meet the daily recommendation of 0.6 mg/day. Niacin intake was inadequate in 4 years’ group while other age groups met and exceeded the recommended daily intake. Lastly, the daily mean intake of Vitamin C was insufficient relative to the recommended dietary intake of 30 mg for the 5-year-olds.
Calcium, Iron, Vitamin A, Vitamin B1, Vitamin B2, Niacin, Vitamin C intake of the children as percentages of recommended nutrient intake

RNI: Recommended nutrient intake.
Cal: calcium.
Fe: iron.
Vit. B1: thiamin.
Vit. B2: riboflavin.
Vit. C: Ascorbic acid.
Discussion
This present paper describes the anthropometry, energy, and nutrient intake of children living in orphanage homes in Kogi state. From the questionnaire reports for the dietary pattern of 120 children who took part in the study, meals were frequently cooked and consumed in school, with occasional intake of beverages at school; however, most of the food cooked in school was not nutrient-dense, and the majority of the children relied on snacks such as biscuits, bread, etc. Even though the results indicate that the children ate three time in a day, which aligns with minimum recommended feeding frequency for young children as outlined by WHO,(Reference Micha, Mannar and Afshin24) Only a small proportion of children reported eating less than three meals daily (9.2%), which may pose a risk for insufficient energy and nutrient intake, resulting in malnutrition in rapidly growing children. Most of these foods consumed three times daily were majorly carbohydrate food sources, inadequate and few protein foods, fruits, and vegetables, as compared to the study by Adeomi et al. (Reference Adeomi, Aliyu and Sabageh18) that recorded high dietary diversity among children living in orphanage homes in southwestern Nigeria.
Meal skipping was relatively uncommon, with 86.7% of the children reporting they never skipped meals. Among those who did skip meals, breakfast (5.8%) and supper (7.5%) were the most commonly missed. This is consistent with patterns seen in low-income institutional settings, where meal routines are influenced by food availability, food preference, and caregiver schedules.(Reference Olatunji, Okafor and Ojo25) The reasons provided for skipping meals were lack of food (6.74%), which reflects the presence of intermittent food insecurity in some orphanages, which could stem from funding limitations, poor food supply chains, or inadequate planning. Dislike of food (5.61%) and lack of hunger (4.49%) suggest challenges related to dietary monotony and mealtime environment, as also reported in studies by Kumwenda et al.(Reference Kumwenda, Nyondo-Mipando and Ziyaya26) and UNICEF.(27) A Comparative finding by Adegboye et al.(Reference Adegboye, Yusuf and Ogundare28) study on institutionalized children in Kwara State, showed similar patterns, where 12% of children skipped meals due to unavailability, and 8% due to poor taste or monotony of meals. When children frequently reject food or express disinterest in eating, it often signals limited dietary diversity, poor palatability, or psychosocial issues, especially in institutional care.
It was observed that 50.8% of orphanage children carried food to school, while 37.5% never did. This aligns with global evidence that children in institutional care often face inconsistent access to nutritious school-time meals, which are crucial for meeting daily dietary requirements during growth-critical years.(29) Children who miss meals during school hours may face increased risk of nutrient deficiencies, reduced concentration, and poor academic performance.(29) Among those who brought food, Moi-moi (steamed bean pudding) was the most commonly consumed item (56.7%), followed by rice (31.7%) and root/tuber-based meals like yam or plantain (18.3%). While Moi-moi provides plant-based protein, the overall lack of dietary variety suggests limited micronutrient intake, which is common in institutional settings where meal planning is driven by affordability and availability.(Reference Kinyua, Odhiambo and Mbithe30)
The snack profile was dominated by low-nutrient, high-calorie foods: 22.7% of children consumed biscuits, 16.7% consumed bread, and only 0.6% consumed nutrient-dense snacks like roasted groundnuts. Furthermore, 6.6% of the children consumed sugary beverages like Bobo, Zobo, or Coke daily, and 55.8% consumed them occasionally. Recent studies show that frequent consumption of sugar-sweetened beverages and processed snacks during early childhood is associated with increased risks of poor diet quality, childhood obesity, and non-communicable diseases later in life.(Reference Paruthi31,Reference Swan, Powell, Knowles, Bush and Levy32) The predominance of starchy and sweet foods in the school-time diet points to poor dietary diversity and a potential imbalance in macronutrient and micronutrient intake. These patterns underline the urgent need for nutrition education and dietary intervention programs targeted at caregivers in orphanages and school settings.
The result from the anthropometric data shows a high burden of malnutrition among children residing in orphanage homes, with girls experiencing greater rates of severe stunting (20.8%), wasting (10.8%), severe thinness (9.2%), and overweight (6.7%) than boys. Boys, on the other hand, had a slightly higher prevalence of underweight (11.7%) and lower rates in all other indices. These results illustrate a dual burden of malnutrition, where both undernutrition and early signs of over nutrition coexist in the same population, a trend increasingly observed in developing countries. These findings are in line with recent evidence from institutional settings across sub-Saharan Africa. A study by Akinyemi et al.(Reference Akinyemi, Olatunde and Adewale33) on institutionalized children in southwestern Nigeria found higher rates of severe stunting (18.2%) and wasting (7.4%) among girls, which they attributed to subtle caregiver biases, shared meal practices, and lack of tailored feeding programs in orphanages. Similarly, Tugira et al.(Reference Tugira, Wafula and Nduati34) in a study of 165 orphaned children in Kenya reported higher stunting among females, and underweight was more common in boys, which is similar to the current findings.
Globally, stunting in children under five remains a critical public health concern. According to the UNICEF-WHO-World Bank Joint Child Malnutrition Estimates, the global prevalence of stunting was 22.3%, with sub-Saharan Africa carrying the highest burden.(35) Our study’s stunting rates (17.0% in boys, 20.8% in girls) fall within this range, highlighting that children in institutional care are not spared from the broader nutrition crisis in the region. The relatively higher rate of overweight among girls (6.7%) also aligns with findings from Okoye et al.,(Reference Okoye, Nwachukwu and Ogunbanwo36) who noted an emerging trend of early childhood overweight in urban orphanage homes in Nigeria due to energy-dense, nutrient-poor diets, especially from overreliance on starchy foods and sweetened beverages.(Reference Okoye, Nwachukwu and Ogunbanwo36) This again reinforces the presence of the nutrition transition even within low-income institutional settings. The disproportionate burden of malnutrition among girls suggests the need for gender-sensitive feeding and monitoring strategies. Cultural norms may unknowingly influence caregiver behaviour, leading to unequal food distribution or attention to health. These trends reflect inadequacies in the current feeding practices within orphanage systems. Uniform food portions without considering age, sex, or nutritional needs can lead to both deficiency and excess in different children.
Prendergast and Kamath(Reference Prendergast and Humphrey37,Reference Kamath, Kavana and Ergod38) have shown that children in orphanages with high rates of malnutrition suffer cognitive delays compared to non-orphans, suggesting that this rate of malnutrition may have an impact on the performance of the orphanage children in this study. Despite eating three meals a day, the rate of stunting is most likely caused by a lack of micronutrients; there was an insufficient amount of macronutrients in the diet to supply the necessary amino acids and minerals for growth and regulation of glucose. In fact, the majority of the high-protein foods eaten in orphanages come from plants and have minimal biological value. The high rates of malnutrition were explained by the limited consumption of high biological value proteins from animal sources that offer a balanced and sufficient quantity of proteins for growth.
Children aged 2–3 years met the required energy intake (1299.6 kcal), which met 115.5% of their recommended nutrient intake (RNI). This is encouraging as adequate caloric intake is crucial for proper growth and development at this age. These results align with FAO/WHO guidelines(39) and support findings from Omotayo et al.(Reference Omotayo, Adejoke and Osotimehin40) in Ibadan, Nigeria, where institutionalized children aged 2–5 years had an energy intake between 95–120% of RNI. This adequacy suggests that caloric access in these orphanages, at least quantitatively, is sufficient; however, the energy intake in older children (4–5 years) was below requirement. This might be due to inadequate intake and small quantity and inability to access food by the subjects. Protein intake of the children were adequate in 4 years and 2 years of age groups while ages 5 years and 3 years were above recommendation, this could be attributed to high consumption of beans, and okpa called Bambara nut which has high protein content, which was consumed two to four times per week, this result is similar to the findings of Singwa et al.(Reference Singwa, Tanya, Ngangmou, Navti, Tamfuh and Ejoh41) A similar finding by Izuka et al. (Reference Izuka, Olatona, Onajole and Adeniyi42) in the nutritional status of children under five living in an orphanage home in Lagos State Nigeria, found that children living in the orphanage met the daily macronutrient requirements compared to children living in the communities. The daily fat intake was suboptimal in all age groups except in 3-year-olds, who had a lower intake. This is concerning for this age group, given that fats are essential not only as energy-dense macronutrients but also for neurological development and absorption of fat-soluble vitamins.(43) The relatively low fat intake is similar to the result from Mokoro et al.(Reference Mokoro, Oloya and Aligo44) in Uganda, where dietary fat deficiencies were common in institutional settings due to limited use of oils and animal sources.(Reference Mokoro, Oloya and Aligo44) Carbohydrates are the preferred fuel for the active brain and growing muscles. They are found in a variety of foods. The consumption of carbohydrates exceeded the recommended intake in two age groups (age 5 and 3 years old), were age 2 and 4 years had a lower intake despite a high frequency of consumption of carbohydrate foods. High carbohydrate intake is attributed to excessive consumption of cassava flour, rice, maize, and millet, bakery products such as biscuits, bread buns, and chin-chin, which are made of refined flour. While carbohydrates formed the bulk of most meals (e.g. rice, yams, beans), the low intake observed in children aged 4 and 2 years reflects either small portion sizes, eating once or twice per day, and children who skipped meals due to different reasons like sickness, food rejection, and no availability of food. In similar studies by Nduka et al.(Reference Nduka, Oguoma and Ajayi45) and FAO,(46) carbohydrate intake was found to fall short of recommendations in institutional settings due to infrequent meal variety and insufficient caloric density of starchy staples.
The analysis of micronutrient intake among orphanage children revealed inadequate intake across all age groups, particularly in calcium, vitamin C, and iron. Calcium intake ranged from 141.0 mg to 223.1 mg across age groups, falling far below the WHO/FAO recommended intake of 500–700 mg/day for children aged 2–5 years.(47) This aligns with findings by Ugwoke et al.,(Reference Ugwoke, Ugwu and Ezema48) who reported low calcium intake in Nigerian preschoolers, particularly those in institutional care, due to limited dairy and leafy vegetable consumption. Insufficient calcium during early childhood has been linked to poor bone mineralisation and increased risk of stunting. The mean Iron intake of the children was inadequate for all children aged 2–5years. This pattern is consistent with a recent study by Ibeanu et al.(Reference Ibeanu, Uwaegbute and Onwuka49) and Singwa et al.,(Reference Singwa, Tanya, Ngangmou, Navti, Tamfuh and Ejoh41) which found that older children in low-income settings often suffer from declining iron intake due to over-reliance on plant-based diets low in bioavailable haem iron and inadequate consumption of animal protein. Iron deficiency, if sustained, could lead to cognitive delays, fatigue, and weakened immunity, particularly in environments where infectious disease burden is high.(Reference Ibeanu, Uwaegbute and Onwuka49) There is then an increased need to meet the iron needs of the children in these orphanages and even provide iron supplements to them. Vitamin A intake was generally adequate across age groups is in line with the findings of Ayogu.(50) Vitamin A is critical for vision, immune function, and epithelial integrity, and its deficiency remains one of the leading causes of preventable childhood blindness in sub-Saharan Africa.(Reference Ayogu51) Low riboflavin, vitamin C were attributed to low intake of animal foods and low consumption of fruits and vegetables. Animal foods are rich sources of micronutrients, and when their consumption is low, micronutrient intakes may also be low. This may contribute to general body weakness due to poor glucose metabolism. A similar study by Akinyemi et al.(Reference Akinyemi, Olatunde and Adewale33) reported low vitamin C consumption in institutionalised children in Osun State due to limited access to fresh fruits and vegetables. Vitamin C plays an important role in iron absorption and immune defense, and prolonged deficiency could compromise growth and resistance to infections. Collectively, these results suggest that although some progress has been made in protein-energy nutrition, micronutrient deficiencies, often called “hidden hunger”, remain prevalent among orphanage children. The monotony of institutional diets, limited funding, and lack of caregiver nutrition training may explain these patterns. There is a critical need for dietary diversification and fortification strategies, as well as nutrition-sensitive programming that addresses the root causes of poor food quality in orphanage settings.
Conclusion
This study revealed adequate, over sufficient, and low intake of macro and micronutrients. Factors that influenced nutritional inadequacy in the orphanage homes were a lack of food, improper feeding habits, and a lack of variety of food sources. The assessment of nutritional status using indicators such as stunting, wasting, thinness and MUAC for children showed that the children were malnutrition while few showed no evidence of malnutrition, the rate of stunting and wasting and thinness was observed more in girls than the males, the prevalence of stunting/severe stunting and wasted/severe wasting was more as compared to thinness/severe thinness and obesity. There was low intake of animal protein like meats, eggs, and milk, and fruit and vegetables were scarcely consumed. Children growing up in orphanages are the most vulnerable and disadvantaged members of society, especially if measures to improve their food intake and good nutritional status are not addressed.
Recommendation
Based on the findings of this research, Awareness sessions, including nutrition counselling, should be arranged on a regular basis in orphanages to improve the knowledge of caretakers. More research is needed to provide an iron supplementation study on the study group, as they could be at risk of anemia due to low iron intake and other micronutrients. There is a need to further characterise the eating habits of the children with picking eating behavior, particularly those in lower weight percentiles, and to accesses any related long-term or developmental consequences. The government and other stakeholders should develop an appropriate policy framework to support the nutritional needs of children in orphanages.
Acknowledgements
Ministry of women affairs, lokoja, ministry of mercy orphanage lokoja, Margaret Garba Ohiani orphanage, Zango-daji, Lokoja, Stage corner-stone Christian orphanage lokoja, vitory orphanage, kappa, Christ treasured royal orphanage ministry ogidi, Ekundayo children home, lasanlu, great grace orphanage, one heart one soul calvary catholic prayer ministry, mercy orphanage, ugwalawo, Eju chegahi orphanage, AITAM orphanage, anyigba, ojo gbana orphanage, odu-gegeli, ministry of mercy orphanage, otutulu, god’s will orphanage, Anyigba, Holy family pro-life centre Anyigba The researchers acknowledge all these institutions, and persons involved in all phases of the survey and participants. I also acknowledged the use of AI (ChapGPT) which was used as an insight to generate words for discussion and correction of grammar.
Authorship
Nweze E.I carried out the research wrote the manuscript, Ibeanu V. conceived the idea to carry out the research, interpreted this data with Chukwuemeka’s support. Onyia U. verified the analytical methods, supervised the statistical analysis and gave additional inputs to the study design; and all authors discussed the results, contributing to the final document and had primary responsibility for final content; All authors read and approved the final manuscript.
Financial support
This Survey received no funding.
Competing interests
The authors declare none.
Ethical standards disclosure
This study was conducted according to the guidelines in the Declaration Nutrition and dietetics department, university of Nigeria. All procedures involving research study participants were approved by the Ethical Committee of the Ministry of women affairs, Kogi state. Written informed consent was obtained from all subjects.


 Open access
Open access