


Dietary education in UK-based cardiac rehabilitation (CR) is most frequently delivered in two group-based or individual classes and largely reflects the current consensus of the cardioprotective diet(Reference James, Butler and Nichols1). The Mediterranean-style diet and dietary approaches for the management of overweight and obesity, dyslipidaemia and hypertension are strongly advocated in the educational content of UK-based CR(Reference James, Butler and Nichols1). Education of this nature can elicit positive dietary modification in people with CHD. Dietary education as part of, or in addition to, core CR has been shown to increase participants’ intake of fruits, vegetables and fish and successfully modify fat and/or carbohydrate intake in accordance with the education given(Reference Laursen, Johansen and Joensen2–Reference Zwisler, Soja and Rasmussen4).
Few studies have investigated the effect of targeted dietary education on modifying protein intake in people with CHD. Adequate protein intake (> 1·2 g/kg body mass, for people with a chronic long-term condition(Reference Bauer, Biolo and Cederholm5,Reference Deutz, Bauer and Barazzoni6) ) supports preservation of lean mass and physical function(Reference Campbell, Deutz and Volpi7). This is particularly important in cohorts, such as those with CHD, where weight loss is often encouraged, but is caveated with the need to minimise loss of lean, as opposed to adipose tissue(Reference Cava, Yeat and Mittendorfer8). Low lean mass(Reference Nichols, O’doherty and Taylor9) and related pathologies (e.g. frailty(Reference Purser, Kuchibhatla and Fillenbaum10) and sarcopenia(Reference Zhang, Zhu and Liu11)) are common and worsen prognosis in people with CHD. We recently showed that education concerning the importance of dietary protein intake is a low priority in UK-based CR and warrants increased focus(Reference James, Butler and Nichols1). Given that targeted education interventions can initiate favourable changes to dietary intake(Reference Laursen, Johansen and Joensen2–Reference Zwisler, Soja and Rasmussen4), evidence-based interventions designed to increase protein intake could be useful adjuncts to standard CR.
This pilot randomised controlled trial was primarily aimed at assessing whether a targeted education intervention, designed to increase protein intake in people with CHD, can be implemented as an adjunct to a standard 6-week CR programme. Secondary aims were to (1) identify the prevalence of low protein intake in CR attendees with CHD, (2) identify whether protein intake was different based on poor physical function and (3) identify the intervention effect on sit-to-stand ability and risk of sarcopenia. The findings of this pilot study are intended to inform a definitive, adequately powered study.
Methods
Study design
This single-centre, parallel-group, two-arm pilot randomised controlled trial was implemented as an adjunct to a standard CR programme, using a pragmatic study design. The trial is conducted and reported in accordance with the Consolidated Standards of Reporting Trials 2021 statement: extension to randomised pilot and feasibility trials(Reference Eldridge, Chan and Campbell12). Volunteers provided baseline data at the start of their 6-week CR programme. Those with protein intake < 1·2 g/kg per d were randomised to an intervention protein group (PG) or a control group (CG). Intervention endpoint and follow-up data were collected post-6 and 12 weeks. Study activities were predominantly undertaken in person, with remote options available if participants preferred.
Patient and public involvement
Feedback on the study design and study documents was provided by members of the Public Involvement in Research Group at the Sheffield Hallam University Advanced Wellbeing Research Centre prior to submission for Research Ethics Committee (REC) review. Feedback from the public involvement group was considered, and the study was amended as appropriate. For example, some sections of the patient-facing documents were reworded to ensure that they were easily understood by a lay audience.
Cardiac rehabilitation
Study participants were recruited from three community-based CR programmes in Newcastle-upon-Tyne, UK, after referral from primary care. The CR programme involved twelve core sessions, ideally attended twice per week over 6 weeks or over a longer time as needed. All sessions involved supervised, circuit-based exercise (45 min), combining both aerobic and resistance exercises. Six of twelve sessions were supplemented with 1 h of education about CHD secondary prevention, including one dietitian-led nutritional education session based around the Eatwell Guide(13). The six education sessions were delivered cyclically by relevant healthcare professionals. New patients attended the CR centres weekly to start their 6-week programme due to a rolling referral process from primary care. Accordingly, each patient received their standardised dietitian-led nutritional education session at a different point in their 6-week course.
Intervention
Eligible participants were assigned an alphanumeric code and randomised (1:1) to the PG or CG. The allocation sequence was generated a priori by a member of the research team using RAND, ROUNDUP and RANK spreadsheet functions (MS Excel).
The intervention consisted of one pre-recorded dietary education session lasting ∼20 min, in addition to (and mimicking the current embedded delivery of) the dietary education session received as part of the standard CR programme. The intervention either summarised the information provided in core CR dietary education (CG) or contained targeted information designed to educate participants on how to increase and improve the quality of their dietary protein intake (PG). The PG intervention explained the advantages of increasing protein intake, presented target protein intake by body weight and provided example daily menus. The content was aligned with UK Government dietary guidance(13) and our understanding of the cardioprotective diet, with emphasis on incorporating sufficient and varied sources of high-quality protein (defined as having a Digestible Indispensable Amino Acid Score of ≥ 75 %(14)). The format of delivery replicated how the core dietary education session was delivered, in terms of being instructor led with an opportunity for the participant to ask questions about their learning. However, the educational content was pre-recorded to ensure intervention consistency between participants. In accordance with the pragmatic study design, the intervention length was kept to approximately 20 min to avoid excessive participant burden and allow the intervention to be embedded within the current CR resource (i.e. delivered at the location of the existing CR sessions and during a time that clinical CR staff were present).
Creation of the education sessions was multistage. We collaboratively updated the currently used dietary education material in accordance with the British Association for Cardiovascular Prevention and Rehabilitation’s recommended practices. Using this material as a template, new educational material for the PG was created. Several iterations of the material were reviewed by members of the research team, an National Health Service (NHS) dietitian and CR co-ordinators before final approval of all co-authors. Participants watched their assigned pre-recorded education session via a laptop at their usual CR session or were emailed a web link to access the video remotely during their first week of the CR programme. This was intended to give the participants the greatest opportunity possible to make behavioural changes. Where the participant accessed the video remotely, verbal confirmation was requested that this had been completed. The participant was also asked to briefly summarise their learning to a researcher.
Participants
We included people, ≥ 50 years, enrolled in standard CR with a dietary education component, following a recent clinical diagnosis of CHD or related cardiac event. Pronounced declines in muscle mass (1–2 % per year) and strength/function (1–5 % per year) occur after 50 years of age(Reference Keller and Engelhardt15); accordingly, this cohort was considered to be likely to attain the greatest benefit from an intervention designed to increase protein intake. All participants provided written informed consent. Potentially eligible participants were initially identified by the existing cardiac care team before being provided with study information. After at least 24 h, participants provided their informed consent to participate and began recording their dietary intake in a 3-d food diary at home. Those with protein intake < 1·2 g/kg per d at baseline assessment were eligible for the intervention, chosen as expert groups recommend a target protein intake of at least 1·2 g/kg per d for older adults with chronic diseases(Reference Bauer, Biolo and Cederholm5,Reference Deutz, Bauer and Barazzoni6) . Exclusion criteria included a contraindication to light exercise, being medically unable to alter their diet and known stage 4 or 5 chronic kidney disease.
Study procedures
Baseline data were collected at the start of the CR programme. Initial follow-up was completed ideally 6 weeks from baseline assessments; this was adjusted as needed to align with the participant finishing their core CR programme. Additional follow-up assessments were conducted 6 weeks after completion of the CR programme (12 weeks).
Anthropometry
Stature (m), body mass (kg) and waist circumference (cm) were measured by an exercise instructor or cardiac nurse during the standard induction of people joining the CR programme.
Dietary intake
A 3-d food diary (two weekdays and one weekend day) was completed at home, while participants maintained their usual diet. Written instructions and an example food diary entry were provided, including instructions to specify the volume, frequency and brand names of all food and drinks consumed. A researcher obtained any missing details from the food diary during discussions with participants. Analysis of energy and macronutrient content of common foods is similar between researcher-led weighed portion analysis and participant-reported estimated food diaries (CV for protein content: 10·7 %)(Reference Curtis, Hills and Arjomandkhah16). Reliable quantification of macronutrient consumption can be obtained with 3 d of food diary data (r = 0·8)(Reference Singh, Verest and Salathé17). Based on a within-person CV of 12 % for daily protein intake based on weighed 3-d dietary records(Reference dos Santos Vaz, Bittencourt and Almeida18), to detect a 15 % change in an individual’s protein intake between repeated diaries with 95 % confidence, 2–3 d of diet reporting are sufficient(Reference Willett19).
Questionnaires
The Physical Activity Vital Signs questionnaire asks: (1) How many days during the past week have you performed physical activity where your heart beats faster and your breathing is harder than normal for 30 min or more? And (2) How many days in a typical week do you perform activities like this?(Reference Greenwood, Joy and Stanford20) The SARC-F + EBM uses self-reported signs of indicative sarcopenia, age and BMI to generate a sarcopenia risk score, where ≥ 12 points indicates risk of sarcopenia(Reference Kurita, Wakita and Kamitani21).
Participants completed a researcher-developed questionnaire (online Supplementary Material 1), comprising a five-point Likert scale response to the statement ‘I feel like I have a good understanding of how the food I eat can affect my health’ and a list of thirteen foods from which to identify good protein sources. Feedback on the intervention was requested at week 6.
Sit-to-stand test
Participants completed five successive chair stands as quickly as possible using a chair with a standard seat height and a straight back. Inability to complete five repetitions in ≤ 15 s indicates probable sarcopenia(Reference Cruz-Jentoft, Bahat and Bauer22).
Statistical analyses and justification of sample size
Food diary data were inputted into dietary analysis software (Nutritics Professional Plus v5·81, 2022) by one researcher. Total energy (kcal/d), macronutrient and micronutrient values collected over 3 d are presented as average intake per d. Macronutrient intakes were corrected for body mass. RMR was estimated using the Mifflin-St Jeor equation(Reference Mifflin, St Jeor and Hill23).
Statistical analyses were performed using SPSS (SPSS IBM Corp, Version 27.0). Given the modest sample size, non-parametric methods were used for all analyses. Variables are reported as frequency (percentage) or median (25th, 75th percentile). Demographic characteristics are stratified by baseline protein intake (≥ 1·2 or < 1·2 g/kg per d). Associations between protein intake and variables of interest were calculated using Spearman’s rank correlations. Due to missing data, descriptive statistics are reported with the number of participants for individual variables. The median change between timepoints is reported for the PG and CG (complete cases) for dietary intake, sit-to-stand performance and sarcopenia risk score. Effect sizes are reported, defined as small (0·2), medium (0·5) and large (0·8) effects(Reference Coolican24). Due to a lack of statistical power and consistent with the Consolidated Standards of Reporting Trials guidance for reporting pilot trials, P-values are not reported(Reference Eldridge, Chan and Campbell25).
Pilot studies require a minimum of twenty-four participants(Reference Julious26). Anticipating 20 % attrition at follow-up, we aimed to recruit thirty participants with low protein intake (fifteen per group) over 12 months. We previously identified protein intakes < 1·2 g/kg per d in 70 % of people with CHD (James et al., unpublished data). Accordingly, we estimated that screening approximately forty-three patients at baseline would be sufficient to meet the intended sample size.
Missing data
To facilitate the calculation of the primary outcome (protein intake (g/kg per d)), we used the last observation carried forward for the missing follow-up body mass values. For transparency, we also present absolute changes in protein intake without data imputation. All other variables underwent complete case analysis.
Results
Between February 2022 and July 2023, ninety-five people were approached to participate in this study (Figure 1). Baseline data were provided by thirty-four consenting participants (35·7 % uptake); twenty-seven (79·4 %) had low protein intake and were randomised to the PG (n 15) or CG (n 12). One participant chose to view the educational video remotely. No other study activities were completed remotely.
Study recruitment (February 2022–July 2023). CR, cardiac rehabilitation.

Baseline demographics
Table 1 shows baseline characteristics. Baseline protein intake (g/kg per d) was associated with waist circumference (r = −0·348, P = 0·044; n 34) but not sit-to-stand time (r = 0·029, P = 0·878; n 31) or age (r = 0·189, P = 0·285; n 34).
Baseline characteristics. Median (IQR) or frequency (%)

IQR, interquartile range; PAVS, Physical Activity Vital Signs.
*n 24, †n 6.
Four participants (three in the low protein group (PG)) were unable to complete the sit-to-stand test unaided (median protein intake 0·87 g/kg per d). Twenty-nine participants who completed the test did so in < 15 s. Three (8·8 %) participants scored ≥ 12 points on the SARC-F + EBM questionnaire, of which one had a protein intake < 1·2 g/kg per d.
Intervention effect and evaluation
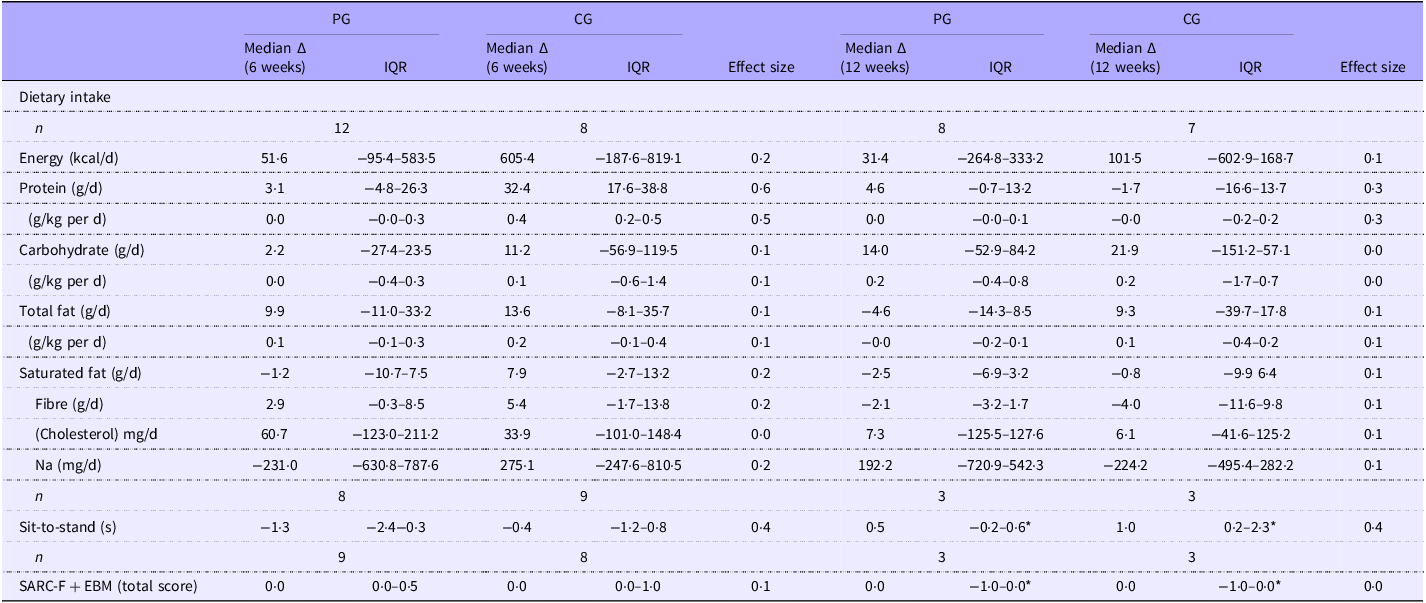
Table 2 shows a complete case analysis of the intervention effect. Variables of interest for all cases are presented in online Supplementary Table S1. Baseline median dietary protein intake was lower in the CG (0·7 (0·5–0·8) g/kg per d) than the PG (0·9 (0·7–1·1) g/kg per d). Individual data points are shown in Figure 2.
Change in outcome variables between timepoints (complete cases)

*Median (range).
Individual change in protein intake in the (a) control and (b) intervention groups. Median (interquartile range) protein intake was 0·7 (0·5–0·8), 1·0 (0·9–1·1) and 0·9 (0·7–1·2) g/kg per d in the control group and 0·9 (0·7–1·1), 1·0 (0·9–1·2) and 1·1 (0·9–1·2) g/kg per d in the intervention group at baseline, week 6 and week 12, respectively. The dashed line indicates target protein intake.

At week 6, the median change in protein intake was 0·0 (−0·0–0·3) and 0·4 (0·2–0·5) g/kg per d in the PG and CG, respectively (medium effect size: 0·5). At week 12, there was no change in protein intake in either group Figure 2(a) and (b). Effect sizes between groups for all other variables were small to medium. Participants considered the educational information to be new to them (38 %), helpful (100 %), easy to understand (100 %) and inspiring dietary changes (78 %; online Supplementary Table S2 and Material 2).
Discussion
This pilot randomised controlled trial aimed to identify whether a targeted educational intervention to increase dietary protein intake in people with CHD and low protein intake could be implemented as an adjunct to standard CR dietary education. This information was intended to inform the implementation of a definitive trial. Low protein intake was prevalent in CR attendees (79·4 %). Changes to primary and secondary outcomes were minimal. The intervention appeared well-received by those who completed the study; however, uptake of the study was low, and attrition was high, suggesting that recruitment to a larger trial in a timely manner would be unfeasible.
Protein and other dietary intake
A high prevalence of low protein intake in older adults is reported in the present study (79·4 %) and by others (70·8 %)(Reference Hengeveld, Boer and Gaudreau27), potentially explained by a limited understanding of the importance of protein intake in this cohort(Reference Carrillo, Chaya and Viadel28). Although people attending structured CR programmes are uniquely positioned to receive targeted protein education, current dietary education in UK-based CR programmes contains minimal focus on increasing protein intake(Reference James, Butler and Nichols1). Older people with chronic diseases need 1·2–1·5 g/kg per d of dietary protein(Reference Bauer, Biolo and Cederholm5,Reference Deutz, Bauer and Barazzoni6) ; this is higher than recommended for healthy younger adults(Reference Trumbo, Schlicker and Yates29) to compensate for age-related anabolic resistance, insulin resistance, physical inactivity and inflammatory status(Reference Bauer, Biolo and Cederholm5,Reference Guillet, Prod’homme and Balage30,Reference Volpi, Mittendorfer and Rasmussen31) . We report that protein intake was inversely associated with waist circumference (r = −0·348). Elevated waist circumference increases cardiometabolic risk independently of BMI(Reference Powell-Wiley, Poirier and Burke32). The association between higher protein intake and lower adiposity is likely due to the satiety and thermogenic response-promoting properties of protein compared with other macronutrients(Reference Drummen, Tischmann and Gatta-Cherifi33). Weight management is a core focus of dietary education in one-quarter of the UK CR programme(Reference James, Butler and Nichols1); one way to support this could be through dietary interventions promoting adequate protein intake as part of CR.
Previously, two 30-min education sessions based on the Mediterranean diet, incorporated into a 6-week CR programme, did not influence protein intake(Reference Moore, Tsakirides and Rutherford34). Our study extends these findings, demonstrating that targeted protein-specific education was not more effective than standard dietary education at increasing protein intake. The increase in protein intake was greater in the CG at week 6 (compared with the PG), possibly attributed to the higher median protein intake at baseline in the PG (median 0·9 g/kg per d, v. 0·7 g/kg per d in the CG). The ‘ceiling effect’ determines that the magnitude of dietary change following intervention is smaller in people with higher baseline adherence to a favourable dietary pattern(Reference Fernandez-Lazaro, Toledo and Buil-Cosiales35). That is, those with a lower protein intake at baseline in the present study had greater room for improvement following intervention. Alternatively, participants who have inadvertently become aware that they were allocated to the control group may be motivated to change their behaviour to improve their protein intake(Reference Hébert, Frongillo and Adams36,Reference McCambridge, Kypri and Elbourne37) .
We acknowledge that the ‘dose’ of the intervention in the present study was minimal. To the best of our knowledge, the effect of targeted education sessions to increase protein intake has not previously been assessed in CR. We, therefore, did not have a reference point for the most effective intervention dose. Instead, we used a pragmatic intervention design intended to mimic the current embedded delivery of dietary education practices in the UK-based CR. This avoided introducing an additional independent variable by changing the education methods as well as the content. That the currently used dietary education dose for CR was not sufficient to elicit meaningful changes in dietary intake is, in itself, an important finding of this feasibility study. Furthermore, median values for self-reported moderate-to-vigorous physical activity already met or exceeded the exercise guidelines recommended by the Association of Chartered Physiotherapists in Cardiovascular Rehabilitation at baseline in both groups(38) and increased further in the intervention group over the course of the study (online Supplementary Table 1). An increased exercise training stimulus increases protein intake requirements, further highlighting the need for effective dietary support in those attending exercise-based CR.
The change in most nutritional components, excluding protein, was similar across groups at both time points (effect sizes ≤ 0·3). Three nutrition-focused sessions were suggested as the minimum required to positively influence dietary intake during CR(Reference Lara-Breitinger, Lynch and Kopecky39), with empirical support for up to six dietary education sessions over 3 weeks favourably altering fat, fruit and vegetable intake(Reference Froger-Bompas, Laviolle and Guillo40). Conversely, the same dietary components were successfully altered following one dietary education session during a 4-week CR programme(Reference Laursen, Johansen and Joensen2). The addition of behaviour change techniques in the latter study is notable(Reference Laursen, Johansen and Joensen2), highlighting a potential avenue to influence dietary intake in shorter CR programmes. The rationale for the two sessions in the present study was that we wanted to replicate standard care identified in our previously published national survey, thereby using a ‘real-world’ approach(Reference James, Butler and Nichols1).
Physical function and sarcopenia risk
Similar to others(Reference Coelho-Júnior, Milano-Teixeira and Rodrigues41), we found no association between sit-to-stand time and protein intake at baseline. Sit-to-stand time and other measures of physical function improve following CR completion(Reference Rengo, Savage and Shaw42,Reference Marzuca-Nassr, Seron and Román43) . Participants in the PG completed the sit-to-stand test more quickly after the intervention (−0·9 s). Given the lack of change in protein intake in the PG, the protein intervention is unlikely to be causal. The CG saw a smaller improvement in sit-to-stand performance (−0·4 s), coinciding with a median reduction in physical activity (Physical Activity Vital Signs response; −0·5 d per week) between baseline and week 12. Together, these might signify either deconditioning or the presence of a new injury that would preclude physical activity and worsen sit-to-stand performance. Alternatively, as participants in the CG had a higher SARC-F + EBM score at baseline compared with those in the PG, it could be speculated that standard CR is not adequately tailored to improve physical function in participants at a higher risk of sarcopenia. Of the three participants identified as being at risk of sarcopenia via the SARC-F + EBM questionnaire, only one had a low protein intake. Due to our small sample size, it is difficult to form a conclusion about this finding. Additionally, objective measures of body composition and muscle function and quality have greater utility to detect sarcopenia and should be prioritised over risk-based questionnaire scores where available for laboratory-based studies.
Acceptability of the intervention
Encouragingly, all participants reported the information in the educational sessions to be helpful. The high proportion of participants who reportedly planned to change their diet based on the information given to them (88·9 and 65·2 % in the PG and CG groups, respectively) is likely influenced by self-selection of the participant group (i.e. people attending CR are actively addressing their long-term health). Despite most participants newly planning to adjust their diet, half reported that the educational information given was already known to them, and overall, we saw minimal change in dietary intake at either time point. This suggests that lack of information is not the main barrier to healthful dietary choices, as, ultimately, many did not appear to act on their intention to change. This potentially strengthens the argument for incorporating behaviour change techniques into CR delivery.
Uptake of the intervention from invited participants (36·7 %) was lower than for previous similar trials (≥ 48 %; 3, 4). Furthermore, attrition at 12 weeks for randomised participants, although similar between groups, was more than double the anticipated level (44 %), likely precluding implementation of a full-scale trial. In practice, our findings suggest that additional support might be needed to increase protein intake in people with CHD. Strategies could include increasing the number of education sessions, incorporating behaviour change techniques or providing protein supplementation.
Strengths and limitations
We evaluated a novel educational intervention designed to increase protein intake using a pragmatic study design to determine real-world feasibility. Additionally, we report the effectiveness of standard CR dietary education to increase protein intake in people with CHD. Protein intake is a comparatively under-reported outcome, evidenced by previous similar studies that evaluated the effectiveness of CR dietary education on intake of fruits, vegetables, fish, fats and carbohydrates.
Limitations of this study include the small sample size and differences in baseline protein intakes between the randomly assigned PG and CG. We used food diaries to estimate dietary intake. Although self-reported dietary intake is widely collected in nutrition research, under-reporting of dietary intake is common when using this approach.
Summary
Low protein intake was prevalent in people with CHD; however, it did not appear to be associated with sarcopenia risk or sit-to-stand time. The findings of this pilot study were intended to inform a larger randomised controlled trial. Although the intervention effect cannot be definitively reported due to the present study being underpowered, it appears that protein intake was not altered following a targeted protein education intervention. Additionally, despite the intervention being well-received by study completers, the low recruitment rate and high attrition substantially limit both the implementation of a definitive trial and the interpretation of efficacy. New interventions to increase protein intake should be developed using patient involvement for assessment in future research and using methods beyond the constraints of current CR delivery methods.
Implications for practice
The education content was reviewed favourably by participants, who largely reported subsequent intent to alter their diet. Therefore, the lack of knowledge of a healthy diet among participants does not appear to be a limiting factor in eliciting behaviour change. Dietary education as part of CR should be reviewed and steps taken to improve its effectiveness.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107235.
Acknowledgements
We would like to thank the participants for their time and commitment. We would also like to thank the CR teams at each of our study sites, including cardiac nurses, dietitians and exercise practitioners, for their help and support, which made this study possible.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
E. J.: conceptualisation, data curation, formal analysis, methodology, project administration, writing – original draft, writing – review & editing; R. D.: methodology, writing – review & editing; R. B-S.: data curation, writing – review & editing; E. R.: methodology, writing – review & editing; S. G.: conceptualisation, methodology, supervision, writing – review & editing; S. N.: conceptualisation, methodology, supervision, writing – review & editing; A. F. O.: conceptualisation, methodology, supervision, writing – review & editing.
The authors declare no conflicts of interest.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Health Research Authority Northeast-Tyne and Wear South Research Ethics Committee; 21/NE/0117. Written informed consent was obtained from all subjects. The trial was registered at ClinicalTrials.gov on 10 August 2021 (identifier NCT04999358).






 Open access
Open access