


Schizophrenia spectrum disorders (SSDs), including schizophrenia and schizoaffective disorders, are among the leading causes of disability worldwide, with their rising prevalence causing increased burden over recent decades. Reference Vigo, Thornicroft and Atun1,2 People living with SSDs experience profound reductions in life expectancy, dying an average of 10–20 years earlier than the general population. Reference Correll, Solmi, Veronese, Bortolato, Rosson and Santonastaso3 The majority of these of premature deaths can be attributed to physical health comorbidities, particularly outcomes related to metabolic syndrome, such as cardiovascular disease (CVD). Reference Correll, Solmi, Veronese, Bortolato, Rosson and Santonastaso3
Weight gain is a major modifiable risk factor for CVD in SSDs, with the side-effects of antipsychotic medications playing a central role. For example, meta-analyses of individuals initiating antipsychotic treatment report rapid weight gain, with clozapine and olanzapine associated with the greatest increases. Reference Tek, Kucukgoncu, Guloksuz, Woods, Srihari and Annamalai4,Reference Burschinski, Schneider‐Thoma, Chiocchia, Schestag, Wang and Siafis5 Further evidence indicates that switching to certain antipsychotic medications can induce additional weight gain. Reference Siskind, Gallagher, Winckel, Hollingworth, Kisely and Firth6 The burden of antipsychotic-associated weight gain goes beyond increased risks of CVD and metabolic syndrome, contributing to increased stigma, Reference Townsend, Pareja, Buchanan-Hughes, Worthington, Pritchett and Brubaker7 reduced treatment adherence Reference De, Smith, Navagnanavel, Au, Maksyutynska and Papoulias8 and poorer quality of life. Reference Masand and Gupta9 Behavioural approaches, including structured dietary modification and exercise programmes, have shown some efficacy for weight management in people with SSDs; however, their effects are typically modest, and implementation can be resource intensive. Reference Stevens, Smith, Bussey, Innerd, McGeechan and Fishburn10,Reference Lee, Piernas, Stewart, Michalopoulou, Hajzadeh and Edwards11 Pharmacological adjuncts have, therefore, been explored as alternative or complementary strategies. Among these, metformin has demonstrated modest efficacy in reducing antipsychotic-associated weight gain, with pooled estimates suggesting an average benefit of approximately 3 kg relative to placebo and no clear excess of adverse events. Reference Yu, Lu, Lai, Hahn, Agarwal and O’Donoghue12 Despite these gains, the overall impact of existing behavioural and pharmacological interventions remains insufficient to address the high prevalence and severity of obesity observed in SSDs, underscoring the need for more effective therapeutic options. Reference Vancampfort, Firth, Correll, Solmi, Siskind and De Hert13
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have emerged as a major advance in the management of obesity and type 2 diabetes in the general population, facilitating weight loss through a combination of glucose-dependent insulin secretion, delayed gastric emptying and centrally mediated appetite regulation. Reference Nauck, Heimesaat, Behle, Holst, Nauck and Ritzel14,Reference Doyle and Egan15 Early GLP-1 RAs such as exenatide and liraglutide produced clinically meaningful weight loss in the general population. Reference Vosoughi, Atieh, Khanna, Khoshbin, Prokop and Davitkov16 An individual participant data meta-analysis of exenatide and liraglutide trials in people with schizophrenia reported modest weight loss of almost 4 kg, which is comparable to that observed with metformin, but also identified higher rates of adverse events among participants receiving these two agents. Reference Siskind, Hahn, Correll, Fink‐Jensen, Russell and Bak17 In contrast, newer GLP-1 RAs such as semaglutide and tirzepatide have demonstrated substantially greater weight reductions in the general population. For example, Wilding and colleagues reported weight loss of almost 15% versus placebo after 68 weeks of 2.4 mg semaglutide. Reference Wilding, Batterham, Calanna, Davies, Van Gaal and Lingvay18 Furthermore, studies examining tirzepatide have yielded substantial weight loss exceeding 15% across similar time frames, Reference Jastreboff, Aronne, Ahmad, Wharton, Connery and Alves19 with comparative effectiveness studies concluding that tirzepatide is superior to semaglutide in terms of weight loss. Reference Aronne, Horn, le Roux, Ho, Falcon and Gomez Valderas20 Similarly to the large liraglutide and exenatide studies, these large semaglutide and tirzepatide studies excluded people with SSDs. Of the trials that have examined semaglutide in people with SSDs, results have mirrored and exceeded those seen in the general population, with no evidence of unwanted effects regarding medication interaction or psychosis symptoms. Reference Siskind, Baker, Arnautovska, Warren, Russell and DeMonte21 However, results of semaglutide and tirzepatide studies have not been systematically evaluated in SSD populations to date. The aim of this study, therefore, is to synthesise the available evidence evaluating the effectiveness and safety of semaglutide and/or tirzepatide in individuals with SSDs.
Method
This systematic review and meta-analysis was conducted as per the Preferred Reporting of Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria, Reference Page, Moher, Bossuyt, Boutron, Hoffmann and Mulrow22 and followed a publicly available protocol (PROSPERO identifier: CRD420251247162; registered 9 December 2025; data extracted 15 December 2025; no amendments were made to the protocol). The PRISMA checklist can be found in the Supplementary Material.
Searches were conducted on 6 December 2025 across PubMed, EMBASE, PsycINFO, Scopus and CENTRAL databases. The full search strategy can be found in the Supplementary Material. Duplicates were automatically excluded, with titles and abstracts screened by two independent reviewers (M.T. and K.V. (see ‘Acknowledgements’ section)). Following title and abstract screening, full-text articles were retrieved and screened by two independent researchers (U.A. and K.V.), and data extracted by two independent researchers (M.T. and K.V.) using a custom spreadsheet. Agreement between independent reviewers was 100% across all screening and extraction stages, therefore no senior arbitration was required. The reference lists of these full texts were also examined. The inclusion criteria used to identify appropriate studies were:
-
(a) population: people diagnosed with SSDs according to the ICD-x or DSM-x criteria, or via medical records – studies including mixed diagnostic populations were eligible if results for participants with SSDs were reported separately, or if the recruited sample consisted exclusively of individuals with SSDs despite broader eligibility criteria;
-
(b) intervention: semaglutide or tirzepatide at any dosage across any time frame;
-
(c) comparator: placebo control groups only;
-
(d) outcome: any outcomes;
-
(e) study design: randomised controlled trials (RCTs) only.
Statistical analysis
Outcomes were meta-analysed when there were at least three component studies. If fewer than three studies reported similar outcomes, these were narratively reviewed. For continuous outcomes, units were standardised where appropriate (see Supplementary Table 1 for full information), and a random-effects meta-analysis was subsequently conducted with the restricted maximum likelihood method, with heterogeneity quantified using τ 2. Prediction intervals were also created. Publication bias was assessed with funnel plot asymmetry unless there were fewer than ten component studies, in which case publication bias was not assessed. Reference Higgins and Green23 Adverse events were pooled using the terminology reported in the original trial publications, with no reclassification of adverse event definitions undertaken. Serious adverse events were defined according to the criteria used in each individual trial. Adverse events were also meta-analysed if there were three or more studies reporting the same adverse events. For adverse events, events and non-events were converted into risk ratios, with log- transformed risk ratios meta-analysed using the same methods as for continuous outcomes and back-transformed into risk ratios for interpretation.
Risk-of-bias assessment
Risk of bias for each study was determined with the Cochrane Risk of Bias 2 (RoB2) tool, Reference Sterne, Savović, Page, Elbers, Blencowe and Boutron24 by two independent researchers (M.T. and K.V.). Although a senior researcher (D.S.) was available to arbitrate any disputes, this was not required as agreement between the two independent researchers was 100%. Supplementary material for each component study was also reviewed.
Certainty assessment
The certainty of meta-analysed outcomes was assessed with the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, Reference Zhang, Akl and Schünemann25 rating outcomes in terms of risk of bias, inconsistency, indirectness, imprecision and publication bias.
Results
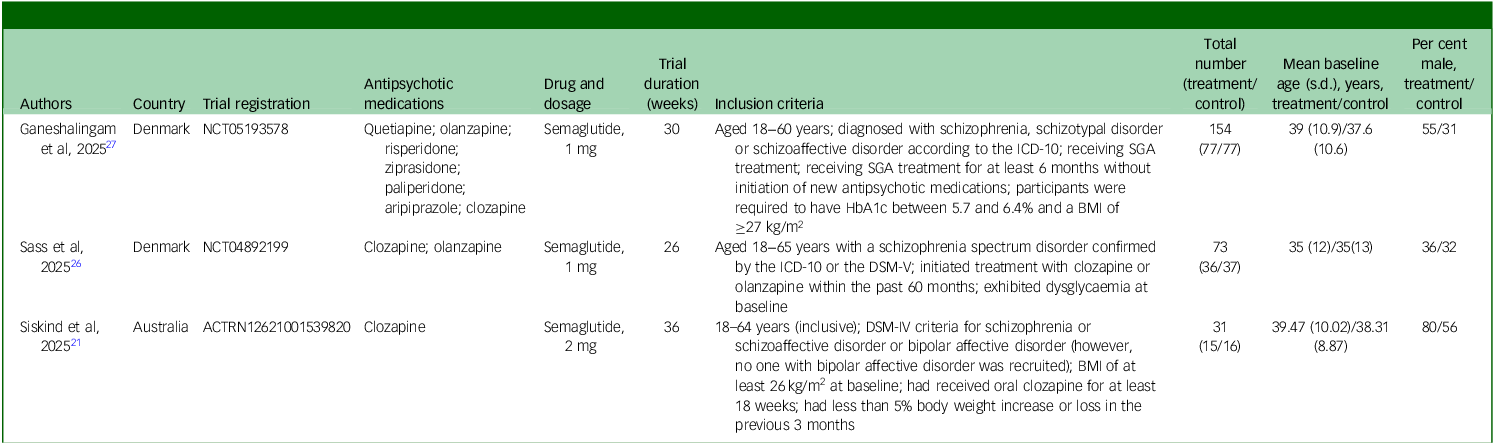
From an initial pool of 253 studies, 148 were screened at the title and abstract level, after which 11 studies were retrieved for full-text review. Following full-text review, three studies satisfied the inclusion criteria and were included in the final review. Reference Siskind, Baker, Arnautovska, Warren, Russell and DeMonte21,Reference Sass, Klausen, Schwarz, Rasmussen, Giver and Hviid26,Reference Ganeshalingam, Uhrenholt, Arnfred, Gæde, Düring and Stenager27 The PRISMA flowchart can be found in Fig. 1 and full reasons for full text exclusion can be found in Supplementary Table 2. Full descriptive information of each component study can be found in Table 1. Two studies were conducted in Denmark, Reference Ganeshalingam, Uhrenholt, Arnfred, Gæde, Düring and Stenager27,Reference Fink-Jensen, Wörtwein, Klausen, Holst, Hartmann and Thomsen28 with the third conducted in Australia, Reference Siskind, Baker, Arnautovska, Warren, Russell and DeMonte21 with two studies conducted in community dwelling samples (one study did not specify the setting). All three studies examined semaglutide (total n = 258), with two studies examining 1.0 mg dosages and one study examining 2.0 mg. No studies examining tirzepatide were found. Trial durations ranged from 26 to 36 weeks. Regarding the risk of bias of component studies, every study was deemed to have low risk of bias (see Supplementary Table 3 for full information).
Preferred Reporting of Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.

Description of included studies

SGA, second-generation antipsychotic; HbA1c, haemoglobin A1c; BMI, body mass index.
Continuous outcomes
Meta-analysis
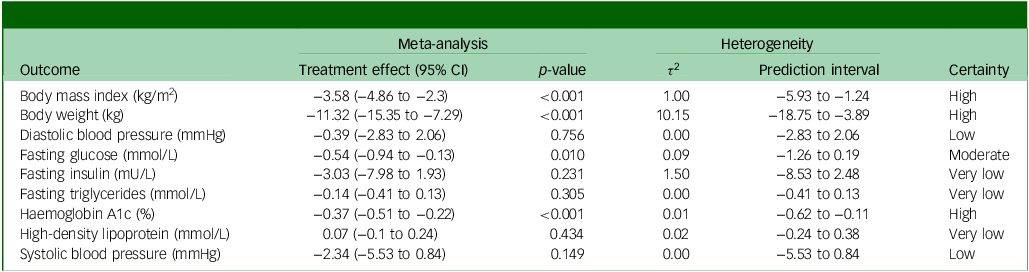
Nine continuous outcomes were collected across all three component studies and included in the meta-analysis. Three outcomes yielded significant results with a high degree of certainty: body mass index (pooled treatment effect: −3.58 kg/m2; 95% CI −4.86 to −2.3 kg/m2; p ≤ 0.001), body weight (pooled treatment effect: −11.32 kg; 95% CI −15.35 to −7.29 kg; p ≤ 0.001) and haemoglobin A1c (pooled treatment effect: −0.37%; 95% CI −0.51 to −0.22%; p ≤ 0.001). Fasting glucose also yielded a significant treatment effect (−0.54 mmol/L; 95% CI −0.94 to −0.13 mmol/L; p = 0.01) at moderate certainty. All other outcomes, outlined in Table 2, were not statically significant, with either low or very low levels of credibility. Full descriptions on how credibility was graded is shown in Supplementary Table 4.
Meta-analysis results of continuous outcomes

Narrative synthesis
Across outcomes not included in the meta-analysis, the most consistent effects were observed for anthropometric and body composition measures. For example, significant and consistent reductions were reported across the two studies that measured body fat percentage and waist circumference, which reported consistent decreases in visceral fat; however, this was not significant in the Sass et al trial. Reference Sass, Klausen, Schwarz, Rasmussen, Giver and Hviid26 Furthermore, Siskind et al Reference Siskind, Baker, Arnautovska, Warren, Russell and DeMonte21 reported significant decreases in fat mass, lean mass and body fat percentage, and Ganeshalingam et al Reference Ganeshalingam, Uhrenholt, Arnfred, Gæde, Düring and Stenager27 reported significant decreases in hip circumference. In contrast, there were no significant changes in waist/hip ratio and bone mineral content in any of the three trials.
For cardiometabolic and glycaemic outcomes, effects were mostly inconsistent. Two studies reporting on insulin resistance yielded consistent decreases, but neither reached statistical significance. C-peptide demonstrated opposing, non-significant effects across studies, and no clear signal was observed for the Framingham Cardiovascular Index. Similarly, lipid and vascular markers showed no consistent pattern, with non-significant and conflicting effects for low-density lipoprotein and total cholesterol, but consistent reductions in triglycerides and heart rate across studies, albeit without statistical significance. Liver and renal biomarkers were largely unchanged, except for a significant reduction in alkaline phosphatase and significant increase in creatinine, reported by Sass et al. Reference Sass, Klausen, Schwarz, Rasmussen, Giver and Hviid26
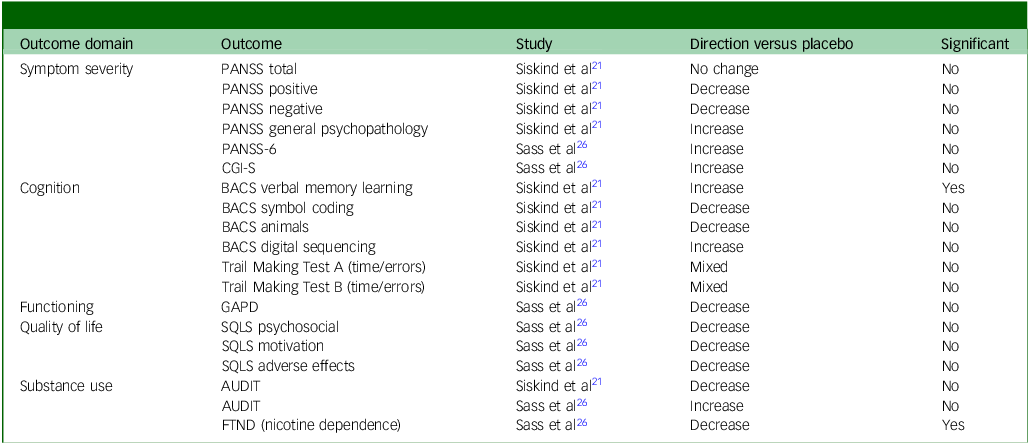
Across psychiatric symptom severity, cognition and functioning, no consistent evidence of clinical worsening was observed. Psychosis symptoms, measured using the Positive and Negative Syndrome Scale total and subscale scores; overall symptom severity, measured using the Clinical Global Impression − Severity scale; and most areas of cognitive performance, measured with Brief Assessment of Cognition in Schizophrenia, showed non-significant and/or conflicting results across studies. Measures related to substance use and quality of life were similarly mixed, although a significant reduction in nicotine dependence was reported by Sass et al. Reference Sass, Klausen, Schwarz, Rasmussen, Giver and Hviid26 Physical activity and sedentary behaviour outcomes were highly variable and imprecise. Finally, clozapine and norclozapine concentrations showed no significant or consistent changes as reported by Siskind et al. Reference Siskind, Baker, Arnautovska, Warren, Russell and DeMonte21 Full information on outcomes not included in the meta-analysis can be found in Table 3 and Supplementary Table 5.
Clinical, cognitive, and functional outcomes not included in the meta-analysis

PANSS, Positive and Negative Syndrome Scale; CGI-S, Clinical Global Impression–Severity; BACS, Brief Assessment of Cognition in Schizophrenia; GAPD, Global Assessment of Psychosocial Disability; SQLS, Schizophrenia Quality of Life Scale; AUDIT, Alcohol Use Disorders Identification Test; FTND, Fagerström Test for Nicotine Dependence.
Adverse events
Meta-analysis
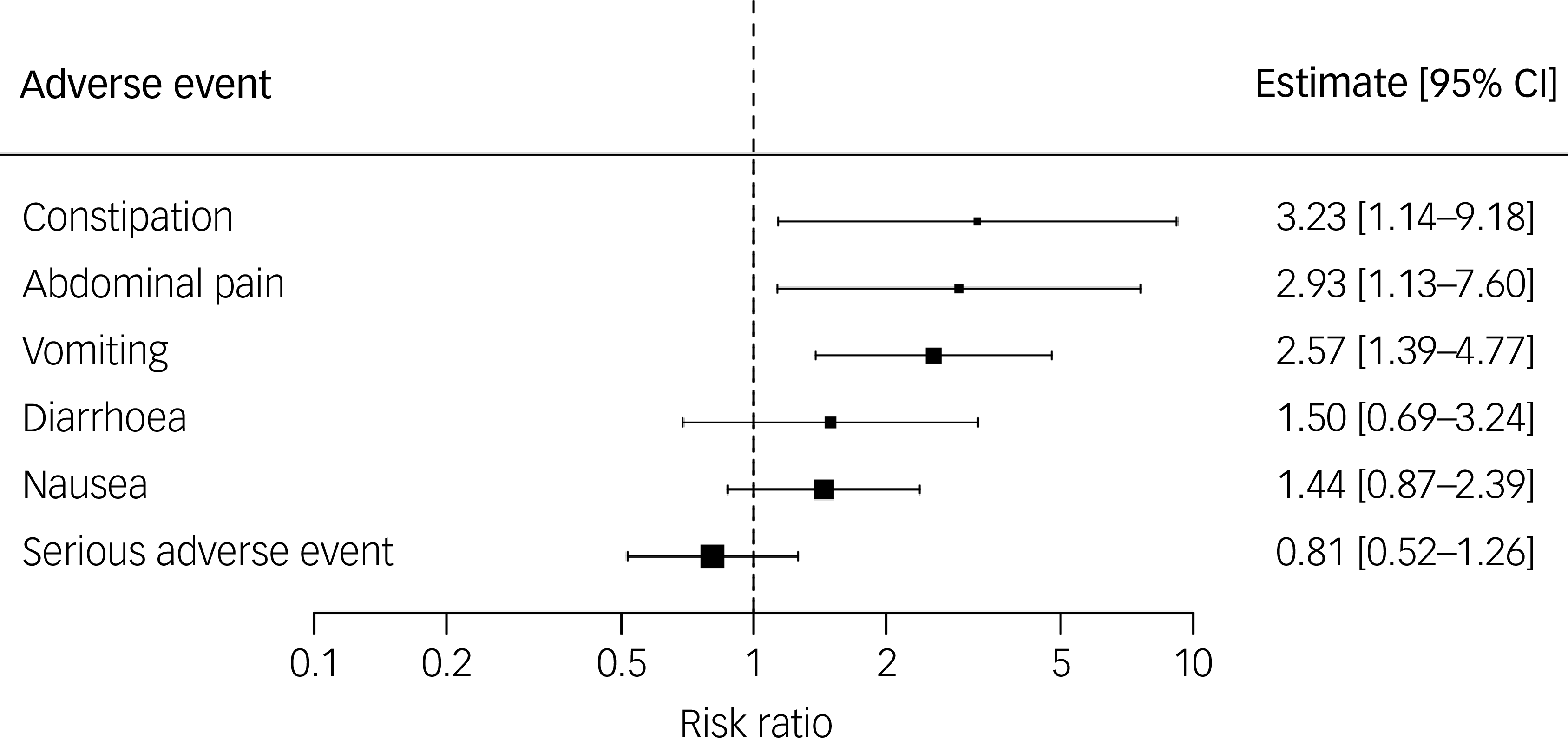
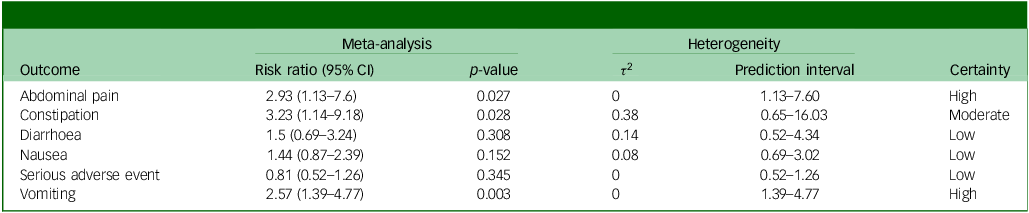
Six types of adverse events were reported in enough studies to be included in the meta-analysis: any serious adverse events, abdominal pain, vomiting, diarrhoea, nausea and constipation (one study did not report ‘any adverse events’ and therefore was not included in the meta-analysis). The risks of abdominal pain (risk ratio 2.93; 95% CI 1.13−7.60; p = 0.03) and vomiting (risk ratio 2.57; 95% CI 1.39−4.77; p ≤ 0.01) were significantly higher in the semaglutide group, with a high degree of certainty. Furthermore, the risk of constipation (risk ratio 3.23; 95% CI 1.14−9.18; p = 0.03) was significantly higher in the semaglutide group, with a moderate degree of certainty. All other adverse event outcomes did not significantly differ between groups. Full information can be found in Table 4 and Fig. 2, and details on how certainty was graded are in Supplementary Table 6.
Forest plot showing risks of adverse events in semaglutide versus placebo groups.

Meta-analysis results of adverse events

Narrative synthesis
No consistent or replicated adverse events were observed across studies in terms of the non-meta-analysed adverse events. Most adverse events were reported by single studies, with study-level risk ratios being highly imprecise because of low event counts. Rates of any adverse event and adverse events leading to discontinuation were broadly comparable between semaglutide and control groups, with risk ratios close to unity where reported, suggesting no clear excess overall treatment-related harm.
Where individual adverse events were reported in more than one study, direction of effect was frequently inconsistent, particularly for gastrointestinal and neurological symptoms such as dizziness, fatigue, headache and flatulence. Gastrointestinal events were common across studies, but showed variable effect sizes and limited reproducibility. Psychiatric adverse events, including psychiatric admissions, self-harm and suicidal behaviour, were infrequently reported and did not demonstrate a consistent pattern of increased risk. Importantly, no consistent changes in serious adverse events, infections or mortality-related outcomes were observed. Full adverse event data can be found in Supplementary Table 7.
Discussion
This systematic review and meta-analysis synthesised the published RCTs evaluating semaglutide and/or tirzepatide in people with SSDs. None of the identified trials in this population examined tirzepatide. In all three included trials, semaglutide yielded clinically meaningful improvements in weight and glycaemic outcomes, with high certainty evidence for reductions in body mass index, body weight and haemoglobin A1c, and moderate certainty for fasting glucose, compared with placebo. Across outcomes that were not meta-analysed, semaglutide was also associated with broadly consistent improvements across adiposity-related measures, including body fat percentage, waist circumference and visceral fat. These reductions in weight and glycaemic outcomes are notable, considering the substantial cardiometabolic burden in people with SSDs Reference Correll, Solmi, Veronese, Bortolato, Rosson and Santonastaso3 and the limited comparative efficacy of existing adjunctive strategies. For example, weight loss from placebo-controlled metformin trials is 3 kg compared with 11 kg with semaglutide in the current review. Reference Siskind, Leung, Russell, Wysoczanski, Kisely and Holscher29 These findings are broadly consistent with treatment effects reported for obesity management with semaglutide within the general population, reinforcing the potential of this drug class as an effective pharmacological strategy for addressing antipsychotic-associated metabolic dysfunction. Reference Wilding, Batterham, Calanna, Davies, Van Gaal and Lingvay18,Reference Lincoff, Brown-Frandsen, Colhoun, Deanfield, Emerson and Esbjerg30 Notably, the 11% reduction in body weight observed in this review provides preliminary evidence that similar weight-loss effects may be achievable in people with SSDs, despite the use of a lower semaglutide doses (1.0−2.0 mg compared with 2.4 mg in general population trials) and shorter trial durations (68−104 weeks in general population studies versus 26−36 weeks across the three component RCTs). Reference Wilding, Batterham, Calanna, Davies, Van Gaal and Lingvay18,Reference Lincoff, Brown-Frandsen, Colhoun, Deanfield, Emerson and Esbjerg30 Importantly, there was also no consistent evidence of psychiatric deterioration or reductions in function, reducing concern about major pharmacokinetic interactions in people with SSDs. From a clinical perspective, these findings support semaglutide as a promising adjunctive metabolic intervention for people with SSDs, particularly where obesity and indices of metabolic syndrome threaten long-term health and antipsychotic switching is infeasible.
Several mechanistic features support the potential utility of GLP-1 RA-based therapies in people with SSDs. Importantly, their metabolic actions occur independently of the dopaminergic and serotonergic pathways targeted by antipsychotic medications, reducing the likelihood of direct pharmacological interaction, as evidenced in this review. Furthermore, preclinical studies suggest that antipsychotic exposure (particularly clozapine and olanzapine) may suppress endogenous GLP-1 signalling, with downstream effects on hepatic glucose production, glucagon secretion and appetite regulation. Reference Smith, Vickers, Cognard and Shepherd31 Collectively, these mechanisms provide a biologically plausible rationale for GLP-1 RA therapy as an adjunct treatment to counteract antipsychotic-associated metabolic dysfunction.
Regarding safety, meta-analysed adverse events indicated increased risks of gastrointestinal events, including abdominal pain, vomiting and constipation, with moderate-to-high certainty. In contrast, there was no evidence of an increased risk of serious adverse events. This adverse event profile is consistent with the tolerability profile of semaglutide as seen in large studies in the general population. Reference Wilding, Batterham, Calanna, Davies, Van Gaal and Lingvay18,Reference Lincoff, Brown-Frandsen, Colhoun, Deanfield, Emerson and Esbjerg30 The consistent findings of gastrointestinal adverse events, however, have practical implications for prescribing. In SSD populations, adverse events that affect hydration, appetite and treatment adherence may be particularly consequential, Reference Schneider-Thoma, Efthimiou, Bighelli, Dörries, Huhn and Krause32,Reference De Hert, Detraux, van Winkel, Yu and Correll33 and implementation should therefore include pragmatic safeguards: careful dose escalation, anticipatory management of constipation and nausea/vomiting, monitoring for dehydration and reduced oral intake, and proactive follow-up in the early weeks of treatment. This is of particular importance to people receiving clozapine, which has an enhanced adverse event profile compared with some other antipsychotic medications. Reference Tanzer, Pham, Warren, Barras, Kisely and Siskind34 The timing of adverse events relative to dose escalation is also an important factor to consider, and was not reported in a any of the component studies. Future research should aim to include this level of adverse event information because of its clinical relevance. Furthermore, considering the high baseline physical comorbidity in people with SSDs, Reference Trott, Plever, Anzolin, McCarthy and Siskind35 clinicians should also consider routine metabolic monitoring and a low threshold for review where symptoms suggest intolerance or emerging complications.
The results of this review should be interpreted considering some limitations. First, only three trials were available, limiting precision for many outcomes, reducing the ability to explore effect modifiers and limiting the confident interpretation of heterogeneity and prediction intervals. Second, antipsychotic exposure may influence interpretation of the findings. Clozapine and olanzapine, for example, are associated with particularly high cardiometabolic risk, Reference Burschinski, Schneider‐Thoma, Chiocchia, Schestag, Wang and Siafis5 with one included trial exclusively recruiting individuals treated with clozapine and another with clozapine and/or olanzapine. Although this increases the clinical relevance of the findings, heterogeneity in antipsychotic treatment across trials may contribute to differences in baseline metabolic risk and treatment response. Third, follow-up ranged from 26 to 36 weeks, which is only sufficient to demonstrate short-term outcomes, not to characterise longer-term durability, maintenance strategies or outcomes such as incident diabetes, cardiovascular events or mortality. Fourth, adverse event reporting varied across trials, with many adverse event types having low cell counts or inconsistently defined, thereby leaving uncertainty around less common, but clinically relevant outcomes. Fifth, the evidence base relates specifically to semaglutide at 1.0–2.0 mg, with no trials of tirzepatide being identified, representing a major gap considering tirzepatide’s comparative efficacy versus semaglutide in weight loss in non-SSD populations. Reference Aronne, Horn, le Roux, Ho, Falcon and Gomez Valderas20 Finally, although all included studies were judged to be low risk of bias, the total sample was low, and therefore results should be interpreted with caution.
Future research should prioritise larger, longer trials with harmonised outcome sets and robust safety reporting, including stratification by antipsychotic class (particularly clozapine/olanzapine), baseline metabolic status and key potential moderators of adherence. Trials should also examine implementation questions that matter clinically: optimal titration and tolerability protocols in SSDs, strategies to support adherence in the presence of gastrointestinal-related adverse events, comparative effectiveness against metformin and/or combined approaches, and whether improvements in adiposity translate into downstream cardiometabolic and functional outcomes. Considering that GLP-1 RAs markedly suppress appetite, leading to substantial reductions in overall food intake, it would be prudent to evaluate the quality of dietary intake and potential risk of micronutrient deficiencies during administration. Trials that explore co-commencement of GLP-1 RAs at time of antipsychotic initiation to ameliorate weight gain are needed. Furthermore, evidence on the efficacy and safety of tirzepatide is urgently needed in this population as no studies were found. Finally, aiming for an effective long-term management of antipsychotic-induced weight gain, studies should also explore combining pharmacological treatment with GLP-1 RAs with behavioural approaches targeting key lifestyle behaviours, including nutrition and physical activity, which may help to maximise the effects of both treatment approaches and improve cardiometabolic health in the long term. Reference Arnautovska, Milton, Trott, Soole and Siskind36
In conclusion, the current RCT evidence supports semaglutide as an effective adjunctive therapy to improve weight and glycaemic outcomes in people with SSDs, with adverse events characterised by gastrointestinal effects and no signal for serious adverse events in pooled analyses. Although these findings are clinically promising, larger trials of longer duration are required to define durability, identify who benefits most and more comprehensively evaluate long-term safety in this high-risk population.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12001
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study. All analytical code is available upon reasonable request.
Acknowledgements
The authors wish to thank Kathryn Vitangcol (K.V.) for her assistance with article screening, data extraction and risk-of-bias assessment.
Author contributions
M.T. conceptualised the paper, conducted initial searches, analysed the data and wrote the manuscript. U.A. was involved in screening and manuscript drafting, as well as editing. D.J. and G.R. assisted with manuscript writing and editing, including critical revisions. D.S. supervised the project, conceptualised the paper, and assisted in write up and critical revisions of the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
D.S. was a member of the BJPsych Editorial Board, and did not take part in the review or decision-making process of this paper. All other authors have nothing to declare.




 Open access
Open access
eLetters
No eLetters have been published for this article.