


Up to 10% of brachial plexopathies are iatrogenic, most commonly caused by stretching or compression of nerve tissue during procedure-related positioning such as in cardiothoracic surgeries. Reference Desai and Nemcek1 Brachial plexus injury has been prospectively reported in 0.5%–9.6% of coronary artery bypass grafting (CABG) surgeries with conventional methods. Reference Unlu, Velioglu, Kocak, Becit and Ceviz2 Minimally invasive cardiac surgery (MICS) CABG is a technique that has been developed to maximize clinical outcomes and minimize postoperative complications by avoiding sternotomy. Reference McGinn, Usman, Lapierre, Pothula, Mesana and Ruel3 We report a case of acute brachial plexopathy following MICS CABG.
A 70-year-old male, with coronary artery disease and worsening unstable angina, was noted to have painless flaccid paralysis of the left arm after regaining consciousness from MICS CABG. The surgery was performed through a small left thoracotomy without cardiopulmonary bypass, while the patient was positioned in 25 degrees right lateral decubitus with the left arm abducted above his head. The procedure was moderately prolonged (5 hours) due to technical factors related to the presence of pectus excavatum. On initial examination postoperatively, there was no movement in any muscle of the left arm and areflexia in the entire left upper extremity. The patient had circumferential, multi-dermatomal paresthesia with pinprick and light touch deficits circumferentially distal to the elbow. The examination of the cranial nerves and lower extremities was unremarkable. On day 3, a brain magnetic resonance imaging (MRI) showed a tiny cortical focus of Diffusion Weighted Imaging hyperintensity in the right parietal lobe. MRI of the cervical spine showed degenerative changes with severe narrowing of the left neural foramen at C5-C6. MRI of the left brachial plexus (Figure 1) demonstrated subtly increased Short Tau Inversion Recovery (STIR) signal at the level of the upper trunk, thought to represent intraneural edema. On day 6, the patient regained 2/5 (manual muscle testing, MRC scale) strength in most left upper extremity muscles except for 4+/5 strength of finger flexion and 0/5 shoulder abduction. He was discharged on day 7, with outpatient appointments in physiotherapy and occupational therapy. Three weeks later, shoulder abduction was still graded 0/5 and shoulder external rotation 1/5. Wrist extension and finger extension were graded 2/5. Elbow extension was 4- while elbow flexion, wrist flexion, and finger abduction had improved to 4+/5. Pinprick sensation remained diminished in the axillary cutaneous territory but was normal in the forearm. Initial nerve conduction studies showed an unelicitable left axillary motor response and reduced sensory amplitude of the left radial and left medial antebrachial cutaneous nerves (Table 1). At month 2, dexterity and motor strength in left upper extremity continued to improve except for marked weakness of shoulder abduction and external rotation. The repeat electrodiagnostic study showed very frequent positive sharp waves and fibrillation potentials in the left deltoid and infraspinatus muscles, with a neurogenic recruitment pattern (Table 1). At month 3, shoulder abduction and external rotation strength grading improved to 4/5 with 4+ to 5 strength in the rest of the upper extremity. By 1 year, the patient had fully recovered all upper extremity function and sensation.
Short Tau Inversion Recovery (STIR)-weighted coronal MRI of the brachial plexus demonstrating mildly increased signal involving the left brachial plexus at the level of the upper trunk and posterior cord representing edematous changes (yellow arrows).

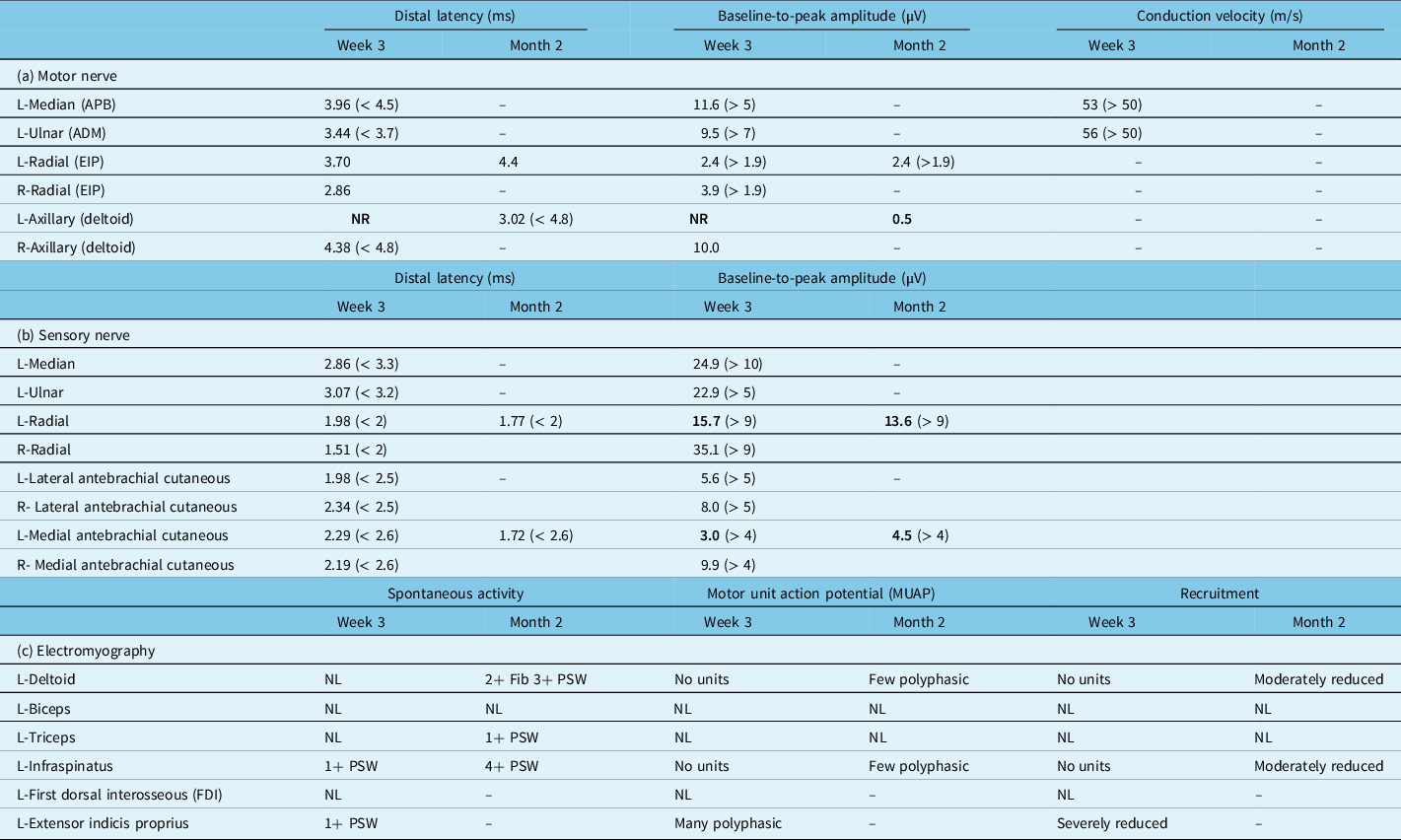
Motor (a) and sensory (b) nerve conduction studies and (c) needle electromyography of patient’s left upper extremity after 3 weeks and 2 months of follow-up (normal values are mentioned in parentheses; abnormal values are highlighted in bold; corresponding values in the right-side upper extremity were in the normal range, which are not shown all here in this table)

ADM = abductor digiti minimi; APB = abductor pollicis brevis; EIP = extensor indicis proprius; Fib = fibrillation; NL = normal; NR = not recordable; PSW = positive sharp waves.
To date, excellent short-term and long-term outcomes of MICS CABG have been reported, Reference Guo, Vo and Horsthuis4 with no previous report of sustained brachial plexus injury. We report the single case of postoperative brachial plexopathy out of nearly 600 MICS CABG procedures that have been performed at our center, with 100% follow-up. Reference Guo, Vo and Horsthuis4 The MICS CABG procedure is enabled by positioning the patient in a right lateral decubitus with the left arm abducted over the head. Reference McGinn, Usman, Lapierre, Pothula, Mesana and Ruel3 In that position, the upper trunk may be vulnerable to compression Reference Winfree and Kline5 by the posterior bow of the clavicle. Reference Logan and Black6 In contrast, the classic brachial plexopathy following traditional CABG with median sternotomy is due to the traction on the C8 anterior primary ramus. Reference Levin, Wilbourn and Maggiano7
In our case, the electrodiagnostic studies revealed a patchy pattern of involvement with main abnormalities in the distribution of the upper trunk (i.e. deltoid, infraspinatus) and posterior cord (i.e. extensor indicis) supported by the electromyography. The C8 innervated median, ulnar motor amplitudes, and ulnar sensory amplitude were within normal limits. The low radial sensory amplitude is consistent with upper trunk or posterior cord lesion. In upper trunk brachial plexopathy, an asymmetrically reduced (> 50%) or absent lateral antebrachial cutaneous sensory response is expected but was normal in our patient. Plexopathy can cause selective involvement of nerve fascicles, which can explain such electrodiagnostic findings. The consistently low medial antebrachial cutaneous sensory amplitude suggests there was traction on the lower trunk or medial cord and is consistent with the patient’s initial distal weakness and sensory loss. The upper trunk localization was confirmed by MRI of the brachial plexus (Figure 1). Increased STIR signal abnormality has been previously reported in stretch injuries of the brachial plexus. Reference Tharin, Kini, York and Ritter8
Given the rapidity of the clinical improvement, it is likely that there was a significant element of transient focal conduction block, except in the axillary territory where significant axonotmesis was demonstrated. The clinical significance of the C5-6 neural foraminal stenosis is unclear as the patient was asymptomatic prior to the cardiac surgery and the most severely affected muscles (i.e. deltoid and infraspinatus) are principally supplied by the C5 nerve roots. Reference Furukawa, Miyaji and Kadoya9 The absence of pain makes acute brachial neuritis unlikely.
Even with less-invasive robotic/laparoscopic techniques, measures to lower the incidence of iatrogenic peripheral nerve injuries include monitoring of patient positioning throughout the procedure, keeping the head and neck in a neutral position, limiting arm abduction, extension, and external rotation in the supine position, properly padding the shoulders during positioning, and if available, continuous monitoring of the somatosensory potential.Reference Winfree and Kline 5 All measures had been performed in the reported patient with, nevertheless, a poor initial neurological outcome followed by complete resolution. In conclusion, brachial plexopathies are much rarer after MICS CABG compared to CABG with median sternotomy. Due to the abducted position in MICS CABG, the brachial plexopathy may affect the upper plexus predominantly rather than the C8 anterior ramus, as seen post sternotomy. The ultimate outcome of brachial plexopathies post MICS CABG will depend on the degree of demyelination and axon loss. In this case, there was an excellent functional recovery, as has been previously reported for the vast majority of patients with brachial plexopathies after CABG. Reference Jellish and Oftadeh10
Data Availability Statement
The data that support the findings of this case study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors would like to thank the study patient, who provided verbal consent for all aspects of the publication.
Statement of Authorship
SMF, JZ, and MR were involved in the clinical assessment of the case. Data collection was done by SMF and JZ. MK assessed neuroimaging investigations. SMF, JZ, PB, and JW interpreted the electrodiagnostic studies. All authors (SMF, MR, PB, JW, MK, and JZ) were involved in drafting of the manuscript for intellectual content and revised the final version of the manuscript.
Competing Interests
The authors report no conflict of interest directly related to this case report. MR has received support from Medtronic in the Minimally Invasive versus Sternotomy (MIST) trial. PB has received support for expert testimony from Canadian Medical Protective Association.
Ethical Publication Statement
We confirm we have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.


 Open access
Open access