


Highlights
-
Our systematic literature review gauged the frequency, severity and types of complications as well as treatment failure rates of MME for cSDH.
-
We found that MMAE is generally a safe procedure, with high success rates.
-
Careful, meticulous technique is critical to keep complication rates at a minimum.
Introduction
A chronic subdural hematoma (cSDH) is an organized, encapsulated blood collection in the space between the dura mater and arachnoid mater, that is, the subdural space. There are many risk factors for the development of cSDH, which include trauma, anticoagulation/antiplatelet use, alcohol consumption, liver cirrhosis, chronic renal failure and hematologic disease. Reference Sim, Min, Lee, Kim and Kim1 The incidence of cSDH is significantly higher in the elderly population (>80 years) and has increased in the past years. Reference Rauhala, Helén and Huhtala2,Reference Balser, Farooq, Mehmood, Reyes and Samadani3 The traditional theory was that most cSDHs result from a tear in the bridging veins, which first causes the accumulation of an acute SDH that then becomes chronic over time. However, this theory has been abandoned in recent years, and it has now been established that the driving factor in the formation of cSDH is not venous injury, but rather injury to the cells lining the inner border of dura mater, called the dural border cells. Reference Edlmann, Giorgi-Coll, Whitfield, Carpenter and Hutchinson4 When damaged, they cause an inflammatory reaction, leading to fibrogenesis and neo-angiogenesis. Various inflammatory mediators are recruited to repair these damaged cells as part of the body’s repair mechanism, and new, fragile capillaries are formed to provide blood supply to these neomembranes. These capillaries cause repeated slow, insidious bleeding, thereby feeding the hematoma, causing its re-accumulation and expansion. This in turn perpetuates the inflammatory response and creates a vicious cycle. The main arterial supply to the dura mater is through the middle meningeal artery (MMA). The MMA is also the main feeder of the newly formed fragile leaky capillaries supplying the cSDH neomembranes. Embolization of the MMA interrupts blood supply to these neomembranes, stops the inflammatory cycle, facilitates hematoma resolution and reduces recurrence and progression. Reference Hashimoto, Ohashi and Watanabe5
However, the MMA has many important anastomoses and branches that supply critical structures of the central nervous system, a detailed understanding of which is crucial to avoid complications related to middle meningeal artery embolization (MMAE). The MMA most commonly arises as the first branch of the maxillary artery (a terminal branch of the external carotid artery) and enters the skull via the foramen spinosum. Reference Natali, Reddy and Leo6 However, anatomical variations in its origin are common, including origins from the ophthalmic artery or, less commonly, from the persistent stapedial artery. It gives off the petrosal and cavernous branches, each of which supplies the cavernous sinus, middle fossa floor, trigeminal nerve, Gasserian ganglion, tensor tympani muscle and tympanic cavity and the labyrinthine segment of the facial nerve. Reference Martínez, Domingo and Sattur7 The petrosal branch supplies the facial nerve, and the cavernous branch of the MMA can anastomose with small perforators from the inferolateral trunk of the internal carotid artery. The anterior division may send orbital branches through the superior orbital fissure that anastomose with the recurrent meningeal branch of the ophthalmic artery, and in rare cases, the MMA can also connect to the vertebral artery or posterior inferior cerebellar artery. Reference Shotar, Premat and Lenck8 Lastly, the MMA may also form collaterals with extracranial arteries (e.g., superficial temporal artery). Although this is not so much a risk with regard to non-target embolization, it is nevertheless important to recognize because the presence of such anastomoses, if they are not recognized and occluded, can lead to hematoma recurrence. Reference Geibprasert, Pongpech, Armstrong and Krings9,Reference Tubbs, Walker, Demerdash, Matusz, Loukas and Cohen-Gadol10
Because of this high anatomical variability, pre-procedural imaging, such as CT angiography, can be considered, although its value remains unproven at this point. At the very least, the internal and external carotid artery angiographic runs should be studied carefully for the identification of high-risk anatomy, such as an ophthalmic origin, which might represent a contraindication to embolization. Knowledge and recognition of these variations and their connections are critical for safe and effective results. Reference Shotar, Premat and Lenck8,Reference Pilawska, Dębicka and Krzyżewski11 One series of more than 100 MMAEs identified variant anatomy as one factor associated with increased procedural morbidity, again emphasizing the importance of anatomical familiarity. Reference Martínez, Domingo and Sattur7
In addition to the risks of non-target embolization, cSDH patients are often old and frail, and thus, the risk of complications when performing MMAE for cSDH may be substantial and includes risks related to direct catheter manipulation and embolization, often in an atherosclerotic vascular tree, access complications and “indirect” systemic risks, for example, due to general anesthesia (GA), and fasting and dehydration prior to the procedure.
We performed a comprehensive literature review focusing on complications of MMAE in the setting of cSDH to gauge the frequency, severity and types of complications that have been reported to occur during and shortly before and after this procedure.
Methods
Search strategy
We conducted a systematic review of the literature using PubMed/Medline and Google Scholar as the primary databases to identify studies related to MMAE. The search strategy employed combinations of the keywords “(middle meningeal artery) AND ((embolization) OR (complication)),” “((complication OR side effect OR risk OR adverse event* OR safety) AND (middle meningeal artery))” and “(complication OR side effect OR risk OR adverse event*) AND (middle meningeal artery).”
Inclusion and exclusion criteria
Studies were included if they focused on patients undergoing MMAE for cSDH. Other inclusion criteria included patients aged 18 years or older, studies published within the last 30 years, full-text availability and reported complications. Only studies in English involving human subjects were considered. Exclusion criteria included meta-analyses, reviews, commentaries, conference abstracts and studies without original data on complications. No gray literature sources were included in this review.
Screening process
The initial title and abstract screening was conducted using Covidence by four reviewers (JO, GJ, YS, OB). Articles were included if they involved endovascular treatment of the MMA. During the full-text review, studies were categorized based on the type of disorder treated, creating distinct groups for analysis. The full-text review was performed by 3 reviewers (GJ, YS or OB), and 20 studies were cross-checked by a second reviewer from the same group to ensure accuracy. Another author was consulted in cases of discrepancy (JO).
Data extraction
A data extraction sheet that included key study characteristics, demographics of the study patient samples, treatment-related variables of interest, adjunctive treatments (e.g., MMAE as stand-alone treatment vs. as an adjunct to surgery), frequencies and types of complications and clinical outcomes was developed to ensure a standardized, consistent approach in capturing relevant information across studies.
Statistical analysis
The results of the literature review were summarized using descriptive statistics to provide an overview of the safety and efficacy of MMAE. No meta-analysis was performed due to the heterogeneity of the extracted data.
Frequency of reported complications, their clinical consequences and management strategies were summarized. We categorized complications into (1) procedure-related neurological complications (ischemic events, intracranial hemorrhage, cranial nerve palsy, aphasia, visual changes), (2) procedure-related intracranial vascular complications (MMA rupture, fistula), (3) procedure-related access complications (femoral artery dissection, radial artery perforation, retroperitoneal hematoma, femoral artery occlusion, conversion from radial to femoral route), (4) post-procedural neurological complications (post-intervention seizures and delirium, worsening neurological deficits, worsening headache), (5) post-procedural systemic complications (infections, contrast agent allergy, acute kidney injury, deep venous thrombosis) and (6) miscellaneous complications. Clinical outcomes included treatment failure (hematoma recurrence or progression) and rescue surgery (hematoma re-accumulation, which necessitated repeat or rescue surgery).
Results
A total of 4103 studies were screened, 600 of which were identified as potentially relevant and included in the full-text screening. Of those, 173 were included in the analysis, as well as an additional 3 articles that were added by backward citation searching, resulting in a total of 176 included articles (46 case reports of single cases, 13 case reports in which 2 cases were described, 14 case series, 94 retrospective studies, 6 prospective observational studies and 5 randomized controlled trials) (see also Figure 1).
PRISMA flow diagram for the systematic literature review of the complications of middle meningeal artery embolization for chronic subdural hematoma. MAE = middle meningeal artery embolization; SDH = subdural hematoma.

Patient demographics and clinical details
Excluding the case reports and case series, the total number of patients included in these studies was 9780. Of those, 7245 (75.9%) were males and 2295 (24.1%) were females. Five studies including 136 patients did provide a breakdown by sex. The mean/median age range was 62.1–82.5 years. Across 42 articles encompassing 2232 patients, presenting symptoms were documented as follows: headache was the most common symptom, occurring in 1063 patients (47.6%). This was followed by motor deficits, limb weakness and hemiparesis in 426 patients (19.1%) and gait instability in 542 patients (24.2%). Fewer patients experienced cognitive decline and altered mental status (393 patients, 17.6%), focal neurological deficits (308 patients, 13.8%), speech difficulties and aphasia (90 patients, 4%) or seizures (41 patients, 1.8%). Seventy-six articles totaling 6126 patients documented the embolic agent used. Particles were the most commonly used embolic agent (2049 patients, 33.4%), followed by Onyx (1999 patients, 32.6%), followed by N- butyl 2- cyanoacrylate (NBCA) (973 patients, 15.9%) and coils (639 patients, 10.4%). Onyx plus coils were used in 52 patients (0.8%). Fifty-two articles, which included 7274 patients, reported complications related to MMAE (see also Figure 2). Complications were seen in 239 of 7274 patients (3.3%).
Top panel (A): Overall complication rate of middle meningeal artery embolization in chronic subdural hematoma patients. Middle panel (B): Types of complications seen in these patients. Lower panel (C): Breakdown of procedure-related neurological complications.

Procedure-related neurological complications
Procedure-related neurological complications were reported in 87 of 7274 patients (1.2%). Aphasia was present in five patients (0.07%). Visual changes due to retinal artery embolization were seen in 16 patients (0.2%). Ischemic changes, including asymptomatic, minor and major strokes, were seen in 39 cases (0.5%). Facial nerve palsy, either due to skull base anastomoses or inadvertent embolization of the petrosal branch of MMA, which feeds the geniculate ganglion, occurred in 16 cases (0.2%). Intracranial hemorrhage, whether intracerebral or extracerebral, was seen in 11 cases (0.2%) (see also Table 1).
Summary of complications reported during middle meningeal artery embolization for chronic subdural hematoma

Table 1 Long description
The table presents a summary of complications reported during middle meningeal artery embolization for chronic subdural hematoma. It includes data from various studies, detailing the total number of cases and the types of complications observed. The table is organized into columns: Title, Total number of cases, Procedure-related neurological complications, Procedure-related intracranial vascular complications, Procedure-related access complications, and Post-procedural neurological, systemic and miscellaneous other symptoms. Each row corresponds to a different study, listing the specific complications encountered. For example, Hung A et al reported 91 cases with 1 procedure-related neurological complication and 3 access site hematomas. The table provides a comprehensive overview of the various complications, their frequencies, and the studies in which they were reported.
PCA = posterior cerebral artery; MMA = middle meningeal artery; AVF = arteriovenous fistula; DVT = deep venous thrombosis; PE = pulmonary embolism; MI = myocardial infarction.
Procedure-related intracranial vascular complications
Eight articles reported procedure-related intracranial vascular complications, all of which were related to the MMA, in eight patients (0.1%). Two studies reported MMA rupture, Reference Kan, Maragkos and Srivatsan24 and three studies reported iatrogenic MMA arteriovenous fistula formation. Reference Shotar, Meyblum and Premat35,Reference Imai, Kato, Ito, Morishima, Aki and Shirakami36 Out of these, one case was of a fistula between MMA and the transverse sinus. Reference Orscelik, Senol and Bilgin20 Overt MMA perforation was seen in two cases. Reference Salem, Helal and Gajjar61,Reference Abdelsalam, Ramsay and Luther62
Procedure-related access complications
Eighteen articles reported access complications in 45 patients (0.6%). Twenty-three cases (0.3%) of access site hematoma were reported. Eight cases of pseudoaneurysm at the puncture site were seen. Two cases (<0.1%) of bleeding from the external iliac artery were reported. One case (<0.1%) each of femoral artery dissection, radial artery perforation, retroperitoneal hematoma, femoral artery occlusion and external carotid artery spasm were seen. Radial access failure occurred in seven cases (0.1%), necessitating conversion to femoral access.
Post-procedural neurological complications
Post-procedural neurological complications were seen in 37 of 7274 patients (0.5%). Post-MMAE seizures were seen in 21 patients (0.3%). Post-intervention delirium was seen in eight patients (0.1%), worsening headache in five patients (0.1%) and worsening neurological deficits such as numbness, venous infarct, balance difficulties and weakness were observed in one patient each (<0.1%).
Post-procedural systemic complications
Systemic complications in the post-procedural phase were seen in 55 of 7274 patients (0.8%). Infectious complications, including pneumonia and empyema, were noted in 49 cases (0.7%). Acute kidney injury and contrast agent allergy were each reported in two cases (<0.1%). Reference Carpenter, Rock and Dowlati37,Reference Liu, Ni and Zuo60 Deep vein thrombosis occurred in two cases (<0.1%). Reference Carpenter, Rock and Dowlati37
Miscellaneous complications
Miscellaneous complications were documented in five patients (<0.1%), all of which were related to the endovascular devices used. Catheter entrapment was reported in two cases (<0.1%). Reference Salem, Kuybu and Nguyen Hoang26,Reference Ma, Hoz and Doheim63 A retained catheter was observed in three cases (<0.1%). Reference Mohamed, Villabona and Kennion56,Reference Salem, Helal and Gajjar61
Case reports and case series on MMA embolization complications
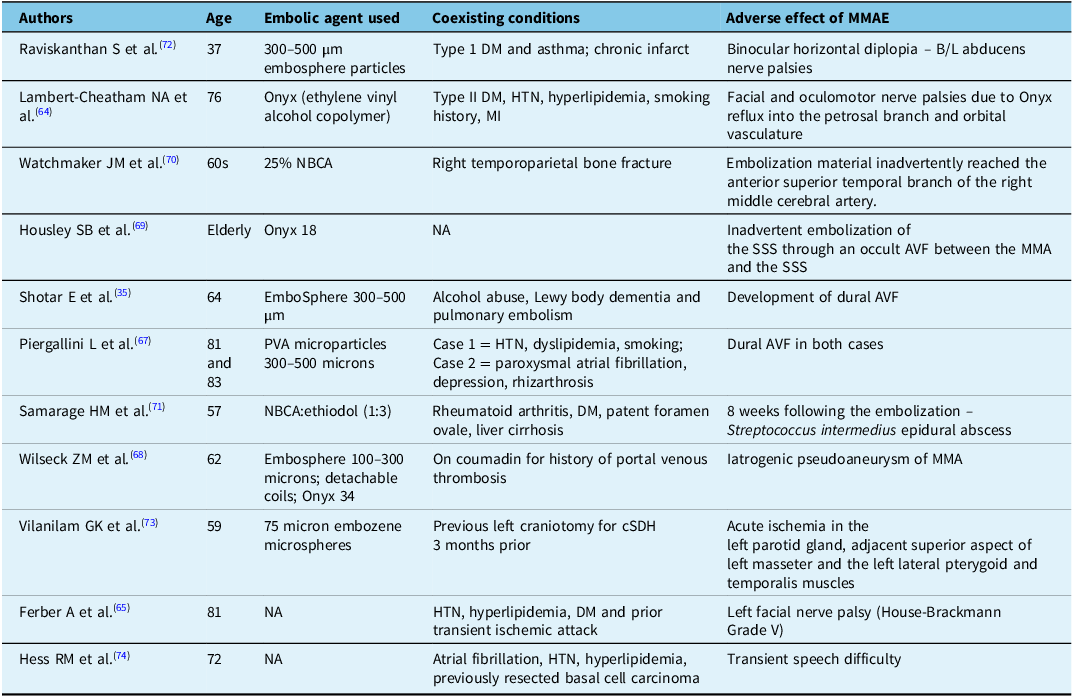
Eleven case reports totaling 12 patients specifically reported on complications related to MMAE. One case involved a combined facial and oculomotor nerve palsy, Reference Lambert-Cheatham, Pasmanter and Nagia64 while another reported facial nerve palsy. Reference Ferber, Zhou and Greenwald65 Three cases developed iatrogenic dural arteriovenous fistulas after MMAE with particles, one of which was managed conservatively, Reference Shotar, Premat and Barberis66 while coiling was performed in the other two. Reference Piergallini, Dargazanli, Derraz and Costalat67 There was one report of an iatrogenic pseudoaneurysm of the MMA post-embolization, which was treated with ethylene vinyl alcohol embolization. Reference Wilseck, Khan, Chaudhary and Gemmete68 In one instance, there was inadvertent occlusion of the superior sagittal sinus during MMA embolization through an occult arteriovenous fistula between the MMA and the superior sagittal sinus. This was treated with venous thrombectomy using a combination of aspiration and a stent retriever, which led to flow restoration. Reference Housley, Cappuzzo, Waqas, Lim and Levy69 In another case, NBCA reached the anterior superior temporal branch of the contralateral middle cerebral artery, but the patient did not develop any neurological symptoms post-procedure. Reference Watchmaker, Sisti and Shigematsu70 Lastly, one patient developed epidural empyema following NBCA embolization of the MMA Reference Samarage, Harary, Morales, Kaneko and Kim71 (see also Table 2).
Summary of complications reported in case reports and case series during middle meningeal artery embolization for chronic subdural hematoma

Table 2 Long description
A table comparing complications from middle meningeal artery embolization in chronic subdural hematoma cases. The table has 11 rows and 5 columns. Column headers are Authors, Age, Embolic agent used, Coexisting conditions, and Adverse effect of MMAE. Row 1: Authors, Raviskanthan S et al.; Age, 37; Embolic agent used, 300-500 µm embosphere particles; Coexisting conditions, Type 1 DM and asthma; chronic infarct; Adverse effect of MMAE, Binocular horizontal diplopia – B/L abducens nerve palsies. Row 2: Authors, Lambert-Cheatham NA et al.; Age, 76; Embolic agent used, Onyx (ethylene vinyl alcohol copolymer); Coexisting conditions, Type II DM, HTN, hyperlipidemia, smoking history, MI; Adverse effect of MMAE, Facial and oculomotor nerve palsies due to Onyx reflux into the petrosal branch and orbital vasculature. Row 3: Authors, Watchmaker JM et al.; Age, 60s; Embolic agent used, 25% NBCA; Coexisting conditions, Right temporoparietal bone fracture; Adverse effect of MMAE, Embolization material inadvertently reached the anterior superior temporal branch of the right middle cerebral artery. Row 4: Authors, Housley SB et al.; Age, Elderly; Embolic agent used, Onyx 18; Coexisting conditions, NA; Adverse effect of MMAE, Inadvertent embolization of the SSS through an occult AVF between the MMA and the SSS. Row 5: Authors, Shotar E et al.; Age, 64; Embolic agent used, EmboSphere 300-500 µm; Coexisting conditions, Alcohol abuse, Lewy body dementia and pulmonary embolism; Adverse effect of MMAE, Development of dural AVF. Row 6: Authors, Piergallini L et al.; Age, 81 and 83; Embolic agent used, PVA microparticles 300-500 microns; Coexisting conditions, Case 1 = HTN, dyslipidemia, smoking; Case 2 = paroxysmal atrial fibrillation, depression, rhizarthrosis; Adverse effect of MMAE, Dural AVF in both cases. Row 7: Authors, Samarage HM et al.; Age, 57; Embolic agent used, NBCA:ethiodol (1:3); Coexisting conditions, Rheumatoid arthritis, DM, patent foramen ovale, liver cirrhosis; Adverse effect of MMAE, 8 weeks following the embolization – Streptococcus intermedius epidural abscess. Row 8: Authors, Wilseck ZM et al.; Age, 62; Embolic agent used, Embosphere 100-300 microns; detachable coils; Onyx 34; Coexisting conditions, On coumadin for history of portal venous thrombosis; Adverse effect of MMAE, Iatrogenic pseudoaneurysm of MMA. Row 9: Authors, Vilanilam GK et al.; Age, 59; Embolic agent used, 75 micron embozene microspheres; Coexisting conditions, Previous left craniotomy for cSDH 3 months prior; Adverse effect of MMAE, Acute ischemia in the left parotid gland, adjacent superior aspect of left masseter and the left lateral pterygoid and temporalis muscles. Row 10: Authors, Ferber A et al.; Age, 81; Embolic agent used, NA; Coexisting conditions, HTN, hyperlipidemia, DM and prior transient ischemic attack; Adverse effect of MMAE, Left facial nerve palsy (House-Brackmann Grade V). Row 11: Authors, Hess RM et al.; Age, 72; Embolic agent used, NA; Coexisting conditions, Atrial fibrillation, HTN, hyperlipidemia, previously resected basal cell carcinoma; Adverse effect of MMAE, Transient speech difficulty.
DM = diabetes mellitus; HTN = hypertension; MI = myocardial infarction; AVF = arteriovenous fistula; MMA = middle meningeal artery; SSS = superior sagittal sinus; cSDH = chronic subdural hematoma.
Treatment failure
Although not a complication, treatment failure indicates that patients underwent a seemingly futile procedure with all its associated risks, and therefore, it was included as a variable of interest in this systematic review. Treatment failure was defined as cases where there was re-accumulation or progression of the hematoma, or when rescue surgery was required after MMA embolization in stand-alone MMA embolization cases, or repeat surgery following MMA embolization plus surgery in cases where adjunctive MMA embolization was performed alongside surgery. Hematoma recurrence was commented on in 56 articles, which included 4702 patients, and it was seen in 284 cases (6.0%). Twenty-eight articles, which included 2915 patients, mentioned hematoma progression, and it was reported in 120 patients (4.1%). Repeat or rescue surgery was mentioned in 52 articles, which included 5001 patients, and was necessary in 306 patients (6.1%).
Discussion
Our systematic review found that complications related to MMA embolization for cSDH occur in approximately 1 out of 30 patients. Neurological complications, occurring both during the procedure and in the post-procedural phase, were the most frequent type of complications, followed by systemic complications and access complications.
Several recent randomized trials have reported low complication rates associated with MMAE in cSDH. The STEM trial reported a 3% complication rate for both stand-alone and adjunct MMAE, aligning with our findings. Reference Fiorella, Monteith and Hanel75 The MAGIC-MT trial, focusing on nonacute SDH, noted facial nerve palsy in 0.3% of cases. Reference Liu, Ni and Zuo60 A 2024 study by Debs et al. observed no embolization-related complications in postoperative MMAE patients. Reference Debs, Vale and Walker76 In contrast, the EMBOLISE trial reported serious adverse events, including disabling stroke, in 2% of cases. Reference Davies, Knopman and Mokin59 Overall, complication rates across trials remain below 5%.
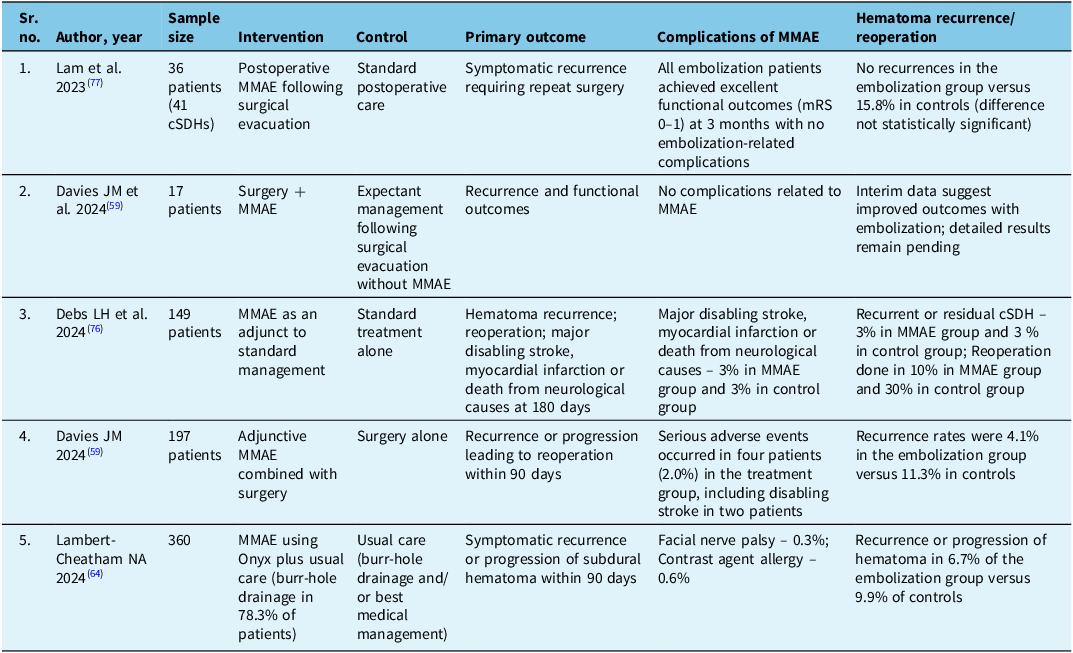
We found that hematoma recurrence was seen in 6% of cases. Hematoma expansion was reported in 4.1% cases, and repeat or rescue surgery was necessary in 6.1% cases (see also Table 3), which again closely resembles recurrence and progression rates of recently published trials. Reference Davies, Knopman and Mokin59,Reference Liu, Ni and Zuo60 The repeat surgery rate of 6.1% that we found ranges between published trial data, with MAGIC-MT (3%) reporting slightly lower and STEM (10%) slightly higher rates of repeat surgery. Reference Liu, Ni and Zuo60,Reference Fiorella, Monteith and Hanel75
Overview of the five included randomized controlled trials

Table 3 Long description
The table compares outcomes of different interventions for chronic subdural hematoma across five studies. It has six columns: Sr. no., Author, year, Sample size, Intervention, Control, Primary outcome, Complications of MMAE, and Hematoma recurrence/reoperation. The table includes five rows of data. Row 1: Sr. no. 1, Author Lam et al. 2023, Sample size 36 patients (41 cSDHs), Intervention Postoperative MMAE following surgical evacuation, Control Standard postoperative care, Primary outcome Symptomatic recurrence requiring repeat surgery, Complications of MMAE All embolization patients achieved excellent functional outcomes (mRS 0-1) at 3 months with no embolization-related complications, Hematoma recurrence/reoperation No recurrences in the embolization group versus 15.8% in controls (difference not statistically significant). Row 2: Sr. no. 2, Author Davies JM et al. 2024, Sample size 17 patients, Intervention Surgery + MMAE, Control Expectant management following surgical evacuation without MMAE, Primary outcome Recurrence and functional outcomes, Complications of MMAE No complications related to MMAE, Hematoma recurrence/reoperation Interim data suggest improved outcomes with embolization; detailed results remain pending. Row 3: Sr. no. 3, Author Debs LH et al. 2024, Sample size 149 patients, Intervention MMAE as an adjunct to standard management, Control Standard treatment alone, Primary outcome Hematoma recurrence; reoperation; major disabling stroke, myocardial infarction or death from neurological causes at 180 days, Complications of MMAE Major disabling stroke, myocardial infarction or death from neurological causes – 3% in MMAE group and 3% in control group, Hematoma recurrence/reoperation Recurrent or residual cSDH – 3% in MMAE group and 3% in control group; Reoperation done in 10% in MMAE group and 30% in control group. Row 4: Sr. no. 4, Author Davies JM 2024, Sample size 197 patients, Intervention Adjunctive MMAE combined with surgery, Control Surgery alone, Primary outcome Recurrence or progression leading to reoperation within 90 days, Complications of MMAE Serious adverse events occurred in four patients (2.0%) in the treatment group, including disabling stroke in two patients, Hematoma recurrence/reoperation Recurrence rates were 4.1% in the embolization group versus 11.3% in controls. Row 5: Sr. no. 5, Author Lambert-Cheatham NA 2024, Sample size 360, Intervention MMAE using Onyx plus usual care (burr-hole drainage in 78.3% of patients), Control Usual care (burr-hole drainage and/or best medical management), Primary outcome Symptomatic recurrence or progression of subdural hematoma within 90 days, Complications of MMAE Facial nerve palsy – 0.3%; Contrast agent allergy – 0.6%, Hematoma recurrence/reoperation Recurrence or progression of hematoma in 6.7% of the embolization group versus 9.9% of controls.
CSDH = chronic subdural hematoma; MMAE = middle meningeal artery embolization; mRS = modified Rankin Scale. Studies included in review (n = 176).
Overall, our results show that there is immense interest in, and potential for, MMAE in the management of patients with cSDH, whether as a stand-alone treatment or as an adjunctive treatment to surgery. However, it needs to be done safely. Our results also show that complications, although less frequent when performing MMAE, may have devastating consequences and may result in permanent disability.
Furthermore, the cSDH patient population is typically elderly and frail, requiring careful consideration of renal function, potential access-related challenges and limited physiological resilience to recover from complications. Due to the advanced age and frailty of these patients, GA presents a significant risk. Furthermore, GA is required when using liquid embolic agents like Onyx since they can induce pain during injection. Coils, on the other hand, are painless and might make it possible to perform MMAE without GA. Some however contend that distal penetration is necessary for the treatment to be successful, supporting the use of liquid embolic agents rather than coils. Future studies are required to answer this question, and for now, a flexible approach may be best – using coils if the patient is unable to undergo GA or if there are hazardous anastomoses and Onyx when distal penetration seems safely achievable. As an alternative, some interventionalists anecdotally report that injecting lidocaine into the MMA before employing Onyx allows for Onyx embolization to be carried out without GA.
Ultimately, each type of embolic agent has different advantages and disadvantages, and even within one subtype (e.g, liquid embolic agents like Onyx, NBCA and particles), different specific physical properties, such as viscosity, polymerization time and penetration capacity, can influence both procedural safety profiles and chances of success. Early experience with MMA embolization for cSDH was mostly with particles. However, in the last years, several materials have been used, including microparticles (e.g., PVA or tris-acryl gel), NBCA (cyanoacrylate) glue, Onyx, PHIL, SQUID and coils. Initial particle-based approaches have mostly given way to liquid agents, and even hybrid approaches that use different embolic agents (e.g., coils and particles, coils and liquid embolics) have been studied. Unfortunately, the information provided on the specific embolic agents used was scarce, and we were unable to perform a meta-analysis to determine the procedural risk for each different embolic agent.
Embolization precision can be increased by a host of other techniques, including super-selective catheterization and/or balloon-assisted approaches, to minimize the risk of non-target embolization. In terms of practical recommendations, it is recommended to perform nBCA or Onyx embolization under high magnification, with careful attention to the deflection point at the foramen spinosum, which helps define the safe reflux margin. To maintain anatomical orientation, it is recommended to use true anteroposterior (AP) and lateral projections. One should ensure that, on the AP view, the embolysate remains distal to the orbital roofs, and on the lateral view, it should not track posteriorly along the petrous ridge. Although detailed information on the technical approach was not provided in most cases, it seems prudent to use such precautions, specifically in instances with prominent anastomoses to the orbit and intracranial arteries, or when a distal catheter position cannot be safely reached. In the latter case, liquid embolics should be avoided altogether, and proximal coiling is recommended instead. Eventually, systematic exploration of these variables will lead to standardized protocols in enhancing patient outcomes and minimizing complications within the management of cSDHs.
Limitations
This study has limitations. First, our review captures the literature at a specific point in time; however, as evidence on MMAE for cSDH continues to rapidly accumulate and endovascular techniques and technologies evolve, repeating this review in the future might yield very different results. The evolution of embolic agents and techniques of neurointervention in the study timeframe may also have influenced the reported complication rates, and the results of our review may partly reflect temporal trends. The heterogeneity of the extracted data prevented us from performing a quantitative data synthesis, and we had to rely primarily on descriptive statistics. Additionally, our analysis was limited by the language of the articles included, although it is likely that most of the relevant literature is published in English. Many papers provided only a basic overview of complications, with only few offering a detailed breakdown. Consequently, certain complications – typically considered minor and transient, such as femoral artery pseudoaneurysms or urinary tract infections following catheterization for GA – may have been underreported, and our systematic review likely underestimates the true complication rates.
Conclusion
Our systematic review for MMAE in cSDH shows that MMAE is a viable adjunct therapy option and, in some cases, may provide a substitute for conventional surgical techniques. Even though the overall complication rate is low (roughly 3%), the possibility of severe complications highlights the need for careful procedural planning and meticulous technical execution. Optimizing the choice of embolic agent, procedural methods, and anesthetic management is essential due to the considerable anatomical diversity and the frailty of the patient population. In order to improve long-term results, increase patient safety and refine these strategies, future research including prospective trials that follow standardized protocols will be crucial.
Author contributions
Conception and design: JO, MG
Data acquisition, analysis and interpretation: GJ, YS, OB
Drafting the work: GJ, JO
Critically revising for important intellectual content: JO, MG
Final version approval: GJ, YS, OB, MG, JO
Funding statement
The authors received no funding support.
Competing interests
Johanna Ospel is a Steering committee member of an MMA for cSDH study funded by Penumbra Inc. Mayank Goyal holds grants from Medtronic and Cerenovus; receives royalties from Microvention; has received consulting fees from Microvention, Penumbra, Stryker, Philips, Medtronic and Mentice; and holds stocks from Circle Neurovascular. The remaining authors have nothing to disclose.




Target article
Complications of Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: A Systematic Literature Review
Related commentaries (1)
Reviewer Comment on Jindal et al. “Complications of Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: A Systematic Literature Review”