

Depression and anxiety are the most common psychological disorders with an increase in recent years(Reference Goodwin, Dierker and Wu1). The global prevalence of depression and anxiety has been reported to be 4·7 % and 7·3 %, respectively(Reference Baxter, Vos and Scott2,Reference Ferrari, Somerville and Baxter3) . In Iran, according to the national reports, about 21 % and 20·8 % of adult population are affected by depressive and anxiety symptoms, respectively(Reference Noorbala, Yazdi and Yasamy4). These mental disorders have been shown to increase the risk of several chronic diseases, including diabetes mellitus, CVD and cancers(Reference Bobo, Grossardt and Virani5). Moreover, they may decrease the quality of life and impose a significant economic burden on both individuals and society(Reference Chodavadia, Teo and Poremski6).
Previous evidence has indicated an association between the dietary intakes of micronutrients, macronutrients and individual foods and depression and anxiety(Reference Wang, Liu and Compher7,Reference Aucoin, LaChance and Naidoo8) . To identify diet–disease relations, nutritional epidemiologists recommend analysing overall diets rather than focusing on single nutrients or foods(Reference Hu9). To date, several dietary patterns have been examined in relation to depression and anxiety. Among these, the Dietary Approaches to Stop Hypertension (DASH) eating plan, originally developed for hypertension prevention, has received attention, partly due to its emphasis on nutrient-rich foods and biological pathways, including oxidative stress and inflammation, that overlap with those implicated in mental disorders(Reference Mijailović, Milojević-Rakić and Mihajlović10–Reference Tan, Wang and Tomiyama13). This dietary pattern comprises a diet high in vegetables, fruit, low-fat dairy products, nuts and legumes, and whole grains and low in Na, red and processed meats, and sugar-sweetened beverages (SSB) and sweets(Reference Fung, Chiuve and McCullough14), which provides good quantities of K, Ca, Mg and fibre and limited amounts of total fat, saturated fat and cholesterol. Several studies have shown that individual components of the DASH diet are significantly associated with mental health outcomes. Increased intake of fruits, vegetables and whole grains, key elements of the DASH diet, has been linked to lower levels of depression and anxiety(Reference Gibson-Smith, Bot and Brouwer15), likely due to their antioxidant, anti-inflammatory and neuroprotective properties(Reference Wu, Li and Zhou16). In contrast, higher consumption of red and processed meats, SSB and sweets, foods discouraged in the DASH diet, has been associated with greater depressive and anxiety symptoms, possibly through mechanisms such as inflammation and gut dysbiosis(Reference Nucci, Fatigoni and Amerio17–Reference Gomes, Silva and Marçal19). Therefore, assessing the overall DASH dietary pattern allows for a comprehensive understanding of how a balanced and health-promoting diet may influence mental well-being more effectively than examining individual dietary components in isolation. Moreover, previous studies have shown that anxiety and depression similar to hypertension are associated with hypothalamic–pituitary–adrenal axis hyperactivation and overproduction of catecholamine(Reference Johnson20,Reference Hamer and Steptoe21) . It has been reported that Mg may help reduce catecholamine secretion from the adrenal gland(Reference Joris, Plat and Bakker22). Furthermore, endothelial dysfunction, a shared risk factor for hypertension, anxiety and depression(Reference Yannoutsos, Levy and Safar23), may improve with adherence to the DASH diet(Reference Rifai, Hayden and Pisano24). These connections suggest that the DASH diet could potentially alleviate symptoms of depression and anxiety.
A review of the literature shows inconsistent findings regarding the DASH diet’s relationship with depression and anxiety(Reference Tan, Wang and Tomiyama13). Investigating this relationship is particularly important in Middle Eastern countries due to the high prevalence of depressive and anxiety symptoms in the region and its distinct dietary practices. In Iran, some research found no significant associations between greater adherence to the DASH diet and depression and anxiety in adult populations(Reference Valipour, Esmaillzadeh and Azadbakht25,Reference Saharkhiz, Khorasanchi and Karbasi26) , and others reported potential benefits for specific groups like adolescents(Reference Khayyatzadeh, Mehramiz and Mirmousavi27) and university students(Reference Faghih, Babajafari and Mirzaei28). Notably, the clinical trial by Daneshzad et al., which had a different study design, focused exclusively on women with type 2 diabetes, thereby limiting both the comparability with observational studies and the generalisability of its findings(Reference Daneshzad, Heshmati and Basirat29). The current study, which includes a larger and more diverse sample of adults aged 35–65 years, aims to fill gaps in existing research and enhance understanding of the DASH diet’s potential mental health benefits. Therefore, the present study aimed to investigate the association between adherence to the DASH diet and the risk of depression and anxiety severity in a large group of Iranian adults.
Methods
Study population
The current cross-sectional study was conducted within the framework of the Mashhad Stroke and Heart Atherosclerotic Disorder (MASHAD) study, a prospective cohort study to evaluate 10-year cardiovascular risk among the population of the study. Detailed information about the protocol of the study described previously(Reference Ghayour-Mobarhan, Moohebati and Esmaily30). Briefly, in the initial (cross-sectional) phase of the MASHAD study, 9704 individuals aged 35–65 years were recruited from the urban population of Mashhad, Iran, between 2010 and 2011. Participants were selected using a stratified cluster random sampling method across three major regions of the city, each divided into nine clusters based on local healthcare service areas. In the current analysis, participants were selected from a total of 9704 individuals enrolled in the MASHAD study. Among them, 6696 participants had complete dietary data. From this subset, nine individuals were excluded due to missing data on depression, and seven were excluded due to missing data on anxiety. Notably, six individuals had missing data for both depression and anxiety. Additionally, approximately 150 participants were excluded because their reported daily energy intake was implausible (< 800 or > 4200 kcal/d). After applying these inclusion and exclusion criteria, 6537 participants remained for the analysis related to depression, and 6539 participants were included in the analysis related to anxiety. The study was described to all participants, and written informed consent was obtained from all subjects. The study was conducted in accordance with the Declaration of Helsinki, and its protocol was reviewed and approved by an institutional ethics committee.
Depression and anxiety assessment
All participants completed depression and anxiety questionnaires on recruitment to the study. Beck Anxiety Inventory (BAI) which is a self-reported measure of anxiety, was used to evaluate the severity of anxiety. Scoring intervals are described as follows: minimal anxiety level (0–7), mild anxiety level (8–15), moderate anxiety level (16–25) and severe anxiety level (26–63). Beck Depression Inventory II (BDI-II) which is a self-reported measure of depression was used to assess depression among subjects, and scoring intervals are described as follows: minimal depression (0–13), mild depression (14–19), moderate depression (20–28) and severe depression (29–63)(Reference Dozois, Dobson and Ahnberg31,Reference Ulusoy, Sahin and Erkmen32) . These questionnaires were previously validated for use in the Iranian population(Reference Ghassemzadeh, Mojtabai and Karamghadiri33,Reference Kaviani and Mousavi34) .
Dietary intake and Dietary Approaches to Stop Hypertension diet assessment
Dietary intake was evaluated by nutritionists using a semi-quantitative FFQ prior to the study. Semi-quantitative FFQ includes sixty-five food items, and each food item has five frequency groups for consumption. This questionnaire had been previously validated among Iranian population(Reference Ahmadnezhad, Asadi and Miri35). For the assessment of micro- and macronutrient intakes, we employed the Diet Plan 6 software (Forestfield Software Ltd.), which had been adapted to include traditional Iranian dishes by integrating data from the Iranian food composition tables(Reference Azar and Sarkisian36). DASH diet was determined using DASH dietary scores based on FFQ and the nutrients that are emphasised or minimised in the DASH diet(Reference Fung, Chiuve and McCullough14). This dietary pattern emphasises on eight food components including high intake of fruits, vegetables, nuts and legumes, low-fat dairy products, and whole grains and low intake of SSB and sweets, Na, and red and processed meats. We computed the energy-adjusted intakes of the above-mentioned nutrients and foods using residual method(Reference Willett, Howe and Kushi37). Then, participants were classified into deciles based on their energy-adjusted intakes of nutrients and foods. Participants received the score of 10 if they were at the highest decile of fruits, vegetables, whole grains, low-fat dairy products, nuts and legumes and lowest decile of red and processed meat, SSB and sweets, and Na. They received 1 if they were at the highest decile of red and processed meat, SSB and sweets, and Na and lowest decile of fruits, vegetables, whole grains, low-fat dairy products, nuts and legumes. The overall DASH diet score was calculated by summing up scores of eight components and ranged from 8 to 80.
Baseline characteristic assessment
General characteristics including age, gender, occupation, marital status, medical history, smoking, height, weight and physical activity level were assessed by two professional healthcare providers and a certified nurse via interview and examination as previously described(Reference Ghayour-Mobarhan, Moohebati and Esmaily30). Physical activity was assessed using a structured questionnaire derived from the Scottish Heart Health Study/MONICA questionnaire(Reference Bolton-Smith, Woodward and Tunstall-Pedoe38) and based on the James and Schofield equations for human energy requirements(Reference James and Schofield39). The questionnaire included questions about activity during work, leisure time and time spent in bed. Total energy expenditure was calculated by applying the integrated energy index values to each activity domain. BMR was computed using the standard FAO/WHO/UNU equations(Reference Joint40), and physical activity level was subsequently derived as the ratio of total energy expenditure to BMR, expressed as a dimensionless value. BMI was calculated as weight in kilograms divided by height in metres squared.
Statistical analysis
In the present study, subjects were categorised according to deciles of DASH diet score. General characteristics of study participants across tertiles of DASH diet score were compared using one-way ANOVA for continuous variables and Chi-square test for categorical variables. Comparison of age-, sex- and energy-adjusted dietary intakes of participants across tertiles of DASH diet score was performed using ANCOVA. To account for the potential inflation of type I error due to multiple testing, the Bonferroni correction was applied. Adjusted P-values were calculated by dividing the significance threshold (α = 0·05) by the number of comparisons performed. Statistical significance was interpreted based on these corrected thresholds. Ordinal logistic regression, in three different levels of adjustments, was applied to examine the association between DASH diet score and depression and anxiety severity. This method was selected because depression and anxiety severity were categorised into ordered levels (minimal, mild, moderate and severe), allowing the analysis to appropriately account for the ordinal nature of the outcome and preserve the rank information between categories. In the first model, adjustments were made for age (continuous) and energy intake (kcal/day) in all analyses. Additionally, for analyses conducted on the total population, sex was also included as a covariate. Further adjustments were made for marital status (married/single/divorced), educational level (university graduated/non-university education), job status (student/employee/unemployed/retired), smoking status (smoker/non-smoker), physical activity (continuous) and presence of chronic diseases (including dyslipidaemia, hypertension, diabetes and osteoporosis) (yes/no) for men. In the case of women, in addition to the factors mentioned in the second model for men, we also controlled for current pregnancy and lactation (yes/no). In the final model, we controlled for BMI (continuous) to find the obesity-independent association. In addition, to assess the robustness of our results, we performed sensitivity analyses by repeating the main models after excluding pregnant and lactating women. In all statistical analyses, the lowest tertile of the DASH diet score was considered as the reference category. To compute the overall trend of OR across tertiles of DASH diet score, we considered these tertiles as an ordinal variable. All analyses were conducted using SPSS software (version 20; SPSS Inc). P-values < 0·05 were considered statistically significant.
Results
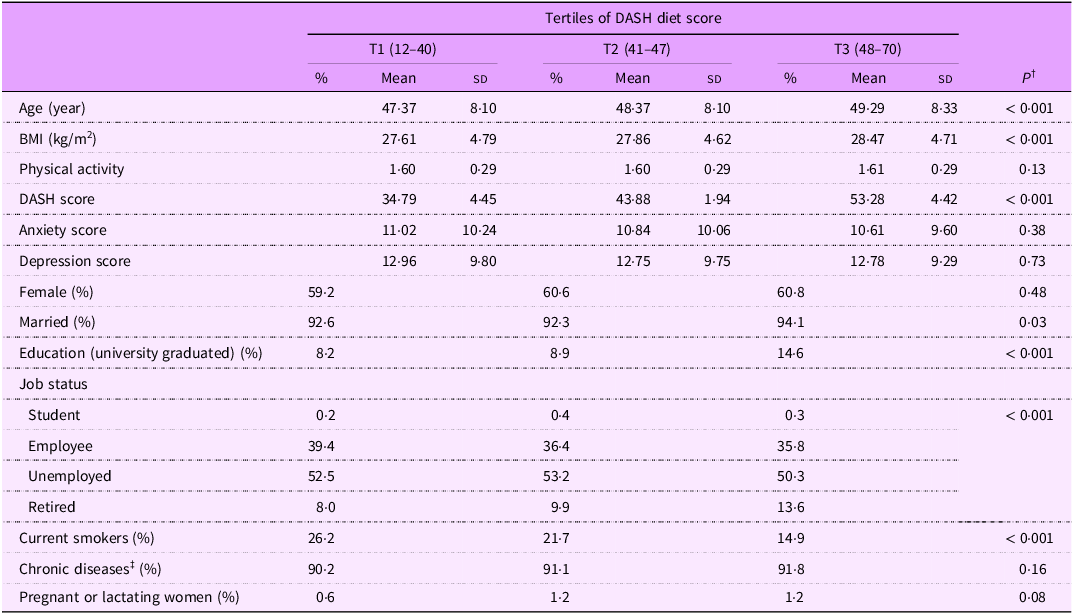
Among participants with depression (n 6537) and anxiety (n 6539), the distribution of symptom severity was as follows: for depression, 59·8 % reported minimal, 18·6 % mild, 14·3 % moderate and 7·3 % severe levels, whereas for anxiety, 47·3 % experienced minimal, 27·4 % mild, 15·3 % moderate and 9·9 % severe symptoms. General characteristics of participants across tertiles of DASH diet score are presented in Table 1. Individuals in the highest tertile of DASH diet score were older, had higher BMI, were more likely to be married and university-graduated and were less likely to be current smokers and unemployed than those in the lowest tertile. No significant differences were found across tertiles of DASH diet score in terms of other general characteristics. DASH score ranges for each tertile were as follows: T1: 12–40, T2: 41–47 and T3: 48–70. The corresponding mean (sd) of DASH scores in each tertile was T1: 34·79 (sd 4·45), T2: 43·88 (sd 1·94) and T3: 53·28 (sd 4·42).
Characteristics of study participants by categories of DASH diet score*

DASH, Dietary Approaches to Stop Hypertension.
*All values are mean (sd), unless indicated.
† ANOVA for continuous variables and Chi-square test for categorical variables.
‡ Chronic diseases included dyslipidaemia, hypertension, diabetes and osteoporosis.
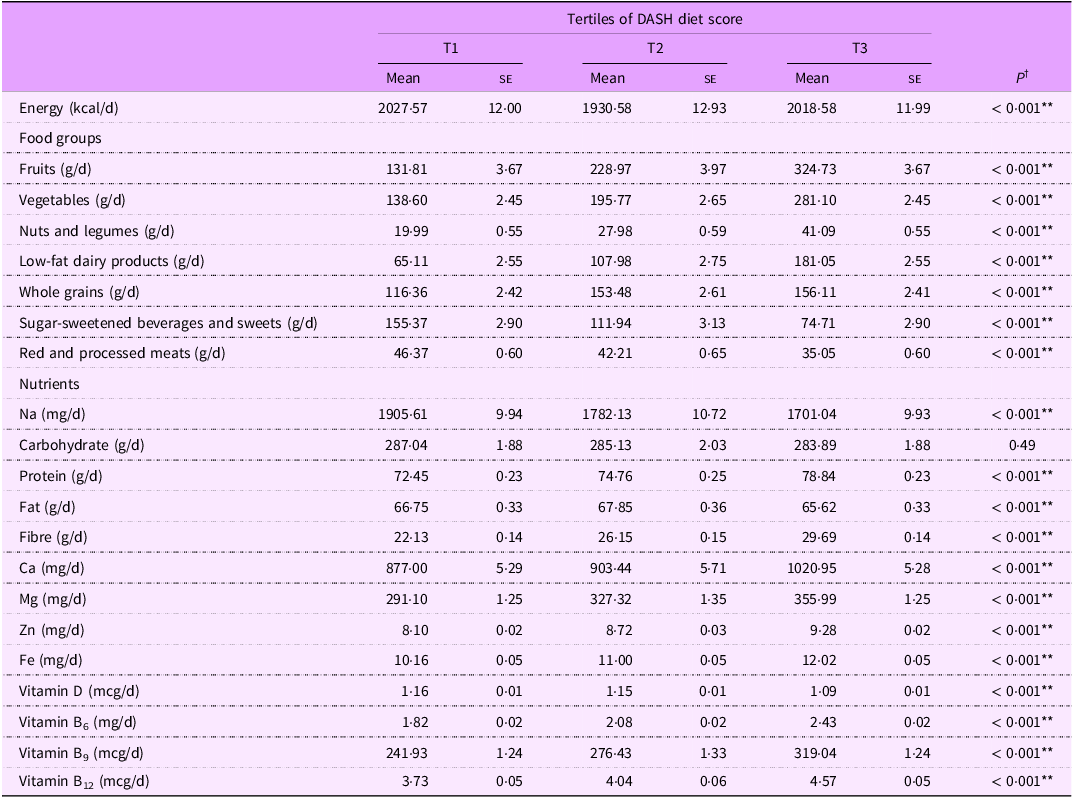
Table 2 summarises food groups and nutrients intakes of study participants. Among the twenty-one dietary variables analysed using ANCOVA, twenty showed statistically significant differences across tertiles of DASH diet score after Bonferroni correction (adjusted significance threshold: P < 0·0024). Only carbohydrate intake did not differ significantly between groups (P = 0·49) so that individuals in the top tertile of DASH diet score had higher intakes of fruits, vegetables, nuts and legumes, low-fat dairy products, whole grains, protein, fibre, Ca, Mg, Zn, Fe, vitamin B6, vitamin B9 and vitamin B12 and lower intakes of energy, SSB and sweets, red and processed meats, Na, fat and vitamin D compared with those in the bottom tertile.
Dietary intakes of study participants by tertile categories of DASH diet score*

DASH, Dietary Approaches to Stop Hypertension.
*All values are mean (se); energy intake is adjusted for age and sex, all other values are adjusted for age, sex and energy intake.
† ANCOVA for all variables.
** P < 0·0024 after Bonferroni correction.
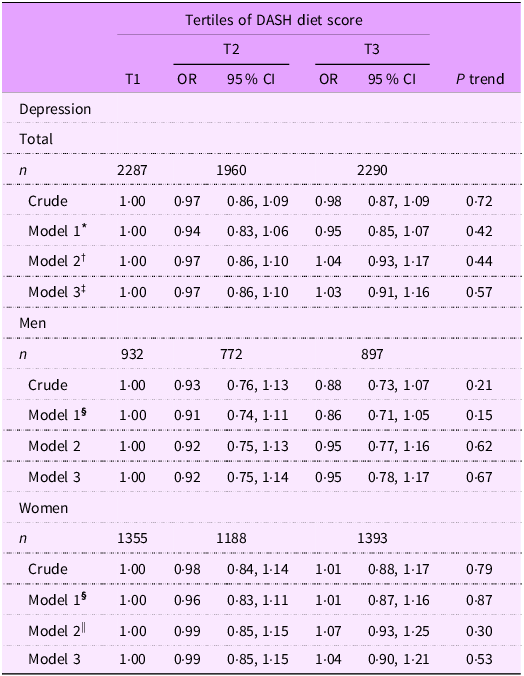
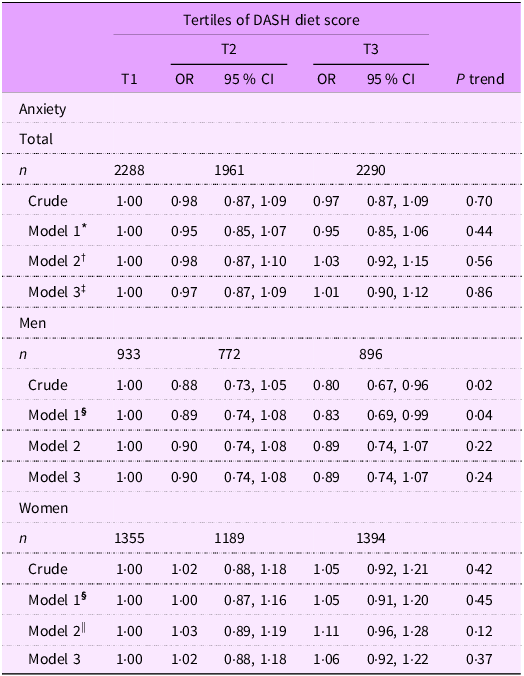
Total and gender-stratified crude and multivariable-adjusted OR (95 % CI) for depression and anxiety severity across tertile categories of DASH diet score are illustrated in Tables 3 and 4, respectively. In the crude model, we found no statistically significant association between adherence to the DASH diet and the severity of depression in the total population (OR: 0·98; 95 % CI: 0·87, 1·09), as well as in sex-stratified analyses for both men and women (men: OR: 0·88; 95 % CI: 0·73, 1·07; women: OR: 1·01; 95 % CI: 0·88, 1·17). These non-significant associations remained even after controlling for potential confounders (total: OR: 1·03; 95 % CI: 0·91, 1·16; men: OR: 0·95; 95 % CI: 0·78, 1·17; and women: OR: 1·04; 95 % CI: 0·90, 1·21). In terms of anxiety, we found that men in the third tertile of DASH diet score had lower risk of experiencing more severe anxiety compared to those in the first tertile (OR: 0·80; 95 % CI: 0·67, 0·95). This significant association continued after adjustment for age and energy intake (OR: 0·83; 95 % CI: 0·69, 0·99). However, further controlling for marriage status, education, job status, smoking, physical activity, chronic diseases and BMI changed this relationship to non-significant (OR: 0·89; 95 % CI: 0·74, 1·07). In the total population as well as in women, we failed to find any significant association between high adherence to the DASH diet and the severity of anxiety either before (total: OR: 0·97; 95 % CI: 0·87, 1·09; women: OR: 1·05; 95 % CI: 0·92, 1·21) or after controlling for potential confounders (total: OR: 1·01; 95 % CI: 0·90, 1·12; women: OR: 1·06; 95 % CI: 0·92, 1·22).
Multivariable-adjusted OR (95 % CI) for depression across tertile categories of DASH diet score in the total population and stratified by gender

DASH, Dietary Approaches to Stop Hypertension.
* Model 1: Adjusted for age, sex and energy intake.
† Model 2: Further adjusted for marriage status, education, job status, smoking, physical activity and chronic diseases.
‡ Model 3: Further adjusted for BMI.
§ Model 1: Adjusted for age and energy intake.
|| Model 2: Further adjusted for marriage status, education, job status, smoking, physical activity, chronic diseases, current pregnancy and lactating.
Multivariable-adjusted OR (95 % CI) for anxiety severity across tertile categories of DASH diet score in the total population and stratified by gender

DASH, Dietary Approaches to Stop Hypertension.
* Model 1: Adjusted for age, sex and energy intake.
† Model 2: Further adjusted for marriage status, education, job status, smoking, physical activity and chronic diseases.
‡ Model 3: Further adjusted for BMI.
§ Model 1: Adjusted for age and energy intake.
|| Model 2: Further adjusted for marriage status, education, job status, smoking, physical activity, chronic diseases, current pregnancy and lactating.
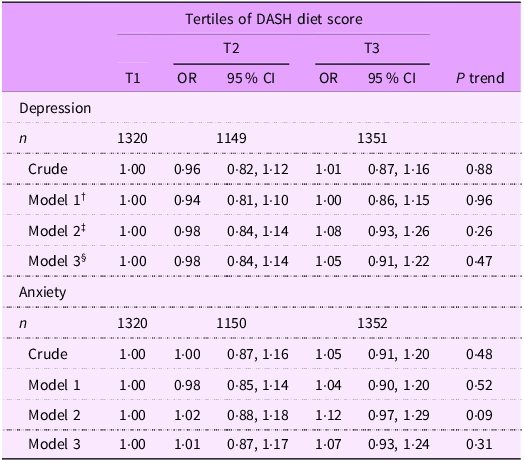
Multivariable-adjusted OR (95 % CI) for depression and anxiety severity across tertiles of DASH diet score among women, excluding pregnant and lactating individuals, are presented in Table 5. After conducting these analyses, no significant associations were found between adherence to the DASH diet and the severity of depression and anxiety, in either the crude model (depression: OR: 1·01; 95 % CI: 0·87, 1·16; anxiety: OR: 1·05; 95 % CI: 0·91, 1·20) or the fully adjusted model (depression: OR: 1·05; 95 % CI: 0·91, 1·22; anxiety: OR: 1·07; 95 % CI: 0·93, 1·24).
Multivariable-adjusted OR (95 % CI) for depression and anxiety severity across tertile categories of DASH diet score among women, excluding pregnant and lactating individuals

DASH, Dietary Approaches to Stop Hypertension.
† Model 1: Adjusted for age and energy intake.
‡ Model 2: Further adjusted for marriage status, education, job status, smoking, physical activity and chronic diseases.
§ Model 3: Further adjusted for BMI.
Discussion
Our findings revealed no significant association between adherence to the DASH diet and odds of depression and anxiety severity, neither in men nor in women. This outcome contributes to the growing body of literature that presents a nuanced understanding of the association between DASH diet and mental health.
Previous research has shown mixed results regarding the association between DASH diet and depression and anxiety. In line with our findings, Saharkhiz et al. in a cross-sectional study among 181 Iranian girls found no significant association between adherence to the DASH diet and risk of depression and anxiety(Reference Saharkhiz, Khorasanchi and Karbasi26). Similarly, Meegan et al. in a cross-sectional study among 2047 Irish adults did not observe any significant association between high dietary quality (greater DASH score) and anxiety, either in men or in women(Reference Meegan, Perry and Phillips41). Non-significant associations between adherence to DASH diet and risk of depression and anxiety were also reported in other observational studies(Reference Valipour, Esmaillzadeh and Azadbakht25,Reference Recchia, Baghdadli and Lassale42) .
Several prior epidemiological studies have showed that either moderate or greater adherence to the DASH diet is protectively related to the risks of depression and anxiety. For instance, Valipour et al. in a cross-sectional study among 3846 general public adults in Isfahan, Iran, reported no significant association between greater adherence to DASH diet and depression or anxiety, both in the overall population and in gender-specific analyses. Nevertheless, their results indicated a significant inverse association between moderate adherence to the DASH diet and depression in women, while no such association was observed in men. Notably, this significant protective association was not seen concerning anxiety in relation to moderate adherence to the DASH diet(Reference Valipour, Esmaillzadeh and Azadbakht25). Another research, conducted prospectively with a cohort of 14 051 Spanish university graduates, revealed that among four DASH diet indices (including Dixon, Mellen, Fung and Günter), higher adherence to the Mellen and Fung indices was not related to the risk of depression. In contrast, the findings showed that moderate adherence to these indices was associated with a reduced risk of depression(Reference Perez-Cornago, Sanchez-Villegas and Bes-Rastrollo43). The opposite results were obtained in Khayyatzadeh et al.’s study among 580 Iranian adolescent girls so that greater, but not moderate, adoption of the DASH diet was inversely associated with the odds of depression(Reference Khayyatzadeh, Mehramiz and Mirmousavi27). Furthermore, findings of another cross-sectional study on 240 university students indicated an inverse association between higher adherence to the DASH diet and depression and anxiety(Reference Faghih, Babajafari and Mirzaei28). It should be kept in mind that the present study focused on an older demographic (with the average age of 48·36 years) compared to previous research that primarily involved younger populations. Additionally, the heterogeneous results might be explained by the different sample size, study designs, underlying confounding factors and various methods for the evaluation of adherence to DASH diet and depression/anxiety.
The effect of DASH diet on mood state has also been investigated in some clinical trials(Reference Daneshzad, Heshmati and Basirat29,Reference Torres and Nowson44) . Torres et al. in a randomised, parallel intervention study among postmenopausal women who generally did not differ from each other in depressive symptoms at baseline showed that a moderate-Na DASH-type diet which included lean red meat on most days resulted in an improvement in mood after 14 weeks(Reference Torres and Nowson44). Another clinical trial was conducted to explore the effect of DASH diet on mental health among sixty-six Iranian women with type 2 diabetes and indicated that a 12-week DASH diet significantly reduced depression and anxiety scores(Reference Daneshzad, Heshmati and Basirat29). Of note, in this trial, the Depression, Anxiety, and Stress Scale-21 (DASS-21) was used to assess mental disorders. The contrasting findings between the present study and the two above-mentioned clinical trials may be attributed to variations in study design, population characteristics and dietary adherence levels. These clinical trials focused on specific subgroups, postmenopausal women and women with type 2 diabetes, who may have unique psychosocial or metabolic factors influencing their mental health outcomes. This underscores the potential variability in the impact of dietary patterns on mood based on individual health profiles and demographic factors.
To the best of our knowledge, there is only one study available that reported a positive association between depression and the Fung DASH score. Cross-sectional findings of the study conducted by Elstgeest et al. on 1312 individuals aged over 55 years indicated that women exhibiting current symptoms of depression had higher DASH scores(Reference Elstgeest, Winkens and Penninx45). The differing findings between our study and that of Elstgeest et al. may be attributed to several factors, including age-related differences and the specific characteristics of the populations studied. While both studies utilised cross-sectional analyses, our broader age range (35–65 years) may have introduced variability in dietary habits and mental health outcomes that obscured any potential associations.
Altogether, as studies in this field are inconsistent, further rigorously designed research is necessary to elucidate these complex associations between DASH diet and mental health.
In the present study, no significant association was observed between adherence to DASH diet and depression and anxiety. Several possible explanations may account for these null findings. First, the use of self-reported measures for both dietary intake and mental health symptoms may have introduced measurement error, potentially attenuating true associations(Reference Satija, Yu and Willett46). Second, reverse causality cannot be ruled out in this cross-sectional design, as individuals with poor mental health may alter their dietary behaviours in unpredictable ways(Reference Satija, Yu and Willett46). Third, residual confounding from unmeasured factors, such as genetic predisposition, chronic stress or sleep disturbances, might have influenced the outcomes independent of dietary quality(Reference Coombes, Landi and Choi47–Reference Fang, Tu and Sheng49). Future longitudinal studies with more accurate dietary assessment methods and larger or more diverse populations are warranted to better elucidate these complex relationships.
After adjustment for the potential confounding variables, we failed to find any significant relationship between DASH diet and depression and anxiety. However, DASH diet might be related to these mental health disorders through various pathways. One possible pathway could be attributed to the high content of fruit and vegetables in this dietary pattern. Recent evidence has shown that polyphenols found commonly in fruit and vegetables might have a beneficial role in anxiety and depressive symptoms probably in part via regulating monoamine neurotransmitters(Reference Mijailović, Milojević-Rakić and Mihajlović10). In addition, given the involvement of oxidative stress and inflammation in the pathogenesis of anxiety and depression symptoms(Reference van Dooren, Schram and Schalkwijk11), another possible mechanism that may underlie the link between DASH diet and these psychological disorders is the beneficial effects of DASH diet on reducing inflammation and oxidative stress levels(Reference Asemi, Samimi and Tabassi12).
The relatively large sample size, use of a valid FFQ for dietary assessment, controlling for several confounders and stratified analysis based on gender could be mentioned as some of the strengths of this study. However, several limitations of our study should be acknowledged. First, the close-ended response nature of FFQ for assessment of dietary intakes as well as psychological questionnaires for assessment of anxiety and depression might result in misclassification of participants. In addition, the use of a short semi-quantitative FFQ, although validated, may have limited sensitivity in capturing absolute dietary intake. Given the large sample size, a concise FFQ was selected to ensure feasibility and participant compliance. While the reproducibility and validity coefficients were within acceptable ranges and comparable to those reported in other regional validation studies(Reference Rezazadeh, Omidvar and Tucker50), we acknowledge the potential for measurement error inherent to recall-based dietary assessments. This limitation may have attenuated observed associations and should be considered when interpreting the findings. Moreover, although we controlled for several confounders, the possible effects of residual confounders cannot be ruled out. Additionally, our study was conducted among Mashhadi adults. Therefore, the extrapolation of our findings to all Iranian people must be done cautiously. Additionally, although the DASH diet addresses several nutrition-related mechanisms relevant to mental health, it does not incorporate certain aspects such as dietary fat quality and overall dietary diversity, which are considered in other dietary indices. Finally, although pregnant and lactating women were included in the analysis to ensure wider generalisability, their unique physiological status could potentially influence dietary patterns and mental health outcomes. However, adjustment for pregnancy and lactation status in the models helped reduce the risk of confounding.
Conclusion
In conclusion, we found no significant association between adherence to DASH diet and depression and anxiety severity in the total participants as well as both genders. As studies in this field are inconsistent, further longitudinal studies with rigorous design and larger or more diverse populations are needed to come to a definite conclusion.
Acknowledgements
The authors wish to thank all subjects who kindly participated in our study.
Financial support
This project was financially supported by the Mashhad University of Medical Sciences, Mashhad, Iran (grant number: 85134).
Competing interests
The authors declare that they have no competing interests.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Ethics Committee of Mashhad University of Medical Sciences, Mashhad, Iran (ethics code: IR.MUMS.REC.1386.250). The study was described to all participants, and written informed consent was obtained from all subjects.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process: During the preparation of this work, the author(s) used ChatGPT, 2025, in order to check grammar. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Authorship
S.S., H.R.R. and M.G-M. contributed to the conception and design of the study, analyses and interpretation of data; M.A., M.M., F.M.S., N.S. and M.G-M. contributed to data collection; S.S., N.S., M.O-K. and N.N. drafted the manuscript; G.A.F. and M.G-M. edited and revised the manuscript. All authors have read and approved the final version of the manuscript for publication. M.G-M. has primary responsibility for final content.

 Open access
Open access