


Highlights
-
This is the first study describing post-stroke spasticity treatment in everyday clinical practice within Canada.
-
There were evidentiary gaps in provision of post-stroke spasticity treatment including overuse of systemic oral baclofen and potential underuse of focal spasticity injections.
-
Strategies to improve alignment of PSS treatment with guideline recommendations is warranted.
Introduction
Spasticity is defined as a “velocity- and muscle length-dependent increase in resistance to externally imposed muscle stretch. It results from hyperexcitable descending excitatory brainstem pathways and from the resultant exaggerated stretch reflex responses. Other related motor impairments, including abnormal synergies, inappropriate muscle activation and anomalous muscle coactivation, coexist with spasticity and share similar pathophysiological origins” (1). This condition can limit joint movement and overall mobility, as well as contribute to secondary maladaptation such as joint stiffness and pain (2, 3). Spasticity can be an impairing feature of a number of disorders including stroke, a common neurological disease resulting from a sudden loss of brain function by a brain blood vessel blockage or rupture that leads to neuronal cell death (4). Post-stroke spasticity (PSS) has been reported to occur in 25% to 40% of stroke survivors, with 2% to 13% experiencing disabling or problematic spasticity where there is a need for intervention when marked limitation in range of motion occurs and/or imposes a profound negative impact on comfort, function, or well-being (3, 5, 6). While variable, the prevalence of PSS appears highest in the first 6 months after stroke (6); development of new onset PSS at 12 months is considered infrequent (7).
The Canadian Stroke Best Practice Recommendations for the management of PSS include rehabilitation treatments (antispastic pattern positioning, range of motion exercise and/or stretching [supported by limited-to-moderate evidence levels]), oral anti-spasticity medications, focal injections with botulinum toxin and intrathecal baclofen; it is strongly advised that complex cases of spasticity be referred to a specialist for management (8). Over the years, oral medications have been used to treat spasticity of various origins (9–11). However, high-quality evidence on their effectiveness in PSS is lacking, and dose-dependent side effects of drowsiness, sedation, muscle weakness and fatigue are common (12–16). The Canadian Stroke Best Practice Recommendations indicate that oral anti-spasticity medications, specifically baclofen and tizanidine, can be considered for the treatment of more generalized disabling spasticity after a stroke (supported by limited evidence), but caution that benefits appear to be marginal and the side effects of fatigue and drowsiness are common (8). Botulinum toxin injection is widely considered the treatment of choice for focal or multifocal spasticity based on established evidence of its safety and efficacy in the local reduction of spasticity after injection (17, 18). Recommendations suggest injections with botulinum toxin for the pharmacological treatment of focal symptomatically distressing spasticity after stroke; this recommendation is based on strong evidence for range of motion, and for upper and lower extremities among those treated more than 6 months after stroke (8). Intrathecal baclofen and surgical intervention are recommended for consideration in specific cases of severely disabling and/or painful spasticity (3, 8).
Understanding PSS treatment in everyday clinical practice may identify opportunities to optimize PSS treatment and improve patient care; to date, few such studies have been conducted (11, 19, 20). We previously described time to initiation of PSS treatment and discussed issues related to delays in treatment (21). The objective of this retrospective observational cohort study was to describe the types of PSS treatment received in Alberta, Canada, using high-quality population-based administrative health data and discuss their use in relation to guideline recommendations (8).
Methods
The institutional review board at the University of Alberta approved this study (Pro00093914), which used retrospective administrative data without any direct intervention or personal identifiable information; informed consent was waived. This study is reported according to the Reporting of Studies Conducted using Observational Routinely Collected Data (RECORD) guidelines (22).
Study design
A retrospective observational population-based cohort study was conducted using administrative health data from Alberta between April 1, 2002 and March 31, 2020 that included adults who experienced a stroke between April 1, 2012 and March 31, 2017 and subsequently initiated spasticity treatment up to March 31, 2019; a look-back period before the stroke as far back as April 1, 2002, and a follow-up period after PSS initiation that extended for ≥1 year up to March 31, 2020 were included (see Supplementary Figure 1 for a study diagram).
Data source
The Canadian healthcare system is publicly funded, providing residents with universal access to all medically necessary hospital and physician services without paying out-of-pocket; universal prescription drug coverage is not included. In Alberta, individuals are responsible for the cost of prescription drugs outside of hospitals, auxiliary hospitals and nursing homes. Many individuals and their dependents have coverage for prescription drugs provided through employer-sponsored private supplementary health insurance plans. Others have coverage through federal or provincial sponsored plans. Alberta Health supplementary benefit plans include a premium-based plan and a premium-free plan (for seniors [aged ≥65 years], adults in the Assured Income for the Severely Handicapped program, those considered low-income and people diagnosed as being palliative).
In Alberta, the fourth most populous Canadian province (3.9 to 4.2 million people [2012 to 2017]), healthcare is administered under the Alberta Health Care Insurance Plan (AHCIP), in which over 99% of Albertans participate (23). Each participant is assigned a unique person-level identifier (Personal Health Number); this was used to link individuals across datasets. A person-level data extract from the Discharge Abstract Database (DAD), National Ambulatory Care Reporting System (NACRS), Millennium Scheduler, Virtual Address eXtension (VAX), Practitioner Claims, Pharmaceutical Information Network (PIN) and Vital Statistics were linked to the Population Registry that contains demographic information for all Albertans with AHCIP coverage; data were then deidentified by the data custodians and provided to the researchers. DAD and NACRS include information on patients discharged from hospitals and facility-based ambulatory care settings including emergency departments, respectively; International Classification of Disease – Version 10 – Canadian Enhancement (ICD-10-CA) codes are used and contain a most responsible diagnosis code and secondary codes. Institutional-based spasticity clinic data was captured from the two largest spasticity clinics in Alberta, one located in Calgary (the Foothills Medical Centre; visits captured in Millennium Scheduler) and one located in Edmonton (the Glenrose Rehabilitation Hospital; visits captured in VAX). Practitioner Claims include information on physician billing; up to three ICD – Version 9 – Clinical Modification (ICD-9-CM; Alberta specific) diagnostic codes can be listed. PIN contains information on dispensed prescription medications from all community pharmacies. Information on deaths was obtained from Vital Statistics. Records that were duplicates or contained an invalid Personal Health Number were discarded by the data custodians. Variables were checked for missing data and inconsistencies by the researchers; inconsistent data were corrected using data logic or information majority.
Cohort selection
The PSS treatment cohort creation was previously described in detail (21). Briefly, cohort selection was as follows: 1) adults (aged ≥18 years) who experienced a stroke in the community and received acute care between April 1, 2012 and March 31, 2017 (24), 2) had AHCIP coverage ≥2 years before the index stroke, and ≥3 after the index stroke or until death, whichever occurred earlier, 3) initiated spasticity treatment after the stroke (up to March 31, 2019), defined as the first community pharmacy dispensation of an anti-spasticity medication (baclofen [oral or intrathecal], tizanidine, or dantrolene), first focal botulinum toxin injection (inpatient or community), or first of ≥2 spasticity clinic visits after the stroke event, with none of these treatments occurring during the 2 years before the stroke (Supplementary Table 1). Treatment provided at spasticity clinic visits could include, but not be limited to, patient education, prescriptions for oral anti-spasticity medications and intrathecal baclofen pumps, focal injections with botulinum toxin, prescribed exercises by physical and/or occupational therapy (stretching, strengthening and neuromuscular electrical stimulation), and/or prescribed orthoses. Among those who experienced a subsequent stroke, the index stroke date was reassigned to the closest stroke that occurred before initiation of PSS treatment.
Study measures
Baseline characteristics determined on the index stroke date included age, sex and stroke type. Relative to the index stroke event, those who experienced a previous stroke as far back as April 1, 2002, and those who experienced a subsequent stroke up to March 31, 2020 were reported.
The type of initial PSS treatment was reported overall, and according to defined time points after stroke (e.g., <3 months, 3–6 months, 6–12 months and >12 months) (25); those who received ≥2 initial PSS treatments (occurred on the same day) was reported. The type of physician (i.e., primary care physician, physiatrist, spasticity clinic [physiatrist/nurse], neurologist and other) that prescribed/provided the initial PSS treatment was also reported. After PSS treatment initiation, annual spasticity treatment was reported overall and according to the initial PSS treatment; all instances of ≥1 treatment with oral anti-spasticity medication, focal botulinum toxin injection, spasticity clinic visit, intrathecal baclofen and surgical intervention during a given year were measured (up to March 31, 2020, when AHCIP coverage ended, or death, whichever occurred earlier). Types of PSS treatment received were also measured at any time after the stroke up to March 31, 2020 (had ≥1 spasticity treatment type – as an initial treatment or started thereafter), time (number of days) from the stroke event until the start of the treatment type, and the prescribing physician type were reported; the annual number of injections was determined for focal botulinum toxin.
Among those who received oral baclofen and had ≥1 year follow-up thereafter, the first dose (mg/day), along with the last dose received within 1 year after starting this treatment was reported; among those who received a high dose (>60 mg/day (26)) within 1 year, time (number of days) from starting oral baclofen until the beginning of high-dose use and the prescribing physician type were reported.
Considering that dispensations for baclofen, tizanidine and dantrolene could only be determined in the community setting, the number of individuals who initiated these drugs ≤7 days after discharge from the inpatient setting related to the stroke event was assumed to estimate the number of individuals who initiated this type of treatment within the inpatient setting.
Statistical analysis
Descriptive statistics were reported as counts and percentages, means and standard deviations (SD), or medians and interquartile ranges (IQR), where appropriate. Analyses were performed using Statistical Analysis System (SAS) 9.4 software (SAS Institute Inc., Cary, North Carolina, USA). In accordance with data custodian privacy standards, outcomes with one to nine individuals were reported as <10, and associated results censored (e.g., presented as a range) so that the number of individuals (e.g., one to nine) could not be calculated.
Results
Subject selection
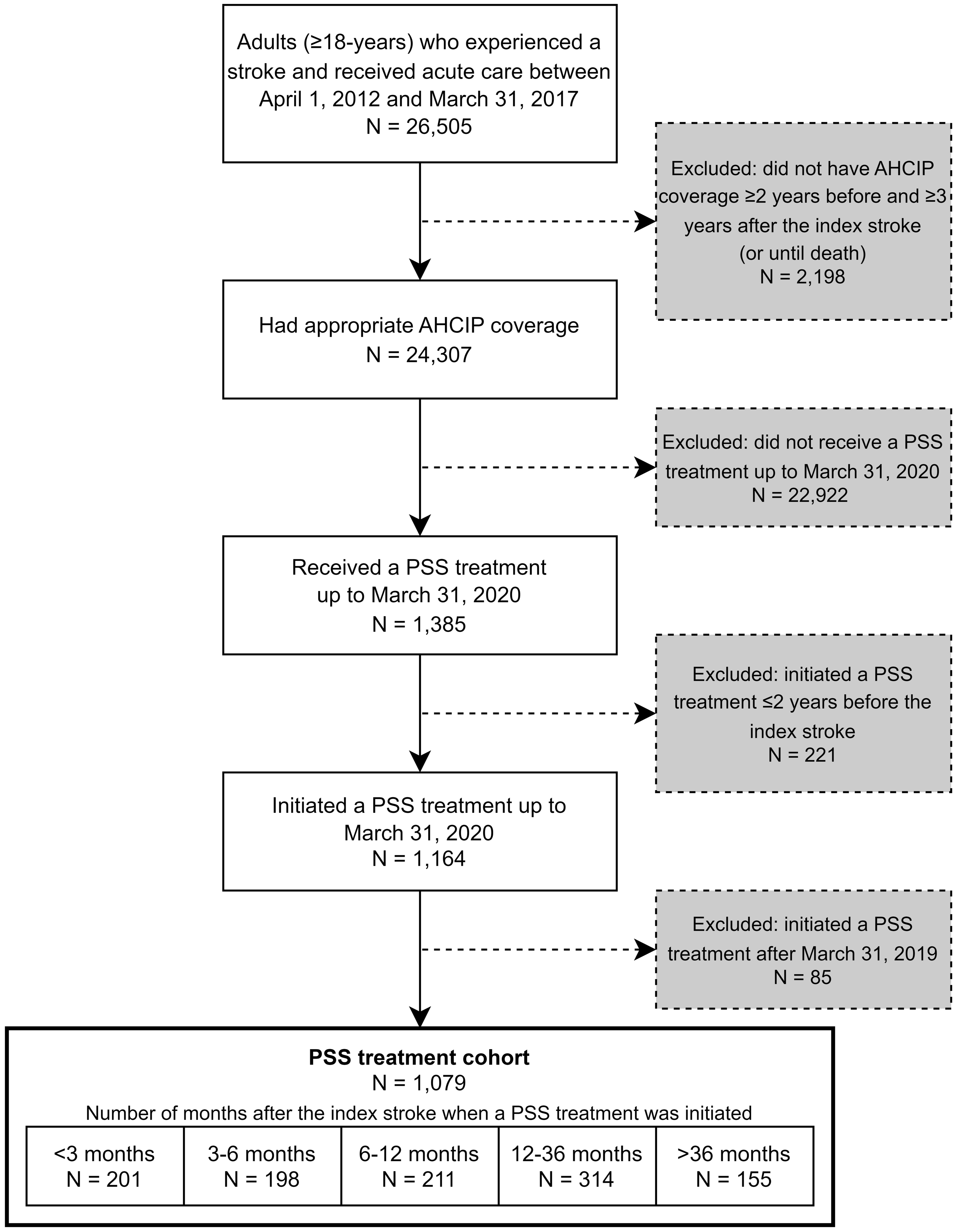
Of 26,505 adults who had a stroke during the inclusion period, 1,079 were included in the PSS treatment cohort (Figure 1; see Supplementary Figure 2 for data linkage) (21).
Cohort selection flow diagram. Abbreviations: AHCIP = Alberta Health Care Insurance Plan; PSS = post-stroke spasticity.
Characteristics
Characteristics of this study cohort have been previously reported in detail (21). Briefly, on the date of the index stroke (ischemic stroke: 81.1% [n = 875]; hemorrhagic stroke: 18.9% [n = 204]), the mean age was 61 (SD 15) years, and 52.1% (n = 562) were male (21). A total of 13.6% (n = 147) experienced a previous stroke and 4.5% (n = 49) had a subsequent stroke that occurred a median of 892 (IQR: 1,091) days after the index stroke event; <10 individuals experienced ≥2 subsequent strokes (21).
Post-stroke spasticity treatment initiation
Within the cohort, the most common initial PSS treatment was an oral anti-spasticity medication (62.3%) (Table 1). Baclofen was most common in 60.9% of the total cohort and accounted for 97.8% of those who initiated an oral anti-spasticity medication; it was most often prescribed by primary care physicians (78.6%). Focal injection with botulinum toxin was initially given to 23.3% of the cohort and largely prescribed by physiatrists (58.6%). A spasticity clinic visit occurred initially in 18.6% (Table 1). Among the defined time points after stroke, those who received an oral anti-spasticity medication as their initial PSS treatment was numerically greater at each time point after stroke (from 49.3% at <3 months post-stroke to 70.2% at >12 months post-stroke). Focal injection with botulinum toxin ranged from 21.7% to 24.4% at the same time points, and those who initially visited a spasticity clinic was numerically lower at each time point after stroke (from 29.9% at <3 months post-stroke to 9.2% at >12 months post-stroke) (Table 1). Less than 10% of individuals initiated oral baclofen (9.7%), tizanidine (n <10) and dantrolene (n <10) ≤7 days after discharge from an inpatient setting after their stroke.
Initial PSS treatment
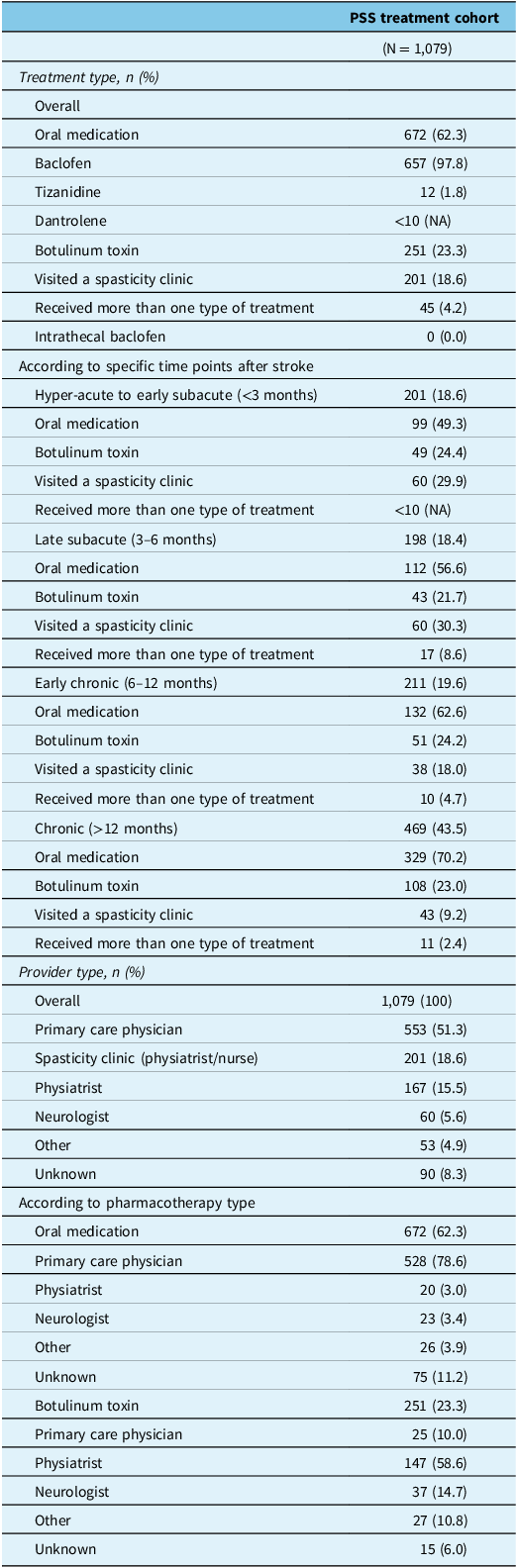
Abbreviations: NA = not applicable; PSS = post-stroke spasticity.
Post-stroke spasticity treatment after initiation
After initiating PSS treatment, the proportion of those who received ≥1 spasticity treatment of any kind decreased annually (second year 45.3%; third year 41.8%; fourth year 38.9%; fifth year 35.4%); oral anti-spasticity medications, focal botulinum toxin injections and spasticity clinic visits followed this pattern to varying degrees as shown in Supplementary Table 2. Among those who initiated PSS pharmacotherapy, 37.5% (initiated an oral anti-spasticity medication) and 53.3% (initiated focal botulinum toxin injection) had ≥1 PSS treatment in their second year after initiation; those who visited a spasticity clinic as their initial treatment had 64.6% received ≥1 PSS treatment in their second year. The majority of those who initially visited a spasticity clinic also received ≥1 focal botulinum toxin injection annually thereafter (Supplementary Table 2). After initiating PSS treatment, <10 individuals per year subsequently received surgical intervention for spasticity (Supplementary Table 2).
Post-stroke spasticity treatments received
Among the total cohort, anti-spasticity treatment types that were started at any time after the stroke were oral baclofen (n = 744; 69.0%), focal botulinum toxin injection (n = 407; 37.7%), a spasticity clinic visit (n = 257; 23.8%) and oral tizanidine (n = 34; 3.2%); 16 individuals received surgical intervention, 11 received oral dantrolene and none received intrathecal baclofen (Table 2). Among those who received oral baclofen, this drug was started a median of 348 (IQR 741) days (11.4 months) after the stroke, and it was primarily prescribed by primary care physicians (77.6%) (Table 2). Among those that received focal botulinum toxin, the first injection occurred a median of 311 (IQR 446) days (10.2 months) after the stroke, and it was primarily prescribed by physiatrists (72.2%); the annual median number of injections that individuals received were 3.9 (IQR 1.8) (Table 2). Among those that received oral tizanidine, this drug was started a median of 342 (IQR 563) days (11.2 months) after the stroke, and it was primarily prescribed by primary care physicians (52.9%) (Table 2).
Post-stroke spasticity pharmacotherapies received (at any time after the stroke – as an initial PSS treatment or thereafter up to March 31, 2020)
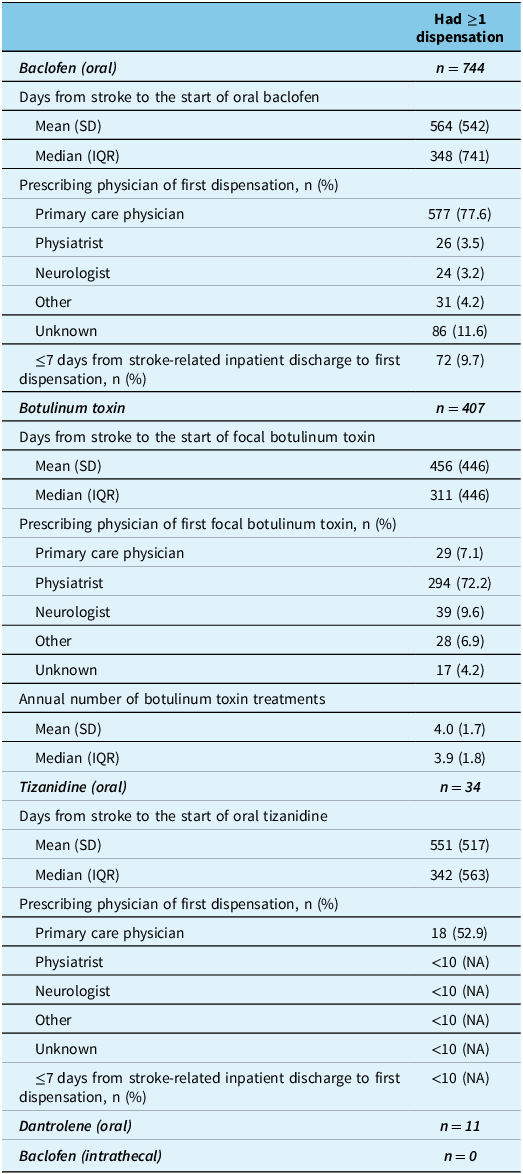
Abbreviations: IQR = interquartile range; NA = not applicable; PSS = post-stroke spasticity; SD = standard deviation.
Treating dose of oral baclofen
Among those who received oral baclofen (as an initial PSS treatment or thereafter) and had ≥1 year of follow-up (n = 677), 67.5% received a starting dose of ≤20 mg/day, 30.6% received >20 to ≤60 mg/day and 1.9% received >60 mg/day. The last dose received during the 1 year period after starting oral baclofen was the starting dose in the majority of cases (86.5% to 90.4%) (Table 3). A total of 21 individuals received ≥1 dispensation for a dose >60 mg/day within 1 year after starting oral baclofen, which was prescribed by primary care physicians (there were no identifiable prescriptions by physiatrists, neurologists or other types). This dose (>60 mg/day) was received a mean of 58 (SD 103) days and a median of 0 (IQR 76) days after starting oral baclofen; 13 received this as their starting dose within the community (Table 3).
Oral baclofen use during the 1 year period after starting this medication
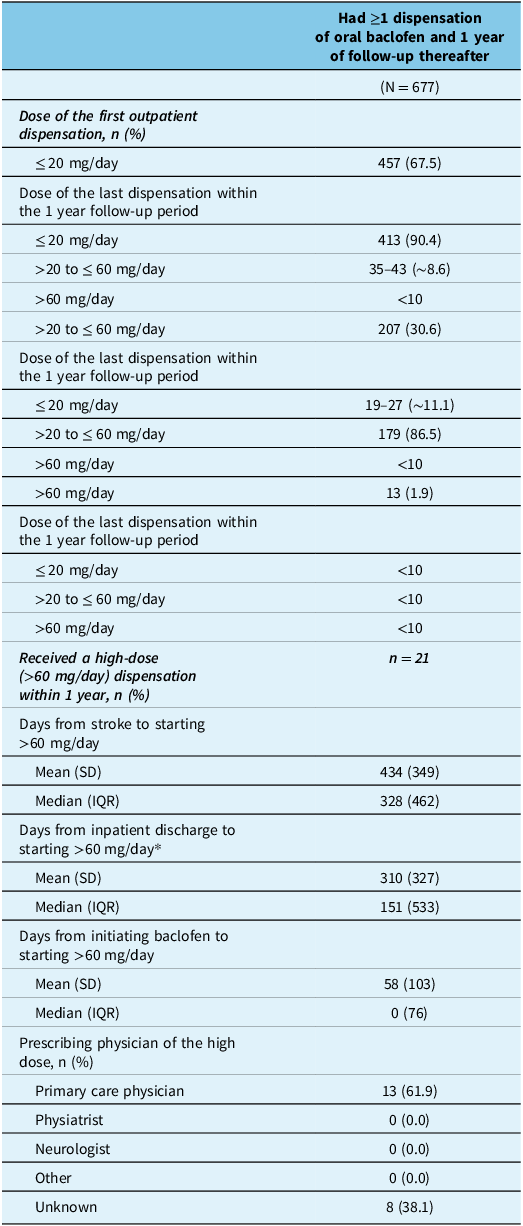
* Inpatient discharge was determined from the date an individual was discharged from hospital; as <10 were discharged from the emergency department, this calculation is reported for 12–20 individuals. Abbreviations: IQR = interquartile range; SD = standard deviation.
Discussion
In this retrospective population-based cohort study of 1,079 adults in Alberta, Canada, who received PSS treatment, the most common pharmacotherapies were oral baclofen (received as an initial PSS treatment: 60.9%; received any time after stroke: 69.0%) that was primarily prescribed by primary care physicians and focal botulinum toxin injection (received as an initial PSS treatment: 23.3%; received any time after stroke: 37.7%) that was primarily prescribed by physiatrists. A total of 23.8% were seen at a spasticity clinic (18.6% as an initial PSS treatment) where care included rehabilitation therapies from the interdisciplinary team, as well as pharmacotherapies that were primarily focal botulinum toxin injection. It is possible that these were complex cases of spasticity, as the Canadian Stroke Best Practice Recommendations strongly advise referral to a specialist in these situations (8). Results from this study identify areas of concordance along with gaps in the provision of guideline recommended PSS care (8), including overuse of oral baclofen and possible underuse of focal injections with botulinum toxin. These findings merit further investigation and development of strategies to improve alignment of PSS treatment with guideline recommendations that in turn will support better PSS care. Also, considering that the annual proportion of those who received ≥1 treatment for spasticity (any kind) decreased to 45.3% in the second year after initiating PSS treatment, an understanding of the underlying reasons for this decrease is warranted.
Oral medications are the most commonly used pharmacotherapies to treat spasticity, among which oral baclofen is used most frequently (9–11). Baclofen, a gamma aminobutyric acid (GABA)-b agonist, has a limited ability to cross the blood–brain barrier because it is mainly water-soluble (27, 28). Consequently, many individuals with spasticity as a result of cerebral damage, such as stroke, appear to need higher doses to treat spasticity, which may cause dose-dependent adverse side effects (3). In a double-blind, cross-over trial comparing baclofen with placebo in individuals with PSS, 50% (oral baclofen; average dose was 30 mg/day) versus 15% (placebo) reported adverse events (13). The Canadian Stroke Best Practice Recommendations indicate that oral anti-spasticity medications, specifically baclofen and tizanidine, can be considered for the treatment of more generalized disabling spasticity after a stroke, but caution that benefits appear to be marginal and the side effects of fatigue and drowsiness are common (8). Because of these limitations and lack of high-quality evidence of effectiveness, the use of these drugs for the treatment of PSS has been suggested to be limited (3). As over two-thirds of individuals received oral baclofen in this study, and 21 individuals received a dose above the advised therapeutic range (received >60 mg/day; advised dose range is 15–60 mg/day (26)), this represents a gap in optimal PSS management.
Botulinum toxin injection is the standard of care for focal and multifocal disabling spasticity to support passive range of motion, pain and potentially active function (29–33); repeat injections once every 3 to 4 months is recommended (34, 35). The Canadian Stroke Best Practice Recommendations suggest injections with botulinum toxin for the pharmacological treatment of focal symptomatically distressing spasticity after stroke (8). Findings from this study indicate areas of concordance with recommendations along with potential areas for improvement; while individuals treated with focal botulinum toxin received injections every 4 months, it is possible that this treatment was underutilized, as only 37.7% of individuals received botulinum toxin injections.
In follow-up to findings from our previous study that supports strategies to improve earlier identification and initiation of PSS treatment (21), results from this study show that there is also an opportunity to improve PSS treatment type. Potential reasons for the prevalent use of oral baclofen and limited use of focal injections with botulinum toxin may include limited awareness of clinical practice guidelines, a lack of referral or access to specialists that perform botulinum toxin injections for the treatment of spasticity, and/or drug cost (8, 36). Results from a survey of primary care physicians across Canada found that the vast majority (87%) felt their knowledge of beneficial evidence-based treatments for the management of spasticity was deficient (37). Additionally, wait times for access to spasticity clinics and/or community physiatry clinics, where most focal botulinum toxin injections are performed, can vary greatly based on geographical location, available physician expertise and rehabilitation health human resource (38, 39). These challenges have also been identified by expert consensus panels in the United Kingdom and Italy as high-priority barriers within the community setting (lack of awareness by community healthcare providers of available treatments, and limited access to specialized spasticity services and expertise in the community), along with lack of patient education (40, 41). These experts proposed a number of potential solutions to overcome these barriers including creating greater opportunities and improving the utilization of existing resources for practical education and training initiatives for clinicians and allied healthcare professionals, enabling a framework/process for specialized spasticity physicians to visit individuals living with PSS in the community, particularly those who may be less likely to receive a referral for specialist treatment such as those in long-term care facilities who have cognitive difficulties, and encouraging the empowerment of patients and caregivers by providing an educational path for spasticity, optimal treatments and rehabilitation that allows them to participate actively in the management of their condition (40, 41). The drug cost of botulinum toxin may have been a barrier for some in this study – specifically, those who were not covered under a private drug insurance program or an Alberta Health premium-based or premium-free plan.
This study has several important strengths, including the large size and population-based design. However, this study is also subject to limitations that should be taken into consideration when interpreting results. Retrospective administrative claims-based studies use administrative data as opposed to medical records, therefore creating the potential for misclassification of study cohorts or outcomes. To address this limitation, a case definition established by the Canadian Stroke Best Practices, Stroke Quality Advisory Committee was used to identify stroke cases in this study (24). Inpatient rehabilitation specifically for spasticity and non-publicly funded community-based rehabilitation was not captured within provincial administrative data and therefore not included; as a result, the number of individuals who received non-pharmacological PSS treatment may be greater than included in this study. Although only community pharmacy dispensations for baclofen, tizanidine and dantrolene could be determined at the time of this study, <10% received their first dispensation for one of these drugs ≤7 days after inpatient discharge; therefore, the vast majority of these individuals likely started these pharmacotherapies in the community setting. PIN only provides information on prescription medication dispensations from community pharmacies and therefore may not represent actual medication uptake by individuals; indication is also not provided, so off-label use for conditions other than spasticity may have occurred.
Conclusions
To our knowledge, this is the first population-based cohort study describing PSS treatment in everyday clinical practice within Canada. Findings indicate areas of concordance with recommendations for PSS treatment (individuals treated with focal botulinum toxin received injections every 4 months) along with gaps in provision of guideline concordant PSS care including the overuse of oral baclofen and possible underuse of focal injections with botulinum toxin. Further investigation into the barriers to optimal PSS treatment is warranted, along with pursuing strategies and interventions to improve PSS care.
Data availability
The datasets analyzed during the current study are not publicly available because the data custodians, Alberta Health Services and Alberta Health do not allow users of the data to publish the data. Please contact the corresponding author for requests related to the data used in this study.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2024.342.
Acknowledgments
We thank the participants of this study. This study is based in part on anonymized raw data from Alberta Health and Alberta Health Services that was provided by the Alberta Strategy for Patient Oriented Research Unit housed within Alberta Health Services. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta or Alberta Health Services. Neither the Government of Alberta/Alberta Health nor Alberta Health Services express any opinion in relation to this study. SK was supported by the Kidney Health Research Chair and the Division of Nephrology at the University of Alberta.
Author contribution
LS, HL, KM, KV and SK contributed to the study concept and design; HL, KV and PUN conducted the analyses; KM prepared the initial manuscript. All authors contributed to the interpretation of the data and critical revision of the manuscript for important intellectual content as well as approved the final version to be published and agreed to be accountable for all aspects of the work ensuring that questions related to the accuracy of integrity of any part of the work are appropriately investigated and resolved. SK provided study supervision.
Funding Statement
Funding for the study was provided by Allergan Inc. to LR. The funder had no role in the study design, analysis, interpretation of the data, drafting of the manuscript or in the decision to submit for publication. The funders had the right to comment on the protocol and the manuscript prior to submission, but final decisions remained with LR and SK.
Competing interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: HL, KM, KV, PUN, LR, TW and SK are members of the Alberta Real World Evidence Consortium (ARWEC) and the Alberta Drug and Therapeutic Evaluation Consortium (ADTEC); these entities (at the University of Alberta, University of Calgary and Institutes of Health Economics) conduct research including investigator-initiated industry-funded studies (ARWEC) and government-funded studies (ADTEC). Payment received for consultancy, participation on an advisory board and/or honoraria were reported for AbbVie (LS, SD and JY), Ipsen (LS and SD) and Merz (LS, SD and JY) outside of the submitted work within the past 3 years. Allergan (now an AbbVie company) is a manufacturer of a botulinum toxin product and provided the funding for this study to LR (see funding statement for details). No other conflict of interest was declared. All authors of this study had complete autonomy over the content and submission of the manuscript, as well as the design and execution of the study.







 Open access
Open access