


Introduction
Cognitive impairments represent an independent component of schizophrenia, exerting a substantial influence on the progression of the disease and having a pronounced impact on functional outcomes [Reference Jauhar, Johnstone and PJ.1, Reference Kane and Lencz2]. Specifically, these factors encompass social isolation, stigma, substance use, poor dietary habits, and reduced prospects of finding a partner [Reference Jauhar, Johnstone and PJ.1]. Furthermore, the unemployment rate of people with schizophrenia is reported to be more than 80% in Europe [Reference Marwaha, Johnson, Bebbington, Stafford, Angermeyer and Brugha3], making the effective treatment of schizophrenia an urgent issue. These conditions are largely attributable to impairments of neurocognition, including memory, attention, and executive functioning, as well as social cognition [Reference Green, Horan and Lee4, Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5]. Social cognition is defined as the cognitive processes underlying social interactions, and comprises the following domains: emotion perception (the ability to identify and recognize emotions from facial expressions or other cues), emotion processing (the ability to understand and manage emotions), theory of mind [ToM] (the ability to infer the mental states of others), social perception (the general processes required for decoding, understanding, and interpreting social cues), attributional bias (the way an individual usually interprets the cause of social behavior), and empathy [Reference Green, Horan and Lee4, Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5].
Social cognition plays a critical role in the social functioning of people with schizophrenia [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5]. A meta-analysis revealed that people with schizophrenia exhibit significant impairments in the domains of emotion perception (Hedges’ g = 0.89), emotion processing (Hedges’ g = 0.88), ToM (Hedges’ g = 0.96), and social perception (Hedges’ g = 1.04) relative to healthy controls [Reference Savla, Vella, Armstrong, Penn and Twamley6]. Furthermore, social cognition mediates the relationship between neurocognition and functional outcomes [Reference Halverson, Orleans-Pobee, Merritt, Sheeran, Fett and Penn7] and has a greater influence on real-world functioning than neurocognition [Reference Kharawala, Hastedt, Podhorna, Shukla, Kappelhoff and Harvey8]. Hence, the development of treatments for social cognitive impairments is an extremely important goal in schizophrenia.
Pharmacological interventions targeting social cognitive impairments have not been comprehensively evaluated in previous studies from two perspectives: intervention and outcome [Reference Bürkner, Williams, Simmons and Woolley9–Reference Kishi, Ikuta, Oya, Matsunaga, Matsuda and Iwata13]. First, with regard to interventions, there have been individual meta-analyses on oxytocin [Reference Bürkner, Williams, Simmons and Woolley9], antipsychotics [Reference Gabay, Kempton and Mehta10–Reference Feber, Peter, Chiocchia, Schneider-Thoma, Siafis and Bighelli12], and anti-dementia drugs [Reference Kishi, Ikuta, Oya, Matsunaga, Matsuda and Iwata13], which indicates that intranasal oxytocin and atypical antipsychotic drugs may improve ToM [Reference Bürkner, Williams, Simmons and Woolley9] and emotion processing [Reference Gabay, Kempton and Mehta10], respectively, while anti-dementia drugs (e.g., donepezil, galantamine, rivastigmine, and memantine) may elicit limited effects [Reference Kishi, Ikuta, Oya, Matsunaga, Matsuda and Iwata13]; however, no network meta-analysis (NMA) comprehensively comparing the effects of interventions that include other drugs has been reported. Furthermore, NMA is also necessary when assessing randomized controlled trials (RCTs) that compare active drugs. Second, with respect to outcomes, the domains of social cognition were not considered [Reference Bürkner, Williams, Simmons and Woolley9, Reference Kishi, Ikuta, Oya, Matsunaga, Matsuda and Iwata13], or only the domains of ToM on oxytocin [Reference Bürkner, Williams, Simmons and Woolley9] and emotion processing on antipsychotics [Reference Gabay, Kempton and Mehta10, Reference Feber, Peter, Chiocchia, Schneider-Thoma, Siafis and Bighelli12] were included. To date, no comprehensive meta-analyses encompassing all domains of social cognition have been reported. Therefore, there is a strong need for further synthesis of existing research to facilitate the rational selection of compounds, with the aim of contributing to the development of novel therapeutic interventions to address social cognitive impairments.
To our knowledge, no quantitative comparison has been made regarding the ability of psychotropic drugs to enhance social cognition in people with schizophrenia. Notably, this is the first NMA to systematically and comprehensively examine the effects of a diverse array of pharmacological interventions on each domain of social cognition. This study signifies a substantial advancement in the development of treatments for social cognitive dysfunction.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA 2020) guidelines were followed in the execution of this study [Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow14]. The protocol was preregistered in the PROSPERO International Prospective Register of Systematic Reviews (registration number CRD42021293224), and a published protocol [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15] is available.
Search strategy
From inception to July 10, 2021, a comprehensive literature search was conducted using the following electronic bibliographic databases: PubMed, Embase, the Cochrane Central Register of Controlled Trials, PsycINFO, ClinicalTrials.gov, and the International Clinical Trials Registry Platform. The search terms were as follows: “schizophrenia,” “pharmacological intervention,” “social cognition,” and “randomized controlled trial” (see Supplementary 1Material 1) [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15].
Eligibility criteria
The following inclusion criteria [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15] were applied to articles or clinical trial information:
-
(1) RCTs including cluster and crossover trials.
-
(2) Patients with schizophrenia or schizoaffective disorder based on F20–F29 of the International Statistical Classification of Diseases and Related Health Problems Version 10 or Schizophrenia Spectrum and Other Psychotic Disorders of the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), DSM-IV, or DSM-III.
-
(3) Drug interventions (e.g., hormone-related drugs, psychostimulants, antidementia drugs, antipsychotic drugs, antibiotics, and supplements). With regard to the types of interventions, day-only or single doses were also included in this review.
-
(4) At least one outcome was used for the evaluation of social cognition.
Original articles or clinical trial information written in any language were included.
Study selection
YY removed duplicate studies before the initial screening. The 10 investigators (RK, HO, YH, YS, KT, SI, RS, TH, TU, and YY) were divided into five groups, with each group consisting of two investigators. The manuscripts were then divided into five batches by YY, with each pair of investigators overseeing one-fifth of all manuscripts. The first round of screening was conducted independently by each pair of investigators based on the original title and abstract. Subsequently, any study that was selected by at least one reviewer was subjected to a second round of screening. In the subsequent second screening, five groups of two reviewers each independently evaluated the eligibility of the full text. The senior reviewer (RO) was tasked with resolving any disagreements that arose in these evaluations [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15].
Data extraction
A total of six investigators (RK, HO, SI, TH, TU, and YY) were divided into three groups, with each group consisting of two individuals. These groups were tasked with independently extracting the following relevant information from the included studies: author, trial design, participants’ demographics, details of the intervention, and measurement tools. For measurements of social cognition, data were extracted through outcomes related to the following domains: emotion perception, emotion processing, ToM, social perception, attributional bias, and empathy [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5]. Utilizing these data, we then proceeded to assess the effects of interventions on each of the six domains. The senior reviewer (RO) arbitrated in the event of any disagreements. In instances where the relevance of the measurement to social cognition was ambiguous, MN sought further elucidation from the authors regarding the outcomes. For ongoing clinical trial information included in the second screening, MN also requested detailed information from the researcher(s). In instances where MN did not receive a response from the author(s), they made up to three follow-up inquiries, separated by 1-week intervals. If this approach proved unsuccessful or impracticable, the studies in question were excluded from the analysis. It was noted that several studies satisfied the inclusion criteria for the systematic review but lacked pertinent information regarding the measures of social cognition that had been utilized. Consequently, the results of these studies were excluded from the meta-analysis [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15].
Quality assessments and risk of bias
Three groups of two investigators (RK, HO, SI, TH, TU, and YY) independently performed a quality assessment using the Cochrane Risk of Bias 2 Tool [Reference Sterne, Savović, Page, Elbers, Blencowe and Boutron16]. This tool assessed potential biases through signaling questions in the following domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. To enhance the precision of the quality assessments, all members participated in a training course on quality assessment using the Cochrane Risk of Bias 2 tool. This course included self-study materials and two days of exercises organized by Cochrane Japan. The senior reviewer (RO) arbitrated in the event of any disagreements [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15].
Targeted domains of social cognition and intervention
We focused on the following six domains of social cognition: emotion perception, emotion processing, ToM, social perception, attributional bias, and empathy [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5]. For drug interventions, a wide variety of candidates were considered for inclusion (e.g., hormone-related drugs, psychostimulants, antidementia drugs, antipsychotic drugs, antidepressant drugs, antibiotics, and supplements) [Reference Yamada, Okubo, Tachimori, Uchino, Kubota and Okano15].
Statistical analyses
For each domain of social cognition, we constructed a network diagram in which nodes represent the domains of the pharmacological interventions and edges connect interventions that were directly compared in the selected trials. Subsequently, a hierarchical Bayesian model was developed to obtain integrated estimates of the effect sizes between interventions. A detailed explanation regarding the model structure is provided in the Supplementary Materials (see Supplementary Material 2). The standardized mean difference (SMD) was used as the measure of observed effect sizes, and the SMD values in the selected trials were calculated using available information from each study. The specific definitions and calculation methods of the observed SMD are also described in the Supplementary Materials (Supplementary Material 2).
Posterior distributions of the effect sizes were sampled via Markov chain Monte Carlo (MCMC) simulation based on the Gibbs sampling algorithm. Four chains were run with a burn-in period of 5,000 iterations, followed by 100,000 iterations (thinned every 10th sample) per chain. Convergence was assessed by examining trace plots. If multi-arm trials were included in the analysis, inconsistency between direct and indirect comparison was examined using the node-splitting method, estimating the inconsistency factor, and comparing the analysis model with the unrelated mean effects model [Reference Dias, Welton, Caldwell and Ades17]. Heterogeneity between trials was evaluated via comparison of the analysis model with the unrelated study effects model. Model comparison was performed using the deviance information criterion [Reference Spiegelhalter, Best, Carlin and Van Der Linde18]. More details and results on the inconsistency and heterogeneity evaluation are provided in the Supplementary 1Materials (see Supplementary Material 2, Figure S1, and Table S1). Sensitivity analyses were performed to assess the robustness of the results with respect to assumptions about the within-study correlation in multi-arm trials, detailed in the Supplementary Materials (Supplementary Material 2, Section 4). With regard to the assessment scales, sensitivity analyses were conducted using exclusively the scales recommended in the Social Cognition Psychometric Evaluation (SCOPE) study [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5, Reference Pinkham, Penn, Green, Buck, Healey and Harvey19]. In the context of the emotion processing domain, a sensitivity analysis was conducted employing solely the Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT) [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5]. Estimated effect sizes were presented as posterior means with 95% credible intervals (CIs), and the treatment rankograms were provided based on the cumulative probability of being ranked in terms of effectiveness among the interventions in the MCMC chains.
The analysis was conducted using R (ver. 4.2.2). Model construction and estimation were performed with the gemtc package [Reference van Valkenhoef, Kuiper and van Valkenhoef20]. We added a sampling function for the inconsistency factor to the original code in the package. The code with this addition is available from https://github.com/t-yui/gemtc/tree/inconsistency_factor.
Results
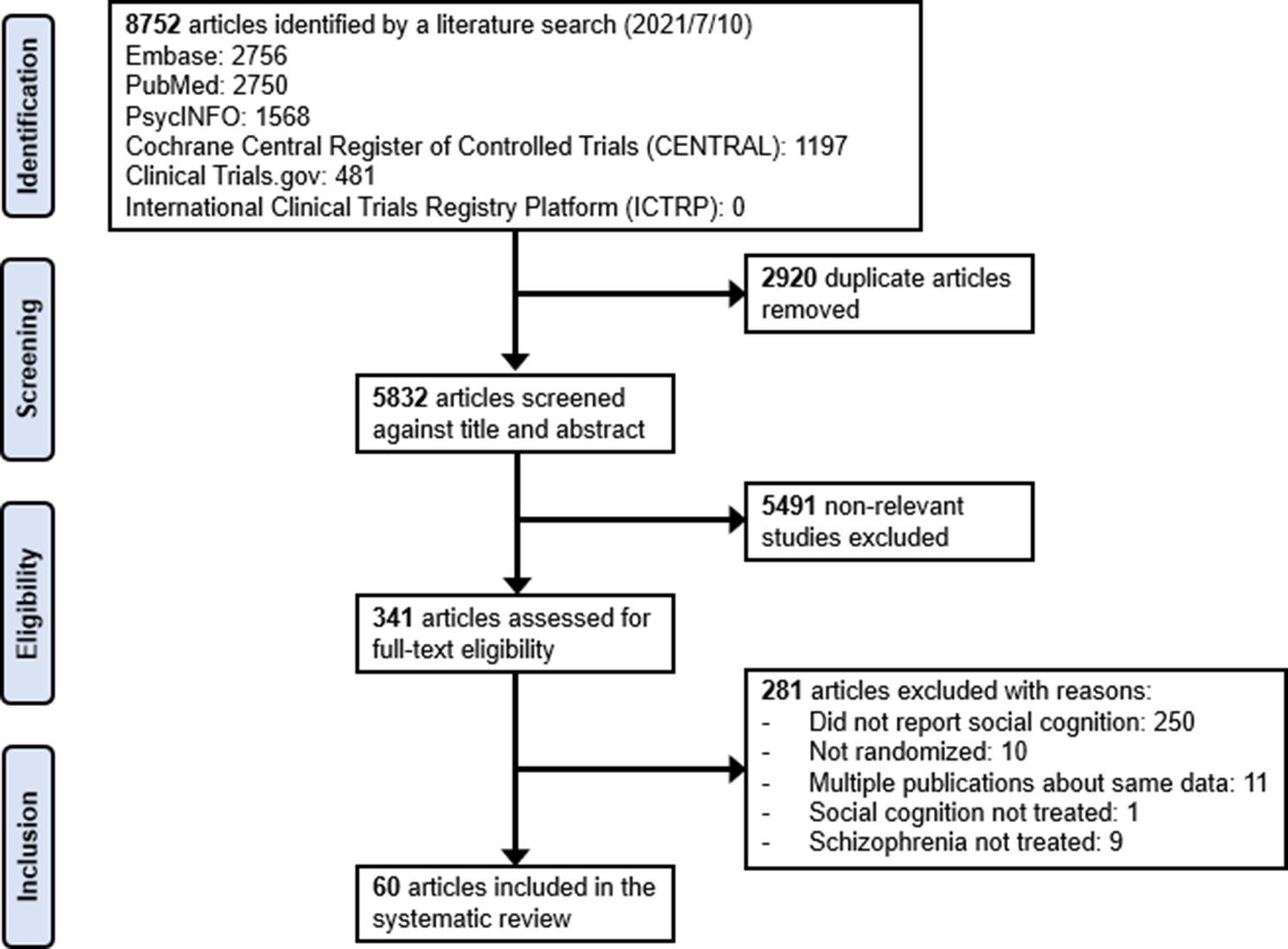
The preliminary search yielded a total of 8,752 records. After the elimination of duplicates, 5,832 articles were screened by title and abstract, leaving 341 potentially eligible records. A subsequent full-text review identified 60 articles that met the inclusion criteria for the systematic review. The primary reasons for exclusion were that the outcomes or the assessment of the outcomes did not align with the established inclusion criteria. The PRISMA study selection flowchart is shown in Figure 1. A summary of the risk of bias is presented in Figure 2.
PRISMA study selection flowchart.

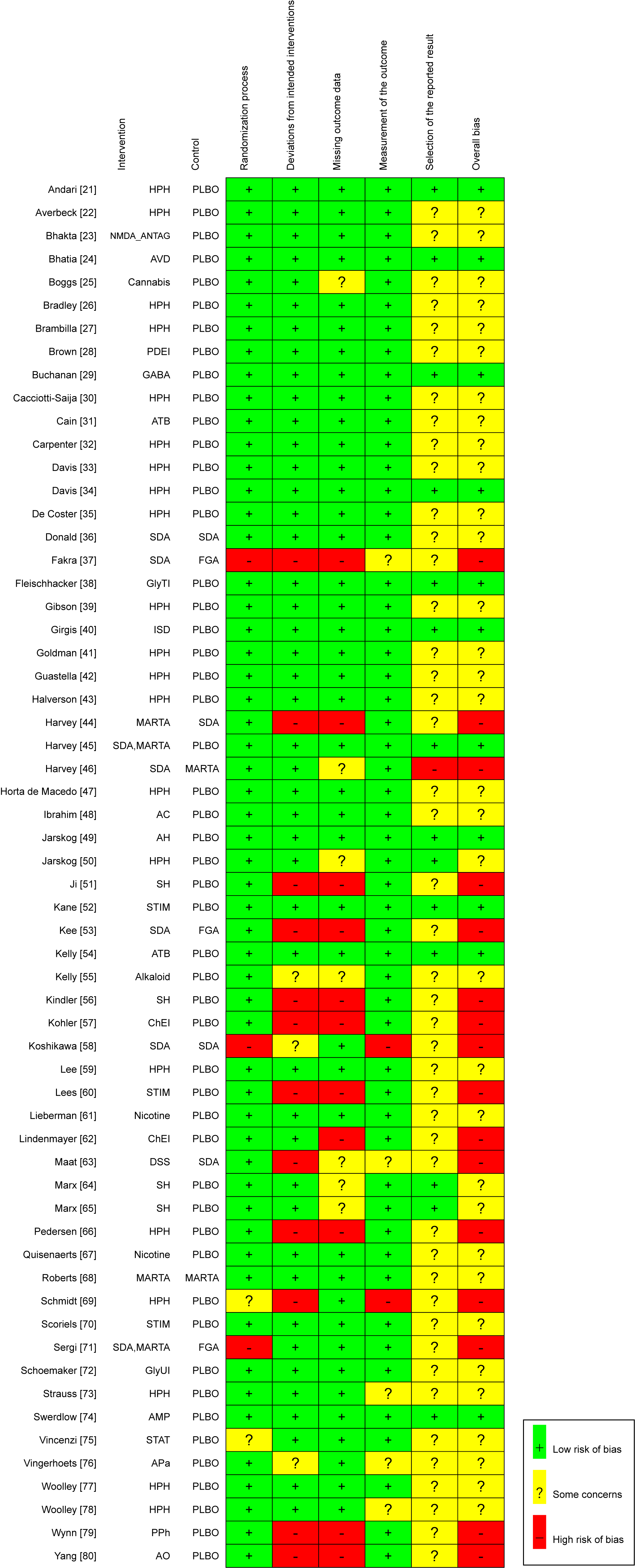
Risk of bias of included studies. HPH, hypothalamic hormone; NMDA_ANTAG, N-methyl-D-aspartate antagonist; AVD, antiviral drug; PDEI, phosphodiesterase 9 inhibitor; GABA, γ-aminobutyric acid (A) α2/α3 partial agonist; ATB, antibiotic; SDA, serotonin–dopamine antagonist; GlyTI, glycine transporter inhibitor; ISD, immunosuppressive drug; MARTA, multi-acting receptor-targeted antipsychotic; AC, anticonvulsant; AH, antihistamine; SH, sex hormone modulator; STIM, stimulant; ChEI, cholinesterase inhibitor; DSS, dopamine system stabilizer; GlyUI, selective glycine uptake inhibitor; AMP, amphetamine; STAT, statin; APa, antiparkinson; PPh, polyphenol; AO, antioxidant; PLBO, placebo; FGA, first-generation antipsychotic.

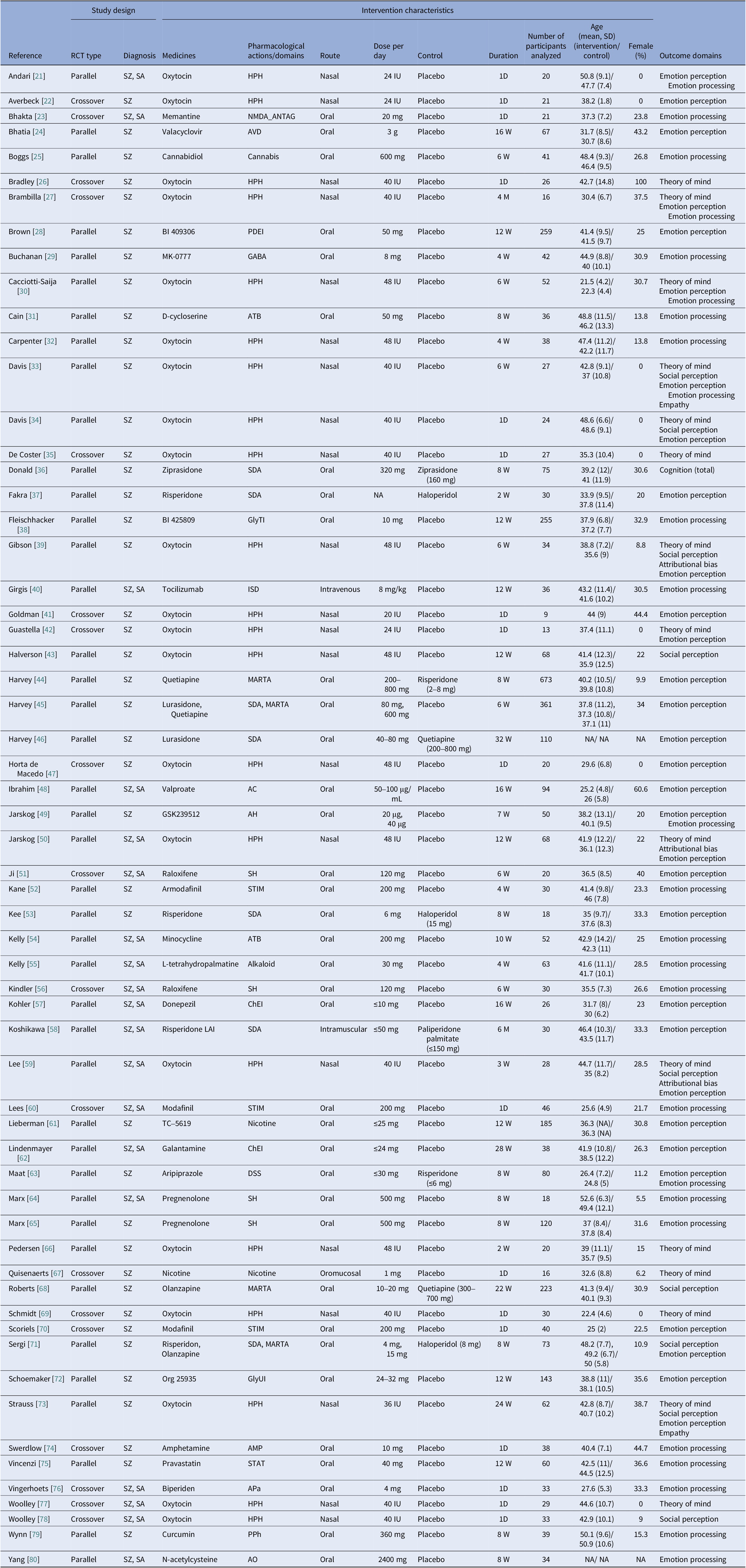
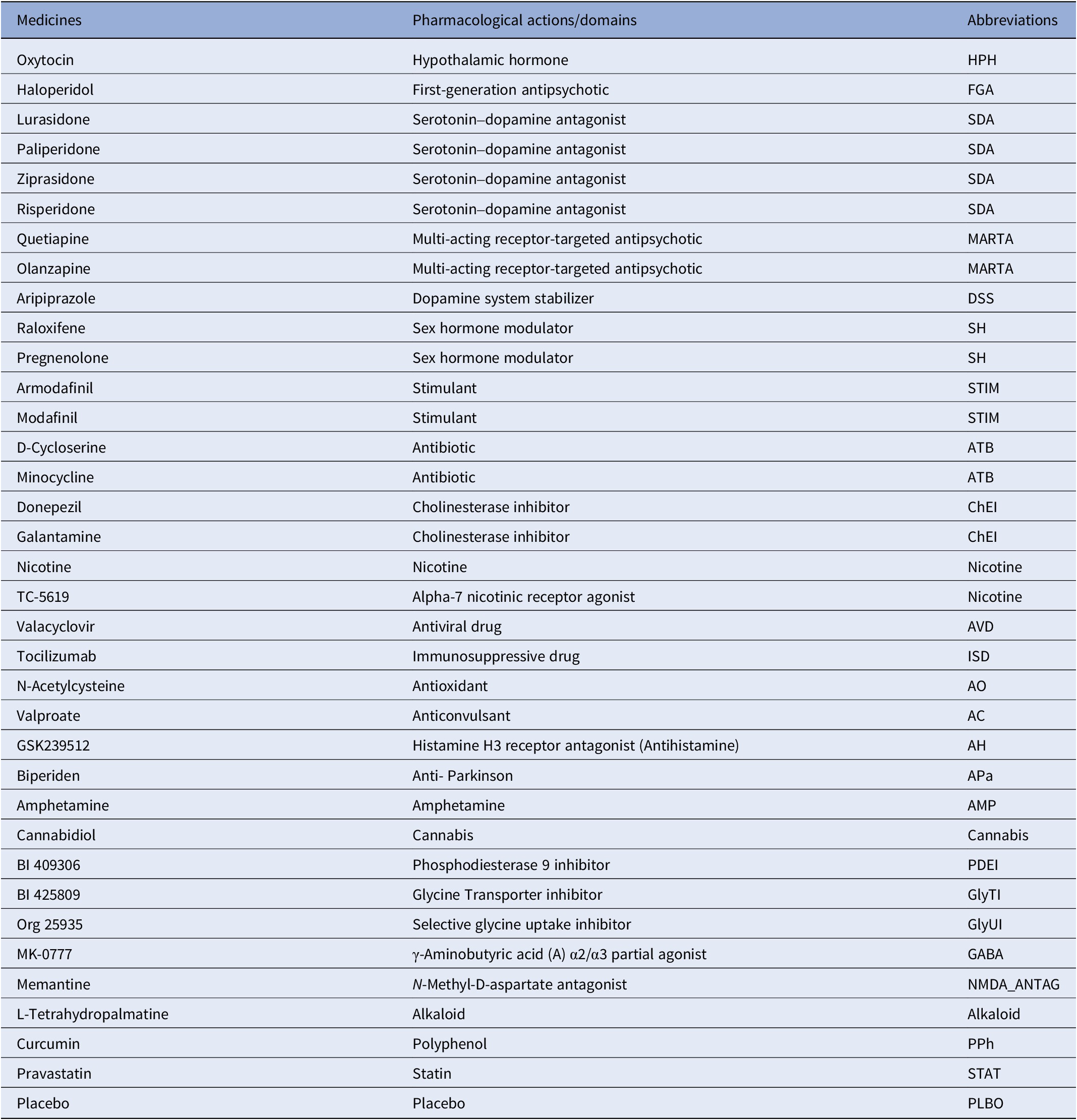
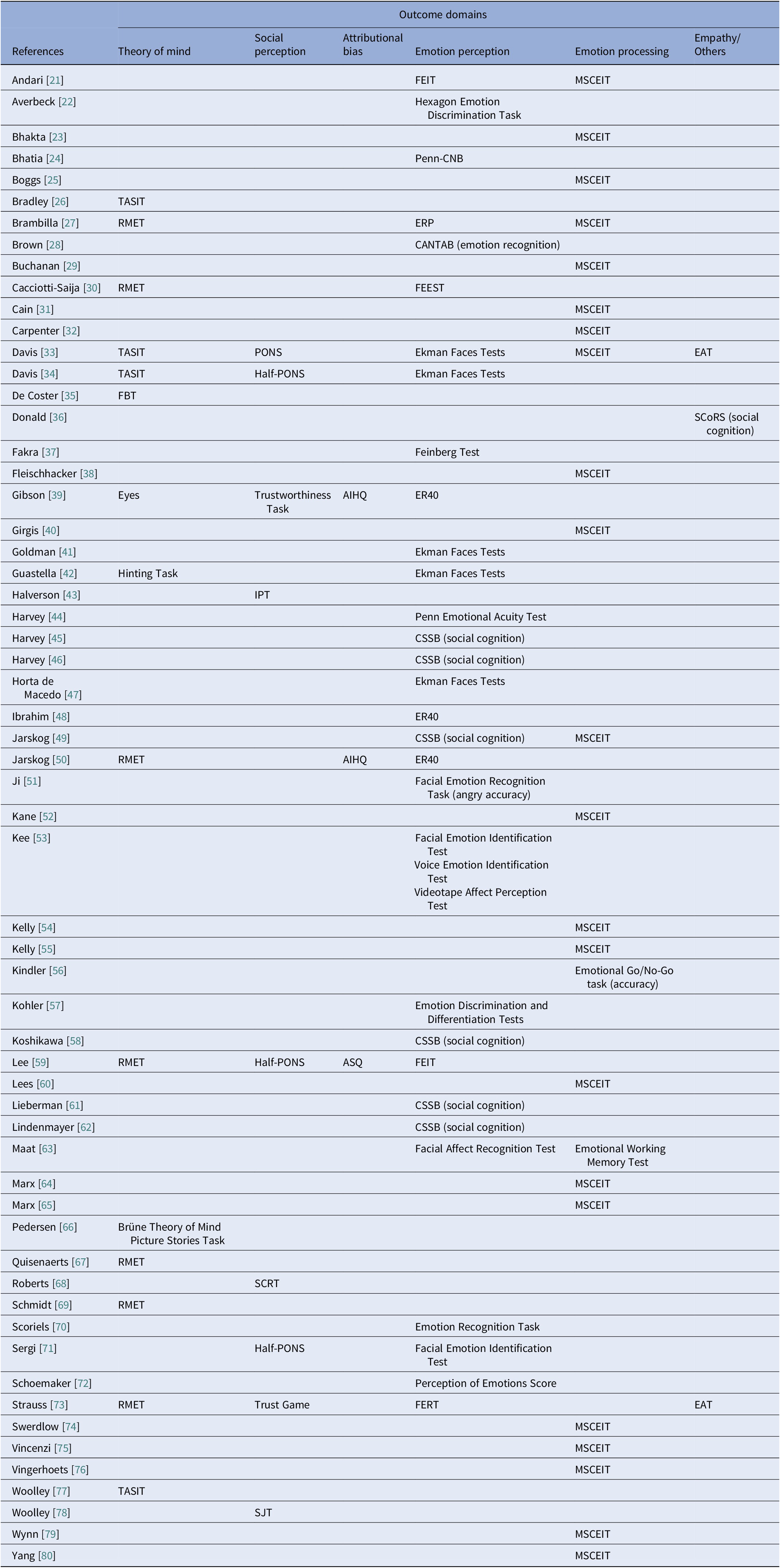
Table 1 presents a comprehensive overview of the characteristics of the included studies. The 60 studies encompassed a total of 4,270 subjects. A total of 36 interventional agents were identified, which were subsequently classified into 27 domains based on their respective mechanisms of action (see Table 2). The hypothalamic hormone oxytocin emerged as the most prevalent intervention agent, with 21 studies (35% of all studies), followed by serotonin–dopamine antagonists with 7 studies (11%) (Tables 1 and 2). Regarding outcomes, rating scales were extracted for each domain of social cognition (Table 3). The majority of these domains were focused on emotion perception (31 studies, 51%), followed by emotion processing (24 studies, 40%) and ToM (15 studies, 25%). The MSCEIT was used for most of the emotion processing evaluations (22 studies), though it should be noted that multiple tools were employed, including the Penn Emotion Recognition Test (three studies) and Face Emotion Identification Test (two studies) in the domain of emotion perception, and the Reading the Mind in the Eyes Task (seven studies) and The Awareness of Social Inference Test (four studies) for the domain of ToM (see Tables 1 and 3). An evaluation of risk of bias was conducted. The results indicated that 55 (91.6% of all studies), 45 (75%), and 53 (88.3%) studies exhibited low risk of bias in the randomization process, deviations from intended interventions, and measurement of outcomes, respectively (Figure 2).
Summary of included publications

Abbreviations: RCT, randomized controlled trial; SD, standard deviation; D, day(s); W, week(s); M, month(s); SZ, schizophrenia; SA, schizoaffective disorder; NA, not available; LAI, long-acting injection; HPH, hypothalamic hormone; NMDA_ANTAG, N-methyl-D-aspartate antagonist; AVD, antiviral drug; PDEI, phosphodiesterase 9 inhibitor; GABA, γ-aminobutyric acid (A) α2/α3 partial agonist; ATB, antibiotic; SDA, serotonin–dopamine antagonist; GlyTI, glycine transporter inhibitor; ISD, immunosuppressive drug; MARTA, multi-acting receptor-targeted antipsychotic; AC, anticonvulsant; AH, antihistamine; SH, sex hormone modulator; STIM, stimulant; ChEI, cholinesterase inhibitor; DSS, dopamine system stabilizer; GlyUI, selective glycine uptake inhibitor; AMP, amphetamine; STAT, statin; APa, anti-Parkinson; PPh, polyphenol; AO, antioxidant.
Pharmacological actions/domains

Summary of the applied social cognition measures

Abbreviations: TASIT, The Awareness of Social Inference Test; RMET, Reading the Mind in the Eyes Task; FBT, False Belief Task; Eyes, Reading the Mind in the Eyes Test; Half-PONS, Half Profile of Nonverbal Sensitivity; SCRT, Social Cue Recognition Task; IPT, Interpersonal Perception Task; SJT, Social Judgment Task; AIHQ, Ambiguous Intentions and Hostility Questionnaire; ASQ, Attributional Style Questionnaire; FEIT, Face Emotion Identification Test; Penn-CNB, Penn Cognitive Neuropsychological Battery; ERP, Emotional Priming Paradigm; FEEST, Facial Expressions of Emotions Task; ER40, Penn Emotion Recognition Test; CSSB, CogState Schizophrenia Battery; CANTAB, Cambridge Neuropsychological Test Automated Battery; FERT, Facial Emotion Recognition Test; MSCEIT, Mayer–Salovey–Caruso Emotional Intelligence Test; EAT, Empathic Accuracy Task; SCoRS, Schizophrenia Cognition Rating Scale.
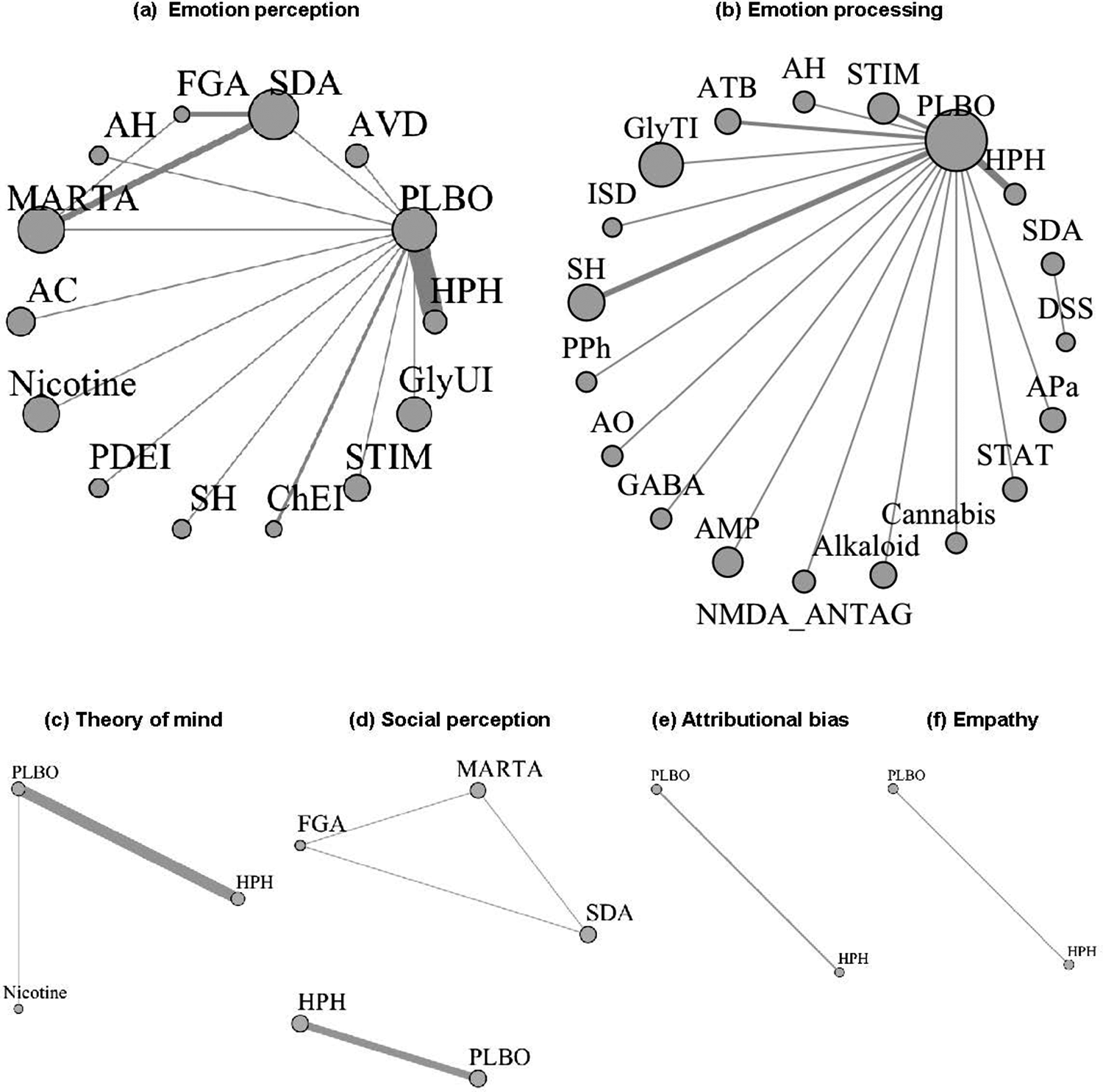
The network plot for each domain of social cognition is shown in Figure 3. The thickness of the join line represents the number of studies, and the size of the node represents the number of subjects. In emotion perception, serotonin–dopamine antagonists, multi-acting receptor-targeted antipsychotics, and first-generation antipsychotics formed a closed loop, indirect comparison of multi-acting receptor-targeted antipsychotics versus first-generation antipsychotics (p = 0.2921, effect size, 0.89; 95% CI, −0.19 to 2.1). In emotion processing, the largest number of studies compared placebo and hypothalamic hormones, followed by sex hormone modulators. For ToM, the majority of the comparisons were between placebo and hypothalamic hormones. With respect to social perception, the network of serotonin–dopamine antagonists, multi-acting receptor-targeted antipsychotics, and first-generation antipsychotics formed a closed loop (Figure 3).
Network plot of outcomes related to social cognition. HPH, hypothalamic hormone; NMDA_ANTAG, N-methyl-D-aspartate antagonist; AVD, antiviral drug; PDEI, phosphodiesterase 9 inhibitor; GABA, γ-aminobutyric acid (A) α2/α3 partial agonist; ATB, antibiotic; SDA, serotonin–dopamine antagonist; GlyTI, glycine transporter inhibitor; ISD, immunosuppressive drug; MARTA, multi-acting receptor-targeted antipsychotic; AC, anticonvulsant; AH, antihistamine; SH, sex hormone modulator; STIM, stimulant; ChEI, cholinesterase inhibitor; DSS, dopamine system stabilizer; GlyUI, selective glycine uptake inhibitor; AMP, amphetamine; STAT, statin; APa, anti-Parkinson; PPh, polyphenol; AO, antioxidant; PLBO, placebo; FGA, first-generation antipsychotic.

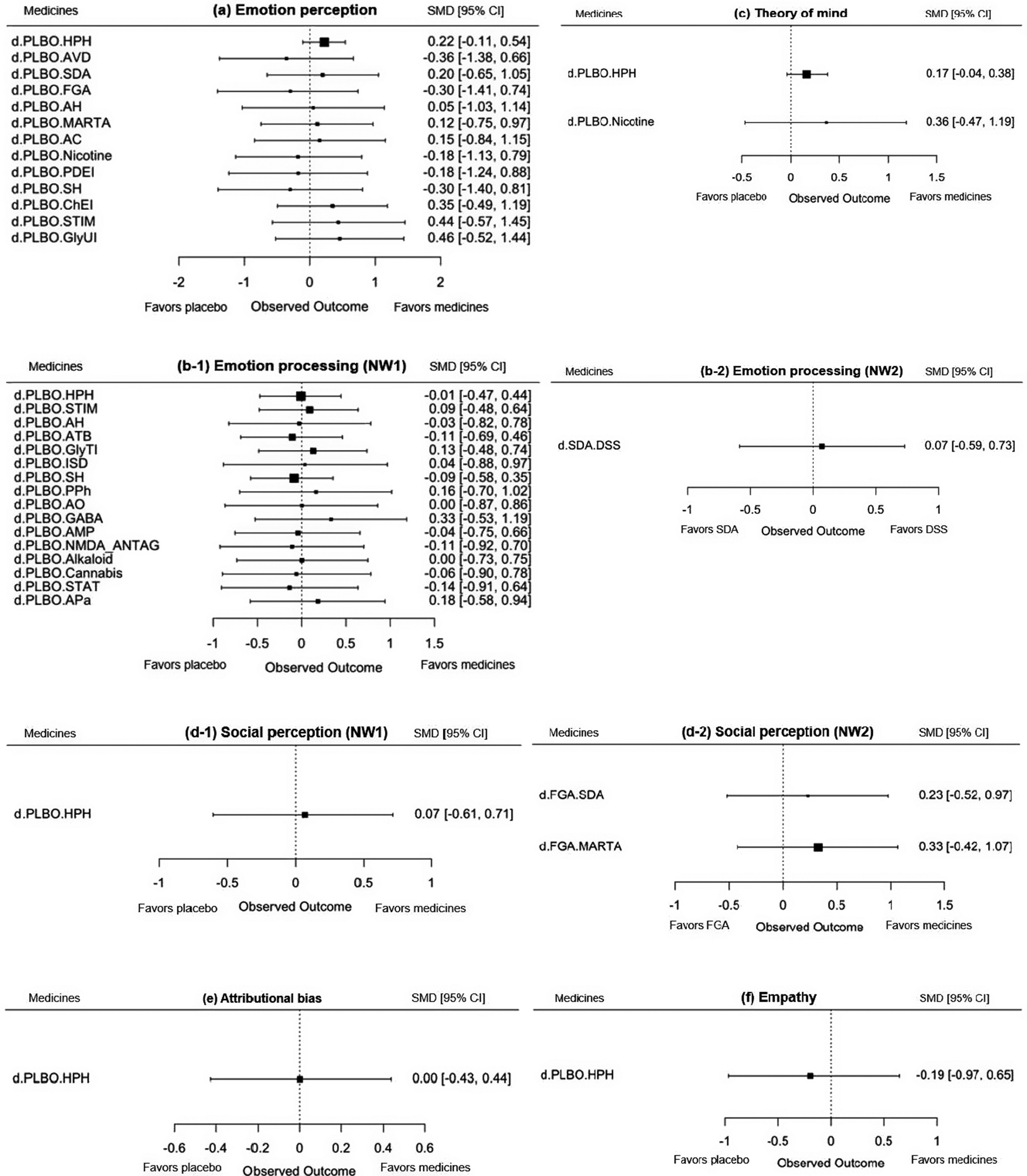
Forest plots of drugs (Figure 4) and league tables (Supplementary 1Figures 1–3) for each domain of social cognition are shown. The analysis revealed that no drug demonstrated a significant improvement in any domain with respect to emotion perception, as evidenced by the findings for hypothalamic hormones (SMD, 0.22; 95% CI, −0.11 to 0.54), selective glycine uptake inhibitors (SMD, 0.46; 95% CI, −0.52 to 1.44), and stimulants (SMD, 0.44; 95% CI, −0.57 to 1.45); for emotion processing, γ-aminobutyric acid (A) α2/α3 partial agonist (GABA), which was functionally selective for the α2 and α3 subunits, with 10–20% of the potency of a γ-aminobutyric acid (A) α2 full agonist (SMD, 0.33; 95% CI, −0.53 to 1.19); for ToM, hypothalamic hormones (SMD, 0.17; 95% CI, −0.04 to 0.38) and nicotine (SMD, 0.36; 95% CI, −0.47 to 1.19); and for social perception, hypothalamic hormones (SMD, 0.07; 95% CI, −0.61 to 0.71) (Figure 4). With regard to the assessment scales, sensitivity analyses were conducted using exclusively the scales recommended in the SCOPE study and using the MSCEIT (emotion processing domain) solely. However, the results were largely consistent with the main analysis (Supplementary 1Figure 4).
Forest plot of drugs versus placebo for outcomes related to social cognition. SMD, standardized mean difference; CI, credible interval; NW, network; HPH, hypothalamic hormone; NMDA_ANTAG, N-methyl-D-aspartate antagonist; AVD, antiviral drug; PDEI, phosphodiesterase 9 inhibitor; GABA, γ-aminobutyric acid (A) α2/α3 partial agonist; ATB, antibiotic; SDA, serotonin–dopamine antagonist; GlyTI, glycine transporter inhibitor; ISD, immunosuppressive drug; MARTA, multi-acting receptor-targeted antipsychotic; AC, anticonvulsant; AH, antihistamine; SH, sex hormone modulator; STIM, stimulant; ChEI, cholinesterase inhibitor; DSS, dopamine system stabilizer; GlyUI, selective glycine uptake inhibitor; AMP, amphetamine; STAT, statin; APa, anti-Parkinson; PPh, polyphenol; AO, antioxidant; PLBO, placebo; FGA, first-generation antipsychotic.

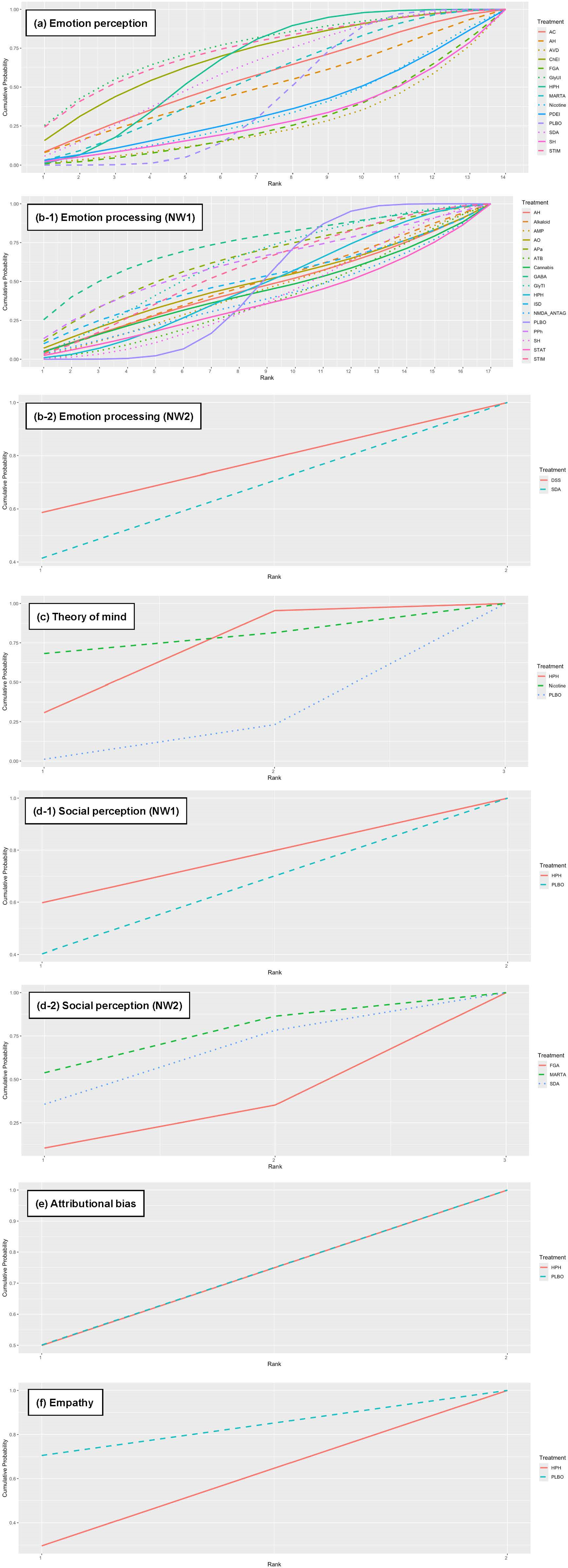
Figure 5 shows the rank probability of treatment choice for each domain of social cognition: for emotion perception, the most effective choice was selective glycine uptake inhibitors, followed by stimulants. For emotion processing, the most effective treatment was GABA. With respect to ToM, the best choice was nicotine (Figure 5).
Ranked probability of outcomes related to social cognition. NW, network; HPH, hypothalamic hormone; NMDA_ANTAG, N-methyl-D-aspartate antagonist; AVD, antiviral drug; PDEI, phosphodiesterase 9 inhibitor; GABA, γ-aminobutyric acid (A) α2/α3 partial agonist; ATB, antibiotic; SDA, serotonin–dopamine antagonist; GlyTI, glycine transporter inhibitor; ISD, immunosuppressive drug; MARTA, multi-acting receptor-targeted antipsychotic; AC, anticonvulsant; AH, antihistamine; SH, sex hormone modulator; STIM, stimulant; ChEI, cholinesterase inhibitor; DSS, dopamine system stabilizer; GlyUI, selective glycine uptake inhibitor; AMP, amphetamine; STAT, statin; APa, anti-Parkinson; PPh, polyphenol; AO, antioxidant; PLBO, placebo; FGA, first-generation antipsychotic.

Discussion
In this study, we report the first NMA to comprehensively evaluate the effects of pharmacotherapy in all domains of social cognition. In the domains of ToM, social perception, attributional bias, and empathy, the number of studies was limited, and the networks were relatively sparse. A cautious approach is imperative when interpreting NMA in these domains, and it is anticipated that further accumulation of research findings will be necessary before a re-examination of these analyses can be undertaken. While no agents demonstrated substantial enhancement in each domain of social cognition, our findings identified several candidate compounds that offer directions for future research.
Oxytocin was the most frequently extracted intervention drug in this systematic review (35% of all studies), and no significant improvements were identified in any of the domains of social cognition. An earlier meta-analysis found an effect size of 0.2 when restricted to ToM, but no substantial improvement in overall social cognitive functioning [Reference Bürkner, Williams, Simmons and Woolley9]. Oxytocin, a neuropeptide predominantly synthesized in the hypothalamic nucleus, functions as a neurotransmitter and neuromodulator within the brain. Research has demonstrated its role in fostering social attachment and the formation of social bonds [Reference Young and Barrett81]. Therefore, it is assumed to be related to social cognition, and meta-analyses have reported improvement effects on empathy (Hedges’ g = 0.49) and ToM (Hedges’ g = 0.21) in neurodevelopmental disorders [Reference Keech, Crowe and Hocking82]. Conversely, the present review found that oxytocin did not enhance any domains of social cognition, indicating that the mechanism of action of oxytocin may differ in social cognition in neurodevelopmental disorders and social cognitive impairment in schizophrenia.
Glycine, stimulants, and GABA represent novel compounds that have emerged as promising candidates for the treatment of social cognitive impairments in schizophrenia. Specifically, selective glycine uptake inhibitors (SMD, 0.46) and stimulants (SMD, 0.44) have been identified as leading candidates for emotion perception, with GABA (SMD, 0.33) demonstrating promise in emotion processing (Figure 5). However, there are still a few validation studies of these candidate compounds, and the RCTs have been relatively small in size (Table 1). Further validation by large-scale RCTs is needed to determine the most effective therapeutic uses of these compounds.
Accurately measuring pharmacological effects on social cognition requires the implementation of uniform rating scales for each domain of social cognition. In the present study, we comprehensively examined the effects of drug intervention on domains of social cognition that had not been previously reported. However, our findings revealed no significant improvement in any domain. This may be indicative of genuine pharmacological ineffectiveness; however, methodological limitations, such as heterogeneity of tools, short treatment duration, and underpowered trials, are also considered to be involved. One factor contributing to this issue is the utilization of diverse scales for assessing social cognition, particularly in domains other than emotion processing (Table 3). This methodological approach poses a significant challenge in determining the effectiveness of these scales [Reference Okano, Kubota, Okubo, Hashimoto, Ikezawa and Toyomaki83].
The development and dissemination of an international battery of measures of social cognition is an urgent issue. The SCOPE study sought to establish consensus on the theoretical structure of social cognition in schizophrenia and to systematically evaluate the psychometric properties of existing measures [Reference Pinkham, Penn, Green, Buck, Healey and Harvey19]. In the present study, the MSCEIT was utilized uniformly in 22 of 24 studies (91%) for the purpose of emotion processing. On the other hand, for the domains of emotion perception, ToM, social perception, and attributional bias, respectively, 12, 80, 11, and 66% of the studies employed the scales recommended in the SCOPE study. It is expected that, in the future, a comprehensive evaluation battery for social cognition, employing the recommended rating scales, will be developed and utilized in clinical trials.
In light of the pervasive utilization of pharmacological strategies for the treatment of schizophrenia, the current findings have substantial implications for enhancing social cognitive function. Notably, since no effective medication for social cognition currently exists, cognitive rehabilitation – which has demonstrated efficacy – remains the first-line treatment [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5]. However, the identification of candidate compounds, such as selective glycine uptake inhibitors and GABA, suggests that future large-scale, targeted RCTs may reveal the potential to enhance social cognitive function.
Limitations
This study has several limitations. First, the duration of illness, duration of medication, and concomitant therapy were not taken into account in the analysis. The intervention effects of various medications may differ depending on these factors. Especially, inclusion of very short-duration (e.g., 1-day) trials may dilute the capacity to detect meaningful effects. Second, given that no stratification is performed based on concomitant antipsychotic class, interactions with candidate drugs may occur. Third, there was little closed-loop formation in the current NMA. Therefore, indirect comparisons regarding the precise effects of various drugs could not be adequately examined. Finally, compounds with high rank probability of treatment choice were discussed as promising candidate drugs, but fundamentally, none of the drugs significantly improved social cognitive function compared to a placebo. The rank probability of treatment choice is merely an indicator of priority for each drug selection.
Conclusions
At present, no pharmacological interventions have been demonstrated to be efficacious for social cognitive impairments in schizophrenia. Consequently, there is a need for future research to explore novel candidate compounds that diverge from conventional mechanisms of action and that are tailored to address social cognition. Moreover, the dissemination of a uniform test battery to measure social cognition is an urgent issue [Reference Corbera, Kurtz, Achim, Agostoni, Amado and Assaf5, Reference Franzen, Watermeyer, Pomati, Papma and Nielsen84]. In sum, a larger RCT is warranted to test the intervention effects of the new candidate compounds on each domain of social cognition.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2026.10159.
Data availability statement
Detailed search strategies and analysis methods are available online as Supplementary Materials.
Acknowledgments
The authors would like to express their gratitude to all researchers who provided data in response to their requests for additional data related to their studies.
Author contribution
YY, RO, and NW designed this study. MN, RK, HO, YH, YS, KT, SI, RS, TH, TU, and YY collected information of literature. RK, HO, YH, YS, KT, SI, RS, TH, TU, YY, and RO reviewed the literature. YT and HT conducted the statistical analysis. RO, NW, HT, TS, NH, SI, and TN provided supervision. YY wrote the first draft of the manuscript, and RO and NW reviewed it and provided critical revisions. Other authors also revised the manuscript. All authors approved the final version of the manuscript.
Financial support
This work was partially supported by the Japan Agency for Medical Research and Development Grant No. JP20dk0307092 to RO, as well as the Japan Society for the Promotion of Science KAKENHI Grant No. 24 K10697 to YY. The funders had no role in the study design, collection, analysis, and interpretation of data, writing of the report, and decision to submit the article for publication.
Competing interests
The authors declare none.



 Open access
Open access
Comments
No Comments have been published for this article.