Statement of Research Significance
Research Question(s) or Topic(s): This study sought to better understand how often former elite American football players express subjective cognitive complaints, contributions to these complaints, and how their subjective complaints relate to objective cognitive test performance and biological measures of neurodegeneration from cerebrospinal fluid and neuroimaging. Main Findings: The majority of the former athletes reported subjective cognitive complaints, which were associated with symptoms of depression, anxiety, and impulsivity. Subjective cognitive complaints were associated with lower parahippocampal cortical thickness and with lower objective cognitive test performance after accounting for symptoms of depression. Study Contributions: This study uniquely examined relationships between subjective cognitive complaints and biomarkers of neurodegeneration in former American football players. Associations between subjective cognitive complaints and objective measures such as cognitive performance and regional cortical thickness support the potential utility of subjective complaints as a marker of cognitive decline or neurodegeneration in the setting of repetitive head impacts.
Introduction
Subjective cognitive complaints (SCC) are perceived declines in cognitive abilities relative to baseline reported by the patient, their friend, or family member informant, regardless of the patient’s performance on formal cognitive testing (Burmester et al., Reference Burmester, Leathem and Merrick2016; Mendonça et al., Reference Mendonça, Alves and Bugalho2016). SCC are commonly reported in healthy older adults (Röhr et al., Reference Röhr, Pabst, Riedel-Heller, Jessen, Turana, Handajani, Brayne, Matthews, Stephan, Lipton, Katz, Wang, Guerchet, Preux, Mbelesso, Ritchie, Ancelin, Carrière and Guaita2020) and across neurological conditions including early Alzheimer’s disease (AD; Donovan et al., Reference Donovan, Amariglio, Zoller, Rudel, Gomez-Isla, Blacker, Hyman, Locascio, Johnson, Sperling, Marshall and Rentz2014), Parkinson’s disease (Purri et al., Reference Purri, Brennan, Rick, Xie, Deck, Chahine, Dahodwala, Chen-Plotkin, Duda, Morley, Akhtar, Trojanowski, Siderowf and Weintraub2020; Siciliano et al., Reference Siciliano, Tessitore, Morgante, Goldman and Ricciardi2024), multiple sclerosis (Beier et al., Reference Beier, Amtmann and Ehde2015), epilepsy (Feldman et al., Reference Feldman, Lapin, Busch and Bautista2018), and traumatic brain injury (TBI; Anderson, Reference Anderson2021; French et al., Reference French, Lange and Brickell2014; Jamora et al., Reference Jamora, Young and Ruff2012; Levy et al., Reference Levy, Saling and Anderson2023; Spencer et al., Reference Spencer, Drag, Walker and Bieliauskas2010; Vos et al., Reference Vos, Williams, Poritz, Ngan, Leon-Novelo and Sherer2020). Self-reported SCC have shown a small but significant association with objective cognitive functioning, particularly when comprehensive measures of SCC were used (Burmester et al., Reference Burmester, Leathem and Merrick2016). SCC in the setting of normal cognitive test performance, termed subjective cognitive decline (SCD) in the AD literature, have been associated with increased risk for developing dementia in epidemiological studies, suggesting that SCC could be early indicators of future cognitive decline for some individuals (Jessen et al., Reference Jessen, Amariglio, Buckley, Van Der Flier, Han, Molinuevo, Rabin, Rentz, Rodriguez-Gomez, Saykin, Sikkes, Smart, Wolfsgruber and Wagner2020; Kang et al., Reference Kang, Li, Mahajan, Spat-Lemus, Durape, Chen, Gurnani, Devine, Auerbach, Ang, Sherva, Qiu, Lunetta, Au, Farrer and Mez2024; Mitchell et al., Reference Mitchell, Beaumont, Ferguson, Yadegarfar and Stubbs2014; Parfenov et al., Reference Parfenov, Zakharov, Kabaeva and Vakhnina2020; Pike et al., Reference Pike, Cavuoto, Li, Wright and Kinsella2022; Tsutsumimoto et al., Reference Tsutsumimoto, Makizako, Doi, Hotta, Nakakubo, Makino, Shimada and Suzuki2017).
SCC are strongly influenced by a multitude of factors, including 1) demographic characteristics such as race, ethnicity, and education (Röhr et al., Reference Röhr, Pabst, Riedel-Heller, Jessen, Turana, Handajani, Brayne, Matthews, Stephan, Lipton, Katz, Wang, Guerchet, Preux, Mbelesso, Ritchie, Ancelin, Carrière and Guaita2020); 2) health-related factors such as sleep, chronic pain, obesity, cardiovascular health, and concussion history (Roberts et al., Reference Roberts, Zafonte, Speizer, Baggish, Taylor, Nadler and Weisskopf2021; Walton et al., Reference Walton, Kerr, Mannix, Brett, Chandran, DeFreese, McCrea, Guskiewicz, Meehan and Echemendia2022; Westoby et al., Reference Westoby, Mallen and Thomas2009); and 3) psychological and personality factors such as symptoms of depression, anxiety, and stress (Donnelly et al., Reference Donnelly, Donnelly, Warner, Kittleson and King2018; Hill et al., Reference Hill, Mogle, Wion, Munoz, DePasquale, Yevchak and Parisi2016; Karr et al., Reference Karr, Rau, Shofer, Hendrickson, Peskind and Pagulayan2019; Ryu et al., Reference Ryu, Lee, Kim and Lee2016, Reference Ryu, Lee, Kim and Lee2016; Sabatini et al., Reference Sabatini, Woods, Ukoumunne, Ballard, Collins and Clare2022). Depressive symptoms in particular are a major contributor to SCC and have been found to partially mediate the relationship between subjective and objective cognition (Hill et al., Reference Hill, Bhargava, Bratlee-Whitaker, Turner, Brown, Mogle and Pike2021; Kim et al., Reference Kim, Chu, Oh, Lee, Choi and Kim2024). In addition, given the potential for bias in self-reported SCC, research has suggested that informant-reported SCC can more accurately predict cognitive and functional decline (Jiménez-Huete et al., Reference Jiménez-Huete, Del Barrio, Riva, Campo, Toledano and Franch2017; Pérez-Blanco et al., Reference Pérez-Blanco, Felpete, Patten, Mallo, Pereiro, Campos-Magdaleno and Juncos-Rabadán2022).
While SCC have been studied in AD and TBI, fewer studies have examined the characteristics of SCC in the context of repetitive head impacts (RHI). Exposure to RHI, which can result in both symptomatic TBI and asymptomatic non-concussive impacts, is commonly observed in contact/collision sports and has been associated with neuropsychiatric and cognitive disorders later in life (Alosco et al., Reference Alosco, Tripodis, Baucom, Mez, Stein, Martin, Haller, Conneely, McClean, Nosheny, Mackin, McKee, Weiner and Stern2020; Levitch et al., Reference Levitch, Zimmerman, Lubin, Kim, Lipton, Stewart, Kim and Lipton2018; Montenigro et al., Reference Montenigro, Alosco, Martin, Daneshvar, Mez, Chaisson, Nowinski, Au, McKee, Cantu, McClean, Stern and Tripodis2017; Roberts et al., Reference Roberts, Pascual-Leone, Speizer, Zafonte, Baggish, Taylor, Nadler, Courtney, Connor, Grashow, Stillman, Marengi and Weisskopf2019). Substantial exposure to RHI is considered a primary risk factor for chronic traumatic encephalopathy (CTE), a neurodegenerative disease characterized by the perivascular accumulation of hyperphosphorylated tau at the depths of cortical sulci (Bieniek et al., Reference Bieniek, Cairns, Crary, Dickson, Folkerth, Keene, Litvan, Perl, Stein, Vonsattel, Stewart, Dams-O’Connor, Gordon, Tripodis, Alvarez, Mez, Alosco and McKee2021; McKee et al., Reference McKee, Stein, Huber, Crary, Bieniek, Dickson, Alvarez, Cherry, Farrell, Butler, Uretsky, Abdolmohammadi, Alosco, Tripodis, Mez and Daneshvar2023; Mez et al., Reference Mez, Daneshvar, Kiernan, Abdolmohammadi, Alvarez, Huber, Alosco, Solomon, Nowinski, McHale, Cormier, Kubilus, Martin, Murphy, Baugh, Montenigro, Chaisson, Tripodis, Kowall and McKee2017, Reference Mez, Daneshvar, Abdolmohammadi, Chua, Alosco, Kiernan, Evers, Marshall, Martin, Palmisano, Nowinski, Mahar, Cherry, Alvarez, Dwyer, Huber, Stein, Goldstein, Katz and McKee2020). The proposed clinical syndrome of CTE, termed traumatic encephalopathy syndrome (TES), includes self- or informant-reported SCC as well as objective deficits on memory and/or executive functioning tests to comprise its core clinical feature of cognitive impairment (Katz et al., Reference Katz, Bernick, Dodick, Mez, Mariani, Adler, Alosco, Balcer, Banks, Barr, Brody, Cantu, Dams-O’Connor, Geda, Jordan, McAllister, Peskind, Petersen, Wethe and Stern2021).
Higher levels of SCC have been reported in former elite athletes with exposure to RHI compared to the general population (Brett et al., Reference Brett, Sullivan, Asken, Terry, Meier and McCrea2025; Cunningham et al., Reference Cunningham, Broglio, O’Grady and Wilson2020). Former contact-sport athletes have also reported more SCC than age-matched former non-contact-sport athletes, though informant-reported SCC did not differ (Willer et al., Reference Willer, Tiso, Haider, Hinds, Baker, Miecznikowski and Leddy2018). Findings have been mixed regarding whether SCC in former athletes with RHI exposure correspond to objective cognitive deficits (Allen et al., Reference Allen, Cole, Walton, Kerr, Chandran, Mannix, Guskiewicz, Meehan, Echemendia, McCrea and Brett2023; Bryant et al., Reference Bryant, Kerr, Walton, Barr, Guskiewicz, McCrea and Brett2023; Van Patten et al., Reference Van Patten, Iverson, Terry, Levi and Gardner2021; Willer et al., Reference Willer, Tiso, Haider, Hinds, Baker, Miecznikowski and Leddy2018). Similar to the older adult literature, greater SCC in former contact sport athletes often occur in the context of health and neuropsychiatric factors including symptoms of depression and anxiety, fatigue, and history of concussion (Brett et al., Reference Brett, Kerr, Chandran, Walton, Aggarwal, Gifford, Mannix, DeFreese, Echemendia, Guskiewicz, Meehan and McCrea2023; Bryant et al., Reference Bryant, Kerr, Walton, Barr, Guskiewicz, McCrea and Brett2023; Guskiewicz et al., Reference Guskiewicz, Marshall, Bailes, McCrea, Cantu, Randolph and Jordan2005; Plessow et al., Reference Plessow, Pascual-Leone, McCracken, Baker, Krishnan, Baggish, Connor, Courtney, Nadler, Speizer, Taylor, Weisskopf, Zafonte and Meehan2020; Walton et al., Reference Walton, Kerr, Mannix, Brett, Chandran, DeFreese, McCrea, Guskiewicz, Meehan and Echemendia2022). It remains unclear whether SCC in individuals with exposure to RHI are predictive of future cognitive decline or risk for CTE and related dementias.
Cerebrospinal fluid (CSF) and magnetic resonance imaging (MRI) markers provide objective measurements of neural injury or degeneration. In cognitively healthy older adults, early AD, and TBI populations, SCC have been linked to CSF markers of AD, positive amyloid PET imaging, smaller hippocampal volumes, larger white matter hyperintensity volume, and reduced cortical thickness (Amariglio et al., Reference Amariglio, Mormino, Pietras, Marshall, Vannini, Johnson, Sperling and Rentz2015; Dauphinot et al., Reference Dauphinot, Bouteloup, Mangin, Vellas, Pasquier, Blanc, Hanon, Gabelle, Annweiler, David, Planche, Godefroy, Rivasseau-Jonveaux, Chupin, Fischer, Chêne, Dufouil and Krolak-Salmon2020; Dhana et al., Reference Dhana, DeCarli, Dhana, Desai, Krueger, Evans and Rajan2022; Ly et al., Reference Ly, Merritt, Ozturk, Clark, Hanson, Delano-Wood and Sorg2023; Visser et al., Reference Visser, Verhey, Knol, Scheltens, Wahlund, Freund-Levi, Tsolaki, Minthon, Wallin, Hampel, Bürger, Pirttila, Soininen, Rikkert, Verbeek, Spiru and Blennow2009). However, research is limited on whether SCCs in RHI are related to biomarkers of neurodegeneration.
The prevalence of SCC and their correlates in individuals with exposure to RHI are poorly understood, and few studies to date have examined SCC in the context of both cognitive performance and biomarkers. The present study examined comprehensive self- and informant-reported measures of SCC alongside neuropsychological assessment and CSF and MRI measures in a sample of former elite American football players. We characterized (1) frequency of SCC, globally and domain-specific in a cohort of mainly symptomatic players; (2) neuropsychiatric symptom correlates for SCC; (3) concordance between self- and informant-reported complaints; (4) associations between SCC and neuropsychological test performance; and (5) associations between SCC and CSF and neuroimaging biomarkers. We hypothesized that most of the sample would report SCC and that neuropsychiatric symptoms, particularly depressive symptoms, would be strongly associated with SCC. We predicted that in the setting of neuropsychiatric symptoms, the former football players would report higher levels of SCC than their informants, and that there would be no association between SCC and neuropsychological factor scores after accounting for depressive symptoms. Finally, we predicted significant associations between SCC and CSF and neuroimaging markers of neurodegeneration but not between SCC and AD-specific CSF biomarkers given the age range of the sample.
Methods
Participants and study design
This study represents a secondary analysis of data from the Diagnostics, Imaging, and Genetics Network for the Objective Study and Evaluation of Chronic Traumatic Encephalopathy (DIAGNOSE CTE) Research Project (Alosco et al., Reference Alosco, Mariani, Adler, Balcer, Bernick, Au, Banks, Barr, Bouix, Cantu, Coleman, Dodick, Farrer, Geda, Katz, Koerte, Kowall, Lin, Marcus and Wethe2021). The goals of the DIAGNOSE CTE Research Project included characterizing the clinical presentation of CTE, refining and validating clinical research diagnostic criteria (i.e., traumatic encephalopathy syndrome [TES]), and examining risk factors and biomarkers for CTE. The DIAGNOSE CTE Research Project enrolled 180 male, former elite American football players between ages 45 and 74, including 120 former professional football players (12+ years of total football play with 4+ seasons playing professionally) and 60 former college football players (6+ years of football play with 3+ at the college level). There were no enrollment criteria for presence or severity of cognitive or neuropsychiatric symptoms, and recruitment was aimed at enrolling former football players across the continuum of symptom severity. The project also enrolled 56 men without exposure to RHI or TBI who were not included in this study because they were recruited to be cognitively and psychiatrically asymptomatic. All participants needed to have English as their primary language, an available study partner who knows them well, and no contraindications to study procedures (e.g., MRI, lumbar puncture [LP]). Participants were excluded if they had a history of clinical stroke, major sensory impairments that could affect neuropsychological testing, impaired decisional capacity, or a clinically significant medical or neurological condition (e.g., infectious disease, metabolic disease). Recruitment for the DIAGNOSE CTE Research Project was coordinated nationally through Boston University using an extensive multimedia campaign, including targeted videos, newsletter posts, flyer distribution at community events, email distribution of electronic flyers to alumni groups, social media, and poster/billboard advertising. The project aimed to recruit approximately 40% Black former football players based on the proportion who have historically played in the National Football League. A detailed overview of the study including eligibility criteria for each exposure-based subgroup (unexposed, former college football players, and former professional football players), recruitment, and retention procedures have been described elsewhere (Alosco et al., Reference Alosco, Mariani, Adler, Balcer, Bernick, Au, Banks, Barr, Bouix, Cantu, Coleman, Dodick, Farrer, Geda, Katz, Koerte, Kowall, Lin, Marcus and Wethe2021). Participants completed clinical interviews, self-report questionnaires of cognitive, neurological, and neuropsychiatric symptoms, neuropsychological testing, MRI, LP, and blood draw.
All participants provided written informed consent to be evaluated for the DIAGNOSE CTE Research Project. The present study was completed in accordance with the Helsinki Declaration. All Participant Evaluation Site institutions (Boston University [BU] Medical Campus Institutional Review Board #H-34799, Cleveland Clinic [CC] Institutional Review Board #16-1694, Mayo Clinic Institutional Review Boards #16-002662, New York University [NYU] School of Medicine Institutional Review Board #i16-01032 CR3) and associated sites (Banner Alzheimer’s Institute [BAI] and Brigham and Women’s Hospital [BWH]) involved in the DIAGNOSE CTE Research Project received approval by their respective institutional review boards.
Subjective cognitive complaints (SCC)
AD8: The Eight-item Ascertain Dementia (AD8) questionnaire is a screening tool for global SCC that asks if an individual has experienced a change (yes/no) in the last several years in general cognition and various activities of daily living. It was originally developed and validated as a brief informant interview (Galvin et al., Reference Galvin, Roe, Powlishta, Coats, Muich, Grant, Miller, Storandt and Morris2005) but can also reliably differentiate between normal aging and mild dementia as a self-rating tool (Galvin et al., Reference Galvin, Roe, Coats and Morris2007). A cut-off of two endorsed items has been found to optimize sensitivity and specificity for dementia and cognitive impairment in self- and informant-reported AD8 (Galvin et al., Reference Galvin, Roe, Xiong and Morris2006; Passler et al., Reference Passler, Kennedy, Crowe, Clay, Howard, Cushman, Unverzagt and Wadley2021).
Cognitive Change Index (CCI): The CCI assesses self-reported perception of decline in memory, language, and executive functioning (Rattanabannakit et al., Reference Rattanabannakit, Risacher, Gao, Lane, Brown, McDonald, Unverzagt, Apostolova, Saykin and Farlow2016). This study used the first 12 out of 20 items pertaining to memory (CCI-12). Respondents rated perceived change from 1 (no change) to 5 (much worse/severe problem), with total scores ranging from 12 to 60. While many studies including the Alzheimer’s Disease Neuroimaging Initiative use a cutoff of 16 to indicate significant memory complaint, recent research has shown that a cutoff of 20 optimizes sensitivity in predicting cognitive decline (Risacher et al., Reference Risacher, West, McDonald, Tallman, Glazier, Gao, Brown, Apostolova, Brosch, Farlow, Unverzagt and Saykin2017). Informant ratings were not obtained for the CCI as part of this study.
Behavior Rating Inventory of Executive Functioning – Adult (BRIEF): The BRIEF-A is a 75-item self- or informant-report measure that captures views of an individual’s executive functions or self-regulation in their everyday environment (Roth et al., Reference Roth, Isquith and Gioia2005). It is sensitive to executive dysfunction in mild cognitive impairment and subjective cognitive complaints in older adults (Rabin et al., Reference Rabin, Roth, Isquith, Wishart, Nutter-Upham, Pare, Flashman and Saykin2006). The Metacognition Index (BRIEF MI) reflects one’s ability to get started on activity, to hold information in active working memory, to plan and organize problem-solving approaches, to monitor and complete tasks, and to maintain organization in the environment (Roth et al., Reference Roth, Lance, Isquith, Fischer and Giancola2013). A T-score cut-off of 65 or above is typically interpreted as clinically significant. Of note, the Behavioral Regulation Index (BRI) of the BRIEF was excluded because it primarily captures emotional control and inhibition rather than cognitive self-regulation, which was the focus of the current study.
Neuropsychiatric symptoms
The following neuropsychiatric symptom measures were selected to represent the broad range of mood, behavioral, and health symptoms that can affect cognition:
Beck Depression Inventory (BDI-II): The BDI-II is a 21-item self-report inventory measuring the severity of depression over the past two weeks, with total scores ranging from 0 to 63 and higher scores indicating greater severity (Beck et al., Reference Beck, Steer and Brown1996).
Beck Anxiety Inventory (BAI): The BAI is a 21-item self-report inventory measuring the intensity of cognitive, affective, and somatic symptoms of anxiety over the past seven days, with total scores ranging from 0 to 63 and higher scores indicating greater severity (Beck et al., Reference Beck, Epstein, Brown and Steer1988).
Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): The PCL-5 is a 20-item self-report inventory measuring the severity of symptoms of PTSD over the past month in response to a traumatic event, with total scores ranging from 0 to 80 and higher scores indicating greater severity (Blevins et al., Reference Blevins, Weathers, Davis, Witte and Domino2015).
Alcohol Use Disorders Identification Test (AUDIT): The AUDIT is a 10-item screening tool for unhealthy alcohol use that measures alcohol intake, potential dependence on alcohol, and experience of alcohol-related harm (Saunders et al., Reference Saunders, Aasland, Babor, de la Fuente and Grant1993). Total scores range from 0 to 40, with higher scores indicating more problematic use.
Epworth Sleepiness Scale (ESS): The ESS is an 8-item self-report inventory measuring an individual’s general level of daytime sleepiness, with total scores ranging from 0 to 24 and higher scores indicating greater daytime sleepiness (Johns, Reference Johns1991).
Barratt Impulsiveness Scale (BIS-11): The BIS-11 is a 30-item self-report inventory measuring an individual’s trait impulsivity, with total scores ranging from 30 to 120 and higher scores indicating greater impulsivity (Patton et al., Reference Patton, Stanford and Barratt1995).
Neuropsychological testing
Neuropsychological evaluation encompassed tests of attention, visual scanning, and psychomotor speed; executive functions; learning and episodic memory (verbal and visual); language; and visuospatial abilities. A complete list of tests and reporting of participants’ performances has been described elsewhere (Alosco et al., Reference Alosco, Barr, Banks, Wethe, Miller, Pulukuri, Culhane, Tripodis, Adler, Balcer, Bernick, Mariani, Cantu, Dodick, McClean, Au, Mez, Turner, Palmisano and Johnson2023). Composite factor scores were derived through a principal component analysis (PCA) of standardized neuropsychological test scores among all participants (football players and controls), which yielded a five-factor solution. The five factors were named (1) Verbal Learning and Memory, (2) Executive Function and Psychomotor Speed, (3) Visual Learning and Memory, (4) Number Span Forward and Backward, and (5) Verbal Fluency. Higher factor scores represent better cognitive performance. This study focused on the Verbal Learning and Memory and Executive Function and Psychomotor Speed factors because this sample of football players most consistently showed low scores on tests of verbal memory and the Trail Making Test (Alosco et al., Reference Alosco, Barr, Banks, Wethe, Miller, Pulukuri, Culhane, Tripodis, Adler, Balcer, Bernick, Mariani, Cantu, Dodick, McClean, Au, Mez, Turner, Palmisano and Johnson2023), and these cognitive domains are thought to be most affected in CTE (Katz et al., Reference Katz, Bernick, Dodick, Mez, Mariani, Adler, Alosco, Balcer, Banks, Barr, Brody, Cantu, Dams-O’Connor, Geda, Jordan, McAllister, Peskind, Petersen, Wethe and Stern2021). The Verbal Learning and Memory factor (hereafter referred to as “verbal memory”) included immediate, short, and long delay recall scores from the Neuropsychological Assessment Battery (NAB) list learning test (Stern & White, Reference Stern and White2003). The Executive Functioning and Processing Speed factor (hereafter referred to as “executive functioning/processing speed”) included scores from Trail Making Test Parts A and B (Reitan, Reference Reitan1958), NAB Mazes Test (Stern & White, Reference Stern and White2003), and the Symbol Digit Modalities Test (A. Smith, Reference Smith1973). Factor scores were not calculated for 10 participants due to missing data or questionable validity based on performance validity tests (Tombaugh, Reference Tombaugh1997).
MRI
MRI was acquired on Siemens 3T MAGNETOM Skyra (Erlangan, Germany; software version VE11) across all four sites. Neuroimaging protocols included T1-, T2-, and diffusion MRI. Harmonization and quality control procedures have been described (Alosco et al., Reference Alosco, Mariani, Adler, Balcer, Bernick, Au, Banks, Barr, Bouix, Cantu, Coleman, Dodick, Farrer, Geda, Katz, Koerte, Kowall, Lin, Marcus and Wethe2021). All structural sequences were acquired at high resolution (1 × 1 × 1 mm3, 176 slices, 256 × 256 cm2 field of view) in the sagittal plane, including T1 MPRAGE (TR = 2530 ms, TE = 3.36 ms, TI = 1100 ms) and T2-weighted FLAIR (TR = 5000 ms, TE = 388 ms, TI = 1800 ms).
Brain masking was performed using a technique based on multi-atlas brain segmentation (Del Re et al., Reference Del Re, Gao, Eckbo, Petryshen, Blokland, Seidman, Konishi, Goldstein, McCarley, Shenton and Bouix2016). Pre-processing (motion correction and average, automated Talaraich transformation, intensity normalization), cortical reconstruction, and volumetric segmentation were performed using the freely available FreeSurfer image analysis suite (version 7.1) (Fischl, Reference Fischl2012). Hippocampal volume was obtained from automatic subcortical segmentation using a probabilistic brain atlas (Fischl et al., Reference Fischl, Salat, Busa, Albert, Dieterich, Haselgrove, Van Der Kouwe, Killiany, Kennedy, Klaveness, Montillo, Makris, Rosen and Dale2002). Cortical thickness was calculated as the measure of the distance (in mm) between the gray/white matter boundary to the gray matter/CSF boundary at each vertex on the cortical surface. Regions of interest for cortical thickness included the bilateral entorhinal cortex, parahippocampal cortex, rostral anterior cingulate cortex (rACC), and rostral middle frontal gyrus (rMFG) for their involvement in memory and executive functioning and previous association with SCC in setting of head injury (Gasquoine, Reference Gasquoine2013; Luck et al., Reference Luck, Danion, Marrer, Pham, Gounot and Foucher2010; Ly et al., Reference Ly, Merritt, Ozturk, Clark, Hanson, Delano-Wood and Sorg2023; Meiberth et al., Reference Meiberth, Scheef, Wolfsgruber, Boecker, Block, Träber, Erk, Heneka, Jacobi, Spottke, Walter, Wagner, Hu and Jessen2015). Findings from the DIAGNOSE CTE Research Project have shown lower hippocampal volume, entorhinal cortex thickness, and parahippocampal gyrus thickness in the former football players compared to the unexposed asymptomatic controls (Arciniega et al., Reference Arciniega, Baucom, Tuz-Zahra, Tripodis, John, Carrington, Kim, Knyazhanskaya, Jung, Breedlove, Wiegand, Daneshvar, Rushmore, Billah, Pasternak, Coleman, Adler, Bernick, Balcer and Bouix2024).
CSF biomarkers
All sites used uniform methods and prefabricated sample collection kits for CSF collection (Alosco et al., Reference Alosco, Mariani, Adler, Balcer, Bernick, Au, Banks, Barr, Bouix, Cantu, Coleman, Dodick, Farrer, Geda, Katz, Koerte, Kowall, Lin, Marcus and Wethe2021). CSF measurements included beta-amyloid protein1-42 (Aβ1-42), phosphorylated-tau181 (p-tau181), total tau (t-tau), and neurofilament light (NfL). CSF Aβ1-42, p-tau181, and t-tau were measured using Lumipulse technology (Fujirebio, Ghent, Belgium) as previously described (Gobom et al., Reference Gobom, Parnetti, Rosa-Neto, Vyhnalek, Gauthier, Cataldi, Lerch, Laczo, Cechova, Clarin, Benet, Pascoal, Rahmouni, Vandijck, Huyck, Le Bastard, Stevenson, Chamoun, Alcolea and Blennow2022). NfL was measured using an in-house enzyme-linked immunosorbent assays (Rosengren et al., Reference Rosengren, Wikkelsø and Hagberg1994).
CSF biomarkers were selected based on the amyloid – tau – neurodegeneration (A/T/N) framework (Gauthier et al., Reference Gauthier, Zhang, Ng, Pascoal and Rosa-Neto2018; Jack et al., Reference Jack, Bennett, Blennow, Carrillo, Dunn, Haeberlein, Holtzman, Jagust, Jessen, Karlawish, Liu, Molinuevo, Montine, Phelps, Rankin, Rowe, Scheltens, Siemers, Snyder and Silverberg2018). While the A/T/N framework was originally proposed for AD, it has since been used to investigate biomarker prognostic value in other neurodegenerative diseases (Barba et al., Reference Barba, Abu-Rumeileh, Halbgebauer, Bellomo, Paolini Paoletti, Gaetani, Oeckl, Steinacker, Massa, Parnetti and Otto2023; Delmotte et al., Reference Delmotte, Schaeverbeke, Poesen and Vandenberghe2021). CSF Aβ1-42 and p-tau181 are biomarkers of hallmark AD neuropathological changes but have limited utility for CTE (Bergauer et al., Reference Bergauer, van Osch, van Elferen, Gyllvik, Venkatesh and Schreiber2022; Jack et al., Reference Jack, Bennett, Blennow, Carrillo, Dunn, Haeberlein, Holtzman, Jagust, Jessen, Karlawish, Liu, Molinuevo, Montine, Phelps, Rankin, Rowe, Scheltens, Siemers, Snyder and Silverberg2018; Olsson et al., Reference Olsson, Lautner, Andreasson, Öhrfelt, Portelius, Bjerke, Hölttä, Rosén, Olsson, Strobel, Wu, Dakin, Petzold, Blennow and Zetterberg2016). CSF t-tau is a nonspecific marker of neuronal injury and degeneration that has been associated with greater exposure to RHI in former professional football players (Alosco et al., Reference Alosco, Tripodis, Fritts, Heslegrave, Baugh, Conneely, Mariani, Martin, Frank, Mez, Stein, Cantu, McKee, Shaw, Trojanowski, Blennow, Zetterberg and Stern2018). CSF NfL is a non-specific marker of neuroaxonal damage that is related to disease severity in different neurological disorders and has been associated with greater hippocampal volume decline in active boxers (Bernick et al., Reference Bernick, Shan, Zetterberg, Banks, Mishra, Bekris, Leverenz and Blennow2020; Bridel et al., Reference Bridel, van Wieringen, Zetterberg, Tijms, Teunissen, Andreasson, Axelsson, Bäckström, Bartos, Bjerke, Blennow, Boxer, Brundin, Burman, Christensen, Fialová, Forsgren, Frederiksen, Gisslén and Gray2019; Gaetani et al., Reference Gaetani, Höglund, Parnetti, Pujol-Calderon, Becker, Eusebi, Sarchielli, Calabresi, Di Filippo, Zetterberg and Blennow2018).
Demographic, athletic, and genetic characteristics
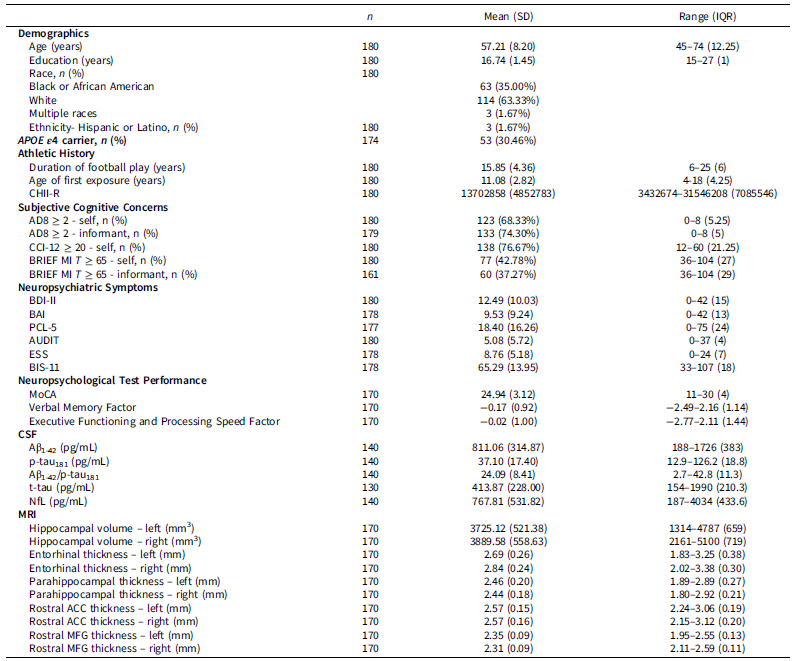
Semi-structured interviews and online questionnaires were used to collect demographic data, medical history, and athletic history (Table 1), as well as other variables not relevant to the present study. For athletic history, proxy measures for exposure to RHI included total years of football play, age of first exposure to football, and a cumulative head impact index (CHII-R) calculated as the lifetime load of rotational acceleration based on helmet accelerometer data and number of years played (Daneshvar et al., Reference Daneshvar, Nair, Baucom, Rasch, Abdolmohammadi, Uretsky, Saltiel, Shah, Jarnagin, Baugh, Martin, Palmisano, Cherry, Alvarez, Huber, Weuve, Nowinski, Cantu, Zafonte and Mez2023). CHII-R was selected due to the primary role of rotational acceleration and deceleration in diffuse axonal injury (D. H. Smith et al., Reference Smith, Meaney and Shull2003). Apolipoprotein E (APOE) genotyping was conducted using standard methodology as described elsewhere (Alosco et al., Reference Alosco, Mariani, Adler, Balcer, Bernick, Au, Banks, Barr, Bouix, Cantu, Coleman, Dodick, Farrer, Geda, Katz, Koerte, Kowall, Lin, Marcus and Wethe2021). For the purposes of this study, participants were categorized as being an APOE ϵ4 carrier or non-carrier. Race and ethnicity were self-reported.
Participant demographic, athletic, neuropsychiatric, and biomarker characteristics (n = 180)

Note: APOE = apolipoprotein E, CHII-R = cumulative head impact index rotational, AD8 = Eight-item Ascertain Dementia, CCI-12 = Cognitive Change Index 12-item, BRIEF MI = Behavior Rating Inventory of Executive Functioning Metacognition Index, BDI-II = Beck Depression Inventory Second Edition, BAI = Beck Anxiety Inventory, PCL-5 = Post-Traumatic Stress Disorder Checklist for DSM-5, AUDIT = Alcohol Use Disorders Identification Test, ESS = Epworth Sleepiness Scale, BIS-11 = Barratt Impulsiveness Scale Version 11, MoCA = Montreal Cognitive Assessment, CSF = cerebrospinal fluid, NfL = neurofilament light, MRI = magnetic resonance imaging, ACC = anterior cingulate cortex, MFG = middle frontal gyrus.
Statistical analyses
The proportion of participants reporting SCC was determined using established cut-offs described above (AD8 ≥ 2, CCI-12 ≥ 20, BRIEF MI ≥ 65). T-tests and chi-square tests evaluated whether SCC and No SCC groups by each measure differed in terms of demographics (e.g., age, race, education), APOE ϵ4 carrier status, athletic history (e.g., total years of football play, age of first exposure to football, and CHII-R), and self-reported neuropsychiatric symptoms (e.g., BDI-II, BAI, PCL-5, AUDIT, ESS, and BIS-11). Race was dichotomized as White and non-White due to the small number of participants in some categories.
Elastic net regression was used to evaluate the relative importance of the above demographic, genetic, athletic, and neuropsychiatric features as correlates of each measure of SCC. Elastic net is a feature selection technique that combines L1 and L2 regularization penalties and can effectively handle multicollinearity (i.e., correlations between features such as symptoms of depression, anxiety, and PTSD; Zou & Hastie, Reference Zou and Hastie2005). Each variable was scaled to a mean of 0 and standard deviation of 1 to ensure model coefficient comparability. Five-fold cross-validation with 1,000 iterations was used to estimate model coefficients for each feature. Model hyperparameters (α, λ) were tuned using nested ten-fold cross-validation.
Inter-rater concordances between self- and informant-reported AD8 total scores and BRIEF MI T scores as continuous values were assessed using intraclass correlation coefficients (ICC). Informant-rated CCI scores were not collected as part of the study. Discrepancy scores were calculated as informant minus self-reported scores, and t-tests determined whether discrepancy scores differed from 0. Positive discrepancy scores reflect when informants reported higher scores than participants’ self-reports, while negative discrepancy scores reflect when participants’ self-reports were higher than their informants. Pearson’s correlation test (r) assessed whether discrepancies between self and informant reports were associated with symptoms of depression as measured by the BDI-II, since depression is a reliable and the most studied predictor of SCC (Burmester et al., Reference Burmester, Leathem and Merrick2016).
Multiple linear regressions assessed relationships between each self- and informant-reported measure of SCC (as continuous values and z-score normalized) and objective cognitive performance in verbal memory and executive functioning/processing speed, adjusting for age, race, education, and APOE ϵ4 carrier status. Additional models included symptoms of depression as a covariate (i.e., BDI-II total scores). Similar linear regressions assessed relationships between self-reported SCC and CSF (Aβ1-42, p-tau181, Aβ1-42/p-tau181 ratio, t-tau, and NfL) and MRI (bilateral hippocampal volume, bilateral rostral anterior cingulate, rostral middle frontal gyrus, entorhinal cortex, and parahippocampal cortical thickness) biomarkers adjusting for age, race, education, and APOE ϵ4 carrier status. Regressions for hippocampal volume additionally adjusted for intracranial volume, while regressions for cortical thickness adjusted for mean thickness (Barnes et al., Reference Barnes, Ridgway, Bartlett, Henley, Lehmann, Hobbs, Clarkson, MacManus, Ourselin and Fox2010; Dhamala et al., Reference Dhamala, Ooi, Chen, Kong, Anderson, Chin, Yeo and Holmes2022). Post-hoc sensitivity analyses adjusted for symptoms of depression in regressions involving parahippocampal regions given evidence of structural changes in these regions related to depression (Papmeyer et al., Reference Papmeyer, Giles, Sussmann, Kielty, Stewart, Lawrie, Whalley and McIntosh2015; Zhou et al., Reference Zhou, Li, Ma, Rossi, Zhu and Li2016). False discovery rate adjustments were made within CSF and MRI models to correct for multiple comparisons.
Results
Rates of SCC
The final sample included 180 former elite football players with a mean age of 57.21 + 8.20 years (Table 1). Global SCC, defined as an AD8 ≥ 2, were reported by the majority of the sample (123 of 180, 68%). 138 (77%) reported subjective memory complaints as measured by CCI ≥ 20, and 77 (43%) reported subjective executive functioning complaints as measured by BRIEF MI T ≥ 65. Overall, 140 (78%) participants reported SCC by any measure.
Correlates of SCC
Across all self-reported measures of SCC (AD8, CCI, and BRIEF MI), former football players with SCC had fewer years of education (AD8: p = .01, CCI: p = .01, BRIEF MI: p = .02) and had higher total scores on the BDI-II (AD8, CCI, and BRIEF MI: p < .001), BAI (AD8, CCI, and BRIEF MI: p < .001), PCL-5 (AD8, CCI, and BRIEF MI: p < .001), ESS (AD8, CCI, and BRIEF MI: p < .001), and BIS-11 (AD8, CCI, and BRIEF MI: p < .001) compared to football players without SCC (Supp. Tables 1–3). Race (White vs. non-White; AD8: p = .26, CCI: p = .97, BRIEF MI: p = .31), APOE ϵ4 carrier status (AD8: p = .06, CCI: p = .44, BRIEF MI: p = .10), age of first exposure to football (AD8: p = .43, CCI: p = .38, BRIEF MI: p = .69), and CHII-R (AD8: p = .24, CCI: p = .23, BRIEF MI: p = .55) did not differ between participants with or without SCC for any measure. Former football players with global SCC were younger (AD8: p = .01) than those without global SCC (Supp. Table 1). Those with subjective memory complaints played more years of football (CCI: p = .03) than those without subjective memory complaints (Supp. Table 2). Former football players with global SCC or subjective memory complaints reported greater alcohol use (AD8: p = .03, CCI: p < .001) than those without global SCC or subjective memory complaints (Supp. Tables 1, 2).
Elastic net regression revealed that BDI-II, BAI, and BIS-11 total scores had the highest model coefficients (i.e., were the strongest correlates of SCC) across all demographic, genetic, athletic, and neuropsychiatric features, though their relative importance varied depending on the SCC measure (Figure 1). BDI-II total score had the highest model coefficient for global SCC and executive dysfunction complaints, while BIS-11 had the highest model coefficient for subjective memory complaints.
Standardized model coefficients from elastic net regression for (A) eight-item ascertain dementia (AD8) – global subjective cognitive complaints (SCC), (B) cognitive change index (CCI) – memory complaints, and (C) behavior rating inventory of executive functioning metacognition index (BRIEF-MI) executive functioning complaints.
Note: Errors bars show standard error for each model coefficient. CCI = Cognitive Change Index, BRIEF MI = Behavior Rating Inventory of Executive Functioning Metacognition Index, AFE = age of first exposure, CHII-R = cumulative head impact index (rotational), BDI-II = Beck Depression Inventory Second Edition, BAI = Beck Anxiety Inventory, PCL-5 = Post-traumatic Stress Disorder Checklist Fifth Edition, AUDIT = Alcohol Use Disorders Identification Test, ESS = Epworth Sleepiness Scale, BIS-11 = Barratt Impulsiveness Scale.

Agreement between self- and informant-reported SCC
133 of the 180 (74%) informants for the football players reported global SCC (AD8 ≥ 2). 60 of the 161 (37%) informants who completed the informant BRIEF reported executive functioning complaints (BRIEF MI T ≥ 65). There was moderate reliability between self- and informant-reported AD8 total scores (ICC = 0.73, 95% confidence interval (CI) [0.65, 0.79]). There was also moderate reliability between self- and informant-reported BRIEF MI T scores (ICC = 0.72, 95% CI [0.63, 0.79]).
On average, informants endorsed more items on the AD8 than the participants’ self-ratings (AD8 mean discrepancy = 0.36, t(178) = 2.33, p = .02, Cohen’s d = 0.17). In contrast, informants responded with lower BRIEF MI T scores than participants’ self-ratings (BRIEF MI T-score mean discrepancy = −2.27, t(160) = −2.24, p = .03, Cohen’s d = −0.18). Negative discrepancy scores (i.e., greater self-ratings compared to informant ratings) were associated with higher levels of depressive symptoms for both the AD8 (r = −0.15, t (177) = −2.02, p = .04) and BRIEF MI (r = −0.22, t (159) = −2.87, p = .005).
Associations between SCC and neuropsychological performance
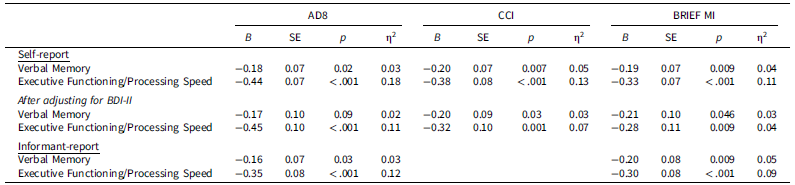
Adjusting for age, race, education, and APOE ϵ4 carrier status, self-reported SCC by all measures were associated with neuropsychological test performances in both verbal memory and executive functioning/processing speed (Table 2). Small effects were observed in the associations between SCC and verbal memory, and medium-to-large effects were observed in the associations between SCC and executive functioning/processing speed. When additionally adjusting for symptoms of depression, associations were attenuated (small to medium effect sizes) but remained significant except for the relationship between AD8 and verbal memory. Informant-reported SCC were also associated with neuropsychological test performances in verbal memory and executive functioning/processing speed, with small effects observed between SCC and verbal memory and medium-to-large effects observed between SCC and executive functioning/processing speed.
Multiple linear regressions of neuropsychological performance in memory and executive functioning/processing speed on subjective cognitive complaints as continuous variables, with and without adjusting for symptoms of depression

Note: AD8 = Eight-item Ascertain Dementia, CCI = Cognitive Change Index, BRIEF MI = Behavior Rating Inventory of Executive Functioning Metacognition Index, BDI-II = Beck Depression Inventory Second Edition. Covariates include age, race, education, and APOE ϵ4 carrier status.
Associations between SCC and biomarkers
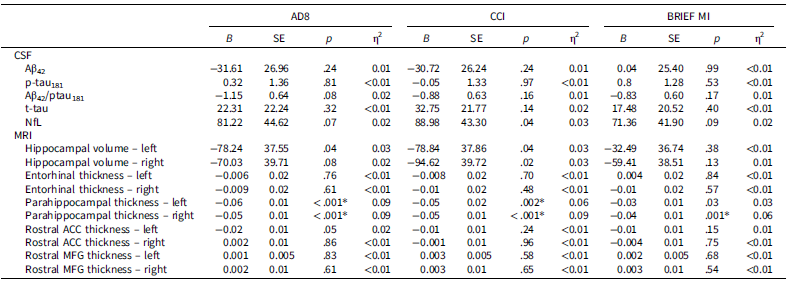
Adjusting for age, race, education, APOE ϵ4 carrier status, and mean cortical thickness, AD8, CCI, and BRIEF MI scores were associated with lower right parahippocampal cortical thickness with medium effect sizes (Table 3). AD8 and CCI were additionally associated with lower left parahippocampal cortical thickness with medium effect sizes. Associations between AD8 and CCI and bilateral parahippocampal cortical thickness were attenuated after adjusting for symptoms of depression but remained significant (AD8 left parahippocampal: p = .001, right hippocampal: p = .04; CCI left parahippocampal: p = .02, right parahippocampal: p = .03). The association between BRIEF MI and right parahippocampal cortical thickness was no longer significant after adjusting for symptoms of depression (p = .26). SCC were not associated with hippocampal volume or cortical thickness in other regions of interest, nor were they associated with any CSF measures.
Multiple linear regressions of cerebrospinal fluid and neuroimaging biomarkers on subjective cognitive complaints

Note: * indicates p-values that remained significant after false discovery rate adjustment for multiple comparisons (i.e., q < .05). AD8 = Eight-item Ascertain Dementia, CCI = Cognitive Change Index, BRIEF MI = Behavior Rating Inventory of Executive Functioning Metacognition Index, CSF = cerebrospinal fluid, NfL = neurofilament light, MRI = magnetic resonance imaging, ACC = anterior cingulate cortex, MFG = middle frontal gyrus. Covariates include age, race, education, APOE ϵ4 carrier status, total intracranial volume (only for hippocampal volume analyses), and mean cortical thickness (only for cortical thickness analyses).
Discussion
In this sample of 180 former elite American football players, 68% reported global SCC, 77% reported subjective memory complaints, and 43% reported subjective executive functioning complaints. SCC were associated with fewer years of education and greater reported neuropsychiatric symptoms, particularly symptoms of depression and impulsivity. Self- and informant-reported SCC were moderately concordant. SCC were associated with neuropsychological test performance in memory and executive functioning/processing speed, and these relationships were attenuated after adjusting for depressive symptoms. SCC were also associated with lower parahippocampal cortical thickness but not with hippocampal volume or any CSF measures.
Factors associated with SCC
Former football players with SCC on average had fewer years of education and reported more symptoms of depression, anxiety, post-traumatic stress, sleepiness, and impulsivity than former football players without SCC. Additionally, those who endorsed global SCC tended to be younger. Neuropsychiatric symptoms (e.g., depression, anxiety, impulsivity) were most strongly associated with SCC, with depression showing the strongest association with global SCC and self-reported executive functioning complaints, and impulsivity showing the strongest association with subjective memory complaints.
Depressive symptoms are well-established as a robust predictor of SCC, particularly of memory, in the general population, normal aging, mild cognitive impairment, TBI, and in former elite athletes (Brett et al., Reference Brett, Nader, Kerr, Chandran, Walton, DeFreese, Guskiewicz and McCrea2022; Bryant et al., Reference Bryant, Kerr, Walton, Barr, Guskiewicz, McCrea and Brett2023; Donnelly et al., Reference Donnelly, Donnelly, Warner, Kittleson and King2018; French et al., Reference French, Lange and Brickell2014; Hohman et al., Reference Hohman, Beason-Held and Resnick2011; Plessow et al., Reference Plessow, Pascual-Leone, McCracken, Baker, Krishnan, Baggish, Connor, Courtney, Nadler, Speizer, Taylor, Weisskopf, Zafonte and Meehan2020; Roberts et al., Reference Roberts, Zafonte, Speizer, Baggish, Taylor, Nadler and Weisskopf2021; Ryu et al., Reference Ryu, Lee, Kim and Lee2016; Sabatini et al., Reference Sabatini, Woods, Ukoumunne, Ballard, Collins and Clare2022; Van Patten et al., Reference Van Patten, Iverson, Terry, Levi and Gardner2021; Zlatar et al., Reference Zlatar, Muniz, Galasko and Salmon2018). Depressive symptoms also predict subjective executive dysfunction (Smit et al., Reference Smit, Koerts, Bangma, Fuermaier, Tucha and Tucha2024). The association between depression and SCC is thought to be explained by oversensitivity to and misinterpretation of normal lapses in cognitive function (Meltzer et al., Reference Meltzer, Kapoor, Fogel, Elbulok-Charcape, Roth, Katz, Lipton and Rabin2017).
Neuropsychiatric symptoms such as impulsivity have been increasingly recognized as risk factors for and symptoms of dementia syndromes (Bateman et al., Reference Bateman, Gill, Hu, Foster, Ruthirakuhan, Sellek, Mortby, Matušková, Ng, Tarawneh, Freund‐Levi, Kumar, Gauthier, Rosenberg, Ferreira de Oliveira, Devanand, Ballard and Ismail2020; Ismail et al., Reference Ismail, Smith, Geda, Sultzer, Brodaty, Smith, Agüera-Ortiz, Sweet, Miller and Lyketsos2016; Sakurai et al., Reference Sakurai, Li, Inamura, Masuoka and Hisatsune2020). Impulsivity has been described as a symptom of neurobehavioral dysregulation (one of the core clinical features of TES) in individuals with substantial exposure to RHI (Katz et al., Reference Katz, Bernick, Dodick, Mez, Mariani, Adler, Alosco, Balcer, Banks, Barr, Brody, Cantu, Dams-O’Connor, Geda, Jordan, McAllister, Peskind, Petersen, Wethe and Stern2021; Pulukuri et al., Reference Pulukuri, Fagle, Trujillo-Rodriguez, van Amerongen, Bernick, Geda, Wethe, Peskind, Katz, Alosco, Palmisano, Tripodis, Adler, Balcer, Reiman, Shenton, Cummings and Stern2025). However, research is still limited regarding how impulsivity relates to SCC and whether RHI may modify any such relationship. This is the first study to demonstrate a relationship between SCC and impulsivity; while impulsivity has been linked to objective cognitive decline in older adults, no older adult or athlete-specific research to date has directly addressed the association between SCC and impulsivity. Taken together, these findings support the importance of assessing not only mood symptoms but also behavioral symptoms when evaluating SCC in former elite athletes with exposure to RHI.
There were no consistent associations observed between SCC and measures of RHI exposure (e.g., years of play, AFE to football, CHII-R). Only total years of football play differed by 1.65 years between those with memory complaints and those without as measured by the CCI. These results suggest that RHI exposure per se may not directly predict SCC in midlife.
Comparing self- and informant-reported SCC
Discrepancies between self-report and informant report of SCC are prominent in early AD, with informant reports showing stronger associations with progression to MCI and dementia (Edmonds et al., Reference Edmonds, Weigand, Thomas, Eppig, Delano-Wood, Galasko, Salmon and Bondi2018; Milanovic et al., Reference Milanovic, Wood-Ross, Butters, Fischer, Flint, Gerretsen, Herrmann, Lanctôt, Mah, Mulsant, Pollock, Rajji and Bowie2023; Peng et al., Reference Peng, Wang, Lin, Lee, Lin, Lin and Wang2023; Pérez-Blanco et al., Reference Pérez-Blanco, Felpete, Patten, Mallo, Pereiro, Campos-Magdaleno and Juncos-Rabadán2022; Ryu et al., Reference Ryu, Kim, Kim, Park, Park, Youn, Lee, Lee, Lee, Jeong, Choi, Han, Kim, Na, Park, Yim and Yang2020). The present study found moderate concordance between self- and informant-reported SCC and that depressive symptoms were associated with greater discrepancies between self- and informant-reported SCC. These results are consistent with past findings that greater discrepancies of self-reported SCC over informant-reported scores have been linked to depression (Scholz & Donders, Reference Scholz and Donders2024). People with depressive symptoms may over-report or overestimate SCC relative to informants and their objective cognitive performance due to a negative cognitive bias (Serra-Blasco et al., Reference Serra-Blasco, Torres, Vicent-Gil, Goldberg, Navarra-Ventura, Aguilar, Via, Portella, Figuereo, Palao, Lam and Cardoner2019). These findings lend support for use of informant-reported SCC measures like the AD8 and BRIEF to corroborate patient reports when significant depressive symptoms are present.
Associations between SCC and objective neuropsychological measures
All self-reported and informant-reported SCC measures were associated with verbal memory and executive functioning/processing speed performance. Associations were attenuated when adjusting for symptoms of depression but most remained significant. These results differ from the findings of Bryant et al. (Reference Bryant, Kerr, Walton, Barr, Guskiewicz, McCrea and Brett2023) and Van Patten et al. (Reference Van Patten, Iverson, Terry, Levi and Gardner2021), who did not observe associations between subjective and objective cognition in former elite athletes. However, their samples were younger (mean age of 38) and fewer of the athletes reported SCC, respectively. The present study’s findings replicate those of Allen et al. (Reference Allen, Cole, Walton, Kerr, Chandran, Mannix, Guskiewicz, Meehan, Echemendia, McCrea and Brett2023), who found associations between subjective and objective cognitive performance in former professional American football players even after adjusting for depressive symptoms. The literature has been mixed on whether relationships between SCC and objective cognitive performance can be fully explained by depression (Burmester et al., Reference Burmester, Leathem and Merrick2016), though population-based studies of older adults have found associations independent of affective symptoms (Benito-León et al., Reference Benito-León, Mitchell, Vega and Bermejo-Pareja2010; Rouch et al., Reference Rouch, Anterion, Dauphinot, Kerleroux, Roche, Barthelemy and Laurent2008). Clinically, these results suggest that in individuals with exposure to RHI, gathering information about SCC would be most useful for older, symptomatic former athletes and SCC should always be considered in the context of mood and behavioral symptoms.
Associations between SCC and CSF and neuroimaging biomarkers
Results of the current study revealed no associations between SCC measures and CSF biomarkers of AD, which is inconsistent with previous studies from the AD literature (Amariglio et al., Reference Amariglio, Mormino, Pietras, Marshall, Vannini, Johnson, Sperling and Rentz2015; Wolfsgruber et al., Reference Wolfsgruber, Jessen, Koppara, Kleineidam, Schmidtke, Frölich, Kurz, Schulz, Hampel, Heuser, Peters, Reischies, Jahn, Luckhaus, Hüll, Gertz, Schröder, Pantel, Rienhoff and Wagner2015). Hallmark AD biomarkers such as CSF Aβ1-42 and p-tau181 have demonstrated limited utility in CTE, and there are not yet validated biomarkers for CTE or that specifically relate to cognitive impairment in TES (Bergauer et al., Reference Bergauer, van Osch, van Elferen, Gyllvik, Venkatesh and Schreiber2022; Da Silva Soyombo et al., Reference Da Silva Soyombo, Rocha, Xavier, Oliveira and Torres2022; Katz et al., Reference Katz, Bernick, Dodick, Mez, Mariani, Adler, Alosco, Balcer, Banks, Barr, Brody, Cantu, Dams-O’Connor, Geda, Jordan, McAllister, Peskind, Petersen, Wethe and Stern2021; Turk et al., Reference Turk, Geada, Alvarez, Xia, Cherry, Nicks, Meng, Daley, Tripodis, Huber, Budson, Dwyer, Kowall, Cantu, Goldstein, Katz, Stern, Alosco, Mez and Stein2022). The relatively younger mean age of participants in the present sample (M = 57.21 ± 8.20) may also partially account for the absence of association with AD-related biomarkers. Further research is needed to elucidate the relationship between CSF biomarker – particularly those useful for detecting CTE after its onset – and subjective and objective cognition in individuals with RHI exposure.
SCC was significantly associated with lower cortical thickness in parahippocampal regions, independent of symptoms of depression. A previous study in this sample found that the former football players showed lower parahippocampal cortical thickness and volume compared to controls without exposure to RHI, even when excluding participants with positive AD biomarkers (Arciniega et al., Reference Arciniega, Baucom, Tuz-Zahra, Tripodis, John, Carrington, Kim, Knyazhanskaya, Jung, Breedlove, Wiegand, Daneshvar, Rushmore, Billah, Pasternak, Coleman, Adler, Bernick, Balcer and Bouix2024). Associations between SCC and MRI markers have been found in individuals with increased risk for dementia or with history of head injuries (Dauphinot et al., Reference Dauphinot, Bouteloup, Mangin, Vellas, Pasquier, Blanc, Hanon, Gabelle, Annweiler, David, Planche, Godefroy, Rivasseau-Jonveaux, Chupin, Fischer, Chêne, Dufouil and Krolak-Salmon2020; Ly et al., Reference Ly, Merritt, Ozturk, Clark, Hanson, Delano-Wood and Sorg2023). These results implicate SCC as a potential risk factor and/or early manifestation of neurodegenerative changes corresponding to memory decline in the setting of RHI exposure, independent of the depression often seen in this population.
Clinical implications
Based on these findings, individuals with exposure to RHI who are concerned about cognitive and behavioral changes later in life (i.e., CTE) would benefit from a comprehensive evaluation that includes validated measures of SCC, objective testing of cognitive performance across domains, and measures of mood (e.g., depression, anxiety) and behavioral (e.g., impulsivity) symptoms. Given the role of depression, anxiety, and impulsivity in SCC and risk of misdiagnosing neurodegenerative disease, clinical evaluations should not rely solely on SCC (Edmonds et al., Reference Edmonds, Delano-Wood, Galasko, Salmon and Bondi2014). Obtaining informant-reported cognitive complaints may be informative in the setting of significant depressive symptoms to evaluate for negative bias in the patient’s self-reported complaints. Use of biomarkers has not yet been validated for CTE but can be helpful in ruling out other neurodegenerative disease processes such as AD.
Treatment of individuals with RHI exposure should include education regarding the state of research surrounding RHI exposure, CTE, and TES. Specifically, it remains unclear whether RHI exposure per se predicts SCC in midlife, and whether SCC in individuals with RHI exposure are linked to future cognitive decline. Nonetheless, individuals with extensive RHI exposure should be advised to monitor and promote their brain health through targeted interventions (e.g., for sleep disruption, pain, substance use) and psychiatric treatment for mental health disorders (Belanger et al., Reference Belanger, Wortzel, Vanderploeg and Cooper2020). Neurobehavioral symptoms have not been strongly associated with p-tau severity in autopsy-confirmed CTE (Alosco et al., Reference Alosco, White, Bell, Faheem, Tripodis, Yhang, Baucom, Martin, Palmisano, Dams-O’Connor, Crary, Goldstein, Katz, Dwyer, Daneshvar, Nowinski, Cantu, Kowall, Stern and Mez2024). However, individuals with a history of head injury or RHI are more likely to develop mental health disorders (Buddenbaum et al., Reference Buddenbaum, Recht, Rodriguez, Newman and Kawata2024; McAllister & McCrea, Reference McAllister and McCrea2017). Considering their impact on SCC, treatment of depression, anxiety, and poor behavioral control should be a prominent focus for this population.
Clinicians should be mindful of potential stigma surrounding the disclosure of mental health and cognitive concerns, particularly among men and former football players, which may lead to underreporting of symptoms. It is important to openly address stigma during discussions with patients and their families while educating them about clinically salient symptoms of brain health decline, modifiable behaviors, and relevant interventions. Clinicians should also be mindful that psychiatric symptoms do not exclude the presence of a neurodegenerative disease.
Limitations
Given the cross-sectional nature of this analysis, causal or directional inference cannot be made. SCC and cognitive impairment on neuropsychological assessment are nonspecific findings and can reflect multiple etiologies including mood, stress, fatigue, pain, and poor sleep (Bryant et al., Reference Bryant, Kerr, Walton, Barr, Guskiewicz, McCrea and Brett2023). SCC may not necessarily indicate a neurodegenerative process, particularly at the individual level, so longitudinal studies are needed to investigate the predictive value of self- and informant-reported SCC to progressive cognitive and neurodegenerative decline in individuals with RHI. Further research is also needed to explore associations between SCC and biomarkers in former football players with and without objective cognitive impairment to inform the utility of biomarkers in SCD in this population.
This study lacked a control group of individuals with SCC without exposure to RHI, as the control group recruited for the DIAGNOSE CTE Research Project were required to be asymptomatic. Future research should ideally include a psychiatric comparison group of participants with similar levels of mood and behavioral concerns but no substantial exposure to RHI. While recruitment in DIAGNOSE CTE was intended to capture former football players across the spectrum of symptom severity, there was likely selection bias in that those who have been exposed to media regarding the deleterious effects of head injuries and are more concerned about their own risk of CTE are more likely to engage in this type of research. Thus, the present findings may overestimate the rates and severity of SCC in the population of former football players and may not be generalizable to former football players who are asymptomatic or averse to seeking help due to stigma. Given the restricted demographics (e.g., highly educated male American football players with 6+ years of organized play) of this study’s sample, findings also may not be generalizable to and should be replicated in women and in other sources of RHI including military exposure, intimate partner violence, and other contact and collision sports with varying levels of play.
Conclusion
SCCs in former American football players with RHI exposure were most strongly associated with depression, anxiety, and impulsivity. Self-reported SCC generally aligned with informant reports. Greater SCC was associated with worse memory and executive functioning on neuropsychological testing as well as lower parahippocampal thickness, suggesting that SCC may be a marker of cognitive decline and neurodegeneration. Individuals with exposure to RHI would benefit from comprehensive evaluations including both subjective and objective measures of cognition while considering the impact of mood and behavioral symptoms. Future research should explore how SCC and their relationships to objective clinical measures in individuals with RHI exposure may differ from other at-risk populations such as preclinical AD.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S1355617726101866.
Acknowledgements
We thank the research participants and their families whose help and willingness to contribute to the DIAGNOSE CTE Research Project made this work possible.
Funding statement
This work was supported by grants from the National Institutes of Health (U01NS093334; P30AG072978; R01NS078337; K23NS102399; P30AG019610; K01AG054762; R01NS100952; RF1NS122854). This publication was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through BU-CTSI Grant Number 1UL1TR001430. The primary funding source is the National Institute of Neurological Disorders and Stroke (NINDS), through a U01 Research Project Cooperative Agreement (U01NS093334). HZ is a Wallenberg Scholar and a Distinguished Professor at the Swedish Research Council supported by grants from the Swedish Research Council (#2023-00356, #2022-01018, and #2019-02397), the European Union’s Horizon Europe research and innovation program under grant agreement No 101053962, and Swedish State Support for Clinical Research (#ALFGBG-71320). JLC is supported by NIGMS grant P20GM109025; NIA grant R35AG71476; NIA R25 AG083721-01; Alzheimer’s Disease Drug Discovery Foundation (ADDF); Ted and Maria Quirk Endowment; Joy Chambers-Grundy Endowment. IK is supported by ERC Starting Grant (804326) and NINDS R01 NS100952. KB is supported by the Swedish Research Council (#2017-00915 and #2022-00732), the Swedish Alzheimer Foundation (#AF-930351, #AF-939721, #AF-968270, and #AF-994551), Hjärnfonden, Sweden (#ALZ2022-0006, #FO2024-0048-TK-130 and FO2024-0048-HK-24), the Swedish state under the agreement between the Swedish government and the County Councils, the ALF-agreement (#ALFGBG-965240 and #ALFGBG-1006418), the European Union Joint Program for Neurodegenerative Disorders (JPND2019-466-236), the Alzheimer’s Association 2021 Zenith Award (ZEN-21-848495), the Alzheimer’s Association 2022-2025 Grant (SG-23-1038904 QC), La Fondation Recherche Alzheimer (FRA), Paris, France, the Kirsten and Freddy Johansen Foundation, Copenhagen, Denmark, Familjen Rönströms Stiftelse, Stockholm, Sweden, and an anonymous filantropist and donor.
Competing interests
J. S. Adler, M. T. Ly, E. Yhang, E. Peskind, and Y. Tripodis report no disclosures relevant to the manuscript; C. H. Adler consulted for Avion, CND Life Sciences, Jazz, and Precon Health; L. J. Balcer is Editor-in-Chief of the Journal of Neuro-Ophthalmology; C. Bernick receives research support from the Ultimate Fighting Championship, Top Rank promotions, Haymon Boxing, Las Vegas Raiders, and Professional Bull Riders, and is a paid consultant for Aurora Concussion Therapy Systems, Inc. (St. Paul, MN); H. Zetterberg has served at scientific advisory boards and/or as a consultant for Abbvie, Acumen, Alector, Alzinova, ALZPath, Amylyx, Annexon, Apellis, Artery Therapeutics, AZTherapies, Cognito Therapeutics, CogRx, Denali, Eisai, Enigma, LabCorp, Merry Life, Nervgen, Novo Nordisk, Optoceutics, Passage Bio, Pinteon Therapeutics, Prothena, Quanterix, Red Abbey Labs, reMYND, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures in symposia sponsored by Alzecure, BioArctic, Biogen, Cellectricon, Fujirebio, Fujirebio, Lilly, Novo Nordisk, Roche, and WebMD, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work); K. Blennow reports having served as a consultant and at advisory boards for Abbvie, AC Immune, ALZPath, AriBio, Beckman-Coulter, BioArctic, Biogen, Eisai, Lilly, Moleac Pte. Ltd, Neurimmune, Novartis, Ono Pharma, Prothena, Quanterix, Roche Diagnostics, Sunbird Bio, Sanofi and Siemens Healthineers; has served at data monitoring committees for Julius Clinical and Novartis; has given lectures, produced educational materials and participated in educational programs for AC Immune, Biogen, Celdara Medical, Eisai and Roche Diagnostics; and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program, outside the work presented in this paper; S. J. Banks reports no disclosures relevant to the manuscript; W. B. Barr provides expert witness testimony in legal cases involving concussion and CTE; J. V. Wethe reports no disclosures relevant to the manuscript; M. W. Bondi reports no disclosures relevant to the manuscript; L. Delano-Wood reports no disclosures relevant to the manuscript; R. C. Cantu is a Senior Advisor to the NFL Head Neck & Spine Committee; Vice President, National Operating Committee on Standards for Athletic Equipment; and Chair, Scientific Advisory Committee, Co-Founder, and Medical Director, Concussion Legacy Foundation. He is a member of the Medical Science Committee for the National Collegiate Athletic Association Student-Athlete Concussion Injury Litigation, and he receives royalties for published books from Houghton Mifflin Harcourt; M. J. Coleman reports no disclosures relevant to the manuscript; D. W. Dodick served as consultant for: Amgen, Atria, CapiThera Ltd., Cerecin, Ceruvia Lifesciences LLC, CoolTech, Ctrl M, Allergan, AbbVie, Biohaven, Escient, GlaxoSmithKline, Halion, Lundbeck, Eli Lilly, Novartis, Impel, Satsuma, Theranica, WL Gore, Genentech, Nocira, Perfood, Praxis, AYYA Biosciences, Revance, Pfizer; received honoraria from: American Academy of Neurology, Headache Cooperative of the Pacific, Headache Cooperative of New England, Canadian Headache Society, MF Med Ed Research, Biopharm Communications, CEA Group Holding Company (Clinical Education Alliance LLC), Teva (speaking), Amgen Japan (speaking), Eli Lilly Canada (speaking), Lundbeck (speaking), Pfizer (speaking), Vector Psychometric Group, Clinical Care Solutions, CME Outfitters, Curry Rockefeller Group, DeepBench, Global Access Meetings, KLJ Associates, Academy for Continued Healthcare Learning, Majallin LLC, Medlogix Communications, Medica Communications LLC, MJH Lifesciences, Miller Medical Communications, WebMD Health/Medscape, Wolters Kluwer, Oxford University Press, Cambridge University Press; serves on the board (non-profit) for: American Brain Foundation, American Migraine Foundation, ONE Neurology, Precon Health Foundation, Global Patient Advocacy Coalition, Atria Health Collaborative, Atria Academy of Science and Medicine, Arizona Brain Injury Alliance, Domestic Violence HOPE Foundation/Panfila, CSF Leak Foundation; receives research support from: Department of Defense, National Institutes of Health, Henry Jackson Foundation, Sperling Foundation, American Migraine Foundation, Henry Jackson Foundation, Patient Centered Outcomes Research Institute (PCORI); holds stock options/shareholder/patents/board of directors in: Ctrl M (options), Aural analytics (options), Axon Therapeutics (board/options), ExSano (options), Palion (options), Keimon Medical (Options), Man and Science, Healint (options), Theranica (options), Second Opinion/Mobile Health (options), Epien (options), Nocira (options), Matterhorn (shares), Ontologics (shares), King-Devick Technologies (options/board), Precon Health (options/board), ScotiaLyfe (Board), EigenLyfe (Options/Board), AYYA Biosciences (options), Axon Therapeutics (options/board), Cephalgia Group (options/board), Atria Health (options/employee); holds patent 17189376.1-1466:vTitle: Onabotulinum Toxin Dosage Regimen for Chronic Migraine Prophylaxis (Non-royalty bearing) and has patent application submitted for Synaquell® (Precon Health); D. H. Daneshvar reports no disclosures relevant to the manuscript; M. D. McClean reports no disclosures relevant to the manuscript; J. Mez reports no disclosures relevant to the manuscript; J. N. Palmisano reports no disclosures relevant to the manuscript; B. Martin reports no disclosures relevant to the manuscript; A. P. Lin is a paid consultant to Agios Pharmaceuticals (Cambridge, MA, USA), Biomarin Pharmaceuticals (Novato, CA, USA), and Moncton MRI (Moncton, Canada). He is the co-founder of BrainSpec, Inc.; I. K. Koerte receives research funding from Abbott Inc. and receives royalties for book chapters published by Thieme Publishers. Her spouse is managing board member of Siemens AG, and she thus holds stock options at Siemens and Siemens Healthineers; S. Bouix reports no disclosures relevant to the manuscript; J. L. Cummings has provided consultation to Acadia, Acumen, ALZpath, Annovis, Aprinoia, Artery, Biogen, Biohaven, BioXcel, Bristol-Myers Squib, Eisai, Fosun, GAP Foundation, Green Valley, Janssen, Karuna, Kinoxis, Lighthouse, Lilly, Lundbeck, LSP/eqt, Merck, MoCA Cognition, New Amsterdam, Novo Nordisk, Optoceutics, Otsuka, Oxford Brain Diagnostics, Praxis, Prothena, ReMYND, Roche, Scottish Brain Sciences, Signant Health, Simcere, sinaptica, TrueBinding, and Vaxxinity pharmaceutical, assessment, and investment companies; M. E. Shenton reports no disclosures relevant to the manuscript; E. M. Reiman is a compensated scientific advisor for Alzheon, Denali, Cognition Therapeutics, Valley, Retromer Therapeutics, and Vaxxinity, and a co-founder of ALZpath; R. A. Stern is a member of the Board of Directors of King-Devick Technologies, Inc. (Chicago, IL, USA), and he receives royalties for published neuropsychological tests from Psychological Assessment Resources, Inc. (Lutz, FL, USA); M. L. Alosco reports no disclosures relevant to the manuscript.