


Introduction
Long-term residential care (LTRC) is a place of residence and work in which older adults and staff share a right to safety from violence; however, researchers have documented an alarming prevalence of various forms of violence in LTRC (Banerjee et al., Reference Banerjee, Daly, Armstrong, Szebehely, Armstrong and Lafrance2012; Brophy et al., Reference Brophy, Keith and Hurley2019; Daly et al., Reference Daly, Banerjee, Armstrong, Armstrong and Szebehely2011; McDonald et al., Reference McDonald, Sheppard, Hitzig, Spalter, Mathur and Mukhi2015; Yang et al., Reference Yang, Liu, Pien, Yang and Cheng2025). Staff working in LTRC are often held responsible for protecting residents from abuse and neglect while also protecting themselves and their co-workers from workplace violence (Funk et al., Reference Funk, Spencer and Herron2021; Novek et al., Reference Novek, Herron, Funk, Aubrecht, Spencer and Luo2022). In addition, staff are trained to anticipate and respond to responsive behaviors from residents living with dementia, which may be experienced as violent by staff and other residents (Dupuis et al., Reference Dupuis, Wiersma and Loiselle2012; Herron & Rosenberg, Reference Herron and Rosenberg2019). This puts staff in a unique position to describe, explain, and inform solutions to make LTRC a safer place to live and work.
Existing research on violence in LTRC is often focused on violence from one group toward others (e.g., from residents, residents living with dementia, staff, family members, or co-workers). Moreover, different terms are often used to describe violence from each distinct group (e.g., violence, responsive behaviours, abuse, conflict, and incivility). This siloing can, in turn, contribute to a fragmented research and policy environment. Specifically, the frequency and nature of different forms of violence can be obscured by different terms and scales of analysis, and relationships between different forms of violence are not well understood. As such, responses to violence may be less effective (Novek et al., Reference Novek, Herron, Funk, Aubrecht, Spencer and Luo2022). Furthermore, such research silos may make it harder to identify contextual influences on violence within LTRC. To begin to address this challenge, our sequential mixed method study (a) documents the frequency of multiple forms of violence directed toward staff by multiple groups (i.e., residents, family carers, and co-workers) in two Canadian provinces and (b) explores how staff understand these multiple forms of violence from multiple groups, using a contextualized analysis of descriptions of contributing factors. Drawing on our findings and conceptualizing violence in LTRC as complex, multi-directional, and best explored in the setting as a whole (rather than narrowing in on a single relationship), we identify a lack of trust, resources, and support for relational care as conditions influencing all of the forms of violence across all of the relationships examined in this study.
Connecting forms of violence across relationships in LTRC
The term violence generally refers to psychological, physical, and/or sexual acts that may cause harm to another person. Initially, most research on violence in LTRC focused on individual acts with limited consideration of the role of social practices, institutional culture, and environment on violence (Enmarker et al., Reference Enmarker, Olsen and Hellzen2011). Over the last two decades, researchers have begun to describe the conditions of work and care in LTRC as a form of structural violence or slow violence that causes harm by inhibiting individual self-development and self-expression (Banerjee et al., Reference Banerjee, Daly, Armstrong, Szebehely, Armstrong and Lafrance2012; Herron & Wrathall, Reference Herron and Wrathall2018; Herron et al., Reference Herron, Spencer, Novek, Funk, Kelly and Aubrecht2024). This structural lens pushes researchers to see different forms of violence in the context of LTRC as related to, and shaped by, broader overarching conditions. While this theoretical framing has informed research on violence toward staff from residents, it has not been applied to violence in other relationships in LTRC, such as conflict with family members. We review these separate literatures below.
There is substantial research on violence and responsive behaviors from residents directed toward staff, documenting frequency and structural factors (Song et al., Reference Song, Nassur, Rupasinghe, Haq, Boström, Reid, Andersen, Wagg, Hoben, Goodarzi, Squires, Estabrooks and Weeks2023). A Canadian study from 2012 found 90 per cent of staff members reported experiencing physical violence from a resident or relative; one-third were ‘criticized or told off’ every day, and one-third experienced ‘unwanted sexual attention’ on a nearly daily basis (Banerjee et al., Reference Banerjee, Daly, Armstrong, Szebehely, Armstrong and Lafrance2012: 393). A more recent study of nurses’ experiences of violence in British Columbia, Canada, found that LTRC nurses experienced more violence than nurses in other sectors, and rates of reported violence have increased compared to two decades ago (Havaei et al., Reference Havaei, MacPhee and Ma2020). Researchers have attributed the prevalence of violence in LTRC to a range of factors such as inadequate staffing levels, high workloads, inadequate training, lack of time to relate to residents on a personal level, and rushing care (Banerjee et al., Reference Banerjee, Daly, Armstrong, Szebehely, Armstrong and Lafrance2012; Brophy et al., Reference Brophy, Keith and Hurley2019; Song et al., Reference Song, Nassur, Rupasinghe, Haq, Boström, Reid, Andersen, Wagg, Hoben, Goodarzi, Squires, Estabrooks and Weeks2023). Notably, staff often avoid formally reporting violence they experience from residents in the workplace due to management being dismissive, excessive reporting requirements, fear of being blamed for the incident, and concerns about loss of employment (Banerjee et al., Reference Banerjee, Daly, Armstrong, Szebehely, Armstrong and Lafrance2012; Brophy et al., Reference Brophy, Keith and Hurley2019; Song et al., Reference Song, Nassur, Rupasinghe, Haq, Boström, Reid, Andersen, Wagg, Hoben, Goodarzi, Squires, Estabrooks and Weeks2023). As such, independent mixed methods analysis is important for more accurately capturing different forms and frequencies of violence and factors contributing to violence from different actors.
Less is known about violence that staff experience from family carers, although there is extensive literature on ‘conflicts’ or disagreements between family carers and staff. Family carers of LTRC residents play a vital role in care, providing insights into residents’ lives prior to admission, providing direct care while visiting, and working with staff to ensure their family member’s physical, social, and emotional needs are met (Barken et al., Reference Barken, Daly and Armstrong2017; Bauer et al., Reference Bauer, Fetherstonhaugh, Tarzia and Chenco2014). However, family carers and staff sometimes disagree on how to meet care needs (Bauer et al., Reference Bauer, Fetherstonhaugh, Tarzia and Chenco2014). Staff often navigate tensions between facility guidelines and requests from family members (Abrahamson et al., Reference Abrahamson, Suitor and Pillemer2009). Staff can experience family carer expectations as unrealistic and demanding in the resource-strained context of their workplace (Train et al., Reference Train, Nurock, Manela, Kitchen and Livingston2005). The greater the discrepancy between family expectations and actual practice, the more conflict occurs (Abramson et al., Reference Abrahamson, Suitor and Pillemer2009; Bauer et al., Reference Bauer, Fetherstonhaugh, Tarzia and Chenco2014). In addition, when staff do not have enough time to perform care, they report having more conflict with family carers (Abrahamson et al., Reference Abrahamson, Suitor and Pillemer2009). When residents witness conflict between family and staff, it can be distressing, and frequent experiences of family/staff conflict are associated with low levels of job satisfaction, symptoms of depression among staff, and higher levels of staff burnout (Abramson et al., 2009; Dymchuk et al., Reference Dymchuk, Mirhashemi, Chamberlain, Beeber and Hoben2023; Falzarano et al., Reference Falzarano, Reid, Schultz, Meador and Pillemer2020). Although the term conflict is used in this literature, staff may experience conflict as a form of relational violence, or it may escalate into psychological violence (e.g., yelling and swearing). Furthermore, using the term conflict, instead of violence, may inadvertently minimize staff experiences of violence from family carers. Importantly, these experiences of violence may influence other relationships and acts of violence within the facility and are clearly related to organizational and structural conditions.
Many studies have shown that LTRC staff experience various forms of psychological and relational violence from co-workers; however, this form of violence is usually described using the terms bullying and incivility (Cooke & Baumbusch, Reference Cooke and Baumbusch2021; Johnston et al., Reference Johnston, Phanhtharath and Jackson2010; Mammen et al., Reference Mammen, Lam and Hills2023). Newer staff may experience bullying and incivility from senior staff asserting their power over them, for example, by refusing to help them or answer their questions, belittling them when they ask for help, and intimidating them (Booi et al., Reference Booi, Sixsmith, Chaudhury, O’Connor, Young and Sixsmith2021; Cassie & Crank, Reference Cassie and Crank2018; Pickering et al., Reference Pickering, Nurenberg and Schiamberg2017). Bullying can also include other forms of psychological violence, continual criticism, sarcasm, racism, and fabricating complaints (Campbell, Reference Campbell2016; Johnston et al., Reference Johnston, Phanhtharath and Jackson2010). Some research has found that staff members were more likely to be targeted for bullying when they performed at a higher level than the other employees, or they were already emotionally exhausted, or perceived as less dedicated to their work (Booi, Reference Booi, Sixsmith, Chaudhury, O’Connor, Young and Sixsmith2021; Cassie & Crank, Reference Cassie and Crank2018). Being chronically bullied can influence attentiveness to resident care (Hogh et al., Reference Hogh, Baernholdt and Clausen2018). LTRC staff also experience more subtle, insidious, passive-aggressive behaviors with ambiguous intent to harm (Cooke & Baumbusch, Reference Cooke and Baumbusch2022). Cooke and Baumbusch (Reference Cooke and Baumbusch2021) found that health care aides experienced peer incivility on a near-daily basis. Coworkers’ reputations among families were also compromised by staff blaming inadequate care on their coworkers in front of the residents’ families (Cooke & Baumbusch, Reference Cooke and Baumbusch2022). Chronic staffing shortages, staffing arrangements, and workload issues can contribute to instances of peer incivility toward health care aides (Cooke et al., Reference Cooke, Murray, Baumbusch and Kelly2019).
It is clear from the literature that various forms of violence take place in LTRC, albeit each with different terminology (e.g., violence, responsive behaviours, family conflict, bullying), measures, literature, and policies. However, few studies report on concrete acts or violent events in context, which may contribute to under-reporting and a lack of understanding of the way these forms of violence manifest together. Our study seeks to analyse the prevalence and context of violence in LTRC using a common language across relationships.
Research design
To explore violent situations in LTRC, we used a team-based comparative case study approach (Herron et al., Reference Herron, Novek, Kruth, Spencer, Funk, Aubrecht, Kelly, Weeks and Brownridge2021). In this analysis, we focused on two of the methods employed in the case study: surveys and interviews, using an exploratory mixed methods approach (Ivankova et al., Reference Ivankova, Creswell and Stick2006; Subedi, Reference Subedi2016).
After obtaining ethics approval from multiple universities and regional health authorities, a purposeful sample of staff who lived in Manitoba and Nova Scotia and worked in LTRC was recruited. Posters and emails with a link to an online survey were sent to relevant organizations (e.g., health care worker unions, long-term care organizations) and posted on websites and social media, asking staff to help researchers understand factors influencing violence and safety for those who receive and provide long-term care. All surveys were completed online, and recruitment continued until no further participants responded (between July 2021 and April 2022 in Manitoba and between April 2022 and January 2023 in Nova Scotia).
The survey instrument was reviewed by a knowledge user advisory committee, including long-term care organizations and union representatives, and an accessibility consultant to ensure the relevance and accessibility of questions. The survey included demographic questions about age, gender, racial identification, and urban or rural residence. Following standards on the use of race-based data from the Canadian Institute for Health Information (2022), we asked ‘Which of the following best describes your racial identification’ (with varying response options), because the social construct of race and processes of racialization may influence the forms and frequency of violence they experience, specifically violence directly as a result of physical appearance or racial difference, to which white-presenting persons are not exposed. However, we did not ask participants about their ethnicity. In addition, no questions were asked about the size of the facility in which people worked; however, both provinces have a mixture of small (less than 80 beds), medium (80–120 beds), and large (more than 120 beds) facilities (Canadian Institute for Health Information, 2026). To measure the frequency of violence, we included a modified version of the Conflict Tactics Scale (CTS; Straus et al., Reference Straus, Hamby, Boney-McCoy and Sugarman1996), which asked participants about different acts or events rather than using terms such as physical or psychological violence that are more open to interpretation. We suspected that the frequency of violence in the original instrument might produce a ceiling effect and therefore changed the frequencies in our instrument to provide a broader range. We also added items about sexual violence not contained in the CTS that were more appropriate for the LTRC environment. Importantly, the value of using this type of scale is that it is based on concrete acts/items, which makes it more difficult for respondents to under-report violence by rationalizing events. The survey concluded by asking participants if they wished to take part in a follow-up interview.
Survey participants who expressed interest in being interviewed and reported experiencing at least one form of violence were contacted by the research team to participate in a telephone or video interview between July 2021 and September 2023. Remote interviews were required at the outset of the project due to COVID-19 pandemic restrictions, but they also offered participants a degree of privacy and anonymity while discussing experiences of violence. Interviews followed a guide that asked participants to describe their interactions with co-workers, family members, and residents, as well as asking about training and practices in relation to violence prevention in their workplace. Building on the survey data, participants were asked if they felt comfortable describing a violent situation that they reported in the survey (e.g., I noticed in your survey that you reported being insulted weekly, would you feel comfortable describing a situation when that happened to you?). Finally, participants were also asked what changes they thought might prevent violence in LTRC. On average, the interviews lasted approximately 1 hour and 20 minutes, and all interviews were digitally recorded and transcribed verbatim to enhance confirmability.
Survey data were analysed descriptively by running frequencies and crosstabulations with chi-square tests of significance. Chi-square is an appropriate test of association between categorical variables in non-parametric data (e.g., cf. McHugh, Reference McHugh2013). The qualitative analysis of interview data involved developing a coding protocol that outlined the coding process and identified deductive categories based on the survey constructs (e.g., training, violent situations, and physical violence). Next, the research team read through the transcripts together, developing inductive codes that either aligned with survey constructs or emerged as something new and distinct (e.g., family relations and training on the job). After creating transcript summaries for six interviews and developing preliminary codes to review as a team, each subsequent transcript was coded by two team members using the full codebook. The coding team met weekly to discuss coding notes and impressions and ensure consistency in the coding process. Following an explanatory sequential mixed methods design (Ivankova et al., Reference Ivankova, Creswell and Stick2006; Subedi, Reference Subedi2016), we outline the quantitative results first and then explore the qualitative themes that helped to explain some of these patterns, including mistrust and lack of understanding of LTRC and dementia care, impractical training and working conditions, and insufficient resources and inflexible dementia care. In the findings below, participants have been given pseudonyms to protect their confidentiality.
Findings
Of the 240 survey respondents, 95 were from Manitoba, and 145 were from Nova Scotia. Almost half of the survey participants (46.9%) were nurses, 27.5% were health care aides or continuing care assistantsFootnote 1, and 25.8% worked in other areas such as recreation and housekeeping. While 33.3% of survey respondents chose not to report their age, of the remaining respondents, 43.8% were 50 years of age and older, 31.9% were 36–49 years of age, and 24.4% were 18–35 years of age. Most participants were women (89.2%). Of those who disclosed their racial identification, 77% (n = 185) identified as white, and the remaining participants identified as belonging to a racialized group (e.g., 10 participants identified as East/Southeast Asian, 8 identified as Black, 4 identified as South Asian, and 3 identified as Metis, 2 identified as Middle Eastern, and 2 Identified as Indigenous, and 2 identified as First Nations).Footnote 2 In terms of preparatory training, 39.7% obtained a bachelor’s or graduate degree, and 60.3% held a high school or college diploma. Half (50.0%) of the respondents worked 40 hours or more a week, while 21.8% worked 30–39 hours per week, and 28.2% worked 29 hours per week or less. The majority of participants (62.4%) worked in urban centres with a population of more than 10,000 people.
The 29 interview participants’ demographic profile generally mirrors the broader trends in the recruitment survey, with the exception that 19 participants were from Manitoba and 10 were from Nova Scotia. Of the interview participants, 18 were nurses, six were health care aides, two were recreation staff, and three were housekeeping staff. Most interview participants identified as women (N = 26) and white (N = 21), while smaller numbers identified as Asian (N = 2), Black (N = 2), or Indigenous (N = 1).
Frequency of violence
Based on the modified conflict tactics scale, we report on the frequency of psychologicalFootnote 3, physical, and sexual violence across different relationships in LTRC. Almost all survey respondents (98.2%) reported experiencing at least one form of violence within the past year. Violence from residents was the most common source of violence, with 97.2% of staff experiencing at least one form of violence from residents during the past year. Nevertheless, over half of the staff surveyed (53.2%) reported experiencing at least one form of violence from family carers, and close to half (42.5%)Footnote 4 of staff reported experiencing some form of violence from coworkers within the previous year. Tables 1 and 2 provide complete details of reported violence from residents, family, and coworkers.
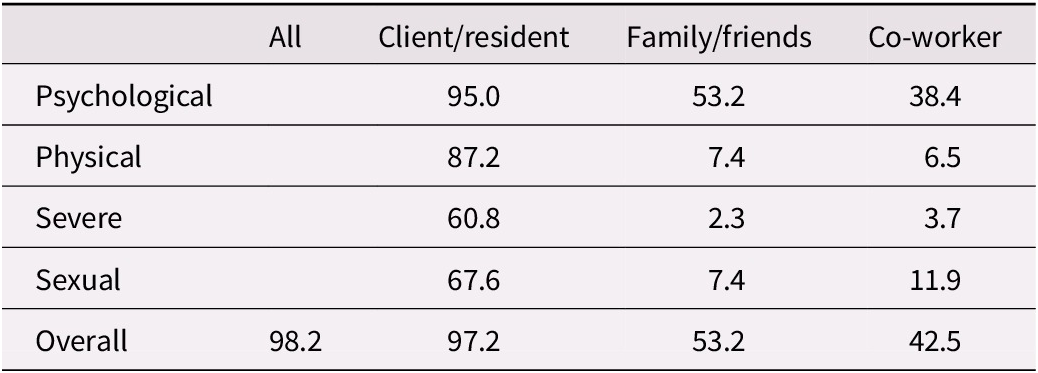
Past year prevalence rates of violent victimization across group types (%; N = 240)

Table 1. Long description
The table lists five rows for types of violent victimization: psychological, physical, severe, sexual, and overall. Columns are All, Client or resident, Family or friends, and Co-worker. For psychological victimization, rates are 95.0 percent for Client or resident, 53.2 percent for Family or friends, and 38.4 percent for Co-worker. For physical, rates are 87.2 percent for Client or resident, 7.4 percent for Family or friends, and 6.5 percent for Co-worker. For severe, rates are 60.8 percent for Client or resident, 2.3 percent for Family or friends, and 3.7 percent for Co-worker. For sexual, rates are 67.6 percent for Client or resident, 7.4 percent for Family or friends, and 11.9 percent for Co-worker. The overall prevalence rates are 98.2 percent for All, 97.2 percent for Client or resident, 53.2 percent for Family or friends, and 42.5 percent for Co-worker. The highest rates across all types are consistently found in the Client or resident group.
Past year prevalence of individual forms of violence from various groups (%)
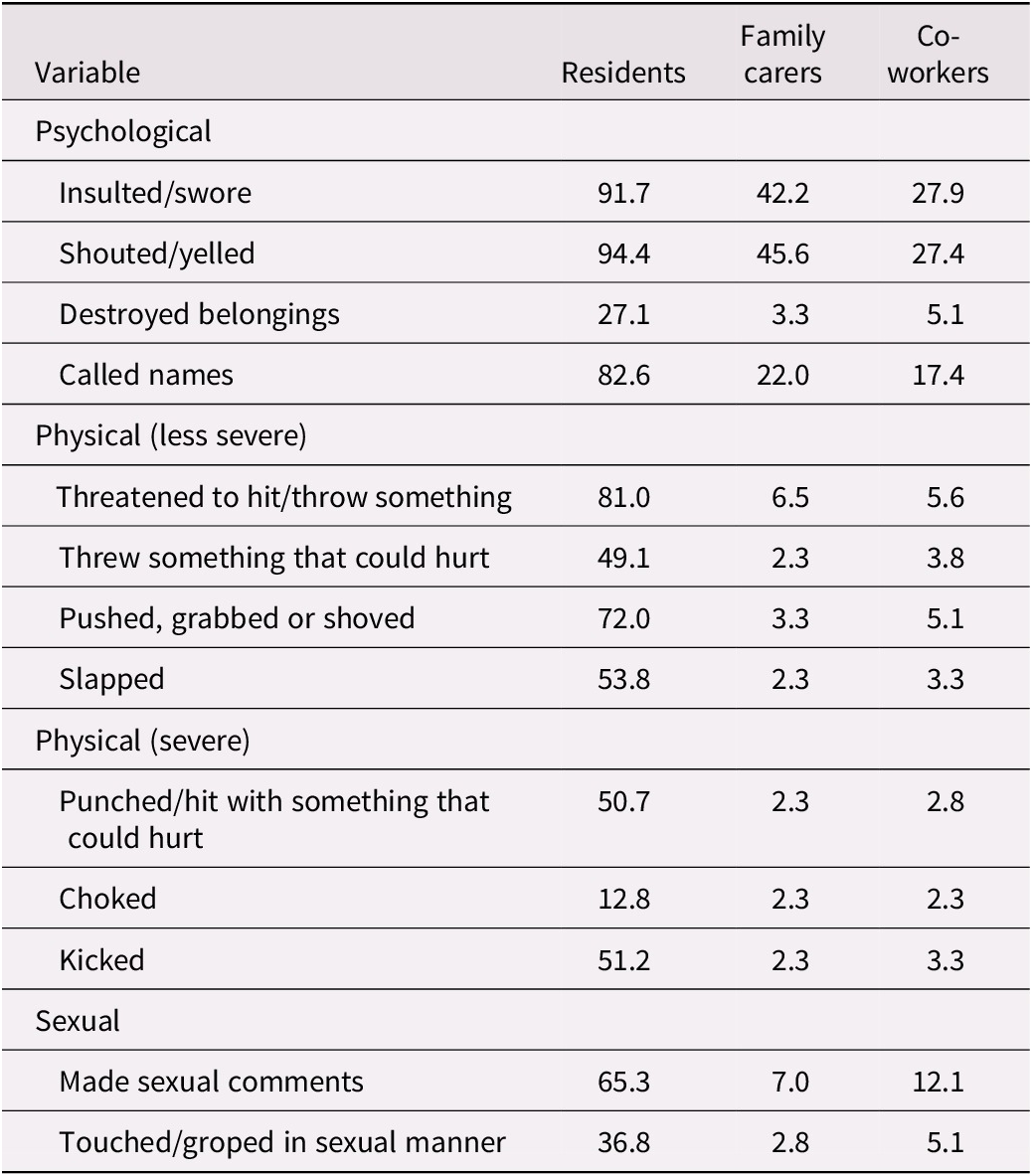
Table 2. Long description
The table has four columns: Variable, Residents, Family carers, Co-workers. For psychological violence, insulted or swore: residents 91.7 percent, family carers 42.2 percent, co-workers 27.9 percent; shouted or yelled: residents 94.4 percent, family carers 45.6 percent, co-workers 27.4 percent; destroyed belongings: residents 27.1 percent, family carers 3.3 percent, co-workers 5.1 percent; called names: residents 82.6 percent, family carers 22.0 percent, co-workers 17.4 percent. For physical (less severe), threatened to hit or throw something: residents 81.0 percent, family carers 6.5 percent, co-workers 5.6 percent; threw something that could hurt: residents 49.1 percent, family carers 2.3 percent, co-workers 3.8 percent; pushed, grabbed or shoved: residents 72.0 percent, family carers 3.3 percent, co-workers 5.1 percent; slapped: residents 53.8 percent, family carers 2.3 percent, co-workers 3.3 percent. For physical (severe), punched or hit with something that could hurt: residents 50.7 percent, family carers 2.3 percent, co-workers 2.8 percent; choked: residents 12.8 percent, family carers 2.3 percent, co-workers 2.3 percent; kicked: residents 51.2 percent, family carers 2.3 percent, co-workers 3.3 percent. For sexual violence, made sexual comments: residents 65.3 percent, family carers 7.0 percent, co-workers 12.1 percent; touched or groped in sexual manner: residents 36.8 percent, family carers 2.8 percent, co-workers 5.1 percent. Residents consistently report the highest prevalence across all forms and subtypes.
Violence from family carers
Psychological violence from family carers was the most commonly reported form of violence staff experienced in this relationship, experienced by 53.2% of participants (see Table 1), including but not limited to being insulted/sworn at or shouted/yelled at (see Table 2). Nurses (66.4%) and health care aides (44.4%) were significantly more likely to report psychological violence from family carers than other staff members (35.2%; p < .001) as were respondents who reported working with greater numbers of residents on a daily basis (30+ residents = 60.9% vs. < 30 residents = 45.4%; p < .05) and caring for higher proportions of residents with diagnoses of dementia or cognitive impairment (75% + = 62%; 50–74% = 52.5%; < 50% = 26.5%; p < .01; see Table 3).
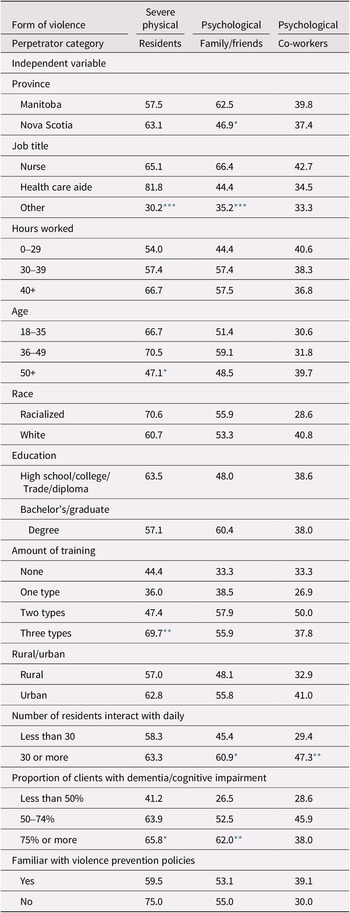
Independent variables by severe physical violence from residents and psychological violence from family/friends and co-workers in the year prior to the study (%)

Table 3. Long description
The table lists independent variables in the first column, with subcategories indented under each. The next three columns show percentages for severe physical violence by residents, psychological violence by family/friends, and psychological violence by co-workers, respectively. For Province, Manitoba shows 57.5, 62.5, and 39.8; Nova Scotia shows 63.1, 46.9 (asterisk, p less than .05), and 37.4. For Job title, Nurse: 65.1, 66.4, 42.7; Health care aide: 81.8, 44.4, 34.5; Other: 30.2 (triple asterisk, p less than .001), 35.2 (triple asterisk), 33.3. For Hours worked, 0–29: 54.0, 44.4, 40.6; 30–39: 57.4, 57.4, 38.3; 40 plus: 66.7, 57.5, 36.8. For Age, 18–35: 66.7, 51.4, 30.6; 36–49: 70.5, 59.1, 31.8; 50 plus: 47.1 (asterisk), 48.5, 39.7. For Race, Racialized: 70.6, 55.9, 28.6; White: 60.7, 53.3, 40.8. For Education, High school/college/trade/diploma: 63.5, 48.0, 38.6; Bachelor’s/graduate degree: 57.1, 60.4, 38.0. For Amount of training, None: 44.4, 33.3, 33.3; One type: 36.0, 38.5, 26.9; Two types: 47.4, 57.9, 50.0; Three types: 69.7 (double asterisk, p less than .01), 55.9, 37.8. For Rural/urban, Rural: 57.0, 48.1, 32.9; Urban: 62.8, 55.8, 41.0. For Number of residents interacted with daily, Less than 30: 58.3, 45.4, 29.4; 30 or more: 63.3, 60.9 (asterisk), 47.3 (double asterisk). For Proportion of clients with dementia/cognitive impairment, Less than 50 percent: 41.2, 26.5, 28.6; 50–74 percent: 63.9, 52.5, 45.9; 75 percent or more: 65.8 (asterisk), 62.0 (double asterisk), 38.0. For Familiar with violence prevention policies, Yes: 59.5, 53.1, 39.1; No: 75.0, 55.0, 30.0. Asterisks indicate statistical significance: one asterisk for p less than .05, two for p less than .01, three for p less than .001.
* p < .05.
** p < .01.
*** p < .001.
Mistrust and lack of understanding of LTRC and dementia care
During interviews, staff described swearing, yelling, and threats from family carers as particularly harmful and almost impossible to address, insofar as they were grounded in a pervasive context or climate of mistrust. They attributed this in part to families’ feelings of guilt about institutionalization, but also to their lack of understanding of the conditions of LTRC or the capabilities of people living with dementia. For instance, Luella, a nurse, described psychological violence she experienced from family members as being some of the worst she’s experienced, and she believed this could be addressed if families knew more about dementia and LTRC. She described a particular incident where a family member swore and yelled at her, saying:
‘You little bitches’ that’s what she says, ‘You little bitches need to get…’ And I’m like ‘Well…okay…’ so it’s just that kind of verbal stuff like: ‘You have no integrity.’ ‘I don’t know how you sleep at night,’ like, these kind of things. And it’s like she’s blaming me for years of trauma, years of, like feeling like she’s neglecting - like it’s all her guilt and her feeling - like some folks I think feel that the way they can advocate for their loved one is by tearing the nurses apart.
Luella further described that this family member blamed the staff for mismanaging her mother’s chronic health conditions. Although she acknowledged that ‘things could have been done differently’ she emphasized that it was not ‘the fault of a single staff member,’ expressing some frustration with the system of care not being set up to provide optimal care.
A health care aide, Tim, advanced a similar explanation to Luella in the following excerpt:
Sometimes you get the verbal abuse from families, especially when their loved one has dementia, that they do not get what level they are at, so they think that they are more capable, than what they are. Or, they get that report of a different resident was in the resident’s room or something, or they see some of that stuff. And they yell at the staff, they blame the staff.
Tim suggested that some family members are not present enough to assess the capacity of their family member with dementia and sometimes have unrealistic expectations of their relative, staff, or LTRC, leading them to blame staff for incidents they perceive as a violation of privacy or property of the resident. Other staff believed family members tended to overthink or might themselves lack the capacity to understand the situation. For example, Kayla, a nurse, stated:
Anything you say is kind of- the family overthinks it like, you are arguing - you do not want to cause the argument to get worse. So, you have to say, like short, little things to help de-escalate the situation. But sometimes they are so past that point. Especially, family members also have dementia, they may not be able to understand what you are saying. So, you just kind of have to let them explode and then you are like you feel like crap later. (Kayla).
Many staff interviewed tended to draw on and reproduce generalizing and unsubstantiated portrayals of relatives as themselves lacking emotional and/or cognitive capacity. Although in part this may reflect efforts to nurture empathetic understanding so as to cope by not taking it personally, this interpretive strategy can inadvertently undermine family concerns through implying a reduced capacity for reasonable communication (Funk et al., Reference Funk, Spencer and Herron2021).
In a final example, Ella, an early-career nurse, attributed psychological violence from family carers to their unrealistic expectations, distrust, and lack of understanding of staff work:
cause their expectations is not realistic for the units. I’m trying to think a lot of what there are, a lot of what their complaints are, other than those little things that for us is very minute, like things that should be organized in the room… It’s just more like they do not trust us. They just do not trust the staff or especially- I think they just do not understand what we do because they do not see it. They do not see us do care. They do not see what we go through. They think that maybe we are not trying our hardest…
In explaining the violence in this situation, Ella revealed value conflicts between family carers and staff about the type of care that should and can be provided in LTRC. She and other staff expressed some frustration that family members appeared to have little understanding or empathy for the challenging conditions under which staff are working. She also described a relational dynamic that was neither trusting nor supportive. Ultimately, however, staff tended to cope with psychological violence through interpretive strategies that appeared to have the unfortunate function of serving to dismiss, minimize, or discredit family members’ concerns or expertise (e.g., as unreasonable, unrealistic, or uninformed).
Violence from residents
As noted above, a vast majority of respondents reported experiencing violence from residents, ranging from severe physical (60.8%) forms to psychological forms (95.0%; see Table 1). Physical violence from residents (87.2%) was reported far more often than physical violence from family carers (7.4%) and co-workers (6.5%; see Table 1). Around half of the respondents reported being kicked (51.2%), punched (50.7%), slapped (53.8%), or having had something that could hurt them thrown at them (49.1%) by a resident within the previous year (see Table 2). Additionally, nearly three-quarters (72.0%) reported being pushed, grabbed, or shoved by residents during the past year, and approximately two-thirds of respondents (65.3%) reported that they had experienced unwanted sexual comments, while over one third (36.8%) had been groped or touched in a sexual manner by residents within the past year (see Table 2).
Frustration with working conditions, insufficient resources, and inflexible dementia care
In describing violent situations involving people living with dementia, staff comments in interviews highlighted the challenges and frustration of insufficient, unsupportive, or inflexible conditions of care. They spoke about unmet social needs and a lack of space, privacy, ownership, and control for residents, as well as understaffing and rushing care as factors contributing to violent situations or responsive behaviours among residents living with dementia. At times, staff comments also endorsed bio-medical framings that link violence to a diagnosis of dementia, cognitive impairment, delirium, or mental illness. For example, Alaina, a nurse, described violent situations as a product of a resident’s ‘disease process,’ saying,
We have a few residents that are quite possessive. And I mean, in their disease process, everything is theirs. They, this is my chair. Nope, this is my chair. We have one resident that sat on that same couch for years. And then for somebody to go and say ‘no, you are not sitting here.’ Oh, he was beside himself. Because he sat in that same spot every day for years.
While Alaina initially attributed possessiveness to the disease process, she revealed a tension between a sense of ownership over a chair and a lack of actual ownership as a problem that precipitated a violent situation. Similar issues were noted around privacy and security. In staff descriptions of violent situations, people living with dementia were often framed as more likely to get into a confrontation with someone who entered their room without permission. Hana, a health care aide, explained:
I would say it affects the ones with dementia more than the ones that do not have dementia because the ones that do not have dementia can understand why Mr. So-and-So, wandered into their room. Whereas the one with dementia just ‘Why is that man in here? Why is that woman in my room?’ And they get upset and confrontational.
While Hana attributed violent situations involving people living with dementia to a lack of ability to understand another resident wandering into their room, in doing so, she also revealed a lack of privacy and security in resident rooms. In this context, staff’s responsibility to intervene in resident-to-resident violence could also place staff at an increased risk of experiencing violence from a resident.
In another example, Ella explained that there was more violence experienced in her unit because it was a behavioural unit for people who have a history of being violent. She questioned the logic of this arrangement, which she believes ‘burns us out,’ adding, ‘it’s a very small unit. It’s a circle, right for pacing, so they do bump into each other.’ In this case, the demands on staff and a lack of space for residents to move without bumping into each other were viewed as factors contributing to violence (Herron, Reference Herron, Spencer, Novek, Funk, Kelly and Aubrecht2024). Another staff member noted that some residents ‘escalate when they get around others and some residents escalate when they’re alone,’ suggesting that all residents have different social needs and preferences and not meeting these needs contributes to escalating violence (Fiona, nurse).
Many staff pointed out that understaffing contributed to violent situations involving people living with dementia because more time and staff were needed to support relational and consensual care, prevent rushing care, and to intervene to prevent violent situations. Hana reasoned,
I would say it increases it [violence], because the minute you do not have time to sit there with the resident, you are instantly rushing them, and most dementia patients do not like to be rushed… Staff the facility according to their needs, not just the numbers that are in the facility. Right now, they just look at, ‘Well, you have 20 residents, this is the staff that you require.’ Well, it depends on what needs those 20 residents have. If 10 of them just need a little bit of help, then yes, that would be okay for staff. But if you have, over half of them that have dementia, that are wanderers, that can be violent, I think you need more staff on the floor.
Hana emphasized the needs of people living with dementia and the complexity and time required to negotiate direct care. She also suggested that more staff are needed to intervene if people living with dementia like to walk or are understood as ‘wanderers’ because this may contribute to violence.
Similarly, Brenda, a nurse, suggested that more staff were required to provide direct care to people living with dementia:
So, if I have to do a dressing change on somebody who’s not oriented, I do bring somebody with me to help with holding a limb to help to calm them so that they don’t, so that they’re not threatened or that they’re not going to react to what I’m doing to them, because I know it’s invasive, I know that it’s going to be a, it could be potentially problematic. So I think a big part of it is trying to be aware of the potentials. And then making sure that you have some kind of a system or a backup to be able to work in that.
Brenda further highlighted the range of strategies, albeit sometimes problematic (e.g., restraint), required to ensure care is non-threatening when a person living with dementia is confused and that staff do not get hurt.
Kayla likewise indicated that more staff are required to provide consensual care and prevent violence. She explained:
So they might get upset and then they’re embarrassed and they don’t want to be changed. So, if you have to come back in 15 minutes, well 15 minutes you might have to do another resident, so. If we had a good amount of staff, we would be able to go back and change them or give them the options- options to receive care, and then come back multiple times.
Kayla suggested that being able to offer residents a choice in their care would prevent violence; however, there is not enough staff to do so.
Ella noted that sometimes staffing was inconsistent with the routines of residents living with dementia on her unit. She said:
Some of them tend to be more aggressive at night, maybe because they were sleeping all day. And so, they are just awake. So we have had many times we had to call a code, because we are less staffed, and we need other people from the facility to come help us just try to calm this person down.
Staff descriptions of violent situations involving people living with dementia highlight the complex and unmet care needs of people living with dementia. They also reveal assumptions about how all residents should live, including what they should share, when they should receive care, where they should move, and when they should go to bed. When people living with dementia were not compliant with these expectations, staff believed this could ‘trigger’ a violent situation.
As shown in Table 3, the frequency of severe physical violence reported by residents was significantly associated with respondents’ job title, age, the number of different types of training they received, and working with a higher proportion of residents with cognitive impairment or dementia. As might be expected (because of their more frequent presence and engagement in personal care), both nurses (65.1%) and health care aides (81.8%) were more likely to report severe physical violence from residents during the past year than other designations of staff (e.g., management, kitchen staff; 30.2%; p < .001). Older staff (50+) were less likely to report severe physical violence from residents. Specifically, 47.1% of staff aged 50 and older had experienced severe physical violence from residents compared to 70.5% of those aged 30–39 and 66.7% of those aged 18–35 (p < .05). Interestingly, staff were significantly more likely to report severe physical violence from residents when they received more types of on-the-job training (such as dementia and person-centred care approaches, violent prevention and de-escalation). More than two thirds (69.7%) of those with three or more types of training reported severe physical violence from residents while less than half of those with fewer types of training reported experiencing this form of violence from residents (p < .01). It could be that these staff are more sensitized to recognize different forms of violence and perhaps be more likely to report them, as a result of increased training. In interviews, however, staff expressed both negative (i.e., ineffective online modalities; impractical strategies for the context) and positive (valued some helpful strategies to intervene, de-escalate, and protect people, reduced fear) perceptions of training.
Impractical or useful training?
Multiple staff commented that training to understand, prevent, or anticipate responsive behaviours was impractical for the context in large part because of a lack of time, staff, and space to effectively implement these strategies. For example, Luella described the value of dementia care and person-centred care training in helping her to understand responsive behaviours, but she said,
It’s not always super practical in a clinical setting when you’re like, suuuper understaffed, or a lot of inexperienced nurses kind of just like shoved into like charge positions and stuff. And you don’t always have the time, or the energy or the [pause] [small breath] even just like the physical space to sit down and do something like that.
While staff with more training may have had more knowledge to prevent and intervene in a range of situations, they could not effectively implement more upstream approaches to violence prevention in ways that would reduce reports of violence; however, this does not explain why they experience more violence than those with less training.
Interestingly, some participants mentioned that some training made them more comfortable intervening in risky situations:
I understand better the techniques to de-escalate the situation so that, you know, to protect the safety of the staff, including myself. And also, to protect the person that is demonstrating the behavior because often, like it often is fear-based. I’ve got that technique to try and help them, and focus on, helping them, and it helped me to not focus on my fears… (Sarah, nurse).
Other staff suggested that hands-on training helped them ‘to get out of a situation’ (Mira, nurse) and made them feel less fearful and more comfortable intervening to protect themselves, other staff, and residents. This may be another reason why staff with more training report experiencing more violence. This connection may also reflect greater efforts to target training toward staff believed to be more likely to encounter violence. For instance, Ella explained that she worked in a special unit where ‘the most aggressive’ residents were placed because staff have higher levels of training and they ‘can handle them.’ Staff working on specialized units or floors for people living with dementia and people who have a history of violence may thus receive more training and more residents with a history of violence, although this does not necessarily mean the conditions of their work support the effective use of that training.
Discussion
As outlined in the introduction and literature review, violence can be common and widespread in many forms in residential LTRC. Our study findings confirm this unfortunate finding and further call into question the standard approach of exploring violence by relationship type rather than looking at the care work setting as a whole, which may miss the extent of these issues and important nuances in terms of how violence manifests. Indeed, our study demonstrates that violence toward staff in LTRC manifests across different types of relationships.
Our study sheds light on the value of using mixed-methods research to explore, but also critically reflect on, possible explanations for trends revealed in quantitative survey data. The interviews with research participants offered tentative explanations for some of the statistically significant associations in the quantitative data, even as these interviews also revealed important interpretive nuances and, at times, more problematic framings. For example, participants’ perspectives that family members may not fully understand the realities and strains of working in LTRC or perhaps ‘take out’ their frustration on staff members, highlight a context of mistrust and tension that operates in both directions. However, some staff described the violence they experienced from family members as more harmful than that which they experienced from residents, highlighting the importance of validating staff experiences of violence from family members as a form of violence rather than softening the language used to describe this experience. Staff also expressed frustration that the system of care is not set to provide residents with optimum (e.g., one-on-one or flexible care) and that family members lack understanding or empathy for the challenging conditions under which staff are working. Ultimately, the interview findings reveal how, particularly in a context of broader resource constraints, family members and staff become pitted against one another. It is not surprising that families’ expectations of care are likely to be positioned as unrealistic, uninformed, or unreasonable within this organizational environment (Klostermann, Reference Klostermann2020).
Staff perceived dementia and cognitive impairment as increasing their experiences of violence in LTRC, in large part, because of the lack of staff and time to meet the complex care needs of residents living with dementia, consistent with recent systematic reviews on this topic (Song et al., Reference Song, Nassur, Rupasinghe, Haq, Boström, Reid, Andersen, Wagg, Hoben, Goodarzi, Squires, Estabrooks and Weeks2023). In some instances, their explanations reinforced stigmatizing views of people living with dementia as incapable of understanding the norms and expectations of LTRC or resolving conflicts (Herron et al., Reference Herron, Spencer, Novek, Funk, Kelly and Aubrecht2024). In making this point, our goal is not to place blame on particular staff; rather, our goal is to point out how, at times, problematic explanations arise and are reinforced because of the difficult working conditions. Moreover, in voicing their frustrations and challenges working with people living with dementia, staff ultimately painted a broader picture of an inflexible and under-resourced organizational environment that may enable a culture of strain, stress, and violence for all those who live, work, and visit.
Whether increased training experiences may heighten staff capacities to recognize and report violence needs to be more fully explored. However, it was noteworthy that staff interviewed for this study described learning about violence prevention and intervention, but being constrained by workloads and pace when it came time to use these skills. While previous research has documented staffing and workload as factors influencing violence in LTRC (Banerjee et al., Reference Banerjee, Daly, Armstrong, Szebehely, Armstrong and Lafrance2012; Song et al., Reference Song, Nassur, Rupasinghe, Haq, Boström, Reid, Andersen, Wagg, Hoben, Goodarzi, Squires, Estabrooks and Weeks2023), preparatory and on-the-job training in violence prevention and de-escalation techniques are often promoted as solutions (Booi et al., Reference Booi, Sixsmith, Chaudhury, O’Connor, Young and Sixsmith2021; Brophy et al., Reference Brophy, Keith and Hurley2019; Gozalo et al., Reference Gozalo, Prakash, Qato, Sloane and Mor2014). However, when on-the-job training is provided in conditions that do not support full implementation, staff will make use of the training only when and where it is feasible. In the context of our study, dementia care training in particular was often framed as impractical, while hands-on training about how to de-escalate or ‘get out of’ a violent situation was framed as useful for staff managing their fears and own safety. Importantly, increasing demands to perform on-the-job training that is perceived as impractical may contribute to burnout and a sense of frustration with the organization in which staff work. This resonates with earlier research on personal support worker training, where students and recent graduates expressed satisfaction with the preparatory education they received but shared they were challenged to apply it in their work settings (Kelly, Reference Kelly2017).
Limitations and suggestions for future research
The mixed-method, multi-site exploratory design is a strength of our research; however, the study has a few important limitations to note. While our purposeful, nonrandom sample yielded rich qualitative descriptions and explanations of violence, it may have skewed our quantitative findings. Additionally, there was not enough gender diversity in the sample to analyse this variable quantitatively; however, this is consistent with the gendered nature of the workforce. Furthermore, our qualitative data could not explain instances of co-worker violence, and further research is needed to explore how this violence interacts with other forms of violence in LTRC. Finally, because of the forms of data collection we chose to use at the outset of the COVID-19 pandemic, remote surveys and interviews, we were unable to access and include the perspectives of older adults on the violence they experience and witness in LTRC. To truly understand violence in the LTRC setting as a whole, residents’ perspectives must be included. Future research should include more in-depth ethnographic work exploring the multi-directional and interactional features of violence in LTRC.
Conclusion
Our mixed methods exploratory case study sheds light on how shared conditions of stress, strain, and mistrust perpetuate violence across relationships in the context of LTRC. Our quantitative analysis indicates that almost all staff reported experiencing at least one form of violence from residents, and many experienced one or more forms of violence from family and friends of residents. Severe physical violence from residents was more likely to be reported as having occurred in the past year when participants had received more on-the-job training and were providing care to a higher proportion of clients living with dementia or cognitive impairment. The qualitative data reveal that staff ascribed psychological violence from family or friends of residents to an absence of understanding and ‘unrealistic’ expectations of LTRC and dementia care, revealing tensions and mistrust that run in both directions. Interviews with staff evinced the limitations of violence prevention training as well as barriers to effectively implementing their training in practice.
Our results paint a complex picture of many forms of violence in LTRC as well as the mixture of interrelated factors that contribute to this problem. With this in view, we advocate for a more holistic approach to violence prevention in LTRC focused on addressing the structural and environmental conditions that precipitate violence rather than isolating particular types of violence and violent incidents. Most importantly, there is an urgent need to rebuild relationships of trust and provide conditions of care that promote safety for all those who live, work, and visit within LTRC.
Acknowledgement
We thank the members of the Knowledge User Advisory Committee for their contributions to the study design and their overall commitment to seeing improvements in long-term care.
Financial support
This Safe Places for Aging and care Project is funded by the Canadian Institutes of Health Research Project Grant (No: PJT 173395). The study is also funded, in part, by the Canada Research Chairs programme.
Competing interests
None to declare.


 Open access
Open access