Choline is an essential micronutrient involved in neurotransmitter synthesis, cell membrane signalling, lipid transport and methyl-group metabolism(Reference Zeisel and da Costa1). It exists in two forms in food: water-soluble (free choline, phosphocholine and glycerophosphocholine) and fat-soluble (phosphatidylcholine and sphingomyelin)(Reference Zeisel, Mar and Howe2). Fat-soluble choline is abundant in animal-derived foods such as red meat, eggs and fish, whereas plant-based foods primarily provide water-soluble choline(Reference Zeisel, Mar and Howe2). Betaine, derived from choline via an irreversible reaction, is an intracellular osmolyte and a methyl donor(Reference Arumugam, Paal and Donohue3). Dietary betaine mainly comes from plant foods such as cereals and vegetables(Reference Dobrijević, Pastor and Nastić4). Despite their biological importance, the gut microbiota can also metabolise unabsorbed choline and betaine into trimethylamine, which is further converted in the liver to trimethylamine-N-oxide (TMAO)(Reference Wang, Klipfell and Bennett5,Reference Fennema, Phillips and Shephard6) . TMAO is a potential risk factor for multiple health outcomes, including CVD, hypertension, diabetes and all-cause mortality(Reference Li, Lu and Yuan7). Therefore, depending on intake levels, choline and betaine may have both protective and detrimental effects on human health.
Only a few epidemiologic studies have examined the association between choline-containing compounds and betaine intake and mortality risk and produced conflicting findings. Two large US cohort studies reported that higher intake of total choline or phosphatidylcholine was associated with an increased risk of all-cause and CVD mortality(Reference Zheng, Li and Rimm8,Reference Mazidi, Katsiki and Mikhailidis9) . In three racially diverse cohorts, total choline intake was positively related to the risk of death from any cause and cardiometabolic diseases among black Americans and Chinese but not among white Americans. However, the positive association of betaine intake with all-cause and cardiometabolic mortality was only predominant in Chinese(Reference Yang, Lipworth and Shu10). A recent US cohort study revealed a nonlinear association between total choline intake and all-cause mortality, where moderate choline intake was associated with a lower mortality risk(Reference Peng, Zhang and Cai11). In contrast, null associations were observed between total choline intake and all-cause or CVD mortality in large Swedish and Japanese cohorts(Reference Karlsson, Winkvist and Strid12,Reference Nagata, Wada and Tamura13) . Nevertheless, the Swedish cohort showed an inverse association between betaine intake and all-cause mortality in women rather than in men(Reference Karlsson, Winkvist and Strid12). Instead, higher betaine intake was associated with a reduced risk of death from coronary heart disease in Japanese men but not in Japanese women(Reference Nagata, Wada and Tamura13). A systematic review and dose–response meta-analysis of cohort studies found that dietary choline was positively associated with all-cause and CVD mortality, and betaine intake increased the stroke mortality risk at doses of 50–250 mg/d(Reference Sharifi-Zahabi, Soltani and Asiaei14). The inconsistent findings are likely due to differences in dietary habits(Reference Zhao, Liu and Yu15), genetic backgrounds(Reference da Costa, Corbin and Niculescu16) and gut microbial composition(Reference Jardon, Canfora and Goossens17). Most previous studies were conducted in Americans, who consumed plenty of animal-derived foods (e.g. red meat, eggs and dairy products)(Reference Vennemann, Ioannidou and Valsta18,Reference Wallace and Fulgoni19) . Epidemiologic evidence on dietary choline and betaine and all-cause mortality remains scarce among Eastern populations with predominantly plant-based diets high in vegetables and staple foods(Reference Zhao, Liu and Yu15). Variations in food sources of choline affect not only total choline intake but also the intake and proportions of its different forms(Reference Van Parys, Karlsson and Vinknes20). Choline intake from various choline-containing compounds may be linked to mortality in distinct ways(Reference Yang, Lipworth and Shu10,Reference Karlsson, Winkvist and Strid12,Reference Nagata, Wada and Tamura13) , and this should be explored within the context of specific dietary patterns.
Against this background, we prospectively investigated the association of dietary total choline, individual choline forms and betaine with all-cause mortality in Chinese adults over 18 years, using data from the China Health and Nutrition Survey (CHNS).
Methods
Study design and participants
CHNS is an ongoing, open cohort study designed to assess the effects of social and economic transformations on nutritional and health outcomes in China. Initiated in 1989, the CHNS has been subsequently conducted in 1991, 1993, 1997, 2000, 2004, 2006, 2009, 2011 and 2015. The study population is selected through a multistage, random cluster sampling method across each participating province. The study protocol received approval from the Institutional Review Boards at the University of North Carolina at Chapel Hill and the National Institute of Nutrition and Food Safety, China Centre for Disease Control and Prevention. Written informed consent was obtained from all participants. The study profiles are available in prior publications(Reference Popkin, Du and Zhai21,Reference Zhang, Zhai and Du22) .
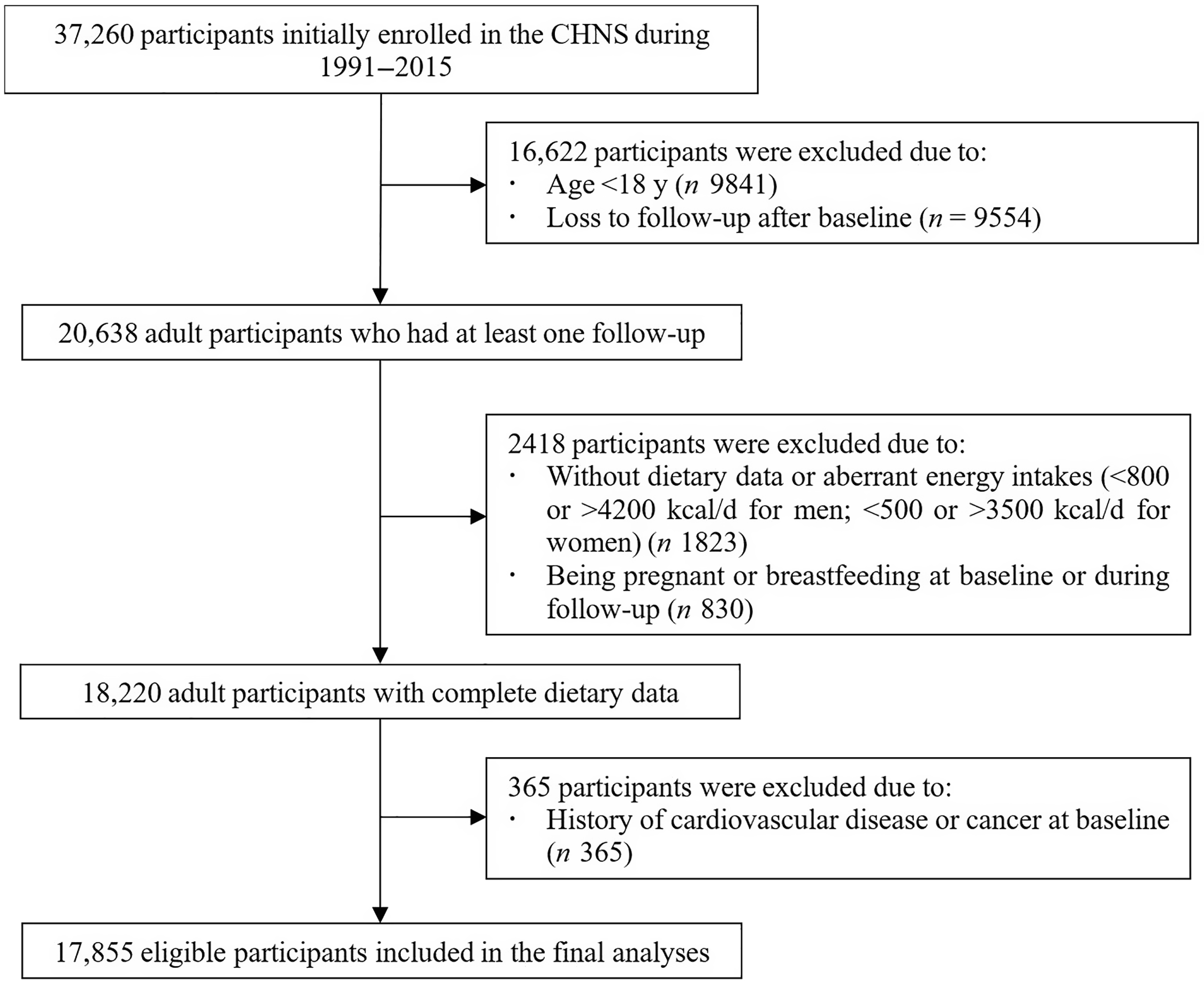
In the current study, we used data from the CHNS 1991–2015 because only children under age 6 and adults aged 20–45 were included in 1989(Reference Zhang, Zhai and Du22). We excluded participants who: (1) were younger than 18 years old, (2) only participated in the baseline survey, (3) had no dietary data or extreme energy intake [< 3347 or > 17573 kJ/d (< 800 or > 4200 kcal/d) for men; < 2092 or > 14644 kJ/d (< 500 or > 3500 kcal/d) for women], (4) were pregnant or breastfeeding at baseline or during follow-up and (5) had CVD or cancer at baseline. Finally, 17 855 participants were eligible for analyses.
Dietary assessment
Dietary intake was assessed repeatedly using three consecutive 24-hour dietary recalls at the individual level, in conjunction with household food consumption, including edible oil and condiments, obtained through weighing and measuring food inventories over the same 3-day period for each survey round. The 3 days were randomly selected and evenly distributed across the week to capture variability in dietary patterns. Cross-checking household and individual intake data allowed accuracy verification. In cases of significant discrepancies, follow-up visits were conducted to resolve inconsistencies and confirm reported food consumption. The accuracy of the dietary method has been validated previously(Reference Zhai, Guo and Popkin23). We estimated the intake of energy and nutrients by multiplying the nutrient content of the standard portion size (100 grams) obtained from the Chinese Food Composition Tables(24–26) with the consumption of each food item. Total choline, choline-containing compounds (free choline, phosphocholine, glycerophosphocholine, phosphatidylcholine and sphingomyelin) and betaine intake were estimated using the USDA Database for the Choline Content of Common Foods, release 2(27). Water-soluble choline was calculated as the sum of free choline, phosphocholine and glycerophosphocholine. Fat-soluble choline was estimated by adding up phosphatidylcholine and sphingomyelin. The ratio of fat-soluble to water-soluble choline was also derived. Nutrient intake was adjusted for total energy intake (2500 kcal/d for men and 2100 kcal/d for women) with the residual method(Reference Willett, Howe and Kushi28). To best represent long-term intake, we calculated the cumulative average intake of total choline, choline-contributing compounds and betaine.
Additionally, we calculated the Chinese Health Eating Index (CHEI) score to quantify the overall diet quality. CHEI includes twelve adequacy components (total grains, whole grains and mixed beans, tubers, total vegetables, dark vegetables, fruits, dairy products, soybeans, fish and seafood, poultry, eggs, seeds and nuts) and five limitation components (red meat, cooking oils, sodium, added sugars and alcohol)(Reference Yuan, Li and Wu29). Each component was scored 0–5 or 0–10(Reference Yuan, Li and Wu29). Total score ranges from 0 to 100, with higher scores indicating better adherence to the Chinese Dietary Guidelines 2016(Reference Yuan, Li and Wu29).
Death ascertainment
The primary outcome was all-cause mortality. Mortality data were collected using household registries through a face-to-face household survey, which was updated during each follow-up round. Trained interviewers asked whether any household members were still living in the household at the time of the survey. If a death or relocation had occurred, the month of the event was documented. The age-specific mortality rates observed in the CHNS aligned with figures from China’s 2000 census and the 2002 Demographic Yearbook(Reference Zimmer, Kaneda and Spess30).
Covariates
Information on demographic characteristics (e.g. age, sex, residence, education level, per capita annual household income and marital status), lifestyle factors (e.g. smoking status, alcohol drinking status and physical activity) and medical history of hypertension, diabetes, CVD and cancer was obtained through structured questionnaires. Per capita annual household income, calculated as annual household income inflated to 2011 by household size, was categorised into tertiles within each survey year. Physical activity level (PAL) was expressed as multiples of basal metabolic rate, using coefficients for different intensities of occupational physical activity (PA) according to the Chinese Dietary Reference Intakes (2000 edition)(31): 1·3 for very light PA in both sexes (working in a sitting position, e.g. office worker, watch repairer, etc.), 1·6 and 1·5 for light PA (working in a standing position, e.g. salesperson, laboratory technician, teacher, etc.), 1·7 and 1·6 for moderate PA (e.g. student, driver, electrician, metal worker, etc.), 2·1 and 1·9 for heavy PA (e.g. farmer, dancer, steel worker, athlete, etc.) and 2·4 and 2·2 for very heavy PA (e.g. loader, logger, miner stonecutter, etc.) in men and women, respectively. Body weight and height were measured after participants removed their shoes, hats and heavy garments using calibrated equipment. BMI was calculated as weight (kg) divided by height squared (m2).
Statistical analysis
Participants provided their person-time data from the baseline (date of the first dietary assessment conducted during adulthood) until the time of death, loss to follow-up, or the end of the latest survey round in 2015, whichever came first. A cumulative average approach was employed to update continuous covariates at each wave, such as total energy intake, BMI, PAL and CHEI score. Missing values for covariates were first imputed using the last observation carried forward method. After imputation, the proportion of missing data for most covariates was low (0·03 % to 3·3 %), except for BMI, which had a higher missing rate (9·1 %). The remaining missing values were subsequently replaced with sex-specific median values for continuous variables and the mode for categorical variables.
We performed all analyses for men and women separately. Participants were classified into five groups according to sex-specific quintiles (Q) of choline and betaine intake. General characteristics were expressed as mean (standard deviation) or median and interquartile range for continuous variables and numbers (percentages) for categorical variables. We used time-dependent Cox proportional hazards regression models to estimate multivariable-adjusted hazard ratios (HR) and 95 % CI with the first quintile as the reference(Reference Amorim and Cai32). We fitted three models introducing potential confounders based on prior knowledge and existing literature. Model 1 was adjusted for age and cumulative average total energy intake. Model 2 was further adjusted for cumulative average BMI, residence (urban or rural areas), education level (middle school or below, high school, or college and above), per capita annual household income level (low, middle or high), marital status (married or unmarried), cumulative average PAL, ever or current smoker (yes or no), current alcohol drinker (yes or no), history of hypertension (yes or no) and history of diabetes (yes or no). Model 3 was additionally adjusted for cumulative average CHEI score and cumulative average betaine or total choline intake (i.e. betaine was adjusted for in models of choline and vice versa). The proportional hazard assumption was examined by using the Schoenfeld residual test. We tested linear trends using the median value within each quintile as a continuous variable. Furthermore, we conducted restricted cubic spline regression analyses, with four knots positioned at the 5th, 35th, 65th and 95th percentiles of the distribution of energy-adjusted cumulative average nutrient intake, to assess nonlinear associations between choline or betaine intake and mortality risk(Reference Harrell33).
In addition, we conducted subgroup analyses to explore whether the association of dietary choline and betaine with all-cause mortality varied by age (< 50 v. ≥ 50 years), marital status (married v. unmarried), education level (middle school or below v. high school and above), per capita annual household income level (low v. middle v. high), BMI (< 24 v. ≥ 24 kg/m2), smoking status (yes v. no), drinking status (yes v. no), PAL (low v. high), history of hypertension (yes v. no) and history of diabetes (yes v. no). We tested interactions between dietary choline and stratified factors using the likelihood ratio test with a multiplicative interaction term.
We performed several sensitivity analyses to check the robustness of the estimated associations. First, we excluded participants with a history of hypertension or diabetes at baseline because participants might have changed their dietary habits after diagnosis of these diseases. Second, we stopped updating the dietary information of individuals who developed CVD or cancer during follow-up. Third, we excluded participants who passed away within the initial two years of follow-up to minimise reverse causation. Finally, we fitted an alternative model by additionally adjusting for the consumption of major food sources of choline or betaine (online Supplementary Table 1) based on Model 2 to control the confounding of other food components in the food rich in choline or betaine.
All statistical analyses were performed using R version 4.4.1 (R Foundation for Statistical Computing). A two-sided P < 0·05 was considered significant.
Results
Participant characteristics
A total of 9027 men and 8828 women were included in the final analysis (Figure 1). The mean (sd) age at baseline was 40·3 (sd 16·1) years for men and 42·4 (sd 16·3) years for women. The mean total choline intake was 238·9 mg/d in men and 213·4 mg/d in women. Phosphatidylcholine was the most abundant choline (135·8 mg/d in men and 122·8 mg/d in women), followed by free choline (59·3 mg/d in men and 52·0 mg/d in women). The top five food sources of total choline were cereals, red meat, eggs, vegetables and beans (online Supplementary Table 1). Water-soluble choline was primarily derived from cereals, vegetables, red meat, beans and tubers. The main contributors to fat-soluble choline intake were eggs, red meat, cereals, beans and white meat. The mean betaine intake was 141·1 mg/d in men and 117·1 mg/d in women. Betaine was mainly sourced from cereals, vegetables, white meat, red meat and condiments. We observed no significant sex differences in major food sources of choline and betaine.
The flow chart of sample selection from the China Health and Nutrition Survey.

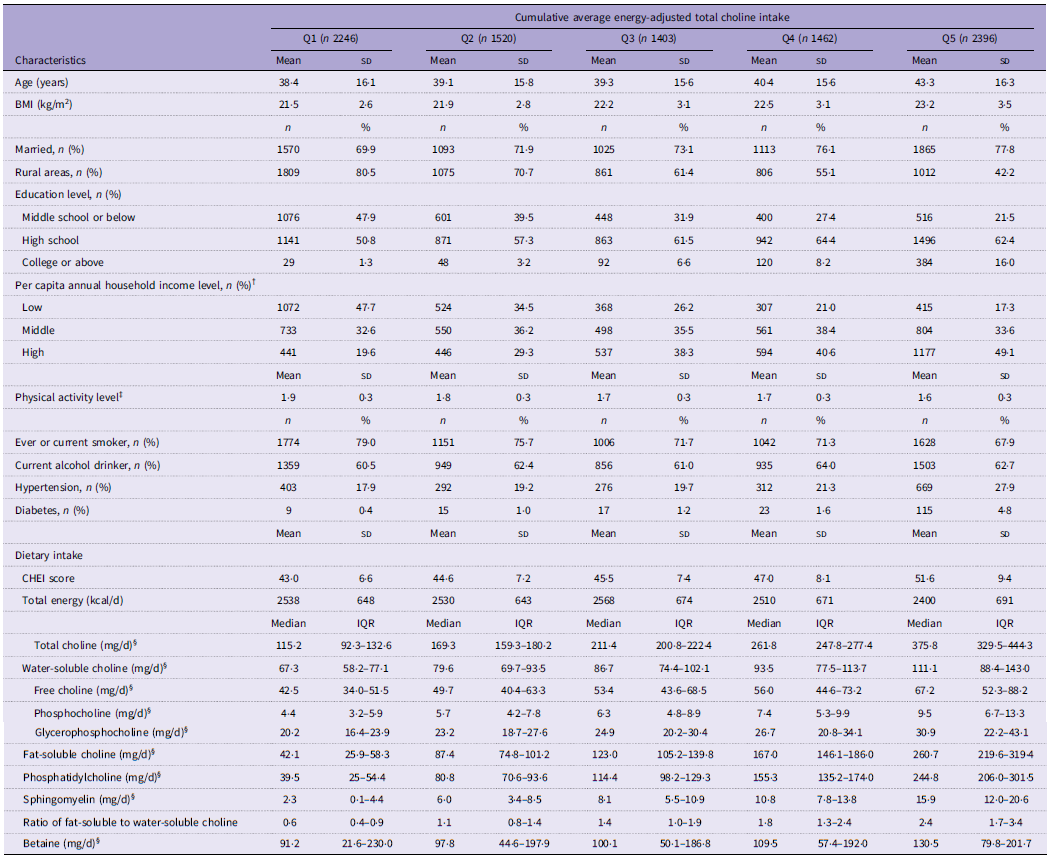
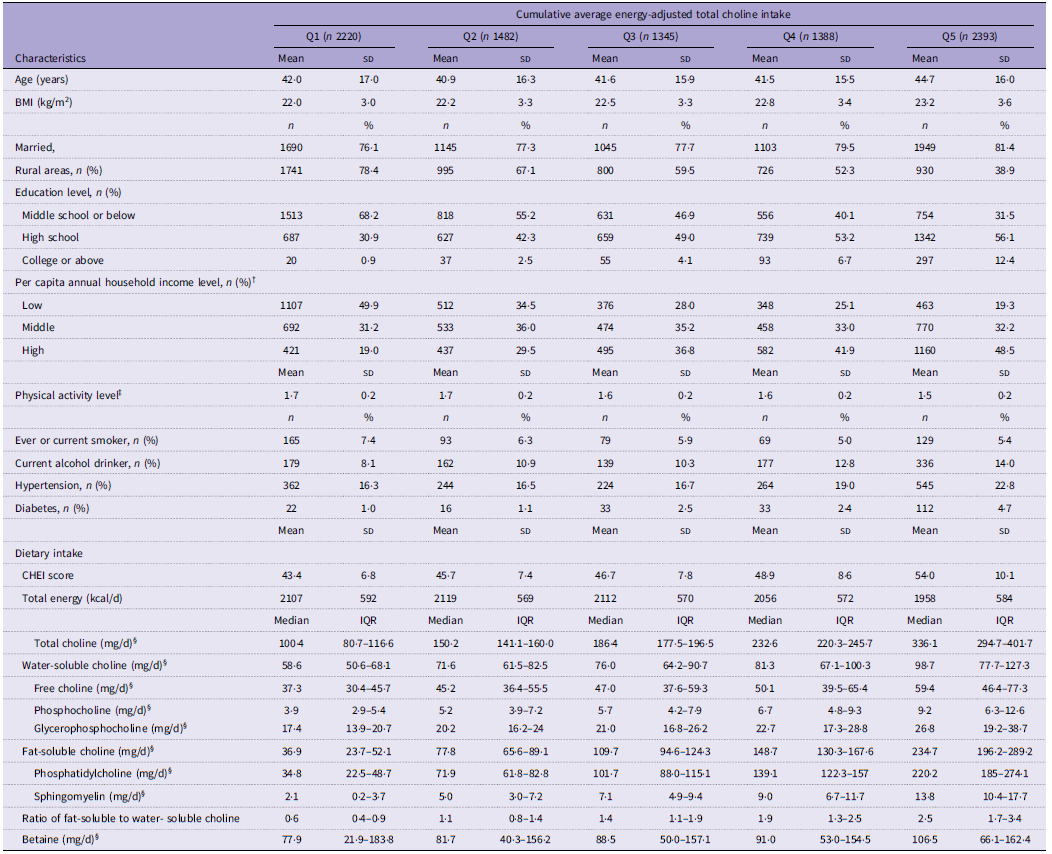
Baseline characteristics of the participants based on quintiles of cumulative average total choline intake are shown in Tables 1 and 2. Men and women with higher total choline intake tended to have higher BMI, higher CHEI scores, greater education and household income levels and lower PAL, were more likely to be married and have a history of hypertension and diabetes, but were less likely to live in rural areas than those with lower intake. Men with higher total choline intake were also older and less likely to be smokers. Women in higher quintiles of total choline intake were more likely to consume alcohol compared with those in lower quintiles. Intakes of all individual choline forms and betaine, as well as the ratio of fat-soluble to water-soluble choline, increased with total choline intake.
Baseline characteristics of the male participants according to quintile of cumulative average energy-adjusted total choline intake in China Health and Nutrition Survey * (Mean values and standard deviations; numbers and percentages; median values and interquartile ranges)

Abbreviations: Q, quintile; CHEI, Chinese Healthy Eating Index.
* Continuous variables were expressed as means (standard deviation) or medians (interquartile range) and categorical variables as numbers (percentages).
† Per capita annual household income was divided into tertiles within each survey year.
‡ Physical activity level was calculated as the ratio of total energy expenditure and basal metabolic rate. In this survey, physical activities were divided into five categories according to the type of professional activities, so we used the multiple of basal metabolic rate as an alternative to physical activity level.
§ Adjusted for average total energy intake using the residual method: 2500 kcal/d for men.
Baseline characteristics of the female participants according to quintile of cumulative average energy-adjusted total choline intake in China Health and Nutrition Survey * (Mean values and standard deviations; numbers and percentages; median values and interquartile ranges)

Abbreviations: Q, quintile; CHEI, Chinese Healthy Eating Index.
* Continuous variables were expressed as means (standard deviation) or medians (interquartile range) and categorical variables as numbers (percentages).
† Per capita annual household income was divided into tertiles within each survey year.
‡ Physical activity level was calculated as the ratio of total energy expenditure and basal metabolic rate. In this survey, physical activities were divided into five categories according to the type of professional activities, so we used the multiple of basal metabolic rate as an alternative to physical activity level.
§ Adjusted for average total energy intake using the residual method: 2100 kcal/d for women.
Association of dietary choline and betaine with all-cause mortality
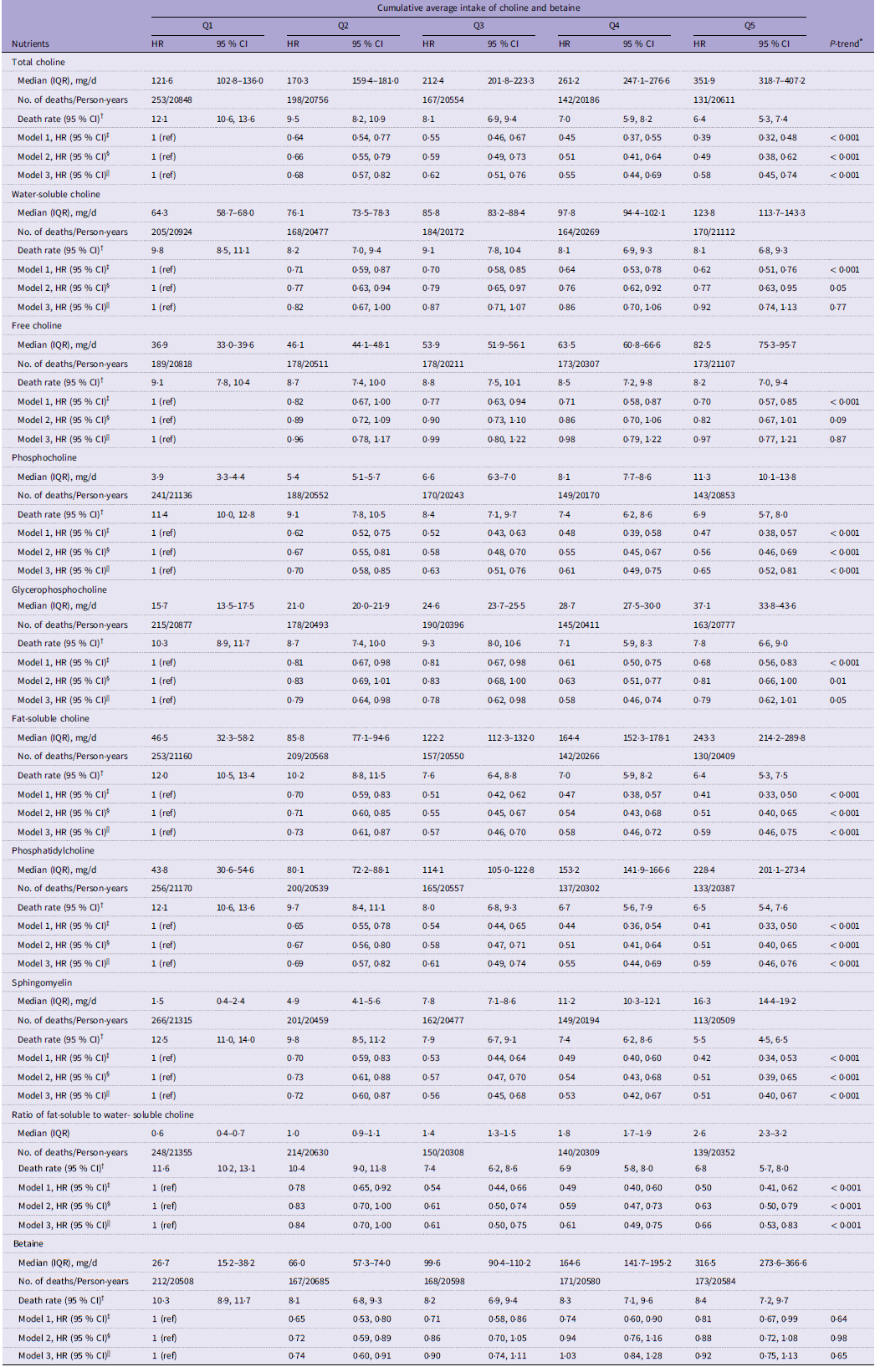
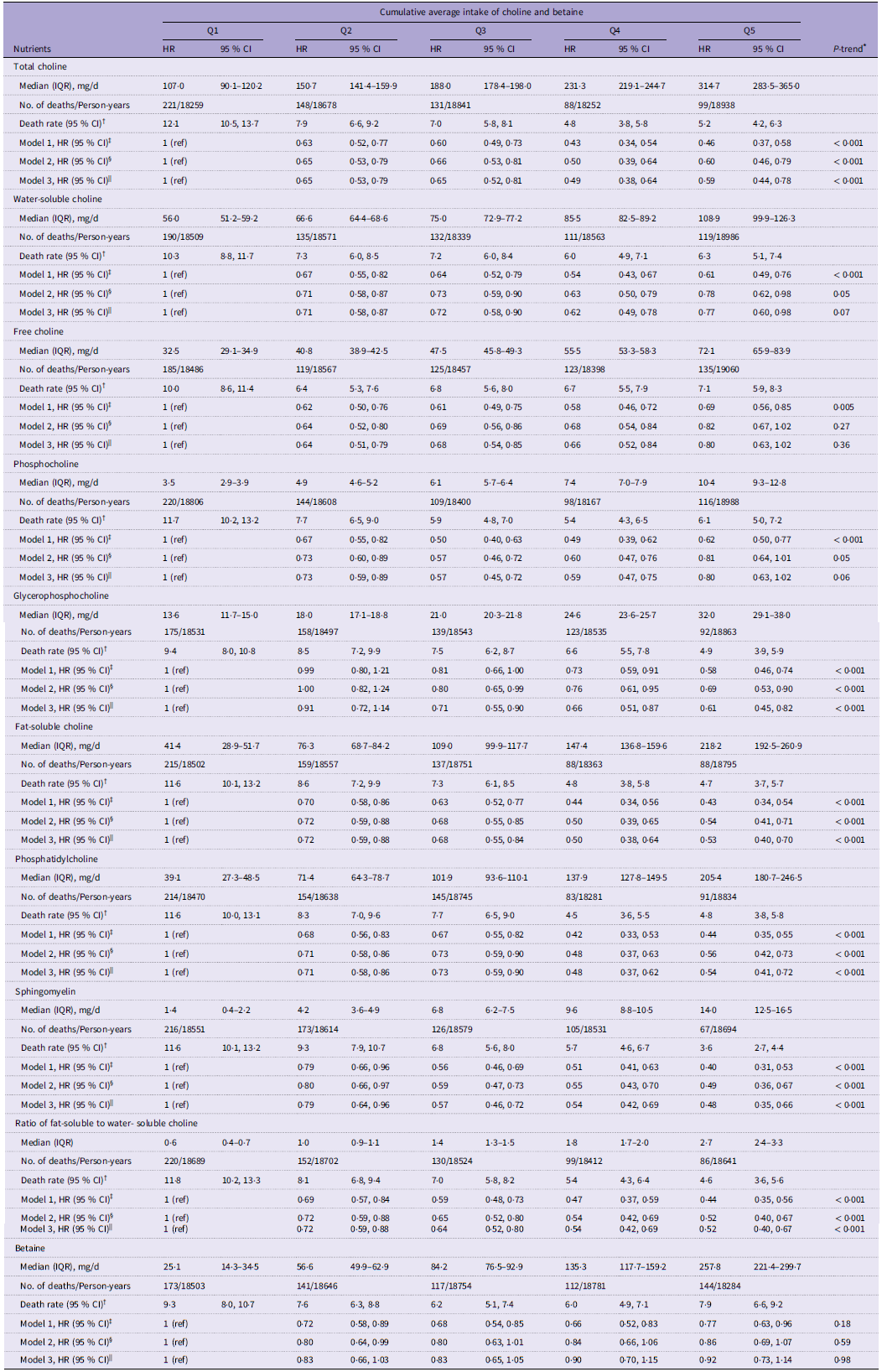
During a median follow-up of 9·1 years and 195 923 person-years at risk, 891 men and 687 women died. Higher total choline intake was associated with a decreased risk of all-cause mortality in both sexes (Tables 3 and 4). With the lowest quintile of total choline intake as the reference, the multivariable-adjusted HR for the second to highest quintiles were 0·68 (95 % CI: 0·57, 0·82), 0·62 (95 % CI: 0·51, 0·76), 0·55 (95 % CI: 0·44, 0·69) and 0·58 (95 % CI: 0·45, 0·74) in men and 0·65 (95 % CI: 0·53, 0·79), 0·65 (95 % CI: 0·52, 0·81), 0·49 (95 % CI: 0·38, 0·64) and 0·59 (95 % CI: 0·44, 0·78) in women (both P-trend < 0·001). Similarly, men and women with higher fat-soluble choline intake had a lower risk of death (Tables 3 and 4). The multivariable-adjusted HR (95 % CI) across quintiles were 1, 0·73 (95 % CI: 0·61, 0·87), 0·57 (95 % CI: 0·46, 0·70), 0·58 (95 % CI: 0·46, 0·72) and 0·59 (95 % CI: 0·46, 0·75) in men and 1, 0·72 (95 % CI: 0·59, 0·88), 0·68 (95 % CI: 0·55, 0·84), 0·50 (95 % CI: 0·38, 0·64) and 0·53 (95 % CI: 0·40, 0·70) in women (both P-trend < 0·001). Water-soluble choline intake was not associated with mortality risk in men (Table 3). However, compared with women in the lowest quintile of water-soluble choline intake, those in the higher quintiles experienced a reduced risk of all-cause mortality (HRQ2–Q5 v. Q1: 0·71 (95 % CI: 0·58, 0·87), 0·72 (95 % CI: 0·58, 0·90), 0·62 (95 % CI: 0·49, 0·78) and 0·77 (95 % CI: 0·60, 0·98)), although no significant linear trend (P-trend = 0·07) (Table 4). A higher fat-soluble to water-soluble choline ratio was associated with a lower risk of all-cause mortality in both sexes (Tables 3 and 4). Compared with quintile 1, the HR of all-cause mortality for quintiles 2 through 5 were 0·84 (95 % CI: 0·70, 1·00), 0·61 (95 % CI: 0·50, 0·75), 0·61 (95 % CI: 0·49, 0·75) and 0·66 (95 % CI: 0·53, 0·83) in men and 0·72 (95 % CI: 0·59, 0·88), 0·64 (95 % CI: 0·52, 0·80), 0·54 (95 % CI: 0·42, 0·69) and 0·52 (95 % CI: 0·40, 0·67) in women (both P-trend < 0·001).
Hazard ratios (HR) and 95 % CI of all-cause mortality according to quintile of cumulative average energy-adjusted choline and betaine intake in men

Abbreviations: Q, quintile; IQR, interquartile; No., number; HR, hazard ratio; CHEI, Chinese Healthy Eating Index.
* Linear trends across the quintiles were tested using a continuous variable with the median values in each quintile.
† Death rate, per 1000 person-years.
‡ Model 1 was adjusted for age (years, continuous) and total energy intake (kcal/d, continuous).
§ Model 2 was adjusted for the covariates in model 1 plus BMI (kg/m2, continuous), residence (urban, rural), education level (middle school or below, high school, college or above), household income level (low, middle, high), marital status (married, unmarried), physical activity level (continuous), ever or current smoker (yes, no), current alcohol drinker (yes, no), history of hypertension (yes, no), and history of diabetes (yes, no).
|| Model 3 was adjusted for the covariates in model 2 plus CHEI score (continuous), and energy-adjusted betaine/choline intake (mg/d, continuous; betaine was adjusted for in models of choline and vice versa).
Hazard ratios (HR) and 95 % CI of all-cause mortality according to quintile of cumulative average energy-adjusted choline and betaine intake in women

Q, quintile; IQR, interquartile; No., number; HR, hazard ratio; CHEI, Chinese Healthy Eating Index.
* Linear trends across the quintiles were tested using a continuous variable with the median values in each quintile.
† Death rate, per 1000 person-years.
‡ Model 1 was adjusted for age (years, continuous) and total energy intake (kcal/d, continuous).
§ Model 2 was adjusted for the covariates in model 1 plus BMI (kg/m2, continuous), residence (urban, rural), education level (middle school or below, high school, college or above), household income level (low, middle, high), marital status (married, unmarried), physical activity level (continuous), ever or current smoker (yes, no), current alcohol drinker (yes, no), history of hypertension (yes, no) and history of diabetes (yes, no).
|| Model 3 was adjusted for the covariates in model 2 plus CHEI score (continuous) and energy-adjusted betaine/choline intake (mg/d, continuous; betaine was adjusted for in models of choline and vice versa).
Regarding individual choline-contributing compounds, intakes of phosphocholine (HRQ5 v. Q1 = 0·65 (95 % CI: 0·52, 0·81)), phosphatidylcholine (HRQ5 v. Q1 = 0·59 (95 % CI: 0·46, 0·76)) and sphingomyelin (HRQ5 v. Q1 = 0·51 (95 % CI: 0·40, 0·67)) were inversely associated with the risk of all-cause mortality in men (all P-trend < 0·001) (Table 3). Free choline intake was not related to mortality risk in men, while men in the medium quintiles of glycerophosphocholine intake had a lower mortality risk compared to those in the bottom quintile (HRQ2–Q4 v. Q1 = 0·79 (95 % CI: 0·64, 0·98), 0·78 (95 % CI: 0·62, 0·98) and 0·58 (95 % CI: 0·46, 0·74); P-trend = 0·05) (Table 3). In women, higher intakes of glycerophosphocholine (HRQ5 v. Q1 = 0·61 (95 % CI: 0·45, 0·82)), phosphatidylcholine (HRQ5 v. Q1 = 0·54 (95 % CI: 0·41, 0·72)) and sphingomyelin (HRQ5 v. Q1 = 0·48 (95 % CI: 0·35, 0·66)) were linked with a reduced risk of death (all P-trend < 0·001) (Table 4). However, women with moderate intake of free choline (HRQ2–Q4 v. Q1 = 0·64 (95 % CI: 0·51, 0·79), 0·68 (95 % CI: 0·54, 0·85) and 0·66 (95 % CI: 0·52, 0·84); P-trend = 0·36) and phosphocholine (HRQ2–Q4 v. Q1 = 0·73 (95 % CI: 0·59, 0·89), 0·57 (95 % CI: 0·45, 0·72) and 0·59 (95 % CI: 0·47, 0·75); P-trend = 0·06) experienced a lower risk of all-cause mortality than those with low intake (Table 4). No association between betaine intake and all-cause mortality risk was found in either men or women (Tables 3 and 4).
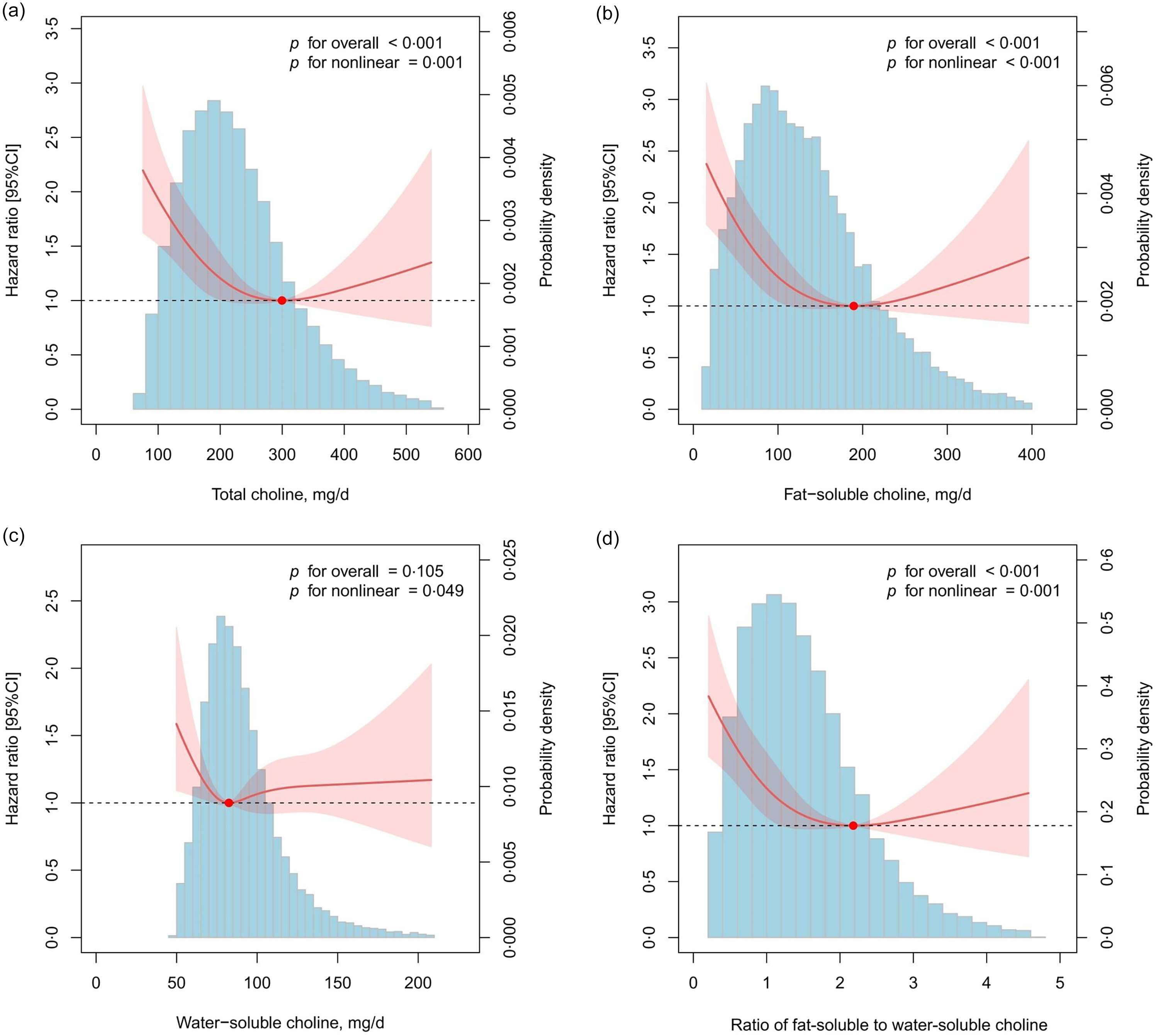
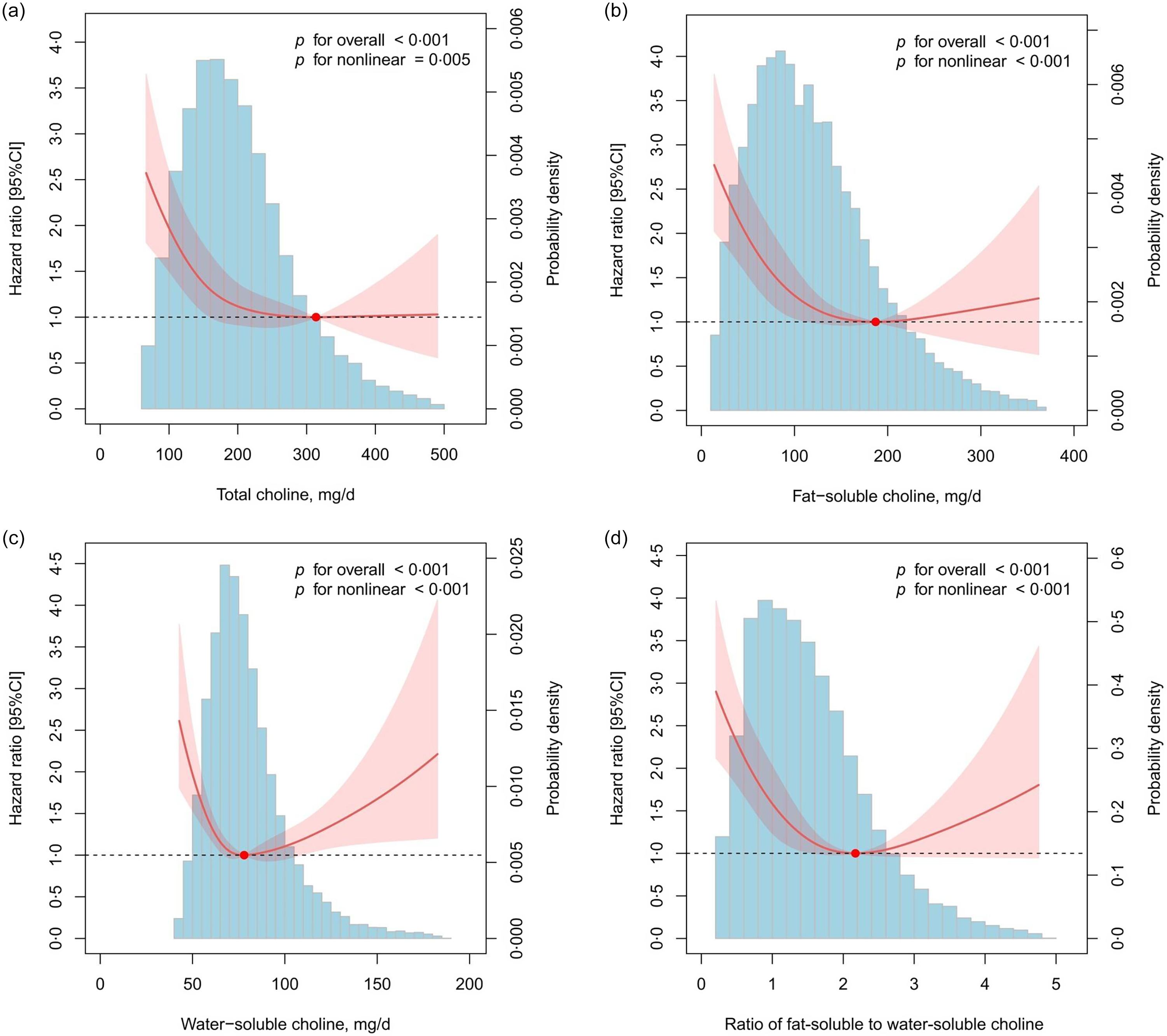
Restricted cubic spline analyses further revealed a reverse J-shaped association between total choline intake and all-cause mortality risk in men (P-nonlinear = 0·001; Figure 2(a)) and an L-shaped association in women (P-nonlinear = 0·005; Figure 3(a)), both with an inflection point at around 300 mg/d. The dose–response curve for fat-soluble choline intake followed a reverse J-shape in both sexes, with a turning point at approximately 200 mg/d (both P-nonlinear < 0·001; Figures 2(b) and 3(b)). Interestingly, a J-shaped association between water-soluble choline intake and all-cause mortality risk was observed in women, with an inflection point at approximately 75 mg/d (P-nonlinear < 0·001; Figure 3(c)), while a null association was found in men (Figure 2(c)). In addition, we found a reverse J-shaped association between ratio of fat-soluble to water-soluble choline and all-cause mortality risk in both sexes (both P-nonlinear ≤ 0·001; Figure 2(d) and 3(d)). A fat-soluble to water-soluble choline ratio of 2·2 was associated with the lowest risk for all-cause death. For individual choline forms, we observed reverse J-shaped associations of dietary phosphocholine, glycerophosphocholine, phosphatidylcholine and sphingomyelin with the risk of all-cause mortality (all P-nonlinear < 0·005), while no link was found between free choline intake and death risk in men (online Supplementary Figure 1). In women, the dose–response curves for free choline and phosphocholine intake displayed a J-shaped pattern, whereas those for phosphatidylcholine and sphingomyelin intake showed a reverse J shape (all P- nonlinear < 0·001; online Supplementary Figure 2). Additionally, there was a linear association between glycerophosphocholine intake and all-cause mortality in women (P-overall < 0·001, P-nonlinear = 0·084).
Nonlinear association between cumulative average energy-adjusted dietary intake of total (a), fat-soluble (b), water-soluble choline (c) and ratio of fat-soluble to water-soluble choline (d) and all-cause mortality in men. The red solid lines represent multivariable-adjusted HR, and the shaded areas represent their 95 % CI. The reference lines are denoted by the black dashed lines at a HR of 1·0. The blue histograms show the fraction of the participants (density) with different choline/betaine intakes. To minimise the potential effects of extreme values, participants with the bottom 1 % and top 1 % of choline intake were excluded from the analysis. The reference was the value corresponding to the lowest HR. Four knots were fitted at the 5th, 35th, 65th and 95th percentiles. Analysis was adjusted for age (years, continuous), total energy intake (kcal/d, cumulative average), BMI (kg/m2, cumulative average), residence (urban or rural areas), education level (middle school or below, high school, or college or above), household income level (low, middle, or high), marital status (married or unmarried), PAL (cumulative average), ever or current smoker (yes or no), current alcohol drinker (yes or no), history of hypertension (yes or no), history of diabetes (yes or no), CHEI score (cumulative average) and energy-adjusted betaine intake (mg/d, cumulative average).

Nonlinear association between cumulative average energy-adjusted dietary intake of total (a), fat-soluble (b), water-soluble choline (c) and ratio of fat-soluble to water-soluble choline (d) and all-cause mortality in women. The red solid lines represent multivariable-adjusted HR, and the shaded areas represent their 95 % CI. The reference lines are denoted by the black dashed lines at a HR of 1·0. The blue histograms show the fraction of the participants (density) with different choline/betaine intakes. To minimise the potential effects of extreme values, participants with the bottom 1 % and top 1 % of choline intake were excluded from the analysis. The reference was the value corresponding to the lowest HR. Four knots were fitted at the 5th, 35th, 65th and 95th percentiles. Analysis was adjusted for age (years, continuous), total energy intake (kcal/d, cumulative average), BMI (kg/m2, cumulative average), residence (urban or rural areas), education level (middle school or below, high school, or college or above), household income level (low, middle, or high), marital status (married or unmarried), PAL (cumulative average), ever or current smoker (yes or no), current alcohol drinker (yes or no), history of hypertension (yes or no), history of diabetes (yes or no), CHEI score (cumulative average) and energy-adjusted betaine intake (mg/d, cumulative average).

Subgroup analyses
No significant interactions between total choline intake and stratified factors were observed in men (online Supplementary Table 2). In women, the choline-mortality association was modified by diabetes status (P–interaction = 0·04) (online Supplementary Table 3). When stratified by diabetes status, the inverse association was only significant in women without a history of diabetes.
Sensitivity analyses
The association between dietary choline or betaine intake and all-cause mortality remained robust after excluding participants with a history of hypertension or diabetes at baseline (online Supplementary Tables 4 and 5), stopping updating dietary intake after diagnosis of CVD or cancer during follow-up (online Supplementary Tables 6 and 7), excluding deaths occurred within the first 2 years of follow-up (online Supplementary Tables 8 and 9) and further adjusting for major food sources of choline or betaine (online Supplementary Tables 10 and 11). An exception was that betaine intake became inversely associated with all-cause mortality risk after additional adjustment for consumption of cereals, vegetables, white meat, red meat and condiments (P-trend = 0·004 for men and 0·002 for women; online Supplementary Tables 10 and 11).
Discussion
In this large population-based prospective cohort of Chinese adults, the risk patterns of all-cause mortality with total choline intake were reverse J-shaped in men and L-shaped in women. At low intake levels, higher total choline intake was associated with a reduced risk of all-cause mortality; however, when total choline intake surpassed a certain threshold (∼300 mg/d), the mortality risk no longer decreased with increasing choline intake. Dietary fat-soluble choline (phosphatidylcholine and sphingomyelin) had a reverse J-shaped association with all-cause mortality in both sexes, where mortality risk decreased with higher fat-soluble choline intake until approximately 200 mg/d. Intriguingly, we observed a J-shaped association between dietary water-soluble choline (primarily free choline) and all-cause mortality in women, but a null association in men. An optimal ratio of fat-soluble to water-soluble choline was around 2·2 in both sexes. Both low and high intake of water-soluble choline were associated with an elevated risk of mortality compared with moderate intake (∼75 mg/d) in women. Betaine intake was not associated with all-cause mortality in either sex.
In line with our findings, a recent follow-up study of the US National Health and Nutrition Examination Survey 2011–2018 reported a similar nonlinear association with reduced risk of all-cause mortality at moderate total choline intake(Reference Peng, Zhang and Cai11). In contrast, an earlier cohort study using National Health and Nutrition Examination Survey data from 1999 to 2010 found that higher total choline intake was associated with an increased risk of all-cause mortality(Reference Mazidi, Katsiki and Mikhailidis9). Likewise, the Shanghai Men’s and Women’s Health Studies observed a positive association between total choline intake (mean: 297 mg/d) and all-cause mortality(Reference Yang, Lipworth and Shu10). The Southern Community Cohort Study also reported a positive association between total choline intake and all-cause mortality in black Americans (mean: 404 mg/d), but not in white Americans (mean: 362 mg/d)(Reference Yang, Lipworth and Shu10). However, the Västerbotten Intervention Programme study found no significant association in Swedish adults (mean: 278 mg/d in men and 255 mg/d in women)(Reference Karlsson, Winkvist and Strid12). Of note, our participants had much lower total choline intake (mean: 239 mg/d in men and 213 mg/d in women) compared with other populations (mean: 255∼404 mg/d)(Reference Mazidi, Katsiki and Mikhailidis9–Reference Karlsson, Winkvist and Strid12), which may partially explain the observed nonlinear association of both lower and potentially higher total choline intake with increased all-cause mortality risk in our study.
Different forms of choline exhibit variations in absorption and metabolism, although they are interconverted in the body(Reference Zeisel, Mar and Howe2). Few studies have examined the association between intakes of individual choline forms and all-cause mortality. In the Nurses’ Health Study and Health Professionals Follow-up Study, higher phosphatidylcholine intake was associated with an increased risk of all-cause mortality in American men and women, while other forms of choline were not investigated(Reference Zheng, Li and Rimm8). Similarly, the Southern Community Cohort Study reported a positive association between phosphatidylcholine intake and all-cause mortality in both black and white Americans; however, the positive association between dietary sphingomyelin, free choline and phosphocholine and all-cause mortality risk was only significant in black Americans(Reference Yang, Lipworth and Shu10). In contrast to the US cohorts, dietary phosphatidylcholine and phosphocholine were not related to all-cause mortality in the Shanghai Men’s and Women’s Health Studies, whereas free choline intake was positively associated with and glycerophosphocholine and sphingomyelin intake were inversely associated with all-cause mortality(Reference Yang, Lipworth and Shu10). In the Västerbotten Intervention Programme study, Swedish men in the medium quintiles of phosphatidylcholine, phosphocholine and free choline intake and Swedish women in the medium quintiles of glycerophosphocholine intake had significantly lower risks of all-cause mortality than those in the first quintiles, suggesting moderate intake of these choline forms associated with reduced all-cause mortality risk(Reference Karlsson, Winkvist and Strid12). Nevertheless, the authors failed to identify these potential non-linear associations in their analyses. Additionally, higher free choline intake was linked to a decreased risk of all-cause mortality in Swedish women(Reference Karlsson, Winkvist and Strid12). Inconsistent with these findings, we observed that the risk of all-cause mortality decreased dramatically when intakes of total and individual fat-soluble choline (phosphatidylcholine and sphingomyelin) fell below certain limits in Chinese men and women. However, in terms of water-soluble choline, increased risks of all-cause mortality were observed at lower phosphocholine and glycerophosphocholine intake, and free choline intake was not associated with all-cause mortality in Chinese men. Nevertheless, both lower and higher intake of free choline and phosphocholine were related to elevated all-cause mortality risks, and glycerophosphocholine intake was inversely linked to all-cause mortality in Chinese women.
We further observed a reverse J-shaped association between the ratio of fat-soluble to water-soluble choline and all-cause mortality, with an inflection point around 2·2 in both sexes, which has not been reported in previous studies. The balance between fat-soluble and water-soluble choline may influence absorption, transport, tissue targeting and physiological functions of choline in the body(Reference Goh, Cheam and Wang34,Reference Cho, Aardema and Bunnell35) . Fat-soluble choline forms are transported in lipoproteins and play key roles in cell membrane integrity, lipid transport and cellular signalling(Reference Goh, Cheam and Wang34). In contrast, water-soluble forms are more readily available in plasma and may be preferentially utilised for neurotransmitter synthesis (e.g. acetylcholine) and methylation pathways (e.g. via betaine)(Reference Goh, Cheam and Wang34). This ratio may offer additional insight into refining choline intake recommendations, particularly for individuals with liver dysfunction, metabolic syndrome or cardiovascular risk.
The discrepancy is likely due to differences in dietary patterns, food sources of choline, genetic variants related to choline metabolism and gut microbial production of TMAO across populations. Traditional Chinese diets are primarily plant-based and rich in cereals and vegetables, whereas Western diets contain a large amount of red meat, eggs and dairy products(Reference Zhao, Liu and Yu15). Red meat, eggs and dairy are primary food sources of choline in Western populations(Reference Vennemann, Ioannidou and Valsta18,Reference Wallace and Fulgoni19) , while plant foods such as cereals, vegetables and beans contribute considerable choline to total intake in our study population. Gut microbiome composition and diversity vary geographically and racially(Reference Gupta, Paul and Dutta36). Western diets and carbohydrate-based diets had different microbiota enterotypes affecting microbiota-choline metabolism(Reference Arias, Arboleya and Allison37). An animal experiment found that choline or TMAO supplementation in a Western diet promoted the development of atherosclerosis by altering intestinal microbiota composition and bile acid metabolism, whereas in a standard chow diet, supplementation with choline or TMAO affected atherosclerosis through different mechanisms(Reference Mu, Zhao and Zhang38). In addition, variants in the genes encoding choline kinase-α, choline dehydrogenase, methylenetetrahydrofolate reductase, phosphatidylethanolamine N-methyltransferase and flavin monooxygenase isoform 3 may alter choline metabolism and consequently impact dietary requirements for choline(Reference Silver, Corbin and Hellenthal39,Reference Ganz, Klatt and Caudill40) . The allele frequencies of these genes exhibit considerable variation among American, African and Chinese descendants(Reference Silver, Corbin and Hellenthal39,Reference Bennett, Parish and Millwood41) , indicating potential population-specific associations.
Our findings are biologically plausible. Choline plays a dual role in human health. As an essential nutrient, choline provides methyl groups for methylation reactions and homocysteine reduction(Reference Niculescu and Zeisel42,Reference Lee, Jacques and Dougherty43) . Choline (especially phosphatidylcholine and sphingomyelin) is also a crucial precursor for synthesising phospholipids, vital for maintaining cell membrane stability and lipid metabolism in the liver(Reference Ueland44,Reference Corbin and Zeisel45) . Additionally, choline serves as a precursor of the neurotransmitter acetylcholine(Reference Blusztajn, Slack and Mellott46). Adequate choline intake supports normal DNA methylation and synthesis of phospholipid and acetylcholine, promoting cardiovascular, liver and brain health. However, excessive choline intake may lead to abnormal methylation and promote the formation of TMAO, increasing the risk of cancer and CVD(Reference Kulis and Esteller47,Reference Thomas and Fernandez48) .
The sex difference in the association between dietary choline and all-cause mortality may be driven by multiple biological factors. Sex hormones influence not only the de novo synthesis of choline(Reference Young49) but also the composition and metabolic function of the gut microbiome(Reference Ahmed and Spence50). In addition, sex-specific differences in one-carbon metabolism may contribute to the association. Prior studies have shown that choline intake is differentially associated with circulating one-carbon metabolites in men and women, potentially due to differential expression or regulation of enzymes such as methylenetetrahydrofolate reductase and betaine-homocysteine methyltransferase(Reference Sadre-Marandi, Dahdoul and Reed51,Reference Van Parys, Brække and Karlsson52) . In the case of free choline, which is highly bioavailable and rapidly absorbed, excessive intake may potentially lead to metabolic imbalances or dysregulation of methylation pathways(Reference Mödinger, Schön and Wilhelm53). This effect may be more pronounced in women, who could be more sensitive to such metabolic perturbations. However, this finding should be interpreted with caution and warrants further investigation to determine whether it reflects a true biological effect.
Our subgroup analyses suggest that a history of diabetes may modify the association between choline intake and all-cause mortality in women, where the protective association was only pronounced in women free from diabetes but not among those with a history of diabetes. No such interactions were observed in men. These findings were supported by a Canadian cross-sectional study, which showed that higher choline intake was associated with lower insulin resistance in women, rather than in men(Reference Gao, Wang and Sun54). Plasma concentrations of TMAO were higher in diabetics than in non-diabetics(Reference Tang, Wang and Li55), which may counteract the protective effect of high choline in the current study. However, in contrast to our findings, three racially diverse cohort studies reported that higher total choline intake was associated with an increased risk of death, especially among participants with a history of diabetes(Reference Yang, Lipworth and Shu10). The inconsistency is likely attributed to the relatively low total choline intake in our study, which may be insufficient to reveal any harmful effects. Further studies are needed to elucidate the underlying mechanisms.
We found a null association between betaine intake and all-cause mortality in Chinese men and women. Aligning with our findings, the Southern Community Cohort Study reported that betaine intake was not associated with all-cause mortality in black and white Americans(Reference Yang, Lipworth and Shu10). However, a positive link between betaine intake and all-cause mortality was observed in the Shanghai Men’s and Women’s Health Studies(Reference Yang, Lipworth and Shu10). Inconsistently, the Västerbotten Intervention Programme study found an inverse association between betaine intake and overall mortality in Swedish women, potentially due to their high consumption of whole grains(Reference Karlsson, Winkvist and Strid12).
Strengths of this study include a large sample size, a long follow-up period and repeated dietary assessments, which allowed us to examine the long-term associations of dietary choline and betaine with all-cause mortality. However, our study also has some limitations. First, we lacked information on the cause of death in the CHNS, which precludes us from further analysing the association between dietary choline or betaine and cause-specific mortality. Second, 3-day 24-hour dietary recalls have inherent limitations in capturing habitual intake of choline and betaine due to the daily variations in food selection. However, we addressed this methodological constraint by calculating the cumulative average intake across multiple survey cycles, which provides more robust and representative estimates of long-term dietary exposure. In addition, the choline and betaine content of foods borrowed from the USDA database may not be fully accurate due to differences in food types, places of origin and cooking methods between American and Chinese populations. Third, residual confounding is possible despite our comprehensive adjustments for potential confounders. Fourth, while the CHNS covers diverse provinces, socio-economic groups and both urban and rural populations, offering broad representativeness, caution is needed when generalising findings to the entire Chinese population. However, the multistage, random cluster sampling method ensured good representativeness within each surveyed province. Finally, our findings should be interpreted cautiously when generalising to other populations with different dietary habits and genetic backgrounds.
In summary, our results indicate that adequate intake of choline, rather than betaine, is associated with reduced risk of all-cause mortality in Chinese men and women with predominantly plant-based diets; however, excessive intake of water-soluble choline, especially free choline, might promote death in women. Notably, we found that the association between choline intake and mortality was not always linear; both too little and possibly too much intake of certain choline types may increase the risk of death. Both total choline intake and individual choline forms should be considered due to differences in dietary habits and genetic backgrounds in diverse populations.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525103759
Acknowledgements
This research uses data from the China Health and Nutrition Survey (CHNS). We are grateful to research grant funding from the National Institute for Health (NIH), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) for R01 HD30880 and R01 HD38700, National Institute on Aging (NIA) for R01 AG065357, National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) for R01 DK104371 and P30 DK056350, National Heart, Lung and Blood Institute (NHLBI) for R01 HL108427, the NIH Fogarty grant D43 TW009077, the Carolina Population Center for P2C HD050924 and P30 AG066615 since 1989 and the China-Japan Friendship Hospital, Ministry of Health for support for CHNS 2009, Chinese National Human Genome Center at Shanghai since 2009, and Beijing Municipal Center for Disease Prevention and Control since 2011. We thank the National Institute for Nutrition and Health, China Center for Disease Control and Prevention, Beijing Municipal Center for Disease Control and Prevention and the Chinese National Human Genome Center at Shanghai.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Authorship
P. T. and A. F. contributed to the conception of the study and designed the research; P. T., P. C., S. W. and A. F. contributed to data collating; P. T. analysed data and wrote the first draft of the manuscript; J. L., J. S. and D. L. edited and reviewed the manuscript; A. F. critically revised the manuscript. A.F. had primary responsibility for the final content. All authors read and approved the final version of the manuscript.
Declaration of Interests
The author(s) declare none.
Data availability
Data described in the manuscript, code book and analytic code will be shared on reasonable request to the corresponding authors.