


In many low- and middle-income countries, undernutrition remains a major public health challenge for children under five(Reference Williams, Schnefke and Flax1). It manifests in various forms, including stunting, underweight, wasting and micronutrient deficiencies(Reference Williams, Schnefke and Flax1) and is closely linked to higher childhood morbidity and accounts for about one-third of deaths in this age group(Reference Rahman, Bhuiyan and Das2). Persistent undernutrition into adulthood increases morbidity and reduces productivity over the lifespan(Reference Rahman, Bhuiyan and Das2). Globally, 47 million under-five children suffer from acute wasting and 149 million from stunting(Reference Mostafa, Fahim and Das3). Alarmingly, 35 % of South Asian children under five are stunted, and more than 15 % are wasted (<–2 sd WHZ)(Reference Wali, Agho and Renzaho4). In Bangladesh, the prevalence of stunting, underweight and wasting was reported to be 24 %, 22 % and 11 %, respectively(5).
Despite being a sustainable development goal priority, malnutrition remains one of Bangladesh’s most pressing public health issues(Reference Rana, Alam and Islam6). The issue is especially alarming among the urban underprivileged population in metropolitan areas like Dhaka, where an estimated 5000 slums house millions(Reference Rana, Alam and Islam6–Reference Gruebner, Sachs and Nockert8). These slums are characterised by a high population density, poor sanitation, limited clean water access, inadequate drainage, frequent diarrhoea outbreaks and pervasive poverty, all negatively affecting children’s health and nutritional status(Reference Uddin, Koehlmoos and Saha9). Furthermore, the factors contributing to severe acute malnutrition and moderate acute malnutrition (MAM) are multifaceted and include low birth weight, suboptimal infant and young child feeding practices, limited availability of health services, poor hygiene practices and inadequate access to clean water and sanitation facilities(Reference Rahman, Bhuiyan and Das2,Reference Islam, Rahman and Rahman10–Reference Kajjura, Veldman and Kassier12) .
Moderate wasting accounts for over 70 % of global cases(Reference Mostafa, Fahim and Das3,13) yet receives less programmatic attention than severe wasting. Children with MAM face a 3·1-fold higher mortality risk than well-nourished peers(Reference Mostafa, Fahim and Das3,14) and are vulnerable to progressing into severe wasting without timely intervention. This evidence gap hinders cost-effective scale-up of nutrition programs and slows progress towards sustainable development goals(Reference Islam, Rahman and Rahman10,14) . While comprehensive information exists on managing severe acute malnutrition children, there is limited evidence on the management of children with moderate wasting(14). Recognising this need, the WHO has called for additional evidence to inform cost-efficient interventions and initiated the NUTRIMAM trial (ISRCTN53213318) in three South Asian and two African nations. The idea is to provide three types of food supplements, namely, microbiota-directed supplementary food (MDSF), ready-to-use supplementary food (RUSF) and locally available food (LAF), along with comprehensive nutritional and hygiene-focused education. Nutrition education for mothers can improve knowledge, dietary habits and prevention of illness, and these effects are further enhanced when combined with supplementary meals for managing MAM(Reference Kajjura, Veldman and Kassier12,Reference Lassi, Das and Zahid15) . Interventions focused on caregiver education about appropriate complementary feeding have demonstrated significant improvements in nutritional outcomes(Reference Bhandari, Mazumder and Bhan16,Reference Santos, Victora and Martines17) . To effectively address the societal context and practical constraints in targeted communities, the program needs to prioritise practices that are both feasible and culturally acceptable(Reference Williams, Schnefke and Flax1,18,Reference Bekele and Turyashemererwa19) .
To evaluate the practicality and acceptability of supplements and counselling of the NUTRIMAM trial, a formative evaluation was conducted using the trials of improved practices (TIPs) approach(Reference Bekele and Turyashemererwa19). TIPs is a formative research approach that systematically gathers both quantitative and qualitative data from individuals and communities(Reference Bekele and Turyashemererwa19). The data help assess which health behaviours to promote, remove or modify and identify obstacles to adopting new practices such as proper breast-feeding positions, correct handwashing techniques and appropriate complementary feeding(Reference Williams, Schnefke and Flax1). TIPs was specifically selected over other formative research methods (e.g. focus groups and cross-sectional surveys) because it uniquely combines real-world practice testing with iterative participant feedback(18,Reference Shivalli, Srivastava and Singh20) . Developed by the Manoff Group, TIPs involves a structured series of visits where an interviewer and an interviewee engage in a discussion of current practices, potential areas for improvement and collaboratively arrive at one or a few solutions to implement during a trial period(18,Reference Bekele and Turyashemererwa19) . This methodology offers a direct avenue for acquiring insights from the participants engaged in the program and also allows them to participate in innovative activities. It also helps researchers identify techniques that align with cultural norms and are acceptable to the community(Reference Dickin, Griffiths and Piwoz21). This participatory approach is critical for designing acceptable interventions in resource-constrained settings where prescriptive recommendations often fail(Reference Bentley, Johnson and Wasser22).
The objective of this TIPs study was to identify key behavioural issues among mothers or caregivers of MAM children, focusing on breast-feeding, complementary feeding, hygiene, feeding practices during illnesses, strategies for managing picky eaters and approaches for delivering the study supplements. It also aimed to explore perceptions regarding packaged food and preparation of study foods at home. The findings were used to tailor the NUTRIMAM trial interventions, particularly by finalising LAF recipes, developing a feeding card to track supplement consumption, developing scripts for counsellors and designing an educational tool to promote behavioural changes at both individual and household levels.
Methods
Study setting
This formative study employed a cross-sectional design utilising mixed methods in Bauniabadh slum. Bauniabadh slum, located in Dhaka, Bangladesh, represents the complex challenges faced by urban poor communities. As of a 2014 census, it housed over 34 000 residents across more than 8600 households, with an average household size of four(Reference Khalequzzaman, Chiang and Hoque23). Living conditions are typically precarious; only 39 % of homes are constructed with concrete, while the rest are semi-concrete or temporary shelters(Reference Khalequzzaman, Chiang and Hoque23). Shared sanitation and communal kitchens are the norm, used by over 80 % of residents(Reference Khalequzzaman, Chiang and Hoque23,Reference Hasan, Rabbani and Ahmed24) . Although piped water is widely available, concerns remain about its quality(Reference Hasan, Rabbani and Ahmed24). Health system distrust, environmental hazards including frequent flooding and the risk of fires due to informal electrical wiring further exacerbate vulnerabilities(Reference Hasan, Rabbani and Ahmed24).
Study participants and sampling
Trained health workers first visited households in the study area to identify potential MAM children aged 6–24 months using mid-upper arm circumference (MUAC) tape and a total of 630 children were screened. Of these, 206 had an MUAC of 115–130 mm. We invited the caregivers of these 206 children to visit our field office for further assessment. Among them, 192 attended, and their children’s weight and length were measured to calculate weight-for-length z-score. Based on weight-for-length z-score, eighty-six children were classified as MAM. Enrolment was done using a purposive sampling technique and included a total of sixty-five children diagnosed with MAM (–3 ≤ weight-for-length z-score < –2 or 115 ≤ MUAC < 125 mm) and their mother or primary caregiver. Additionally, we excluded children with severe illnesses, persistent diarrhoea, chronic infections or disabilities requiring hospitalisation or currently receiving food supplements for moderate wasting. Each participant was thoroughly informed about the study and written informed consent was obtained from them.
Among the sixty-five enrolled caregiver-child pairs, ten were purposively selected for IDI and ten for household observations. To reflect diversity in the child’s age, one-third of the children were selected from 6–< 12 months age group, one-third from 12–< 18 months age group and remaining one-third from 18–< 24 months age group. The remaining forty-five participants were allocated to the food intervention arms, stratified by the same age groups to ensure balance. As a formative TIPs study, no power calculation was performed. The sample size was based on methodological guidance emphasising thematic saturation, feasibility and diversity of caregiver perspectives(Reference Hennink and Kaiser25–Reference Sharma, Mudgal and Gaur27). The overall flow of screening, enrolment and intervention allocation is illustrated in Figure 1.
Flow diagram of participant screening, enrolment and intervention allocation.

Data collection
We conducted in-depth interviews (IDI) using a semi-structured guide to explore caregivers’ behaviours and challenges related to complementary feeding, breast-feeding, WASH, illness and perceptions of packaged food. We also collected quantitative and anthropometric data using a structured questionnaire. Additionally, we used an observational toolkit to observe and document data on specific behaviours of caregivers at home. To ensure accuracy and reliability of collected data, we provided extensive training for the data collectors covering study objectives, ethics and data collection tools. The interview guideline, observation toolkit and survey questionnaires were adapted from previous studies in similar settings. They were reviewed by the study team and pilot-tested during training and initial field visits. Minor revisions were made based on this pilot feedback.
Anthropometry
Length and weight were measured by trained personnel using infantometer (0·1 cm precision) and digital scales (2 g sensitivity), and MUAC was assessed with standardised tapes. All measurements were taken twice; if discrepancies exceeded defined cut-offs (MUAC: 0·2 cm, weight: 0·10 kg and length: 0·5 cm), a third measurement was taken and the final value was the average of the two closest. Equipment was routinely calibrated for accuracy.
The whole study was conducted in two phases:
Phase-1
A team of trained interviewers conducted ten IDI to explore caregivers’ perceptions about hygiene, immunisation, breast-feeding, complementary feeding, feeding during illness and feeding practices for picky eaters. All the IDI were audio-recorded with consent for accurate transcription and analysis. On average, each IDI took 41 min to complete.
To observe daily activities of caregivers, trained field research assistants visited another ten households. They meticulously observed childcare activities for approximately 7 h and documented their observations using the observation toolkit.
Phase-2
In phase 2, we provided counselling and food interventions to forty-five caregiver–children pairs.
Counselling
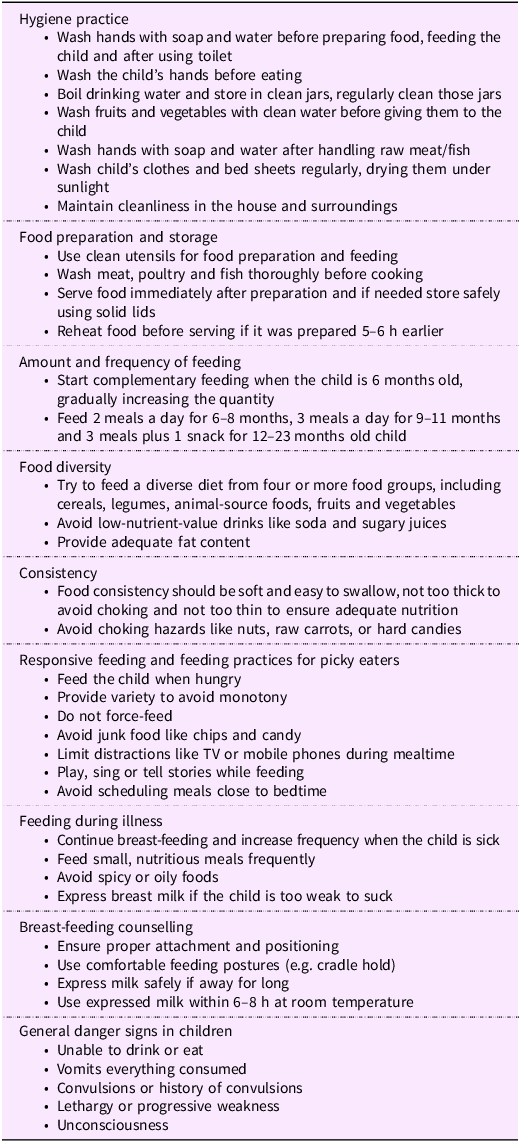
On the first day, each caregiver received counselling on complementary feeding, breast-feeding, WASH, feeding during illness, feeding techniques for picky eaters and vaccination (Table 1). Additionally, field assistants demonstrated a few practices such as steps for handwashing, breast-feeding attachment and positioning.
Recommended practices for caregivers of moderately wasted children aged 6–24 months

Food intervention
All forty-five participants were divided equally into three intervention arms: MDSF, RUSF and LAF (Figure 2). Each participant received one of the three interventions for 6 days. Our study staff also taught the caregiver how to prepare the food, feed the child and store the leftovers. Every participant was also given a feeding card to be filled out by the mothers to record compliance (Figure 3). Separate feeding cards were provided for each serving of meals for six days. The feeding card was adapted from previous community-based nutrition trials in Bangladesh. Trained staff explained its use to caregivers, and the card was applied consistently across all intervention arms.
Nutritional supplements provided to study participants. (a) ready-to-use supplementary food (RUSF) sachets. (b) microbiota-directed supplementary food (MDSF) sachets. (c) Prepared MDSF. (d) Prepared Khichuri. (e) Prepared Payesh. (f) Prepared Suji-Firni.

Feeding cards used to assess consumption of the provided supplements. (a) Card for MDSF and RUSF supplements; (b) card for locally available foods (LAF: Suji-Firni, Khichuri, or Payesh). For each meal, caregivers noted the recipe and meal time, and indicated intake by ticking one of five categories: 25 %, 50 %, 75 %, 100 %, or ‘food not provided’. Sections for participant ID, visit number and date were completed by study staff. All feeding cards were provided in the local language (Bangla) to facilitate understanding and consistent reporting. RUSF, ready-to-use supplementary food; MDSF, microbiota-directed supplementary food.

For the MDSF arm, each child was offered 100 g per day divided into two separate servings (50 g per serving). Mothers were instructed to finish the first serving within 4–5 h and then offer the second serving.
Fifteen children in the RUSF arm were given one RUSF packet per day for 6 days. Each RUSF packet contained 100 g of supplement, and caregivers were instructed to open a packet in the morning and finish it within 24 h.
For the LAF arm, we provided three different recipes, namely Khichuri, Payesh and Suji-Firni to all fifteen participants in a crossover design. Each participant received raw ingredients packaged in zip-lock bags, with a ration sufficient for two meals each day. Caregivers were taught how to prepare the recipes at home.
Follow-up
After the 6-d intervention, follow-up interviews were conducted with all forty-five participants using a semi-structured questionnaire. Responses were obtained and documented regarding their experience of the trial and any obstacles encountered during this period. We also collected consumption data using feeding cards and acceptability data using a seven-point hedonic scale (1 = dislike extremely, 2 = dislike moderately, 3 = dislike slightly, 4 = neither dislike nor like, 5 = like slightly, 6 = like moderately and 7 = like extremely)(Reference Sharif, Butt, Sharif, Khan and Farooq28).
Data analysis
Quantitative data were analysed using R version 4.5.0. Descriptive statistics were presented as medians (interquartile range) or mean (sd) for continuous variables and frequency (percentage) for categorical variables. Group comparisons for continuous data were performed using the One-way ANOVA or Kruskal–Wallis rank-sum test, while categorical data were analysed using Pearson’s χ 2 test or Fisher’s exact test.
Qualitative data from IDI and observations were analysed using NVivo 12. Transcripts were coded, and related codes were organised into themes. Themes were visually represented in matrices to identify patterns and relationships. Finally, data interpretation explored connections, contradictions and explanations to provide insights into caregivers’ perceptions and practices.
Results
Socio-demographic status
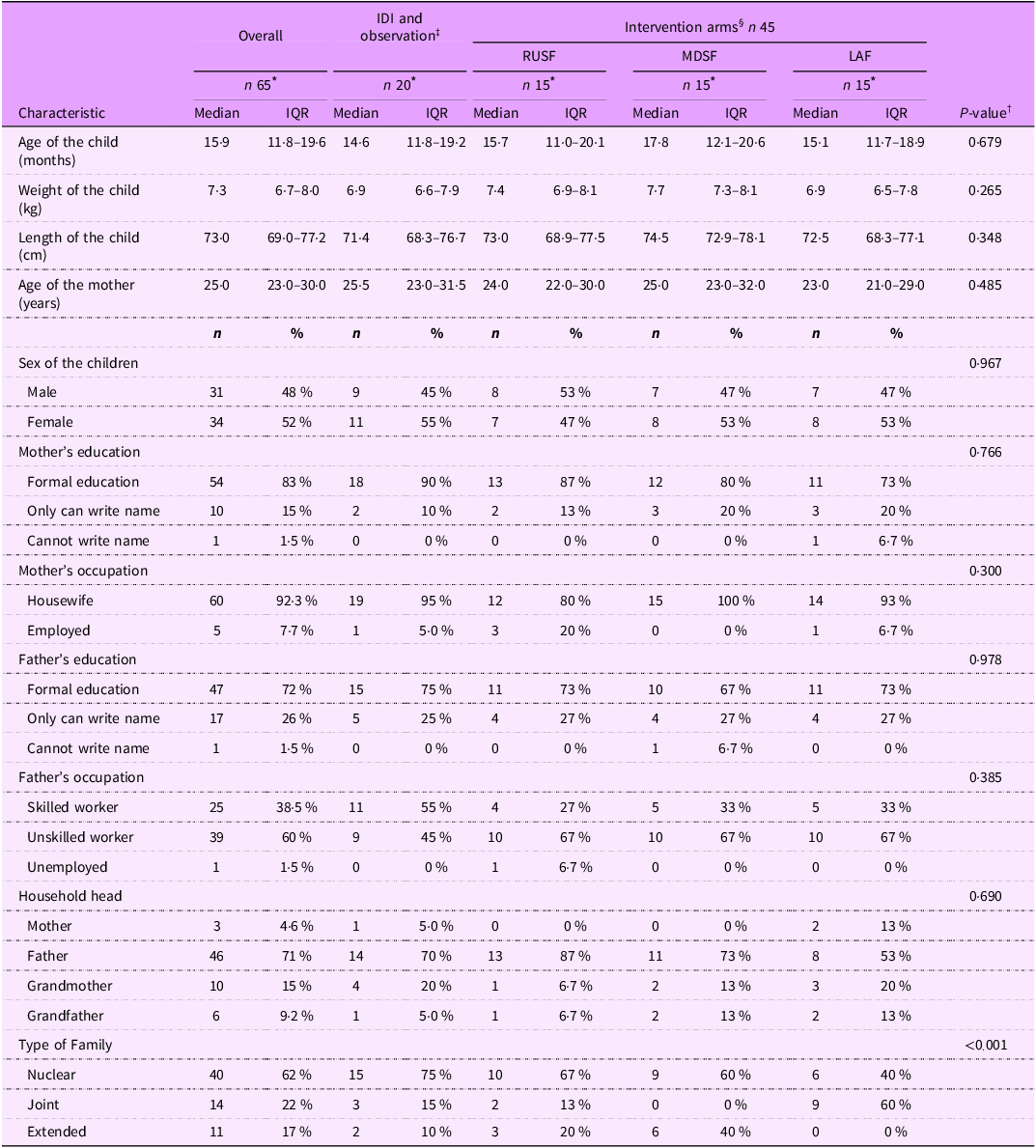
The study involved sixty-five children, with a median age of 15·9 months, median weight of 7·3 kg and length of 73·0 cm. Their gender distribution was almost equal (48 % male, 52 % female). Among them, forty came from nuclear families, fourteen from joint families and eleven from extended families. Around 71 % of households were led by fathers, with less than 5 % led by mothers. Approximately 83 % of mothers had some formal education, while fathers generally had slightly higher education levels, with only one being illiterate. Most mothers (92·3 %) were housewives, while others held positions in service, ready-made garments, tailoring or as housemaids. The fathers’ occupational distribution revealed a higher representation in unskilled labour (60 %), followed by skilled workers (38·5 %), with a minimal percentage (1·5 %) reporting unemployment (Table 2).
Socio-demographic characteristics of children and their primary caregivers or guardians (n 65)

IDI, in-depth interview; RUSF, ready-to-use supplementary food; MDSF, microbiota-directed supplementary food; LAF, locally available food; IQR, interquartile range.
* Median (IQR); n (%).
† Kruskal–Wallis rank sum test; Pearson’s χ 2 test; Fisher’s exact test.
‡ IDI and Observation (n 20) represent participants included in qualitative assessments.
§ RUSF, MDSF and LAF arms (n 45, 15 per arm) represent participants tested for acceptability of supplementary foods.
Findings from in-depth interview and observation
Findings from the initial phase of the study, which included IDI with ten caregivers and structured household observations of 10 caregiver–child pairs, revealed several key issues related to hygiene, breast-feeding and feeding practices. These qualitative insights are presented below.
Knowledge, attitude and practice related to safe drinking water in the community
Most families relied on scheduled water supply (1–3 times daily) or deep tube wells for drinking water. While many mentioned boiling and storing water, gas shortages often prevented them from doing so. Observations revealed that most households did not boil water or use other purification methods. Despite this, most respondents understood the importance of safe drinking water, stating that waterborne diseases such as diarrhoea, cholera or dysentery could occur if they drank untreated water.
‘Recently my husband and children suffered from stomach pain and diarrhoea. If we did not drink boiled water, this problem would be more frequent. I always try to boil water for my family members, but it’s challenging due to insufficient gas supply’ (40-year-old housewife with an 18-month-old child).
Knowledge, attitude and practice related to handwashing, sanitation and hygiene practices
All participants recognised the importance of handwashing with soap to prevent illness. They reported washing hands before meals, while feeding children, after using the toilet and after cleaning their child’s stool. However, while soap and water were generally available, most lacked knowledge of proper handwashing techniques or duration. Observations revealed gaps between reported and actual practices, particularly before food preparation and after handling raw meat or fish and sometimes after cleaning a child’s perineal area.
Regarding sanitation, shared toilets were common. Adults consistently used sanitary latrines, while young children typically used plastic commodes (‘potties’). Mothers usually disposed of this waste in toilets or near open sewer lines. For food hygiene, participants reported washing vegetables before cooking, covering food and cleaning utensils with soap and water. Yet observations showed these practices were inconsistent; some mothers used water only and utensils were not always clean before feeding children.
Mothers’ knowledge and attitude about breast-feeding
Participants were aware of the benefits of breast-feeding for child development. They said it strengthens the child and supports their mental and physical growth. Some mothers also mentioned health benefits for themselves, such as preventing breast pain and fever.
‘If I breastfeed my child, he will be intelligent. Breast milk means nutrition for him. Whatever I am eating, he is getting that nutrition through breast milk. He can’t eat like an adult, so breast milk benefits him. I also fed my child colostrum just after his birth’ (27-year-old mother of a 9-month-old child).
A common misconception was that breast milk alone meets all nutritional needs, leading them to prioritise breast-feeding over complementary feeding even after the recommended age. This perspective was echoed by a mother of a 17 month old:
‘I am breastfeeding my child. It will enhance her physical and mental growth. She will be intelligent, and it will protect her from any diseases. Many people asked me to feed her other food. But I didn’t provide her complementary food because breast milk is enough for her. As much as I can, I will feed her breastmilk. I will give her other food if she does not get breast milk’ (Housewife, age: 27 years).
Conflicting views emerged regarding optimal breast-feeding duration by gender. Some mothers believed boys and girls should be breastfed for the same period, while others expressed the opinion that boys should be breastfed longer than girls, or vice versa. The most common responses suggested 2·5 years for boys and 2 years for girls, while some believed 2 years for boys and 3 years for girls.
‘Our guardians told us that boys should leave the breast milk earlier, and girls should breastfeed for at least up to three years’ (25-year-old housewife having a 19-month-old child).
In contrast, another mother of a 15-month-old boy said:
‘A boy will be a man in later life. They will do more work than the girls in the future life. He needs more nutrition. Girls also need nutrition, but boys require more. So, boys should breastfeed more than girls’ (Housewife, age: 22 years).
Mothers’ practice related to breast-feeding
Breast-feeding frequency varied widely among children, ranging from 1–2 to 15–16 times daily. Mothers dedicated time exclusively for breast-feeding, with each session lasting 10–15 min up to half an hour, though household responsibilities sometimes shortened these sessions. A 23-year-old mother stated that,
‘I used to give enough time to my child during breastfeeding. I do not interrupt her if I do not have much work. I would have even spent 30 min to one hour if I were not too busy. But I usually spend 10 to 15 min breastfeeding if I have other household work. If I were not busy, breastfeeding time is a small leisure time for me also’ (Housewife, having a child of 8 months).
Most mothers preferred lying positions for breast-feeding but sometimes adapted the position to what their child preferred. Another mother of a 21-month-old child stated that,
‘My child preferred both positions. When asleep, he prefers to drink breast milk lying down; when he does not, he prefers to drink sitting. It’s up to him. I always breastfeed him in his preferred position’ (Housewife, 25 years).
However, no participant could describe standard breast-feeding positions, head support techniques or proper nipple alignment. Observations reflected these knowledge gaps, as feeding positions and attachment consistently deviated from recommended practices, and mothers frequently demonstrated limited patience during feeding.
Initiation of complementary feeding
Most mothers introduced complementary foods after 6 months, typically starting with formula or powdered milk while continuing breast-feeding. Homemade foods soon became the norm, with semolina (suji), noodles and bananas as initial choices. Within 2–3 months, children were introduced to family foods such as soft hotchpotch or vegetable blends. Diets gradually diversified to include rice, vegetables, eggs, cow’s milk, lentils and commercial foods like noodles or biscuits. A minority of mothers (20 %) relied on formula milk or commercial feeds for a longer period.
One mother stated about the feeding practices that,
‘We usually eat three times a day. I tried to feed him with me. I gave him snacks between these three meals, like bananas, biscuits, or bread. Due to a gas supply shortage, I couldn’t prepare homemade snacks for him’ (a 21-year-old housewife and mother of a 10-month-old child).
Feeding practices for children
Most mothers encouraged self-feeding and allowed sufficient mealtime, typically avoiding force-feeding. Some engaged their children through talking, playing or walking during feeding sessions. A 40-year-old mother stated that,
‘I never forced my children to eat. If he didn’t want to eat, I tried two or three times, then left the food; sometimes, I kept the food in front of him, and if he liked to eat something, he could. Otherwise, I left the food. I heard forcing is not good, and I never did that’ (Housewife having a child of 18 months old).
However, opposite practices also existed in the community. Some mothers force their children to eat food. One mother admitted:
‘Sometimes I forced my child. She needs to eat some food. If she didn’t eat food, I had to force her. Sometimes I took her outside of the home, sometimes to the roof. Sometimes if she didn’t want to eat, I beat her’ (a garment worker, age: 22 years, mother of a 15-month-old child).
Observations revealed that half of the mothers showed inadequate attention and patience during feeding. Responsive feeding was often lacking with distractions such as mobile phones. Some mothers resorted to force-feeding, without offering an alternative when children refused. If children showed reluctance to eat homemade food, mothers frequently offered commercially prepared alternatives including chocolate, chips, biscuits, cake, bread and noodles. These were usually consumed in the afternoon or evening, replacing dinner.
Feeding during illness
During illness, children commonly reduced their food intake and were reluctant to eat family meals or breastmilk. Mothers reported that their children commonly preferred outside foods during sickness, and they tried to offer whatever foods their children liked. In cases of diarrhoea, all mothers were aware of and practiced administering Oral Rehydration Solution.
Findings of follow-up visit
Handwashing
Most mothers reported washing hands before preparing food, feeding their child and after using the toilet or cleaning the child. Many felt cleaner after following our instructions to wash with soap and water. However, a few struggled due to time constraints, limited soap or water or forgetfulness. Most wished to continue these practices and educate neighbours or relatives, though some were concerned that others might not take them seriously because of social stigma.
Breast-feeding
Almost all mothers understood the recommendation to breastfeed their child up to 2 years, regardless of sex, while following proper techniques. Those who tried the new positions reported greater comfort for themselves and their children and intended to continue in the future.
Responsive feeding
The majority of caregivers practiced responsive feeding by talking, singing or pointing out objects, while avoiding force-feeding and digital distractions. When children refused food, they stored leftovers in closed containers for later use after reheating. Although most successfully boiled drinking water, some faced obstacles such as interruptions in gas or electricity supply during boiling or reheating.
Intervention
Consumption patterns showed that LAF was generally consumed at slightly higher rates than RUSF and MDSF. Overall compliance over the 6-d intervention was good, with mean consumption of 68·9 % for LAF, 68·1 % for RUSF and 62·5 % for MDSF (Table 3). Among the LAF recipes, Suji-Firni was particularly convenient due to its short preparation time (5–8 min), while Khichuri and Payesh required more time.
Consumption (%) of three supplementary foods: RUSF, MDSF and LAF, presented as mean (sd) and median (IQR)

RUSF, ready-to-use supplementary food; MDSF, microbiota-directed supplementary food; LAF, locally available food; IQR, interquartile range.
* One-way ANOVA.
† Kruskal–Wallis rank sum test.
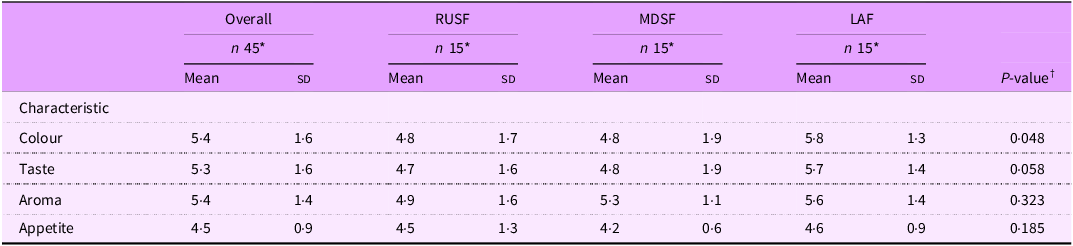
Based on sensory evaluation, mean scores for colour, taste, aroma and appetite were generally favourable across all three supplementary foods (Table 4). LAF scored slightly higher than RUSF and MDSF in all categories, with the highest ratings for colour (5·8 (sd 1·3)) and taste (5·7 (sd 1·4)). A statistically significant difference was observed for colour (P = 0·048), while differences in taste, aroma and appetite were NS. A few mothers noted that the sweetness level was slightly higher than their regular diet, and there was unfamiliarity with packaged foods. Additionally, the sticky texture sometimes caused the food to adhere to the upper palate of the children.
Sensory evaluation scores (mean (sd)) provided by caregivers for three supplementary foods: RUSF, MDSF and LAF

RUSF, ready-to-use supplementary food; MDSF, microbiota-directed supplementary food; LAF, locally available food.
* Mean (sd).
† One-way ANOVA.
Approximately half of the mothers preferred weekly home visits for interventions, while others favoured intervals of 3–4 d between each delivery. Two-thirds felt that all counselling topics could be covered in a single, longer session, though they recognised the difficulty of retaining and applying all information at once. The remaining third recommended shorter, separate sessions focused on specific topics to improve message retention and practical implementation.
Discussion
Formative research using the TIPs method is valuable in the development of behavioural programs as it provides a comprehensive understanding of contextual factors and the current habits and beliefs of community members who might benefit from the program. This understanding is crucial for designing effective programs and predicting their impact on nutrition-related outcomes(Reference Williams, Schnefke and Flax1,Reference Bentley, Johnson and Wasser22,Reference Daelmans, Ferguson and Lutter29–Reference Sanghvi, Jimerson and Hajeebhoy33) . The TIPs process outlined in this article aimed to validate the feasibility of the planned intervention and counselling prior to implementing the ‘NUTRIMAM’ trial. The proposed food interventions were assessed in households, and messages were adjusted during follow-up visits. This study explored caregivers’ usual practices and the barriers they faced when suggested to improve these practices. We also sought to understand their reactions when offered new packaged foods and alternative ways of cooking for their child using locally available ingredients. The process provided additional and often unexpected insights regarding hygiene and feeding practices among caregivers in this context.
The study underscores the significance of adopting safe water practices and the challenges caregivers face in maintaining consistent access to clean water. Despite awareness of waterborne diseases, limited access to resources, such as gas for boiling water, remains a significant barrier. Results from previous research that assessed slum dwellers’ access to safe drinking water in Dhaka appear to corroborate these findings(Reference Haque, Yanez-Pagans and Arias-Granada34). While most caregivers understood the importance of handwashing, a gap between knowledge and observed practice was evident. This discrepancy mirrors global trends where the adoption of handwashing remains limited, despite advocacy efforts in Bangladesh and other regions to promote this crucial technique for disease prevention(Reference Curtis, Danquah and Aunger35–Reference Amin, Sagerman and Nizame38).
Misconceptions about breast-feeding duration and exclusivity highlight the need for targeted education. There is a necessity to emphasise the complementary nature of breast-feeding and the proper introduction of complementary feeding after 6 months. Observations and interviews also revealed varied complementary feeding practices, limited dietary diversity and gaps in responsive caregiving. Similar findings have been reported among mothers of infants aged 6–24 months in Dhaka slums(Reference Saleh, Ara and Hoque39).
The trial of different food supplements, including MDSF, RUSF and LAF, presents nuanced insights into their acceptability and the challenges faced by caregivers. The intervention highlighted generally good acceptance of all three supplementary foods, though practical challenges were noted. Slightly lower intake for some children may reflect the short duration of the intervention and the adaptation period required for new foods or minor illness episodes. Consumption of MDSF and RUSF may potentially be affected by barriers such as unfamiliarity with packaged foods, the sticky texture or more sweetness than their usual diet. Addressing these issues might involve diluting a small portion of MDSF or RUSF with milk or water just before feeding, particularly for children transitioning from exclusive breast-feeding. A previous study also suggested that therapeutic foods be mixed with other ingredients to improve taste and swallowability(Reference Nikièma, Fogny and Kangas40). LAF recipes, particularly Suji-Firni, were more convenient due to shorter preparation times, and higher acceptance of LAF may be attributed to its familiarity, as it uses ingredients already part of children’s regular diets. Moreover, similar sensory scores across all attributes for the three interventions suggest none had undesirable effects, supporting their integration into routine feeding practices.
To enhance the acceptability of MDSF and RUSF, we propose peer-led demonstrations by early adopters, use of single-serving sachets, culturally appropriate packaging and tailored counselling(Reference Nikièma, Fogny and Kangas40–Reference Ahmed, Choudhury and Hossain43). These approaches address barriers related to preparation burden, unfamiliar taste, and distrust of packaged foods and align with successful strategies in similar settings. In contrast, the positive reception of LAF recipes signifies the feasibility of utilising locally available familiar ingredients for scaled-up program, though implementation requires addressing key operational barriers(Reference Bekele and Turyashemererwa19). Evidence from TIPs studies in Uganda shows that caregivers are more likely to adopt recipes that use familiar ingredients and preparation methods(Reference Bekele and Turyashemererwa19). While LAF’s cultural acceptability and caregiver familiarity support adoption, successful scale-up may involve simplifying preparation through pre-mixed ingredient kits(Reference Lassi, Das and Zahid15), introducing community-based production hubs to mitigate shortages of utilities (gas or water)(Reference Haque, Yanez-Pagans and Arias-Granada34) and integrating LAF distribution with existing health service platforms like vaccination campaigns(Reference Lanou, Somé and Koumbem44). These adaptations reflect time‑saving community feeding strategies that have proven effective in similar contexts(Reference Bekele and Turyashemererwa19). However, decentralised production requires strong quality control to prevent nutrient loss and safety issues(Reference Fetriyuna, Purwestri and Jati45). Importantly, cost-effectiveness and supply-chain feasibility of LAF v. packaged supplements will be evaluated in the upcoming NUTRIMAM trial. These assessments will inform sustainability and scalability.
The study was conducted in a single urban slum, and findings may not be generalisable to other slum or rural settings with different socio-economic or cultural contexts; therefore, multi-site replications across diverse settings are needed. Second, the one-week trial period for new techniques, while aligned with the TIPs manual, may be insufficient to assess sustained behaviour change. Increasing the length of this study, as has been shown in earlier studies(Reference Shivalli, Srivastava and Singh20,Reference Dickin and Seim46) and as planned for NUTRIMAM trial, may help assess sustained behaviour change more effectively. Third, feeding practices were assessed through caregiver-reported cards, which are vulnerable to recall and social desirability bias. Direct methods like supplement weighing or observed feeding would strengthen validity. Fourth, unmeasured confounders such as maternal education or prior exposure to nutrition interventions, seasonal income changes, food insecurity or other concurrent health interventions may have influenced the outcomes but were not captured and should be considered in future trials. Occasionally, caregivers may provide information that aligns with societal expectations rather than their actual experiences or intentions, thereby influencing our interpretation of the study findings. Additionally, presence of observers during household visits may have influenced caregiver behaviour, a phenomenon known as the Hawthorne effect(Reference Mostafazadeh-Bora47,Reference McCarney, Warner and Iliffe48) . Although the team aimed to minimise reactivity through rapport-building, this potential observer bias is a recognised limitation in behavioural studies(Reference McCarney, Warner and Iliffe48). Lastly, as a formative, exploratory study, it was not powered for statistical comparisons or hypothesis testing. Despite these limitations, these constraints do not undermine the significance of these findings as fundamental information to shape future interventions or programs.
Conclusion
This mixed-methods TIPs study identified critical context-specific behaviours and preferences affecting feeding practices among caregivers of moderately wasted children in a Dhaka slum. Caregivers reported suboptimal hygiene practices, rarely boiling drinking water and washing hands with water only, and using mobile phones during feeding, reducing responsive engagement. In the supplement trial, all three interventions (MDSF, RUSF and LAF) achieved similar median consumption, but caregivers consistently rated the LAF recipes higher in taste and overall appeal than MDSF or RUSF. These findings suggest that while all supplements were generally acceptable, familiar, locally sourced foods may improve adherence.
Immediate next steps include finalising simplified LAF recipes for household and community kitchens and developing a shelf-stable version of MDSF. Training modules should be developed for community health workers to deliver supplement-specific counselling and reinforce hygiene and feeding practices. Concurrently, policy-level action is needed, requiring multi-stakeholder taskforces involving government, NGO and manufacturers to address systemic barriers, including intermittent utilities and food access challenges, through coordinated community nutrition strategies. Future research should evaluate the cost-effectiveness of these approaches across diverse South Asian contexts while monitoring long-term impacts on child nutrition, growth and development. These steps will help translate formative research insights into sustainable interventions that improve child nutrition and caregiving practices in urban slum settings.
Acknowledgements
We would like to thank all the participants and their parents for sharing their time and providing the consent and information necessary for the successful completion of the study. We appreciate the hard work of our committed data collectors and field staff in obtaining consent, enrolling participants and carrying out all study-related tasks. The authors also acknowledge the contribution of icddr,b’s core donors, including the Government of the People’s Republic of Bangladesh and Canada, for their continuous support and commitment to the icddr,b’s research efforts.
Financial support
This study is part of the NUTRIMAM trial (ISRCTN53213318), funded by the World Health Organization (WHO) (WHO Reference: 2022/1219960-0, 2022/1256900-0, 2024/1435641-0). The funder had no involvement in designing the study, data collection, analysis, interpretation, writing this article or submission for publication.
Competing interests
There are no conflicts of interest.
Authorship
M.H.H.R.: Methodology, Data curation, Visualization, Formal analysis, Writing – Original draft preparation; I.M.: Conceptualization, Methodology, Writing – review & editing; J.F.: Data curation, Writing – review & editing; K.N.S.: Conceptualization, Methodology; T.S.: Writing – review & editing; M.M.R.: Data curation, Writing – review & editing; T.A.: Conceptualization, Writing - Review & Editing, Supervision. All authors read and approved the final manuscript.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Research Review Committee (RRC), Ethical Review Committee (ERC) of icddr,b ensuring strict compliance with ethical standards in all human-involved research procedures (Protocol No: PR-21087). Moreover, this trial is also approved by the Institutional Review Board (IRB) of WHO. Written informed consent was obtained from all subjects/patients. The privacy and anonymity were maintained throughout the study.





 Open access
Open access