


Statement of Research Significance
Research Question(s) or Topic(s):
How does Wechsler Intelligence Scale performance differ between individuals with body dysmorphic disorder and healthy adults, and what does this reveal about their cognitive functioning?
Main Findings:
Individuals with body dysmorphic disorder showed significantly reduced performance on tasks requiring processing speed, yet intact performance on reasoning, problem-solving, and verbal comprehension. Processing speed difficulties were unrelated to anxiety or symptom severity, suggesting that they may represent a stable cognitive feature rather than an effect of emotional distress.
Study Contributions:
This study provides the first clinical evaluation of cognition in body dysmorphic disorder using a comprehensive, internationally utilized cognitive assessment. It identifies a selective cognitive pattern marked by slowed processing speed alongside intact reasoning and verbal abilities. These findings have important implications for assessment and psychological treatment, highlighting the value of adapting interventions to accommodate reduced processing efficiency.
A cognitive profile of body dysmorphic disorder: an investigation using the WAIS-IV
Body dysmorphic disorder (BDD) is a severe psychiatric condition characterized by preoccupation with perceived flaws or defects in physical appearance which are typically unnoticeable to others (American Psychiatric Association, 2013). While under-recognized and underdiagnosed (Rossell et al., Reference Rossell, Castle, Pikoos and Malcolm2023), it is assumed to affect approximately 2–3% of the general population (Schieber et al., Reference Schieber, Kollei, de Zwaan and Martin2015) and involves significant psychological distress, social isolation, and impaired functioning across numerous life domains (Phillips et al., Reference Phillips, Quinn and Stout2008). BDD is classified as an obsessive–compulsive and related disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and is complex, with a variety of factors contributing to its onset and maintenance. Core to the cognitive-behavioral model of BDD is the notion that maladaptive cognitive processes – such as visual misperception and heightened attention to detail – underlie its etiology and maintenance (Fang & Wilhelm, Reference Fang, Wilhelm, Cannon and Widiger2015; Veale, Reference Veale2004).
Previous research examining cognition in BDD compared to controls has shown inconsistent results. Three studies utilizing cognitive batteries found both specific and global differences in BDD (Hanes, Reference Hanes1998; Malcolm et al., Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021; Toh et al., Reference Toh, Castle and Rossell2015). Hanes (Reference Hanes1998) used a battery of cognitive tasks including the New Tower of London Task (Hanes, Reference Hanes1996), the Purdue Pegboard, the Rey Auditory Verbal Learning Task, and the Rey Complex Figure Test to demonstrate impairments in executive function; however, no significant differences were shown in motor function, memory, perceptual organization, and verbal learning. Toh et al.’s (Reference Toh, Castle and Rossell2015) investigation using the Repeatable Battery for the Assessment of Neuropsychological Status reported a global cognitive deficit in BDD, demonstrating a very large effect size (Cohen’s d = 1.36), a finding driven by deficits in the Immediate Memory and Attention indices. The most extensive empirical study on neurocognition in BDD to date (N = 65) identified deficits across a range of domains using the MATRICS Cognitive Consensus Battery (MCCB), including in inhibition/flexibility, processing speed, working memory, visual and verbal learning, and reasoning/problem-solving, although no significant differences were shown for attention/vigilance or social cognition (Malcolm et al., Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021). A recent systematic review of 54 studies demonstrated significant differences across all levels of the cognitive hierarchy, with difficulties increasing in line with greater cognitive complexity (Holmes à Court et al., Reference Holmes à Court, Malcolm, Toh and Rossell2025a). Specific domains demonstrating more consistent results were visuospatial processing, attention, memory, and executive function, and across domains, atypical visual perception, especially a tendency to favor local over global processing, emerged as a likely cognitive marker of BDD. Inconsistencies across the study results were proposed to relate to wide methodological variation – such as differences in task stimuli and presentation – as well as pointing to potential cognitive heterogeneity in the disorder (Malcolm et al., Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021). Qualitatively, individuals with BDD self-report substantial cognitive impairment (Holmes à Court et al., Reference Holmes à Court, Van Rheenan and Rossell2025b).
A comprehensive examination of cognition, using a tool widely employed and understood by clinicians, is critical for advancing both theoretical models and clinical approaches to BDD. Such a tool, the Wechsler Adult Intelligence Scale, Fourth Edition (WAIS-IV; Wechsler, Reference Wechsler2008a) is regarded as the gold standard for measuring adult intelligence globally. The WAIS-IV provides both a global intelligence quotient and a comprehensive evaluation of multiple cognitive domains via four main index scores: verbal comprehension (VCI), perceptual reasoning (PRI), working memory (WMI), and processing speed (PSI). These indices allow for a nuanced understanding of an individual’s cognitive profile, identifying both strengths and weaknesses across domains (Wechsler, Reference Wechsler2008b). For example, the VCI evaluates abilities such as verbal reasoning, concept formation, and knowledge acquisition, while the PRI assesses nonverbal reasoning and problem-solving. The WMI and PSI indices measure the ability to retain and manipulate information and the efficiency of cognitive processing, respectively. The WAIS-IV has been extensively validated in clinical samples, including individuals with mood and anxiety disorders and neurodevelopmental conditions, highlighting applications toward improving the understanding of cognitive profiles of those with psychiatric disorders (e.g., Terry & Lecci, Reference Terry and Lecci2022).
The current study explored cognitive functioning using the WAIS-IV in adults with BDD compared to healthy controls, with a particular focus on identifying patterns of cognitive strengths and deficits across the four indices. Ultimately, this study aims to contribute to a growing body of literature that seeks to improve assessment, treatment, and outcomes for individuals with BDD, guided by a deeper understanding of the cognitive processes that shape their experiences. With these aims in mind, the primary hypothesis was that individuals with BDD would demonstrate significantly reduced performance compared to controls in indices measuring the cognitive skills of visuospatial processing, attention, working memory, and processing speed (i.e., the PRI, WMI, and PSI indices) in alignment with existing studies (Holmes à Court et al., Reference Holmes à Court, Malcolm, Toh and Rossell2025a). Verbal comprehension has not previously been examined in the literature to date, so no predictions were put forward for this index. We additionally explored associations between anxiety and depression, symptoms of BDD, insight, and cognitive performance.
Materials and Methods
Participants and procedure
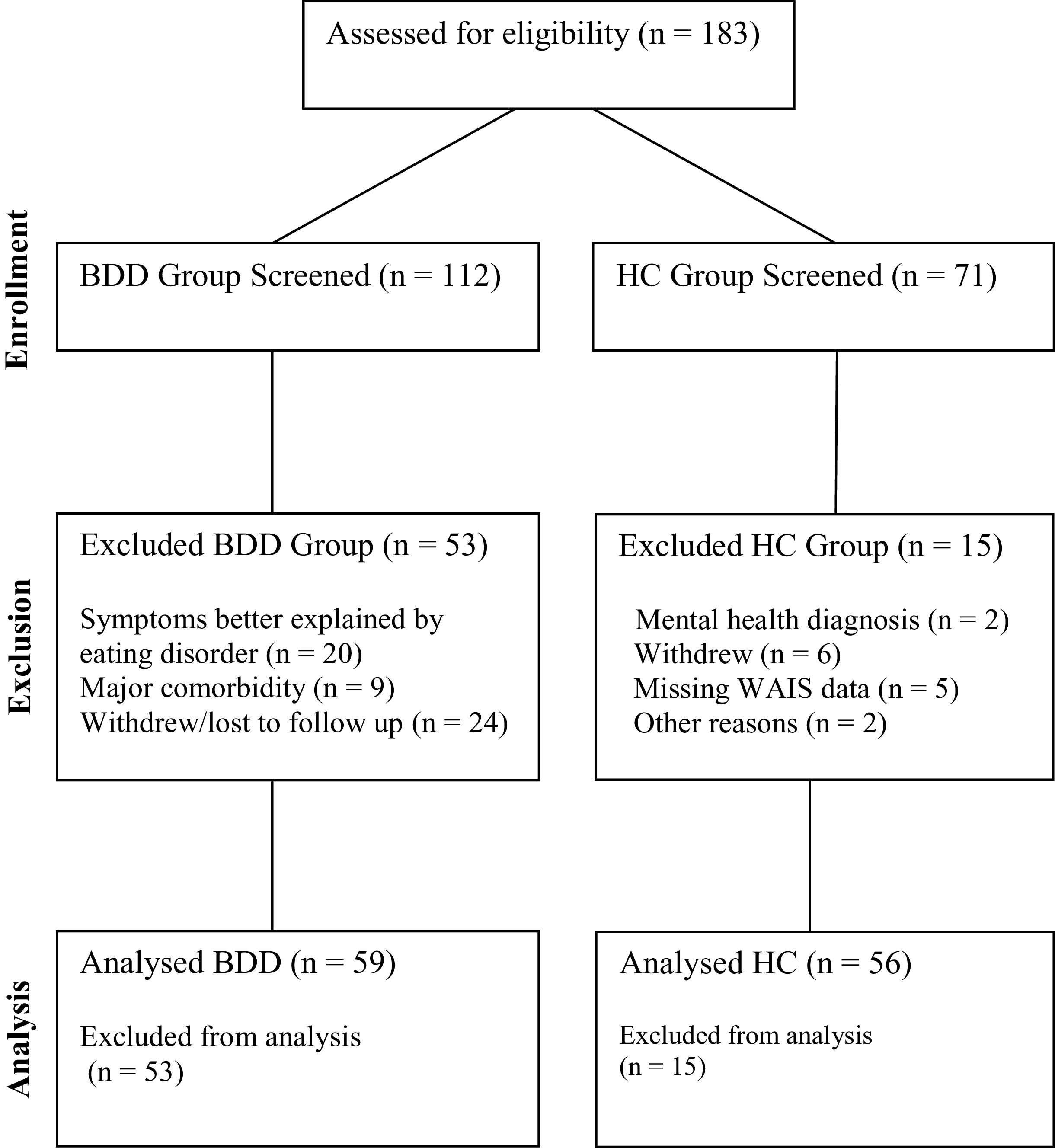
The sample comprised 59 individuals with BDD and 56 healthy controls. The study was conducted at Swinburne University of Technology, Melbourne, Australia, with state-wide recruitment. Participants were recruited as part of a larger clinical trial through treating psychologists and psychiatrists, and broad advertising in the community and on social media. Primary BDD diagnoses were confirmed using the BDD Diagnostic Module for DSM criteria from the Structured Clinical Interview for DSM-5 (BDD-DM; First et al., Reference First, Williams, Karg and Spitzer2015), and additional psychiatric diagnoses were screened using the Mini-International Neuropsychiatric Interview (MINI-7; Sheehan et al., Reference Sheehan, Lecrubier, Sheehan, Amorim, Janavs, Weiller and Dunbar1998). BDD participants’ symptom severity was measured using the Yale-Brown Obsessive-Compulsive Scale Modified for BDD (BDD-YBOCS; Phillips et al., Reference Phillips, Hollander, Rasmussen and Aronowitz1997). Participants taking psychotropic medication were required to have been on a stable dose for at least 8 weeks prior to testing and were excluded from the study if they met criteria for a current eating disorder (within the past 3 months) as measured by the MINI-7. Control participants were excluded if they reported a significant mental illness history (prior diagnosis of depression, eating disorders, bipolar disorder or schizophrenia) or screened positive to any neurodevelopmental disorders or current psychiatric diagnoses via the MINI-7. Individuals with low levels of anxiety and depression were permitted to participate. All participants were between 18–65 years of age, fluent in English, had a minimum premorbid IQ of 70 as scored using the Test of Premorbid Functioning (ToPF; Shura et al., Reference Shura, Ord, Martindale, Miskey and Taber2022) and no uncorrected hearing or visual impairments or significant neurological disorders (e.g., Parkinson’s disease). In accordance with the Helsinki Declaration, participants provided written informed consent, and the Swinburne University Human Research Ethics Committee approved all procedures (SUHREC-5412). Testing occurred between April 2022 and January 2025 with participants recruited as part of the larger clinical trial. This trial included phone screening of inclusion criteria plus a single in-person session conducted by a trained researcher during which time the diagnostic and cognitive assessments were performed. Participant flow through screening and inclusion is summarized in Figure 1.
Participant flow diagram. Note. BDD-YBOCS = Yale-Brown Obsessive-Compulsive Scale Modified for Body Dysmorphic Disorder; MINI-7 = Mini-International Neuropsychiatric Interview, 7th edition.

Measures
Demographic questions relating to age, sex, ethnicity, and education were included in the survey to characterize participants.
Clinical measures
In addition to the BDD-YBOCS, assessment of BDD illness insight occurred through the Brown Assessment of Beliefs Scale (BABS; Eisen et al.,Reference Eisen, Phillips, Baer, Beer, Atala and Rasmussen1998). The short-form DASS-21 was used to assess past week depression, anxiety, and stress symptoms (DASS-21; Lovibond & Lovibond, Reference Lovibond and Lovibond1995).
Cognitive measure
Cognitive function was assessed using the WAIS-IV Australian and New Zealand Language Adapted Edition (WAIS-IV A&NZ; Wechsler, Reference Wechsler2008c), a widely used standardized battery of cognitive ability. The A&NZ edition adapts item content for Australian and New Zealand English while retaining US normative data. The structure of the WAIS-IV battery is summarized in Figure 2. A measure of general cognitive ability is provided through the Full Scale Intelligence Quotient (FSIQ), which is derived from the combination of 10 core subtest scores across four indices. Each index score is derived from combined subtest scores pertaining to that index (see Figure 2). Seven process scores reflect additional aspects of test performance such as response consistency or learning across trials associated with the WMI. Subtest scores are scaled against age-based normative data (M = 10, SD = 3), while index and IQ scores are standardized (M = 100, SD = 15; Wechsler, Reference Wechsler2008c). Internal consistency (Cronbach’s α) was calculated for the WAIS-IV composite scores in the current sample (N = 115). Reliability was good for FSIQ (α = 0.83) and PSI (α = 0.85), acceptable for VCI (α = 0.78) and PRI (α = 0.74). WMI showed lower internal consistency (α = 0.51, 95% CI [0.29, 0.66]), reflecting the modest correlation between DS and AR (r = 0.34).
WAIS-IV component subtests and indices. Note. Adapted from: Wechsler Adult Intelligence Scale – Fourth Edition (WAIS-IV; Wechsler, Reference Wechsler2008a).

Data analysis
All statistical analyses were conducted in R (version 4.2.2; R Core Team, 2024) using the tidyverse (Wickham et al., Reference Wickham, Averick, Bryan, Chang, McGowan, François, Grolemund, Hayes, Henry, Hester, Kuhn, Pedersen, Miller, Bache, Müller, Ooms, Robinson, Seidel, Spinu and Yutani2019) for data management, rstatix (Kassambara, Reference Kassambara2023), and effectsize (Ben-Shachar et al., Reference Ben-Shachar, Lüdecke and Makowski2020) for statistical testing. All tests were two-tailed, with type I error, p < 0.05. Among included participants, cognitive data were complete. Some clinical data were missing (DASS-21: n = 17; BABS: n = 6) and were handled using pairwise deletion for correlation analyses. A priori power analysis was based on effect sizes from Malcolm et al. (Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021) for working memory (d = 1.16), speed of processing (d = 0.85), and reasoning (d = 0.80). Using the lowest of these, d = 0.80, α = 0.05, and power of 95% a total sample of N = 102, n = 51 per group would be needed. This indicated that the present sample (n = 59 BDD, n = 56 HC) provided >98% power to detect effects of these magnitudes (α = 0.05, two-tailed).
Group differences in clinical and demographic characteristics between the BDD and healthy control (HC) groups were analyzed using independent-samples t-tests for continuous variables and chi-square (χ2 ) tests of independence for categorical variables. Given its demonstrated robustness to deviations from normality and equality of variances when group sizes are adequate (≥30 participants), Welch’s t-test was applied throughout (Delacre et al., Reference Delacre, Lakens and Leys2017). To evaluate cognitive performance, we conducted a one-way multivariate analysis of variance (MANOVA) with planned post hoc t-tests comparing the BDD and HC groups on each of the four WAIS-IV index scores (VCI, PRI, WMI, and PSI) and their associated subtests as well as the global IQ index, the FSIQ. Distributional assumptions were assessed using Shapiro–Wilk tests, skewness, and kurtosis; diagnostic statistics and graphical assessments are presented in Supplementary Table S1 and Supplementary Figure S1. To control for multiple comparisons, Holm–Bonferroni corrections were applied in a hierarchically. The four index-level comparisons (VCI, PRI, WMI, PSI) were corrected together (k = 4), while subtest-level comparisons were corrected within each corresponding index domain (VCI: k = 3; PRI: k = 3; WMI: k = 2; PSI: k = 2). For each test, we report the Holm-adjusted p-value, Cohen’s d effect size, and 95% confidence interval.
Full Scale IQ, subtest and process scores were computed and reported descriptively. Because the FSIQ aggregates across the four index domains and can obscure subtle but clinically meaningful index-level differences, FSIQ comparisons are reported for sample characterization purposes rather than as a primary outcome of interest. To examine whether cognitive group differences were attributable to current affective symptoms (anxiety, depression, and stress), ANCOVA with DASS-21 total score as covariate were conducted with any of the index scores that showed group differences. To assess the influence of BDD symptom severity, insight, affective symptoms, and medication status on cognitive performance, indices demonstrating significant differences between BDD and HC groups were correlated with BDD-YBOCS, BABS, the depression and anxiety subscales of the DASS-21, and SSRI medication use (point-biserial correlation).
Preregistration
This study was not preregistered as a standalone investigation. Participants were recruited as part of a preregistered randomized controlled trial examining intranasal oxytocin for BDD (Australian New Zealand Clinical Trials Registry: ACTRN12622000123718). The WAIS-IV was administered as part of the trial’s baseline cognitive assessment battery, and healthy controls were recruited for comparison purposes. The present BDD versus healthy control cognitive comparison represents a protocol-defined baseline characterization of the sample.
Results
Demographic and clinical characteristics
No significant differences were found between the groups regarding sex, age, and years of education (Table 1). On average, participants in the BDD group reported moderate to severe BDD symptom severity on the BDD-YBOCS (Phillips et al., Reference Phillips, Hollander, Rasmussen and Aronowitz1997; Phillips et al., Reference Phillips, Hart and Menard2014), poor insight on the BABS (Eisen et al., Reference Eisen, Phillips, Baer, Beer, Atala and Rasmussen1998), and severe severity across the depression, anxiety, and stress subscales of the DASS-21 (Lovibond & Lovibond, Reference Lovibond and Lovibond1995). Seventy-nine percent of BDD participants had at least one comorbid diagnosis (e.g., depression, generalized anxiety disorder), a pattern common to patients with BDD (Gunstad & Phillips, Reference Gunstad and Phillips2003). At the time of testing, all participants were stabilized on medications (Table 1).
Sociodemographic characteristics of the clinical sample and healthy controls

Note: Values are M (SD) [min–max]. For occupation, ethnicity, and medication categories, participants were able to select multiple options. BDD-YBOCS = Yale-Brown Obsessive-Compulsive Scale Modified for BDD; BABS = Brown Assessment of Beliefs Scale; DASS-21 = Depression Anxiety Stress Scales–21; SSRI = Selective Serotonin Reuptake Inhibitor; SNRI = Serotonin-Norepinephrine Reuptake Inhibitor; NDRI = Norepinephrine-Dopamine Reuptake Inhibitor. ^ Holm–Bonferroni corrected.
*** p < 0.001.
Cognitive comparison
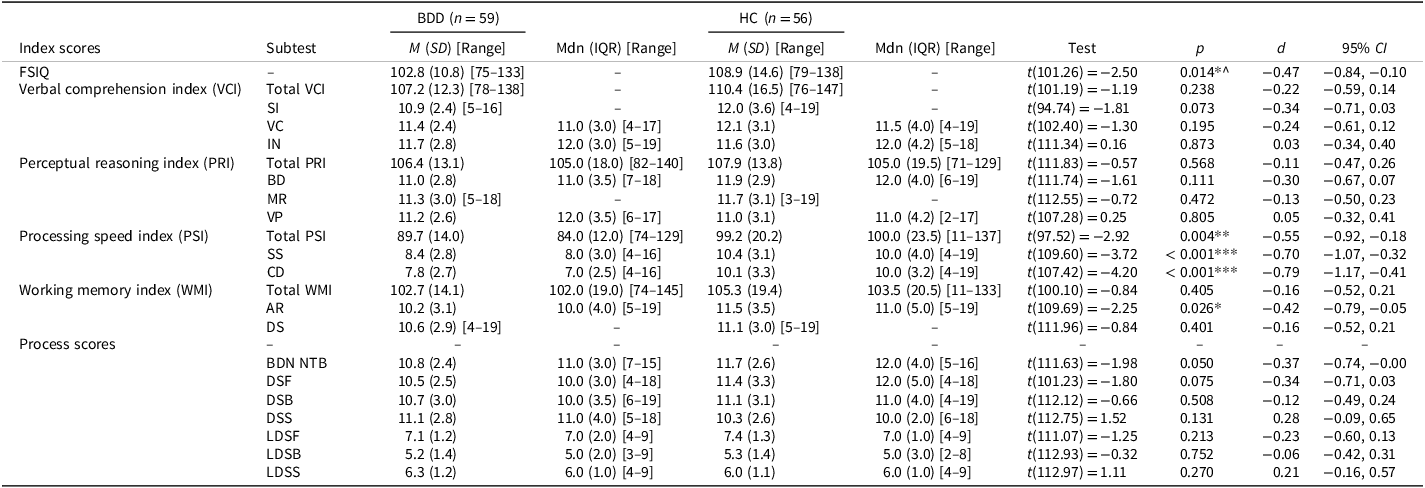
A Welch t-test revealed a statistically significant difference in FSIQ between BDD and HC groups, t(101.26) = −2.50, p = 0.014, 95% CI [−10.78, −1.24]. On average, individuals with BDD (M = 102.85, SD = 10.83) scored lower than healthy controls (M = 108.86, SD = 14.60), with a small-to-medium effect size, d = −0.47, 95% CI [−0.84, −0.10]. However, when a MANOVA was employed to compare the four indices between the two clinical groups, the results were non-significant at an overall level, Pillai’s Trace = 0.073, F(4, 110) = 2.15, p = 0.079. A Welch’s t-test revealed that the BDD cohort exhibited a significantly lower PSI compared to the HC cohort, t(97.52) = −2.92, p(adj) = 0.016, d = −0.55, 95% CI [−0.92, −0.18]. No significant differences were found for the VCI, PRI, or WMI, all ps > 0.37 (Holm-adjusted). All indices, subtest, and process scoring group comparison results are summarized in Table 2.
WAIS-IV subtest and process score descriptive statistics and group comparison tests

Note: CI = confidence interval. WAIS-IV subtest abbreviations: SI = Similarities, VC = Vocabulary, IN = Information, BD = Block Design, MR = Matrix Reasoning, VP = Visual Puzzles, DS = Digit Span, AR = Arithmetic, SS = Symbol Search, CD = Coding. Process score abbreviations: BDN NTB = Block Design No-Time-Bonus, DSF = Digit Span Forward, DSB = Digit Span Backward, DSS = Digit Span Sequencing, LDSF = Longest Digit Span Forward, LDSB = Longest Digit Span Backward, LDSS = Longest Digit Span Sequencing. M = mean, SD = standard deviation, Mdn = median, IQR = interquartile range. Welch’s t-tests were used for all comparisons as they are robust to violations of normality with n >30 per group; medians and IQRs are provided for transparency where distributions deviated from normality. p-Values shown are unadjusted; Holm-adjusted p-values are reported in the Results text. ^ = FSIQ not corrected (reported for sample characterization only).
*p < 0.05. **p < 0.01. ***p < 0.001.
Post hoc Welch’s t-test comparisons on the PSI subtests revealed significant differences between BDD and HC groups for both Symbol Search (SS), t(109.60) = −3.72, p(adj) < 0.001, d = −0.70, 95% CI [−1.07, −0.32], and Coding (CD), t(107.42) = −4.20, p(adj) < 0.001, d = −0.79, 95% CI [−1.17, −0.41]. These represent large effects, with BDD participants performing significantly more slowly than HCs on both tasks. To determine whether the processing speed deficit was independent of general cognitive ability, we conducted an ANCOVA controlling for GAI. The GAI (comprises VCI and PRI) was used rather than FSIQ to avoid collinearity, as PSI contributes directly to the FSIQ composite. The assumption of homogeneity of regression slopes was met (F = 1.73, p = 0.191). After adjusting for GAI, the group difference in PSI remained significant, F(1112) = 7.71, p = 0.006, ηp2 = 0.064. Adjusted means were 90.10, 95% CI [85.79, 94.40] for the BDD group and 98.75, 95% CI [94.34, 103.17] for healthy controls, corresponding to an adjusted Cohen’s d of −0.52, 95% CI [−0.90, −0.15]. This indicates that the processing speed deficit in BDD is not attributable to differences in general cognitive ability. To further examine whether affective symptoms account for the PSI deficit, we conducted an additional ANCOVA with DASS-21 total score as covariate. The homogeneity of regression slopes assumption was met (F = 0.06, p = 0.803). DASS-21 did not significantly predict PSI (F(1, 95) = 0.76, p = 0.386), and the group difference in PSI remained significant after adjustment, F(1, 95) = 7.39, p = 0.008, ηp2 = 0.072. Adjusted means were 87.90, 95% CI [81.37, 94.43] for the BDD group and 102.46, 95% CI [96.34, 108.58] for healthy controls, corresponding to an adjusted Cohen’s d of −0.56, 95% CI [−0.97, −0.15]. This indicates that the processing speed deficit is not attributable to the severity of comorbid affective symptoms. Within the BDD cohort, Pearson correlations indicated that PSI scores were not significantly associated with BDD symptom severity (BDD-YBOCS; r = 0.04, p = 0.801), insight (BABS; r = 0.16, p = 0.275), depression (DASS-21 depression; r = 0.14, p = 0.332), anxiety (DASS-21 anxiety; r = 0.04, p = 0.800), or SSRI medication use (r = 0.19, p = 0.149).
Although the WMI did not show significant differences in the MANOVA, the Arithmetic (AR) subtest showed a significant difference at the uncorrected level, t(109.69) = −2.25, p = 0.026, d = −0.42, 95% CI [−0.79, −0.05], with BDD participants scoring lower than HCs. This effect did not survive family-wise correction.
Discussion
This study examined cognitive performance in individuals with BDD relative to HCs using the WAIS-IV. The primary hypothesis, that cognition at the index level would be impaired in BDD, particularly in the PRI, WMI, and PSI indices, was partially confirmed; individuals with BDD demonstrated significantly lower PSI scores compared to HCs (d = −0.55, 95% CI [−0.92, −0.18]). However, no differences–including no strengths–across the remaining indices were found. Further exploration revealed that both subtests underlying the PSI, that is, the SS and CD, demonstrated significant differences in processing in BDD with large effect sizes (SS: d = −0.70, 95% CI [−1.07, −0.32], and CD d = −0.79, 95% CI [−1.17, −0.41]). Although overall cognition (FSIQ) differed across groups–aligning with previous research (Toh et al., Reference Toh, Castle and Rossell2015) – this finding was driven largely by processing speed differences, as no other significant group comparisons across the other indices or subtests were found. The alternative interpretation – that a general intellectual deficit underlies the PSI findings – is not supported; the ANCOVA controlling for GAI demonstrated that the PSI deficit remained significant after adjusting for general cognitive ability. This specific pattern, of significantly reduced processing speed, is notable in BDD. Reduced processing speed has been found in some previous research, such as Malcolm et al. (Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021) using the MCCB’s symbol coding test in a large sample (N = 65), and by Jefferies-Sewell et al. (Reference Jefferies-Sewell, Chamberlain, Fineberg and Laws2017), who demonstrated reduced processing for emotional stimuli (positive words) using the Affective Go-No Task in a small sample (N = 12). It, however, contradicts Toh et al. (Reference Toh, Castle and Rossell2015)’s finding showing no significant differences in processing speed in BDD using the coding subtest of the RBANS in their smaller sample (N = 21). It is worth noting, however that, while Toh et al. (Reference Toh, Castle and Rossell2015) did not demonstrate a significant difference for this subtest, they did find a large effect size (d = 0.85). Reduced processing speed in BDD may reflect underlying cognitive styles associated with the disorder, such as excessive attention to detail (Toh et al., Reference Toh, Castle and Rossell2017), perfectionism (Buhlmann et al., Reference Buhlmann, Etcoff and Wilhelm2008; Hartmann et al., Reference Hartmann, Thomas, Greenberg, Matheny and Wilhelm2014) and heightened self-monitoring (Feusner et al., Reference Feusner, Hembacher, Moller and Moody2011). These traits may interfere with rapid visual scanning required in the symbol substitution task and ultimately reduce processing speed.
It is noteworthy that the current study did not replicate previous findings of further significant differences across the two other cognitive domains: PRI and WMI. The finding of intact visual reasoning, as measured through the BD, VP, and MR subtests of the PRI, was unexpected given the fairly consistent literature showing differences on these types of tasks (Holmes à Court et al., Reference Holmes à Court, Malcolm, Toh and Rossell2025a). BD, VP, and MR are considered complex visuospatial tasks, involving pattern recognition – at both local and global detail levels – as well as visual problem-solving (Lichtenberger & Kaufman, Reference Lichtenberger and Kaufman2013). A tendency to favor local over global processing, has been flagged as a likely cognitive marker of BDD across behavioral and neurobiological studies (Holmes à Court et al., Reference Holmes à Court, Malcolm, Toh and Rossell2025a). However, an alternative explanation is that previously reported deficits in visuospatial performance may not reflect impaired spatial reasoning per se, but might instead reflect broader difficulties with processing speed. That is, poorer performance on visuospatial tasks in earlier studies may have been driven by time-based demands, rather than a true deficit in visual reasoning ability.
Although the WMI was not significant at the index level, the AR subtest showed a significant difference at the uncorrected level (p = .027, d = −0.42) – consistent with Malcolm et al. (Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021), who demonstrated working memory deficits on a letter–number span task, particularly in their broadly cognitively impaired subgroup. Both AR and the letter–number span task require sustained concentration and mental manipulation of information under time pressure – demands that may be particularly challenging for individuals with BDD given their tendency toward rumination and self-focused attention. In contrast, the DS subtest, which showed no group differences, involves simpler rehearsal processes that may be less susceptible to interference from intrusive thoughts. Additionally, the current study did not stratify participants into cognitive subgroups, as in Malcolm et al. (Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021). It is therefore possible that working memory differences are more pronounced in a subset of individuals with BDD, or emerge selectively on tasks requiring greater effortful processing. Further work should explore these issues.
Of note, SS and CD are pure processing speed measures, where scores directly reflect the number of items completed within a fixed time limit. In contrast, BD and VP primarily assess visuospatial reasoning ability, with time contributing only bonus points. On reasoning tasks, both groups are constrained by the cognitive demands of problem-solving; on pure speed tasks, group differences in processing efficiency become clearly apparent. The PSI deficit therefore likely reflects a genuine processing speed weakness rather than general vulnerability to timed conditions.
Recent transdiagnostic research has documented cognitive dysfunction as a shared feature across psychiatric disorders, conceptualized as a “C factor” that parallels general psychopathology (Abramovitch et al., Reference Abramovitch, Short and Schweiger2021). Within this framework, executive functions and episodic memory have been identified as the most consistently impaired domains (East-Richard et al., Reference East-Richard, R.-Mercier, Nadeau and Cellard2020), while cognitive deficits appear to follow a different clinical trajectory to symptoms – persisting independently of symptom severity and remission status (Chavez-Baldini et al., Reference Chavez-Baldini, Nieman, Keestra, Lok, Mocking, de Koning, Krzhizhanovskaya, Bockting, van Rooijen, Smit, Sutterland, Verweij, van Wingen, Wigman, Vulink and Denys2023). The present findings align with several aspects of this model: PSI was not correlated with BDD severity, insight, depression, anxiety, or medication use, and group differences remained after controlling for affective symptoms. However, the selective nature of the deficit – confined to processing speed with intact performance across other domains – differs from the diffuse pattern typically associated with general psychopathology. This selective profile may reflect disorder-specific mechanisms, such as the perfectionism and excessive attention to detail characteristic of BDD.
An unexpected finding was that healthy controls exhibited greater variability than the BDD group across all WAIS-IV measures – the opposite pattern to Malcolm et al. (Reference Malcolm, Brennan, Grace, Pikoos, Toh, Labuschagne, Buchanan, Kaplan, Castle and Rossell2021). This likely reflects our recruitment methodology: BDD participants were required to meet a symptomatic threshold on the BDD-YBOCS for clinical trial entry, constraining the sample to a narrower severity band, whereas controls recruited through community methods captured a broader spectrum of cognitive ability. The trait-like nature of processing speed deficits – that is, they are independent of symptom severity – suggest that the cognitive cost of a BDD diagnosis is relatively uniform across affected individuals. Importantly, this reduced variability does not undermine the observed group differences.
These findings have implications for both clinical assessment and intervention. Clinically, reduced processing speed may impact the ability of individuals with BDD to engage efficiently in cognitively demanding tasks, particularly those requiring rapid visual discrimination or sustained attention. This has potential implications for treatment planning, suggesting a need to pace interventions accordingly and consider cognitive load when delivering psychoeducation or cognitive-behavioral strategies. Currently BDD has not attracted significant attention from neuropsychologists, yet the results perhaps suggest a need for a comprehensive neuropsychological assessment. Addressing specific cognitive deficiencies can potentially improve overall everyday functioning in BDD.
This study addresses the need for a clinically familiar, standardized assessment of cognition in BDD. Evaluators were not blind to diagnostic group during WAIS-IV administration and scoring; however, the standardized administration procedures and objective scoring criteria of the WAIS-IV minimize potential for evaluator bias. Additionally, performance validity was not formally assessed. Recent reviews highlight that motivational factors, including effort, reward sensitivity, and attitudes toward testing, may contribute to cognitive underperformance in psychiatric samples, and that the ecological validity of standardized neuropsychological tests in clinical populations remains uncertain (Abramovitch et al., Reference Abramovitch, Short and Schweiger2021). While the PSI deficit was independent of current affective symptom severity, the high rate of psychiatric comorbidity in BDD (averaging 2.5 comorbid diagnoses in the current sample) means that contributions from specific comorbid disorders cannot be ruled out. While the WAIS-IV PSI subtests provide clinically meaningful indices of processing speed, computerized tasks measuring reaction time with millisecond precision may offer greater sensitivity and specificity; future research should examine whether similar deficits emerge using such measures. Additionally, while the utility of the WAIS-IV is widely recognized, its subtests do not map neatly onto the cognitive domains typically reported in the BDD literature (Grégoire, Reference Grégoire2013). Future research should make explicit comparisons between specific WAIS subtests and previously studied – often experimental – cognitive tasks, to aid interpretation. A more detailed comparison between WAIS indices and experimental visuospatial tasks may be particularly valuable in clarifying the nature of visuospatial processing difficulties in BDD. Although the sample was relatively large for BDD research, it was predominantly female; given that BDD affects males and females at approximately equal rates in the community (Koran et al., Reference Koran, Abujaoude, Large and Serpe2008), this limits generalisability to the broader population. Longitudinal studies are needed to determine whether processing speed deficits contribute to the development or maintenance of BDD symptoms. The apparent selectivity of the processing speed deficit may partly reflect the WAIS-IV’s measurement structure, which separates cognitive domains into distinct indices differently to batteries such as the RBANS or MCCB. Future studies using alternative assessment approaches would help determine whether this selective profile replicates across measurement paradigms. Given the characteristic low self-esteem in BDD, future research should also examine whether self-efficacy and motivational factors mediate cognitive performance in this population.
Conclusion
The study undertook a comprehensive investigation of cognition in BDD utilizing a gold standard measure, the WAIS-IV, familiar to clinicians and researchers alike. The specific cognitive profile found – characterized by preserved reasoning and verbal abilities but with reduced processing speed – is novel in the context of BDD. Notably, this deficit was independent of general cognitive ability and unrelated to BDD symptom severity, insight, or affective symptoms, suggesting it may represent a stable cognitive feature rather than a state-dependent effect. The observed processing speed weakness may reflect vulnerabilities in cognitive efficiency and visual processing, contributing to a sense of “cognitive deficiency” clinically reported by individuals with the disorder.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1355617726101970
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Acknowledgements
None.
Author contributions
CRediT authorship contribution statement. SLR, WLT, and KHC were involved in the conceptualization and methodology development of this research study. SLR obtained the funding and ethics approval and supervised this work. Additionally, KHàC collected data and conducted statistical analyses. EB collected data, RI provided statistical support. All authors reviewed results. KHàC wrote the original draft, and all authors reviewed and edited the manuscript.
Funding statement
This work was supported by a Senior National Health and Medical Research Council Research Fellowship (GNT1154651 to SR) and funding to RI from the Mental Health Australia General Clinical Trials Network (MAGNET). All funding sources had no role in the study design, collection, analysis or interpretation of the data, writing of the manuscript, or the decision to submit the paper for publication.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical standards
The studies involving humans were approved by Swinburne University’s Human Research Ethics Committee (SUHREC-5412). The studies were conducted in accordance with the local legislation and institutional requirements.
Consent statement
The participants provided their written informed consent to participate in this study.
AI declaration
During the preparation of this work the authors used ChatGPT (GPT-5; OpenAI, 2025) in order to assist with language editing. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.





 Open access
Open access