


Mental health burden in youth
Approximately 20% of the world’s children and adolescents live with various mental health conditions, with anxiety and depression being the most prevalent Reference Steel, Marnane, Iranpour, Chey, Jackson and Patel1,Reference Polanczyk, Salum, Sugaya, Caye and Rohde2 and suicide as a leading cause of death. 3 Given that almost 90% of adolescents in the world live in low- and middle-income countries (LMICs), youth mental health in these settings requires global priority. 4 This population is disproportionately exposed to social determinants, such as poverty, instability and limited access to mental health services, compounding the risk of mental illness. Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones and Patalay5 Many mental health conditions experienced by adults have early onsets, with symptoms typically manifesting during childhood and adolescence. Reference Ng, Tan, Luo, Goh, Ho and Ho6 Although the burden of mental health conditions is high among youth, help-seeking is relatively low because of various factors, including scarce mental health resources, stigma, negative beliefs toward mental health services and treatment, poor mental health literacy, and perceived need for self-sufficiency and autonomy. Reference Aguirre Velasco, Cruz, Billings, Jimenez and Rowe7 This low rate of help-seeking behaviour during adolescence is a concern, as this can lead to poor mental and physical health in adulthood. Reference Fergusson and Woodward8,Reference Costello, Mustillo, Erkanli, Keeler and Angold9
Youth peer-based mental health programmes and supports
A promising yet understudied approach to addressing the gap in supports and services for children and youth is the use of youth peer-based mental health programmes and supports (Y-PBMHPS), in which young people with shared lived experience are trained to provide structured support, information or linkage to care to other youth within community or institutional settings. To date, research on the development and implementation of Y-PBMHPS for youth has been largely restricted to high-income countries (HICs). Reference Cooper, Saunders, Greenburgh, Shah, Appleton and Machin10 In these settings, peer-delivered interventions show evidence of beneficial effects and equivalence with peer and professionally delivered interventions. Reference Fuhr, Weobong, Lazarus, Vanobberghen, Weiss and Singla11,Reference King and Fazel12 One obvious advantage of Y-PBMHPS is that they are not heavily dependent on specialist mental health services, which tend to be limited, expensive or associated with long wait times. Reference Goldner, Jones and Fang13 Y-PBMHPS, especially those based in schools with large enrolments, have access to a large number of peer supporters, resulting in accessible, lower-cost services. Reference Patton, Sawyer, Santelli, Ross, Afifi and Allen14,Reference Rose-Clarke, Bentley, Marston and Prost15 Y-PBMHPS also have the added advantage of dually benefiting the peer supporters and the individuals they support. Reference Bernecker, Williams, Caporale-Berkowitz, Wasil and Constantino16 Their potential utility is further reinforced by the central role of peer influence in shaping young people’s behaviours and help-seeking. Reference Coyle, Bramham, Dundon, Moynihan and Carr17
Conceptually, Y-PBMHPS have the potential to address persistent barriers to mental healthcare access in LMICs by leveraging peers as trusted, low-pressure liaisons who can extend support, information and linkage to care within community settings. Reference Galagali and Brooks18 If effective, such programmes could expand service coverage, reduce treatment gaps and support more equitable task-shared models of care in resource-constrained health systems. Reference Karyotaki, Araya, Kessler, Waqas, Bhana and Rahman19,Reference Belay, Engel, Lee, Le and Mihalopoulos20 Conversely, limited effectiveness or poor feasibility would have important implications for policy prioritisation and the allocation of scarce mental health resources. Their successful implementation is also likely to be shaped by contextual factors common in LMICs, including workforce capacity, training and supervision structures, cultural acceptability, stigma and long-term sustainability.
Building on these considerations, we conducted a rapid review of Y-PBMHPS implemented or developed in LMICs to inform both evidence and decision-making in resource-constrained settings. Specifically, this review sought to (a) characterise the types of Y-PBMHPS reported in LMICs and (b) examine the available evidence on their feasibility and effectiveness in improving mental health outcomes among youth in these contexts.
Method
This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Table 1) and the Joanna Briggs Institute (JBI) manual for evidence synthesis. Reference Aromataris, Lockwood, Porritt, Pilla and Jordan21 The review protocol was retrospectively registered at PROSPERO (identifier CRD42022352576) on 20 August 2022, and made public after execution of the search strategy but before starting title/abstract screening.
In this review, we defined Y-PBMHPS as any support system led, facilitated or provided by people who share common experience or characteristics with the person receiving the support. We characterised peers as those belonging to the same age group and/or those with lived experience of mental health challenges or illness. We also adopted an expanded age range of 15–30 years to characterise youth, in recognition of the cultural and jurisdictional variations surrounding the definition of youth. 22,Reference Puyat23 We acknowledge that peers may share additional specific characteristics (e.g. health status, bereavement or other lived contexts) beyond age or shared experience of mental illness, which may also shape the nature and mechanisms of support.
Criteria for eligible studies
The full inclusion/exclusion criteria are included as Supplementary Material (Supplementary Table 2). We considered for inclusion all peer-reviewed studies that investigated the effectiveness of Y-PBMHPS implemented in schools or in communities in LMICs. The interventions could include peer-based supports, programmes or services that were facilitated or led by youth with or without lived experience of mental illness or psychological distress. Additionally, the intervention could be aimed at specific subpopulations, such as young mothers and young people living with chronic conditions (e.g. HIV). The interventions must have a clearly defined group of clients other than the peer leaders, peer supporters or peer facilitators involved in service delivery. We considered all types of service modes of delivery, including those that were administered in person, through mobile devices or through computers.
To be included for full review, quantitative studies must be about investigations of the impact of an intervention on mental health as a primary or secondary outcome. These outcomes could be in the form of reduction in the incidence, prevalence and severity of mental illness (e.g. anxiety, depression, suicidal ideation), or improvement in psychosocial outcomes, mental health-related knowledge, attitudes and health-seeking behaviour. Qualitative studies were included if they explored youth’s experiences with the intervention, or youth’s perspectives about the intervention’s importance, feasibility, acceptability and accessibility.
We excluded studies that did not investigate an intervention, mental health service programme or supports (wrong study design). Studies that investigated interventions with the following characteristics were also excluded: not conducted in LMICs as classified by the World Bank; 24 not intended for youth as the target client (wrong population); exclusively focused on psychiatric medications or mental health services that required mental health professionals (wrong intervention); and no reported outcomes relevant to mental health or psychosocial outcomes (wrong outcome). Protocols for an intervention and reviews or syntheses were excluded, as well as non-peer-reviewed materials such as books or book chapters, letters to the editor, commentaries, theses and dissertations. Lastly, non-English studies were excluded because of resource constraints for translation, and we acknowledge this as a potential source of language bias.
Search strategy
Medline (Ovid), PsycINFO (EBSCO), CINAHL, CAB Global Health (CAB Direct), Science Citation Index and Social Sciences Citation Index (Web of Science) were searched for quasi-experimental studies, randomised trials and qualitative studies published in English from January 2002 to July 2022, with an updated search to include September 2025. We used search terms that included any relevant clusters of terms related to peer-facilitated interventions, such as ‘peer-led’, ‘peer-based’ and ‘peer-assisted’. Keywords for relevant outcomes included ‘mental health literacy’ as well as major mental illnesses such as ‘depression’, ‘anxiety’ and ‘substance use’ (Supplementary Material). The initial search strategy was executed by a review author (M. Mohebbian) on 29 July 2022, and updated by another review author (U.E.) on 19 September 2025.
Screening and quality assessment
Titles/abstracts were screened independently by two review authors (J.I.M., M. Mohebbian, J.A.M., E.K., M. Mago or J.H.P.). Conflicts in title/abstract screening were resolved by another review author (J.H.P., M. Mohebbian or E.K.). Full review of potentially eligible studies was also conducted by two review authors (J.A.M., M. Mohebbian, E.K., M. Mago, J.H.P., J.I.M. or M.A.B.). Conflicts during full-text review were resolved by consensus. All excluded studies during full review were reviewed by a review author (J.H.P.) and sent for full review when deemed potentially relevant. Some studies were excluded for multiple reasons, although only one reason for exclusion was reported (Fig. 1). We used the Covidence 25 platform for screening and full-text review.
Preferred Reporting Items for Systematic reviews and Meta-Analyses flowchart. LMIC, low- and middle-income country.

We used the following JBI tools to assess the quality of included studies: Checklist for Randomised Controlled Trials, Reference Barker, Stone, Sears, Klugar, Tufanaru and Leonardi-Bee26 Checklist for Quasi-Experimental Studies or Non-Randomised Experimental Studies Reference Barker, Habibi, Aromataris, Stone, Leonardi-Bee and Sears27 and Checklist for Qualitative Research. Reference Lockwood, Munn and Porritt28 One review author performed the primary quality assessment (J.A.M., M.A.B., M.M.1 or E.K.), followed by an independent review (M. Mohebbian, M.A.B., J.H.P. or M. Mago). Because JBI does not prescribe a numerical scoring system or thresholds for classifying study quality, a structured scoring approach was developed for this review to ensure transparency and consistency across designs.
Each JBI checklist item was scored as 0 = No, 1 = Unclear, 2 = Yes, and items were grouped into conceptually coherent domains that reflect key aspects of methodological rigour. For randomised controlled trials (RCTs), domains included (A) randomisation and allocation, (B) blinding, (C) outcome measurement and follow-up, and (D) analysis and reporting. For quasi-experimental studies, domains captured (A) cause and effect, (B) comparability, (C) outcome measurement and (D) statistical analysis. For qualitative studies, domains addressed (A) congruity, (B) methodology/methods, (C) representation and ethics, and (D) interpretation/conclusions.
Domain scores were summed and converted to percentages, and then multiplied by prespecified domain weights to reflect the relative importance of each methodological construct and to prevent domains with more items from dominating the overall score. Weighted domain scores were combined to produce an overall score (0–100%) that was then used to inform the overall assessment of methodological quality as high (≥75%), moderate (50–74%) or low (<50%).
Data extraction and synthesis
Data extraction was initiated on 11 January 2023, and updated on 1 November 2025 by one review author (M. Mohebbian, J.A.M., J.I.M. or E.K.) and independently verified by another review author (J.H.P., M. Mohebbian or M. Mago). For each included study, we extracted information on study design, country where the study was conducted, number and characteristics of study participants, intervention setting, nature and characteristics of the intervention, study outcome and key findings (Supplementary Tables 3 and 4). We also extracted additional contextual descriptors to indicate when studies involved peers who shared specific characteristics beyond age and lived experience of mental illness (i.e. health status, bereavement or other lived contexts), to support cautious interpretation of comparability and transferability across different Y-PBMHPS. Where available, relevant outcomes and key findings from both the quantitative and qualitative components of the study were extracted.
In addition, where reported, we extracted quantitative information required to estimate standardised effect sizes, including group means and standard deviations, and sample sizes, to enable calculation of standardised mean differences (Cohen’s d).
Study findings were grouped by intervention type, study design and mental health outcome, organised according to DSM-V characteristics. 29 No meta-analysis was performed due to the heterogeneity of interventions and populations investigated in the included studies. However, we followed guidelines from the Synthesis Without Meta-Analysis Reference Campbell, McKenzie, Sowden, Katikireddi, Brennan and Ellis30 to summarise review findings.
Results
Our search strategy yielded 6105 titles and abstracts, of which 4436 were unique and 4002 were deemed irrelevant. Of the 434 potentially relevant articles, 5 were irretrievable despite correspondence with the authors. Full-text review of the 329 articles resulted in 34 eligible studies (Fig. 1).
Of the 34 included studies, 3 were based on the same peer-facilitated psychoeducation programme, Reference Mathias, Pandey, Armstrong, Diksha and Kermode31–Reference Kermode, Grills, Singh and Mathias33 4 reported on the same peer-delivered counselling and support programmes, Reference Wogrin, Langhaug, Maruva and Willis34–Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37 and 2 reported on the same screening and brief intervention programme. Reference Jaguga, Kwobah, Giusto, Apondi, Barasa and Korir38,Reference Jaguga, Aalsma, Enane, Turissini, Kwobah and Apondi39 Because these nine studies reported on different aspects of the same intervention, we assessed them as separate studies. Of note, 23 of the included studies (over half) were published within the past 5 years (2020 onward), indicating a recent and growing evidence base in this area. Depression (n = 17) and anxiety (n = 11) were the most commonly reported outcomes (Supplementary Table 4 and Fig. 2).
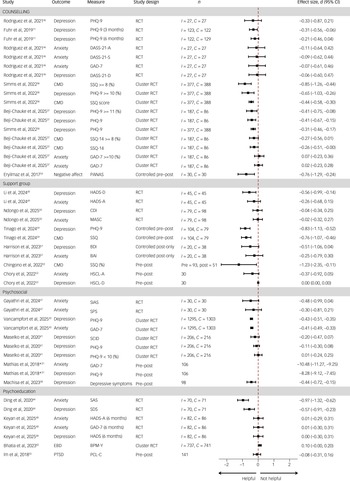
Effect sizes of selected youth peer-based mental health programmes and supports in low- and middle-income countries. *Effect size not plotted. I indicates the number of participants analysed in the intervention group; C indicates the number of participants analysed in the control group. BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BPM-Y, Brief Problem Monitor-Youth; CDI, Children’s Depression Inventory; CMD, Common Mental Disorders; DASS-21, Depression Anxiety Stress Scale, 21 items; DSS, Depresion Symptom Score; EBD, Emotional and Behavioral Difficulties; GAD-7, Generalised Anxiety Disorder, 7 items; HADS, Hospital Anxiety and Depression Scale; HSCL-A, Hopkins Symptom Checklist-Anxiety; HSCL-D, Hopkins Symptom Checklist-Depression; MASC, Multidimensional Anxiety Scale for Children; PANAS, Positive and Negative Affect Schedule; PCL-C, PTSD Check List-Civilian Version; PTSD, post-traumatic stress disorder; RCT, randomised controlled trial; SAS, Self-rating Anxiety Scale; SCID, Structured Clinical Interview for DSM Disorders; SDS, Self-Rating Depression Scale, 20 items; SIAS, Social Interaction Anxiety Scale; SPS, Social Phobia Scale; SSQ, Shona Symptom Questionnaire, 14 items.

Fifteen of the included articles were randomised studies, consisting of six cluster RCTs, Reference Simms, Weiss, Chinoda, Mutsinze, Bernays and Verhey36,Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37,Reference Balaji, Andrews, Andrew and Patel40–Reference Vancampfort, Ward, Kwiringira, Van Damme, Rosenbaum and Mugisha43 eight traditional RCTs Reference Fuhr, Weobong, Lazarus, Vanobberghen, Weiss and Singla11,Reference Ding and Yao44–Reference Ateba Ndongo, Kana, Aminou Sambo, Ketchaji, Awono Noah and Ndie50 and one study described by the authors as quasi-experimental but assessed in this review as a traditional RCT because of the presence of randomised intervention and control groups. Reference Nasution, Keliat and Wardani51 Ten studies were quasi-experimental studies Reference Mathias, Pandey, Armstrong, Diksha and Kermode31,Reference Kermode, Grills, Singh and Mathias33,Reference Chingono, Kasese, Miles and Busza52–Reference Tinago, Frongillo, Warren, Chitiyo, Jackson and Cifarelli59 and nine were qualitative studies. Reference Mathias, Singh, Butcher, Grills, Srinivasan and Kermode32,Reference Wogrin, Langhaug, Maruva and Willis34,Reference Wogrin, Willis, Mutsinze, Chinoda, Verhey and Chibanda35,Reference Jaguga, Kwobah, Giusto, Apondi, Barasa and Korir38,Reference Jaguga, Aalsma, Enane, Turissini, Kwobah and Apondi39,Reference Dhand60–Reference Garriott, Gulubane, Poku, Archibald, Entaile and Tshume63 Notably, eight of the quantitative studies also reported qualitative findings (Supplementary Table 3).
All included studies were conducted in Asia (n = 16) and Africa (n = 18). Among studies conducted in Asia, ten were from India, three were from China and one each was from Indonesia, Pakistan and Turkey. Among studies conducted in Africa, seven were from Zimbabwe, five were from Kenya, two were from South Africa and one each was from Tanzania, Botswana, Cameroon and Uganda. Interventions were predominantly delivered in community settings (n = 22), with seven conducted in schools and five in a clinic or hospital setting (Supplementary Table 3).
The included studies primarily involved adolescents and young people, with ages ranging from 10 to 30 years, and with most samples concentrated in the 15- to 24-year range. Participants were recruited from both rural and urban, school, community, university and clinic-based settings. Several studies focused on specific subpopulations, including adolescents and young people living with HIV, adolescent girls and young women, adolescent mothers and pregnant women, youth with psychological distress or diagnosed mental health conditions, and other vulnerable groups such as refugees, youth with substance use risk or chronic illness.
Most of the included studies reported group-based interventions (n = 24), peer-delivered or peer-facilitated counselling (n = 11) and psychoeducation (n = 8). Some studies combined elements such as group-based counselling Reference Wogrin, Langhaug, Maruva and Willis34–Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37,Reference Vancampfort, Ward, Kwiringira, Van Damme, Rosenbaum and Mugisha43,Reference Dow, Mmbaga, Turner, Gallis, Tabb and Cunningham45,Reference Gayathri, Parthiban, Natarajan and Selvamani47 or group-based self-help groups. Reference Chingono, Kasese, Miles and Busza52,Reference Chory, Callen, Nyandiko, Njoroge, Ashimosi and Aluoch53 Cognitive-based therapy (n = 9) and mindfulness-based training (n = 3) were among the approaches incorporated in peer-facilitated counselling interventions (Supplementary Table 3).
Youth peers performed roles as leaders (n = 6), facilitators (n = 10) or educators (n = 5) in many of the included studies. In 13 studies, youth peers were trained to deliver counselling or structured psychotherapy, facilitate group-based interventions, provide psychoeducation, support screening and brief interventions and offer community-based adherence or wellness support. In a few studies, peers also served as sources of informal support Reference Chory, Callen, Nyandiko, Njoroge, Ashimosi and Aluoch53 or assisted with participant recruitment (Supplementary Table 3). Reference Chingono, Kasese, Miles and Busza52 Across studies, peers were recruited using predetermined criteria that extended beyond age proximity and lived experience of mental health challenges, to include embeddedness, communication skills, leadership qualities and interest in supporting youth well-being. Additional characteristics included being students, community youth leaders or near-peer lay counsellors, as well as adolescents and young adults living with HIV, individuals with other chronic conditions, or former or active substance users.
Quality appraisal
RCTs
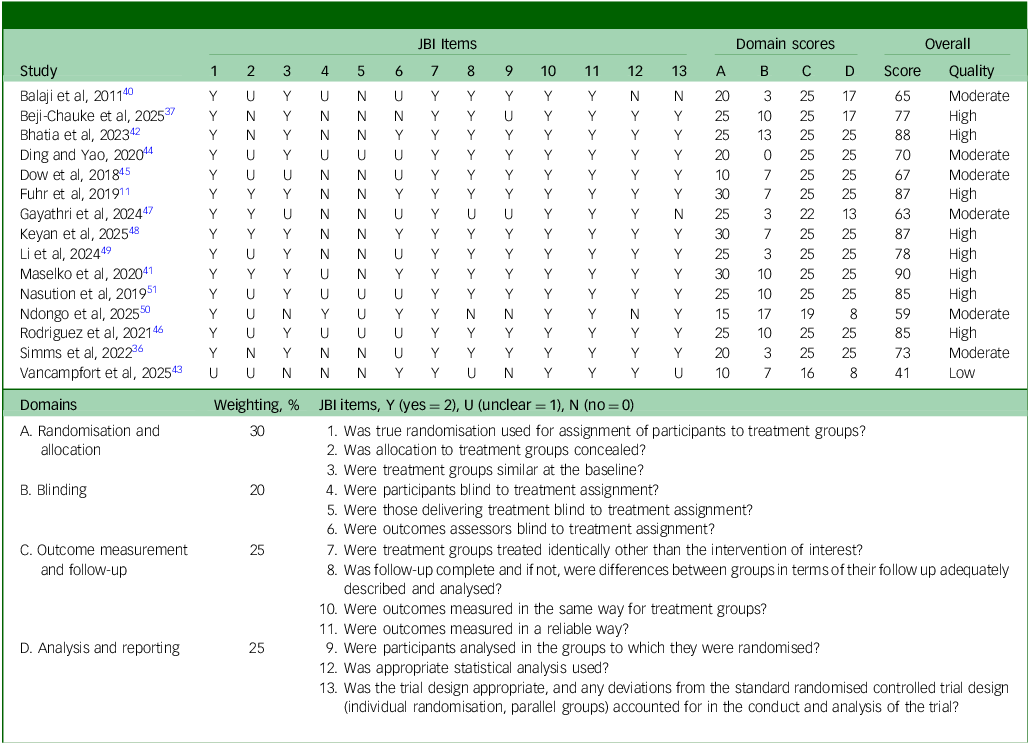
Overall, the methodological quality of the RCTs was mixed (Table 1). Domain-level appraisal showed that randomisation and allocation procedures were variable, with 9 out of 15 trials achieving scores at or above 25 out of 30. Blinding of participants and outcome assessors was consistently weak across all trials. In contrast, outcome measurement and follow-up were generally strong, with 12 out of 15 trials receiving scores of 25 out of 25. Analytical rigour and reporting quality were also relatively robust, with 10 out of 15 trials scoring at or about 25 out of 30. Based on the overall ratings, eight RCTs were classified as high quality and the rest as moderate (n = 6) and low quality (n = 1).
Critical appraisal of included randomised controlled trials (RCTs)

The methodological quality of each randomised controlled trial was assessed using the JBI Critical Appraisal Checklist for RCTs. Individual item scores (0 = N, 1 = U, 2 = Y) were grouped into four domains: randomisation and allocation, blinding, outcome measurement and follow-up, and analysis and reporting. For each domain, item scores were summed and converted to a percentage of the maximum possible domain score. Domain percentages were then multiplied by prespecified domain weights to generate weighted domain scores. The overall methodological quality score represents the sum of all weighted domain scores, expressed as a percentage. Studies were classified as high quality (≥75%), moderate quality (50–74%) or low quality (<50%). Consistent with JBI guidance, these scores reflect methodological quality rather than risk of bias. JBI, Joanna Briggs Institute; N, no; U, unclear; Y, yes.
Quasi-experimental studies
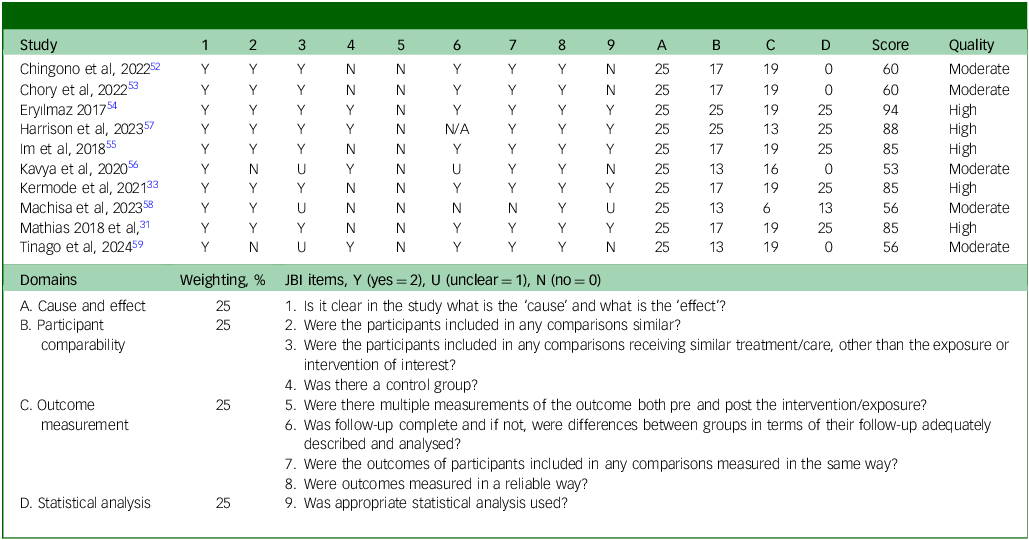
Overall, the methodological quality of the quasi-experimental studies was mixed (Table 2). Domain-level appraisal indicated uniformly strong performance in the cause-and-effect domain, with all ten studies achieving full scores (25/25). In contrast, participant comparability across study groups was limited, with only two out of ten studies receiving full scores in this domain. Outcome measurement was also a common area of weakness, as all studies scored below 20 out of 25. Statistical analysis showed mixed rigour, with only five out of ten studies achieving full scores. Overall, five studies were classified as high quality and five as moderate quality.
Critical appraisal of included quasi-experimental or non-randomised studies of intervention

The methodological quality of each non-randomised study of intervention was assessed using the JBI Critical Appraisal Checklist for non-randomised studies of intervention. Individual item scores (0 = N, 1 = U, 2 = Y) were grouped into four domains: cause and effect, participant comparability, outcome measurement and statistical analysis. For each domain, item scores were summed and converted to a percentage of the maximum possible domain score. Domain percentages were then multiplied by prespecified domain weights to generate weighted domain scores. The overall methodological quality score represents the sum of all weighted domain scores, expressed as a percentage. Studies were classified as high quality (≥75%), moderate quality (50–74%) or low quality (<50%). Consistent with JBI guidance, these scores reflect methodological quality rather than risk of bias. JBI, Joanna Briggs Institute; N, no; U, unclear; Y, yes.
Qualitative studies
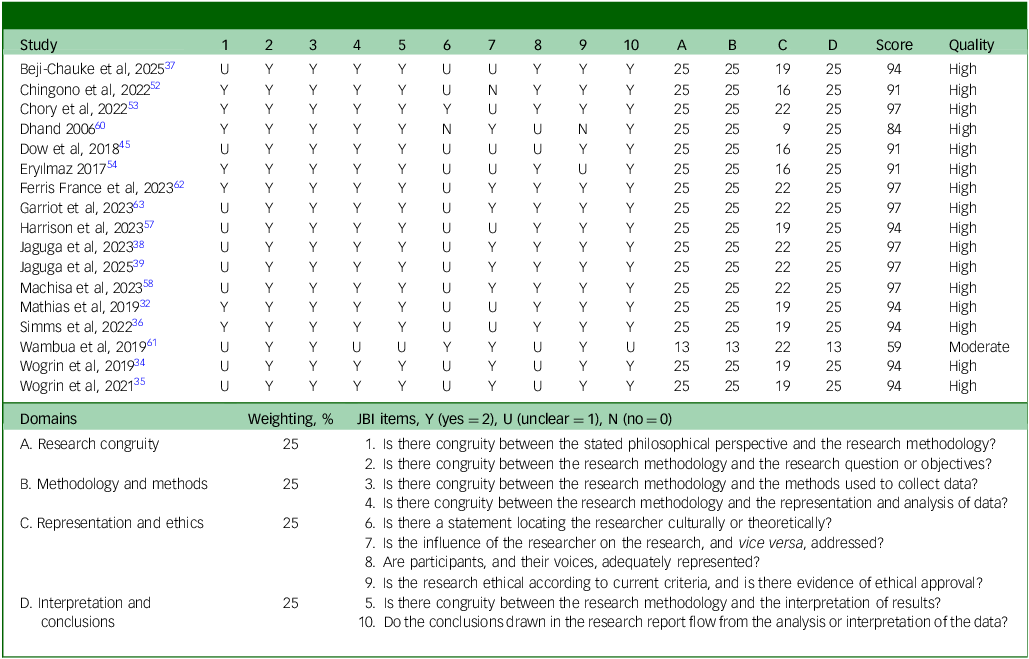
Overall, the methodological quality of the nine qualitative studies and eight quantitative studies with qualitative components was high (Table 3). Domain-level appraisal demonstrated strong congruity between the research questions, methodology and methods, with 16 out of 17 studies receiving full scores (25/25) in both the research congruity and methodology and methods domains. Interpretation and conclusions were likewise robust, with 16 out of 17 studies achieving full scores. In contrast, representation and ethical considerations were less consistently addressed, as only 7 out of 17 studies received full scores in this domain. Based on the proportion of JBI criteria met across domains, all but one study was classified as high quality (16 out of 17).
Critical appraisal of qualitative studies and findings

The methodological quality of each qualitative study was assessed using the JBI Critical Appraisal Checklist for Qualitative Research. Individual item scores (0 = N, 1 = U, 2 = Y) were grouped into four domains: research congruity, methodology and methods, representation and ethics, and interpretation and conclusions. For each domain, item scores were summed and converted to a percentage of the maximum possible domain score. Domain percentages were then multiplied by prespecified domain weights to generate weighted domain scores. The overall methodological quality score represents the sum of all weighted domain scores, expressed as a percentage. Studies were classified as high quality (≥75%), moderate quality (50–74%) or low quality (<50%). Consistent with JBI guidance, these scores reflect methodological quality rather than risk of bias. JBI, Joanna Briggs Institute; N, no; U, unclear; Y, yes.
Intervention effects from quantitative studies
Counselling
Five studies evaluated peer-based counselling interventions, including two individual RCTs, two cluster RCTs and one controlled pre–post study. Across outcomes, depression and anxiety were most commonly assessed. The two high-quality RCTs reported consistently beneficial effects in the small to moderate range, although only one outcome, depression at 3 months, reached statistical significance. Reference Fuhr, Weobong, Lazarus, Vanobberghen, Weiss and Singla11 One cluster RCT, appraised as moderate quality, demonstrated moderate to large beneficial effects, Reference Simms, Weiss, Chinoda, Mutsinze, Bernays and Verhey36 whereas the other high-quality cluster RCT reported negligible to moderate effects. Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37 Overall, peer-based counselling interventions showed a consistent pattern of beneficial effects for depression and common mental disorder outcomes, with less consistent evidence for improvements in anxiety.
Peer support groups
Six studies examined peer-support groups, including two RCTs, two controlled pre–post studies and two uncontrolled pre–post designs. Findings from the RCTs generally trended toward beneficial effects, although only one trial reported a statistically significant, moderate-sized effect. Reference Li, Duan, Cao, Zhou, Kang and Wan49 Non-randomised studies similarly suggested beneficial trends, often with larger observed effects than those reported in RCTs, with the largest effects emerging from moderate-quality controlled Reference Tinago, Frongillo, Warren, Chitiyo, Jackson and Cifarelli59 and uncontrolled pre–post studies. Reference Chingono, Kasese, Miles and Busza52 No clear pattern of differential effectiveness by outcome type was observed, with effects varying across symptom domains.
Psychosocial interventions
Five studies assessed peer-led psychosocial interventions, comprising one RCT, two cluster RCTs and two uncontrolled pre–post studies. The RCT reported moderate beneficial effects that did not reach statistical significance, likely reflecting limited statistical power. Reference Gayathri, Parthiban, Natarajan and Selvamani47 Cluster RCTs showed effects trending toward benefit, ranging from negligible to moderate; negligible effects were observed in a high-quality trial, Reference Maselko, Sikander, Turner, Bates, Ahmad and Atif41 whereas moderate effects were reported in a large-sample cluster RCT Reference Vancampfort, Ward, Kwiringira, Van Damme, Rosenbaum and Mugisha43 appraised as lower quality. Overall, psychosocial interventions demonstrated a general pattern of beneficial effects for both anxiety and depression, although estimates varied by study design and methodological quality.
Psychoeducation
Four studies evaluated peer-led psychoeducation interventions, including two RCTs, one cluster RCT and one pre–post study. Beneficial effects for anxiety and depression were reported in one moderate-quality RCT, Reference Ding and Yao44 whereas the remaining studies found no notable effects. Evidence for the effectiveness of psychoeducation interventions seemed limited and less consistent than for other intervention types.
Acceptability and feasibility of the intervention based on qualitative findings
Not all of the included studies addressed feasibility or acceptability, and those that did reported mixed findings (Supplementary Table 4). Some reported positive aspects like good treatment fidelity and adherence, Reference Fuhr, Weobong, Lazarus, Vanobberghen, Weiss and Singla11,Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37,Reference Dow, Mmbaga, Turner, Gallis, Tabb and Cunningham45,Reference Rodriguez, Eisenlohr-Moul, Weisman and Rosenthal46 and good acceptability of intervention formats that fostered safety and anonymity (e.g. WhatsApp). Reference Chory, Callen, Nyandiko, Njoroge, Ashimosi and Aluoch53 Participants described peer-led sessions as enjoyable because peers were perceived as easier to talk to, more relatable, and more understanding than professional healthcare workers. Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37,Reference Jaguga, Kwobah, Giusto, Apondi, Barasa and Korir38,Reference Harrison, Mtukushe, Kuo, Wilson-Barthes, Davidson and Sher57,Reference Garriott, Gulubane, Poku, Archibald, Entaile and Tshume63 Participants also reported that the sessions were helpful in addressing and resolving challenges such as substance use and involvement in harmful relationships. Reference Jaguga, Kwobah, Giusto, Apondi, Barasa and Korir38,Reference Jaguga, Aalsma, Enane, Turissini, Kwobah and Apondi39,Reference Machisa, Mahlangu, Chirwa, Nunze, Sikweyiya and Dartnall58 Others highlighted challenges that could affect feasibility and acceptability. These challenges included stigma associated with using mental health services, Reference Mathias, Singh, Butcher, Grills, Srinivasan and Kermode32,Reference Garriott, Gulubane, Poku, Archibald, Entaile and Tshume63 limited access to devices, technology or the intervention itself, and insufficient programme resources to support participants. Reference Kermode, Grills, Singh and Mathias33 Complex family dynamics, such as parents withholding permission or making it conditional on completion of chores, further complicated participation. Reference Mathias, Singh, Butcher, Grills, Srinivasan and Kermode32,Reference Kermode, Grills, Singh and Mathias33,Reference Simms, Weiss, Chinoda, Mutsinze, Bernays and Verhey36,Reference Jaguga, Aalsma, Enane, Turissini, Kwobah and Apondi39 Lastly, competing demands on time, Reference Kermode, Grills, Singh and Mathias33,Reference Jaguga, Aalsma, Enane, Turissini, Kwobah and Apondi39,Reference Wambua, Musindo, Machuka and Kumar61 diverse educational backgrounds of participants Reference Wambua, Musindo, Machuka and Kumar61 and difficulty maintaining participant motivation over time Reference Maselko, Sikander, Turner, Bates, Ahmad and Atif41,Reference Wambua, Musindo, Machuka and Kumar61,Reference Garriott, Gulubane, Poku, Archibald, Entaile and Tshume63 were reported to have impacted acceptability and feasibility. These findings underscore the need to consider the specific context and challenges faced by the target youth population in the design and implementation of Y-PBMHPS.
Factors that contribute to the success of Y-PBMHPS based on qualitative findings
A few studies in this review highlighted factors that contributed to the success of Y-PBMHPS. One key factor was the shared experiences among youth peers that fostered vulnerability and open communication, Reference Wogrin, Langhaug, Maruva and Willis34,Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37 and that helped create a safe and supportive space for participants. Reference Mathias, Singh, Butcher, Grills, Srinivasan and Kermode32,Reference Harrison, Mtukushe, Kuo, Wilson-Barthes, Davidson and Sher57 Another factor was the positive connections and supportive community nurtured by these programmes, which helped reduce feelings of isolation and served as a resource for coping and building resilience. Reference Dow, Mmbaga, Turner, Gallis, Tabb and Cunningham45,Reference Harrison, Mtukushe, Kuo, Wilson-Barthes, Davidson and Sher57,Reference Wambua, Musindo, Machuka and Kumar61 A third factor was the use of fun, easy and practical activities that equipped participants with knowledge and skills that boost self-agency, increased self-awareness, enhanced communication skills and induced a sense of accomplishment from helping others. Reference Beji-Chauke, Simms, Abas, Muzariri, Mavhu and Mangenah37,Reference Jaguga, Kwobah, Giusto, Apondi, Barasa and Korir38,Reference Eryılmaz54,Reference Machisa, Mahlangu, Chirwa, Nunze, Sikweyiya and Dartnall58,Reference Ferris France, Byrne, Nyamwanza, Munatsi, Willis and Conroy62 Lastly, the programmes provided role-modelling opportunities where peers who demonstrated independence and competence become inspiration for others to learn and do the same. Reference Mathias, Singh, Butcher, Grills, Srinivasan and Kermode32
Discussion
In this study, we reviewed the existing literature on peer-led or peer-facilitated programmes for youth mental health in LMICs. Our examination of both quantitative and qualitative data from the included studies indicates that Y-PBMHPS in educational and community settings can be feasible, acceptable and effective. The included studies are heterogeneous with respect to the nature of programmes and supports investigated, the roles assumed by youth peers, study settings and methodological quality. Nevertheless, a consistent finding across included studies was the reporting of marked reductions in psychological symptoms, notably depression and anxiety. Overall, the existing evidence underscores the potential of Y-PBMHPS as a promising avenue for broadening the scope of mental health support for youth in resource-constrained environments.
To date, and to our knowledge, only two review studies have focused on Y-PBMHPS with a scope similar to ours. The first, published in 2021, Reference King and Fazel12 synthesised school-based mental health interventions for individuals between 4 and 18 years, based on studies available up to 12 May 2020. It identified a diverse array of study designs and peer roles; and, of the 54 included studies, only 11 assessed intervention efficacy, and just six were conducted in LMICs. The second, a scoping review published in 2025, examined peer-led mental health interventions in LMICs published as of September 2024. Reference Chow, Matungwa, Blackwood, Pronyk and Dow64 It emphasised the role of training, supervision and cultural competence in shaping programme implementation, but did not systematically assess the range of reported outcomes or intervention types. Although our review shares some thematic overlap with these prior syntheses, it makes a distinct and complementary contribution by systematically mapping the breadth of reported intervention effects and identifying key gaps in both the types of interventions evaluated and the methodological rigour of existing studies. This nuanced focus enhances the current evidence base and offers targeted directions for future research and practice in LMIC contexts.
The studies included in this review suggest that a variety of Y-PBMHPS are generally feasible and show trends toward beneficial effects, although the magnitude and consistency of impact vary by intervention type and study quality. Peer-based counselling demonstrated the most consistent benefits, particularly for depression and common mental disorder outcomes, whereas effects for anxiety were less consistent. Psychosocial and support group interventions also tended to show beneficial trends, although estimates varied widely across designs and were often smaller in high-quality randomised trials compared with non-randomised studies. In contrast, evidence for peer-led psychoeducation was limited and largely inconsistent, with beneficial effects observed in one moderate-quality trial. Overall, the pattern of smaller and frequently non-significant effects in high-quality RCTs, relative to larger effects reported in lower-quality or pre–post designs, underscores the need for more rigorous, adequately powered trials to draw definitive conclusions about effectiveness.
A feature of the Y-PBMHPS that this review underscores is the importance of adequate training and supervision for peers, as these will help achieve the interventions’ purported benefits and ensure the safety of peer facilitators and service recipients. Most of the studies included in this review described a form of training lasting from 8 h Reference Rodriguez, Eisenlohr-Moul, Weisman and Rosenthal46 to 40 h Reference Fuhr, Weobong, Lazarus, Vanobberghen, Weiss and Singla11 that peers must undergo before they are deployed to deliver the intervention (Table 1). In one of the included studies, Reference Mathias, Singh, Butcher, Grills, Srinivasan and Kermode32 monthly refresher training was provided to peers over a 5-month intervention period, along with ongoing supervision from the project staff. Some Y-PBMHPS, such as peer support groups described in two studies, Reference Chory, Callen, Nyandiko, Njoroge, Ashimosi and Aluoch53,Reference Wambua, Musindo, Machuka and Kumar61 also involved the presence of mental health professionals, likely indicative of the need to protect the safe spaces provided by peer support groups from participants who could inadvertently threaten them. As others have noted, developing guidelines for selecting, training and supervising youth peers Reference King and Fazel12 would be critical to the effective and safe delivery of Y-PBMHPS.
There is a notable scarcity of published studies from other LMICs, particularly in South American countries. It is likely that some form of evaluation and assessment are happening to monitor and assess Y-PBMHPS in these countries, and that programme proponents may either not submit their evaluations for peer review or publish them in languages other than English. This lack of accessible, peer-reviewed literature from other LMICs is an important gap that future studies should address to help build the evidence base for Y-PBMHPS in low-resource settings. Expanding the evidence base will also support the delivery of effective programmes with high implementation fidelity.
We note some limitations of this review. First, it was not possible for this rapid review to search for non-English publications, and this may have affected the diversity of the evidence included and assessed, such as those coming from South America. Additionally, the methodology excluded reports and documents that were not peer reviewed, omitting potentially valuable insights from the grey literature. Furthermore, the review criteria did not cover interventions or programmes that are active but remain unevaluated or those with evaluations that are ongoing and have yet to be published. This review, therefore, may have overlooked a segment of evidence, including those that are just emerging, that could offer important insights into the scope and impact of peer-led mental health initiatives. Incorporating environmental scans and informal searches of organisational reports and documents to capture a broader spectrum of evidence could help mitigate this limitation in the future.
In conclusion, the body of evidence synthesised in this review suggests that Y-PBMHPS represent a promising avenue for broadening the scope of mental health support in resource-constrained environments. To harness their full potential and ensure safety, it is imperative to establish comprehensive guidelines for selecting, training, supporting and supervising peer facilitators. The unique context and challenges of the target youth population must also be considered in their design and implementation. Further research in other LMICs and conducting health economic and cost-effectiveness studies could help broaden the evidence base and enhance the robustness of these programmes.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.11030
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Acknowledgements
We thank the Philippine Mental Health Association, Youth for Mental Health Coalition and Psychological Association of the Philippines for their support and help in obtaining funding from the Canadian Institutes of Health Research.
Author contributions
J.H.P. contributed to study conceptualisation, methodology, investigation, data curation, visualisation, supervision and funding acquisition, and wrote the original draft of the manuscript. M. Mohebbian contributed to study conceptualisation, methodology, investigation, data curation, visualisation and project administration, and wrote the original draft of the manuscript. E.K. contributed to study investigation, data curation, visualisation and project administration, and wrote the original draft of the manuscript. J.A.M. contributed to study conceptualisation, investigation and funding acquisition, and reviewed and edited the manuscript. M. Mago and J.I.J.M. contributed to data curation, and reviewed and edited the manuscript. M.A.B. contributed to study investigation and data curation, and reviewed and edited the manuscript. U.E. contributed to the methodology and data curation, and reviewed and edited the manuscript. L.I.B.D.C. and C.U.-R. contributed to study conceptualisation and funding acquisition, and reviewed and edited the manuscript. M.T.-C., C.T.H., R.W.L. and R.K. contributed to study conceptualisation, methodology and funding acquisition, and reviewed and edited the manuscript.
Funding
This study was supported by the Canadian Institutes of Health Research (CIHR), Institute of Population and Public Health (IPPH) (funding reference number 183483). J.H.P. is supported by the Michael Smith Health Research British Columbia Scholar Awards (grant number 18299).
Declaration of interest
The authors J.H.P., M. Mohebbian, E.K., J.A.M., M. Mago, M.A.B., J.I.J.M, U.E., L.I.B.D.C., C.U.-R., M.T.-C., C.T.H. and R.K. declare that they have no conflicts of interest related to this work. R.W.L. has received honoraria for ad hoc speaking or advising/consulting, or received research funds, from Abbvie, Asia-Pacific Economic Cooperation, Bausch, BC Leading Edge Foundation, Brain Canada, Canadian Institutes of Health Research, Canadian Network for Mood and Anxiety Treatments, Carnot, CB Solutions, Genome BC, Grand Challenges Canada, Healthy Minds Canada, Janssen, Lundbeck, Michael Smith Foundation for Health Research, MITACS, Neurotorium, Ontario Brain Institute, Otsuka, Shanghai Mental Health Center, Unity Health, Vancouver Coastal Health Research Institute and VGH & UBC Hospital Foundation.




 Open access
Open access
eLetters
No eLetters have been published for this article.