


Neurodivergent conditions such as autism, attention-deficit hyperactivity disorder (ADHD), dyslexia, dyspraxia, dyscalculia, Tourette syndrome and auditory processing disorder and their impact on healthcare delivery are increasingly recognised. Reference Apperly, Lee, van der Kleij and Devine1 In the UK, the prevalence of autism is estimated to be about 2%, and ADHD affects an estimated 2–4% of the population. Reference Morris2 Dyslexia affects around 10% of the population, followed by dyspraxia and dyscalculia, each at 5–6%. 3 Tourette syndrome and auditory processing disorder have a prevalence of approximately 1% and 2–7% respectively. Reference Stern, Burza and Robertson4,Reference Drosos, Papanicolaou, Voniati, Panayidou and Thodi5
Studies indicate a significant overlap between neurodivergent conditions and other neuropsychiatric diagnoses. There is a high prevalence of co-occurring autism in functional neurological disorder (FND), estimated at around 10%. Reference Tamilson, Poole and Agrawal6 A study by Cole et al found that 17.6% of individuals with FND exhibited traits of autism spectrum disorder (ASD) based on a self-reported screening tool. Reference Cole, Elmalem and Petrochilos7 Similarly, a meta-analysis reported the pooled prevalence of autism to be 6.3% among individuals with epilepsy, Reference Strasser, Downes, Kung, Cross and De Haan8 and another meta-analysis found the prevalence of ADHD in people with epilepsy to be 30.7%. Reference He, Yang, Li, Zhao, Li and Li9 Research by Chang et al demonstrated an increased prevalence of ADHD and ASD in individuals who had experienced traumatic brain injury at a young age. Reference Chang, Wu, Huang, Chang, Bai and Chen10 Furthermore, a meta-analysis by Pan et al revealed that individuals with autism were significantly more likely than the general population to present with conditions such as epilepsy and other abnormalities of the nervous system. Reference Pan, Bolte, Kaur, Jamil and Jonsson11 A study by Adeyemo et al highlighted a significant association between mild traumatic brain injury and ADHD. Reference Adeyemo, Biederman, Zafonte, Kagan, Spencer and Uchida12 It is also important to note that many neurological conditions can mimic ADHD symptoms or ASD traits, complicating diagnosis and management.
Understanding the co-occurrence of neurodivergent conditions in neuropsychiatric patients is important. Recognising these overlaps can have significant implications for both the diagnosis and management of neuropsychiatric conditions. Our study, conducted as part of a quality improvement project, aims to investigate the co-occurrence of these conditions to enhance early identification and implement more inclusive, tailored treatment approaches. Additionally, this exploration may shed light on potential shared aetiological pathways or neurobiological mechanisms.
Method
Study design and setting
We conducted a descriptive quantitative cross-sectional study at a tertiary regional neuropsychiatric out-patient clinic based in London, UK. The centre serves a population of approximately 3.2 million people across the south west London and Surrey regions. The median age of this population is ∼40 years. In terms of ethnicity, approximately 75% are White, 9% Asian, 8% Black and 8% Mixed or Other ethnic backgrounds. Referrals to the centre are received not only from neurologists and secondary mental health services, but also from primary care clinicians. Therefore, the sampling frame can be considered broadly representative of the general neuropsychiatric population in the UK. The study targeted every consecutive patient who was seen by the clinicians in the centre over a 6-month period starting in February 2024.
Participants
A total of 166 patients attending the clinic during the study period agreed to participate. All patients were considered eligible if they had the ability to complete the questionnaires and the capacity to consent to the study.
Data collection and instruments
Data collection involved basic demographic information (age, gender, ethnicity), clinical details and responses to two main questionnaires: the Comprehensive Autistic Trait Inventory (CATI) and the Adult ADHD Self-Report Scale, version 1.1 (ASRS-v1.1). Clinical information included history and family background of neurodivergent conditions such as ASD and ADHD, along with primary neurological conditions and psychiatric comorbidities for which they were referred to the neuropsychiatric clinic.
Comprehensive Autistic Trait Inventory
The CATI is a self-report questionnaire designed to measure autistic traits across six dimensions: social interactions; communication; social camouflage; repetitive behaviours; cognitive rigidity; and sensory sensitivity. It contains 42 items and provides a total-scale score as well as six subscale scores. A total-scale score of 134 or above (out of 210) is considered above the threshold for clinically significant autistic traits. Reference English, Gignac, Visser, Whitehouse, Enns and Maybery13
Adult ADHD Self-Report Scale, version 1.1
Developed in conjunction with the World Health Organization and the Workgroup on Adult ADHD, the ASRS-v1.1 includes 18 questions based on DSM-IV-TR criteria, with the first six questions (Part A) forming the basis for the ASRS Screener. If a person scores 14 or above on Part A, their symptom profile strongly suggests a likelihood of an ADHD diagnosis. Reference Lewczuk, Marcowski, Wizla, Gola, Nagy and Koos14
Data collection procedure
Questionnaires were distributed both electronically via email and in paper form during clinic visits, depending on the patient’s preference. Data collected on paper forms was manually entered into the Research Electronic Data Capture (REDCap) system. All data were stored securely within the South West London and St George’s Mental Health NHS Trust computer system, safeguarded by passwords and without personal identifying details.
Informed consent and ethical considerations
Although formal ethical approval was not required as the study is part of a quality improvement project, comprehensive participant information sheets were provided prior to obtaining written consent. These sheets detailed the study’s purpose, potential personal impacts and data dissemination plans, emphasising the anonymity of published data. Participation was entirely voluntary and patients were free to decline without any effect on their care or treatment. Our study complies with the UK Policy Framework for Health and Social Care Research and adheres to the principles of the Declaration of Helsinki (1975, revised 2013).
Data management and data analysis
Data were managed in compliance with the General Data Protection Regulation and the Caldicott Principles regarding identifiable information. Analysis involved calculating individual scores from the CATI and ASRS, collating these scores along with other data on an Excel spreadsheet. The primary focus was on assessing the prevalence of neurodivergent conditions and traits. Analyses were conducted using IBM SPSS Statistics for Windows version 27 (IBM Corp., Armonk, New York, USA).
The reliability of the CATI and ASRS questionnaires within our cohort was evaluated using Cronbach’s α to ensure consistent item scoring. The distributions of total scores from these questionnaires were assessed for normality. Chi-squared tests were used to examine the relationships between diagnoses of FND and epilepsy, and those of ASD/ADHD, including suspected undiagnosed cases and familial histories of ASD/ADHD. Additionally, independent samples t-tests were conducted to compare the CATI and ASRS scores across groups where indicated. One-way analysis of variance (ANOVA) was employed for the analysis of subgroups. Furthermore, Pearson correlation coefficients were calculated to determine the relationship between scores on the CATI and ASRS.
Results
A total of 166 individuals were initially enrolled in the study. Of these, 87 were classified as questionnaire non-responders: 73 did not respond at all and 14 provided incomplete responses. As a result, 79 participants successfully completed all required questionnaires and were included in the final analysis.
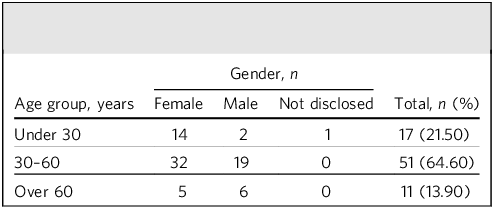
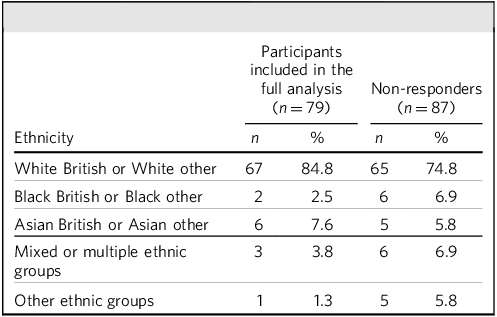
The demographic profile of the 79 participants exhibited considerable diversity in terms of gender, age and ethnic backgrounds (Tables 1 and 2), reflecting the broader population served by the neuropsychiatric clinic. The gender distribution was predominantly female (64.6%). Regarding age, the majority of participants (64.6%) were middle-aged, falling within the 30–60 years age range; 21.5% were under 30 years old and 13.9% over 60. The mean age of the participants was approximately 40.6 years (s.d. = 13.8 years). Ethnic representation in the cohort was predominantly White British or White Other backgrounds, comprising 84.8% of the sample.
Age and gender distribution of participants included in the full analysis (n = 79)

Ethnic background distribution of all participants

Among the non-responders, there were 58 females and 29 males. The mean age of this group was 42.2 years. In terms of ethnicity, 74.7% identified as White British or White Other.
Psychiatric comorbidities
In our cohort of 79 individuals, 26.6% (n = 21) were diagnosed with anxiety disorders, 25.3% (n = 20) with depressive disorders and 11.4% (n = 9) with mixed anxiety and depressive disorders. Additionally, 2.5% (n = 2) had bipolar affective disorder, 12.7% (n = 10) had post-traumatic stress disorder, 3.8% (n = 3) had eating disorders, 1.3% (n = 1) had obsessive–compulsive disorder, 12.7% (n = 10) had personality disorders and 1.3% (n = 1) had substance use disorder. Notably, no participants were diagnosed with psychosis, schizophrenia or schizoaffective disorder.
Neurodivergent conditions
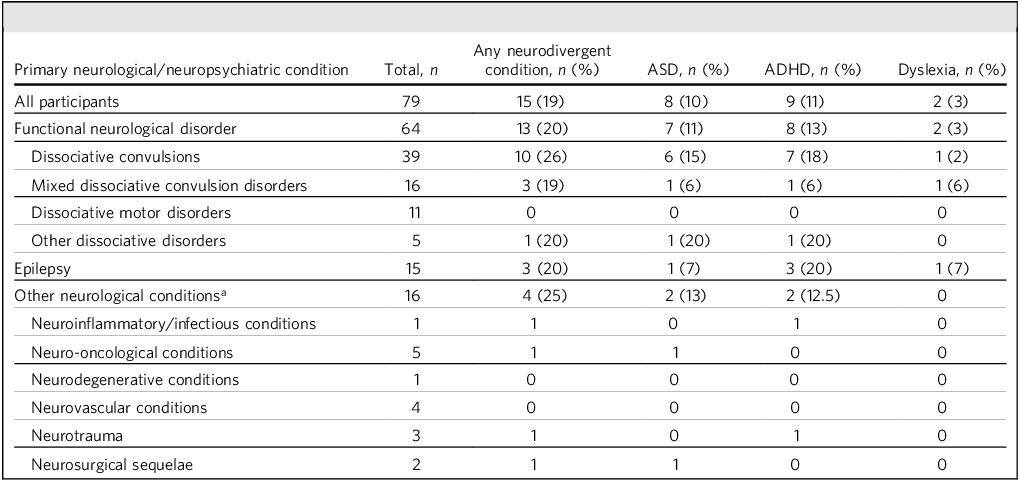
In our cohort, we observed varying prevalences of neurodivergent conditions across specific neurological/neuropsychiatric conditions. ASD was identified in 10% of participants, ADHD in 11% and dyslexia in 3% (Table 3). No other neurodivergent conditions were reported. Among the 64 individuals with FND, 11% were diagnosed with ASD, 13% with ADHD and 3% with dyslexia. Epilepsy was noted in 15 of the FND group, of whom 20% also had ASD, 20% ADHD and 7% dyslexia. Among the 16 individuals assessed for other neurological conditions, ASD was present in 25%, ADHD in 13% and dyslexia in 12.5%.
Neurodivergent conditions and neurological conditions of participants included in the full analysis

ASD, autism spectrum disorder; ADHD, attention-deficit hyperactive disorder.
a. The following conditions were not reported: dyspraxia; dyscalculia; Tourette syndrome; auditory processing disorder.
Among the non-responders, based on clinical records, 62 had a diagnosis of FND, 19 had epilepsy and 21 had other neurological conditions. Additionally, five individuals had a diagnosis of ASD and four had ADHD.
Family history and suspected undiagnosed ASD/ADHD
We found that 17% of participants with FND (n = 64) reported potential/suspected undiagnosed ASD, and 25% suspected they might have ADHD (Fig. 1). Furthermore, 27% of participants with FND noted a family history of ASD or ADHD among first-degree relatives. Analysis of specific FND categories showed varying prevalences. Epilepsy and other neurological conditions show the lowest percentages. Full descriptive details for each diagnostic category are presented in Fig. 1.
Family history and suspected undiagnosed autism spectrum disorder (ASD) and attention-deficit hyperactivity disorder (ADHD). Data are shown for the full analysis sample (n = 79).

ASD and ADHD trait screening questionnaires
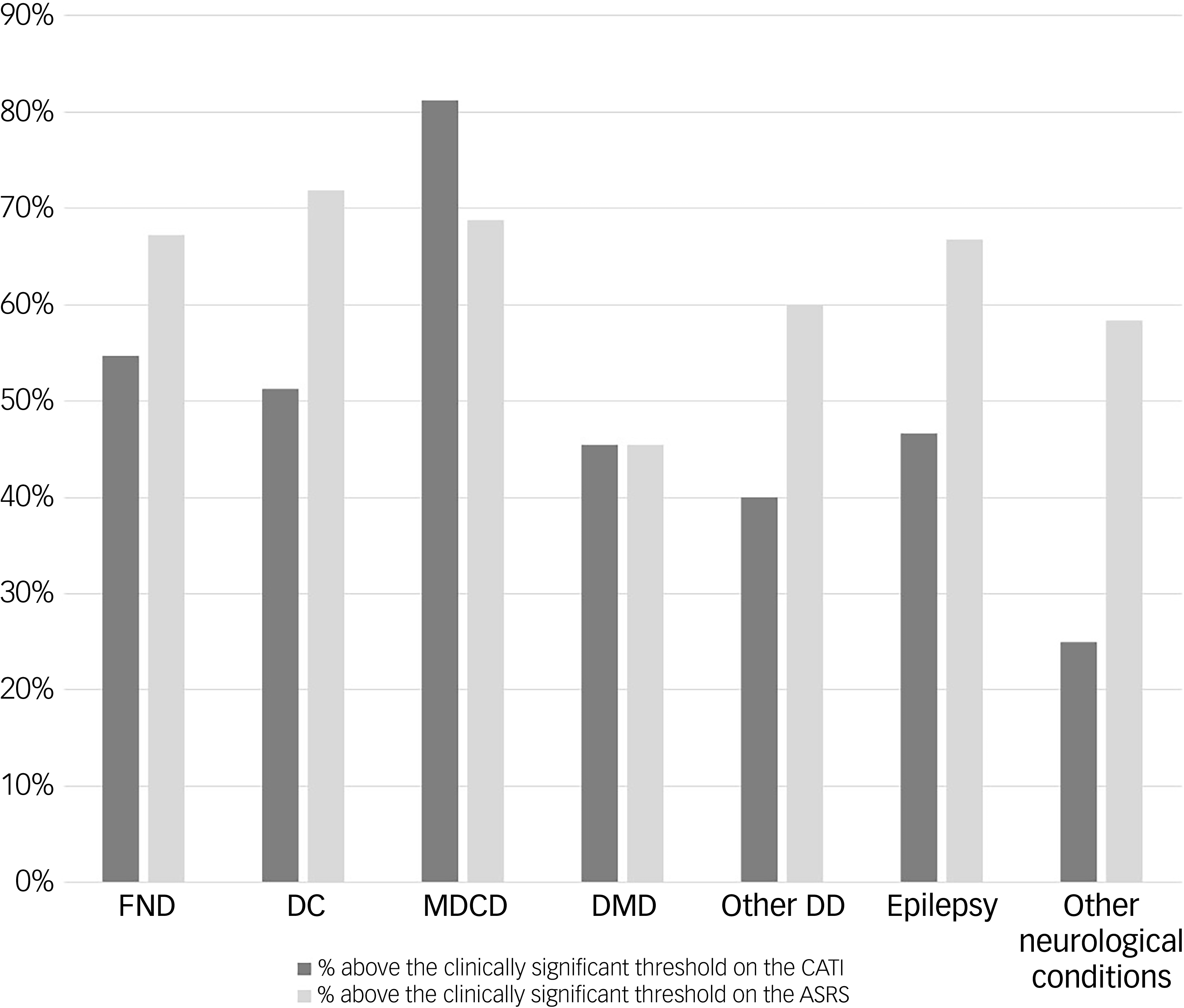
Figure 2 shows percentages of participants meeting clinical significance thresholds on the CATI and ASRS Part A for various neurological conditions. For participants with FND, 54.69% met the CATI threshold and 67.2% met the ASRS threshold. For those with dissociative convulsions, 51.28% and 71.8% met CATI and ASRS thresholds respectively. For epilepsy, 46.67% and 66.7% met CATI and ASRS thresholds respectively. Participants in the ‘Other neurological conditions’ category had the lowest rates, at 25% for the CATI and 58.3% for the ASRS.
Participants (n = 79) meeting clinical significance thresholds on the Comprehensive Autistic Trait Inventory (CATI) and Adult ADHD Self-Report Scale (ASRS) Part A for various neurological conditions. FND, functional neurological disorder; DC, dissociative convulsions; MDCD, mixed dissociative convulsion disorders; DMD, dissociative motor disorder; Other DD, other dissociative disorder.

Figure 3 illustrates the relationship between CATI total scores and ASRS Part A scores, stratified by FND diagnosis. A positive correlation is visible, with higher CATI scores often aligning with higher ASRS scores, although there is considerable variability. The data are divided by FND diagnosis, revealing greater score variability among individuals with FND, particularly for ASRS scores. In contrast, individuals without FND cluster in lower ASRS scores but span a range of CATI scores.
Scatter plot of Comprehensive Autistic Trait Inventory (CATI) total score by Adult ADHD Self-Report Scale (ASRS) Part A score by functional neurological disorder (FND) diagnosis. Threshold lines at CATI total score = 134 and ASRS Part A score = 14 highlight clinical cut-offs.

Statistical analysis
The Cronbach’s α for the 18-item ASRS is 0.902, indicating excellent reliability and strong internal consistency. The CATI scale’s 42 items have a Cronbach’s α of 0.937, also reflecting excellent reliability and high consistency in measuring the same construct. Normality tests for the CATI and ASRS scores using the Kolmogorov–Smirnov and Shapiro–Wilk tests yielded p-values of 0.200 and 0.091 for the CATI, and 0.200 and 0.743 for the ASRS, respectively. None of these results are statistically significant, indicating that the data are normally distributed.
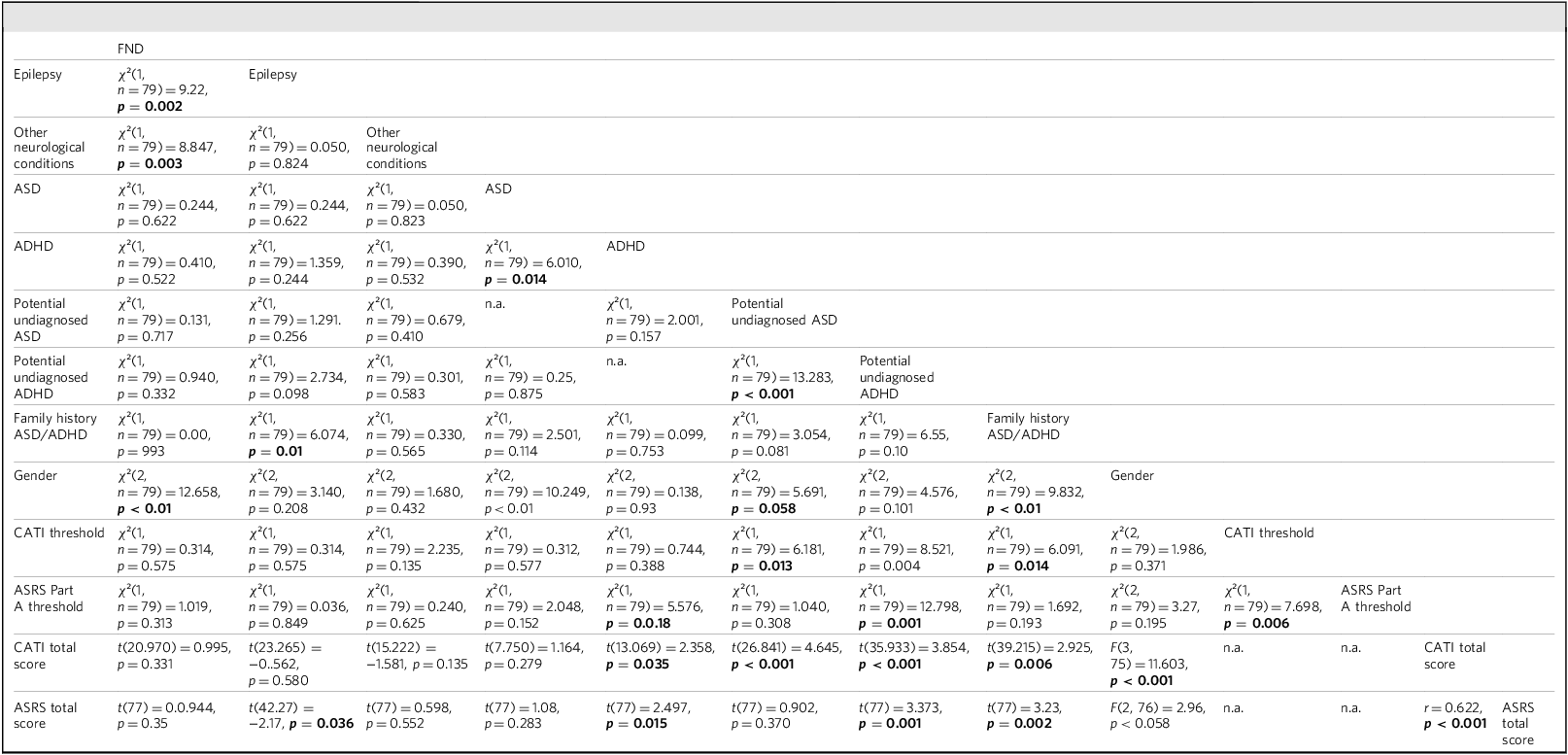
Chi-squared tests revealed (Table 4) that gender was strongly associated with formal ASD diagnoses (χ 2 = 10.249, p < 0.01), the presence of ASD/ADHD in first-degree relatives (χ² = 9.832, p < 0.01) and FND (χ² = 12.658, p < 0.01). Significant relationships were also observed between formal ASD and ADHD diagnoses (χ² = 6.010, p = 0.014) and between suspected undiagnosed ASD and ADHD (χ² = 13.283, p < 0.001). Suspected undiagnosed ASD was significantly linked to the CATI threshold (χ² = 6.181, p = 0.013), and suspected undiagnosed ADHD showed associations with both family history of ASD/ADHD in first-degree relatives (χ² = 6.550, p = 0.010) and the CATI threshold (χ² = 8.521, p = 0.004). Furthermore, undiagnosed ADHD demonstrated significant relationships with the ASRS Part A threshold (χ² = 12.798, p = 0.001), and formal ADHD diagnoses were also related to this threshold (χ² = 5.576, p = 0.018) as expected. Notably, gender differences approached significance for undiagnosed ASD (χ² = 5.691, p = 0.058).
Results matrix of various statistical analyses between categorical and continuous variables

FND, functional neurological disorder; ASD, autism spectrum disorder; ADHD, attention-deficit hyperactive disorder; CATI, Comprehensive Autistic Trait Inventory; ASRS, Adult ADHD Self-Report Scale.
χ², chi-squared test; t, independent samples t-test; F, one-way analysis of variance; r, Pearson’s correlation analysis. Significant results are shown in bold.
The independent samples t-tests (Welch’s) revealed that for individuals with a formal diagnosis of ADHD, the diagnosed group scored higher (mean = 151.67, s.d. = 24.63) on the CATI compared with those without a diagnosis (mean 129.73, s.d. = 36.61; t(13.07) = 2.36, p = 0.035), with a medium effect size (Cohen’s d = 0.617). Similarly, those with suspected undiagnosed ADHD scored significantly higher (mean 155.61, s.d. = 27.17) than their counterparts (mean 125.33, s.d. = 35.56, t(35.93) = 3.85, p < 0.001), showing a large effect size (Cohen’s d = 0.894). For individuals with suspected undiagnosed ASD, scores were notably higher (mean 161.08, s.d. = 21.64) than those without (mean 126.55, s.d. = 35.65; t(26.84) = 4.65, p < 0.001), with a large effect size (Cohen’s d = 1.020). Participants with a family history of ASD/ADHD also scored higher (mean 150.19, s.d. = 31.84) than those without (mean 125.72, s.d. = 35.46; t(39.22) = 2.93, p = 0.006), with a medium effect size (Cohen’s d = 0.708). Non-significant differences were found for FND (t(20.97) = 0.999, p = 0.331), epilepsy (t(23.27) = −0.56, p = 0.580) and ‘other neurological conditions’ (t(15.22) = −1.579, p = 0.135), with small or negligible effect sizes (Cohen’s d = 0.287, −0.149 and −0.495 respectively).
One-way ANOVA revealed significant gender differences for CATI scores; the gender effect was moderate, explaining 31.7% of the variance (F = 11.603, p < 0.001, η² = 0.317), with a sum of squares of 32068.155. Pearson’s correlations analysis shows a moderate positive correlation (0.622) between ASRS total score and CATI total score, indicating that as one score increases, the other tends to increase as well. This correlation is statistically significant (p < 0.001). The 95% confidence interval for this correlation ranges from 0.464 to 0.740, affirming the strength and consistency of the relationship between these scores.
Discussion
Our study explored the prevalence of ASD and ADHD traits in neuropsychiatric patient groups. Our examination of neurological conditions was mainly related to FND, epilepsy and a broader category of other neurological conditions because of data limitations. We discuss our findings in relation to existing literature.
Prevalence of neurodivergent conditions/traits across groups
In our cohort (n = 79), we observed varying prevalence rates of neurodivergent conditions across specific disorders. ASD was identified in 10% of the cohort, ADHD in 11% and dyslexia in 3%. Among the 64 individuals with FND, 11% were diagnosed with ASD, a finding consistent with the meta-analysis by Tamilson et al (2025) on the co-occurrence of ASD and FND. Reference Tamilson, Poole and Agrawal6 Of the participants with FND, 13% had an established ADHD diagnosis, a rate that does not differ from published literature. A literature review by Staunton et al (2024) reported an ADHD prevalence ranging from 7 to 56%, depending on the type of FND and whether the studies assessed confirmed diagnoses or ADHD-related traits. Reference Staunton and Rathnaiah15
Of our participants with a diagnosis of epilepsy (n = 15), 7% had ASD and 20% had ADHD. A meta-analysis by Liu et al reports that 1 in 10 autistic individuals have co-occurring epilepsy. Reference Liu, Sun, Sun, Zou, Chen and Huang16 Additionally, Dunn & Kronenberger reported that ADHD-like symptoms are present in 30%–40% of children with epilepsy. Reference Dunn and Kronenberger17 A meta-analysis by He et al reported an ADHD prevalence of 30.7% in children with epilepsy, Reference He, Yang, Li, Zhao, Li and Li9 and a meta-analysis by Wang et al suggests that ADHD affects 22% of adults with epilepsy. Reference Wang, Yao, Zhang, Xia, Yu and Peng18 This aligns with our findings. The difference in ADHD prevalence between adults and children may be attributed to undiagnosed cases in adults. This might be related to some normative developmental changes in symptoms, considering the age-dependent decline in normative levels of hyperactivity, whereas cut-offs are normed for children and adolescents. Reference Lahey, McBurnett, Biederman, Greenhill, Hynd and Barkley19 Also, only about 15% of those individuals who meet diagnostic criteria in childhood continue to meet strictly defined diagnostic criteria in adulthood, although 65% continue to experience at least some impairing symptoms. Reference Faraone, Biederman and Mick20 In addition, increased awareness in recent years has likely led to higher ADHD diagnosis rates in children compared with the past. In our study, 16% of participants felt they had undiagnosed ASD and 23% believed they had undiagnosed ADHD. These rates were notably higher among individuals with FND than those with epilepsy or other neurological conditions. Specifically, 17% of individuals with FND suspected they had undiagnosed ASD and 25% believed they had undiagnosed ADHD. A significantly higher prevalence of ASD or ADHD among first-degree relatives of individuals with FND and epilepsy has been reported in previous studies. In our study, 27% of participants with FND reported a first-degree family history of ASD or ADHD. Unexpectedly, no participants with epilepsy reported a family history of these conditions, despite existing literature indicating a high familial occurrence. Reference Sundelin, Lichtenstein, Almqvist, Hultman, Tomson and Ludvigsson21 A CATI score above 134 has been validated as the optimal threshold for identifying individuals with significant autistic traits, with 80% of neurotypical individuals in the general population scoring below 134. In our sample, 54.69% of participants with FND and 51.28% of participants with dissociative convulsions (n = 39) met the CATI threshold, indicating a high prevalence of clinically significant symptoms in both groups. An even higher proportion of participants with mixed dissociative convulsion disorder – 81.25% – exceeded the threshold. Of the participants with epilepsy, 46.67% scored above the CATI threshold. Finally, those in the ‘other neurological conditions’ category showed the lowest proportion, with 25% meeting the threshold. Our findings correlate with the higher proportion of suspected undiagnosed ASD in our study sample. Several concepts have been proposed to explain this higher prevalence of co-occurrence, including common neurocognitive differences, vulnerabilities such as trauma, perceptual differences in sensory processing, interoception, alexithymia and theory of mind. Reference Tamilson, Poole and Agrawal6 Additionally, several frameworks proposing shared underlying mechanisms have been suggested to explain this co-occurrence, including the Bayesian hierarchical model proposed by Edwards et al, Reference Edwards, Adams, Brown, Parees and Friston22 differences in sense of agency and the theory of constructed emotions. Reference Tamilson, Poole and Agrawal6,Reference Edwards, Adams, Brown, Parees and Friston22
On the ASRS tool, a score above 14 for Part A has been validated as indicating the presence of clinically significant ADHD traits. In our FND group, 67.2% of individuals scored above this threshold. Among participants with dissociative convulsions, 71.8% scored above the threshold, as did 68.8% of those with mixed dissociative convulsion disorders, 66.7% of those with epilepsy and 58.3% of those with ‘other neurological conditions’. Thus, our findings indicate a remarkably high prevalence of ADHD traits in FND populations. There are no directly comparable studies available, making it difficult to contextualise our results. However, the proportion with ADHD traits observed in our sample appears to be unusually high. Limited data exist on this co-occurrence, and previous studies have not extensively reviewed this relationship. A literature review by Staunton et al reports an increased incidence of comorbid ADHD and FND. Reference Staunton and Rathnaiah15 Anecdotal evidence suggests that treating ADHD with psychostimulants may improve neurological symptoms, but further research is needed to explore this potential link in greater detail.
Overlap between ASD and ADHD traits and gender
Our statistical analysis indicates a strong association between gender and formal ASD diagnoses, the presence of ASD/ADHD in first-degree relatives and functional neurological disorders. Our findings reveal a higher prevalence of ASD diagnoses among females. However, in the general population ASD is generally more prevalent in males. The gender disparity in ASD diagnoses, often attributed to diagnostic biases, has been extensively documented in previous studies. Reference Tamilson, Eccles and Shaw23 Our study also revealed significant relationships between formal ASD and ADHD diagnoses, as well as between potential undiagnosed ASD and ADHD. As expected, suspected undiagnosed ASD was significantly associated with scores above the CATI threshold, and suspected undiagnosed ADHD showed associations with both a family history of ASD/ADHD in first-degree relatives and the CATI threshold score. Furthermore, suspected undiagnosed ADHD demonstrated a significant relationship with the ASRS Part A threshold (χ² = 12.798, p = 0.001). The relationship between ASD and ADHD has been widely studied in the literature. Independent samples t-tests revealed that individuals with a formal ADHD diagnosis scored higher on the CATI compared with those without a diagnosis. Similarly, individuals with potential undiagnosed ADHD scored significantly higher than those without, demonstrating a large effect size. Additionally, individuals with suspected undiagnosed ASD had notably higher scores than those without. Research indicates that 37–85% of autistic individuals meet symptom-based criteria for ADHD, based on questionnaire and clinical rating scale assessments. Reference Eaton, Roarty, Doval, Shetty, Goodall and Rhodes24,Reference Gadow, DeVincent and Pomeroy25 Additionally, approximately 1 in 8 individuals with ADHD also have ASD. Reference Zablotsky, Bramlett and Blumberg26 Therefore, our findings do not present a novel association but rather align with existing research.
One-way ANOVA revealed significant gender differences in CATI scores; the gender effect was moderate. Although ASD is generally more common in males, our study found that female participants were more likely to score high on CATI. This gender influence highlights the issue of missed or misdiagnosed autism in females. Reference Tamilson, Eccles and Shaw23 Pearson’s correlation analysis showed a moderate positive correlation (r = 0.622) between ASRS scores and CATI scores, indicating that as one score increases, the other tends to increase as well. This correlation was statistically significant (p < 0.001) and aligns with the increased prevalence of co-occurring ADHD and ASD reported in the literature. No notable statistically significant associations were found between the subdomains of the CATI or ASRS tools and other variables, including neurological conditions, potential undiagnosed ASD or ADHD, or family history.
Clinical implications and future directions
The significantly higher prevalence of ASD or ADHD conditions or traits in neuropsychiatric patients, particularly those with FND, is striking. This highlights the importance of further research on this topic. These potential links have various implications for the management of neuropsychiatric conditions and service provision. Early identification of co-occurring neurodivergent conditions is crucial, highlighting the need for routine screening for ASD and ADHD among people with FND.
Strengths and limitations
Strengths
This study addresses a clearly defined research question concerning the prevalence of neurodivergence among neuropsychiatric patients. It employed validated instruments (the CATI and ASRS) to assess neurodivergent traits within the sample. A range of statistical analyses were utilised to enhance understanding of the variables studied, adding robustness to the findings.
Limitations
A significant limitation of this study was the high non-response rate, coupled with attrition bias due to incomplete forms/questionnaires. However, there was no significant difference between the profile of participants and non-responders. The analysed sample size was relatively small, which may affect the reliability of the findings. Additionally, the study largely depended on self-reported data for suspected ASD or ADHD, which could introduce discernment bias. The sampling frame was limited to a tertiary neuropsychiatric clinic that treats complex cases, which may limit the generalisability of the results to the broader neuropsychiatric population. However, as the regional service also receives referrals from general practitioners, the study population could still be considered broadly representative of the neuropsychiatric population in the UK. Notably, the study did not include data on conditions such as dyspraxia, dyscalculia or Tourette syndrome, further narrowing the scope of the analysis. Furthermore, the limited number of participants with traumatic brain injury and other neurological conditions restricted the analysis primarily to FND.
About the authors
Andrea De Angelis, Consultant Neuropsychiatrist, Neuropsychiatry Department, Atkinson Morley Regional Neurosciences Centre, St George’s Hospital, London, UK; South West London and St George’s Mental Health NHS Trust, London, UK; and Department of Neuroscience, City St George’s University, London, UK. Grace Fearnehough, ST3, South West London and St George’s Mental Health NHS Trust, London, UK. Bruce Tamilson, Consultant Neuropsychiatrist, Neuropsychiatry Department, Atkinson Morley Regional Neurosciences Centre, St George’s Hospital, London, UK; South West London and St George’s Mental Health NHS Trust, London, UK; Department of Neuroscience, City St George’s University, London, UK; and Division of Psychiatry, University College London, London, UK. Niruj Agrawal, Consultant Neuropsychiatrist, Neuropsychiatry Department, Atkinson Morley Regional Neurosciences Centre, St George’s Hospital, London, UK; South West London and St George’s Mental Health NHS Trust, London, UK; and Department of Neuroscience, City St George’s University, London, UK.
Data availability
The data that support the findings of this study are available from the corresponding author on request.
Acknowledgements
We thank Dr Norman Poole (consultant neuropsychiatrist), Dr Sarah Cope (principal clinical psychologist), Ms Billie James (assistant psychologist), Ms Holly Zephrine (nurse specialist) and all other staff at the Department of Neuropsychiatry, St George’s Hospital, for their valuable contributions and support in facilitating this study.
Author contributions
A.D.A. contributed to conceptualisation, methodology, project administration, data collection and critical review and editing of the manuscript. G.F. contributed to data collection, data curation and critical review and editing of the manuscript. N.A. provided supervision and contributed to critical review and editing of the manuscript. B.T. contributed to conceptualisation, methodology, data collection, data curation, formal analysis, interpretation of results and drafting and revising the manuscript. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
N.A. is a member of the BJPsych Bulletin editorial board and did not take part in the review or decision-making process of this paper.



 Open access
Open access
eLetters
No eLetters have been published for this article.