


Highlights
-
• Plasma p-tau-217 was the best biomarker to differentiate Aβ status.
-
• Plasma p-tau-217 improves the specificity of Clinical β-Amyloid Positivity Prediction Score (CAPS).
-
• CAPS Plus is a useful screening tool for enrollment in anti-Aβ clinical trials.
Introduction
It has been established globally that some individuals presenting with Alzheimer’s disease (AD)-like symptoms at memory clinics do not exhibit amyloid deposits in their brains. Reference Landau, Horng, Fero and Jagust1 This presents a recruitment challenge for anti-amyloid clinical trials and treatment programs, as Aβ positivity is a critical eligibility criterion. Reference Cummings, Osse, Cammann, Powell and Chen2 This issue has gained increased significance following Health Canada’s approval of lecanemab in October 2025. FDA and Health Canada-approved methods for the diagnosis of brain amyloidopathy are either an amyloid Positron Emission Tomography (PET) scan or a CSF analysis. Reference Hunter, Santos, Tovar-Moll and De Felice3 While CSF analysis offers a reliable, validated and inexpensive method to detect Aβ pathology, it requires a lumbar puncture – an invasive procedure that many patients find unacceptable. Concerns about pain, potential complications and general discomfort may lead to reluctance or refusal, limiting its practicality as a broadly accessible clinical diagnostic tool. Additionally, access to this service may be reduced in rural/remote clinics, which can hinder the engagement of potential participants, thereby limiting diverse representation in anti-Aβ trials. On the contrary, the primary barrier to using amyloid PET scans in a clinical context is their high cost. In the USA, the average cost for an amyloid PET is around $3000, which would equate to more than CA$5000. This makes these scans almost inaccessible outside of very few academic centers across Canada for clinical uses. In Ontario, for example, Aβ-PET scans can be done through a registry at only a handful of participating academic centers. Reference Smith, Phillips and Feldman4 The clinical access to these scans in other Canadian provinces is extremely limited as well. Furthermore, access to specialized PET equipment is limited to large city centers, often making it inaccessible to those in rural and remote locations. From the research standpoint, pharmaceutical sponsors tend to cover the PET scan costs when it comes to screening for clinical trials. However, failed amyloid PET screening results often add to the cost of research. Understandably, an essential step toward determining eligibility for anti-amyloid therapy trials would be the pre-selection of individuals with a high likelihood of being Aβ+ before confirmatory amyloid testing with PET scans or CSF analysis. This approach improves resource allocation, particularly in resource-limited settings like general physician clinics lacking access to confirmatory AD biomarkers. This specific topic in AD research has therefore received some well-deserved attention. For instance, at least three recent papers have proposed algorithms using blood-based biomarkers only (Aβ42/40 and ptau217) that can predict Aβ positivity on PET scans with great accuracy. Reference Niimi, Janelidze and Sato5–Reference Meyer, Kirmess and Eastwood7 Such approaches are believed to reduce screen failure rates in anti-amyloid clinical trials by a sizable margin.
While the accuracy of a purely blood-based biomarker algorithm is excellent, in a situation where there is dementia of uncertain origin, Reference Hunter, Santos, Tovar-Moll and De Felice3,Reference Palmqvist, Warmenhoven and Anastasi6 two considerations drive the desire for algorithms in Canada that incorporate clinical features as part of the scheme. First, the ease and low cost of getting a blood test for AD make this a scalable option for many; the same properties make the results vulnerable to misinterpretation if not interpreted in the correct clinical situation. Anecdotally, memory clinics across Canada are already receiving referrals from physicians regarding cognitively intact patients with positive plasma p-tau results, underlining the necessity of using clinical measures to anchor the use of blood-based biomarkers. Second, in many healthcare facilities across Canada outside urban centers, blood-based AD biomarkers continue to remain relatively inaccessible. Reference Smith, Phillips and Feldman4 Keeping these factors in mind, this group of authors previously proposed a Clinical β-Amyloid Positivity Prediction Score (CAPS) using simple parameters to estimate the likelihood of Aβ pathology in individuals aged 60–80 years with Alzheimer-like symptoms. Reference Lahiri, Seixas-Lima and Roncero8,Reference Lahiri, Roncero and Lima9
Although the CAPS algorithm demonstrated an accuracy of 86% in a small Canadian cohort, its specificity was only 80%, indicating a potential for high false-positive rates. To improve the specificity of CAPS, we assessed the addition of AD blood-based biomarkers, including amyloid beta 42 and 40 (Aβ42 and Aβ40), phosphorylated tau 181 and 217, glial fibrillary acidic protein (GFAP), neurofilament light (NfL) and TDP-43. This investigation led to the incorporation of p-tau-217 into the clinical scheme. The inclusion of plasma p-tau-217 is particularly promising due to its correlation with brain amyloid pathology. Reference Mammel, Hsiung and Mousavi10–Reference Khalafi, Dartora and McIntire12 Elevated levels of p-tau-217 in plasma correlate strongly with amyloid PET and CSF biomarkers, providing a less invasive and more accessible means of detecting AD pathology. We hereby propose a clinical biomarker composite score, termed Clinical Amyloid Positivity Prediction Score Plus (CAPS Plus), which integrates the Neuropsychiatric Inventory–Questionnaire (NPI-Q) score, Reference Kaufer, Cummings and Ketchel13 the rate of decline in mini-mental state examination (MMSE) score over time, the magnitude of cerebrovascular disease burden as measured by Fazekas score Reference Fazekas, Chawluk, Alavi, Hurtig and Zimmerman14 and plasma p-tau217 levels to predict Aβ+ in individuals presenting with clinical Alzheimer’s syndrome, Reference Dubois, Villain and Schneider15 including both prodromal and mild AD. This algorithm is distinct from a biomarker-only approach in the sense that it extends a clinical scoring system to predict brain amyloidopathy Reference Lahiri, Seixas-Lima and Roncero8 and thereby applies the blood results in a clinical context.
Methods
Participant and specimen selection
The same cohort that was studied to develop CAPS was examined in this study. Detailed characteristics of this specific cohort are described elsewhere. Reference Lahiri, Seixas-Lima and Roncero8,Reference Lahiri, Roncero and Lima9 Briefly, all participants had a clinical diagnosis of AD according to the NIA-AA criteria, Reference Boone16 as deemed by memory clinic physicians, including neurologists, geriatricians and geriatric psychiatrists. Only participants from the original CAPS study who had blood were included in the current study as the primary objective is to evaluate how incorporating a novel and accurate blood-based biomarker for AD within a clinical prediction tool can predict Aβ status as determined by CSF analysis, PET scans or both. Details are elaborated in the original CAPS paper. Reference Lahiri, Seixas-Lima and Roncero8 All cohorts in this project followed best practices for blood collection, where, immediately following the collection of venous blood, tubes were inverted 8–10 times and processing was completed within 4 h by centrifugation at 1800 rcf for 15 min. This rigor is important as preanalytical factors account for 50–70% of laboratory test error. Reference Boone16 Specimens were anonymized and sent to collaborators (CW and JC) at the University of British Columbia, who performed biomarker analysis. Specimens were shipped on dry ice and, upon arrival, entered into a bar-coded laboratory inventory management system and stored in a dedicated, alarmed and secured −80°C freezer.
Biomarker analysis
Biomarker concentrations were quantified using single-molecule array (Simoa) immunoassays on the Quanterix HD-X platform (Billerica, MA) following the manufacturer’s protocol. Plasma Aβ42, Aβ40, GFAP and NfL were measured using the Neurology-4-plex E (N4PB) advantage assay (catalog #103670, lot #503420). We also measured plasma using the phosphorylated tau 181 advantage (catalog #103714, lot #503811), AlzPATH phosphorylated tau 217 advantage (catalog #104570, lot #504180) and TDP-43 (catalog #103293, lot #503818). Each assay included an 8-point calibrator curve and two internal kit controls. All specimens were diluted 4-fold on board, assayed in duplicate, and the mean value was reported as the result. Participants were analyzed on a single plate per assay, and quality control measures were documented across all runs (Supplemental Table 1). The average coefficient of variation (CV) for calibrator average enzyme bound was 5.5% with an average error of 5.8%. Internal controls had an average CV of 3.0% and an average error of 7.2%, and all plasma samples had an average CV of 4.9%.
Statistical analysis
Groupwise comparisons were performed between participants dichotomized by amyloid positivity, as determined by CSF analysis (n = 26) or amyloid PET (n = 20) or both (in two cases). Biomarker concentrations were determined to be nonparametric by the Shapiro–Wilk test, and group data are reported as the median with interquartile range. Group comparisons between Aβ+ and Aβ- for demographics, study measures and raw biomarker concentrations were performed using a Mann–Whitney U test for continuous variables or a Fisher’s exact test for categorical variables. To assess the diagnostic utility of plasma biomarkers and CAPS scores, the area under the receiver operating characteristic curve (AUROC) analysis was performed. To determine optimal plasma biomarker cut-offs, Youden’s index was applied to the ROC to select a cut-off with an optimal balance of sensitivity and specificity. To incorporate p-tau-217 into CAPS Plus, the original framework was used, including 0–2 points for total NPI-Q score, 1 point for an MMSE loss of >2 per year and 1 point for a Fazekas score of ≤1. A score of +1 was assigned to individuals with a plasma p-tau 217 above the cut-off, making the maximum possible score as 5, with those ≥4 indicating a high probability of being Aβ+. The Delong test was used to formally compare the ROC curves for CAPS, CAPS Plus and p-tau 217.
Results
Cohort description
Of the 44 participants included in this study, 25 (57%) were determined to be Aβ+ based on amyloid PET or CSF, while 19 (43%) were Aβ−. Comparing between Aβ+ and Aβ− participants, we found no significant differences in age, sex, dementia presentation and duration, MMSE scores and Fazekas score (Table 1). However, Aβ+ participants had higher NPI-Q scores (p = 0.0014) and higher CAPS scores (p = 0.0002) with a larger proportion of CAPS positivity (0.0002), when compared to Aβ− participants (Table 1).
Participant demographics dichotomized by amyloid positivity. Comparisons were performed using a Mann–Whitney U test for continuous variables and a Fisher’s exact test for categorical variables

Note: SCI = subjective cognitive impairment; MCI = mild cognitive impairment; MMSE = mini-mental state examination; NPI-Q = Neuropsychiatric Inventory–Questionnaire; CAPS = Clinical β-Amyloid Positivity Prediction Score; NfL = Neurofilament Light; GFAP = Glial Fibrillary Acidic Protein; and TDP-43 = TAR DNA-binding protein 43.
Plasma biomarkers
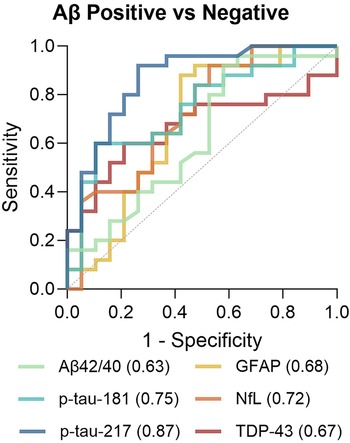
Plasma Aβ42/40, p-tau-181, p-tau-217, NfL, GFAP and TDP-43 were analyzed to determine which plasma biomarkers to incorporate into CAPS. When comparing participants by Aβ status, plasma p-tau-181 (p = 0.0050), p-tau-217 (p < 0.0001), NfL (p = 0.0124) and GFAP (p = 0.0432) were all higher in those who were Aβ positive compared to negative (Table 1, Figure 1). Plasma Aβ42/40 and TDP-43 were not significantly different between groups. To assess the diagnostic utility of these biomarkers, ROC analysis was performed, revealing AUROC values ranging from 0.63 to 0.87 for all biomarkers (Figures 1 and 2). Plasma p-tau-217 far outperformed all other biomarkers with an AUROC of 0.87, as all other markers were 0.75 or lower. These results supported integrating p-tau-217 but not other biomarkers into CAPS Plus. A p-tau-217 cut-off value was generated from the ROC using Youden’s index. The optimum cut-off was determined to be >0.698 pg/mL, indicating a positive value. This cut-off had a sensitivity of 92% (75–98) and a specificity of 74% (51–88) with a Youden index of 0.66.
Plasma biomarkers discriminating participants by amyloid positivity. Amyloid negative (A−) n = 19, amyloid positive (A+) n = 25. (A–F) Concentrations of plasma Aβ42/40, p-tau-181, p-tau-217, NfL, GFAP and TDP-43 dichotomized by amyloid positivity. Comparison done by Mann–Whitney U test. *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001, ****p ≤ 0.0001.

Receiver operating characteristic curves for plasma biomarkers discriminating amyloid-positive and amyloid-negative participants. Area under the receiver operating curve for each biomarker listed in the legend.

CAPS Plus
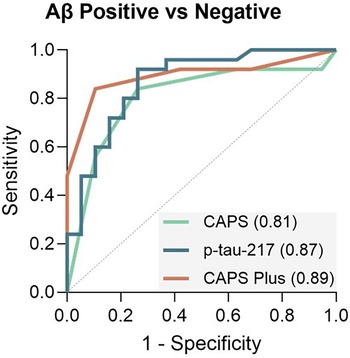
CAPS Plus utilizes the same base framework as the original CAPS scoring system that adds points for higher NPI-Q scores, rapid cognitive decline determined by MMSE decrease and lower Fazekas score. The calculation in CAPS Plus includes 1 point for patients whose plasma p-tau-217 is greater than 0.698 pg/mL (Table 2). Utilizing this new framework, the cut-off for CAPS Plus was a score of 4 or more, which is increased from the original CAPS cut-off at 3 or more. When CAPS Plus was applied to this cohort, it accurately classified the Aβ status of n = 39/44 patients (89%), with 2 false positives and 4 false negatives (Table 2, Figures 3 and 4). Of the false negatives, n = 2 participants had a CAPS Plus score of 1, and n = 2 had a score of 3. The n = 2 participants with false positives both had CAPS Plus scores of 3. In this cohort, CAPS Plus had a sensitivity of 84%, specificity of 89%, positive predictive value (PPV) of 91% and negative predictive value (NPV) of 81%. We further compared how CAPS Plus improves upon the original CAPS and plasma p-tau-217 using ROC analysis (Figure 4). Here we observed that CAPS Plus had an AUROC of 0.89, which is higher than either the original CAPS (0.81) or p-tau-217 alone (0.87). When comparing ROCs, we found that CAPS Plus was a significant improvement over CAPS (p = 0.0028). While we found the CAPS Plus ROC was not significantly different from the p-tau-217 ROC (p = 0.7408), we also found that p-tau-217 alone did not have an improved ROC over the original CAPS either (p = 0.5204). We also assessed the individual sensitivity, specificity, PPV and NPV of CAPS, CAPS Plus and plasma p-tau-217 (Supplemental Table 2). We found that the addition of plasma p-tau-217 improved the specificity of CAPS Plus over the original CAPS as well as p-tau-217 alone. Finally, CAPS Plus had the greatest PPV at 91%.
Histogram of participant CAPS Plus scores, with a score of 4 or more being positive for a high probability of being amyloid positive. Color coding based on amyloid positivity from PET or CSF. Striped pattern indicates those misclassified by the CAPS Plus test.

Receiver operating characteristic curves for CAPS discriminating amyloid-positive and amyloid-negative participants. The figure shows the AUROC for the original CAPS, plasma p-tau-217 and their combination in CAPS Plus.

Clinical β-Amyloid Positivity Prediction Score (CAPS) Plus scoring and performance. Scoring parameters indicate how the CAPS Plus score is generated from a set of variables based on patient status. Those considered positive on CAPS Plus will have a final score of 4 or more to indicate a high probability of amyloid positivity. Test performance indicates how participants were classified based on their amyloid status determined by PET or CSF and measures of validity

Note: NPI-Q = Neuropsychiatric Inventory–Questionnaire; MMSE = mini-mental state examination; PPV = positive predictive value; NPV = negative predictive value.
When investigating those participants who had discordant results, false positives and false negatives, we found that the original CAPS scores would have also misclassified these individuals (Supplemental Table 3). However, for all discordant participants, plasma p-tau-217 alone would have correctly classified these participants’ Aβ status. False-positive participants both had dementia and discordant results for all metrics of the original CAPS framework. Of the false negatives, n = 3/4 had MCI, and n = 1 had dementia. All participants had a CAPS score of 1 (n = 1) or 0 (n = 3) from the NPI-Q, indicating the most discordance here. MMSE decline and Fazekas score were discordant in half of the participants.
Discussion
This study investigated integrating blood-based biomarkers into a previously developed clinical diagnostic tool, CAPS, to classify amyloid positivity. Reference Lahiri, Seixas-Lima and Roncero8 We assessed multiple plasma biomarkers of AD and other dementias, including Aβ42/40, p-tau-181, p-tau-217, NfL, GFAP and TDP-43, for their utility to improve detection of Aβ positivity. Though p-tau-181, GFAP and NfL all showed some ability to differentiate Aβ+ and Aβ−, p-tau-217 significantly outperformed these markers with the highest AUROC of 0.87. Thus, plasma p-tau-217 was selected as the biomarker to be integrated into CAPS to create CAPS Plus. CAPS Plus is a scoring system for the detection of participants with a high likelihood of being Aβ+. It utilizes the NPI-Q, adding 1 point for those with a score of 1 and 2 points for those with a score of ≥2; cognitive decline on MMSE, adding 1 point for a yearly decrease of >2; the Fazekas score, adding 1 point for those with a score <2; and plasma p-tau-217, adding 1 point for those with a positive value. CAPS Plus has a maximum score of 5, with a positive score for Aβ positivity being ≥4.
CAPS Plus improves CAPS specificity
CAPS Plus constitutes a significant advancement over the original CAPS model by notably improving specificity (89% vs 80%) without materially compromising sensitivity (84% vs 89.2%). This enhancement results in a lower false-positive rate, thereby increasing diagnostic precision in identifying individuals with underlying amyloid pathology. Although the gain in area under the curve (AUC) over CAPS alone is modest (0.89 vs 0.86), the marked improvement in specificity represents a clinically meaningful advancement, improving the confidence that those with a positive test have a higher probability of truly being Aβ+. Moreover, CAPS Plus showed enhanced specificity in our cohort when test metrics were compared with p-tau-217 alone. While p-tau-217, on its own, has very high sensitivity, specificity remains below 75%. Reduced specificity implies an increased likelihood of false-positive classifications, which may limit its utility in clinical contexts where diagnostic precision is critical, given the potential toxicity associated with the anti-Aβ agents. Combining CAPS and p-tau-217, referred to as CAPS Plus, significantly improved specificity without greatly reducing sensitivity (see Supplemental Table 2). Integrating plasma p-tau 217 into the CAPS framework achieves this performance gain through a minimally invasive blood draw, avoiding the procedural risks associated with CSF analysis and at a fraction of the cost and complexity of amyloid PET imaging. Importantly, the addition of p-tau-217 to cognitive and imaging factors produces a synergistic effect over and above the clinical model of CAPS, with the combined model emerging as a highly promising predictor of Aβ-positivity. Thus, CAPS Plus offers a practical, scalable solution for enhancing early AD detection in both clinical and research settings.
One key reason for the superior performance of CAPS Plus is the incorporation of plasma p-tau-217, an exceptionally strong biomarker for Alzheimer’s pathology. Recent studies have shown that plasma p-tau-217 can differentiate AD from other neurodegenerative conditions with an accuracy comparable to CSF measures and PET imaging. Reference Khalafi, Dartora and McIntire12,Reference Ashton, Brum and Di Molfetta17,Reference Warmenhoven, Salvadó and Janelidze18 A very recent study demonstrated excellent correlation with brain autopsy. Reference Mammel, Hsiung and Mousavi10 Plasma p-tau-217 demonstrates diagnostic accuracy with AUC values exceeding 0.90 in some cohorts, Reference Santos, Mattos and Pinheiro11 highlighting its robust ability to reflect tau pathology Reference Ossenkoppele, Reimand and Smith19 and amyloid deposition. Reference Palmqvist, Janelidze and Quiroz20 By leveraging p-tau-217, CAPS Plus can capture early biological changes in Alzheimer’s, even before substantial cognitive decline in some cases, positioning it as a critical tool for proactive disease management with anti-amyloid agents.
Clinical utility of CAPS Plus
CAPS Plus can be optimally applied in clinical settings where there is suspicion of early AD, but definitive diagnosis remains unclear. When determining use cases where CAPS Plus may be best applied, we can look at discordant participants detected using CAPS (Supplemental Table 2). Both false-positive participants had dementia and discordant results for all metrics of the original CAPS framework. This may indicate that those in more advanced disease stages and low cerebrovascular burden may not be the best use cases for this tool. Of the four participants with false negatives, n = 3 (75%) had MCI, and the most common discordant result came from the NPI-Q score. This suggests that those in the earliest disease stages with minimal clinical symptoms may not reach the threshold of pathological burden, manifesting the symptoms required for this tool. In these cases, a purely biological tool, such as a PET scan or CSF analysis, may be better for detecting amyloid burden. Reference Palmqvist, Zetterberg and Mattsson21 Ideal use cases for CAPS Plus would be mild cognitive impairment (MCI) and mild dementia, as the scoring scheme was originally developed on these two cohorts. CAPS Plus is also highly relevant for pre-screening candidates for clinical trials that target early or preclinical AD, helping to enrich trial populations with individuals at true biological risk. CAPS Plus can guide physicians in recommending further confirmatory diagnostics, such as amyloid PET scans or CSF studies, and can facilitate earlier initiation of disease-modifying therapies in appropriate circumstances. With an enhanced specificity, CAPS Plus aims to reduce false positives compared to CAPS, potentially saving costs and avoiding unnecessary investigations.
While recent algorithms such as PrecivityAD2 (p-tau217 + Aβ42/40) have achieved excellent performance in large-scale cohorts (AUC ∼ 0.94), Reference Meyer, Kirmess and Eastwood7 CAPS Plus differentiates itself conceptually – namely, by embedding plasma biomarkers within a clinical framework to reduce misinterpretation and improve specificity. In summary, CAPS Plus is complementary to blood-only assays, particularly in healthcare systems where blood biomarkers are not yet fully standardized or widely accessible.
CAPS Plus variants
We have explored two different variants of CAPS Plus in this current work. First, following the original CAPS framework, we added the medial temporal atrophy score (MTAS) into CAPS Plus to create CAPS Plus MT. Here, participants received a score of 1 on CAPS Plus MT if they had an MTAS of ≥2, and a CAPS Plus MT score of ≥4 was used to indicate a high probability of amyloid pathology (Supplemental Table 4). We found CAPS Plus MT underperformed compared to CAPS Plus due to a lower specificity (84%).
Since CAPS Plus requires longitudinal observations, which may sometimes not be available in real-world settings, the second CAPS Plus variant we explored was a baseline variant (CAPS Plus BL) that uses baseline MMSE score rather than loss per year. Here, participants received a score of 1 on CAPS Plus BL if they had a baseline MMSE of <25, and a CAPS Plus BL score of ≥4 was used to indicate a high probability of amyloid pathology (Supplemental Table 5). Although this measure also underperformed on sensitivity (80%) compared to CAPS Plus, it could be used as a suitable alternative when longitudinal data are unavailable.
Limitations
Despite its promise, CAPS Plus requires further validation before widespread clinical adoption. Current data derive from relatively small and selectively recruited samples from a tertiary care memory clinic, often enriched for individuals with high baseline risk of AD. As such, generalizability to broader, more heterogeneous populations remains to be confirmed. Large-scale, prospective studies across diverse clinical and demographic groups are essential to fully establish its utility and cost-effectiveness in real-world settings. The authors are currently in the process of validating these results in a larger Canadian cohort of subjects with neurodegeneration, COMPASS-ND. Reference Chertkow, Borrie and Whitehead22 In this cohort, we had a limited sample size to test combinations of biomarkers, leading us to the chose to include p-tau-217 alone as the top-performing marker. However, as other studies have shown the utility of using multiple biomarker measures, such as adding Aβ42/40 along with p-tau-217, validation in future cohorts should include testing additional biomarker combinations. Reference Meyer, Kirmess and Eastwood7 It is also worth noting that the current CAPS Plus framework uses fixed weights for each component. Future studies with larger numbers could explore data-driven weighting (e.g., logistic regression coefficients, penalized regression or machine learning approaches). This would help determine if greater weighting of p-tau 217 and less of Fazekas can further improve discrimination.
Another limitation to the adoption of CAPS Plus is the standardization of plasma p-tau-217 measurements. As the assay utilized in this study is research use only, some lot-to-lot variability can be expected, and data harmonization may be required to ensure the accuracy of cut-offs developed from a single lot. The development of reference standards and improved assay robustness will be important advancements for the implementation of blood biomarker-based clinical tools.
Conclusion
CAPS Plus is potentially a useful screening tool for enrollment in anti-Aβ treatment programs and clinical trials for AD, specifically addressing people with prodromal and mild AD. The recent approval of lecanemab for clinical use in Canada has heightened the demand for Aβ pre-screening tools in clinical practice. Adding p-tau-217 to CAPS can improve the specificity of predicting Aβ status, especially in subjects with a borderline negative CAP Score. While p-tau-217 alone has a high accuracy in Aβ+ predictivity, CAPS Plus can potentially anchor this powerful blood-based biomarker to the right clinical context.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2026.10530.
Acknowledgments
This present work has been presented at the annual meeting of Clinical Trials on Alzheimer’s Disease (CTAD) in Madrid, Spain (2024), and the Alzheimer’s Association International Conference in Toronto, Canada (2025). We would like to express our sincere gratitude to the patients and their families for helping us complete this work. We are also deeply thankful to each member of the Clinical Trials Unit at Baycrest Academy for Research and Education’s Rotman Research Institute for their unwavering support in conducting this research. For this project, J Cooper was supported by an Alzheimer’s Society of Canada Doctoral award.
Author contributions
Conceptualization: DL, JC, HC, CW. Methodology: DL, JC, HC, CW. Formal analysis: JC, CW. Investigation: DL, JC, BSL, CR. Data curation: DL, JC. Writing – original draft: DL, JC. Writing – review & editing: BSL, CR, HC, CW. Supervision: HC, CW. Funding acquisition: HC, CW.
Funding statement
D Lahiri received funding support from the Sandra Black Award for Clinical Dementia Research (TDRA) for this work. H Chertkow has received partial support through a Canadian Institutes for Health Research (CIHR) grant for this work. C Wellington received partial support from CIHR (grant 451972) for this work.
Competing interests
Dr Howard Chertkow is supported by a Chair in Cognitive Neurology and Innovation from the Baycrest Academy for Research and Education, Baycrest Health Sciences, Toronto. Dr Chertkow has been supported by a Foundation Grant from the CIHR, along with operating funds from the Weston Foundation, Weston Brain Institute and the National Institute of Health (USA) ([Aging Research] – Phase II clinical trial of transcranial direct current stimulation in the treatment of primary progressive aphasia – 1R01AG075111-01A1). Dr Chertkow has participated as a site PI in the past five years for pharmaceutical clinical trial activities sponsored by the following companies: Hoffmann-La Roche Limited, TauRx, Eli Lilly Corp., Anavex Life Sciences, Alector LLC, Biogen MA Inc., IntelGenX Corp. and Immunocal. Dr Chertkow participated as an unpaid advisor in 2020 for the establishment of an international database by Biogen. Dr Chertkow has received honoraria for sitting on advisory boards for Eisai, Biogen and Lilly Inc. in Canada. Dr Chertkow is Scientific Director (unpaid) for the Canadian Consortium on Neurodegeneration in Aging, which receives funding from the CIHR, along with partner support from a set of partners including not-for-profit organizations: Brain Canada, Alzheimer Society of Canada, Womens Brain Health Initiative, Picov Family Foundation, New Brunswick Health Research Foundation, Saskatchewan Health Research Foundation and Ontario Brain Institute. Dr Lahiri has served on a paid advisory board for Eisai. The other authors declare no conflicts of interest related to this work.
Ethical standard
This study was ethically approved by the Rotman Research Institute Ethics Board (22–04) and the University of British Columbia Clinical Research Ethics Board (H22-02802). Written informed consent was obtained from all the participants in the study.







 Open access
Open access