


Introduction
In rapidly ageing societies, informal care is fundamental for many families and for the sustainability of most health-care systems (Brandt et al. Reference Brandt, Haberkern and Szydlik2009; Wolff et al. Reference Wolff, Spillman, Freedman and Kasper2016; Tur-Sinai et al. Reference Tur-Sinai, Teti, Rommel, Hlebec and Lamura2020). Between 12 per cent and 18 per cent of European adults regularly provide informal care to family members (European Commission 2021); in the UK, for example, men and women aged 50 are expected to spend an average of 4.9 and 5.9 years of their remaining lives as informal caregivers (Di Gessa and Deindl Reference Di Gessa and Deindl2024). The importance of informal care is likely to grow further as demand for long-term support increases, tensioning health-care and welfare systems (Cattaneo et al. Reference Cattaneo, Vitali, Regazzoni and Rizzi2025). Rising costs and resource constraints make family caregiving an indispensable complement to formal care, and many European countries increasingly rely on it to ensure the sustainability of care provision (Wolff et al. Reference Wolff, Spillman, Freedman and Kasper2016; Moen and DePasquale Reference Moen and DePasquale2017). However, this raises concerns about unequal consequences across families and social groups (von Saenger et al. Reference von Saenger, Dahlberg, Augustsson, Fritzell and Lennartsson2023), underscoring the need to better understand who becomes a care-giver, at what stage in life and with what consequences. Although numerous studies examined the health consequences of family caregiving (for an overview, see Schulz et al. Reference Schulz, Beach, Czaja, Martire and Monin2020), less attention has been given to the transition into caregiving and how social inequalities across the lifecourse may affect the timing of this transition in later life.
Integration of family caregiving into lifecourse trajectories
Despite the growing prominence of family care in ageing societies, relatively little empirical research has investigated caregiving trajectories. Recent developments have advocated for recognizing family caregiving as a distinct trajectory within the lifecourse, arguing that it is a normative phenomenon whose increasing diversity and cumulative impact on late-life outcomes are inadequately understood (Keating et al. Reference Keating, Eales, Funk, Fast and Min2019). This conceptualization stems from the central assumption in lifecourse research that transitions and trajectories influence the structure and pace of individual lives, as the impact of experiences is critically influenced by when they occur within the lifecourse (Alwin Reference Alwin2012). In particular, Keating and colleagues emphasized the age at onset of the first care episode (i.e. timing within the lifecourse) as crucial in shaping caregiving and other overlapping trajectories in later life (Keating et al. Reference Keating, Eales, Funk, Fast and Min2019). Capturing the lifecourse stage at which individuals become caregivers is fundamental for adequately understanding different pathways into caregiving and their intersection with family and employment. For instance, it makes a significant difference whether caregiving begins before or after retirement, or before or after becoming a grandparent (Hamilton and Cass Reference Hamilton and Cass2017). Due to competing demands (Broese van Groenou and De Boer Reference Broese van Groenou and De Boer2016), a caregiving onset before retirement could interrupt employment and earnings, leading to immediate and long-term financial consequences and career disruption (Heger and Korfhage Reference Heger and Korfhage2020). Conversely, post-retirement caregiving may entail more flexibility, while possibly still affecting health and social engagement (Brandt et al. Reference Brandt, Deindl, Floridi, Heidemann, Kaschowitz, Quashie, Verbakel and Wagner2023). Likewise, assuming care before grandparenthood may compete with family responsibilities to younger generations and constrain the capacity of downward intergenerational transfers, whereas starting after grandparenthood can add to existing family obligations and intensify role conflict (Hamilton and Cass Reference Hamilton and Cass2017).
Researchers have started to move beyond snapshots of individual predictors of caregiving onto larger mechanisms and dynamic processes (Moen and DePasquale Reference Moen and DePasquale2017), aiming to understand pathways to caregiving and its lifecourse timing. Cross-country differences in care systems and support structures are also a crucial contextual factor shaping caregiving onset and its timing across the lifecourse (Keating et al. Reference Keating, Eales, Funk, Fast and Min2019). The extent of formal long-term care provision, the availability of public services, and family norms differ across European welfare regimes (Brandt et al. Reference Brandt, Haberkern and Szydlik2009; Albertini et al. Reference Albertini, Zanasi and Piccitto2023). In contexts with extensive formal care provision, individuals may delay or reduce the intensity of caregiving, whereas in settings with limited support, family members may be more likely to assume care responsibilities earlier and for longer periods. While the present study does not investigate country-level differences, acknowledging this broader institutional variation helps situate our findings. Such institutional differences interact with individual resources and social positions, ultimately influencing both the likelihood and the timing of becoming a care-giver. Nonetheless, differences in age of caregiving onset and the factors that influence such timing remain unexplored.
Numerous studies have explored the social determinants of family caregiving, yet they often adopted a static approach, which understates the complexity of caregiving trajectories within the lifecourse (Rodrigues et al. Reference Rodrigues, Filipovič Hrast, Kadi, Hurtado Monarres and Hlebec2022). Differences in the timing of caregiving onset, particularly at older ages, may be influenced by cumulative processes of social (dis)advantage across various lifecourse domains (Carmichael and Ercolani Reference Carmichael and Ercolani2016; Fast et al. Reference Fast, Keating, Eales, Kim and Lee2021). Social positions result from cumulative exposure to risks during adult life, such as weak attachment to the labour market, family conflicts or reduced social networks (Hradil Reference Hradil2012). These positions are associated with different opportunities and advantages, not only deriving from individual responsibility but also from structural inequalities, and may set pathways to caregiving at a particular age. Several studies indicated that midlife (ages 45–60 for intergenerational caregiving) and late life (ages 60–75 for intra-generational caregiving) are the periods with the highest likelihood of providing family care (Conde-Sala et al. Reference Conde-Sala, Garre-Olmo, Turró-Garriga, Vilalta-Franch and López-Pousa2010; Hajek and König Reference Hajek and König2016).
Focusing on late life as the timing of care transition, a more nuanced understanding of the differences in pathways to caregiving onset may help explain why late-life caregivers suffer more social disadvantage, financial strain and poorer mental and physical health compared to those who become caregivers earlier in life (Keating et al. Reference Keating, Eales, Funk, Fast and Min2019). caregiving onset in this phase often overlaps with end-of-employment trajectories and other family commitments towards parents and children, potentially compromising these responsibilities. Recent studies have examined how the timing of caregiving is linked to other life trajectories such as employment (Raiber et al. Reference Raiber, Visser and Verbakel2022; Simard-Duplain Reference Simard-Duplain2022), family relations (Hamilton and Cass Reference Hamilton and Cass2017; Latham-Mintus et al. Reference Latham-Mintus, Holcomb and Zervos2022) and health (Barnett Reference Barnett2015).
Particularly for intergenerational care, starting to care for parents at an earlier age may imply a longer overlap between caregiving responsibilities and working years, increasing the likelihood of financial strain (Simard-Duplain Reference Simard-Duplain2022). This is especially important in pre-retirement years, as becoming a care-giver at younger ages could negatively impact the final employment years and lead to pension penalties. Earlier caregiving onset could act as a catalyst for the accumulation of inequalities over time, potentially accelerating health and wellbeing deterioration while setting individuals onto trajectories of weaker employment ties or reduced social activities (Fast et al. Reference Fast, Keating, Eales, Kim and Lee2021; Raiber et al. Reference Raiber, Visser and Verbakel2022). Most importantly, the earlier this transition occurs, the more persistent these trajectories are likely to be, with more profound consequences in later life.
Determinants of timing of caregiving onset and intersectionality
Alongside with population ageing, growing social inequalities have become paramount in the study of prerequisites and consequences of informal care (Moen Reference Moen, Binstock and George2001; Cohen et al. Reference Cohen, Sabik, Cook, Azzoli and Mendez-Luck2019; Brandt et al. Reference Brandt, Kaschowitz and Quashie2022). The Informal Care Model posits that caregiving transitions arise from care needs in the family, followed by a decision process involving individual disposition, expectations, social norms and availability of care alternatives (Broese van Groenou and De Boer Reference Broese van Groenou and De Boer2016). Moreover, it is likely that all these steps are socially stratified. While behavioural components are important to understand the onset of care provision, diversity of contexts and the influence of individual axes of inequalities as determinants of the timing of caregiving onset merit special attention. Family caregiving is largely influenced by social determinants such as sex/gender, migration background and socio-economic status (SES), with women and those with lower SES being more likely to provide care (Lee and Tang Reference Lee and Tang2015; Schmitz et al. Reference Schmitz, Quashie, Wagner and Kaschowitz2024). Although substantial evidence exists on the gendered and socio-economic gradient in family caregiving, most research has focused on single social factors associated with being a care-giver, rather than on how the intersection of these factors could affect the timing of becoming a care-giver.
Earlier life events and social determinants such as sex/gender, SES and social class, particularly when considered together, can influence the timing of caregiving onset, and thus mutually shape the consequences for the caregivers’ lifecourse (Carmichael and Ercolani Reference Carmichael and Ercolani2016). Characteristics like the care-giver’s income (lower), sex/gender (female) and partnership status (single) are associated with an increased likelihood of becoming a care-giver (Gaugler et al. Reference Gaugler, Wackerbarth, Mendiondo, Schmitt and Smith2003; Carmichael and Ercolani Reference Carmichael and Ercolani2016; Uccheddu et al. Reference Uccheddu, Gauthier, Steverink and Emery2019). However, the stratification of the timing of caregiving onset by social determinants or their intersections has rarely been investigated. A few studies have documented the gendered nature of caregiving onset, with women typically becoming caregivers at earlier ages on average (Fast et al. Reference Fast, Keating, Eales, Kim and Lee2021; Rodrigues et al. Reference Rodrigues, Filipovič Hrast, Kadi, Hurtado Monarres and Hlebec2022). Such disparities in the timing of caregiving onset are illustrative of sex/gender as context, where a gendered lifecourse determines the impacts of social roles and shapes differential caregiving pathways, opportunities and risks (Kim Reference Kim2023). Regarding migration background, older non-Western immigrant women tend to have earlier caregiving transitions than their non-migrant counterparts (Zhou Reference Zhou2013; Syed Reference Syed2022). This difference in caregiving onset could be due to a stronger emphasis on family obligations, limited support networks or reduced access to stable employment (Syed Reference Syed2022). Further, differences in SES prior to family caregiving are associated with divergent onset timings, where individuals with lower education, lower social class and less skilled occupations become caregivers at earlier life phases (Carmichael and Ercolani Reference Carmichael and Ercolani2016; Moen and DePasquale Reference Moen and DePasquale2017). Low-skilled occupational classes may begin caregiving earlier due to limited resources, including a lower ability to afford paid home care.
While some evidence links social determinants to the age of caregiving onset, few studies have explored this association through a cumulative (dis)advantage perspective (Rodrigues et al. Reference Rodrigues, Filipovič Hrast, Kadi, Hurtado Monarres and Hlebec2022). Differences in the timing of caregiving onset have been investigated in terms of sex/gender, migration background or SES, but not by considering the impact of multiple overlapping social determinants. The intersectionality framework can provide new insights based on the idea that people can access social positions following the intersection of multiple socio-environmental characteristics that have been accumulated throughout the lifecourse (Crenshaw Reference Crenshaw1990). Intersectionality entails that existing interlocking systems of privilege and oppression interact upon the individual social position, creating a perpetuation of structural social and health inequalities that define people’s discrimination experiences (e.g. sexism, racism, classism) (Crenshaw Reference Crenshaw1990; Hill Collins Reference Hill Collins1990; Dressel et al. Reference Dressel, Minkler and Yen1997).
Most importantly, individuals’ intersectional social strata might determine the age of caregiving onset, shaping a distinct impact in the nature of care and other overlapping trajectories. A recent scoping review concluded that family care research has largely overlooked aspects of diversity and intersectionality, calling for the adoption of an intersectional perspective to achieve a more nuanced understanding of caregiving experiences (Hengelaar et al. Reference Hengelaar, Wittenberg, Kwekkeboom, Van Hartingsveldt and Verdonk2023). The novel approach of multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) provides the opportunity to incorporate intersectionality into quantitative analyses (Merlo Reference Merlo2018), but it has not been applied yet in the family care context. Developed by Evans et al. (Reference Evans, Williams, Onnela and Subramanian2018), MAIHDA is useful to gain a nuanced understanding on differences in health-care outcomes (i.e. timing of caregiving onset) across intersectional social strata, while embedding intersectionality within a lifecourse perspective (Bell et al. Reference Bell, Holman and Jones2019; Holman and Walker Reference Holman and Walker2021).
The present study
The aim of the present study was to explore when European older adults became family caregivers and whether such timing in the lifecourse varied across 48 intersectional social strata defined by the intersection of sex/gender, migration background, education and occupation. We considered intra- and intergenerational care relationships separately, expecting greater between-strata timing differences in intra-generational care onset due to greater accumulation of lifecourse inequalities at older ages.
This study makes several key contributions: first, we explicitly address the gap regarding the transition into caregiving and its socially stratified timing, an aspect that has so far received little attention. Second, by applying an intersectional MAIHDA approach, we move beyond single-factor explanations to provide a more nuanced understanding of how multiple dimensions of social (dis)advantage jointly shape the timing of caregiving onset. Third, by distinguishing intra- and intergenerational caregiving, we emphasize that patterns of inequality differ across caregiving contexts and lifecourse phases. These contributions have key practical implications, as the timing of caregiving onset has direct consequences for employment, financial security, health and managing competing family roles. Identifying which population subgroups start caregiving earlier can help policy makers and practitioners anticipate support needs and design more targeted interventions to promote equal ageing. Understanding the unequal timing of caregiving transitions is therefore essential for preventing the reproduction of social and health disadvantage across the lifecourse.
Data and methods
Study population
We drew our data from Waves 1–9 (2004–2022) of the Survey of Health, Ageing and Retirement in Europe (SHARE). This is a European panel study collecting longitudinal data on demographic, socio-economic and health outcomes for adults aged 50+ (Börsch-Supan et al. Reference Börsch-Supan, Brandt, Hunkler, Kneip, Korbmacher, Malter, Schaan, Stuck and Zuber2013). SHARE data are collected through face-to-face computer-assisted personal interviews (CAPI), with methodological details on the survey extensively described elsewhere (Bergmann et al. Reference Bergmann, Kneip, De Luca and Scherpenzeel2017). We excluded individuals who were caregivers at Wave 1 (N = 1,078 providing intra-generational care; N = 818 providing intergenerational care), since our aim was to examine incident caregiving onset rather than ongoing care arrangements. Hence, we focused on later-life transitions into caregiving, omitting individuals who may have entered caregiving at an earlier life stage or those with long-term caregiving duties. Our study concentrated on the population aged 50+, where caregiving onset is most prevalent and where differences in timing are particularly shaped by cumulative processes of social (dis)advantage across various lifecourse domains. Thus, the design of SHARE fitted our focus on later-life transitions, since caregiving that begins in later life often overlaps with other major lifecourse transitions such as retirement or grandparenthood. Out of N = 34,285 individuals with more than two consecutive observations and who became informal long-term caregivers between Wave 2 and Wave 9, we excluded N = 18,678 respondents with incomplete information on all caregiving variables of interest (i.e. who they cared for, how often). From the remaining N = 15,607 respondents, we excluded 740 individuals (4.74 per cent) for whom the intra- or intergeneration of caregiving could not be determined (care recipient being classified as ‘other relative’) and another 755 individuals (4.84 per cent) with missing information in any of the socio-demographic variables of interest (sex/gender, migration background, education and occupation). Given the relatively low rate of missing data while assuming that data was missing at random (Dong and Peng Reference Dong and Peng2013), we applied listwise deletion, a standard practice in MAIHDA analyses that require complete data on outcome and strata-defining variables. This resulted in a final sample of N = 14,112, of which N = 10,146 became intra-generational caregivers and N = 3,966 intergenerational caregivers. After undergoing all the exclusion criteria, excluded caregivers at baseline with all the available variables were 8.1 per cent and 4.3 per cent (N = 432 and N = 320, respectively). A total of N = 220 (1.55 per cent) individuals became both intra- and intergenerational caregivers, but they were only classified into either group based on their first care transition.
Study variables
Outcome variable: age of caregiving onset
Informal long-term caregiving was defined as providing personal care to an adult family member daily during at least three consecutive months. SHARE distinguishes between informal family care outside of the household – ‘In the last 12 months, have you personally given any kind of help to a family member from outside the household?’, followed by the questions ‘Was this help with personal care (e.g. dressing, bathing or showering, eating, getting in or out of bed or using the toilet)?’ and ‘How often?’ – and inside the household – ‘Is there someone living in this household whom you have helped regularly during the last 12 months with personal care, such as washing, getting out of bed, or dressing? (By regularly we mean daily or almost daily during at least three months. We do not want to capture help during short-term sickness of family members.)’. Both questions were coded as binary variables (0 = No; 1 = Yes), hence we included individuals who answered yes to any of them, only selecting those who provided daily personal care outside of the household. The two variables were added up, resulting in a binary caregiving variable either inside or outside the household (yes/no).
We opted to collapse inside and outside the household care due to our focus on the timing of care onset, and to retain a sufficient sample size to further classify into intra- and intergenerational care and intersectional strata. Since Waves 4 and 5 did not distinguish personal care and other types of support outside the household, we followed the strategy by Nolan et al. (Reference Nolan, Aaltonen and Danielsbacka2024) and limited caregiving outside of the household to Waves 1–2 and 6–8, as opposed to Waves 1–9 for caregiving inside the household. We only included individuals who provided care to identifiable family members, and we used this information to classify caregiving into intra- and intergenerational (Table S1). The first wave when an individual became a care-giver was used to set the corresponding age, which was the outcome variable in all analyses.
Interest variables: intersectional social strata
We created 48 intersectional social strata through the unique combinations of sex/gender (two categories), migration background (two categories), education (three categories) and occupation (four categories) (2 x 2 x 3 x 4 = 48). This number of strata, as is common in MAIHDA analyses, allowed us to capture the granularity of intersectional differences with precision-estimates while ensuring sufficient interpretability. The socio-demographic variables were selected since they are known to be related to social (dis)advantages and access to particular social positions, in a way where they represent the effects produced by systems of privilege and oppression, especially at their intersections. Sex/gender was coded as male or female since SHARE only provides this imperfect binary categorization. Nonetheless, we opted to employ the term sex/gender to account for the conflation of sex and gender in the survey item. Migration background was categorized as yes or no after the question ‘Were you born in the country of interview?’. Education was assessed according to the International Standard Classification of Education (ISCED-97) and coded as high (ISECD-97 Level 5–6), medium (ISCED-97 Level 3–4) or low (ISECD-97 Level 1–2). Occupation was obtained from the self-reported present or most recent job type, and categorized in four groups based on the International Standard Classification of Occupations (ISCO-88): white-collar high-skill (WCHS), white-collar low-skill (WCLS), blue-collar high-skill (BCHS) and blue-collar low-skill (BCLS). These four variables have been found to be associated with differences in the timing of caregiving onset, although consistently in a separate way and not at their intersections (Carmichael and Ercolani Reference Carmichael and Ercolani2016; Moen and DePasquale Reference Moen and DePasquale2017; Fast et al. Reference Fast, Keating, Eales, Kim and Lee2021; Syed Reference Syed2022; Kim Reference Kim2023).
Analytical strategy
We employed the MAIHDA approach, which is based on multilevel models where individuals at the first level are nested within the intersectional social strata at the second level (Evans et al. Reference Evans, Williams, Onnela and Subramanian2018). In previous studies, MAIHDA models have been found to create more accurate and more precise predictions than fixed-effect models, with improved scalability, model parsimony and ability to deal with small subgroup samples (Merlo Reference Merlo2018; Van Dusen et al. Reference Van Dusen, Cian, Nissen, Arellano and Woods2024). For more detailed information about MAIHDA, we encourage consulting the recently published tutorial paper by Evans et al. (Reference Evans, Leckie, Subramanian, Bell and Merlo2024). This methodology allowed us to assess the variation in age of caregiving onset across intersectional strata, thus determining the discriminatory accuracy of the intersectional strata in explaining the variance of the outcome. We used restricted maximum likelihood (REML) estimation to fit a series of linear multilevel models.
We first calculated a null model (Model 1), which allowed to map the differences in age of caregiving onset across the intersectional social strata. Model 1 takes the form:
 \begin{equation}{{\text{Y}}_{{\text{ij}}}}{\text{ = }}{{{\unicode{x03B2} }}_{\text{0}}}{\text{ + }}{{{\upsilon }}_{{\text{0j}}}}{\text{ + }}{{{\unicode{x03BC} }}_{{\text{0ij}}}}\end{equation}
\begin{equation}{{\text{Y}}_{{\text{ij}}}}{\text{ = }}{{{\unicode{x03B2} }}_{\text{0}}}{\text{ + }}{{{\upsilon }}_{{\text{0j}}}}{\text{ + }}{{{\unicode{x03BC} }}_{{\text{0ij}}}}\end{equation} Level 2:  ${{{\upsilon }}_{{\text{0j}}}}{{\sim}}{\text{N}}{\text{ }}(0,\;{{\sigma }}_v^2)$)
${{{\upsilon }}_{{\text{0j}}}}{{\sim}}{\text{N}}{\text{ }}(0,\;{{\sigma }}_v^2)$)
Level 1:  ${{{\unicode{x03BC} }}_{{\text{0ij}}}}{{\sim}}{\text{N}}{\text{ }}(0,\;{{\sigma }}_{\unicode{x03BC}}^2)$)
${{{\unicode{x03BC} }}_{{\text{0ij}}}}{{\sim}}{\text{N}}{\text{ }}(0,\;{{\sigma }}_{\unicode{x03BC}}^2)$)
where Yij indicates the age of caregiving onset for individual i in intersectional stratum j and β0 denotes the intercept. Then, υ0j and µ0ij are stratum-level and individual-level random effects with means of zero and variances  ${{\sigma }}_v^2\,$and
${{\sigma }}_v^2\,$and  ${{\sigma }}_{{\unicode{x03BC} }}^2$, respectively.
${{\sigma }}_{{\unicode{x03BC} }}^2$, respectively.
With this model we calculated the variance partition coefficient (VPC) as follows:
 \begin{equation}{\text{VPC}} = { }\frac{{{{\sigma }}_{\text{v}}^2}}{{{{\sigma }}_{\text{v}}^2 + {{ \sigma }}_{{\mu }}^2}} \times 100\end{equation}
\begin{equation}{\text{VPC}} = { }\frac{{{{\sigma }}_{\text{v}}^2}}{{{{\sigma }}_{\text{v}}^2 + {{ \sigma }}_{{\mu }}^2}} \times 100\end{equation}The VPC measures level of variation in the outcome between intersectional strata and is analogous to the intra-class correlation coefficient (ICC), where values ≥ 5 per cent can indicate a fair magnitude of clustering (Axelsson Fisk et al. Reference Axelsson Fisk, Mulinari, Wemrell, Leckie, Perez Vicente and Merlo2018; Merlo Reference Merlo2018). Further, we fitted a model adjusted for the strata-defining variables as fixed effects (Model 2), which takes the form:
 \begin{equation}{{\text{Y}}_{{\text{ij}}}}{\text{ = }}{{{\unicode{x03B2} }}_{\text{0}}}{\text{ + }}{{{\unicode{x03B2} }}_{\text{1}}}{{\text{x}}_{{\text{ij}}}}{\text{ + }}{{{\upsilon }}_{{\text{0j}}}}{\text{ + }}{{{\unicode{x03BC} }}_{{\text{0ij}}}}\end{equation}
\begin{equation}{{\text{Y}}_{{\text{ij}}}}{\text{ = }}{{{\unicode{x03B2} }}_{\text{0}}}{\text{ + }}{{{\unicode{x03B2} }}_{\text{1}}}{{\text{x}}_{{\text{ij}}}}{\text{ + }}{{{\upsilon }}_{{\text{0j}}}}{\text{ + }}{{{\unicode{x03BC} }}_{{\text{0ij}}}}\end{equation}where xij is a vector with the strata-defining individual variables and β1is a vector containing the corresponding parameter values. By fitting Model 2, we accounted for the additive effects explaining the outcome variance. With this model we were able to calculate the VPC and the proportional change in variance (PCV), which is the difference in variance explained at the strata-level compared to Model 1. PCV is calculated as follows:
 \begin{equation}{\text{PCV}} = { }\frac{{\begin{array}{*{20}{c}}
{\begin{array}{*{20}{c}}
{\begin{array}{*{20}{c}}
{{{\sigma }}_{v{\text{ Model }}1}^2 - \,{{\sigma }}_{v{\text{ Model }}2}^2}
\end{array}}
\end{array}}
\end{array}}}{{{{\sigma }}_{v{\text{ Model }}1}^2}}{ } \times { }100\end{equation}
\begin{equation}{\text{PCV}} = { }\frac{{\begin{array}{*{20}{c}}
{\begin{array}{*{20}{c}}
{\begin{array}{*{20}{c}}
{{{\sigma }}_{v{\text{ Model }}1}^2 - \,{{\sigma }}_{v{\text{ Model }}2}^2}
\end{array}}
\end{array}}
\end{array}}}{{{{\sigma }}_{v{\text{ Model }}1}^2}}{ } \times { }100\end{equation}If Model 2 does not explain the total strata variance (i.e. PCV < 100 per cent), this would mean that the observed inequalities were due to intersectional interaction effects (i.e. multiplicative effects) (Bell et al. Reference Bell, Holman and Jones2019). Country dummies were included as covariates in Model 2 to account for country-specific factors affecting both timing of the event and predictor variables (Table S4). Lastly, we examined the strata-level residuals to determine which particular intersectional strata were exposed to significant multiplicative effects. If the residuals’ 95 per cent CI did not cross zero, such strata would have either significantly negative (advantageous) or positive (hazardous) intersectional interaction effects. All models were fitted separately for intra- and intergenerational groups. The analyses were conducted in Stata/BE®18.0 (Statacorp, College Station, TX, USA), and statistical significance was based on a two-tailed p-value < 0.05 for regression coefficients.
Results
Descriptive statistics
Our sample consisted of 10,146 individuals who became intra-generational caregivers and 3,966 who became intergenerational caregivers (Table 1). Within the intra-generational group, a large majority provided care to their partner or spouse (95.60 per cent), followed by siblings (3.64 per cent). Regarding intergenerational care, most individuals cared for their parents – mainly mothers (71.72 per cent) – followed by in-laws (22.35 per cent), step-parents (3.56 per cent), grandparents (0.98 per cent) and aunts and uncles (0.66 per cent) (Table S1). Overall, there were differences in socio-demographic characteristics between intra- and intergenerational caregivers. The average age of caregiving onset was higher for intra-generational caregivers (70.18 years; SD = 9.93) than for intergenerational caregivers (59.56 years; SD = 6.06). The proportion of women was lower among intra-generational caregivers (53.32 per cent compared to 68.68 per cent), whereas there were more caregivers with a migration background among the intra-generational group (11.20 per cent versus 6.76 per cent in intergenerational caregivers). Educational levels were generally lower among intra-generational caregivers compared to the intergenerational group (19.25 per cent versus 26.65 per cent with high education, and 43.87 per cent versus 29.05 per cent with low education, correspondingly). A similar pattern was seen for occupation, where the intra-generational sample had fewer white-collar and lower-skilled occupations than intergenerational caregivers (27.37 per cent versus 31.92 per cent with WCHS, and 24.47 per cent versus 19.97 per cent with BCLS, correspondingly).
Socio-demographic characteristics of the intra- and intergenerational caregiving sample

Intra-generational caregiving
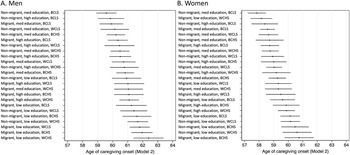
The predicted ages of intra-generational caregiving onset for each intersectional stratum are presented in Figure 1 (average = 70.18 years; SD = 9.93). There were clear between-strata disparities, with a remarkable difference of more than 11 years between those with the lowest age of onset (65.17 years, consisting of women without a migration background, high education and BCLS occupation), and the highest age of onset (75.97 years, formed by men with a migration background, low education and WCHS occupation). Trends in Figure 1 show that in general women became caregivers at a younger age, higher education implied earlier onset and there was a gradual decrease of onset age in blue-collar and less-skilled occupations.
Predicted age of caregiving onset by intersectional social strata, for intra-generational care. Estimates and their 95 per cent confidence intervals were obtained from Models 1a and 1b, adjusting for country dummies. WCHS: white-collar high-skill; WCLS: white-collar low-skill; BCHS: blue-collar high-skill; BCLS: blue-collar low-skill.

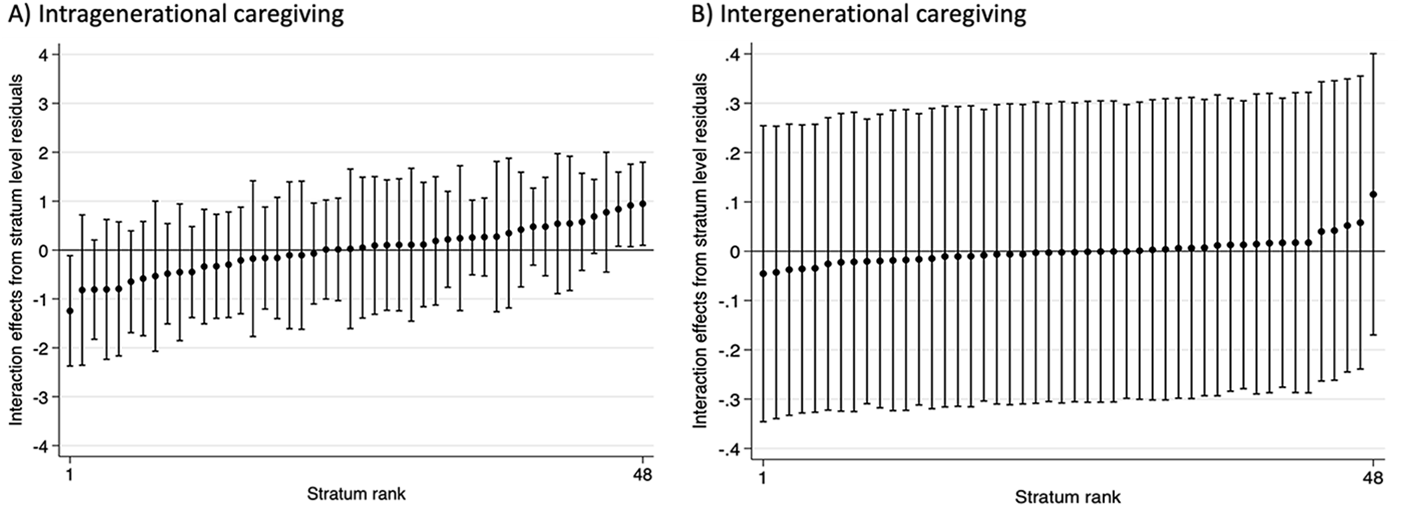
Results on intra-generational caregiving obtained from the MAIHDA models are displayed in Table 2. The VPC in Model 1a indicated that 7.14 per cent of the differences in age of caregiving onset were explained at the strata level, suggesting a fair level of clustering (Axelsson Fisk et al. Reference Axelsson Fisk, Mulinari, Wemrell, Leckie, Perez Vicente and Merlo2018). This is consistent with the heterogeneous pattern observed in Figure 1. After adjusting for the main effects in Model 2a, the VPC decreased to 0.76 per cent, meaning that some amount of clustering at the strata level remained. Notably, a PCV of 90.00 per cent indicated that additive effects could not explain all the outcome variance. This implies that 10 per cent of the differences in the age of caregiving onset between strata were due to multiplicative effects, that is, intersectional interaction effects. The main effects in Model 2a show that, on average, the age of caregiving onset was lower for women, higher for respondents with a migration background, higher for those with low education and lower for those with BCLS occupations. While the average main effects are informative, they can only partially explain the cumulative impact, which is better reflected through their intersections (Figure 1). Figure 2A shows the strata-level residuals obtained from Model 2a, where some multiplicative interaction effects are revealed. Three strata had positive interaction effects, meaning that their age of caregiving onset was older than expected based on the main effects only (i.e. 0-level line), whereas one stratum had negative interaction effects, meaning an earlier onset than expected (see Tables S2 and S3 for intersectional strata details). These results suggest the presence of some intersectionality effects, as shown by a PCV value below 100 per cent (90.00 per cent).
Strata-level residuals obtained from Models 2a and 2b, both for (A) intra- and (B) intergenerational care. Models 2a and 2b were controlled for country dummies.

Results from MAIHDA models predicting age of caregiving onset, both for inter- and intra-generational care

Notes: CI: confidence interval; VPC: variance partition coefficient; PCV: proportional change in variance. Models 2a and 2b were controlled for country dummies.
Significance levels:
* p < 0.05, ** p < 0.01, *** p < 0.001.
Intergenerational caregiving
The predicted ages of intergenerational caregiving onset for each intersectional stratum are presented in Figure 3 (average = 59.56 years; SD = 6.06). There was a difference of four and a half years between the intersectional strata with the lowest age of onset (57.84 years, consisting of women without a migration background, medium education and BCLS occupation) and the strata with the highest age of onset (62.39 years, formed by men with a migration background, low education and BCHS occupation). Overall, women had a lower age of onset, similar to respondents with mid or high education and BCLS occupations.
Predicted age of caregiving onset by intersectional social strata, for intergenerational care. Estimates and their 95 per cent confidence intervals were obtained from Models 2a and 2b, adjusting for country dummies. WCHS: white-collar high-skill; WCLS: white-collar low-skill; BCHS: blue-collar high-skill; BCLS: blue-collar low-skill.

Table 2 also shows the MAIHDA results for intergenerational caregiving, where a VPC of 3.69 per cent in Model 1b suggested a poorer level of clustering at the strata level. In fact, when adjusting for the main effects in Model 2b, the VPC was reduced to 0.07 per cent, meaning that almost all the clustering at the strata level was explained away by those main effects. A PCV of 98.20 per cent confirmed that the largest majority of differences in age of caregiving onset were explained by additive effects, leaving only around 2 per cent of the outcome variance to be explained by multiplicative effects. The main effects were very similar to those in intra-generational care, since women became caregivers at a younger age, respondents with a migration background at an older age, those with low education at an older age and those with BCLS occupations at a younger age. Again, these average main effects can point towards general trends, but they can only partially explain the cumulative impact on the age of caregiving onset, which is better reflected through their intersections (Figure 3). Figure 2B shows the strata-level residuals obtained from Model 2b. Since all the confidence intervals overlapped with 0, no statistically significant multiplicative interaction effects were revealed. This is aligned with a PCV value close to 100 per cent (98.20 per cent), meaning that practically all between-strata differences were due to additive effects.
Discussion
The objective of the current study was to examine the timing of family caregiving onset in late midlife, with a particular focus on exploring differences in age of onset across intersectional social strata. These strata were created by the combination of sex/gender, migration background, education and occupation of the caregivers. We used SHARE data to analyse intersectional inequalities in the age of caregiving onset by employing the MAIHDA framework, considering intra- and intergenerational caregiving separately. We found more than 11 years of difference between intersectional strata for intra-generational care when, for instance, the partner became a care-giver. For intergenerational care, these differences were up to four and a half years. Although there were some intersectional interaction effects in the intra-generational case, we did not find this pattern in the intergenerational analyses. For both generational groups, being a woman and low-skill occupations were linked with an earlier onset of caregiving. We found no clear association between migration background and timing of caregiving onset. More surprisingly, high education was associated with an earlier onset of caregiving.
Although there is some evidence indicating the differences in caregiving onset and its consequences across intersecting social determinants (Gaugler et al. Reference Gaugler, Wackerbarth, Mendiondo, Schmitt and Smith2003; Cohen et al. Reference Cohen, Sabik, Cook, Azzoli and Mendez-Luck2019; Nikzad-Terhune et al. Reference Nikzad-Terhune, Gaugler and Jacobs-Lawson2019; Willert and Minnotte Reference Willert and Minnotte2021), to date no study had investigated differences in the age of caregiving onset with an intersectional approach. We used the tenet of timing within the lifecourse theory to explore stratified pathways into family caregiving. Our findings on sex/gender and occupation are in line with previous studies that analysed them as separate predictors of the timing of caregiving onset (Gaugler et al. Reference Gaugler, Wackerbarth, Mendiondo, Schmitt and Smith2003; Carmichael and Ercolani Reference Carmichael and Ercolani2016; Moen and DePasquale Reference Moen and DePasquale2017; Nikzad-Terhune et al. Reference Nikzad-Terhune, Gaugler and Jacobs-Lawson2019). Furthermore, we provide new empirical insights by considering the intersection of both social determinants. We found significant intersectional interaction effects for intra-generational caregiving, indicating the fundamental role of social position in shaping differential pathways into family caregiving. A lifelong exposure to interlocked systems of power and oppression is reflected in the differences in age of onset across intersectional strata (Bauer Reference Bauer2014). Our results illustrate the heterogeneities across intersectional strata, such as women in blue-collar occupations starting caregiving earlier than other groups. Prior evidence shows that gendered and class-related inequalities can shape the timing and intensity of caregiving (Carmichael and Ercolani Reference Carmichael and Ercolani2016; Fast et al. Reference Fast, Keating, Eales, Kim and Lee2021), suggesting that women with lower SES tend to experience caregiving earlier in life (Navaie-Waliser et al. Reference Navaie-Waliser, Spriggs and Feldman2002; Tokunaga and Hashimoto Reference Tokunaga and Hashimoto2017; Zygouri et al. Reference Zygouri, Cowdell, Ploumis, Gouva and Mantzoukas2021). In line with intersectionality theory, these patterns may reflect the cumulative effects of interlocking systems of gender and class disadvantages (Crenshaw Reference Crenshaw1990; Hill Collins Reference Hill Collins1990). Although our study cannot establish causal mechanisms, findings are consistent with structural intersectional inequalities contributing to earlier caregiving onset among women in blue-collar occupations, with potential implications for the remaining lifecourse. This underscores the importance of adopting an intersectional lens to gain a more nuanced understanding of disparities in family caregiving and unequal lifecourses.
Our findings linking higher education with an earlier onset of caregiving, despite not having available direct comparisons in the literature, are opposed to the overall trend that associates lower SES (education, income or wealth) with a higher rate of care onset (Carmichael and Ercolani Reference Carmichael and Ercolani2016). However, our results are aligned with evidence revealing positive associations between higher education and likelihood of caregiving, particularly for women with tertiary education (Brandt et al. Reference Brandt, Haberkern and Szydlik2009; Baji et al. Reference Baji, Golicki, Prevolnik-Rupel, Brouwer, Zrubka, Gulácsi and Péntek2019; Sacco et al. Reference Sacco, König, Westerlund and Platts2022; Albertini et al. Reference Albertini, Zanasi and Piccitto2023). To test for over-control bias, we also conducted analyses with only education included (without occupation). The effect direction remained unchanged, indicating the robustness of a positive educational gradient in the timing of caregiving onset. It seems probable that lower educational qualifications may not necessarily align with low-skill occupations for older cohorts in SHARE, which reinforces the need to use an intersectional approach that considers multiple determinants simultaneously. Since higher levels of education are associated with greater financial security and better health in later life (Tur-Sinai et al. Reference Tur-Sinai, Teti, Rommel, Hlebec and Lamura2020), this could translate into improved access to resources, more active and productive ageing, and a greater likelihood to be healthy and thus engage in caregiving. Despite assortative mating, the influence of strong cultural norms regarding spousal support, gendered expectations or unequal health trajectories within ageing partnerships may still lead to earlier caregiving onset for high-educated women, who may also have older parents. Aligned with this, individuals with lower education may have to rely on publicly funded services and formal care at an earlier age, only becoming informal caregivers at later life phases (Albertini et al. Reference Albertini, Zanasi and Piccitto2023).
Some social determinants, such as sex/gender, migration background or SES, influence the access to social positions within status hierarchies that affect the timing of caregiving onset. While gendered inequalities and other forms of stratification are thoroughly embedded in care work research, less is known about how the social environments associated with these attributes produce and reproduce persistent inequalities (Moen and DePasquale Reference Moen and DePasquale2017). Hence, mapping social heterogeneity and vulnerability in the context of family caregiving is fundamental to further understanding the drivers of such inequalities. We shed some light onto how social stratification can shape pathways to caregiving, with a particular focus on the lifecourse and the timing of such transitions. Our findings emphasize the importance of how caregiving trajectories unequally unfold across the lifecourse, and their intersectional nature through cumulative (dis)advantages. More attention should be paid to how diverse caregiving pathways, particularly the age of onset, may in fact be reproducing inequalities experienced throughout the lifecourse.
The present study has several strengths, including the large longitudinal sample and an intersectionality-informed, sophisticated analysis that had not been applied to informal caregiving research in late life. However, our study also has imitations. First, the composition of the groups followed an intra- and intergenerational perspective, yet these categories are broad and heterogeneous. For instance, caring sisters and partners and adult children and stepchildren were pooled together. We opted for broader categories to avoid further exclusion of care-giver groups from the analysis. The average age in the intergenerational group was slightly biased upwards, as it would probably be younger if SHARE were not a survey on older people. We focused on late-life caregiving due to its high prevalence, prominence and interrelation with cumulative lifecourse inequalities, yet, given the increasing relevance of care among younger populations (Lacey et al. Reference Lacey, Letelier, Xue and McMunn2025), future studies should investigate the timing of caregiving onset in younger cohorts. Second, different generations entail a mix of age-period-cohort effects, which future research should disentangle. We could not account for period effects (i.e. financial crisis, Covid-19) due to the unbalanced nature of our dataset, and while country dummies were included to control for contextual differences across welfare regimes, future studies should investigate how period differences affect caregiving onset. Third, we did not include confounders such as care-giver characteristics because the additional fixed effects would not have a straightforward interpretation in the MAIDHA framework. Nonetheless, future studies should investigate potential pathways and explanations for differences in caregiving onset across intersectional strata. Fourth, we excluded individuals who did not become caregivers, as this was beyond the scope of our study. While prospective or matched designs for the stratified caregiving onset would provide valuable insights on selection into caregiving, our aim was to characterize caregivers regarding the stratified timing of onset. Fifth, we opted for listwise deletion to handle missing data given the low proportion of incomplete cases (4.74 per cent) while we assumed that data were missing at random (Dong and Peng Reference Dong and Peng2013). We considered methods like multiple imputation to mitigate sample selectivity but dismissed them due to the practical challenges of their implementation, given the complex data structure. The same issue and limitations also apply to the missingness for outside-household caregiving in Waves 4–5, which we decided to exclude to ensure consistent definitions and minimize complexity with three simultaneous imputations. Sixth, we could only capture the timing of caregiving onset between waves, leading to a potential overestimation of age for a maximum of 12 months. However, given that one year is relatively small in comparison with the differences of 11 and 4.5 years between intersectional groups, and the larger standard deviations in the outcomes (9.93 and 6.06 years), such potential maximal divergence would not undermine the conclusions and implications of our study. Further, although SHARE provides comprehensive assessment instruments, we could not obtain more detailed information about the care situation. We had to omit race or ethnicity indicators since they were not collected in SHARE. Given their potential critical role in cumulative processes of social disadvantage in the late lifecourse, future European studies should incorporate race/ethnicity data to better understand the intersectionality of informal caregiving onset. Additionally, our sample included multiple countries with differences in health-care settings, such as institutional care support or social norms, which may affect the age of caregiving onset. Although we accounted for country differences, future research should focus on intersectional stratification differences across several health-care settings, drawing on larger national samples with sufficient statistical power to detect intersectional disparities. Finally, future studies should examine the trajectory or patterns of family caregiving, not only in the onset, from an intersectional perspective.
Potential implications include informing practitioners and policy makers that diverse family caregiving situations have different support needs and require stratified approaches over the lifecourse. The fact that certain groups are at higher risk of becoming caregivers earlier in life (e.g. women in low-skill occupations) should be considered to enable tailoring care-giver support strategies and public health campaigns in a more intersectional approach. Conceptual implications may concern the lifecourse theory of caregiving and potential research questions that relate the onset of caregiving with health and socio-economic trajectories. While we found an intersectional pattern in the age of caregiving onset, particularly for intra-generational caregivers, more theorizing about the lifecourse effects of the exact timing of the onset of caregiving would be warranted. Whether the effects on family behaviour, mental and physical health, work life and pension are intersectionally stratified is currently unknown. Additionally, having the optimal combination of resources during the onset of caregiving would be part of such a lifecourse theory of caregiving.
Conclusions
This study was designed with the objective of examining when in the lifecourse individuals aged 50+ become caregivers to older family members and how this timing varies across intersectional social strata. We found marked inequalities: women and those in low-skill occupations tended to enter caregiving earlier, and intersectional effects were especially visible in intra-generational care. These findings highlight that caregiving onset is not only a widespread lifecourse transition but also one that is socially stratified.
Understanding inequalities in family caregiving, including its timing within the life course, is fundamental for the wellbeing of individuals and their families. Earlier caregiving onset has been linked to poorer physical and mental health, increased financial strain and reduced social participation (Hank Reference Hank2011; Kaschowitz and Brandt Reference Kaschowitz and Brandt2017; Schulz et al. Reference Schulz, Beach, Czaja, Martire and Monin2020; Rodrigues et al. Reference Rodrigues, Filipovič Hrast, Kadi, Hurtado Monarres and Hlebec2022), underscoring the broader consequences for caregivers themselves. Our findings provide useful insights for designing support systems that recognize when in the lifecourse specific subgroups are most likely to require assistance. By identifying those assuming family caregiving responsibilities earlier, policy makers can better anticipate support needs and tailor interventions accordingly. From a social policy perspective, acknowledging these disparities is critical to designing support systems that consider the unequal timing of caregiving trajectories and their overlap with other major late lifecourse transitions, such as retirement. Addressing intersectional inequalities is essential to avoid the reproduction of disadvantage in later life and to ensure that support reaches those at greatest risk. Future research should bring together socio-economic and health perspectives on family caregiving, with a particular focus on intersectional disparities throughout the lifecourse. How specifically health and wealth trajectories are affected by an earlier onset and how these trajectories vary by intersectional social strata needs further investigation.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X26100592.
Acknowledgements
This work was funded by the Einstein Foundation Berlin (grant number EZ-2019-555-2), supporting the Einstein Center Population Diversity (ECPD) in Berlin. The salary of EA-P is funded with the Einstein Foundation’s grant. We would like to thank all members of the Einstein Center Population Diversity (ECPD) who contributed to the development of ideas that led to this article. This article uses data from SHARE Waves 1, 2, 4, 5, 6, 7, 8 and 9 (DOIs: 10.6103/SHARE.w1.710, 10.6103/SHARE.w2.710, 10.6103/SHARE.w4.710, 10.6103/SHARE.w5.710, 10.6103/SHARE.w6.710, 10.6103/SHARE.w7.710, 10.6103/SHARE.w8.710, 10.6103/SHARE.w9.710). See Börsch-Supan et al. (Reference Börsch-Supan, Brandt, Hunkler, Kneip, Korbmacher, Malter, Schaan, Stuck and Zuber2013) for methodological details. The SHARE data collection has been funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N◦211909, SHARE-LEAP: GA N◦227822, SHARE M4: GA N◦261982) and Horizon 2020 (SHARE-DEV3: GA N◦676536, SERISS: GA N◦654221) and by DG Employment, Social Affairs and Inclusion. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the US National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org, accessed on 1 July 2024).
Author contributions
EAP, JLOS and PG conceptualised the study. EAP and PG reviewed the existing literature. PG and EAP designed the methodology, and EAP carried out the data curation and formal analysis. AS, SS and MB provided theoretical insights and helped interpreting the findings, contributing to data visualisation. PG supervised the study, PG and JLOS administered the project. EAP was the main contributor in writing the original manuscript draft. All authors were involved in reviewing and editing the current manuscript for submission. All authors read and approved the final manuscript.
Competing interests
The authors declare no competing interests.
Ethical standards
The Ethics Council of the Max Planck Society for the Advancement of Science granted SHARE’s Ethics approval. The analyses conducted in this study with anonymized data align with the approval granted by the ethics committee.
This article uses data from SHARE Waves 1, 2, 4, 5, 6, 7, 8 and 9. SHARE data are publicly available (www.share-eric.eu, accessed 3 July 2024).






 Open access
Open access