


Highlights
-
• Patients treated with IVT at PSCs may achieve outcomes comparable to those treated at CSCs.
-
• Patients treated with tenecteplase and transferred to CSCs for endovascular therapy experienced shorter needle-to-groin times than those treated with alteplase.
-
• The “Primary Stroke Center Effect” underscores the importance of earlier arrival at stroke centers.
Introduction
Intravenous thrombolysis (IVT) is a specific, effective, time-dependent reperfusion therapy for acute ischemic stroke. Each 15-minute decrease in treatment delay is estimated to provide an average of one month of additional disability-free life. Reference Meretoja, Keshtkaran and Saver1 This increased chance of achieving better clinical outcomes with faster administration has not only been observed with alteplase but also with tenecteplase, demonstrating a 1.8% and 0.2% increase in the probability of achieving excellent functional outcome at 90 days with a 30-minute reduction in the onset-to-needle time, and with every 10-minute reduction in door-to-needle time, respectively. Reference Singh, Almekhlafi and Bala2 Fast delivery of this treatment can be accomplished not only in comprehensive stroke centers (CSCs) that offer more advanced therapies (i.e., endovascular thrombectomy (EVT), decompressive craniectomy, intensive care unit) but also in centers that have the capability only to offer urgent neuroimaging and to administer IVT. Reference Alberts, Latchaw and Jagoda3 These primary stroke centers (PSCs) usually are located in suburban and rural areas, and they can be the closest hospital able to offer prompt diagnosis, urgent neuroimaging and IVT treatment to their catchment area. Considering the time-sensitive nature of stroke therapies, it is recommended that patients with suspected acute stroke be transported to the nearest stroke center. Reference Heran, Lindsay and Gubitz4
A definite pathway for patients with suspected large vessel occlusion (LVO) regarding transportation to PSCs or CSCs is still in question. Attempts to model a decision-making process for patients with LVO have been made taking into consideration several challenges including regional geography, transportation times, and treatment times at these facility types. Reference Holodinsky, Williamson and Demchuk5 In addition, it is hypothesized that tenecteplase with its ease of use could contribute to faster IVT delivery in any center and decrease transfer times from PCSs to CSCs, a critical aspect especially in patients eligible to receive EVT. Reference Ospel, Dmytriw and Regenhardt6 The pharmacokinetic and pharmacodynamic profile of tenecteplase is better than alteplase, with longer half-life, less binding to plasminogen activator inhibitor-1 and higher fibrin specificity. Reference Moussaddy, Demchuk and Hill7
Treatment of acute ischemic stroke is highly time-sensitive, where PSCs play a key role in treating patients. It is therefore of utmost importance to efficiently transfer patients with suspected LVOs from PSCs to CSCs. In this secondary analysis of the AcT (Alteplase Compared to Tenecteplase) registry-linked randomized controlled trial, we sought to investigate the clinical outcomes and workflow times of patients treated with IVT in PSCs. In addition, we evaluated key metrics in patients transported from PSCs to CSCs for potential EVT enrolled in this trial. Reference Sajobi, Singh and Almekhlafi8
Methods
Study design and population
This is a subgroup analysis from the AcT trial. Reference Menon, Buck and Singh9 AcT was a phase 3, multicenter, prospective, pragmatic randomized controlled trial that assessed the non-inferiority of tenecteplase compared to alteplase for IVT in eligible patients aged ≥18 years with an acute ischemic stroke within 4.5 hours. A total of 22 centers participated in the trial, of which five were PSCs and the rest were CSCs. PSCs were defined as hospitals with resources and processes to offer IVT to patients with an acute ischemic stroke, but without the capability to offer EVT. CSCs were defined as centers with capability to offer IVT and EVT.
Acute stroke care in Canada is organized into a tiered based on center capabilities. Under the Canadian Stroke Best Practices guidelines, PSCSs correspond to Level 3 or 4 hospitals. Level 3 PSCs provide IVT with or without virtual telestroke support but lack dedicated inpatient stroke units. Level 4 PSCs offer onsite thrombolysis and maintain acute inpatient stroke units, with neurosurgical services available at some centers. CSCs, classified as Level 5 hospitals, provide advanced stroke care including EVT, neurosurgery, and advanced imaging services. CSCs receive patient transfers from PSCs for complex interventions. Catchment areas for PSCs vary regionally and are not uniformly defined, generally encompassing surrounding communities to provide timely access to acute stroke treatments. Given the wide geography, patients are transported to the nearest thrombolysis-capable center if they are in the <4.5-hour window (also eligible for AcT trial). Reference Heran, Lindsay and Gubitz4,Reference Adewusi, Demchuk and Stotts10
Efficacy and safety outcomes
The primary outcome was the proportion of patients with excellent functional outcome defined as having an mRS 0–1 at 90 days to 120 days after randomization. We assessed the following secondary outcomes: mRS 0–2 at 90 to 120 days, actual mRS score achieved at 90 to 120 days, return to baseline function (defined as return to pre-stroke function), EuroQol Visual Analogue Scale (EQ-VAS) at 90 to 120 days, EuroQol 5-Dimension 5-Level questionnaire (EQ5D5L) and EuroQol 5-Dimension (EQ5D) index, length of hospital stay, length of hospital stay for more than seven days, EVT utilization rates, eTICI score ≥2b and rAOL score of ≥2b on initial angiography for those who underwent EVT. LVO was defined on baseline CT angiography as occlusions of the intracranial internal carotid artery, the M1 segment of the middle cerebral artery, the proximal or dominant M2 segment of the middle cerebral artery or the basilar artery.
Additionally, we analyzed the following safety outcomes: mortality at 90 days, symptomatic intracerebral hemorrhage at 24 hours, defined as any intracerebral hemorrhage that was temporally related to, and directly responsible for worsening of the patient’s neurological condition, other intracranial bleeding (subarachnoid hemorrhage, subdural hemorrhage and intraventricular hemorrhage), peripheral bleeding requiring blood transfusions, any hemorrhage, orolingual angioedema and other serious adverse events.
Workflow time metrics
The following data on prehospital and in-hospital workflow times were collected from linked registries (QuiCR for Alberta and OPTIMISE for all other Canadian provinces except for Alberta): For both PSC and CSC: onset-to-door time (time of stroke symptom onset to patient arrival at the emergency department [ED]), onset-to-randomization time (time of stroke symptom onset to randomization), onset-to-needle time (time of stroke symptom onset to IVT administration), door-CT-time (time of emergency department arrival to first slice of CT imaging); CT-to-randomization time (time of first slice of CT imaging to randomization), door-to-needle time (time of ED arrival to IVT administration), and for CSC only: onset-to-puncture time (time of stroke symptom onset to groin puncture for EVT), door-to-puncture time (time of ED arrival to groin puncture time for EVT); door-to-reperfusion time (time of ED arrival to reperfusion time for EVT) and puncture-to-first-reperfusion time (time of groin puncture to reperfusion time for EVT). First reperfusion time is defined as the first time recanalization status was achieved during the procedure.
Additionally, for patients transferred from PSCs to CSCs for potential EVT, the following data were collected: onset-to-door time and onset-to-CT time at PSCs, CT-to-puncture time, onset-to-needle time, needle-to-puncture time (time of IVT administration to groin puncture time for EVT), eTICI score of ≥2b/3 on initial angiography run for EVT, puncture-to-successful reperfusion time and needle-to-first reperfusion time (time from IVT administration to time recanalization status achieved).
Statistical analysis
Descriptive analysis was performed to compare baseline demographic and clinical characteristics of patients enrolled at PSCs and those enrolled at CSCs. Baseline characteristics were summarized using frequencies and proportions for categorical variables, mean with standard deviation (for normally distributed continuous variables) and medians with interquartile ranges (for non-normally distributed continuous variables). Mixed-effects Poisson regression analysis was conducted to determine the association between center type (PSC vs CSC) and the respective primary, secondary and safety outcomes. Age, sex, baseline stroke severity (NIHSS), location of intracranial occlusion, door-to-needle time and thrombolytic drug given were included as fixed effects variables, and site was included as a random effects variable. For models assessing workflow times as an outcome, mixed-effects Poisson regression analysis was used adjusting for age, sex, NIHSS, drug type and location of occlusion as fixed effects variables and participating site as random effects variable.
We report effect estimates as rate ratios (adjusted and unadjusted). A p-value of <0.05 was considered significant. Similar unadjusted and adjusted analysis was done comparing differences in outcomes between alteplase and tenecteplase in patients who presented at CSC and PSC, respectively. All analysis was considered exploratory. In addition, we also conducted secondary analysis to assess heterogeneity in treatment effects in the intention-to-treat population for primary outcome (mRS 0–1 at 90 to 120 days) and key safety outcomes by type of enrolling hospital (PSCs vs. CSCs). Evidence of a treatment-by-sub-group variable interaction was tested by including a multiplicative interaction term (thrombolytic type*center type) in the mixed effects logistic regression model adjusted for age, sex, baseline stroke severity and stroke onset-to-needle time as fixed effects, and site, and registry (QuiCR vs. OPTIMISE) as random effects. Statistical significance for each subgroup analysis was considered exploratory and conducted at alpha < 0.05.
The variables chosen for the adjusted analysis were selected to account for known confounders influencing outcomes, including demographic, clinical and treatment-related factors. In contrast, the secondary analysis focused on assessing treatment effect heterogeneity by center type, prioritizing key modifiers of treatment response while avoiding over-adjustment. Stata v17.0 software was used for all analyses.
Standard protocol approvals, registrations and patient consents
Approval from the ethical standards committee was received to conduct this secondary analysis.
Results
Baseline characteristics
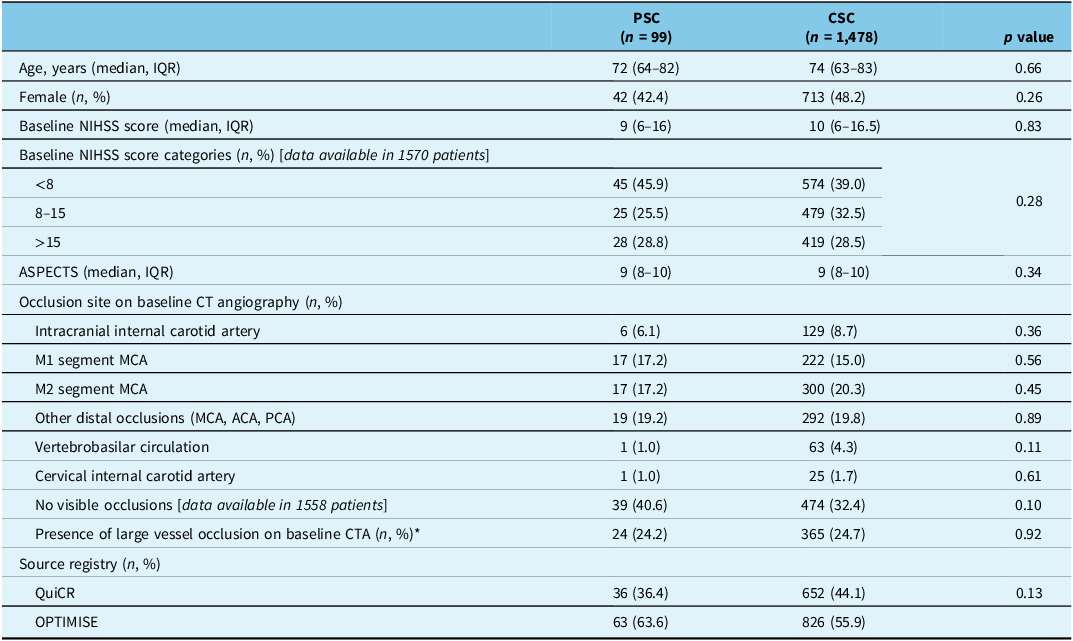
Of 1577 participants enrolled in the AcT trial, 99 (6.27%) were enrolled at PSCs (56: tenecteplase, 43: alteplase) and 1478 (93.72%) (750 tenecteplase, 728: alteplase) at CSCs. Baseline demographic, clinical and radiological characteristics were similar between the two groups and by thrombolytic type (Table 1 and Supplemental Table 1).
Baseline demographic, clinical, and radiological characteristics of patients treated in PSCs and CSCs

IQR= interquartile range; NIHSS= National Institutes of Health Stroke Scale; ASPECTS= Alberta Stroke Program Early CT Score; ICA= internal carotid artery; MCA= middle cerebral artery; ACA= anterior cerebral artery; PCA= posterior cerebral artery; PSC= primary stroke centers; CSC= comprehensive stroke centers; LVO = large vessel occlusion. CTA = computed tomography angiography
Analysis: Mann–Whitney (age, NIHSS). Chi2.
* LVO patients randomized at PSCs and transferred for endovascular thrombectomy counted in PSC group.
Outcomes
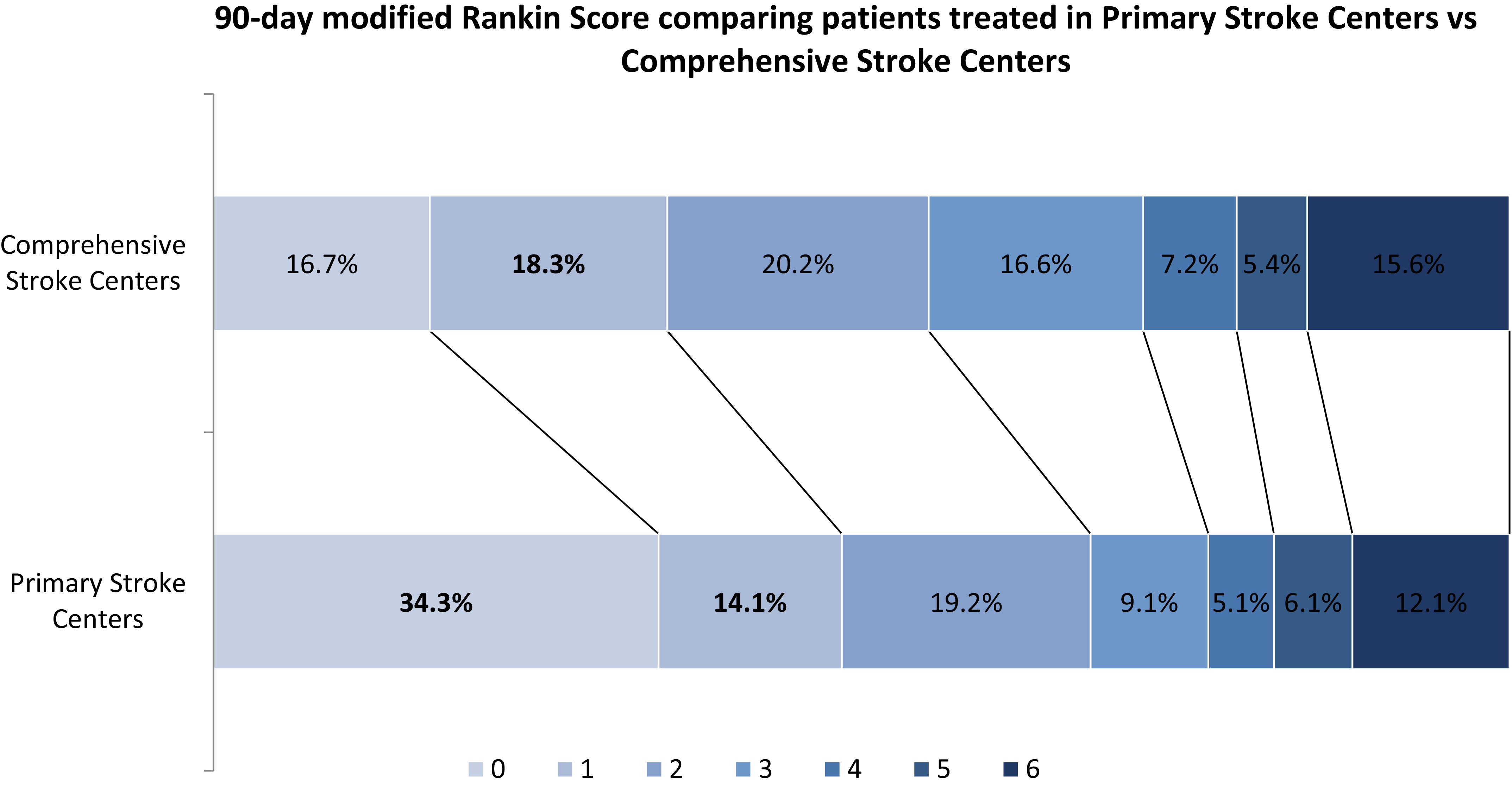
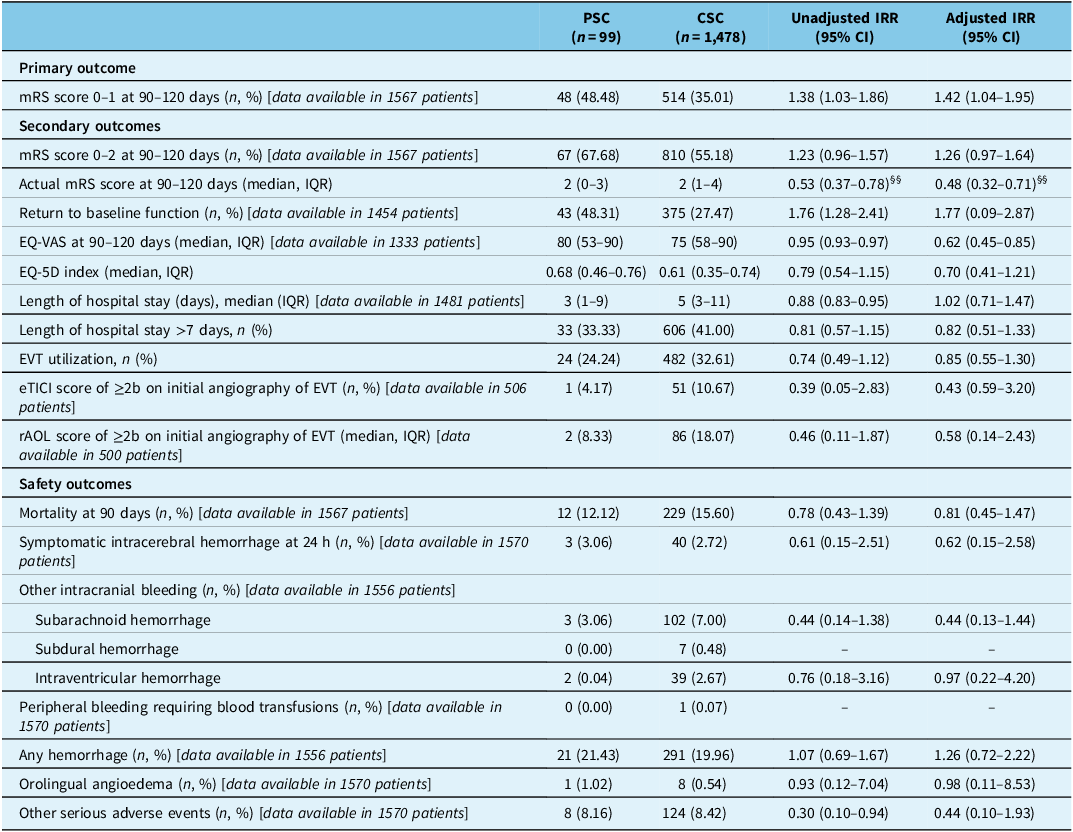
The proportion of excellent functional outcome (mRS 0–1) at 90 to 120 days was significantly higher for patients treated at PSCs compared to CSCs (48.48% versus 35.01%; adjusted Incidence Rate Ratio (IRR), 1.42 [95% CI, 1.04–1.95, p = 0.026]). Ordinal mRS and return to baseline function were statistically different between the PSC and CSC group, showing lower mRS scores (median, 2 (0–3) vs 2 (1–4) points; adjusted IRR, 0.48 [95% CI 0.32–0.71) and higher proportion of patients with return to baseline pre-stroke function among patients enrolled at PSCs (48.31% versus 27.47%; adjusted IRR 1.77 (95% CI 0.09–2.87) (Figure 1). Likewise, EQ-VAS score at 90 days was significantly higher in patients treated at PSCs compared to CSCs [median (IQR), 80 (53–90) versus 75 (58–90) points; adjusted IRR 0.62 [95% CI 0.45–0.85]. Rate of EVT utilization, successful reperfusion on initial angiographic run in patients undergoing EVT was similar (Table 2 and Supplemental Table 2).
90-day mRS comparing patients treated in PSCs vs CSCs.

Efficacy and safety outcomes in patients treated in PSCs compared to CSCs

mRS= modified Rankin Scale; EQ-VAS= EuroQol-visual analog scales; EVT= endovascular thrombectomy; rAOL= revised arterial occlusion scale; eTICI= extended thrombolysis in cerebral infarction; NIHSS= National Institutes of Health Stroke Scale; PSC= primary stroke centers; CSC= comprehensive stroke centers; IQR= interquartile range. IRR: Incidence Rate Ratio
Analysis: Poisson.§§OR (ologit). Adjusted for age, sex, baseline NIHSS, intracranial occlusion, drug type, and door-to-needle time.
All safety outcomes including mortality at 90 days, symptomatic intracerebral hemorrhage at 24 hours, peripheral bleeding requiring transfusion, orolingual angioedema and other serious adverse events were similar between the two groups (Table 2, Supplemental Tables 2 and 3).
There was no difference in primary outcome between patients treated with tenecteplase versus alteplase at PSCs (50% versus 46.51%; adjusted IRR 1.01 [95% CI 0.58–1.75) and at CSCs (35.92% versus 34.07%; adjusted IRR 1.08 [95% CI 0.95–1.23). Likewise, safety outcomes were similar stratifying by thrombolytic type in PSCs and CSCs (Supplemental Tables 2 and 3).
Workflow metrics
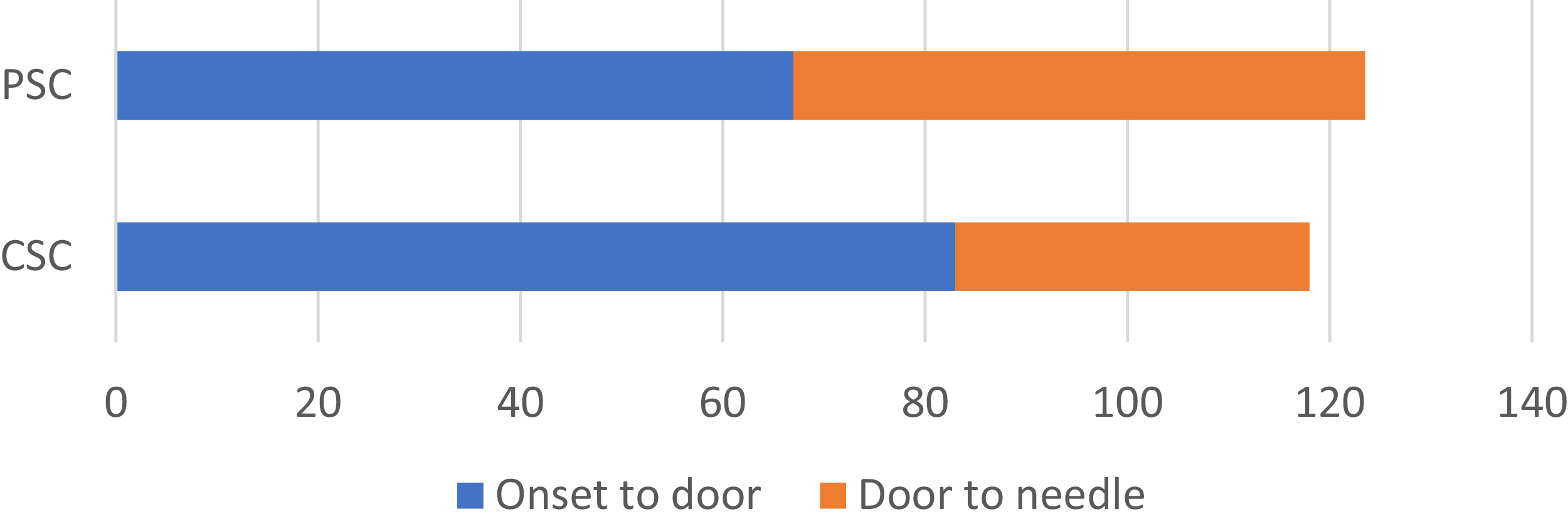
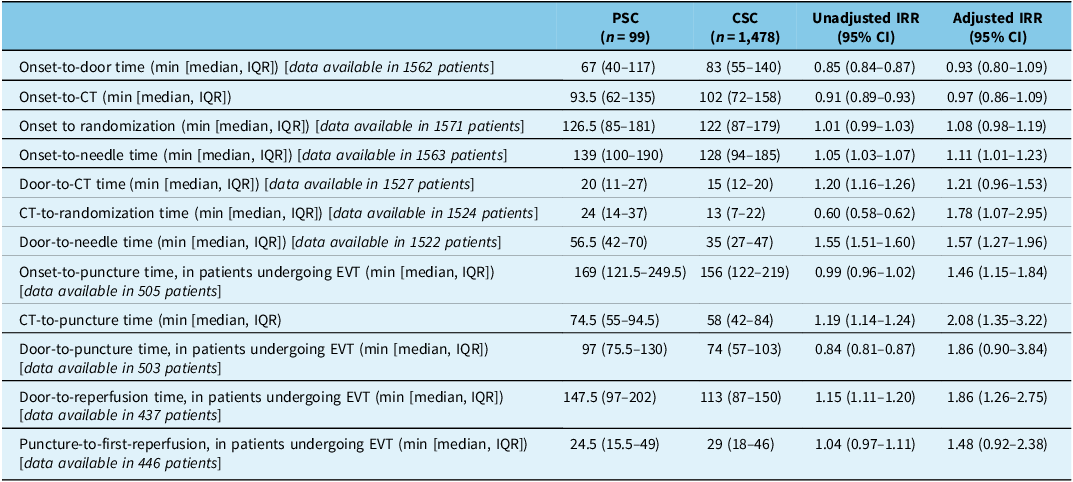
Onset-to-needle (median (IQR) 139 (100–190) versus 128 minutes (94–185); adjusted IRR 1.11 [95% CI 1.01–1.23]) and door-to-needle times (median (IQR) 56.5 (42–70) versus 35 minutes (27–47); adjusted IRR 1.57 [95% CI 1.27–1.96]) were significantly longer at PSCs compared to CSCs (Figure 2). Likewise, the CT-to-randomization time was longer in PSCs compared to CSCs (median (IQR) 24 (14–37) versus 13 minutes (7–22); adjusted IRR 1.78 [95% CI 1.07–2.95]). There was no difference between PSC and CSC for other workflow metrics such as onset-to-door, onset-to-CT, door-to-CT and onset-to-randomization times (Table 3).
Onset-to-door and door-to-needle times in patients treated in PSCs and CSCs. PSC= primary stroke centers; CSC= comprehensive stroke centers. Values correspond to the median. Numbers represent minutes.

Workflow times in patients arriving at PSCs and CSCs

EVT= endovascular thrombectomy; CI= confidence interval; IQR= interquartile range; IRR= Incidence Rate Ratio; PSC= primary stroke centers; CSC= comprehensive stroke centers. Onset: stroke symptom onset. Door: hospital arrival. Needle: intravenous thrombolysis start. Puncture: groin puncture, EVT start.
Analysis: Poisson. Adjusted for age, sex, baseline NIHSS, intracranial occlusion, and drug type.
For patients who underwent EVT, presentation at a PSC was associated with significantly longer onset-to-puncture (median, 169 versus 156 minutes; adjusted IRR, 1.46 [95% CI, 1.15–1.84]), initial CT (at PSC)-to-puncture (median 74.5 versus 58 minutes; adjusted IRR, 2.08 [95% CI, 1.35–3.22,) and door-to-reperfusion times (median 147.5 versus 113 minutes; adjusted IRR, 1.86 [95% CI, 1.26–2.75) as compared to those presenting at CSC. Puncture-to-first reperfusion time (median, 24.5 versus 29 minutes; adjusted IRR, 1.86 (95% CI, 1.26–2.75]) was similar in both groups. (Supplemental table 4).
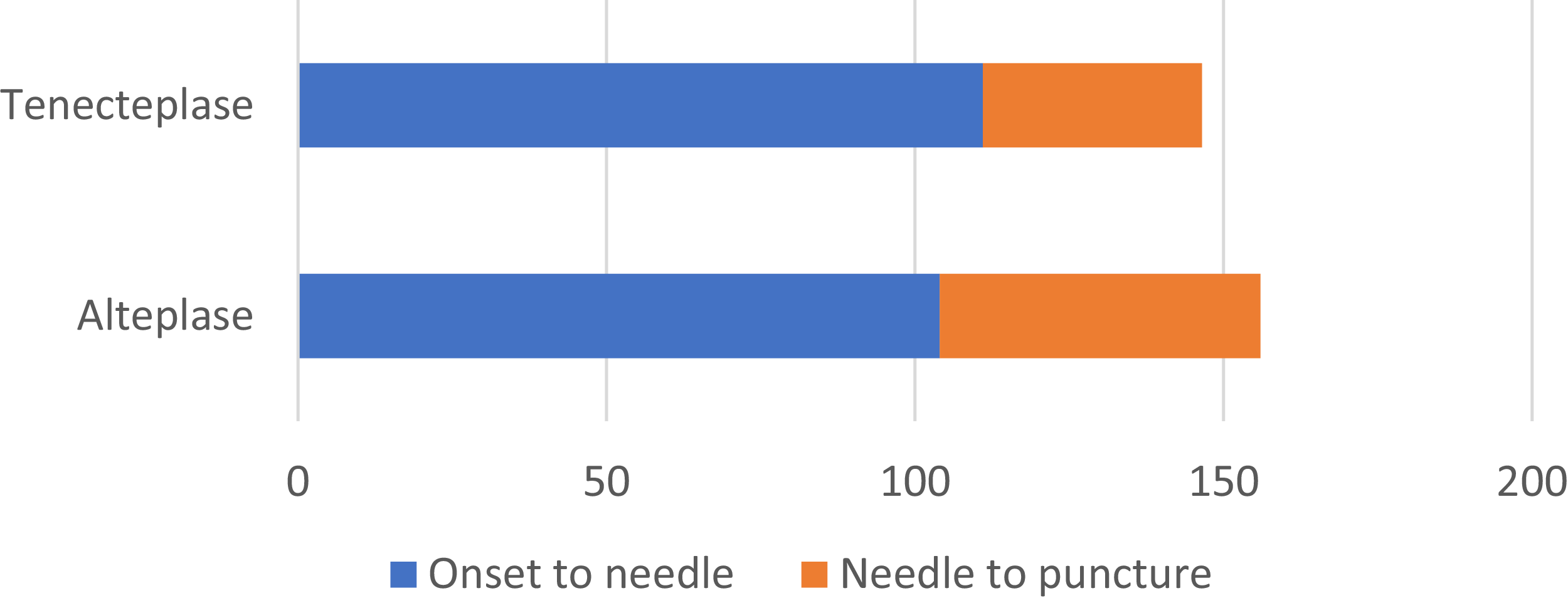
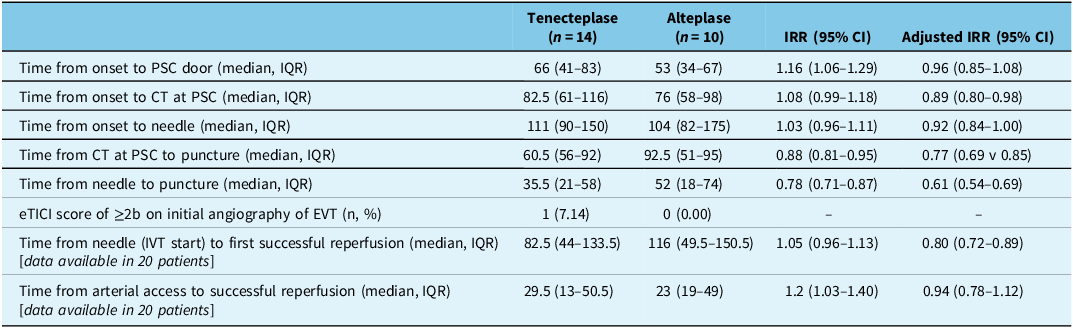
The workflow times comparing patients who received tenecteplase vs alteplase for the subgroup of patients transferred from PSCs to CSCs are shown in Table 4. There were 24 patients in total who were transferred for EVT, 14 of whom received tenecteplase. The following time metrics were significantly lower in patients that received tenecteplase compared to alteplase: CT-to-puncture time (median, 60.5 versus 92.5 minutes; adjusted IRR, 0.77 [95% CI, 0.69–0.85]); needle-to-puncture time (median, 35.5 versus 52 minutes; adjusted IRR, 0.61 [95% CI, 0.54–0.69]) and needle-to-reperfusion time (median, 82.5 versus 116 minutes; adjusted IRR: 0.80 [95% CI, 0.72–0.89) (Figure 3). Meanwhile, groin-to-reperfusion time was similar between the two groups (median, 29.5 versus 23 minutes; adjusted IRR: 0.94 [95% CI, 0.78–1.12]).
Onset-to-needle and needle-to-puncture times in patients transferred from PSCs to CSCs for potential EVT, by thrombolytic type. PSC= primary stroke centers; CSC= comprehensive stroke centers. Values correspond to the median. Numbers represent minutes.

Workflow times in patients transferred from PSCs to CSCs for potential EVT, by thrombolytic type

Onset: stroke symptom onset. Door: hospital arrival. Needle: intravenous thrombolysis start. Puncture: groin puncture, EVT start. IQR= interquartile range; PSC= primary stroke centers; CSC= comprehensive stroke centers; IVT = intravenous thrombolysis; eTICI= extended thrombolysis in cerebral infarction. IRR= Incidence Rate Ratio
Analysis: Poisson. Adjusted for age, sex, baseline NIHSS, intracranial occlusion, drug type, and door-to-needle time.
There was no significant interaction for primary and safety outcomes (Supplemental Table 5).
Discussion
In this subgroup analysis of the AcT trial, we found that patients treated with IVT at PSCs had higher rates of excellent functional outcome and return to baseline function with similar safety outcomes as compared to those who were treated at CSCs. Moreover, the workflow at PSCs was less efficient than CSCs, with slower door-to-needle, door-to-CT, door-to-puncture and door-to-reperfusion times. Interestingly, among patients who were treated in PSCs and subsequently transferred to CSCs for EVT, those who received tenecteplase had faster workflows, with more efficient CT-to-needle and needle-to-puncture times, compared to their counterparts who received alteplase.
It is possible that early arrival to a stroke center could account for improved functional outcomes at 90 to 120 days, since prompt IVT is a pivotal treatment in the hyperacute phase of the stroke, as is early clinical stabilization. While a well-defined “bundle of care” is described for hemorrhagic stroke, Reference Ma, Hu and Song11 but not for patients with ischemic stroke, patients treated at PSCs may receive faster temperature, blood pressure, oxygenation and glycemic control than patients admitted to a CSC several minutes later in the very early phase of the ischemic stroke. Additionally, our unadjusted analysis showed that patients treated at PSCs stayed fewer days at hospital compared to patients at CSCs (a median of 3 versus 5 days, respectively). Further investigation is needed to explore whether the length of stay is associated with center type. For instance, this could involve examining whether the proximity of PSCs to patient’s families and communities contributes to shorter stays, or if shorter stays at PSCs reflect a less medically complex patient population.
Although it is well-known that one of the key predictors of length of stay is the severity of the stroke, Reference Chang, Tseng, Weng, Lin, Liou and Tan12 these two groups could have unmeasured baseline clinical or sociodemographic differences that our registries did not capture, despite having similar age, NIHSS, EVT rate, hemorrhagic complications and serious adverse events.
The performance of PSCs and CSCs regarding time metrics and clinical outcomes has been explored previously. The Transfer to the Closest Local Stroke Center vs Direct Transfer to Endovascular Stroke Center of Acute Stroke Patients With Suspected Large Vessel Occlusion in the Catalan Territory, RACECAT trial, which enrolled patients with suspected LVO in a drip-and-ship versus mothership model, showed more patients receiving IVT at local stroke centers compared to EVT-capable stroke centers (60.4% and 47.5%, respectively), with a difference in onset-to-needle times (120 and 155 minutes, respectively), similar door-to-needle times (30 and 33 minutes, respectively) and similar clinical outcomes at 90 days. Reference De La Ossa, Abilleira and Jovin13 A cohort study with participants that received reperfusion therapies recruited from Get With the Guidelines Stroke registry showed better door-to-needle times at CSCs and EVT-capable centers compared to PSCs, without significant difference in functional independence at discharge between CSCs and PSCs. Reference Raychev, Sun and Schwamm14 Door-to-needle time is key time metric in acute stroke care. In patients treated with IVT with or without EVT, lower door-to-needle times led to better clinical outcomes including home time and overall mortality, with chances of good outcome improving with each 15-minute period of optimization in the door-to-needle time. Reference Man, Solomon and Mac Grory15 Several simple and effective measures have been identified to improve this time metric, such as establishing a STAT stroke protocol, transporting patients to CT in the EMS stretcher and giving IVT near the CT room. Reference Kamal, Holodinsky and Stephenson16 The observed delays to treatment at PSCs, despite otherwise similar measured variables, are likely multifactorial. CT-to-randomization time was observed to be significantly longer at PSCs compared to CSCs (23.5 minutes vs 12 minutes; p < 0.001), suggesting that randomization procedures themselves may have contributed to the longer door-to-needle times. Additional factors may include less established or standardized acute stroke workflows, fewer research staff on site, and lower overall experience with trial procedures compared to CSCs. In our prespecified sub-analysis, despite prolonged door-to-needle and door-to-puncture times, a higher proportion of patients in PSCs had better clinical outcomes compared to CSCs. In the unadjusted analysis, onset-to-door time was lower in PSCs compared to CSCs (67 versus 83 minutes, respectively) likely due to geographic and logistical reasons.
The paradoxical finding of better outcomes at PSCs despite less efficient workflows may reflect several factors. First, PSCs may have enrolled patients with less complex presentations or fewer comorbidities, while CSCs more often manage higher-acuity cases, including LVOs requiring thrombectomy. All PSCs that participated in the trial receive suspected stroke cases within 4.5 hours from their surrounding regions, similar to other PSCs. These sites follow a “drip and ship” model: patients within 4.5 hours of onset are initially taken to the nearest PSC and are transferred to a CSC only if EVT is indicated. If there is a high suspicion of LVO, bypass to the closest CSC is possible at the discretion of the transporting physician. None of these PSCs utilized telestroke services during the time of the study. Second, site-level enrollment patterns could have introduced subtle selection effects, whereby clinicians at PSCs randomized patients perceived as more stable or likely to benefit. Third, although workflow metrics such as door-to-needle times were longer at PSCs, the overall care environment may have been less complex, with fewer competing demands compared to high-volume CSCs, allowing for more consistent implementation of thrombolysis protocols. Finally, the relatively small number of patients recruited at PSCs increases the likelihood that the observed differences are due to random variation rather than systematic effects. Importantly, AcT was conducted during the COVID-19 pandemic, which impacted overall recruitment and explains why the numbers were lower than expected. Nonetheless, it was the first pragmatic acute stroke trial in Canada to include PSCs, making it a crucial stepping stone for future clinical trial capacity-building at these centers. Since AcT used broad inclusion criteria, enrolling patients regardless of age or baseline disability, the trial also provides unique insights into the feasibility of extending trial participation beyond CSCs to better reflect real-world populations. Since AcT was a pragmatic clinical trial, inclusion criteria were broad – as in, all patients independent of their age and baseline disability were eligible for enrollment. Although we did not collect pre-morbid mRS owing to nature of the trial, we did collect a pragmatic functional outcome of “return to baseline pre-stroke function” – which meant to ask if the patients with premorbid disability achieved their pre-morbid baseline status. We found that there was indeed a significant difference between the two groups: a higher proportion of PSC patients achieved return to baseline pre-stroke function compared to CSC patients (43 of 89 [48.31%] vs 375 of 1,365 [27.47%], respectively.
Certain time metrics at PSCs differed depending on the thrombolytic that was used for patients transferred to CSCs. For instance, despite similar door-to-needle times among those receiving tenecteplase and alteplase (56.5 minutes for both), those who were transferred to a CSC for EVT and received tenecteplase presented with lower CT-to-puncture (60.5 versus 90.5 minutes) and needle-to-puncture (35.5 versus 52 minutes) times. Even though we did not collect door-in-to-door-out times, it is evident that the transportation to a CSC was more efficient for those who were treated with tenecteplase. The pharmacological advantages of tenecteplase compared to alteplase, its effectiveness, safety, and the evidence that supports its use are well described elsewhere. Reference Miller and Warach17–Reference Streib20 Additionally, there are several real-world experiences that have shown reassuring results when alteplase has been replaced by tenecteplase. Reference Rodriguez, Prasad and Olson21–Reference Hendrix, Collins and Griessenauer24 The possibility to give a single bolus of tenecteplase, instead of a bolus plus a 1-hour of continuous administration of alteplase through an infusion pump, with the risk of lower plasma level if there are delays between bolus and infusion, Reference Kobayashi, Saito, Kawabata and etal25 explains its success in shortening key workflow times especially for patients that are transferred to a CSCs to receive EVT in ambulances without the capability of continuous infusion administration. We did not find differences in early recanalization between patients treated with tenecteplase or alteplase at PSCs. The EXTEND-IA TNK trial (part 1), a randomized controlled trial of tenecteplase versus alteplase in patients with LVO treated in the 4.5-hour window, showed a substantial reperfusion of 22% and 10%, favoring tenecteplase. Reference Campbell, Mitchell and Churilov26 The sub-analysis of the AcT trial in patients with medium-vessel occlusions showed a significant difference in intracranial recanalization favoring tenecteplase, Reference Bala, Singh and Ignacio27 without difference in the subgroup analysis for patients with LVO. Reference Bala, Singh and Buck28
The higher rate of EVT utilization observed in CSCs compared to PSCs despite similar proportions of large vessel occlusions is likely multifactorial. Patient selection and transfer logistics could contribute to this. For example, patients initially assessed at PSCs must be transferred to CSCs for EVT, and prolonged transport times may render some patients ineligible for intervention. CSCs also tend to manage a greater proportion of severe strokes and complex cases, contributing to higher EVT rates. Additionally, the expanding indications for EVT in medium vessel occlusions may further increase EVT utilization at CSCs.
Our findings challenge the prevailing assumption that CSCs uniformly provide superior outcomes compared to PSCs. Specifically, the observation that patients who remained at PSCs demonstrated outcomes that were comparable, if not better, than those treated at CSCs raises important questions about the potential advantages of PSC care. These benefits may stem from highly standardized, guideline-adherent care pathways, more streamlined inpatient management, or faster transitions to rehabilitation services often integrated within PSC settings. The observed 13.5% absolute difference in outcomes between PSCs and CSCs is notable, approaching the effect size of thrombolysis itself. While this comparison is made cautiously, this “PSC effect” highlights the importance of decentralized care models, particularly in geographically widespread or resource-limited regions, where equitable access to acute stroke care is critical. Future research should explore the mechanisms underlying this effect and assess whether specific organizational practices or resource allocations at PSCs contribute to these outcomes.
This study has certain limitations. First, the study population considers only patients enrolled in the AcT trial; thus, generalizability to other regions and countries with different stroke systems of care may be limited. Second, the number of patients transferred to CSCs for potential EVT and its workflow characteristics are insufficient to draw firm conclusions regarding workflow and time metrics in this subgroup of patients. Third, as a subgroup analysis of a randomized controlled trial, our study should be regarded as a hypothesis-generating exploratory analysis. Comparisons between PSCs and CSCs are observational and may be influenced by site-level enrollment and case-mix differences not fully captured in the trial. Observed outcomes can also be influenced by workflow metrics, referral patterns and treatment capabilities, but it is difficult to determine the relative contribution of each, and the effect is likely multifactorial. The percentage of patients enrolled from PSCs was only 6.2%, reflecting challenges in conducting research at these centers. However, it is important to note that the trial was conducted during the COVID-19 pandemic, which likely impacted overall recruitment. Additionally, this was the first acute stroke trial conducted at PSCs in Canada, making it a crucial stepping stone for building research capacity and facilitating future clinical trials at these centers.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2026.10590.
Data availability statement
Anonymized data not published within this article will be made available by request from any qualified investigator. Please send data access requests to bkmmenon@ucalgary.ca. Such requests must be approved by the respective ethics boards and appropriate data custodians.
Acknowledgments
We thank the Canadian Stroke Consortium for their support of the trial recruitment efforts and the Canadian Institutes of Health Research (grant numbers 419722 and 450890), the Alberta Strategy for Patient-Oriented Research Support Unit, Alberta Innovates, the Heart and Stroke Foundation, and the University of Calgary for funding support.
Author contributions
DG, NS, BKM: Conceptualization, study design, methodology, data analysis, and manuscript drafting. DG, NS, KI: Statistical analysis, interpretation of data, and manuscript revision. DG, NS: Literature review, manuscript writing, and final approval of the manuscript. AT, HM, AG, MH, HK, JS, FB, MAT, GH, AA, DD, AMD, RHS, LC, TTS, MAA: Data interpretation, critical review of the manuscript, and revisions for important intellectual content.
Funding statement
Canadian Stroke Consortium; Canadian Institutes of Health Research (grant numbers 419722 and 450890); Alberta Strategy for Patient Oriented Research Support Unit; Alberta Innovates; Heart and Stroke Foundation; University of Calgary.
Competing interests
BKM has stock options in Circle NVI and has consulted for Biogen and Boehringer Ingelheim. LC has received payments by Servier and consulting fees from Ischaemavie RAPID, Circle NV, and Canadian Medical Protective Association. JS has a grant from Medtronic to the University of Manitoba. AMD has received consulting fees from Hoffman La Roche (advisory board member); honoraria from Boehringer Ingelheim (CME events); has patent and stocks for Circle CVI (stroke imaging software); has been DSMB chair for LT 3001-203 and LT 3001-205 studies; and chair, board of directors of Canadian Stroke Consortium for which has received annual stipend. TTS has received consulting fees from Circle NVI. RHS has stock options in FollowMD and receives salary support for research from the Heart & Stroke Foundation of Canada, Sandra Black Centre for Brain Resilience & Recovery, and Ontario Brain Institute. AG reports consulting fees and honoraria from Alexion, Biogen Eisai, and Servier Canada; research support from Alberta Innovates, the Alzheimer Society of Canada, the Alzheimer Society of Alberta and Northwest Territories, Brain Canada, the Canadian Institutes of Health Research, Campus Alberta Neuroscience, the Government of Canada INOVAIT and New Frontiers in Research programs, the France-Canada Research Fund, the Heart and Stroke Foundation of Canada, Microvention, MSI Foundation, and Panmure House; and stock/stock options from SnapDx Inc. and Collavidence Inc. (Let’s Get Proof) – all outside the scope of the published work. All other authors declare no competing interests.



 Open access
Open access